

Abstract
Objective.
Despite increasing prevalence of end-stage renal disease (ESRD), little attention has been directed to how occupational exposures may contribute to risk. Our objective was to investigate the relationship between metalworking fluids (MWF) and ESRD in a cohort of 36,703 male autoworkers.
Methods.
We accounted for competing risk of death, using the subdistribution hazard approach to estimate subhazard ratios (sHRs) and 95% confidence intervals (CIs) in models with cubic splines for cumulative exposure to MWF (straight, soluble, or synthetic).
Results.
Based on 501 ESRD cases and 13,434 deaths, we did not observe an association between MWF and ESRD overall. We observed modest associations between MWF and ESRD classification of glomerulonephritis and diabetic nephropathy. For glomerulonephritis, the 60th percentile of straight MWF was associated with an 18% increased subhazard (sHR=1.18, 95% CI (0.99, 1.41)). For diabetic nephropathy, the subhazard increased 28% at the 60th percentile of soluble MWF (sHR=1.28, 95% CI (1.00, 1.64)). Differences by race suggest that Black males may have higher disease rates following MWF exposure.
Conclusions.
Exposure to straight and soluble MWF may be related to ESRD classification, though this relationship should be further examined.
Keywords: Kidney diseases, cutting fluids
Keywords: End-stage renal disease, chronic kidney disease, nephropathy, diabetes, diabetic nephropathy, glomerulonephritis, metalworking fluids, nitrosamines, G-estimation
End-stage renal disease (ESRD), defined as kidney failure requiring kidney replacement therapy, is the advanced stage of chronic kidney disease (CKD). In the U.S., about one in three adults aged 65 years and older has CKD,1 and almost 800,000 have ESRD. The annual cost to Medicare was approximately $35 billion, accounting for about 7% of total Medicare spending, although the ESRD population constitutes less than 1% of the total Medicare population.2
Occupational exposures are underappreciated as potential contributors to kidney disease.3 Although occupation has been recognized as associated with CKD and ESRD, studies with quantitative exposure measurements are needed to characterize the nature of these relationships.4 Metalworking fluids (MWF) are common occupational exposures that have not been widely studied with CKD. In the U.S. alone, more than a million workers are exposed to MWF daily.5 Metalworking involves varying processes such as cutting, grinding, and joining of metal, and MWF facilitates these processes by cooling and lubricating metal.5
MWF can be characterized into three types: straight (mineral oils with no water content), soluble (a mixture of oil and water base), and synthetic (water based, no oil content). The composition of these MWF varies. MWF are complex mixtures with additives formulated to achieve performance specifications.6 The additives can generally be grouped into corrosion inhibitors, emulsifiers, coupling agents, and biocides.7 During metal operations, these fluids mix with particles and impurities and become aerosolized into a mist, which workers may inhale. The mists have been found to contain sulfonates, non-ionic surfactants, ethanolamines, microbial products, biocides, and variable alkalinity.5 At least two components, medium-chain chlorinated paraffin and diethanolamine, have demonstrated harmful kidney effects in animal studies,8,9 though the impact of these components on humans is not known. Given that MWF types vary in their contents, we suspect that a relationship with ESRD would vary by MWF fluid type.
Of the MWF types, straight oils have been reported to contain a high concentration of PAHs, particularly during periods when these oils were less refined.6 PAHs have been associated with advanced stage CKD previously. A meta-analysis10,11 of studies of PAHs and kidney disease found no association with hydrocarbons and early stage CKD (odds ratio=0.95, 95% CI (0.6, 1.4)), yet there was a 6-fold increased odds of end-stage disease (odds ratio=5.9, 95% CI (3.8, 9.3)). Chronic, low-level PAH exposure is thought to gradually damage kidney tissue, and animal studies demonstrate glomerular more so than tubular damage following PAH exposure.10,11 Accordingly, straight MWF containing PAHs may be associated with advanced kidney disease and kidney failure, and the ESRD classification of glomerulonephritis in particular may be affected.
While there is a precedent for focusing on late stage kidney disease for this occupational exposure, the challenge is that most individuals with CKD die prior to developing kidney failure. This occurs because patients with CKD are at an increased risk of cardiovascular death as well as from other causes.1 Thus, ESRD and all-cause mortality are not independent, violating the non-informative censoring assumption of traditional Cox proportional hazards models.1,12 To address this issue, competing risk models may be used.
We examined the relationship between MWF and ESRD in a population of autoworkers with quantitative estimates of cumulative exposure accounting for death as a competing event.
METHODS
We examined this relationship in the United Autoworkers – General Motors (UAW-GM) study; the cohort consists of over 46,000 workers from three automobile manufacturing plants in Michigan, U.S. Workers were eligible to be in the study if they had worked for at least three years between 1941 and 1984, and had >50% of their work history available. Only 3% of the entire cohort was lost to follow-up. The details of the autoworker cohort are described elsewhere.13 For the present analysis, follow-up begins January 1, 1973, when Michigan began collecting data on patients classified with ESRD.14 In this analysis, we included a total of 32,025 male cohort members who were alive at the start of follow-up and followed them through December 31, 2009. Follow-up ended in 2009, reflecting the budget, study design, and work approved for this funded project.
Exposure assessment
Details of the exposure assessment for the three MWF (straight, soluble, and synthetic) have been described.13,15 Briefly, exposure measurements of airborne total particulates (mg/m3) were collected by the company over decades and independently by study industrial hygienists across plants, departments, and jobs in the mid-1980s. Individual work histories were obtained through 1994. To estimate each worker’s annual exposure intensity for each fluid type per year, work histories were linked to a job-exposure matrix containing MWF-specific exposure estimates. Time-varying cumulative exposure (mg/m3-year) to straight, soluble, and synthetic MWF was determined for each subject. Cumulative exposure was lagged 15 years, accounting for the gap between work histories and the end of follow-up as well as allowing for latency.
Outcome ascertainment
We linked the UAW-GM cohort with the National Death Index to identify deaths and to the United States Renal Data System (USRDS) registry to determine ESRD diagnoses. Patients enter the national USRDS database after a physician files a CMS-2728 Medical Evidence Form, indicating they have initiated kidney replacement therapy (dialysis or kidney transplant). Each ESRD patient has a date of first service, determined by starting dialysis or kidney transplant, whichever occurs first. On the form, the primary attributing cause of ESRD may be indicated, including diabetic nephropathy, hypertensive nephropathy, and glomerulonephritis. In addition to ESRD overall, these three main classification groups are examined separately in the analyses described below. Hypertensive nephropathy is considered less specific and prone to greater misclassification,16 therefore, analyses for this classification are only presented in the Supplementary Material. Other classification groups of ESRD were not studied due to small numbers. A subject’s follow-up ends at the earliest occurrence of ESRD diagnosis, death, or December 31, 2009.
Statistical Analyses
Descriptive statistics were generated for the two outcomes, ESRD and mortality, and the at-risk person-years contributed toward ESRD; statistics were also examined for at-risk person-years toward death but were similar and therefore are not presented. Cox proportional hazard regression models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for the association between cumulative exposure to each MWF type (straight, soluble and synthetic with a 15-year lag) and ESRD. Risk sets were created using time since hire as the analytic timeline for models that also adjusted for race (White or Black), year hired, plant, calendar year, age, and the other two types of MWF. To be consistent with the literature on ESRD,12 our main analysis uses competing risk models, which were generated using the Fine and Gray competing risk method based on the subdistribution hazard.17 This approach allows individuals who experience the competing event to continue to contribute at-risk person-time to the event of interest. In SAS, we ran PROC PHREG with the EVENTCODE option. The competing risk model generates a subhazard ratio (sHR) and 95% CI.
The relationships between occupational exposures and chronic disease are typically non-linear, and non-parametric regression methods may be preferred.18 Exposure-response patterns for the association between ESRD and each MWF type were examined using restricted cubic splines with knots at 75th, 90th, and 99th percentiles of cases. All models were stratified to look at the associations separately for Black and White men and models were generated for ESRD overall and ESRD classification group.
A spline curve was generated for each MWF and estimates of the association with ESRD are presented at the upper deciles (60th through 90th percentiles) of exposure, based on the distribution of exposed cases. The reference group includes those not exposed to that particular fluid. We also fit models for each MWF using a continuous term for the cumulative exposure variable instead of a spline, and these results serve as our test of trend. We also fit a model with a categorical exposure variable as a point of comparison with the spline, with subjects not exposed to the specific MWF as the reference group and exposure quartiles determined by the distribution in exposed cases. The primary presentation of results is focused on the competing risk models, a preferred modeling approach for ESRD.
As a sensitivity analysis, we performed g-estimation with a structural nested accelerated failure time model19 to account for time-varying confounding by prior exposure, which can cause healthy worker survivor bias.20 See Supplementary Material for details.
All analyses were performed using SAS 9.4 (SAS Institute, Cary, NC). The Institutional Review Board at University of California, Berkeley approved the data collection procedures for this study.
RESULTS
Among the 32,025 workers, mean age at baseline was 53 years old and mean time since hire was 28 years; 83% were White (Table 1). There were 501 ESRD cases and 13,434 deaths during follow-up. Although Blacks comprised approximately 17% of person-years, they make up 34% of total ESRD cases. Relative to at-risk person-time, ESRD cases were more likely to be exposed to straight, soluble and synthetic fluids and, among the exposed, to have higher cumulative exposure.
Table 1:
Characteristics of ESRD cases, deaths, and person-time distribution, UAW-GM cohort men only, 1973–2009
| Person-years | ESRD | Deaths | |
|---|---|---|---|
| Characteristic | N=863,632 | N=501 | N=13,434 |
| Total workers, n | 32,025 | ||
| Age, mean (SD) | 52.90 (13.95) | 65.13 (12.47) | 68.68 (12.98) |
| Race, % | |||
| Whites | 83.06 | 65.87 | 82.05 |
| Blacks | 16.94 | 34.13 | 17.95 |
| Plant, % | |||
| Plant 1 | 24.24 | 38.92 | 32.05 |
| Plant 2 | 38.27 | 35.33 | 44.25 |
| Plant 3 | 36.49 | 25.75 | 23.69 |
| Calendar year of hire, mean (SD) | 1963 (10.46) | 1960 (10.45) | 1956 (10.00) |
| Years since hire, mean (SD) | 28.56 (11.94) | 39.22 (11.51) | 38.75 (12.20) |
| Straight MWF* | |||
| Non exposed | 56.95 | 48.82 | 45.82 |
| Exposed | 43.05 | 51.18 | 54.18 |
| Cumulative, mg/m3-year, mean (SD) | 1.92 (8.66) | 2.65 (9.40) | 3.10 (12.02) |
| Soluble MWF* | |||
| Non exposed | 28.88 | 13.37 | 14.00 |
| Exposed | 71.12 | 86.63 | 86.00 |
| Cumulative, mg/m3-year, mean (SD) | 6.67 (12.68) | 10.24 (14.97) | 12.33 (18.00) |
| Synthetic MWF* | |||
| Non exposed, % | 75.77 | 73.45 | 70.70 |
| Exposed, % | 24.23 | 26.55 | 29.30 |
| Cumulative, mg/m3-year, mean (SD) | 0.46 (3.05) | 0.56 (4.22) | 0.82 (4.49) |
Abbreviations: ESRD, end-stage renal disease; MWF, metalworking fluids; SD, standard deviation
MWF exposure in units of mg/m3-year with 15-year lag
Among 501 ESRD cases, there were 184 cases of diabetic nephropathy (123 White males and 61 Black males), 178 cases of hypertensive nephropathy (100 White males and 78 Black males), and 59 glomerulonephritis cases (44 White males and 15 Black males), with the remaining designated as other or unknown cause. The crude background rate of ESRD among men was 580 cases per million person-years, but varies by race with 460 and 1169 per million person-years for White and Black men, respectively.
Figure 1A presents splines for the relationship between each type of MWF and ESRD estimated using standard Cox proportional hazards regression. There appeared to be no association between straight MWF and ESRD. For soluble and synthetic MWF, the natural log of the HRs were below the null across the range of cumulative MWF and continued to decrease for soluble MWF. Figure 1B displays the association between each MWF and ESRD when modeled with the competing risk model. Overall, there was a shift upward in the natural log of the sHR for each MWF type relative to the standard Cox model. In particular, the estimates for straight MWF were entirely above the null and exhibited an increasing association with increasing exposure, though confidence intervals included the null (not shown). For soluble MWF, the association increased and then decreased at higher cumulative exposure. For synthetic MWF, both models suggested an inverse association between synthetic MWF and ESRD. The splines Figure provide a visual examination of the exposure-response relationship. The spline models generate a single curve for each MWF, and we present results at specific points along the curve in Table 2 (results for both standard Cox and competing risk models). For the remainder of the analyses, we focus on results from the competing risk regression models.
Figure 1.
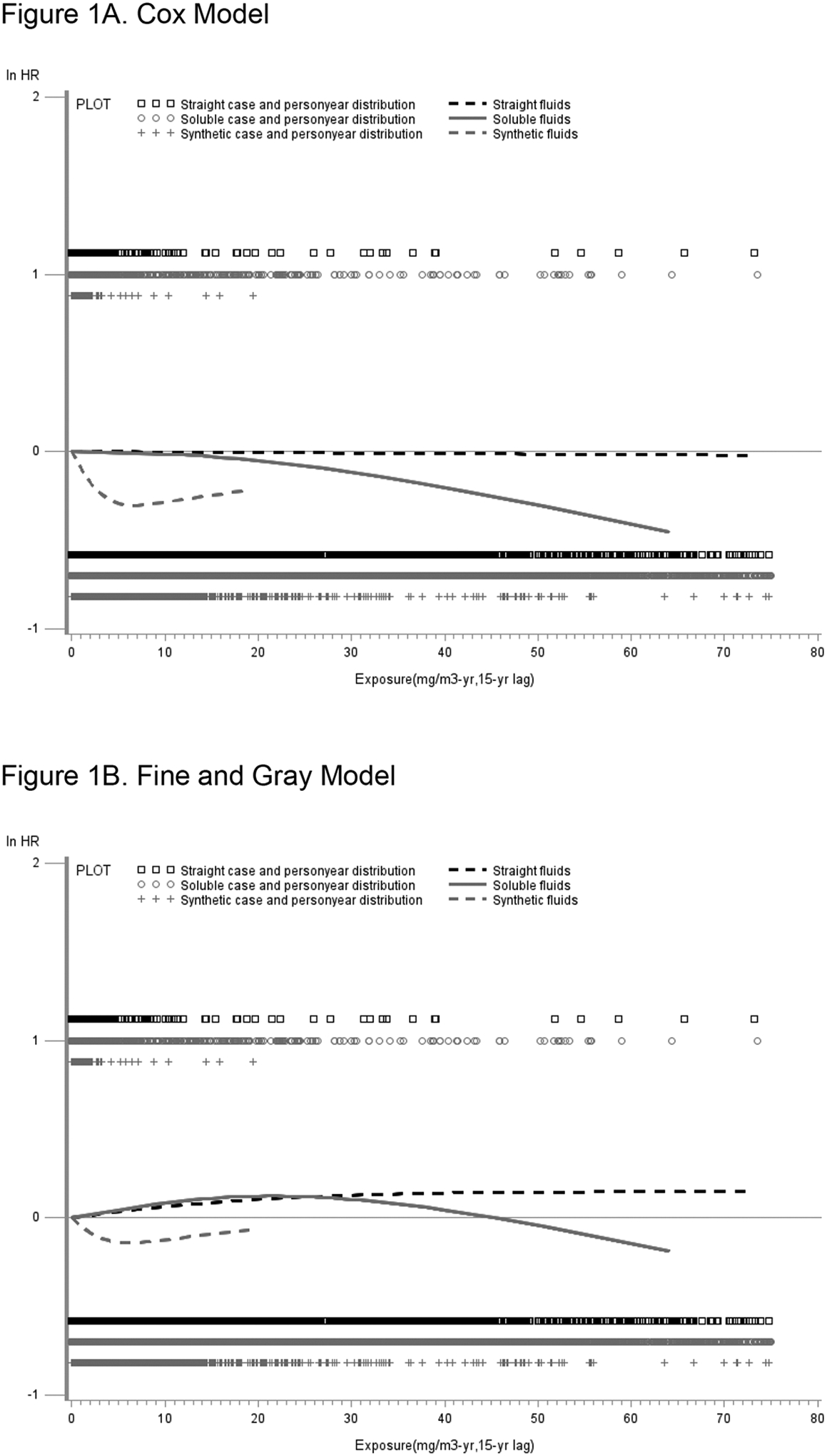
The association between three types of MWF (cumulative exposure to straight, soluble, and synthetic MWF, mg/m3-yr,15-year lag) and ESRD among male autoworkers, controlling for age, race, calendar year, year hired, plant, other MWF, and time since hire as the analytic timeline in the United Autoworkers–General Motors cohort 1973–2009, Michigan, USA. (1A) Cubic splines representing the natural log of the hazard ratio (ln HR) and 95% confidence interval (95% CI) for the association using standard Cox proportional hazards regression models and (1B) cubic splines representing the ln sHR and 95% CI for the association using competing risks models. The solid horizontal line represents the null value. The rug plot above the null indicates ESRD case distribution for straight, soluble and synthetic MWF exposure and the rug plot below the null indicates the person-year distribution for three MWF exposures, respectively. Each spline is truncated at the 99th percentile of the exposed subjects.
Abbreviations: CI, confidence interval; ESRD, end-stage renal disease; MWF, metalworking fluids; ln HR, natural log of the hazard ratio
Table 2:
Association between metalworking fluids and ESRD: Exposure modeled with cubic splines in standard Cox proportional hazards regression and competing risk regression, among all Males.
| Cumulative exposure | Standard Cox | Fine and Gray | ||||||
|---|---|---|---|---|---|---|---|---|
| mg/m3-yr, | ESRD n=501† | ESRD n=501† | Death n=13,434 | |||||
| MWF type | Percentile* | 15-yr lag | HR‡ | 95% CI | sHR‡ | 95% CI | sHR‡ | 95% CI |
| Straight | 60 | 1.44 | 1.00 | 0.96, 1.04 | 1.01 | 0.97, 1.05 | 1.00 | 0.99, 1.01 |
| 70 | 2.12 | 1.00 | 0.94, 1.06 | 1.01 | 0.96, 1.07 | 1.00 | 0.99, 1.01 | |
| 80 | 4.26 | 1.00 | 0.88, 1.12 | 1.03 | 0.92, 1.15 | 1.01 | 0.99, 1.03 | |
| 90 | 11.91 | 0.99 | 0.75, 1.32 | 1.07 | 0.83, 1.40 | 1.02 | 0.97, 1.07 | |
| Soluble | 60 | 9.33 | 0.99 | 0.86, 1.14 | 1.08 | 0.93, 1.26 | 1.00 | 0.97, 1.02 |
| 70 | 13.30 | 0.98 | 0.81, 1.19 | 1.11 | 0.91, 1.35 | 1.00 | 0.96, 1.03 | |
| 80 | 18.67 | 0.96 | 0.75, 1.22 | 1.13 | 0.88, 1.45 | 1.00 | 0.95, 1.04 | |
| 90 | 28.74 | 0.90 | 0.67, 1.20 | 1.11 | 0.83, 1.50 | 1.00 | 0.94, 1.05 | |
| Synthetic | 60 | 0.84 | 0.92 | 0.81, 1.05 | 0.96 | 0.85, 1.09 | 0.99 | 0.97, 1.01 |
| 70 | 1.51 | 0.87 | 0.70, 1.08 | 0.93 | 0.76, 1.15 | 0.99 | 0.96, 1.03 | |
| 80 | 1.81 | 0.85 | 0.66, 1.10 | 0.92 | 0.72, 1.18 | 0.99 | 0.95, 1.03 | |
| 90 | 2.90 | 0.79 | 0.56, 1.14 | 0.89 | 0.64, 1.26 | 0.99 | 0.93, 1.04 | |
Abbreviations: CI, confidence interval; ESRD, end-stage renal disease; HR, hazard ratio; MWF, metalworking fluids
For each MWF type, a restricted cubic spline was used to estimate the HR; we present the HR at specific points along the spline, based on percentile of exposure for the exposed cases
Distribution of ESRD cases and person-time in each spline are shown in Figures 1A and 1B
Adjusted for age, race, calendar year, year hired, plant, other MWFs, and with time since hire as the analytic timeline
In Table 3, we present results by ESRD classification, with sHR estimates at specific points along the spline curve for each MWF. For all males, among the 184 cases of diabetic nephropathy, there was an increasing ESRD subhazard with increasing cumulative exposure for both soluble and synthetic MWF. For glomerulonephritis, we observed an increasing exposure-response pattern for straight MWF, with a sHR of 1.18 (95% CI 0.99, 1.14) at the 60th percentile of cumulative exposure (corresponding to 1.44 mg/m3-yr). For hypertensive nephropathy, results were similar to ESRD overall (Supplementary Materials). When we used a continuous term to model exposure to each MWF instead of a spline, the p-values indicated there was no statistically significant linear relationship (data not shown).
Table 3:
Association between metalworking fluids and ESRD classification: Exposure modeled with cubic splines in competing risk regression.
| Cumulative exposure | All males | White males | Black males | |||||
|---|---|---|---|---|---|---|---|---|
| ESRD classification | MWF type | Percentile* | sHR† | 95% CI | sHR† | 95% CI | sHR† | 95% CI |
| Diabetic nephropathy | n=184 cases | n=123 cases | n=61 cases | |||||
| Straight | 60 | 0.99 | 0.94, 1.04 | 1.01 | 0.96, 1.07 | 0.97 | 0.68, 1.39 | |
| 70 | 0.99 | 0.92, 1.07 | 1.02 | 0.94, 1.10 | 0.95 | 0.58, 1.57 | ||
| 80 | 0.98 | 0.84, 1.14 | 1.04 | 0.89, 1.22 | 0.87 | 0.38, 1.97 | ||
| 90 | 0.95 | 0.66, 1.39 | 1.12 | 0.75, 1.67 | 0.46 | 0.12, 1.79 | ||
| Soluble | 60 | 1.28 | 1.00, 1.64 | 1.24 | 0.90, 1.71 | 1.39 | 0.94, 2.05 | |
| 70 | 1.38 | 0.98, 1.92 | 1.32 | 0.86, 2.01 | 1.56 | 0.91, 2.66 | ||
| 80 | 1.45 | 0.96, 2.20 | 1.36 | 0.81, 2.27 | 1.75 | 0.88, 3.49 | ||
| 90 | 1.38 | 0.84, 2.26 | 1.23 | 0.68, 2.24 | 1.87 | 0.80, 4.38 | ||
| Synthetic | 60 | 1.15 | 0.93, 1.41 | 1.07 | 0.87, 1.32 | 1.73 | 1.04, 2.87 | |
| 70 | 1.25 | 0.88, 1.77 | 1.12 | 0.78, 1.61 | 2.32 | 1.05, 5.10 | ||
| 80 | 1.29 | 0.87, 1.93 | 1.14 | 0.75, 1.73 | 2.54 | 1.05, 6.16 | ||
| 90 | 1.39 | 0.82, 2.39 | 1.18 | 0.66, 2.10 | 2.99 | 0.96, 9.28 | ||
| Glomerulonephritis | n=59 cases | n=44 cases | n=15 cases | |||||
| Straight | 60 | 1.18 | 0.99, 1.41 | 1.21 | 1.00, 1.47 | 4.16 | 1.00, 17.27 | |
| 70 | 1.28 | 0.98, 1.65 | 1.33 | 1.00, 1.76 | 3.76 | 0.78, 18.15 | ||
| 80 | 1.59 | 0.96, 2.63 | 1.73 | 1.00, 3.00 | 0.64 | 0.07, 6.04 | ||
| 90 | 2.09 | 0.77, 5.67 | 2.48 | 0.82, 7.54 | - | - | ||
| Soluble | 60 | 1.02 | 0.66, 1.57 | 1.15 | 0.73, 1.79 | 0.64 | 0.21, 1.92 | |
| 70 | 1.02 | 0.57, 1.83 | 1.21 | 0.66, 2.22 | 0.55 | 0.13, 2.24 | ||
| 80 | 1.02 | 0.49, 2.14 | 1.28 | 0.58, 2.80 | 0.47 | 0.09, 2.50 | ||
| 90 | 1.00 | 0.40, 2.52 | 1.38 | 0.52, 3.68 | 0.38 | 0.06, 2.44 | ||
| Synthetic | 60 | 0.96 | 0.54, 1.72 | 1.00 | 0.58, 1.71 | - | ||
| 70 | 0.92 | 0.37, 2.31 | 0.98 | 0.40, 2.36 | - | |||
| 80 | 0.90 | 0.32, 2.53 | 0.96 | 0.35, 2.61 | - | |||
| 90 | 0.82 | 0.23, 2.97 | 0.87 | 0.25, 3.10 | - | |||
Abbreviations: CI, confidence interval; ESRD, end-stage renal disease; HR, hazard ratio; MWF, metalworking fluids
For each MWF type, a restricted cubic spline was used to estimate the HR; we present the HR at specific points along the spline, based on percentile of exposure for the exposed cases
Adjusted for age, calendar year, year hired, plant, other MWFs, and time since hire (as the analytic timeline)
The associations between MWF and ESRD classification were examined separately for White and Black males (Table 3). For both, cumulative exposure to soluble MWF was related to an increased subhazard of diabetic nephropathy, though confidence intervals contained the null. Only Black males exhibited an increasing subhazard for diabetic nephropathy with increasing cumulative synthetic exposure (sHR=1.73, 95% CI (1.04, 2.87) at 60% cumulative exposure (0.84 mg/m3-yr)). For glomerulonephritis, there was an association with straight MWF for both White and Black males. Though models suggested a potential association among Black males, the precision of our estimates for glomerulonephritis was limited by case numbers. In models with exposure included as a continuous term rather than a spline, there appeared to be no linear change in the sHR with increasing exposure and the p-values were not statistically significant (data not shown).
For comparison, we generated a competing risk regression for diabetic nephropathy that modeled MWF exposure categorically instead of using splines. Results, stratified by race, are presented in Tables 4A and 4B. The exposure-response patterns were similar to the splines in the two higher categories of cumulative exposure for all three MWF: elevated sHRs were observed for soluble MWF for White males; for Black males, elevated subhazard was observed for synthetic fluids (the 3-fold increase was consistent with the spline model), followed by soluble MWF, and a reduced subhazard for straight MWF. No trend test was statistically significant.
Table 4:
Association between MWFs and diabetic nephropathy: Exposure modeled categorically in Fine and Gray competing risk regression, White and Black males separately
| 4B. Black Males | |||||||
|---|---|---|---|---|---|---|---|
| Cumulative exposure mg/m3-yr, | Cases N=123 | Person-years* | |||||
| MWF type | Percentile | 15-yr lag | N | % | % | sHR† | 95% CI |
| Straight |
0 | 59 | 47.97 | 54.16 | Ref | ||
| <25 | >0 – <0.3 | 16 | 13.01 | 14.37 | 0.78 | 0.39, 1.56 | |
| 25 – <50 | 0.3 – <0.9 | 11 | 8.94 | 11.09 | 0.58 | 0.27, 1.25 | |
| 50 – <75 | 0.9 – <3.0 | 17 | 13.82 | 9.66 | 0.98 | 0.56, 1.75 | |
| ≥75 | ≥3.0 | 20 | 16.26 | 10.71 | 1.04 | 0.62, 1.75 | |
| p-value | 0.22 | ||||||
| Soluble |
0 | 16 | 13.01 | 28.60 | Ref | ||
| <25 | <2.2 | 24 | 19.51 | 22.98 | 1.16 | 0.58, 2.38 | |
| 25 – <50 | 2.2 – <6.2 | 32 | 26.02 | 20.27 | 1.56 | 0.79, 3.08 | |
| 50 – <75 | 6.2 – <16.2 | 26 | 21.14 | 16.71 | 1.19 | 0.59, 2.41 | |
| ≥75 | ≥16.2 | 25 | 20.33 | 11.44 | 1.36 | 0.66, 2.79 | |
| p-value | 0.43 | ||||||
| Synthetic |
0 | 88 | 71.54 | 73.45 | Ref | ||
| <25 | 0 – <0.2 | 9 | 7.32 | 8.78 | 0.73 | 0.31, 1.72 | |
| 25 – <50 | 0.2 – <0.5 | 3 | 2.44 | 4.74 | 0.46 | 0.12, 1.72 | |
| 50 – <75 | 0.5 – <1.5 | 11 | 8.94 | 5.80 | 1.29 | 0.63, 2.66 | |
| ≥75 | ≥1.5 | 12 | 9.76 | 7.24 | 0.91 | 0.48, 1.72 | |
| p-value | 0.37 | ||||||
| 4B. Black Males | |||||||
| Cumulative exposure mg/m3-yr, | Cases N=61 | Person-years** | |||||
| MWF type | Percentile | 15-yr lag | N | % | % | sHR† | 95% CI |
| Straight | 0 | 38 | 62.30 | 65.59 | Ref | ||
| <50 | >0 – <0.9 | 13 | 21.31 | 19.57 | 0.48 | 0.25, 0.91 | |
| ≥50 | ≥0.9 | 10 | 16.39 | 14.90 | 0.58 | 0.28, 1.18 | |
| p-value | 0.15 | ||||||
| Soluble | 0 | 4 | 6.56 | 30.23 | Ref | ||
| <25 | >0 – <2.2 | 17 | 27.87 | 22.51 | 1.89 | 0.62, 5.83 | |
| 25-<50 | 2.2 – <6.2 | 10 | 16.39 | 15.78 | 1.12 | 0.33, 3.85 | |
| ≥50 | ≥6.2 | 30 | 49.18 | 31.48 | 2.10 | 0.71, 6.20 | |
| p-value | 0.95 | ||||||
| Synthetic | 0 | 46 | 75.41 | 87.12 | Ref | ||
| >0 | 15 | 24.59 | 12.88 | 3.08 ‡ | 1.70, 5.58 | ||
| p-value | 0.19 | ||||||
Abbreviations: CI, confidence interval; ESRD, end-stage renal disease; HR, hazard ratio; MWF, metalworking fluids
White males contributed 717,575 person-years
Black males contributed 146,374 person-years
Adjusted for age, calendar year, year hired, plant, other MWFs, and time since hire (as the analytic timeline)
p-value from trend test
G-estimation from the accelerated failure time model estimated that onset of ESRD could have been delayed by an estimated average of 0.46 years (95% CI: −0.23, 6.45) if straight MWF had been banned starting in 1958. The corresponding estimates were 0.58 years (95% CI: −0.68, 2.60) and 1.15 years (95% CI: −0.05, 93.99) for soluble and synthetic fluids, respectively (Supplementary Material).
DISCUSSION
In a population of male autoworkers, there was no association between MWF types and ESRD overall, though within ESRD classification, we observed an association between straight MWF and glomerulonephritis for both Black and White males, while synthetic fluid was associated with diabetic nephropathy among Black males only. However, our case numbers within classification group were limited. G-estimation results with adjustment for healthy worker survivor effect likewise suggest rather weak associations overall. However, the estimates are averaged over all the workers who experienced ESRD, even those who were not exposed and whose date of onset would therefore not have changed under a ban on MWF exposure. These workers still appear in the denominator and thus bring down the average.
While there was a suggested association between straight MWF and glomerulonephritis, higher case numbers are needed for further study. The other MWF types were introduced over time, in part, to reduce workers’ exposure to PAHs,6 resulting in a lower percentage of workers exposed to straight MWF. These factors limit our ability to study the association between straight MWF and glomerulonephritis further. Other epidemiologic studies have also examined the relationship between MWF and glomerulonephritis or ESRD more generally. One cohort study with seven CKD deaths reported no association with MWF.21 A case-control study reported a reduced risk of ESRD following MWF exposure;3 however, exposure was self-reported, MWF type was not collected, and 20% of cases died before interview. Although we cannot say for certain whether PAHs was the specific component of straight MWF that explains the observed association with glomerulonephritis in the present study, previous research suggests mechanisms by which hydrocarbons may harm glomerular cells specifically.22 In vitro studies found that glomerular cells exhibited impaired mitochondrial function and depleted antioxidant resources following hydrocarbon exposure.23 In rats, hydrocarbon exposure reportedly reduced mesangial cell numbers and changed podocyte cell densities in glomeruli, suggesting that hydrocarbon exposure may reduce glomerular function.24
A novel finding was the relationship between soluble and synthetic MWF and diabetic nephropathy. We did not have individual-level diabetes data for the cohort, though the vast majority of ESRD patients with diabetes will be classified as diabetic nephropathy. We cannot determine whether MWF influenced the incidence of diabetes alone from which kidney disease followed or if MWF may have accelerated kidney disease progression among diabetics, although potentially both may occur. Limited prior reports have indicated that diabetes prevalence among autoworkers is elevated relative to the broader U.S. population.25,26 Generally, studies between occupational exposures and diabetes lack quantitative exposure estimates and incident disease. Diabetes and diabetic nephropathy have been associated with exposure to other environmental toxicants and it is thought that the arylhydrocarbon receptor (AhR) may have a role.27–30 Though the mechanisms are not yet understood, the presence of exogenous exposures may further activate AhR signaling pathways that enhance chronic kidney disease progression.29
The associations with diabetic nephropathy observed in our study population raise the question of what MWF component(s) may be influential. Our results for soluble MWF were more stable than those for synthetic MWF, with nearly 90% of cases exposed to soluble but only about a quarter exposed to synthetic. Soluble and synthetic fluids are water-based fluids, but soluble MWF also contain oil and PAHs.6 Nitrites, found in both soluble and synthetic fluids, are a component of potential importance. Nitrate-nitrite-nitrosamines from environmental and dietary sources has been associated with both type 1 and type 2 diabetes.31–33 Less well known is the influence of other MWF components on diabetes and diabetic nephropathy. Study industrial hygienists (including SKH) have previously reported detecting ethanolamines from MWF samples at one of the auto plants.34 All four synthetic MWF samples contained ethanolamines (10–40%), while none of five straight and only two of four soluble fluids (2% and 5%) had detectable levels of the other ethanolamines (limit of detection 0.005%). Diethanolamine specifically was detected in two of four synthetic and semisynthetic MWF, but not in any of five straight or four soluble MWF (i.e., <0.1%). Lastly, MWF contain metal contaminants. Metals have been associated with diabetes and glycemic control.35 It is conceivable that metal contaminants, chemical additives, or both could contribute to development of diabetic nephropathy.
In the autoworkers cohort, the classification of primary attributing cause of ESRD reflects data entry onto the CMS Medical Evidence Form and likely involves misclassification.36 For example, clinical confirmation of glomerulonephritis requires biopsy, though in absence of a biopsy, other factors (i.e., not diabetic, high grade proteinuria and/or nephritic sediment) may lead to an assumption of glomerulonephritis. For diabetic nephropathy, although all cases may have diabetes, there are specific requirements to attribute diabetes as causing kidney failure, though a medical records review found this is not consistently met.37 For the present study, we have no reason to think misclassification occurred differentially with respect to MWF exposure.
The ESRD rate among Black males was more than 2.5 times that of White males in the study population. This is consistent with research showing lifetime ESRD incidence among Blacks in the U.S. is two- to three-fold higher than Whites.38 Further, there appeared to be differences in the associations with respect to MWF type. Black males exhibited associations with MWF and diabetic nephropathy and glomerulonephritis, though these associations were not observed for White males. Possible explanations include unmeasured differences related to jobs and exposure concentrations or personal protective equipment, genetic differences in disease susceptibility or exposure metabolism, or stress related to racism, as well as differences in diet, socioeconomic status, lifestyle factors, and access to quality health care.
For the majority of those with CKD, death precedes ESRD development.1 The competing risk regression model was designed to address the modified chance of observing the event of interest, an approach used in ESRD research. For occupational cohorts in particular, the exposure distribution is often highly skewed, the true response may be non-linear, and the depletion of susceptibles can lead to a strong drop-off in the association at the upper range of exposure.39 Indeed, the use of splines revealed that there were few circumstances in which the exposure-response relationship was monotonic.
As is typical of large occupational cohort studies, we were lacking individual-level information on risk factors for ESRD. For these factors to account for the observed associations, they would also have to be associated with MWF exposure. Typically, this is ultimately what makes a strong risk factor for the outcome a very weak confounder for an occupational study. For example, occupational studies of lung cancer commonly lack smoking data, yet smoking has rarely been found to be a strong confounder. A strength of the study was quantitative exposure estimates, and it is unlikely that risk factors for ESRD would be tightly related to those exposure measures.
On the other hand, a stronger argument for unmeasured confounding could be made for other occupational exposures. In a recent review of existing industrial hygiene records from the UAW-GM study, industrial hygienists, including one from the original research team (SKH), investigated measured air concentrations of asbestos and four chlorinated solvents, trichloroethylene (TCE), methyl chloroform, methylene chloride, and perchloroethylene, by plant, job, operation, and dates used (1971–1990).40 It was determined that asbestos exposure rarely occurred in departments in which MWF were used and that the manner in which solvents were used would have resulted in few workers with exposure to both solvents and MWF, making all of these agents unlikely confounders in this analysis.
The signature strengths of this study are the quantitative exposure estimates, completeness of the cohort, and the number of ESRD cases, which allowed us to study ESRD classification groups.5 ESRD classification is rarely studied with workplace quantitative MWF exposures. Our analysis involved a number of regression models and results were generally of marginal statistical significance and should be viewed cautiously. The results suggesting that MWF exposure may influence ESRD should be replicated, and the component or mixtures that drive these relationships requires more study.
Supplementary Material
KEY MESSAGES.
What is already known about this subject?
The prevalence of end-stage renal disease (ESRD) is increasing in the United States, yet we lack information regarding the contribution of occupational MWF exposures.
What are the new findings?
This study used quantitative estimates of three types of metalworking fluids (straight, soluble, and synthetic) to examine associations with overall ESRD and for ESRD classification groups among male autoworkers.
Glomerulonephritis was associated with straight fluids, while diabetic nephropathy was associated with exposure to soluble fluids.
Associations between MWF exposures and ESRD classification group may differ by race, with associations more evident among Black males.
How might this impact on policy or clinical practice in the foreseeable future?
This research suggests that those with chronic exposure to metalworking fluids may be at elevated risk of chronic kidney disease, and potentially diabetes. Clinicians should consider these fluids as potential contributors to the development of these conditions and conduct appropriate screening evaluations to detect these conditions early.
ACKNOWLEDGEMENTS
Authors appreciate the technical assistance in dataset development provided by Clara Chen and Michel Winter from Boston University Data Coordinating Center. We also thank Elizabeth Lutzker from University of California, Berkeley for assistance in the data linkage.
FUNDING
This publication was supported by grants R01 OH010180, R01 OH010028 funded by the Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers of Disease Control and Prevention or the Department of Health and Human Services.
Footnotes
COMPETING INTERESTS
NONE
DATA AVAILABILITY
The data that can be made available upon reasonable request are deidentified participant data accompanied by a data dictionary. Data can be requested from Liza Lutzker, Data Manager, UC Berkeley, ORCID: 0000-0003-0611-0158. Conditions of reuse would include submission of researcher’s IRB approval to the UC Berkeley IRB and pending permission from the National Death Index and US Renal Data System.
REFERENCES
- 1.Dalrymple LS, Katz R, Kestenbaum B et al. Chronic kidney disease and the risk of end-stage renal disease versus death. J Gen Intern Med 2011;26:379–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Saran R, Robinson B, Abbott KC et al. US Renal Data System 2019 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am J Kidney Dis 2019. [DOI] [PubMed] [Google Scholar]
- 3.Steenland NK, Thun MJ, Ferguson CW, Port FK. Occupational and other exposures associated with male end-stage renal disease: a case/control study. Am J Public Health 1990;80:153–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sponholtz TR, Sandler DP, Parks CG, Applebaum KM. Occupational Exposures and Chronic Kidney Disease: Possible Associations With Endotoxin and Ultrafine Particles. American Journal of Industrial Medicine 2016;59:1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mirer F. Updated epidemiology of workers exposed to metalworking fluids provides sufficient evidence for carcinogenicity. Appl Occup Environ Hyg 2003;18:902–12. [DOI] [PubMed] [Google Scholar]
- 6.Friesen MC, Costello S, Thurston SW, Eisen EA. Distinguishing the common components of oil- and water-based metalworking fluids for assessment of cancer incidence risk in autoworkers. Am J Ind Med 2011;54:450–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Simpson AT, Stear M, Groves JA et al. Occupational exposure to metalworking fluid mist and sump fluid contaminants. Ann Occup Hyg 2003;47:17–30. [DOI] [PubMed] [Google Scholar]
- 8.Cherrie JW, Semple S. Dermal exposure to metalworking fluids and medium-chain chlorinated paraffin (MCCP). Ann Occup Hyg 2010;54:228–35. [DOI] [PubMed] [Google Scholar]
- 9.Program NT. NTP Toxicology and Carcinogenesis Studies of Diethanolamine (CAS No. 111-42-2) in F344/N Rats and B6C3F1 Mice (Dermal Studies) 1999;1–212. [PubMed]
- 10.Ravnskov U. Hydrocarbons may worsen renal function in glomerulonephritis: a meta-analysis of the case-control studies. Am J Ind Med 2000;37:599–606. [DOI] [PubMed] [Google Scholar]
- 11.Ravnskov U. Experimental glomerulonephritis induced by hydrocarbon exposure: a systematic review. BMC Nephrol 2005;6:15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tabrizi R, Moosazadeh M, Sekhavati E et al. Competing Risk Analyses of Patients with End-Stage Renal Disease. Electron Physician 2015;7:1458–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Eisen EA, Tolbert PE, Monson RR, Smith TJ. Mortality studies of machining fluid exposure in the automobile industry I: A standardized mortality ratio analysis. Am J Ind Med 1992;22:809–24. [DOI] [PubMed] [Google Scholar]
- 14.Radican L, Wartenberg D, Rhoads GG et al. A retrospective occupational cohort study of end-stage renal disease in aircraft workers exposed to trichloroethylene and other hydrocarbons. J Occup Environ Med 2006;48:1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Woskie SR, Smith TJ, Hallock MF et al. Size-selective pulmonary dose indices for metal-working fluid aerosols in machining and grinding operations in the automobile manufacturing industry. Am Ind Hyg Assoc J 1994;55:20–9. [DOI] [PubMed] [Google Scholar]
- 16.Pirkle JL, Freedman BI. Hypertension and chronic kidney disease: controversies in pathogenesis and treatment. Minerva Urologica E Nefrologica 2013;65:37–50. [PMC free article] [PubMed] [Google Scholar]
- 17.Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. Journal of the American Statistical Association 1999;94:496–509. [Google Scholar]
- 18.Malloy EJ, Miller KL, Eisen EA. Rectal cancer and exposure to metalworking fluids in the automobile manufacturing industry. Occup Environ Med 2007;64:244–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Picciotto S, Ljungman PL, Eisen EA. Straight Metalworking Fluids and All-Cause and Cardiovascular Mortality Analyzed by Using G-Estimation of an Accelerated Failure Time Model With Quantitative Exposure: Methods and Interpretations. Am J Epidemiol 2016;183:680–8. [DOI] [PubMed] [Google Scholar]
- 20.Picciotto S, Hertz-Picciotto I. Commentary: healthy worker survivor bias: a still-evolving concept. Epidemiology 2015;26:213–5. [DOI] [PubMed] [Google Scholar]
- 21.Silverstein M, Park R, Marmor M, Maizlish N, Mirer F. Mortality among bearing plant workers exposed to metalworking fluids and abrasives. J Occup Med 1988;30:706–14. [PubMed] [Google Scholar]
- 22.Hotz P. Occupational hydrocarbon exposure and chronic nephropathy. Toxicology 1994;90:163–283. [DOI] [PubMed] [Google Scholar]
- 23.Parrish AR, Alejandro NF, Bowes Iii RC, Ramos KS. Cytotoxic Response Profiles of Cultured Renal Epithelial and Mesenchymal Cells toSelected Aromatic Hydrocarbons. Toxicol In Vitro 1998;12:219–32. [DOI] [PubMed] [Google Scholar]
- 24.Nanez A, Alejandro NF, Falahatpisheh MH, Kerzee JK, Roths JB, Ramos KS. Disruption of glomerular cell-cell and cell-matrix interactions in hydrocarbon nephropathy. Am J Physiol Renal Physiol 2005;289:F1291–303. [DOI] [PubMed] [Google Scholar]
- 25.Park RM, Mirer FE. A survey of mortality at two automotive engine manufacturing plants. Am J Ind Med 1996;30:664–73. [DOI] [PubMed] [Google Scholar]
- 26.Gossain VV, Rosenman KD, Gardiner JC, Thawani HT, Tang X. Evaluation of control of diabetes mellitus in a subspecialty clinic. Endocr Pract 2010;16:178–86. [DOI] [PubMed] [Google Scholar]
- 27.Yaqoob M, Patrick AW, McClelland P et al. Occupational hydrocarbon exposure and diabetic nephropathy. Diabet Med 1994;11:789–93. [DOI] [PubMed] [Google Scholar]
- 28.Everett CJ, Thompson OM. Association of DDT and heptachlor epoxide in human blood with diabetic nephropathy. Rev Environ Health 2015;30:93–7. [DOI] [PubMed] [Google Scholar]
- 29.Zhao H, Chen L, Yang T et al. Aryl hydrocarbon receptor activation mediates kidney disease and renal cell carcinoma. J Transl Med 2019;17:302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Duncan BB, Castilhos CD, Bracco PA et al. Aryl-hydrocarbon receptor binding and the incidence of type 2 diabetes: the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil). Environ Health 2020;19:105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Tong M, Neusner A, Longato L, Lawton M, Wands JR, de la Monte SM. Nitrosamine exposure causes insulin resistance diseases: relevance to type 2 diabetes mellitus, non-alcoholic steatohepatitis, and Alzheimer’s disease. J Alzheimers Dis 2009;17:827–44. [PMC free article] [PubMed] [Google Scholar]
- 32.de la Monte SM, Tong M, Lawton M, Longato L. Nitrosamine exposure exacerbates high fat diet-mediated type 2 diabetes mellitus, non-alcoholic steatohepatitis, and neurodegeneration with cognitive impairment. Mol Neurodegener 2009;4:54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bahadoran Z, Ghasemi A, Mirmiran P, Azizi F, Hadaegh F. Nitrate-nitrite-nitrosamines exposure and the risk of type 1 diabetes: A review of current data. World J Diabetes 2016;7:433–440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kenyon EM, Hammond SK, Shatkin J, Woskie SR, Hallock MF, Smith TJ. Ethanolamine exposures of workers using machining fluids in the automotive parts manufacturing industry. Applied Occupational and Environmental Hygiene 1993;8:655–61. [Google Scholar]
- 35.Gonzalez-Villalva A, Colin-Barenque L, Bizarro-Nevares P et al. Pollution by metals: Is there a relationship in glycemic control? Environ Toxicol Pharmacol 2016;46:337–43. [DOI] [PubMed] [Google Scholar]
- 36.Layton JB, Hogan SL, Jennette CE et al. Discrepancy between Medical Evidence Form 2728 and renal biopsy for glomerular diseases. Clin J Am Soc Nephrol 2010;5:2046–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Yuan CM, Nee R, Ceckowski KA, Knight KR, Abbott KC. Diabetic nephropathy as the cause of end-stage kidney disease reported on the medical evidence form CMS2728 at a single center. Clin Kidney J 2017;10:257–262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Grams ME, Chow EK, Segev DL, Coresh J. Lifetime incidence of CKD stages 3–5 in the United States. Am J Kidney Dis 2013;62:245–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Stayner L, Steenland K, Dosemeci M, Hertz-Picciotto I. Attenuation of exposure-response curves in occupational cohort studies at high exposure levels. Scand J Work Environ Health 2003;29:317–24. [DOI] [PubMed] [Google Scholar]
- 40.Shrestha D, Liu S, Hammond SK et al. Risk of renal cell carcinoma following exposure to metalworking fluids among autoworkers. Occup Environ Med 2016;73:656–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that can be made available upon reasonable request are deidentified participant data accompanied by a data dictionary. Data can be requested from Liza Lutzker, Data Manager, UC Berkeley, ORCID: 0000-0003-0611-0158. Conditions of reuse would include submission of researcher’s IRB approval to the UC Berkeley IRB and pending permission from the National Death Index and US Renal Data System.