

Abstract
Previously, the authors reported the utility of urinary vanin‐1 as an early biomarker of kidney injury in spontaneously hypertensive rats and in humans. However, little is known about whether urinary vanin‐1 can be used to predict the clinical outcome. This study aimed to evaluate the predictive power of urinary vanin‐1 based on kidney function decline in hypertensive patients. The authors measured urinary vanin‐1 in 147 patients at the baseline and examined its association with the incidence of ≥20% decline in the estimated glomerular filtration rate (eGFR) using the Cox regression analysis. The mean age of the patients averaged 72.9 ± 8.2 years, and 39% were women. Median (interquartile range) urinary vanin‐1 was 0.33 (0–2.6) ng/mg Cr During a median follow‐up of 12 months, 14 patients showed kidney function decline. A higher urinary vanin‐1 level was associated with an increased risk of kidney function decline (hazard ratio, 9.87; 95% CI, 1.11–87.5) (p = .04) in the fully adjusted model. In conclusion, urinary vanin‐1 is an independent risk factor for kidney function decline in hypertensive patients and it could be useful in clinical settings. The underlying pathophysiologic mechanisms warrant additional investigation.
Keywords: biomarker, chronic kidney disease, progression
1. BACKGROUND
Chronic kidney disease (CKD) has become a worldwide health problem in recent years due to its high prevalence and heavy burden. CKD is a heterogeneous condition with multiple underlying causes, and the blood pressure (BP) is one of the strong risk factors for CKD. 1 , 2 CKD often leads to end‐stage kidney disease (ESKD) 3 and is an independent risk factor for all‐cause mortality including cardiovascular events, 4 , 5 so early detection and appropriate intervention during the progression of CKD are necessary for the prevention of a further increase in the number of patients with ESKD. The identification of novel biomarkers that enable screening for asymptomatic kidney disease or predict a decline in the estimated glomerular filtration rate (eGFR) is important in current CKD research. 6
Traditional kidney biomarkers, such as serum creatinine (Cr) and proteinuria, which are nonspecific for the type of kidney injury, elevate late with CKD progression and lack reliability in predicting a decline in the kidney function. 7 , 8 Previously, we reported that urinary vanin‐1 was a potential renal biomarker. 9 Vanin‐1 is glycosylphosphatidylinositol (GPI)‐anchored pantetheinase, 10 , 11 and antioxidant response‐like elements within the promoter region of vanin‐1 (VNN1) act as stress‐regulated targets and enhance VNN1 expression in the presence of oxidative stress. We detected urinary vanin‐1 in an early stage of CKD using spontaneously hypertensive rats. 12 , 13 In addition, urinary vanin‐1 is closely and independently associated with CKD in hypertensive patients. 14 However, it remains unknown whether vanin‐1 can be used to predict kidney function decline. The aim of this study was to determine whether urinary vanin‐1 can be used as a biomarker of kidney function decline in hypertensive patients.
2. METHODS
2.1. Study population
The study protocol was designed in accordance with the Declaration of Helsinki and approved by the ethics committee of Osaka University of Pharmaceutical Sciences (committee approval number: 0035). This was part of a longitudinal observational study, as described previously. 14 Briefly, adult hypertensive patients were recruited from Kenwakai Hospital (Nagano, Japan) between 2017 and 2019. Eligible participants had BP of at least 140 mmHg systolic or 90 mmHg diastolic or used antihypertensive drugs. Major exclusion criteria included diabetes mellitus (DM), history of congestive heart failure, arterial fibrillation, angina, cardiovascular events in the past 6 months, polycystic kidney disease, IgA nephropathy, dialysis, or eGFR below 15 (ml/min/1.73 m2). We also excluded patients who had undergone kidney transplant. In total, 147 patients participated after providing written informed consent.
2.2. Data collection
Demographic data and laboratory values were collected from the clinical records. Urinary and serum Cr values were measured in a central laboratory by an enzymatic method. The concentration of vanin‐1 in the urine was measured using commercially available ELISA Kits (Cloud‐Clone Corp.), according to the manufacturer's instructions. These values were normalized to the urinary Cr value. The equation calculates eGFR from serum Cr, age, and sex using the following formula: (eGFR [ml/min/1.73 m2] = 194 × age−0.287 × serum Cr−1.094 × [0.739 for women]). 15
Nurses performed a survey to collect information on smoking and alcohol habits, antihypertensive medication, and histories of DM, congestive heart failure, arterial fibrillation, angina, and cardiovascular disease. DM was defined as a self‐reported diagnosis, a fasting glucose level of at least 126 mg/dl, or the use of antidiabetic agents. The body mass index (BMI) was the weight in kilograms divided by the square of the height in meters. The primary end point was set as an eGFR decrease ≥20%. 16 , 17
2.3. Statistical analysis
Data are presented as the mean ± SD or median (interquartile range) for continuous variables and n (%) for categorical variables. The study cohort was stratified into two groups by the median value of urinary vanin‐1. The differences in parametric and nonparametric values between two groups were analyzed with the unpaired t‐test and Mann‐Whitney U test, respectively. The differences in nonparametric values among four groups were analyzed with the Kruskal‐Wallis test. Categorical variables were compared using chi‐squared tests.
Comparison of the status of kidney function decline was conducted by the Kaplan‐Meier method with log‐rank test to determine significance levels. Univariate Cox regression analysis was used to estimate associations between baseline factors including urinary vanin‐1 and the primary end point of an eGFR decrease ≥20%. Multivariable Cox regression analysis adjusted for potential confounding factors was used. The receiver operating characteristic (ROC) curve was used to estimate the predictive power of urinary vanin‐1 and traditional kidney biomarkers. p < .05 was considered significant. All statistical analyses were performed using SPSS for Windows software (ver. 19.0; SPSS Inc.).
3. RESULTS
3.1. Baseline characteristics
The clinical and demographic information of the participants is shown in Table 1. The study cohort was stratified by the median value of urinary vanin‐1 (0.33 ng/mg Cr) into low‐ and high–vanin‐1 groups. The high‐ and low–vanin‐1 groups showed almost the same distribution of age and sex. The high–vanin‐1 group had significantly higher levels of plasma glucose, HbA1c, uric acid, BUN, and Scr than the low–vanin‐1 group. Urinary vanin‐1 levels at baseline of patients with CKD stage 4 (eGFR: less than 30 ml/min/1.73 m2) were higher than those in patients with CKD stages 2–3 (eGFR: 30–59 and 60–89 ml/min/1.73 m2) (Figure 1).
TABLE 1.
Baseline characteristics of patients
| Variable | All (n = 147) | p ‐Value | |
|---|---|---|---|
| Vanin‐1 < 0.33 ng/mg Cr (n = 73) | Vanin‐1 ≥ 0.33 ng/mg Cr (n = 74) | ||
| Age, years | 73.3 ± 6 | 72.4 ± 10.3 | .95 |
| Women, n (%) | 42 | 37 | .458 |
| Current smoker, n (%) | 15 | 21 | .409 |
| Current drinker, n (%) | 58 | 41 | .083 |
| BMI, kg/m2 | 24.1 ± 3.2 | 24.3 ± 3.9 | .94 |
| SBP, mmHg | 131.3 ± 11.8 | 135.3 ± 16.4 | .16 |
| DBP, mmHg | 73.7 ± 9.3 | 74.9 ± 12.7 | .56 |
| Plasma glucose, mg/dl | 125.7 ± 28.7 | 138 ± 37.4 | .017 |
| Hemoglobin, g/dl | 13.6 ± 1.3 | 12.9 ± 1.7 | .007 |
| HbA1c, % | 5.9 ± 0.3 | 6.2 ± 0.8 | .005 |
| LDL cholesterol, mg/dl | 104.2 ± 22.8 | 102.9 ± 24.6 | .801 |
| HDL cholesterol, mg/dl | 62.1 ± 17 | 59.1 ± 15.2 | .11 |
| LDL/HDL | 1.78 ± 0.58 | 1.88 ± 0.71 | .198 |
| Triglycerides, mg/dl | 129 (91‐197) | 115 (95.8‐181.8) | .49 |
| BNP, pg/ml | 27.9 (16.3‐46.7) | 35.9 (16.3‐60.9) | .29 |
| AST, IU/L | 24.9 ± 11.7 | 24.5 ± 8.9 | .70 |
| ALT, IU/L | 22.1 ± 17.6 | 21.5 ± 10.5 | .86 |
| Uric acid, mg/dl | 5.8 ± 1.4 | 6.3 ± 1.4 | .031 |
| BUN, mg/dl | 17.6 ± 5.3 | 22.5 ± 10.8 | <.001 |
| SCr, mg/dl | 0.87 ± 0.3 | 1.22 ± 0.58 | <.001 |
| eGFR, ml/min/1.73 m2 | 64.1 (54.6‐72.4) | 49.2 (28.3‐68.9) | .001 |
| UPCR, g/g Cr | 0.06 (0.04‐0.1) | 0.11 (0.05‐0.21) | .088 |
| UACR, mg/g Cr | 15.8 (7.5‐26.7) | 53 (14.9‐393.8) | <.001 |
| Urinary vanin‐1, ng/mg Cr | 0 (0‐0) | 2.5 (1.2‐5.0) | <.001 |
All results are presented as mean ± SD, median (interquartile range), or n (%).
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; BNP, B‐type natriuretic peptide; BUN, blood urea nitrogen; Cr, creatinine; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; HDL, high‐density lipoprotein; LDL, low‐density lipoprotein; SBP, systolic blood pressure; UACR, urinary albumin‐to‐creatinine ratio; UPCR, urinary protein‐to‐creatinine ratio.
FIGURE 1.
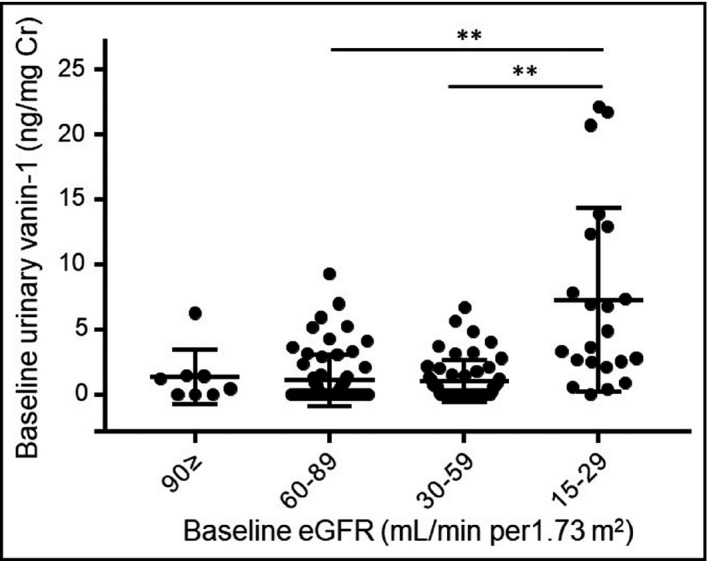
Distribution of urinary vanin‐1 by eGFR in hypertensive patients. eGFR, estimated glomerular filtration rate
3.2. Urinary vanin‐1 and decline in kidney function
The median (interquartile range) follow‐up time was 12 (11.25–14) months. Overall, 14 of 147 (9.5%) patients developed ≥20% decline in eGFR. Comparing patients with ≥20% decline in eGFR and those without it, there were significant differences in eGFR, SBP, UACR, and urinary vanin‐1 at the baseline (Table 2). Urinary vanin‐1 levels, eGFR, SBP, and UACR in patients whose eGFR declined were less favorable than those in patients with no eGFR decline.
TABLE 2.
Comparison of baseline characteristics by the development of eGFR decline during follow‐up
| Variables | Nondecline in eGFR (n = 129) | Decline in eGFR (n = 14) | p‐Value |
|---|---|---|---|
| Age, years | 75 (69.5‐78) | 78 (66.5‐82.5) | .078 |
| Women, n (%) | 50 (38.8) | 5 (35.7) | .82 |
| Follow‐up, month | 13 (11.5‐14) | 12 (11.75‐12.25) | .14 |
| eGFR, ml/min/1.73 m2 | 62.3 (45.4‐72.1) | 35.65 (24.2‐56.2) | <.01 |
| SBP, mmHg | 131 (124‐140) | 150.5 (137‐158) | <.01 |
| UPCR, g/g Cr | 0.06 (0.04‐0.13) | 0.13 (0.035‐1.49) | .52 |
| UACR, mg/g Cr | 20.95 (9.3‐68.6) | 263.3 (13.3‐1789.9) | .013 |
| Urinary vanin‐1, ng/mg Cr | 0 (0‐1.45) | 6.34 (2.44‐13.2) | <.01 |
All results are presented as median (interquartile range) or n (%).
Abbreviations: Cr, creatinine; eGFR, estimated glomerular filtration rate; SBP, systolic blood pressure; UACR, urinary albumin‐to‐creatinine ratio; UPCR, urinary protein‐to‐creatinine ratio.
Univariate Cox regression analysis revealed that antihypertensive medication, BP, eGFR, UACR, and urinary vanin‐1 were risk factors for ≥20% decline in eGFR (Table 3). After adjustment for these potential confounders, urinary vanin‐1 remained a significant risk of ≥20% decline in eGFR (Table 3).
TABLE 3.
Cox regression analysis for the association of urinary vanin‐1 with kidney function decline
| Variables | Univariable | Multivariable | ||
|---|---|---|---|---|
| HR (95% CI) | p ‐Value | HR (95% CI) | p ‐Value | |
| Age, ≥75 years | 2.82 (0.88‐2.82) | 0.08 | 2.23 (0.58‐8.57) | 0.25 |
| Sex | 1.18 (0.39‐3.53) | 0.76 | 0.999 (0.24‐4.15) | 0.998 |
| Smoking | 0.81 (0.18‐3.6) | 0.78 | 1.35 (0.24‐7.66) | 0.73 |
| Drinking | 0.86 (0.30‐2.49) | 0.78 | 1.80 (0.49‐6.62) | 0.37 |
| BMI, ≥25 kg/m2 | 1.44 (0.51‐4.12) | 0.49 | 0.92 (0.26‐3.23) | 0.90 |
| Antihypertensive medication | 0.12 (0.015‐0.97) | 0.046 | 0.03 (0.001‐0.58) | 0.02 |
| BP, ≥140/≥90 mmHg | 4.17 (1.40‐12.5) | 0.01 | 3.89 (1.22‐12.5) | 0.02 |
| eGFR, < 60 ml/min/1.73 m2 | 4.33 (1.19‐15.8) | 0.027 | 3.38 (0.68‐16.7) | 0.14 |
| UACR, ≥30 mg/g Cr | 3.45 (1.07‐11.1) | 0.038 | 2.96 (0.57‐15.4) | 0.19 |
| Urinary vanin‐1, ≥0.33 ng/mg Cr | 16.8 (2.14‐132.9) | <0.01 | 9.87 (1.11‐87.5) | 0.04 |
Abbreviations: 95% CI, 95% confidence interval; BMI, body mass index;BP, blood pressure; eGFR, estimated glomerular filtration rate; HR, hazard ratio; UACR, urinary albumin‐to‐creatinine ratio.
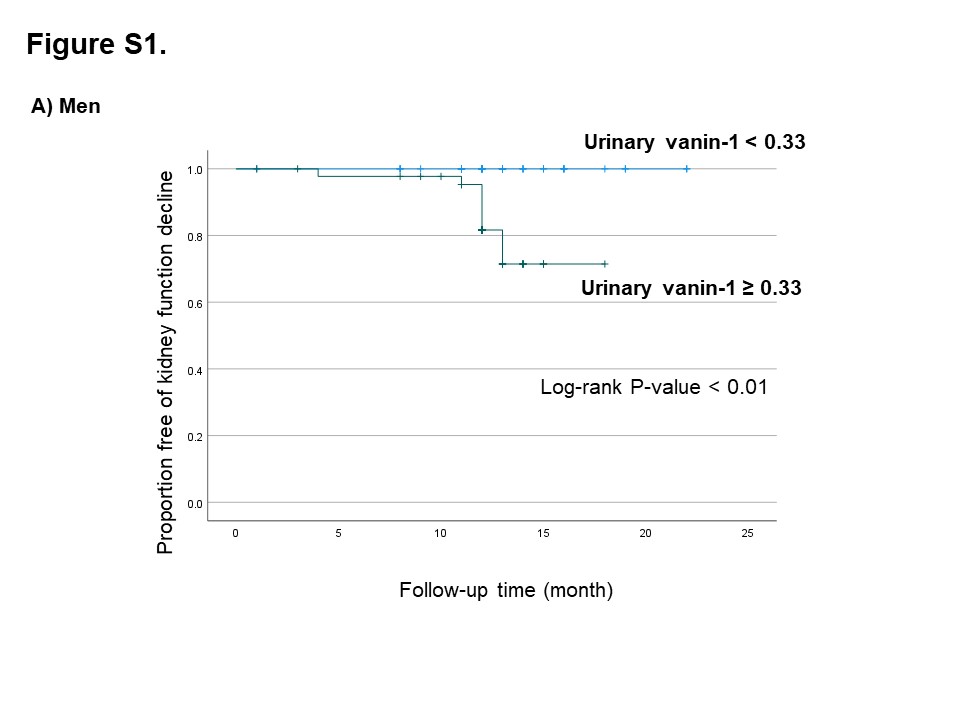
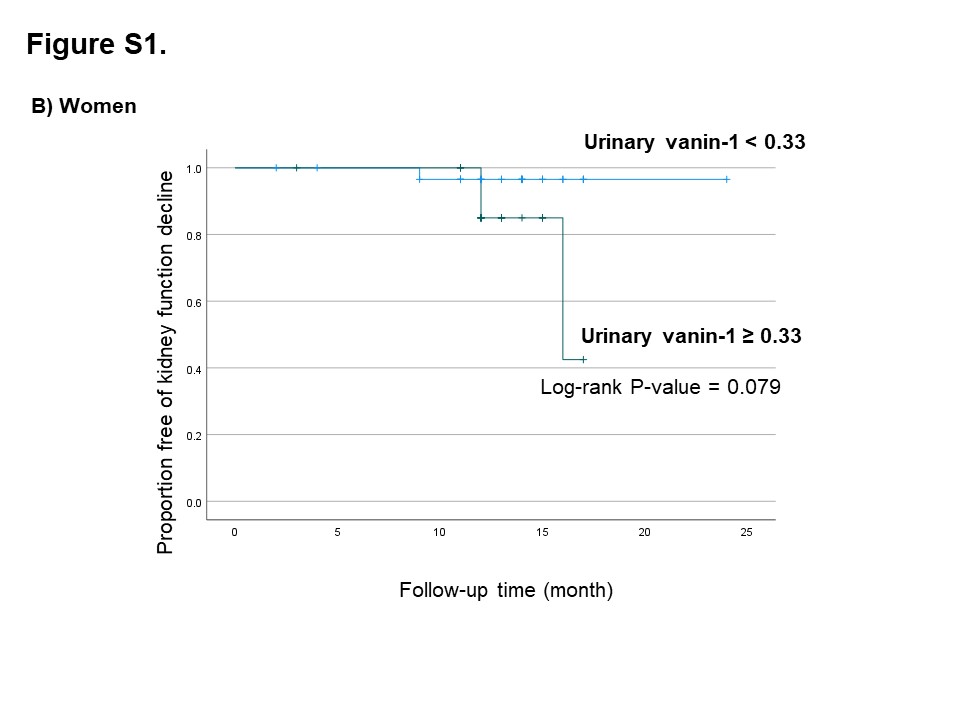
On the basis of the ROC analysis (Figure 2), areas under the curves (AUCs) were 0.823 (p = .008), 057 (p = .57), 0.579 (p = .52), and 0.689 (p = .12) for urinary vanin‐1, UACR, UPCR, and BUN, respectively. The AUC for urinary vanin‐1 showed the highest value, whereas traditional biomarkers were not significant. Next, the Kaplan‐Meier analysis revealed that the high–vanin‐1 group showed a significantly higher risk of developing a decline in eGFR during the follow‐up period (Figure 3). Analysis was also performed evaluating males and females separately, and the high–vanin‐1 group showed a significantly higher risk of developing ≥20% decline in eGFR during the follow‐period in men (log‐rank test, p = .002), but not in women (log‐rank test, p = .079) (Figure S1).
FIGURE 2.
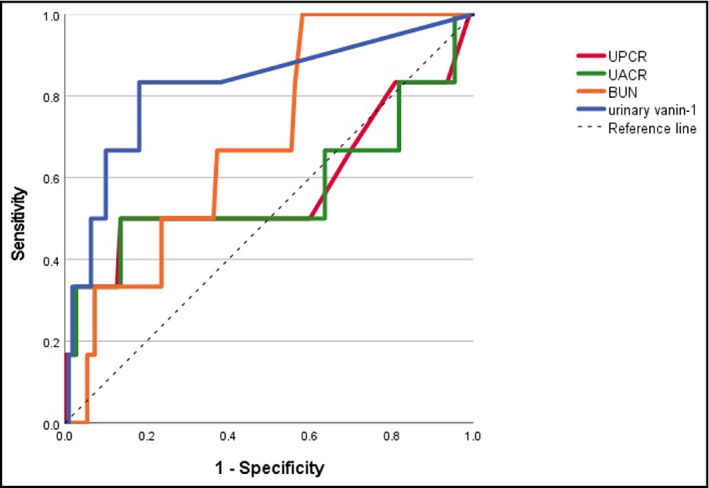
Receiver operating characteristic (ROC) curves for prediction of ≥20% decline in eGFR. The areas under ROC curves (AUCs) were 0.823 (p = .008), 057 (p = .57), 0.579 (p = .52), and 0.689 (p = .12) for urinary vanin‐1, UACR, UPCR, and BUN, respectively. BUN, blood urea nitrogen; UACR, urinary albumin‐to‐creatinine ratio; UPCR, urinary protein‐to‐creatinine ratio
FIGURE 3.
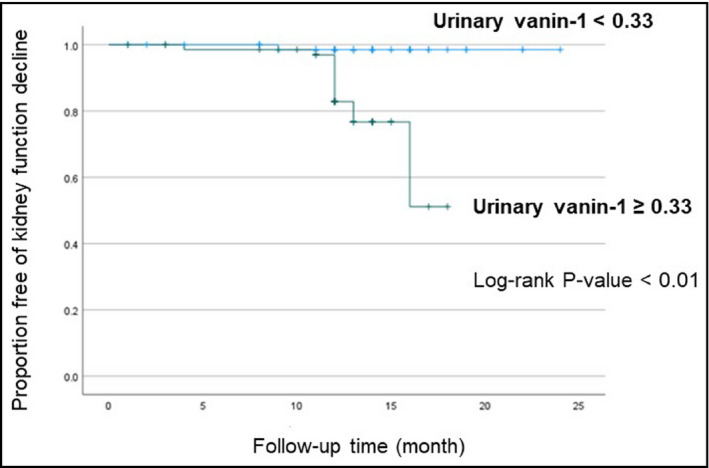
Kaplan‐Meier analysis of incidence of ≥20% decline in eGFR according to urinary vanin‐1 levels
4. DISCUSSION
The present study showed that urinary vanin‐1 may be an independent risk predictor of the reduction in eGFR in adult hypertensive patients. CKD is largely a disease deteriorating over time, and the kidney function of patients physiologically declines without subjective symptoms. Therefore, early detection of the reduction in eGFR using urinary vanin‐1 provides an opportunity for early therapeutic intervention. These findings will help us better understand the pathogenesis of kidney injury and intervene in preventing kidney disease progression and its complications with an improved focus.
CKD progression is characterized as glomerular and tubular injury. Especially, the severity of tubular interstitial damage is closely correlated with the degree of deterioration of renal failure, even more than glomerular lesions. 18 In addition, tubular injury leads to progressive tubulointerstitial fibrosis, which is a common pathway to ESKD. 19 Furthermore, interstitial fibrosis can only be assessed directly by kidney biopsy. Then, the measurement of urinary vanin‐1 could provide a noninvasive method to identify patients at high risk of kidney function decline and predict CKD progression. In our study, we observed that hypertensive patients with eGFR < 60 (ml/min/1.73 m2), higher BP, UACR ≥30 (mg/g Cr), and higher urinary vanin‐1 levels were at significant risk of kidney function decline during the follow‐up period. In the Cox regression analysis, urinary vanin‐1 was shown to be a significant independent risk factor for kidney function decline, even after adjustment for confounding factors. Therefore, our results provide important prognostic information on kidney disease progression independent of traditional risk factors in hypertensive patients.
Among the risk factors for early kidney damage, BP is one of the most important. 20 Indeed, a recent study showed that a higher BP in childhood was correlated with a higher risk of subclinical kidney damage in adults over 30 years of follow‐up. 21 Moreover, short‐term BP variability was independently associated with early kidney abnormalities. 22 Our results revealed that the use of antihypertensive medication decreased the risk of kidney function decline and hypertension elevated the risk, which is in agreement with these previous reports. Even after adjustment for the use of antihypertensive medication and hypertension, our study still revealed urinary vanin‐1 as a significant predictor of a decreased kidney function.
Although the underlying mechanism explaining the value of vanin‐1 to predict the progression of kidney function decline is not clear, it has been suggested that vanin‐1 is involved in oxidative stress, 23 , 24 which contributes to inflammation and fibrosis, subsequently leading to kidney damage. Oxidative stress is initiated by the over‐production of ROS, which is traditionally considered to be an imbalance of pro‐oxidants and antioxidant homeostasis. 25 , 26 In addition, the localization of vanin‐1 may provide important clues concerning the mechanism that underlies the predictive value. Our previous animal studies showed that vanin‐1 was localized in proximal tubular epithelial cells, 9 which are affected at early stages of the disease. The proximal tubules of the kidney are densely packed with mitochondria, thereby providing energy via oxidative phosphorylation to drive the active transport of solutes in proximal tubular reabsorption. 27
This study had some limitations. First, the study population was small. Especially, the number of women was smaller than that of men, with the Kaplan‐Meier analysis showing a difference between men and women in the predictive value of urinary vanin‐1. Second, this study was limited to nondialysis patients. Third, normal individuals were not recruited in this study, so we were unable to determine urinary vanin‐1 in these patients; however, our previous study revealed that urinary vanin‐1 was not detected in nondiabetic and diabetic patients without albuminuria. 28 Finally, this was an observational study and so cannot be used to infer causality; thus, interventional studies are warranted.
In conclusion, our data provide new evidence that urinary vanin‐1 is an independent risk factor for a poor kidney prognosis in hypertensive patients. Its addition to classic markers, such as baseline eGFR and BP, could improve the prediction of a decline in eGFR in these patients. Further studies are needed with larger populations to confirm our findings.
CONFLICT OF INTEREST
None.
AUTHOR CONTRIBUTIONS
KH supervised the conduct of the study and data analysis and had the primary responsibility of writing the manuscript. HM conducted data interpretation and reviewed/edited the manuscript. EK supervised the conduct of the study, collected the data, and conducted data analysis and data interpretation.
Supporting information
Fig S1‐1
{kind=link}
Fig S1‐2
{kind=link}
Supplementary Material
ACKNOWLEDGEMENTS
We thank Clinical Research Support Team in Kenwakai Hospital for their advice.
Hosohata K, Matsuoka H, Kumagai E. Association of urinary vanin‐1 with kidney function decline in hypertensive patients. J Clin Hypertens. 2021;23:1316–1321. 10.1111/jch.14295
Funding information
This work was supported by JSPS KAKENHI (Grant No. JP18K06768).
References
- 1. Wan EYF, Yu EYT, Chin WY, Fong DYT, Choi EPH, Lam CLK. Association of blood pressure and risk of cardiovascular and chronic kidney disease in Hong Kong hypertensive patients. Hypertension. 2019;74:331‐340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Yamagata K, Ishida K, Sairenchi T, et al. Risk factors for chronic kidney disease in a community‐based population: A 10‐year follow‐up study. Kidney Int. 2007;71:159‐166. [DOI] [PubMed] [Google Scholar]
- 3. Levey AS, de Jong PE, Coresh J, et al. The definition, classification, and prognosis of chronic kidney disease: A kdigo controversies conference report. Kidney Int. 2011;80:17‐28. [DOI] [PubMed] [Google Scholar]
- 4. Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH. Longitudinal follow‐up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med. 2004;164:659‐663. [DOI] [PubMed] [Google Scholar]
- 5. Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296‐1305. [DOI] [PubMed] [Google Scholar]
- 6. Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298:2038‐2047. [DOI] [PubMed] [Google Scholar]
- 7. McMahon GM, Waikar SS. Biomarkers in nephrology: Core curriculum 2013. Am J Kidney Dis. 2013;62:165‐178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Li L, Astor BC, Lewis J, et al. Longitudinal progression trajectory of GFR among patients with CKD. Am J Kidney Dis. 2012;59:504‐512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Hosohata K, Ando H, Fujiwara Y, Fujimura A. Vanin‐1: A potential biomarker for nephrotoxicant‐induced renal injury. Toxicology. 2011;290:82‐88. [DOI] [PubMed] [Google Scholar]
- 10. Aurrand‐Lions M, Galland F, Bazin H, Zakharyev VM, Imhof BA, Naquet P. Vanin‐1, a novel GPI‐linked perivascular molecule involved in thymus homing. Immunity. 1996;5:391‐405. [DOI] [PubMed] [Google Scholar]
- 11. Pitari G, Malergue F, Martin F, et al. Pantetheinase activity of membrane‐bound vanin‐1: Lack of free cysteamine in tissues of vanin‐1 deficient mice. FEBS Lett. 2000;483:149‐154. [DOI] [PubMed] [Google Scholar]
- 12. Hosohata K, Yoshioka D, Tanaka A, Ando H, Fujimura A. Early urinary biomarkers for renal tubular damage in spontaneously hypertensive rats on a high salt intake. Hypertens Res. 2016;39:19‐26. [DOI] [PubMed] [Google Scholar]
- 13. Hosohata K, Jin D, Takai S, Iwanaga K. Involvement of vanin‐1 in ameliorating effect of oxidative renal tubular injury in dahl salt‐sensitive rats. Int J Mol Sci. 2019;20:4481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Hosohata K, Matsuoka H, Iwanaga K, Kumagai E. Urinary vanin‐1 associated with chronic kidney disease in hypertensive patients: A pilot study. J Clin Hypertens. 2020;22:1458‐1465. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Matsuo S, Imai E, Horio M, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982‐992. [DOI] [PubMed] [Google Scholar]
- 16. Sugimoto M, Banno H, Sato T, et al. Time‐to‐event analysis of the impact of endovascular aortic aneurysm repair on chronic renal decline. Ann Vasc Surg. 2021. (in press). 10.1016/j.avsg.2021.02.031 [DOI] [PubMed] [Google Scholar]
- 17. Xiao W, Wen Y, Ye P, et al. Noninvasive central pulse pressure is an independent determinant of renal function. J Clin Hypertens. 2020;22:234‐242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Zoja C, Abbate M, Remuzzi G. Progression of renal injury toward interstitial inflammation and glomerular sclerosis is dependent on abnormal protein filtration. Nephrol Dial Transplant. 2015;30:706‐712. [DOI] [PubMed] [Google Scholar]
- 19. Grgic I, Campanholle G, Bijol V, et al. Targeted proximal tubule injury triggers interstitial fibrosis and glomerulosclerosis. Kidney Int. 2012;82:172‐183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Teo BW, Chan GC, Leo CCH, et al. Hypertension and chronic kidney disease in Asian populations. J Clin Hypertens. 2021;23(3):475‐480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Zheng W, Mu J, Chu C, et al. Association of blood pressure trajectories in early life with subclinical renal damage in middle age. J Am Soc Nephrol. 2018;29:2835‐2846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Mule G, Calcaterra I, Costanzo M, et al. Relationship between short‐term blood pressure variability and subclinical renal damage in essential hypertensive patients. J Clin Hypertens. 2015;17:473‐480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Hosohata K. Role of oxidative stress in drug‐induced kidney injury. Int J Mol Sci. 2016;17:1826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Berruyer C, Martin FM, Castellano R, et al. Vanin‐1‐/‐ mice exhibit a glutathione‐mediated tissue resistance to oxidative stress. Mol Cell Biol. 2004;24:7214‐7224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Morgan WA, Kaler B, Bach PH. The role of reactive oxygen species in adriamycin and menadione‐induced glomerular toxicity. Toxicol Lett. 1998;94:209‐215. [DOI] [PubMed] [Google Scholar]
- 26. Liu X, Cao W, Qi J, et al. Leonurine ameliorates adriamycin‐induced podocyte injury via suppression of oxidative stress. Free Radic Res. 2018;52:952‐960. [DOI] [PubMed] [Google Scholar]
- 27. Soltoff SP. ATP and the regulation of renal cell function. Annu Rev Physiol. 1986;48:9‐31. [DOI] [PubMed] [Google Scholar]
- 28. Hosohata K, Ando H, Takeshita Y, et al. Urinary kim‐1 is a sensitive biomarker for the early stage of diabetic nephropathy in otsuka long‐evans tokushima fatty rats. Diab Vasc Dis Res. 2014;11:243‐250. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fig S1‐1
Fig S1‐2
Supplementary Material