

Abstract
Objective:
To assess the morphology and dimensions of mandibular symphysis (MS) in different anteroposterior jaw relationships and to investigate whether craniofacial parameters have any correlation with its shape and/or dimensions.
Materials and Methods:
Lateral cephalograms of subjects with Class I, Class II, and Class III skeletal relationships were traced. Several craniofacial and MS parameters were measured. MS parameters were compared between the three groups using analysis of variance and were correlated with the craniofacial parameters using the Pearson correlation coefficient.
Results:
Larger angle of concavity of the chin, more inclination of the alveolar bone toward the mandibular plane, and larger MS dimensions and area (P < .001) were found with a Class III skeletal relationship compared to Class I and Class II relationships. The Pearson correlation coefficient between Id-Me and AFH was r = 0.83 and between Id-Me and LAFH it was r = 0.81.
Conclusions:
The dimensions and configuration of MS in the Class III relationship were different than those in Class I and Class II relationships; the alveolar part of MS compensated for the skeletal relationship in the Class III pattern. MS dimensions were strongly correlated to anterior facial dimensions.
Keywords: Mandibular symphysis, Anteroposterior jaw relationships
INTRODUCTION
Mandibular symphysis (MS) morphology has an impact on diagnosis and treatment planning in orthodontic patients; it serves as a reference anatomical landmark for esthetics and beauty of the face in general and of the lower part in particular.1,2 Additionally, MS has been considered as one of the predictors for the direction of mandibular growth rotation.3
MS morphology is a complex phenotype that results from the interplay of different genetic, nongenetic, and adaptive factors.4–6 Functional environment has been claimed7–9 to affect the shape and size of MS, such that MS demonstrates an adaptive morphological response to the biomechanical loads experienced at various points in the masticatory cycle. Other factors that may affect the morphology and/or dimension of MS are vertical jaw relationships10,11 and inclination of the lower incisors.12 Inclination of the lower incisors may indirectly affect the shape of MS during the growth period; dentoalveolar compensation occurring during that period as a result of anteroposterior (AP) jaw discrepancy might be reflected in the morphology and dimension of MS.
Vertical growth direction may have an indirect effect on the AP position of the mandible and, subsequently, on MS. However, no studies have been carried out to investigate the relationship between MS and AP jaw discrepancies.
The aims of this study were to assess the morphology and dimensions of the MS in different AP skeletal jaw relationships, to assess if the alveolar part of MS compensates for the skeletal relationship, and to investigate whether different craniofacial parameters have any correlation with its shape and/or dimensions.
MATERIALS AND METHODS
Three hundred and fifty-four lateral cephalograms for adult subjects (176 females and 178 males with mean ages of 22.3 ± 2.9 years and 22.5 ± 2.6 years, respectively) were selected from the pretreatment orthodontic records of patients attending the orthodontic clinics at the Dental Teaching Center/Jordan University of Science and Technology (JUST). Ethical approval to access patients' files was granted by the Institutional Research Board at JUST. Lateral cephalograms were taken for the participants in centric occlusion with lips in repose and Frankfort Plane Horizontal according to natural head position, using an Orthoslice 1000 C (Marne La Vallee Cedex 2, France) with a cephalostat at 64 KVp, 16 Ma, and 0.64 seconds' exposure, as recommended by the manufacturer. Individuals with a history of orthodontic treatment, orthognathic surgery, craniofacial anomalies, or a history of trauma to the mandible were excluded from the study. All subjects had a maxillary to mandibular plane angle that was within normal limits for Jordanians (25.5° ± 5.3°).13
The radiographs were selected according to their skeletal AP jaw relationship (Class I, Class II, or Class III relationship). Class I skeletal relationship was considered when ANB angle = 3° ± 1°, Class II skeletal relationship was considered when ANB angle was >4°, and Class III skeletal relationship was considered when ANB angle was <2°.13 The three groups had similar age and gender distributions (Table 1).
Table 1.
Sample Distribution According to Gender and Anteroposterior Skeletal Jaw Relationship

Lateral cephalograms were traced manually in a dark room using matt acetate tracing paper attached to the radiographs. Points and lines were marked with a 3H pencil. When bilateral structures did not overlap, distances were halved. The cephalometric measured parameters are shown in Table 2.
Table 2.
Definition of the Craniofacial and Dentoalveolar Cephalometric Parameters

MS was traced on each lateral cephalogram. The configuration of MS was drawn on acetate paper using a 3H pencil. All MS tracings were scanned into a computer and processed through a custom-made software program (TechExpert 1.10). When the image of MS appeared inside a special window of the software, it was possible to identify and digitize six points yielding to five angular and five linear measurements to describe the morphology and dimensions of MS. The area of MS was also assessed. All of the variables were measured by the software. The allocated points and measured parameters are defined in Table 3 and illustrated in Figures 1–3. Magnification of linear distances due to scanning was compensated for by the software.
Table 3.
Definition of the Symphysis Points and Measured Parameters

Figure 1.
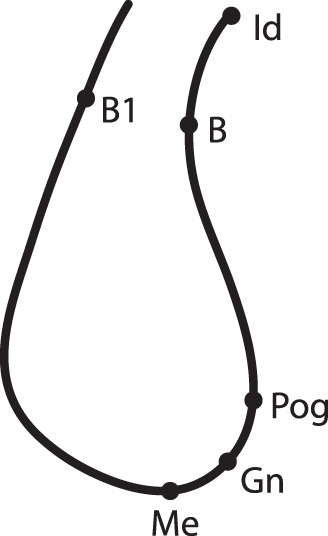
Cephalometric points identified on the mandibular symphysis.
Figure 2.

Angular parameters measured on the mandibular symphysis.
Figure 3.
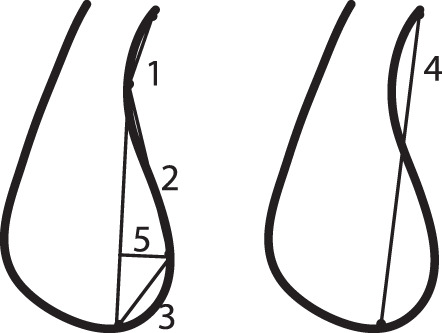
Linear parameters measured on the mandibular symphysis.
Measurement Error
Forty scanned MS were randomly selected to determine measurement error in this study. Digitizing and measurements of the selected scans were repeated for a second time by the same examiner (Dr Al-Khateeb) after a 1-month interval. The method error was calculated using Dahlberg's double determination formula.14 The Houston coefficient of reliability was also calculated.15
Houston's coefficient of reliability was above 92%. The values of Dahlberg error ranged between 0.38° (B-B1-Gn angle) and 0.78° (B-Pog-Me angle) for angular measurements and measured 0.27 mm for the linear measurements.
Statistical Analysis
Means and standard deviations for the cephalometric parameters and those describing MS were calculated for all of the variables using the Statistical Package for the Social Science (SPSS version 19, Chicago, Ill).
General linear model analysis was employed to investigate differences between the measured MS parameters in the three AP groups. Differences between males and females for the total sample were assessed using the t-test for two independent samples. The Pearson correlation coefficient was calculated to assess the relationship between the MS parameters on one hand and craniofacial and dentoalveolar parameters on the other hand. The results of the test were considered to be significant at P < .05.
RESULTS
Different configurations of MS were noticed within the different AP jaw relationships (Figure 4).
Figure 4.
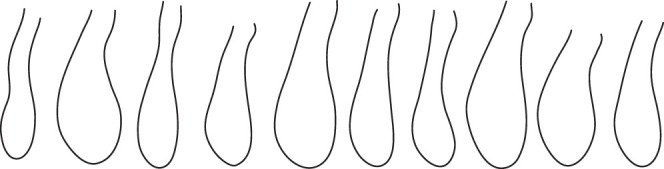
Different configuration of the mandibular symphysis.
Differences Between MS Parameters According to AP Skeletal Relationship
Means, standard deviations, and mean differences of all measured MS parameters for the three AP groups are shown in Table 4. The angle B-B1-Gn (vertical dimension of MS) was significantly smaller in Class II than in Class I (P < .05) and Class III (P < .001) skeletal relationships.
Table 4.
Mean and Standard Deviation (SD) for the Mandibular Symphysis Measured Parameters in the Different Anteroposterior Skeletal Jaw Relationships and the Differences Between Thema

The MS concavity angle (Id-B-Pog) was significantly larger in Class III than in Class I and Class II skeletal relationships (P < .001), while the angle of MS convexity showed no significant difference between the three groups.
Inclination of the alveolar part of MS toward the mandibular plane (Id-B/MP) was significantly more (indicated by a smaller angle) in the Class III group than in the other two groups (P < .001). Inclination of the skeletal part (B-Pog/MP) of MS, however, showed no significant difference among the three groups.
The distances from Id to point B and from point B to Pogonion were significantly larger in the Class III (P < .01) than in the Class II group. Total length of MS (Id-Me) was larger in the Class III group than in the other two groups (P < .05).
Perpendicular distance from Pog to B-Me line was significantly smaller in the Class II than in the Class I (P < .05) and Class III (P < .01) groups. MS area in the Class III group was significantly larger than in the Class I and Class II groups (P < .01).
Differences Between MS Parameters According to Gender
MS measured parameters for males and females, with the differences between them, are shown in Table 5.
Table 5.
Mean and Standard Deviation (SD) for the Mandibular Symphysis Measured Parameters in Males and Females and the Differences Between Thema

Males had a larger B-B1-Gn angle (P < .001) than females, indicating a larger vertical dimension of MS. All linear measurements (except Pog-Me distance) and the area of MS in males were larger than those in females (P < .05 to P < .001).
Correlation Between Craniofacial and Dentoalveolar Parameters and MS Morphology
A correlation ranging from weak to strong (r = 0.30 to r = 0.83) was found between craniofacial and dentoalveolar parameters on one hand and the MS parameters on the other hand (Table 6). All Pearson correlation coefficient (r) values were significant at P < .001.
Table 6.
Pearson Correlation Coefficient (r) Between Some of the Craniofacial (CF) and Dentoalveolar (DA) Parameters on One Hand and the Mandibular Symphysis (MS) Parameters on the Other Hand in the Total Samplea

DISCUSSION
Dentoalveolar compensation is usually a good camouflage for the underlying AP skeletal discrepancy.16,17 Changes in the inclination of the lower incisors to compensate for the skeletal discrepancy in different AP relationships might cause surface remodeling of MS, affecting its morphology.18 Accordingly, this study looked at some of the characteristics of MS in the three AP relationships and investigated the craniofacial and dentoalveolar parameters that might have any correlation with the morphology of MS.
Class III subjects showed less anterior concavity of the MS and a greater inclination of the alveolar part of the MS toward the mandibular plane than did Class I and Class II subjects. This finding was in agreement with the results reported by Yamada et al.12 Retroclination of lower incisors in Class III skeletal relationship is a frequent finding to compensate for the skeletal discrepancy.19–21 It has been suggested that retroclination of the lower incisors would lead to surface remodeling of the outer surface of the dentoalveolar part of MS to follow the inclination of the lower central incisors, leading to its retroclination as well.12,18 Such retroclination of the alveolar part of the symphysis would result in less concavity of the anterior contour of MS.
The convexity of the contour of the skeletal part of MS was evaluated by angular and linear parameters: the angle B-Pog-Me and the Perpendicular distance from Pog to B-Me line, respectively. Although the angular measurement was smaller in the Class III group than in the Class II group, the differences between groups did not reach a significant level. The linear measurement, however, was significantly larger in the Class III group than in the Class I group, while the Class II group showed the smallest distance. This finding demonstrates an increase in chin prominence in Class III skeletal relationship compared to Class I and Class II relationships. The general increase in mandibular size in Class III discrepancy could be one explanation for that.22
The linear distances and angular measurement that expressed the vertical dimension of MS and the area of MS were largest in the Class III group compared to the Class I and Class II groups. Several studies22–24 reported a larger mandible in the Class III relationship, including its symphysis, than in the other AP relationships.
When evaluating the morphology and dimension of MS according to gender, males exhibited larger MS area and longer dimensions than females. Sexual dimorphism has been reported25 between males and females with regard to different aspects of the craniofacial complex.
Several factors were thought to affect the shape and size of MS, such as genetic factors and ethnicity,5,6 inclination of the lower incisors,12,18,26 and facial type.27 In this study a strong correlation was found between the total and lower anterior facial heights on the one hand and the total length of MS on the other hand. This strong correlation may be related to the dentoalveolar compensation in the vertical dimension. As the lower face height increases, upper and lower anterior teeth may continue their eruption in an attempt to maintain a positive overbite, bringing their alveolar bony support with them, resulting in an increase in total MS length.1,27
There was a weak but significant correlation between the lower incisor inclination and MS inclination. Other studies12,19 reported a stronger correlation between these two parameters. In those studies, however, different reference points and lines were used to express the inclination of MS. The reference line for the inclination of the alveolar part of MS in this study passed through point B. Therefore, any variation of this point in the different skeletal patterns would affect the involved angular measurements. Additionally, point B has been used to measure a dentoalveolar parameter when it represents the demarcation between dentoalveolar and skeletal structures.28
Although the differences between the different AP relationships in terms of chin morphology and dimensions were relatively small on a clinical level, with large standard deviations, they can still be of some importance to the clinician. They can be used in combination with the other cephalometric findings and mandibular growth predictors29 to identify the general pattern of the skeletal relationship, which may aid in diagnosis and prediction of the size and/or direction of mandibular growth, especially in skeletal Class III patients. These findings reflect the importance of carrying out a thorough analysis for each patient as a separate entity, taking into consideration her/his craniofacial composition and jaw and chin morphology for the purposes of diagnosis and treatment planning.
CONCLUSIONS
The Class III skeletal jaw relationship exhibited a less concave anterior contour of MS, an increase in its vertical dimension, and more inclination of the alveolar part toward the mandibular plane than did the other AP relationships, reflecting compensation for the skeletal pattern of the jaws.
Larger dimensions and area of MS were found in Class III than in Class I and Class II relationships.
A strong correlation was found between anterior facial height and MS length.
A weak but significant correlation was found between the inclination of the lower incisors and the alveolar part of MS.
ACKNOWLEDGMENTS
The authors are indebted to Computer Engineer Motaz Bayazeed for specially developing the software (TechExpert) that was used in this study.
REFERENCES
- 1.Buschang PH, Julien K, Sachdeva R, Demirjian A. Childhood and pubertal growth changes of the human symphysis. Angle Orthod. 1992;62:203–210. doi: 10.1043/0003-3219(1992)062<0203:CAPGCO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Hoenig JF. Sliding osteotomy genioplasty for facial aesthetic balance: 10 years of experience. Aesthetic Plast Surg. 2007;31:384–391. doi: 10.1007/s00266-006-0177-6. [DOI] [PubMed] [Google Scholar]
- 3.Skieller VB, Bjork A, Linde-Hansen T. Prediction of mandibular growth rotation evaluated from a longitudinal implant sample. Am J Orthod. 1984;86:359–370. doi: 10.1016/s0002-9416(84)90028-9. [DOI] [PubMed] [Google Scholar]
- 4.Gould SJ. The exaptive excellence of spandrels as a term and prototype. Proc Natl Acad Sci USA. 1997;94:10750–10755. doi: 10.1073/pnas.94.20.10750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gould SJ. The Structure of Evolutionary Theory. Cambridge, UK: Belknap Press; 2002. [Google Scholar]
- 6.Sherwood RJ, Hlusko LJ, Duren DL, Emch VC, Walker A. Mandibular symphysis of large-bodied hominoids. Hum Biol. 2005;11:735–759. doi: 10.1353/hub.2006.0020. [DOI] [PubMed] [Google Scholar]
- 7.Beecher RM. Evolution of the mandibular symphysis in Notharctinae (Adapidae Primates) Int J Primatol. 1983;4:99–112. [Google Scholar]
- 8.Brown B. Miocene hominoid mandibles: functional and phylogenetic perspectives. In: Begun DR, Ward CV, Rose MD, editors. Function Phytogeny and Fossils. New York, NY: Plenum Press; 1997. pp. 153–172. [Google Scholar]
- 9.Daegting DJ, Hylander WL. Biomechanics of torsion in the human mandible. Am J Phys Anthropol. 1998;105:73–87. doi: 10.1002/(SICI)1096-8644(199801)105:1<73::AID-AJPA7>3.0.CO;2-E. [DOI] [PubMed] [Google Scholar]
- 10.Bjork A. Prediction of mandibular growth rotation. Am J Orthod. 1969;55:585–599. doi: 10.1016/0002-9416(69)90036-0. [DOI] [PubMed] [Google Scholar]
- 11.von Bremen J, Pancherz H. Association between Björk's structural signs of mandibular growth rotation and skeletofacial morphology. Angle Orthod. 2005;75:506–509. doi: 10.1043/0003-3219(2005)75[506:ABBSSO]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Yamada C, Kitai N, Kakimoto N, Murakami S, Furukawa S, Takada K. Spatial relationships between the mandibular central incisor and associated alveolar bone in adults with mandibular prognathism. Angle Orthod. 2007;77:766–772. doi: 10.2319/072906-309. [DOI] [PubMed] [Google Scholar]
- 13.Hamdan AM, Rock WP. Cephalometric norms in an Arabic population. J Orthod. 2001;28:297–300. doi: 10.1093/ortho/28.4.297. [DOI] [PubMed] [Google Scholar]
- 14.Dahlberg G. Statistical Methods for Medical and Biological Students. London, UK: George Allen and Unwin Ltd; 1940. pp. 122–132. [Google Scholar]
- 15.Houston WJ. The analysis of errors in orthodontic measurements. Am J Orthod. 1983;83:382–390. doi: 10.1016/0002-9416(83)90322-6. [DOI] [PubMed] [Google Scholar]
- 16.Solow B. The dentoalveolar compensatory mechanism: background and clinical implications. Br J Orthod. 1980;7:145–161. doi: 10.1179/bjo.7.3.145. [DOI] [PubMed] [Google Scholar]
- 17.Björk A. Sutural growth of the upper face studied by the implant method. Acta Odontol Scand. 1966;24:109–127. doi: 10.3109/00016356609026122. [DOI] [PubMed] [Google Scholar]
- 18.Yu Q, Pan XG, Ji GP, Shen G. The association between lower incisal inclination and morphology of the supporting alveolar bone—a cone-beam CT study. Int J Oral Sci. 2009;1:217–223. doi: 10.4248/IJOS09047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ellis E, McNamara JA. Components of adult Class III malocclusion. J Oral Maxillofac Surg. 1984;42:295–305. doi: 10.1016/0278-2391(84)90109-5. [DOI] [PubMed] [Google Scholar]
- 20.Ishii N, Deguchi T, Hunt NP. Craniofacial differences between Japanese and British Caucasian females with a skeletal Class III malocclusion. Eur J Orthod. 2002;24:493–499. doi: 10.1093/ejo/24.5.493. [DOI] [PubMed] [Google Scholar]
- 21.Choi HJ, Kim JY, Yoo SE, Kwon JH, Park K. Cephalometric characteristics of Korean children with Class III malocclusion in the deciduous dentition. Angle Orthod. 2010;80:86–90. doi: 10.2319/120108-605.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Mouakeh M. Cephalometric evaluation of craniofacial pattern of Syrian children with Class III malocclusion. Am J Orthod Dentofacial Orthop. 2001;119:640–649. doi: 10.1067/mod.2001.112671. [DOI] [PubMed] [Google Scholar]
- 23.Reyes BC, Baccetti T, McNamara JA., Jr An estimate of craniofacial growth in Class III malocclusion. Angle Orthod. 2006;76:577–584. doi: 10.1043/0003-3219(2006)076[0577:AEOCGI]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 24.Wolfe SM, Araujo E, Behrents RJ, Buschang PH. Craniofacial growth of Class III subjects six to sixteen years of age. Angle Orthod. 2011;81:211–216. doi: 10.2319/051010-252.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chakravarty MM, Aleong R, Leonard G, et al. Automated analysis of craniofacial morphology using magnetic resonance images. PLoS One. 2011;6:e20241. doi: 10.1371/journal.pone.0020241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Endo T, Ozoe R, Kojima K, Shimooka S. Congenitally missing mandibular incisors and mandibular symphysis morphology. Angle Orthod. 2007;77:1079–1084. doi: 10.2319/020106-37.1. [DOI] [PubMed] [Google Scholar]
- 27.Swasty D, Lee J, Huang JC, et al. Cross-sectional human mandibular morphology as assessed in vivo by cone-beam computed tomography in patients with different vertical facial dimensions. Am J Orthod Dentofacial Orthop. 2011;139:e377–e389. doi: 10.1016/j.ajodo.2009.10.039. [DOI] [PubMed] [Google Scholar]
- 28.Proffit WR, Fields HW, Sarver DM. Contemporary Orthodontics 4th ed. St Louis, Mo: Elsevier; 2007. [Google Scholar]
- 29.Björk A. Prediction of mandibular growth rotation. Am J Orthod. 1969;55:585–599. doi: 10.1016/0002-9416(69)90036-0. [DOI] [PubMed] [Google Scholar]