

Abstract
Hepatitis C virus represents one of the most important public health problems nowadays. Several epidemiological studies have shown a continuous increasing rate of prevalence and incidence with severe consequences in terms of mortality. During the last decades, the treatment of the liver infection has evolved, and now there are available new therapies with better side-effect’ profiles and bigger efficiency. The needs for more therapeutically efficacy also stand behind the numerous comorbidities associated to the liver disease, and also for assuring better quality of life for patients and their families.
Keywords: HCV infection, DAAs therapies, health-related quality of life, comorbidities, interferon
Introduction
Hepatitis C virus (HCV) is a member of the family Flaviviridae, with some differences to the other members of the family, especially in its genome organization: HCV is a single stranded, positive sense, RNA virus, its genome having a length of approximately 9600 nucleotides [1,2].
HCV infection represents one of the most important global health issues, having a major impact at the levels of the affected individuals, their families, communities and the whole societies. Moreover, the untreated HCV infection can lead to cirrhosis, hepatocellular carcinoma (HCC) and liver-related death.
The burden of HCV infection has its primary source in the fact that is the major cause of chronic liver disease worldwide, which means just for the C hepatitis diagnosis over 70 million people, according to the estimates of the World Health Organization (WHO) [3].
In epidemiological terms it could be translated in over 1.75 million new HCV infections each year, with a global incidence rate of 23.7/100,000. The WHO studies have shown that the most prominent geographical areas in accordance to the higher rates of HCV infection incidence are the WHO’s Eastern Mediterranean Region (62.5/100,000), respectively the WHO’s European Region (61.8/100,000). Instead, the estimated prevalence in the general population ranging from 0.5 to 6.5%, with the lowest values in Western Europe and the peak reached in Pakistan [3,4].
A very serious issues is the fact that over 75% of the individuals with HCV infection are not aware of their infection, due to the lack of the specific symptoms in the early stages of the disease, and the rate of the chronicity is the 70% to 85% [5,6,7].
Direct or indirect exposure to contaminated blood represents the main route of the virus transmission, in different contexts such as: intravenous and percutaneous drug and needle use, use of contaminated surgical materials, accidents in health care facilities including dentistry and hemodialysis settings, organ transplants, vertical transmission from mother to child and many others [8,9].
Other important problems are the association between HCV infection and HIV, where there are evidences that about 2.3 million out of the estimated 36.7 million individuals living with HIV were positive for antibodies to HCV or anti-HCV positive, respectively the Hepatitis B virus (HBV) and HCV coinfection, with an estimated global prevalence of 1-15% [10].
According to the WHO estimations, in 2016 almost 400,000 people died from cirrhosis and hepatocellular carcinoma that had their roots in HCV infection, out of which is considered that 31% of deaths are attributable to a positive history of injection drug use [3,11].
Material and Methods
Objective
Our study aims was to assess the influence of treatment with DAA-based therapies on the quality of life and on the level of stress perceived by the patients.
Material and Method
We conduct a study on a sample consisting of 73 subjects diagnosed with HCV infection, F3-F4 METAVIR score, and detectable HCVRNA viral load, treated with Ombitasvir/Paritaprevir/Ritonavir/Dasabuvir for 12 weeks. All patients were clinically, biologically and psychologically evaluated at the start of the treatment (SOT), at weeks 4, 8, 12 (end of treatment-EOT), respectively 12 weeks after therapy (sustained viral response-SVR).
At all three moments were collected and registered the clinical data, biological records and the results of psychological assessment.
Psychological Evaluation
The stress level was evaluated applying the Perceived Stress Scale (PSS) [12], a scale that determines in which way a living situation is appraised as stressful by an individual. A high score of PSS means a high level of perceived stress.
We also used Hospital Anxiety and Depression Scale (HADS), a self-reported screening tool that includes 14 multiple-choice questions, in order to identify and to measure the severity of the anxiety and depression symptoms [13].
HADS scores differentiate the following categories: 0-7=considered non-case, 8-10=considered possible case (borderline), and 11-21=considered probable case, which have been reclassified and relabeled as follows: 0-7=normal, 8-10=mild, 11-15=moderate, and ≥16=severe [14].
In our study we used the original recommendation cutoff scores, which proved a specificity of 0.78 and a sensitivity of 0.9, and for depression a specificity of 0.79 and a sensitivity of 0.83 [15].
The WHOQOL-Bref, scale that we used for assesses the subjects’ quality of life, was developed by the World Health Organization (WHO) and published in 1995.
The questions stem from multiple statements about quality of life, health and well-being from people with and without disease, and health professionals.
The WHOQOL-Bref reference to four domains: physical health, psychological, social relationship and environment [16].
Statistical analysis
Statistical analysis was performed using Microsoft Excel (Microsoft Corp., Redmond, WA, USA), and IBM SPSS Statistics 20.0 (IBM Corporation, Armonk, NY, USA) for processing the data. Friedman test was used for consecutively data recorded.
Ethical issues
The study was approved by the Ethics Committee of Craiova University of Medicine and Pharmacy of Craiova (Ethical Approval of Research Project no. 66/23 February 2017) and was in line with the Helsinki Declaration.
All patients were enrolled voluntarily by giving written informed consent and their data were kept secure.
Results
The study sample included 73 subjects (75.3% females), 50.7% (urban area), mean age 68.31±6.63 years, age ranging from 33 to 79 years with adverse events present in 34.0% of patients (asthenia, pruritus, insomnia, 53.3% of them living in urban environment (Figure 1).
Figure 1.
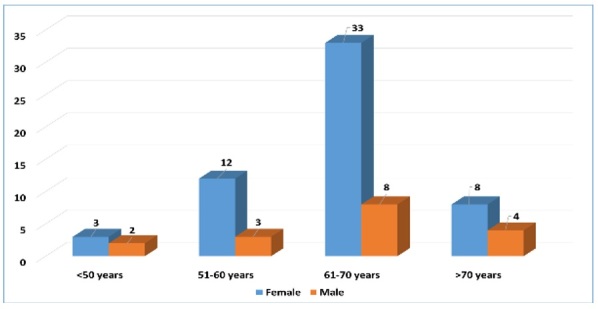
Distribution of study sample according to gender and age groups
At BSL, 53 patients (72.6%) were classified as affected by well compensated cirrhosis (38 Child-Pugh class A and five Child-Pugh class B) on clinical and radiological findings.
The degree of the fibrosis according to METAVIR score was F2 in 3 patients (4.1%), F3 in 24 (32.87%), respectively F4 in 45 (61.64%)
We identified 50 patients (68.49%) as therapy-naïve, while the remaining 23 (31.51%) had been treated before with combination of pegylated interferon and ribavirin.
Fifteen subjects (20.54%) were identified with diabetes mellitus and 26 (35.61%) fulfilled the criteria for obesity class I and II (BMI>30kg/m2).
The chronical kidney disease (CKD) was present on G2 stage in 38 (52.05%) of the subjects, respectively G3 stage on 4 patients (5.47%). None of the patients discontinued treatment.
There were recorded: a high level of perceived stress in 20.5% (SOT), respectively moderate stress 78.1% (SOT), but during the treatment it was significantly improved (χ2(2)=18.33, p<0.0001) (Figure 2).
Figure 2.
Distribution of study sample according to gender and level of perceived stress on the three moments of assessment (χ2(2)=18.33, p<0.0001).
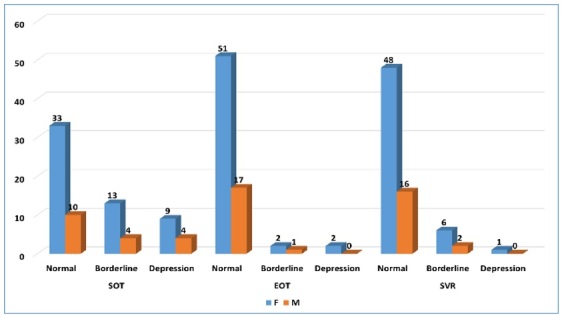
Depression as assessed through HADS was present in 17.8% (SOT), and only in 1.4% at SVR (χ2(2)=24.86, p<0.0001) (Figure 3), similar situation being observed for anxiety: 45.2% (SOT), 9.6%(EOT), 5.5% (SVR) (χ2(2)=33.95, p<0.0001) (Figure 4).
Figure 3.
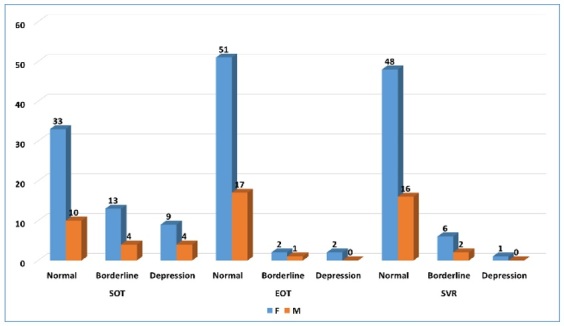
Distribution of study sample according to gender and presence of depression on the three moments of assessment
Figure 4.
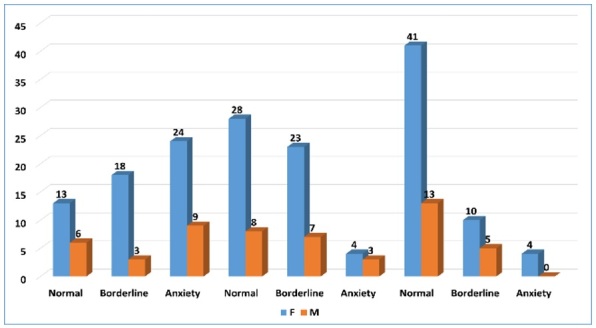
Distribution of study sample according to gender and presence of anxiety on the three moments of assessment
Regarding patients’ quality-of-life under DAA therapy, it was significantly improved in all the domains: physical health (χ2(2)=35.289, p<0.0001), psychological status (χ2(2)=39.42, p<0.0001), social relationships (χ2(2)=54.10, p<0.0001), and environmental quality of perception (χ2(2)=41.52, p<0.0001) (Table 1).
Table 1 .
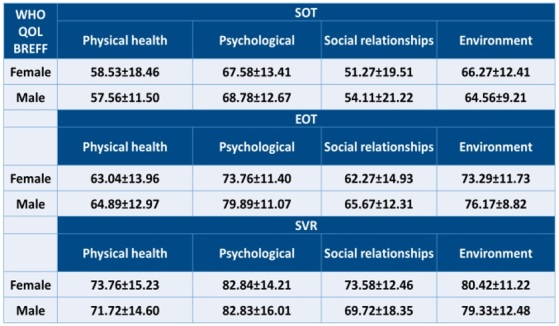
Distribution of study sample according to gender and the four domains of quality of life expressed through average score of WHOQOL-BREF
Discussions
HCV infection therapeutical approaches
One of the most important moments in the history of the HCV infection treatment was the introduction of alpha interferon (IFN-α) over three decades ago [3].
Even if it was considered a milestone in the therapeutical process, the outcomes of this therapy were not so satisfactory, the rate of sustained virological response (SVR) being only around 30-40% [17,18], and mostly in patients infected with genotype 1 of the virus [19,20].
Moreover, this promising therapy presented a significant adverse effect, the Major Depressive Disorder during IFN-α treatment (IFN-MDD), which could occur within a few months after the start of therapy and affected 15% to 40% of the patients.
After this psychiatric side-effect was observed, there were several studies that have used antidepressant medication in order to try to prevent the onset of IFN-MDD. The outcomes of these researches suggest that this kind of prophylactic measures may be specifically useful in individuals that had a positive personal history for depression or they have pre-existing subthreshold depressive symptoms at the moment when the IFN-α therapy and adjunctive antidepressant medication.
Some other potential markers for vulnerability to IFN-MDD identified in the nondepressed patients, before starting the IFN-α treatment, were: poor sleep quality, premorbid elevations in inflammatory cytokines, genetic polymorphisms in the serotonin system, personality, and social support [21,22].
The evolution in the therapeutically methods of HCV infection subsequently evolved from IFN-α to the combination of and pegylated interferon (PEG-IFN) and ribavirin (RBV) [28].
Unfortunately, despite of a better efficacy than interferon monotherapy, the new combination has also proven a broad spectrum of neuropsychiatric side effects such as fatigue, mood disturbances, anxiety, irritability, or agitation [24].
During the last decade, the treatment methods of HCV infection have known a revolutionary moment, when the new direct-acting antivirals (DAAs) were approved and introduced for human use. The novel therapy was successful in terms of reduced virologic response for all genotypes and, also very important, they have shown a reduced profile of side-effects, especially in the field of mental health, in comparison to previous ways of treatment.
DAAs and HCV with comorbidities
The new therapeutically approach seems to be efficient and safe on different categories of patients, and, more than that, there are evidences that showed its beneficial effect on the general health and quality of life too.
Elderly patients
For example, DAA treatment on elderly chronic HCV patients, aging over 65 years, was proved to be highly effective with a success rate that was not different from younger adults [25].
This example is a suggestive one for the advantages of DAAs, since the use of previous antiviral therapies was limited due to the multiple risks such as drug‐drug interaction and side effects.
Chronic kidney disease
Also, the association of HCV infection and chronic kidney disease (CKD), a very common one, had led to limitations in treatment options, the clinicians being concerned about low profile of efficacy and safety of therapies based on interferon. This situation seems to find its solution on DAAs, that proved to be efficient on patients with CKD as comorbidity (SVR12 rates>90% in the context of stage 4-5 CKD) [26].
As above mentioned, the positive effects of DAAs are not limited to the patients with only HCV infection diagnosis, but they have proven their efficacy on difficult-to-treat patients like those with multiple comorbidities, both physical and mental. The new therapy is used now on cases that are associating HCV infection with diabetes, cardiovascular diseases, psychological disturbances and disorders, being also efficient in the control of these conditions too [27,28,29,30].
Diabetes mellitus
The risks for the comorbid association between HCV infection and diabetes mellitus type 2 (T2DM) and/or cardiovascular diseases was lower in the patients treated with DAAs, which achieved the SVR in a shorter period compared to the previous HCV treatments. DAAs has effect on better fasting glucose and HbA1C controls in patients that already associated T2DM or were in prediabetes stages, and also led to the reduction of the antidiabetic treatment [31].
Polypharmacy
An important medical and behavioral issue that are often met among patients with HCV infection is the polypharmacy, as long as the drug-drug interaction represents a general strong challenge and a special condition for the DAAs treatment [32,33].
The wide-known involvement of the cytochrome P450 in the metabolism of drugs and its abnormal activity (increasing or decreasing) due to the drug interaction leads to severe disturbances in the DAAs clearance [33].
The assessment of the drug-interaction effects in the case of DAAs therapies could be now much easier done since this new treatment became available to a larger number of individuals with HCV infection, but it also needs to take into account the severity of liver disease [34].
HCV and Quality of Life
HCV infection represents not only an individual burden for those affected, but also a load in terms of social-relationships disruption within family and community, and a health-issue that leads to an increasing financial expense both for individual and society. Thus, HCV infection could be considered a medical condition that seriously affects the quality of life at individual and societal levels.
Quality of life (QOL), as WHO defined it, represents a broad multidimensional concept that usually includes subjective evaluations of both positive and negative aspects of life [16].
Since the 1980s, another concept, the health-related quality of life (HRQOL), was introduced in order to circumscribe the features of overall quality of life directly related to the health-issued, both physical and mental and was defined as “an individual’s or group’s perceived physical and mental health over time” [35].
As above-mentioned, at individual level, HRQOL includes only the physical and mental health perceptions and their associated features (health risks and conditions, functional status, social support, socioeconomic status). On the community level, HRQOL refers to the community-level resources, conditions, policies, and practices directly connected to the population’s health [36].
For individuals affected by a certain disease, HRQOL is a key element in the assessment of efficacy, safety and satisfaction of any therapeutic intervention, since all these issues were proved to be very important for patients. Also, the self-assessed health status was recognized as a more powerful predictor of mortality and morbidity than other health’s evaluation tools [20,21].
In this respect, since it was introduced, the HRQOL has become an essential tool in assisting the health-care professionals for an accurate appreciation of the diseases and treatments’ impact on the patients’ well-being [37].
More than that, HRQOL is one of the basement’s components of the public health policies, its value as subjective perception of the health-care services being used by health agencies, social services agencies and other stakeholders to build and propose individual and community-justified legislation [23].
HCV infection impacted in a negative way all domains of individual’s quality of life, especially physically and mentally ones that consists in HRQOL indicators. Symptoms and syndromes associated to the HCV infection, such as depression, chronic fatigue and anxiety have led to a significant decreased quality of life of the patients compared to the general population [38,39].
One of the important processes of HCV’s influence on the central nervous system (CNS) it related to the cerebral inflammations due to cytokines and toxic substances freed by the liver that finally have as consequences mood and behavioral disturbances through the abnormal neural processes [40,41,42].
However, it was admitted that it is still difficult to state with full conviction that HCV associated neuropsychiatric symptoms are the outcomes of the virus direct neurotoxicity or of the psychological issues related to the liver disease, such as emotional stress, social stigma and the awareness of having a chronic disease with a long-term prognosis [43,44].
HRQOL was lately measured during several real-life studies on patients with HCV infection and it was reported that those treated with DAAs have shown a long-term improvement of the evaluated items [45,46].
These results have raised other questions toward the fully nature of the HCV infection, since the symptoms classically related to the liver disease (pain, anxiety, depression) were quickly improved once virus disappeared, while others (fatigue, irritability, agitation) remained or had a very slowly decreasing process [45].
One of the strengths of the novel therapies was the shortening of the treatment period and its simplified calendar, allowing the healthcare professionals to be more focused on these patients. This aspect has led to a maximum improvement in the patient’s quality of life after the obtaining of sustain viral response [47,48].
Conclusions
As we mentioned, the HCV infection represents a global health issue, with multiple domains in which its effects, medical, social, economic lead to an increasing burden, both on individual and society.
In this context, it became necessary to have a multidisciplinary approach of the disease, and to use the latest techniques and tools for screening, investigation, therapy and long-term monitoring.
The new therapeutical approaches seem to offer the prerequisites for this contemporary management process with better results for the patients.
Conflict of interests
None to declare.
References
- 1.Simmonds P. Genetic diversity and evolution of hepatitis C virus-15 years on. J Gen Virol. 2004;85(Pt11):3173–3188. doi: 10.1099/vir.0.80401-0. [DOI] [PubMed] [Google Scholar]
- 2.Hoofnagle JH. Course and outcome of hepatitis C. Hepatology. 2002;36(5 Suppl 1):S21–9. doi: 10.1053/jhep.2002.36227. [DOI] [PubMed] [Google Scholar]
- 3.WHO Global Hepatitis Report 2017. Available from: https:// www.who.int/hepatitis/publications/global-hepatitis-report2017/en/ [Accessed 10.06.2021]
- 4.Petruzziello A, Marigliano S, Loquercio G, Cozzolino A, Cacciapuoti C. Global epidemiology of hepatitis C virus infection: An up-date of the distribution and circulation of hepatitis C virus genotypes. World J Gastroenterol. 2016;22(34):7824–7840. doi: 10.3748/wjg.v22.i34.7824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Institute of Medicine (US) Committee on the Prevention and Control of Viral Hepatitis Infection . In: Colvin HM, Mitchell AE, editors. Washington (DC): National Academies Press (US); 2010. Hepatitis and Liver Cancer: A National Strategy for Prevention and Control of Hepatitis B and C. [PubMed] [Google Scholar]
- 6.Hagan H, Campbell J, Thiede H. Self-reported hepatitis C virus antibody status and risk behavior in young injectors. Public Health Rep. 2006;121(6):710–719. doi: 10.1177/003335490612100611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.US Centers for Disease Control and Prevention. Hepatits C. Published 2019. Available at: https://www.cdc.gov/hepatitis/hcv/index.htm [ Accessed 10.06.2021]
- 8.Argentini C, Genovese D, Dettori S, Rapicetta M. HCV genetic variability: from quasispecies evolution to genotype classification. Future Microbiol. 2009;4(3):359–373. doi: 10.2217/fmb.09.8. [DOI] [PubMed] [Google Scholar]
- 9.Sy T, Jamal MM. Epidemiology of hepatitis C virus (HCV) infection. Int J Med Sci. 2006;3(2):41–46. doi: 10.7150/ijms.3.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mavilia MG, Wu GY. HBV-HCV Coinfection: Viral Interactions, Management, and Viral Reactivation. J Clin Transl Hepatol. 2018;6(3):296–305. doi: 10.14218/JCTH.2018.00016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Csete J, Kamarulzaman A, Kazatchkine M, Altice F, Balicki M, Buxton J, Cepeda J, Comfort M, Goosby E, Goulão J, Hart C, Kerr T, Lajous AM, Lewis S, Martin N, Mejía D, Camacho A, Mathieson D, Obot I, Ogunrombi A, Sherman S, Stone J, Vallath N, Vickerman P, Zábranský T, Beyrer C. Public health and international drug policy. Lancet. 2016;387(10026):1427–1480. doi: 10.1016/S0140-6736(16)00619-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cohen S, Williamson G. In: The Social Psychology of Health. Spacapan S, Oskamp S, editors. Newbury Park, CA: Sage; 1988. Perceived Stress in a Probability Sample of the United States. [Google Scholar]
- 13.Snaith RP, Zigmond AS. Windsor, Berkshire (UK): Nfer‐Nelson; 1994. The Hospital Anxiety and Depression Scale manual. [Google Scholar]
- 14.Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- 15.Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002;52(2):69–77. doi: 10.1016/s0022-3999(01)00296-3. [DOI] [PubMed] [Google Scholar]
- 16.World Health Organization. WHOQOL: Measuring Quality of Life. Available from: https://www.who.int/healthinfo/survey/whoqol-qualityoflife/en/index1.html.[Accessed 10.09.2021]
- 17.Davis GL, Esteban-Mur R, Rustgi V, Hoefs J, Gordon SC, Trepo C, Shiffman ML, Zeuzem S, Craxi A, Ling MH, Albrecht J. Interferon alfa-2b alone or in combination with ribavirin for the treatment of relapse of chronic hepatitis C. International Hepatitis Interventional Therapy Group. N Engl J Med. 1998;339(21):1493–1499. doi: 10.1056/NEJM199811193392102. [DOI] [PubMed] [Google Scholar]
- 18.McHutchison JG, Gordon SC, Schiff ER, Shiffman ML, Lee WM, Rustgi VK, Goodman ZD, Ling MH, Cort S, Albrecht JK. Interferon alfa-2b alone or in combination with ribavirin as initial treatment for chronic hepatitis C. Hepatitis Interventional Therapy Group. N Engl J Med. 1998;339(21):1485–1492. doi: 10.1056/NEJM199811193392101. [DOI] [PubMed] [Google Scholar]
- 19.Poynard T, Marcellin P, Lee SS, Niederau C, Minuk GS, Ideo G, Bain V, Heathcote J, Zeuzem S, Trepo C, Albrecht J. Randomised trial of interferon alpha2b plus ribavirin for 48 weeks or for 24 weeks versus interferon alpha2b plus placebo for 48 weeks for treatment of chronic infection with hepatitis C virus. International Hepatitis Interventional Therapy Group (IHIT) Lancet. 1998;352(9138):1426–1432. doi: 10.1016/s0140-6736(98)07124-4. [DOI] [PubMed] [Google Scholar]
- 20.Ogata N, Alter HJ, Miller RH, Purcell RH. Nucleotide sequence and mutation rate of the H strain of hepatitis C virus. Proc Natl Acad Sci U S A. 1991;88(8):3392–3396. doi: 10.1073/pnas.88.8.3392. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lotrich FE. Major depression during interferon-alpha treatment: vulnerability and prevention. Dialogues Clin Neurosci. 2009;11(4):417–425. doi: 10.31887/DCNS.2009.11.4/felotrich. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Su KP, Lai HC, Peng CY, Su WP, Chang JP, Pariante CM. Interferon-alpha-induced depression: Comparisons between early- and late-onset subgroups and with patients with major depressive disorder. Brain Behav Immun. 2019;80:512–518. doi: 10.1016/j.bbi.2019.04.032. [DOI] [PubMed] [Google Scholar]
- 23.Manns MP, McHutchison JG, Gordon SC, Rustgi VK, Shiffman M, Reindollar R, Goodman ZD, Koury K, Ling M, Albrecht JK. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: a randomised trial. Lancet. 2001;358(9286):958–965. doi: 10.1016/s0140-6736(01)06102-5. [DOI] [PubMed] [Google Scholar]
- 24.Davoodi L, Masoum B, Moosazadeh M, Jafarpour H, Haghshenas MR, Mousavi T. Psychiatric side effects of pegylated interferon-α and ribavirin therapy in Iranian patients with chronic hepatitis C: A meta-analysis. Exp Ther Med. 2018;16(2):971–978. doi: 10.3892/etm.2018.6255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Villani R, Monami M, Di Cosimo F, Fioravanti G, Mannucci E, Vendemiale G, Serviddio G. Direct-acting antivirals for HCV treatment in older patients: A systematic review and meta-analysis. J Viral Hepat. 2019;26(11):1249–1256. doi: 10.1111/jvh.13169. [DOI] [PubMed] [Google Scholar]
- 26.Fabrizi F, Donato FM, Messa P. Direct-acting antivirals for hepatitis C virus in patients on maintenance dialysis. Int J Artif Organs. 2017;40(10):531–541. doi: 10.5301/ijao.5000613. [DOI] [PubMed] [Google Scholar]
- 27.Backus LI, Boothroyd DB, Phillips BR, Belperio P, Halloran J, Mole LA. A sustained virologic response reduces risk of all-cause mortality in patients with hepatitis C. Clin Gastroenterol Hepatol. 2011;9(6):509–516. doi: 10.1016/j.cgh.2011.03.004. [DOI] [PubMed] [Google Scholar]
- 28.Cacoub P, Bondin M, Hayes O, Pinsky B, Negro F. Quality of life in patients with psychiatric disorders: pooled analysis from glecaprevir/pibrentasvir registrational studies [AASLD abstract 150] Hepatology. 2018;68(suppl 1) [Google Scholar]
- 29.Hsu YC, Ho HJ, Huang YT. Association between antiviral treatment and extrahepatic outcomes in patients with hepatitis C virus infection. Gut. 2015;64(3):495–503. doi: 10.1136/gutjnl-2014-308163. [DOI] [PubMed] [Google Scholar]
- 30.Janjua NZ, Wong S, Abdia Y, Jeong D, Buller-Taylor T, Adu PA, Samji H, Wilton J, Pearce M, Butt ZA, Yu A, Binka M, Bartlett S, Alvarez M, Krajden M. Impact of direct-acting antivirals for HCV on mortality in a large population-based cohort study. J Hepatol. 2021;75(5):1049–1057 (Epub 2021 Jun 25. doi: 10.1016/j.jhep.2021.05.028. [DOI] [PubMed] [Google Scholar]
- 31.Drazilova S, Gazda J, Janicko M, Jarcuska P. Chronic Hepatitis C Association with Diabetes Mellitus and Cardiovascular Risk in the Era of DAA Therapy. Can J Gastroenterol Hepatol. 2018;2018:6150861–6150861. doi: 10.1155/2018/6150861. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kiser JJ, Burton JR, Everson GT. Drug-drug interactions during antiviral therapy for chronic hepatitis C. Nat Rev Gastroenterol Hepatol. 2013;10(10):596–606. doi: 10.1038/nrgastro.2013.106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Soriano V, Labarga P, Barreiro P, Fernandez-Montero JV, de Mendoza C, Esposito I, Benítez-Gutiérrez L, Peña JM. Drug interactions with new hepatitis C oral drugs. Expert Opin Drug Metab Toxicol. 2015;11(3):333–341. doi: 10.1517/17425255.2015.998997. [DOI] [PubMed] [Google Scholar]
- 34.Kondili LA, Gaeta GB, Ieluzzi D, Zignego AL, Monti M, Gori A, Soria A, Raimondo G, Filomia R, Di Leo A, Iannone A, Massari M, Corsini R, Gulminetti R, Gatti Comini A, Toniutto P, Dissegna D, Russo FP, Zanetto A, Rumi MG, Brancaccio G, Danieli E, Brunetto MR, Weimer LE, Quaranta MG, Vella S, Puoti M. Real-life data on potential drug-drug interactions in patients with chronic hepatitis C viral infection undergoing antiviral therapy with interferon-free DAAs in the PITER Cohort Study. PLoS One. 2017;12(2):e0172159–e0172159. doi: 10.1371/journal.pone.0172159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.The World Health Organization Quality of Life Assessment (WHOQOL): development and general psychometric properties. Soc Sci Med. 1998;46(12):1569–1585. doi: 10.1016/s0277-9536(98)00009-4. [DOI] [PubMed] [Google Scholar]
- 36.Centers for Disease Control and Prevention . Atlanta, Georgia: Centers for Disease Control and Prevention; 2000. Measuring healthy days: Population assessment of health-related quality of life. [Google Scholar]
- 37.McNeil BJ, Weichselbaum R, Pauker SG. Speech and survival: tradeoffs between quality and quantity of life in laryngeal cancer. N Engl J Med. 1981;305(17):982–987. doi: 10.1056/NEJM198110223051704. [DOI] [PubMed] [Google Scholar]
- 38.Modabbernia A, Poustchi H, Malekzadeh R. Neuropsychiatric and psychosocial issues of patients with hepatitis C infection: a selective literature review. Hepat Mon. 2013;13(1):e8340–e8340. doi: 10.5812/hepatmon.8340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Dantzer R, O'Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci. 2008;9(1):46–56. doi: 10.1038/nrn2297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Haroon E, Raison CL, Miller AH. Psychoneuroimmunology meets neuropsychopharmacology: translational implications of the impact of inflammation on behavior. Neuropsychopharmacology. 2012;37(1):137–162. doi: 10.1038/npp.2011.205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Bürgel B, Friesland M, Koch A, Manns MP, Wedemeyer H, Weissenborn K, Schulz-Schaeffer WJ, Pietschmann T, Steinmann E, Ciesek S. Hepatitis C virus enters human peripheral neuroblastoma cells-evidence for extra-hepatic cells sustaining hepatitis C virus penetration. J Viral Hepat. 2011;18(8):562–570. doi: 10.1111/j.1365-2893.2010.01339.x. [DOI] [PubMed] [Google Scholar]
- 42.Forton DM, Thomas HC, Taylor-Robinson SD. Central nervous system involvement in hepatitis C virus infection. Metab Brain Dis. 2004;19(3-4):383–391. doi: 10.1023/b:mebr.0000043983.42843.ac. [DOI] [PubMed] [Google Scholar]
- 43.Forton DM, Hamilton G, Allsop JM, Grover VP, Wesnes K, O'Sullivan C, Thomas HC, Taylor-Robinson SD. Cerebral immune activation in chronic hepatitis C infection: a magnetic resonance spectroscopy study. J Hepatol. 2008;49(3):316–322. doi: 10.1016/j.jhep.2008.03.022. [DOI] [PubMed] [Google Scholar]
- 44.Cillo U, Amodio P, Ronco C, Soni SS, Zanus G, Minazzato L, Salari A, Neri D, Bombonato G, Schiff S, Bianco T. Hepatitis C virus adversely affects quality of life. Blood Purif. 2011;32(2):144–149. doi: 10.1159/000325222. [DOI] [PubMed] [Google Scholar]
- 45.Goñi Esarte S, Juanbeltz R, Martínez-Baz I, Castilla J, San Miguel R, Herrero JI, Zozaya JM. Long-term changes on health-related quality of life in patients with chronic hepatitis C after viral clearance with direct-acting antiviral agents. Rev Esp Enferm Dig. 2019;111(6):445–452. doi: 10.17235/reed.2019.6063/2018. [DOI] [PubMed] [Google Scholar]
- 46.Younossi ZM, Stepanova M, Reddy R, Manns MP, Bourliere M, Gordon SC, Schiff E, Tran T, Younossi I, Racila A. Viral eradication is required for sustained improvement of patient-reported outcomes in patients with hepatitis C. Liver Int. 2019;39(1):54–59. doi: 10.1111/liv.13900. [DOI] [PubMed] [Google Scholar]
- 47.San Miguel R, del Villar V, Perez C, de Frutos M, Mar J, Coma MJ. Role of health-related quality of life measurements in the design of drug clinical trials. Farmacia Hospitalaria. 2010;34(1):16–22. doi: 10.1016/j.farma.2009.07.002. [DOI] [PubMed] [Google Scholar]
- 48.Miguel RS, López-González AM, Sanchez-Iriso E, Mar J, Cabasés JM. Measuring health-related quality of life in drug clinical trials: is it given due importance. Pharm World Sci. 2008;30(2):154–160. doi: 10.1007/s11096-007-9152-9. [DOI] [PubMed] [Google Scholar]