

Abstract
BACKGROUND:
To determine the frequency, characteristics, and use of resources related to electric scooter (e-scooter) injuries in the emergency department (ED) of a major metropolitan area hospital.
METHODS:
We performed a retrospective review of all ED presentations related to e-scooter injuries at a level I trauma center between May 2017 and February 2020. We identified ED presentation data, injury-related data, patients’ clinical course after evaluation, injury diagnosis, surgical procedures, and ED readmissions.
RESULTS:
A total of 3,331 patients with e-scooter injuries presented to the ED over a 34-month period. There was a 6-fold increase in e-scooter-related injuries presenting to the ED, from an average of 26.9 injuries per month before the introduction of shared e-scooter services in August 2018 to an average of 152.6 injuries per month after its introduction. The average injury rate during weekdays was 3.27 per day, with the majority of injuries occurring in the afternoon. The most common mechanism of injury was rider fall (79.1%). There were a total of 2,637 orthopedic injuries, of which 599 (22.7%) were fractures. A total of 296 (8.9%) patients were hospitalized following the initial ED admission, and 462 surgeries were performed within 7 days of ED arrival.
CONCLUSIONS:
The introduction of the shared e-scooter services is associated with a dramatic increase in e-scooter injuries presenting to the ED. E-scooter use carries considerably underestimated injury risks of high-energy trauma and misunderstood mechanisms of injuries. These injuries challenge the healthcare system, with a major impact on both EDs and surgical departments.
Keywords: E-scooter, Scooter, Emergency department
INTRODUCTION
The introduction of electric scooters (e-scooters) and the shared e-scooter services have revolutionized commuting throughout the world.[1,2] These low-cost and environmentally-friendly vehicles have become an attractive alternative for public transportation.[3] The first shared e-scooter service in Israel was introduced in August 2018 by Bird (Bird Rides).[4] Several other companies quickly followed, including Neutron Holdings (Lime-S scooter) and Wind Mobility (Wind e-scooter), increasing to thousands of e-scooters available throughout the cities.[5,6] In 2019, one year following the launching of shared services, Tel-Aviv had the highest rate of shared e-scooter users per capita worldwide, with approximately 7.5% of Israelis using shared e-scooter services on a daily basis.[7]
E-scooters can be located using a free smartphone application, after which they are unlocked and ridden for a nominal fee per minute of use. These scooters are easy to use and achieve a top speed of approximately 24 km/hour.[8] Private e-scooters were introduced for consumers in Israel in 2012, and they were authorized for use as a private mobility vehicle for individuals aged 16 years and older in 2016.[9] The shared service companies recommend that riders should be at least 18 years of age and that they use helmets.[10] Appropriate infrastructure, such as separate bicycle lanes and policy enforcement, however, were not implanted properly and quickly enough.[11] Therefore, thousands of e-scooters can now be found sharing streets and walkways with drivers of cars, cyclists, and pedestrians, resulting in a high rate of accidents requiring emergency department (ED) visits.[11-13]
Severe e-scooter injuries with multiple trauma combining head, abdominal, and musculoskeletal injuries, which inflict a tremendous impact on the healthcare system, have been reported.[1,14,15] According to the Israeli National Trauma and Emergency Medicine Institute, there was a 230% increase in hospital visits in 2019 and 6 deaths due to e-scooter accidents.[16]
Several studies[2,17-19] have reviewed the impact of e-scooter injuries on ED admissions worldwide. However, sample sizes and data on patient hospitalization and clinical course were limited. The location of our medical center at the heart of the Tel-Aviv metropolitan area turned it into the hub of e-scooter injury care. The thousands of injuries treated annually in our center continue to challenge both the ED and the hospital’s surgical departments. The purpose of this study is to report the longest experience to date with e-scooter-related injuries and to characterize their impact on ED resources.
METHODS
Study design
We performed a retrospective investigation of all e-scooter-related injuries (privately owned scooters and those of shared services) treated in the ED, a level I trauma center,[20] over a 34-month period (from May 1, 2017 to February 29, 2020).
Selection of participants
We queried records of patients who presented to the ED during the study period by searching for occurrences of the keywords “electric” or “e” and “scooter”, including common variants, misspellings, and the brand name for the most-used shared e-scooter services both in English and Hebrew (supplementary Table 1). Data were obtained from all of the electronic medical records (EMRs) generated during the ED visit. All charts were then manually reviewed by two orthopedic surgeons among the authors (IS, OS, or SF) to verify that the inclusion criteria were met and to collect relevant data. Non-consensus of the diagnosis was resolved by a third orthopedic surgeon (AK). We included patients who presented to the ED with e-scooter-related injuries either as a rider or as a pedestrian. Injuries related to non-motorized scooters, motorized assisted devices, wheelchairs, roller blades, and bicycles of any kind were excluded.
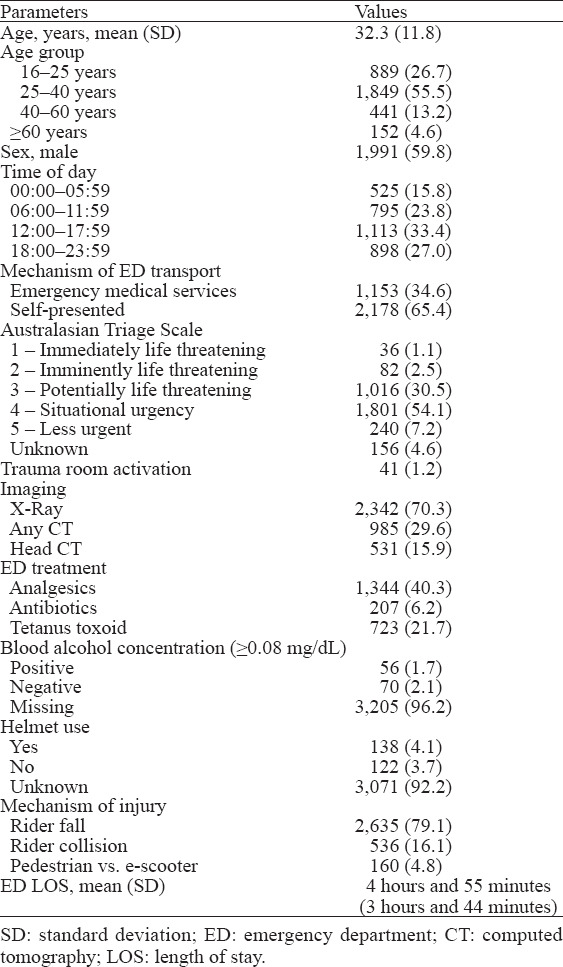
Table 1.
Patient demographics, n (% of total cohort)
Outcomes
The study outcomes were: (1) to characterize ED visits with e-scooter-related injuries during the study period; and (2) to compare ED visits with e-scooter-related injuries before and after the introduction of shared e-scooter services.
Patient records were reviewed for demographic data, including age and sex. ED presentation data included date and time of visit (daytime 06:00–18:00, nighttime 18:00–06:00), transport means to a hospital, and trauma room protocol activation. The triage urgency scale was assessed by a triage nurse according to the Australasian Triage Scale (ATS).[21] Injury-related data, which were routinely documented by a physician during the initial ED admission, included the location of the event, the mechanism of injury, and helmet use. Blood alcohol concentration (BAC) was measured in patients suspected of alcohol intoxication (BAC ≥0.08 mg/dL) at the initial presentation by the triage nurse or the ED physician, and in all patients transported to the trauma room. The mechanism of injury was classified as either “rider fall”, “rider collision” (rider vs. stationary object, pedestrian, or any kind of vehicle), and “pedestrian”. Each patient’s clinical course was reviewed, including initial treatment (analgesics, antibiotics, and tetanus toxoid administration), imaging studies, diagnosis of injuries, ED length of stay, and hospital admissions. Surgical procedures and ED readmissions were documented up to 6 months following the initial ED encounter. Readmissions were not considered as new ED visits for data analysis.
Injury diagnosis
Injuries classified as orthopedic (contusion/laceration, sprain/dislocation, and fractures) were reviewed by an orthopedic surgeon (IS, OS, SF, or AK), and non-orthopedic (head, thoracic, and abdomen) were reviewed by an emergency medicine physician (EZ). Patients were included in multiple categories if they sustained injuries leading to more than one diagnosis (e.g., a patient with both head injury and radius fracture was included in both of the categories “head injury” under non-orthopedic injuries and “fractures” under orthopedic injuries).
Statistical analysis
All analyses were performed with the R version 3.5.0 (R Foundation for Statistical Computing). Overall patient characteristics were summarized by mean±standard deviation (SD) for continuous variables that were tested for normality, or frequency (%) for categorical variables.
RESULTS
During the study period, 3,331 patients were admitted to our level I trauma center ED with e-scooter-related injuries. Figure 1 demonstrates the dramatic increase in e-scooter ED visits throughout the study period, from an average of 26.9 ED visits per month before the introduction of shared e-scooter services in August 2018 to 152.6 ED visits per month after it. Higher injury rates were observed during the summer months (from June to September) compared to the winter months (from December to February). During weekdays, the average injury rate was 3.27 injuries per day, with the majority of injuries occurring during the daytime hours (06:00–18:00). The injury rate was lower during the weekends, with an average of 2.75 injuries per day (Figure 2).
Figure 1.
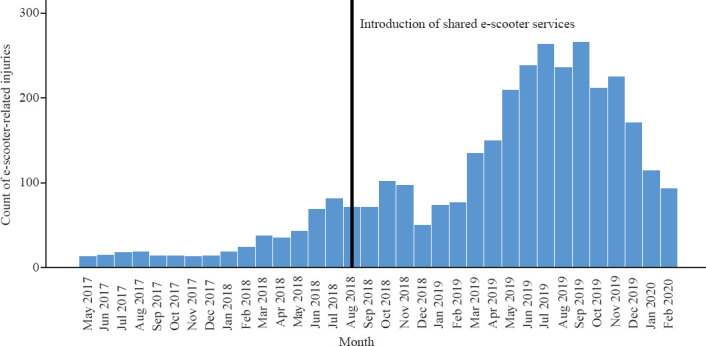
E-scooter-related injuries by month. The line represents the introduction of shared e-scooter services.
Figure 2.
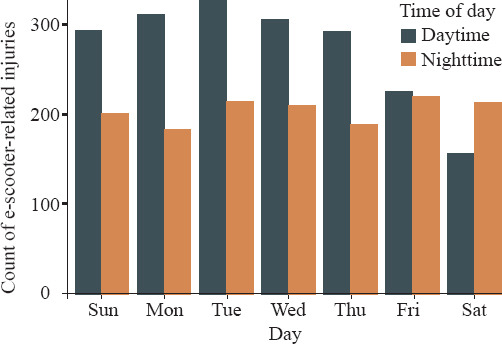
E-scooter-related injuries by day of week and time of day. The time of day is divided into daytime (06:00–18:00) and nighttime (18:00–06:00) and represented by colors.
Table 1 describes the patients’ demographics. Most of them were males (59.8%), with a mean age of 32.3±11.8 years. The greatest number of injuries were sustained by patients who presented to the ED in the afternoon hours (12:00–17:59). Most patients were ambulatory (65.4%), and the rest arrived via emergency medical services, with 3.6% of the patients having been defined at triage with imminently life-threatening injuries (ATS 1+2). Forty-one (1.2%) patients required direct admission and activation of trauma room protocol. The one mortality due to severe head trauma was called in the trauma room soon after ED arrival.
During their stay in the ED, 70.3% of the patients underwent X-ray imaging, with 29.6% of patients undergoing computed tomography (CT) scans as part of their initial evaluation. A total of 126 (3.8%) patients were screened for BAC, and 56 (44.1%) of them tested positive. Helmet use was documented in 7.8% of all ED visits, of which 53.1% used a helmet. The most common mechanism of injury was rider fall (79.1%), followed by rider collision (16.1%), while 4.8% were pedestrians hit by an e-scooter. Most of the patients were between 25 and 40 years of age (55.5%), and the mechanism of injury was rider fall in 81.1% of them. In contrast, 44.1% in the ≥60-year age group were pedestrians (Figure 3). Table 2 presents the injury diagnosis and the patients’ clinical course. A total of 2,637 orthopedic injuries were documented, of them 1,941 (73.6%) were contusions/lacerations and 599 (22.7%, 599/2,637) were fractures. Of the non-orthopedic injuries, head injury was the most common in 581 (17.4%, 581/3,331) patients. A total of 296 (8.9%) patients were hospitalized following the initial ED encounter, and 42.6% of them were sent to the orthopedics department. A total of 462 operations were performed within 7 days of ED arrival, and 77.5% of them were orthopedic surgeries.
Figure 3.
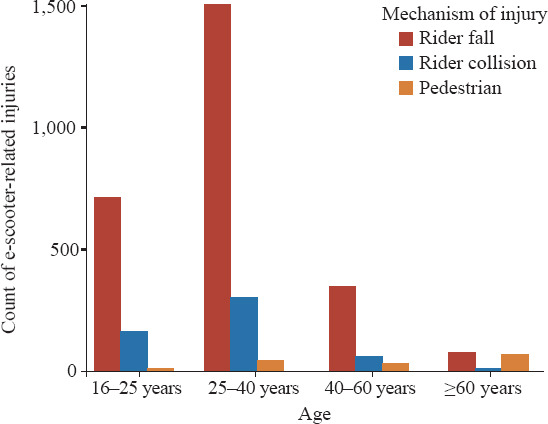
E-scooter-related injuries by age group and mechanism of injury. The mechanisms of injury are indicated by colors.
Table 2.
Injury characteristic and patient outcomes1,2
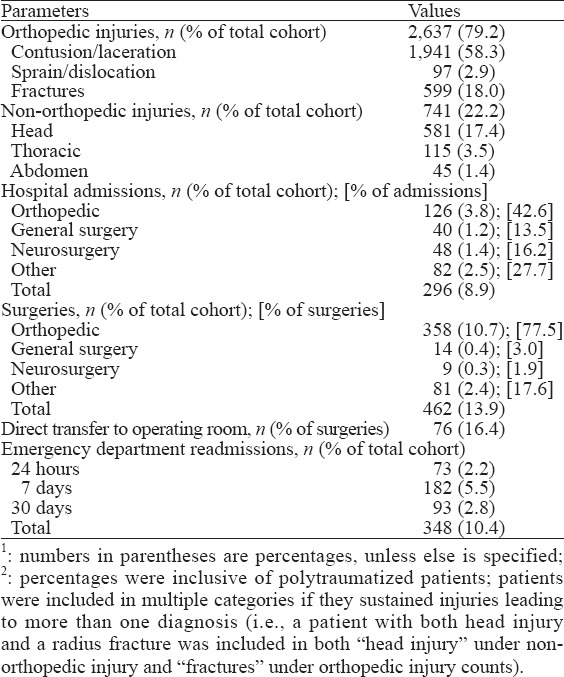
Emergency surgeries comprised 16.4% of the total number, and those patients were transferred to the operating room directly from the ED. A total of 348 (10.4%) ED readmissions of any cause were documented. Supplementary Table 2 reviews the overall orthopedic fracture distribution. Out of a total of 599 fractures, 433 (72.3%) were upper extremity fractures and 166 (27.7%) were lower extremity fractures. Radius/ulna fractures were the most common upper extremity fractures (43.4%) compared to tibia/fibula fractures (9.2%) for the lower extremity.
DISCUSSION
The main finding of this study is a significant 6-fold rise of e-scooter injuries per month sustained by patients who presented to our ED following the launch of shared e-scooter services. E-scooters have revolutionized transportation patterns and gained considerable popularity following the introduction of the shared e-scooter services in 2018, with reported millions of rides in the first two years of service.[22] A number of studies on these issues have recently been published, and their results demonstrated a significant increase in the number of trauma injuries related to e-scooter use.[1,2,19,23] A recent study by Tenenbaum et al[24] investigated the epidemiology and patterns of orthopedic injuries by electric bicycles in Israel. They reported a 30.0% decrease in electric bicycle ED visits and a concurrent increase of 87.5% of e-scooter ED visits in the first quarter of 2019 compared to the same time period one year earlier, calling for an investigation of those e-scooter injuries. To the best of our knowledge, our collection of 3,331 patients over a 34-month period represents the largest study to investigate the surge of e-scooter-related injuries. While other studies showed a higher injury rate during the weekend,[14,25] our results revealed higher rates during the weekdays and during the afternoon hours when commuter traffic is traditionally more substantial and daylight is considerably reduced. The implications of these findings are that e-scooter use has been transformed from a recreational activity to an everyday primary commuter vehicle and, most importantly, that each municipality should investigate the local characteristics of e-scooter usage in order to promote the appropriate policy for increasing safety.
Interestingly, we found higher injury rates during the late-night hours during weekends which we attribute to riders returning home after a social event, possibly involving alcohol consumption. Most injuries were sustained during the summer months, probably due to a high volume of usage during favorable weather conditions. We had expected an increase of injuries during the winter months due to harsh weather and poor road conditions, but the decline we actually observed could be explained by less usage under such conditions.[19,26]
The most common mechanism of injury was rider fall, which may be attributed to lack of rider experience, improper infrastructure, and optional driving license. Nearly one-half of the injuries occurred among pedestrians in the ≥60-year age group, possibly due to e-scooter use on sidewalks for lack of separate bicycle lanes. Although the most common type of injury was contusion/laceration, the more resource- and time-consuming orthopedic injuries were fractures that required treatments varying from early reduction and fixation with casting in the ED to surgery in the operating theatre. Upper limb fractures were more frequent than lower limb fractures, with radius/ulna being the most common among them. Rider fall was the most frequent mechanism of injury. These findings may explain a fall on an outstretched hand as the leading cause of radius/ulna and hand fractures, raising the question of whether wrist and elbow guard use should be mandatory during e-scooter use. Tibia/fibula fractures were the most frequent fractures of the lower limb, mostly secondary to “bumper injury” mechanisms. These injury patterns are characteristics of motorcycle crashes, suggesting the underestimation of the involvement of high-energy trauma.[27,28]
E-scooter high-energy trauma may present with orthopedic injuries (closed/open fractures and dislocations) and non-orthopedic injuries, including head, thoracic, and abdominal trauma. Such diversity of presentations demands a multidisciplinary approach in the ED with the need for numerous medical services, resulting in extended ED length of stay, a high percentage of admission rates, and numerous surgical treatments. High rates of emergency surgeries further emphasize the severity and complexity of injuries that require early surgical treatment. Similar to other studies,[18,29] we observed that the majority of all immediate hospitalizations were to the orthopedic department. Our municipality spreads over a relatively small and flat area, and the local weather is mostly warm and dry. These conditions, which are similar to other cities with high rates of e-scooter use, combine to contribute to its popularity. Therefore, we believe that our study findings can be significant to other medical centers located in cities with similar characteristics.
Limitations
This single center study has the inherent weakness associated with its retrospective nature and its reliance on the accuracy of data extracted from EMRs. Our study did not include e-scooter-related injuries presenting to primary care clinics, which might account for a substantial proportion of injuries and treatment in other facilities. Moreover, ours is a level I trauma center, and our cohort might consist of a larger proportion of high-severity injuries than the actual injury severity distribution in our city. Our results represent the average number of e-scooter-related injuries per month, and they are not standardized for the number of monthly e-scooter miles of travel or the number of e-scooters available in our metropolitan area. The reported e-scooter injury rate per mile of travel is up to 200 times higher than that for motor vehicles.[30] Further research is required to investigate injury risk per mile of travel in our metropolitan area, and caution should be taken when generalizing our study results. Data on alcohol intoxication and helmet use are not routinely collected for each patient admitted to the ED, leading to under-representation of a possible injury risk factor and consequences. While most similar studies are limited by the use of diagnosis codes, such as International Classification of Diseases 10 (ICD-10), a strength of our study is that its data collection used free text for identification of the patient population, thus lowering the number of missing cases due to inaccurate assignment of diagnosis codes and eliminating non-e-scooter cases which might bias the results.
CONCLUSIONS
The introduction of the shared e-scooter services is associated with a dramatic increase in e-scooter injuries presenting to the ED. While e-scooters represent a convenient and environment-friendly mode of transportation, they carry considerable injury risks. The more evidence that is gathered regarding common injuries, the better will be the medical treatment that can be provided. Communities can reduce those risks by developing infrastructures suitable for e-scooter use, such as the provision of bicycle lanes, the mandatory use of helmets and limb-protection gear, and the enforcement of speed limitations and age restrictions.
ACKNOWLEDGEMENTS
We acknowledge Efrat Zandberg, MD, an emergency medicine physician in the Tel-Aviv Sourasky Medical Center, for her contribution in verifying the diagnosis of all non-orthopedic injuries.
Footnotes
Funding: None.
Ethical approval: Institutional review board (IRB) approval was obtained for all aspects of this study in accordance with institutional policies (0142-20).
Conflicts of interests: The authors declare that they have no conflicts of interests.
Contributions: IS and OS had equal contribution and are co-authors as the first author. IS and OS: concept, design, definition of intellectual content, literature search, data acquisition, data analysis, statistical analysis, manuscript preparation, manuscript editing and manuscript review; AW and SF: design, definition of intellectual content, data acquisition, data analysis, manuscript review; AK: concept, definition of intellectual content, manuscript editing and manuscript review.
All the supplementary files in this paper are available at http://wjem.com.cn/EN/10.5847/wjem.j.1920-8642.2022.002.
REFERENCES
- 1.Badeau A, Carman C, Newman M, Steenblik J, Carlson M, Madsen T. Emergency department visits for electric scooter-related injuries after introduction of an urban rental program. Am J Emerg Med. 2019;37(8):1531–3. doi: 10.1016/j.ajem.2019.05.003. [DOI] [PubMed] [Google Scholar]
- 2.Kobayashi LM, Williams E, Brown CV, Emigh BJ, Bansal V, Badiee J, et al. The e-merging e-pidemic of e-scooters. Trauma Surg Acute Care Open. 2019;4(1):e000337. doi: 10.1136/tsaco-2019-000337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Barker R. Electric scooters. Emerg Med Australas. 2019;31(6):914–5. doi: 10.1111/1742-6723.13424. [DOI] [PubMed] [Google Scholar]
- 4.Moses S. E-scooter ridesharing co Bird to launch in Tel Aviv. Available at https://en.globes.co.il/en/article-escooter-ridesharing-co-bird-to-launch-in-tel-aviv-1001248460 .
- 5.Raz-Chaimovich M. E-scooter co Wind to launch in Tel Aviv. Available at https://en.globes.co.il/en/article-e-scooter-co-wind-to-launch-in-tel-aviv-1001266446 .
- 6.Raz-Chaimovich M. Lime e-scooters officially launches Israel operations. Available at https://en.globes.co.il/en/article-lime-e-scooters-officially-launches-israel-operations-1001272352 .
- 7.Etison U, Pick A. Over 10% of Israelis make weekly use of bikes and e-scooters, report says. Available at https://www.calcalistech.com/ctech/articles/0,7340,L-3777899,00.html .
- 8.Ishmael CR, Hsiue PP, Zoller SD, Wang PC, Hori KR, Gatto JD, et al. An early look at operative orthopaedic injuries associated with electric scooter accidents. J Bone Joint Surg Am. 2020;102(5):e18. doi: 10.2106/JBJS.19.00390. [DOI] [PubMed] [Google Scholar]
- 9.Israel National Road Safety Authority. Regulations—electric scooter. Available at https://www.gov.il/he/departments/legalInfo/regulations_scooter .
- 10.Bird Rides, Inc. A look at e-scooter safety. Available at https://www.bird.co/wp-content/uploads/2019/12/Bird-Safety-Report-April-2019.pdf .
- 11.Choron RL, Sakran JV. The integration of electric scooters:useful technology or public health problem? Am J Public Heal. 2019;109(4):555–6. doi: 10.2105/AJPH.2019.304955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.McGuinness MJ, Tiong Y, Bhagvan S. Shared electric scooter injuries admitted to Auckland city hospital:a comparative review one year after their introduction. N Z Med J. 2021;134(1530):21–9. [PubMed] [Google Scholar]
- 13.Cha Sow King C, Liu M, Patel S, Goo TT, Lim WW, Toh HC. Injury patterns associated with personal mobility devices and electric bicycles:an analysis from an acute general hospital in Singapore. Singap Med J. 2020;61(2):96–101. doi: 10.11622/smedj.2019084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Beck S, Barker L, Chan AN, Stanbridge S. Emergency department impact following the introduction of an electric scooter sharing service. Emerg Med Australas. 2020;32(3):409–15. doi: 10.1111/1742-6723.13419. [DOI] [PubMed] [Google Scholar]
- 15.Namiri NK, Lui H, Tangney T, Allen IE, Cohen AJ, Breyer BN. Electric scooter injuries and hospital admissions in the United States, 2014-2018. JAMA Surg. 2020;155(4):357–9. doi: 10.1001/jamasurg.2019.5423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Peleg K. Bicycle and electric scooter injury data report—summary 2019. Available at http://www.gertnerinst.org.il/health_policy/trauma/trauma_research/968.htm .
- 17.Dhillon NK, Juillard C, Barmparas G, Lin TL, Kim DY, Turay D, et al. Electric scooter injury in southern California trauma centers. J Am Coll Surg. 2020;231(1):133–8. doi: 10.1016/j.jamcollsurg.2020.02.047. [DOI] [PubMed] [Google Scholar]
- 18.Trivedi TK, Liu C, Antonio ALM, Wheaton N, Kreger V, Yap A, et al. Injuries associated with standing electric scooter use. JAMA Netw Open. 2019;2(1):e187381. doi: 10.1001/jamanetworkopen.2018.7381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vernon N, Maddu K, Hanna TN, Chahine A, Leonard CE, Johnson JO. Emergency department visits resulting from electric scooter use in a major southeast metropolitan area. Emerg Radiol. 2020;27(5):469–75. doi: 10.1007/s10140-020-01783-4. [DOI] [PubMed] [Google Scholar]
- 20.American Trauma Society. Trauma center levels explained. Available at https://www.amtrauma.org/page/traumalevels .
- 21.Forero R. Literature review on the Australasian Triage Scale (ATS) Available at http://nla.gov.au/nla.arc-128506 .
- 22.Bird Rides, Inc. Tel Aviv hits modeshift milestone with over 5 million bird rides in 2 years. Available at https://www.bird.co/blog/tel-aviv-modeshift-milestone-5-million-bird-rides-2-years .
- 23.Siow MY, Lavoie-Gagne O, Politzer CS, Mitchell BC, Harkin WE, Flores AR, et al. Electric scooter orthopaedic injury demographics at an urban level I trauma center. J Orthop Trauma. 2020;34(11):e424–9. doi: 10.1097/BOT.0000000000001803. [DOI] [PubMed] [Google Scholar]
- 24.Tenenbaum S, Weltsch D, Bariteau JT, Givon A, Peleg K, Thein R, et al. Orthopaedic injuries among electric bicycle users. Injury. 2017;48(10):2140–4. doi: 10.1016/j.injury.2017.08.020. [DOI] [PubMed] [Google Scholar]
- 25.Aizpuru M, Farley KX, Rojas JC, Crawford RS, Moore TJ, Wagner ER. Motorized scooter injuries in the era of scooter-shares:a review of the national electronic surveillance system. Am J Emerg Med. 2019;37(6):1133–8. doi: 10.1016/j.ajem.2019.03.049. [DOI] [PubMed] [Google Scholar]
- 26.Blomberg SNF, Rosenkrantz OCM, Lippert F, Collatz Christensen H. Injury from electric scooters in Copenhagen:a retrospective cohort study. BMJ Open. 2019;9(12):e033988. doi: 10.1136/bmjopen-2019-033988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Amin NH, Jakoi A, Katsman A, Harding SP, Tom JA, Cerynik DL. Incidence of orthopedic surgery intervention in a level I urban trauma center with motorcycle trauma. J Trauma. 2011;71(4):948–51. doi: 10.1097/TA.0b013e31821e601d. [DOI] [PubMed] [Google Scholar]
- 28.Lateef F. Riding motorcycles:is it a lower limb hazard? Singapore Med J. 2002;43(11):566–9. [PubMed] [Google Scholar]
- 29.Bloom MB, Noorzad A, Lin C, Little M, Lee EY, Margulies DR, et al. Standing electric scooter injuries:impact on a community. Am J Surg. 2021;221(1):227–32. doi: 10.1016/j.amjsurg.2020.07.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Rix K, Demchur NJ, Zane DF, Brown LH. Injury rates per mile of travel for electric scooters versus motor vehicles. Am J Emerg Med. 2021;40:166–8. doi: 10.1016/j.ajem.2020.10.048. [DOI] [PubMed] [Google Scholar]