

Abstract
Background:
Epilepsy is the second most common neurological disorder, and it may have a significant effect on sexual functions in epileptic patients.
Materials and Methods:
Sexual dysfunctions were assessed in 146 male patients suffering from generalized tonic-clonic seizure (GTCS) with a seizure-free interval of at least 1 year. Out of 146 patients enrolled, 46 patients had a psychiatric impairment and were excluded from the study, after applying the General Health questionnaire12 (GHQ12) scale and detailed psychiatric evaluation. The remaining patients were evaluated for the presence of sexual dysfunction by applying Arizona Sexual Experience scale (ASEX). Sixty-six patients scoring more than 19 as a cutoff score on the ASEX scale were further interviewed by a psychiatrist, and a diagnosis of sexual dysfunction was made as per ICD 10 Diagnostic criteria.
Results:
Sexual dysfunction was diagnosed in 66% (n = 66) of the patients. Erectile dysfunction was the most common sexual disorder diagnosed in 36% of the patients (n = 36) followed by premature ejaculation in 26% (n = 26) and decreased libido (hypoactive sexual desire) seen in 4% (n = 4) of the patients. In patients with sexual dysfunction, a significant association was observed with the duration of epilepsy and type of therapy (mono/polytherapy) (P value < 0.05). Erectile dysfunction and hypoactive desire were more common in patients taking polytherapy, whereas premature ejaculation was more common in patients on monotherapy.
Conclusion:
Significant impairment of sexual functions was observed in male epileptics with GTCS. A high index of suspicion should be kept in mind by the practicing clinician on diagnosing and treating sexual dysfunction in them.
Keywords: Anti seizure drugs, epilepsy, male, sexual dysfunction
INTRODUCTION
Epilepsy is a common neurological disorder with a worldwide prevalence of 0.5–1.5 percent, and about 30 percent of men with epilepsy may suffer from sexual dysfunction.[1,2] In India, an estimate suggests that 12 million people are living with epilepsy which accounts for one-sixth of the world epileptic population.[3]
Disorder of sexual function encompasses a variety of disorders that affects libido, ability to attain or maintain an erection (erectile dysfunction or impotence), ability to ejaculate, and ability to achieve an orgasm. The most common sexual dysfunctions experienced by men are premature/delayed ejaculation, erectile dysfunction, and hypoactive sexual desire.[2]
A definite correlation has been observed between abnormalities in sexual functions and epilepsy, and evidence suggests that patients with partial epilepsy are more severely affected than idiopathic generalized epileptic patients.[2]
Both epilepsy and antiseizure drugs (ASDs) causes sexual dysfunction mediated by change in sex hormones. The mechanism of reproductive dysfunction in epileptic patients is a result of a disturbance in the activity of GnRH pulse generator, the spread of epileptiform activity to the limbic system, ictal or interictal activity interfering with the hypothalamus hypophysis adrenal axis. ASDs can cause sexual dysfunction directly by influencing neural transmission in pathways among the limbic system and the hypothalamic–pituitary axis (HPA) that are significant for sexual response.[2,4] It has been observed that certain ASDs ssuch as sodium valproate, phenobarbitol may worsen sexual functions while some other ASDs such as oxcarbazepine, lamotrigine, and levetiracetam may actually improve them.[5] Additionally, certain clinical features related to epilepsy such as seizure frequency, age of onset/duration of epilepsy along with the seizure type may also affect sexual functions.[2,5,6]
Despite the presence of an established relationship between sexual dysfunction and epilepsy, there appears to be a wide variation in their reported prevalence.[7] Anywhere between 40% and 70% of male patients with epilepsy are affected by sexual dysfunction, which includes reduced sexual desire, erectile dysfunction, and premature ejaculation.[2,8] On the other hand, few studies have also shown that patients with epilepsy may have a reduced rate of sexual problems or have an improvement in their sexual functioning.[9]
As sexual dysfunction significantly affects the quality of life of patients with epilepsy so while treating these patients, attention must also be paid to their sexual life. Sexual dysfunction in patients with epilepsy is often neglected by the physician, and there is also very limited data available from this part of the country.[9,10] To address the current gap in the literature, this study was conducted to assess the magnitude of sexual dysfunction and identify factors affecting sexual functions in male patients suffering from idiopathic generalized tonic-clonic seizure (GTCS).
MATERIALS AND METHODS
The present study was a cross-sectional observational study conducted jointly by the Departments of Neurology and Psychiatry of a tertiary care level hospital attached to a Medical College in Rajasthan, India after receiving Institutional ethical committee approval. One hundred and forty-six consecutive male patients suffering from idiopathic GTCS in the age range of 18–40 years, attending the outpatient department (OPD) of neurology were enrolled in the study from January 2019 to March 2020, with a seizure-free interval of a minimum of 12 months and on anti-seizure medications for at least 2 years were included in this study. Yes, Ethics committee approval was taken and date of approval was 07/03/2019.
All the patients were examined and detailed history such as the age of onset, duration of epilepsy, frequency of attack, precipitating factors, drug history, and family history was taken.
Diagnosis of idiopathic GTCS was based on detailed history and examination which was done by the neurologist, recorded videos of seizure episodes which were brought by the attendants/patient, abnormal EEG findings, and normal neuroimaging.
The patients not willing to give consent, with a history of pre-existing psychiatric illness including mental retardation, substance abuse/dependence, or suffering from any other comorbid medical and surgical illnesses were excluded from the study.
Assessment tools
One forty-six enrolled participants were first administered a semi-structured proforma which was designed for capturing the socio-demographic and clinical data. Afterward, they were screened for the presence of psychiatric illness by applying the Hindi version of the General Health Questionnaire (GHQ) 12. This scale consists of 12 questions (assessing 12 different symptoms) which evaluates the intensity of mental problems in the recent few weeks or a month. The Hindi version of GHQ 12 is a valid, reliable, and sensitive tool and has been used in the previous study in India.[11]
Out of 146 patients, 100 patients who scored less than 2 (cut-off score) on the General Health questionnaire12 (GHQ12) scale were further interviewed and assessed in detail by a consultant psychiatrist to rule out the presence of any other comorbid psychiatric illness. Subsequently, Arizona sexual experience rating scale (ASEX)[12] was applied to identify sexual dysfunction.[13] ASEX is a five-item scale with a score range from 0 to 30, it includes questions regarding sex drive, arousal, vaginal lubrication/penile erection, ability to reach orgasm, and satisfaction from orgasm.[12] The Cronbach's alpha of this scale is 0.89.[14]
The patients scoring more than 19 as a cut-off score on ASEX were considered to be suffering from sexual dysfunction and were interviewed in detail by a consultant psychiatrist, and a final diagnosis of sexual disorder was made as per criteria of the International Classification of Disease mental and behavioral disorders, clinical description and diagnostic guidelines 10th edition (ICD-10).[15] [Figure 1]
Figure 1.
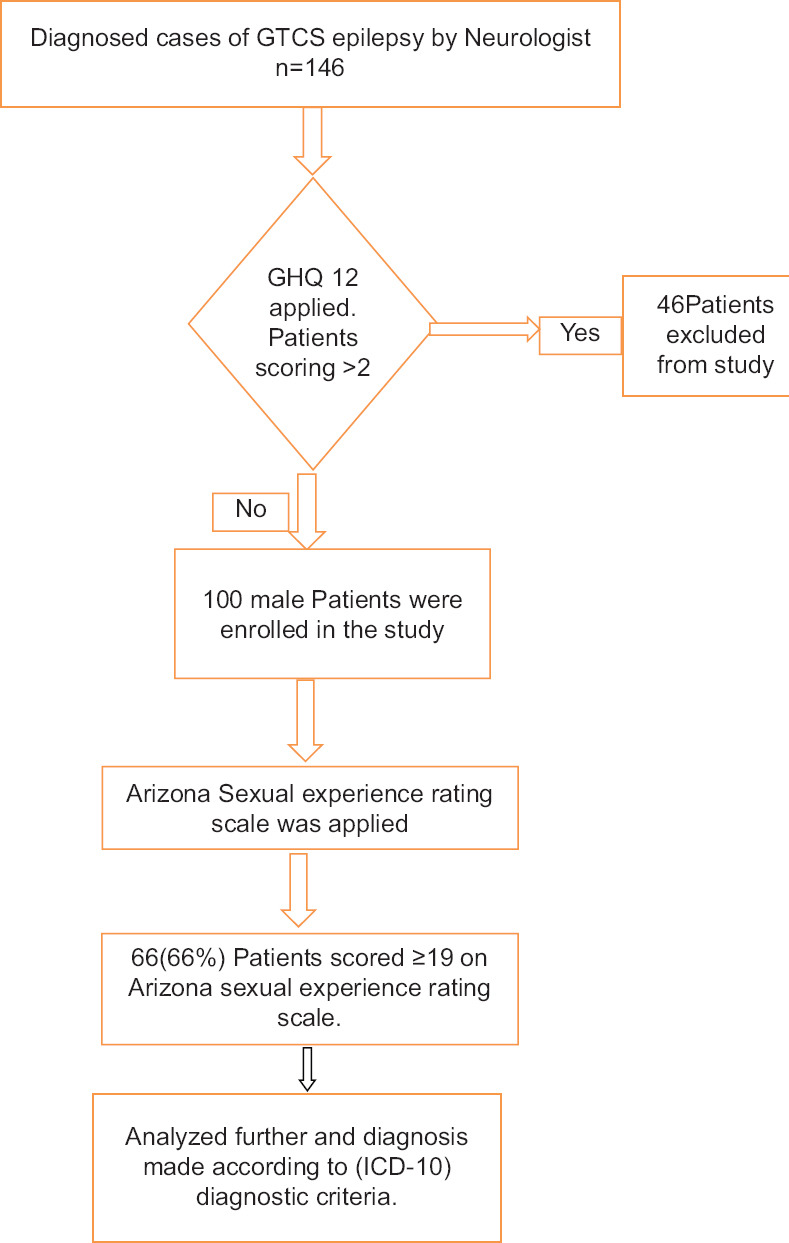
Study Design Flowchart
The data thus collected were compiled and analyzed further. The quantitative data were analyzed by mean and standard deviation, and qualitative data were analyzed in percentage. The statistical analysis was performed by using SPSS 26 version software. An unpaired t test was applied to find out the association between quantitative data. P value < 0.05 was considered significant.
RESULTS
The mean age of our patient population was 28.7 ± 4.95 years. Fifty-two percent of patients were from an urban background, 46% were educated till 10th class, 38% were in service, and 50% had family income between 5,001 and 10,000 Rupees. The majority of participant patients were married (84%), the mean age of first sexual intercourse of such patients being 23.92 ± 3.02 years, and 82% of the patients had only one sexual partner. The mean age of onset of first seizure was 25.32 ± 7.77, and the mean duration of epilepsy was 5.4 ± 4.8. Fifty percent (n = 50) were on monotherapy, 42% (n = 42) were on two drug therapy, and 8% (n = 8) were on three drugs. [Table 1].
Table 1.
Socio-demographic and clinical data of male patients with epilepsy
| Variable | n=100, f% |
|---|---|
| Age | 28.7±4.95 years (mean, S.D) |
| Domicile | |
| Rural | 48 (48%) |
| Urban | 52 (52%) |
| Religion | |
| Hindu | 62 (62%) |
| Muslim | 38 (38%) |
| Marital status | |
| Married | 84 (84%) |
| Unmarried | 16 (16%) |
| Education | |
| Primary | 20 (20%) |
| Secondary | 52 (52%) |
| Senior Secondary | 22 (22%) |
| Graduate | 06 (6%) |
| Occupation | |
| Unemployed | 12 (12%) |
| Laborer | 14 (14%) |
| Farmer | 30 (30%) |
| Service | 38 (38%) |
| Shopkeepers | 06 (06%) |
| Income per month (INR) | |
| <5000 INR | 12 (12%) |
| 5,001-10,000 INR | 50 (50%) |
| 10,001-20,000 INR | 20 (20%) |
| >20,000 INR | 18 (18%) |
| No. of Sexual Partners | |
| Monogamous | 82 (82%) |
| Polygamous | 18 (18%) |
| Duration of Illness | |
| <5 Years | 62 (62%) |
| ≥5 Years | 38 (38%) |
| Therapy (No. of Antiepileptic Drug) AED | |
| 1 Antiepileptic drug | 50 (50%) |
| 2 Antiepileptic drug | 42 (42%) |
| >2 Antiepileptic drug | 08 (8%) |
| Mean age of Onset of Epilepsy | 25.32±7.77 years (mean, S.D) |
| Mean duration of Epilepsy | 4.8±2.8 |
Out of 100 patients, on applying Arizona sexual experience rating scale, 66 participants (66%) scored more than 19 and of such 66 patients, majority were suffering from erectile dysfunction (n = 36, 36%) followed by premature ejaculation (n = 26, 26%) and hypoactive sexual desire (n = 4, 4%) [Tables 2 and 3].
Table 2.
Sexual dysfunction (ASEX >19)
| Sexual Dysfunction | Number of patients | Percent |
|---|---|---|
| Yes | 66 | 66% |
| No | 34 | 34% |
| Total | 100 | 100% |
Table 3.
Sexual dysfunction reported in male patients with epilepsy
| Diagnosis | n=100, (%) |
|---|---|
| Erectile dysfunction | 36 (36%) |
| Premature Ejaculation | 26 (26%) |
| Hypoactive sexual desire | 04 (04%) |
| No sexual dysfunction | 34 (34%) |
A statistically significant association was observed between the sexual dysfunction and total duration of illness. Out of 62 patients with a duration of illness of fewer than 5 years, 44 patients (71%) were diagnosed with sexual dysfunction, whereas out of 38 patients with a duration of illness of more than 5 years, 22 patients (58%) were diagnosed with sexual dysfunction. [Table 4]
Table 4.
Duration of epilepsy and its association with sexual dysfunction
| Duration of epilepsy | n (No. of patients) | Sexual Dysfunction present (n) | Percentage | P |
|---|---|---|---|---|
| <5 Years | 62 | 44 | 71% | 0.018 (Significant) |
| ≥5 Years | 38 | 22 | 58% |
Similarly, a statistically significant association was also observed between the total number of antiseizure medicine and sexual dysfunction. Out of 50 patients who were on monotherapy, 30 patients (60%) had sexual dysfunction while on the other hand, out of the other 50 patients who were on polytherapy, 36 patients (72%) were having sexual dysfunction. [Table 5]
Table 5.
No. of Anti seizure Drugs and its association with sexual dysfunction in epileptic patients
| Antiepileptic Drug | n (No. of patients) | Sexual Dysfunction present (n=number of patients) | Percentage | P |
|---|---|---|---|---|
| Monotherapy (1 Antiseizure drug) | 50 | 30 | 60% | 0.049 (Significant) |
| Polytherapy (2 or more Antiseizure drugs) | 50 | 36 | 72% |
On assessing the effect of monotherapy on sexual dysfunction, it was observed that 85% (n = 12) of patients taking valproate had sexual dysfunction followed by phenytoin (60%) (n = 12), whereas only 37.5% (n = 6) patients taking levetiracetam were experiencing sexual dysfunction. While exploring the relationship between sexual dysfunction and polytherapy, 100% (n = 8) of patients who were taking a combination of three ASDs (phenytoin + valproate + levetiracetam) had sexual dysfunction followed by 87.5% (n = 14) of patients who were taking a combination of valproate with levetiracetam were suffering from sexual dysfunction. Seventy-five percent (n = 6) of patients taking a combination of phenytoin with phenobarbitone were suffering from sexual dysfunction. The least sexual dysfunction was observed in patients who were on a combination of phenytoin with levetiracetam which was 44.4% (n = 8). [Table 6]
Table 6.
Anti-seizure Drugs and Sexual functioning
| Antiepileptic drug (n=number of patients) | Sexual dysfunction present | Normal sexual functioning |
|---|---|---|
| Phenytoin (20) | 12 | 8 |
| Levetiracetam (16) | 6 | 10 |
| Valproate (14) | 12 | 2 |
| Levetiracetam + Valproate (16) | 14 | 2 |
| Phenytoin + Levetiracetam (18) | 8 | 10 |
| Phenytoin + Phenobarbitone (8) | 6 | 2 |
| Phenytoin + Valproate + Levetiracetam (8) | 8 | 0 |
| Total (100) | 66 | 34 |
While evaluating the effect of individual drugs or combination of drugs on sexual dysfunction, it was observed that patients on sodium valproate as monotherapy (n = 14) had both erectile dysfunction and premature ejaculation in 43% (n = 6) cases each with no hypoactive sexual desire disorder. In the patients taking levetiracetam only, 25% (n = 4) had premature ejaculation, and 12.5% (n = 2) had erectile dysfunction while 62.5% (n = 10) had no sexual dysfunction.
Among the patients who were on polytherapy with levetiracetam and valproate (n = 16) 50% (n = 8) of cases had erectile dysfunction; premature ejaculation was present in 25% (n = 4) cases; and hypoactive sexual desire, in 12.5% (n = 2) cases. Among the patients on phenytoin and levetiracetam (n = 18) erectile dysfunction was present in 33.3% (n = 6) of cases and premature ejaculation, in 11.11% (n = 2) cases with no cases of hypoactive sexual desire.
Premature ejaculation was more common among patients who were on dual therapy of phenytoin and phenobarbitone (50%, n = 4). In the present study, hypoactive sexual desire was observed in four patients, out of which, two patients were on a combination of three antiseizure medicines (phenytoin, valproate, and levetiracetam), and the remaining two were on dual therapy of levetiracetam and valproate [Table 7].
Table 7.
Anti-seizure drugs and Sexual dysfunction
| Antiepileptic drug | Erectile dysfunction | PME (Premature ejaculation) | Hypoactive sexual desire | Normal Sexual Functioning |
|---|---|---|---|---|
| Phenytoin (20) | 8 | 4 | 0 | 8 |
| Levetiracetam (16) | 2 | 4 | 0 | 10 |
| Valproate (14) | 6 | 6 | 0 | 2 |
| Levetiracetam+Valproate (16) | 8 | 4 | 2 | 2 |
| Phenytoin+Levetiracetam (18) | 6 | 2 | 0 | 10 |
| Phenytoin+Phenobarbitone (8) | 2 | 4 | 0 | 2 |
| Phenytoin+Valproate+Levetiracetam (8) | 4 | 2 | 2 | 0 |
| TOTAL (100) | 36 | 26 | 4 | 34 |
DISCUSSION
It has been reported that sexual dysfunctions in epilepsy are multi-factorial in origin and could be due to psychosocial factors, type of epilepsy, epileptiform discharges, antiseizure drugs, high seizure burden, etc.[2,5] However, evidence gained from several other studies refutes such factors so implicated in inducing sexual dysfunction.[16] It has been reported that patients with epilepsy have a significantly higher frequency of sexual problems as compared to that observed in adults in the general population.[7,9,17] Bóné and Janszky in 2006[8] have reported that around 40%–70% of male epileptic patients on ASDs suffer from sexual dysfunctions, a finding that has been supplanted in the present study that has documented sexual dysfunctions in 66% of the study population.
Erectile dysfunction in patients with epilepsy shows a prevalence that may vary from 3% to 58% depending on several factors.[18] In the present study, erectile dysfunction was the most common sexual dysfunction, a finding that has been documented by other studies as well.[19,20] The sexual dysfunction of premature ejaculation (PME) was the second most common sexual dysfunction observed in 26% of the study participants, a finding that has been reported by Norwegian study as well (2019).[9]
A study conducted in Brazil observed that 28% of the patients with epilepsy had hypoactive sexual desire,[8] though only 4% study patients’ population reported hypoactive sexual desire in the present study. A poignant observation has been made by Hellmis[10] in 2008, that patients with controlled seizures seem to have a lower rate of hypo sexuality that has been validated by findings of the present study, wherein participant patients who were seizure-free for the last 1 year had reported a low frequency of hypoactive sexual disorder.
It could be concluded from the results of the present study that sexual dysfunctions were more common in epileptic patients with a disease duration of fewer than 5 years, an observation that is in contradiction to that of Hamed et al. (2013),[21] who had made a generalization that chronicity and duration of the disease process of epilepsy are more likely to induce sexual dysfunctions like erectile dysfunction. It would be pertinent to add that most of the present study patients were on ASD polytherapy that could be the confounding factor responsible for such sexual dysfunctions.[22]
Although sexual dysfunction due to anti-seizure medicines has been commonly reported, certain antiepileptic medicines such as oxcarbazepine, lamotrigine, and levetiracetam may in fact improve sexual functioning.[5] However Oliver et al.[9] in their study on epileptic patients could not appreciate any significant association between sexual dysfunction and the use of antiseizure drugs in patients with epilepsy.
While evaluating sexual dysfunction in the present study, it was observed that incidence of erectile dysfunction and hypoactive desire were more in polytherapy, whereas premature ejaculation was more commonly observed in epileptics on monotherapy. In monotherapy patients, it was observed that the majority of patients on valproate had a high percentage of sexual dysfunctions while patients on levetiracetam fared better, an observation that has also been documented by the Iranian study of 2020,[23] that could be due to the fact that valproate modifies gamma-aminobutyric acid-ergic (GABAergic) neurotransmission and could alter secretion of gonadotropins, but its complete effect on reproductive endocrine function is still unknown. In addition, valproate also has direct effects on sperm motility.[24] In the present study, hypoactive sexual drive has been reported in the patients on polytherapy with valproate and levetiracetam, which could be due to the fact that levetiracetam increases brainstem serotonin concentration by inhibiting presynaptic P/Q-type calcium channels, thus, causing reduced sexual drive.[25]
Limitation
Our study is subjected to several limitations like a modest number of participants, restricting statistical power. A larger sample would have provided a better understanding of the relationship between current studies variables. Other methodological issues include overt reliance on a single scale to assess sexual dysfunction and lack of endocrine workup.
CONCLUSION
Patients with epilepsy usually do not report sexual dysfunction by themselves. Looking at the high magnitude of implicit sexual dysfunction in epileptic patients (not being reported), a high index of suspicion should be kept in mind by the practicing neurologist/physician, and such patients necessarily need to be screened on a regular basis to rule out underlying sexual dysfunction, if any.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Fiest KM, Sauro KM, Wiebe S, Patten SB, Kwon CS, Dykeman J, et al. Prevalence and incidence of epilepsy: A systematic review and meta-analysis of international studies. Neurology. 2017;88:296–303. doi: 10.1212/WNL.0000000000003509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Atif M, Sarwar MR, Scahill S. The relationship between epilepsy and sexual dysfunction: A review of the literature. Springerplus. 2016;5:2070. doi: 10.1186/s40064-016-3753-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Amudhan S, Gururaj G, Satishchandra P. Epilepsy in India I: Epidemiology and public health. Ann Indian Acad Neurol. 2015;18:263–77. doi: 10.4103/0972-2327.160093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Kumar DP, Wadwekar V, Nair PP, Menon V, Bhatnagar T. Study of sexual dysfunction in people living with epilepsy at a tertiary care center of South India. Neurol India. 2020;68:861–6. doi: 10.4103/0028-3886.293437. [DOI] [PubMed] [Google Scholar]
- 5.Yang Y, Wang X. Sexual dysfunction related to antiepileptic drugs in patients with epilepsy. Expert Opin Drug Saf. 2016;15:31–42. doi: 10.1517/14740338.2016.1112376. [DOI] [PubMed] [Google Scholar]
- 6.Lambert MV. Seizures, hormones and sexuality. Seizure. 2001;10:319–40. doi: 10.1053/seiz.2000.0512. [DOI] [PubMed] [Google Scholar]
- 7.Rathore C, Henning OJ, Luef G, Radhakrishnan K. Sexual dysfunction in people with epilepsy. Epilepsy Behav. 2019;100:106495. doi: 10.1016/j.yebeh.2019.106495. doi: 10.1016/j.yebeh. 2019.106495. [DOI] [PubMed] [Google Scholar]
- 8.Bóné B, Janszky J. Epilepsy and male sexual dysfunction: Etiology, diagnosis and therapy. Ideggyógy Sze. 2006;59:148–52. [PubMed] [Google Scholar]
- 9.Henning O, Johannessen Landmark C, Træen B, Svendsen T, Farmen A, Nakken KO, et al. Sexual function in people with epilepsy: Similarities and differences with the general population. Epilepsia. 2019;60:1984–92. doi: 10.1111/epi.16311. [DOI] [PubMed] [Google Scholar]
- 10.Hellmis E. Sexual problems in males with epilepsy—An interdisciplinary challenge! Seizure. 2008;17:136–40. doi: 10.1016/j.seizure.2007.11.011. [DOI] [PubMed] [Google Scholar]
- 11.Gautam S, Nijhawan M, Kamal P. Standardisation of hindi version of goldbergs general health questionnaire. Indian J Psychiatry. 1987;29:63–6. [PMC free article] [PubMed] [Google Scholar]
- 12.McGahuey CA, Gelenberg AJ, Laukes CA, Moreno FA, Delgado PL, McKnight KM, et al. The Arizona sexual experience scale (ASEX): Reliability and validity. J Sex Marital Ther. 2000;26:25–40. doi: 10.1080/009262300278623. [DOI] [PubMed] [Google Scholar]
- 13.Luef GJ. Epilepsy and sexuality. Seizure. 2008;17:127–30. doi: 10.1016/j.seizure.2007.11.009. [DOI] [PubMed] [Google Scholar]
- 14.Soykan A. The reliability and validity of Arizona sexual experiences scale in Turkish ESRD patients undergoing hemodialysis. Int J Impot Res. 2004;16:531–4. doi: 10.1038/sj.ijir.3901249. [DOI] [PubMed] [Google Scholar]
- 15.Organisation W. The ICD-10 classification of mental and behavioural disorders. Clinical descriptions and diagnostic guidelines. Geneva: World Health Organisation; 1992. [Google Scholar]
- 16.McIntosh KA, Jette N. Epidemiology of women with epilepsy. In: Bui E, Klein AM, editors. Women with Epilepsy: A Practical Management Handbook. Cambridge: Cambridge University Press; 2014. pp. 1–19. [Google Scholar]
- 17.Zhao S, Tang Z, Xie Q, Wang J, Luo L, Liu Y, et al. Association between epilepsy and risk of sexual dysfunction: A meta-analysis. Seizure. 2019;65:80–8. doi: 10.1016/j.seizure.2019.01.004. [DOI] [PubMed] [Google Scholar]
- 18.Smaldone M, Sukkarieh T, Reda A, Khan A. Epilepsy and erectile dysfunction: A review. Seizure. 2004;13:453–9. doi: 10.1016/j.seizure.2003.12.006. [DOI] [PubMed] [Google Scholar]
- 19.Hamed S, Mohamed K, El-Taher A, Hamed E, Omar H. The sexual and reproductive health in men with generalized epilepsy: A multidisciplinary evaluation. Int J Impot Res. 2006;18:287–95. doi: 10.1038/sj.ijir.3901406. [DOI] [PubMed] [Google Scholar]
- 20.Nikoobakht M, Motamedi M, Orandi A, Meysamie A, Emamzadeh A. Sexual dysfunction in epileptic men. Urol J. 2007;4:111–7. [PubMed] [Google Scholar]
- 21.Hamed SA, Ahmad HK, Youssef AH, Metwaly NA, Hassan MM, Mohamad HO. Erectile function in men with epilepsy: Relationship to psychosocial-, hormonal-, epilepsy- and antiepileptic drugs-related variables. J Neurol Neurosci. 2013;4:5. [Google Scholar]
- 22.Zelená V, Kuba R. Sexual dysfunction in women with epilepsy. Epilepsy & Behavior. 2010;17:615. doi: 10.1016/j.yebeh.2011.01.014. [DOI] [PubMed] [Google Scholar]
- 23.Mazdeh M, Heidari M, Taheri M, Ghafouri-Fard S. Anticonvulsant drugs effects on sex hormone levels and sexual function in men with epilepsy. Future Neurology. 2020;15:FNL43. [Google Scholar]
- 24.Isojärvi JI, Taubøll E, Herzog AG. Effect of antiepileptic drugs on reproductive endocrine function in individuals with epilepsy. CNS Drugs. 2005;19:207–23. doi: 10.2165/00023210-200519030-00003. [DOI] [PubMed] [Google Scholar]
- 25.Calabrò RS, Italiano D, Militi D, Bramanti P. Levetiracetam-associated loss of libido and anhedonia. Epilepsy & Behavior. 2012;4:283–4. doi: 10.1016/j.yebeh.2012.03.013. [DOI] [PubMed] [Google Scholar]