

Abstract
Objective:
To compare the cephalometric characteristics of Down syndrome (DS) subjects with those of normal subjects.
Materials and Methods:
Cephalometric radiographs of 60 Saudi DS subjects and 60 controls with specific inclusion criteria were used. Descriptive statistics were used to describe the quantitative and categorical variables, and the Student's t-test for two independent samples was used to compare the mean values of quantitative variables.
Results:
SBa and SN were higher in controls than in DS subjects, whereas the NSBa was significantly higher in DS subjects than in controls. SNA, Co-A, ANB, and A-Na perp of controls were higher than the DS subjects. However, SN-MP, PP-MP, ANS-Me/N-Me, Y-axis, and Ar-Go-Me of the DS subjects were higher than those of the controls. In addition, U1-NA, U1-NA mm, L1-NB, and L1-NB mm of the DS subjects were also higher than the controls with a more acute U1-L1 angle in DS. NLA was larger in controls than in DS, whereas LL-E and UL-E of the DS subjects were higher than the controls.
Conclusions:
Differences between DS subjects and controls can be found when examining cephalometric radiographs. Anterior and posterior cranial base lengths are shorter with a backward inclination of the posterior cranial base in DS subjects. DS subjects present with a retrognathic maxilla and shorter effective length, with an increased LFH and a hyperdivergent mandible. Bimaxillary dental protrusion can also be expected in DS subjects with prominent lips and a reduced nasolabial angle.
Keywords: Cephalometrics, Down syndrome, Skeletal, Dental, Soft tissue
INTRODUCTION
Down syndrome (DS), which is also known as trisomy 21, trisomy G, and mongolism, is a congenital autosomal (non–sex chromosomes) anomaly characterized by a deficiency in general and mental development, affecting 1 in 600 to 1 in 2000 live births in different populations.1 Individuals with DS present with various characteristic physical and systemic manifestations, with the craniofacial manifestations being the most distinctive.2 Craniofacial features reported include midface deficiency, mandibular prognathism, depressed nasal bridge, slanting eyes with epicanthic folds, ocular hypotelorism, and strabismus. Perioral muscles are also affected by muscle hypotonia, leading to a descending of the angle of the mouth.3
Many studies were performed on Down syndrome subjects using cephalometric radiographs. Among them was a study done by Frostad et al.4 who found that the overall size of the craniofacial complex was smaller in DS subjects. Fink et al.5 concluded that the sagittal area of the endocranium, the area of the midfacial region, and the area of the mandible in subjects with DS is significantly smaller than normal. Fischer-Brandies et al.6 reported that both the maxilla and mandible in DS patients exhibit hypoplasia at birth. In a subsequent study, Fischer-Brandies7 revealed that the maxilla was underdeveloped when compared to normal subjects. Quintanilla et al.8 added that DS subjects usually demonstrate reduction of the anterior skull base and protrusion and proclination of lower incisors.
Recently, Suri et al.9 found that DS patients have a larger cranial base angle, reduced elevation of sella from Frankfort horizontal plane, reduced anterior and posterior cranial base lengths and facial heights, smaller maxilla with reduced anterior basal and apical dimensions, and smaller mandibular ramus and body. Anterior open bite was frequently noted with a forward rotation pattern of both maxillary and mandibular planes. Alió et al.10 concluded that the maxilla in DS subjects showed hypoplasia in both the vertical and the sagittal planes, with a mean deficit of almost 10 mm in the latter.
In Saudi Arabia, a relatively high incidence of DS has been found with a prevalence of 1 in 554 live births.11 With regard to the facial and oral characteristics of Saudi DS subjects, only one study has been reported so far describing them.12 Until today, no report on the cephalometric features of DS subjects in Saudi Arabia has been documented. Therefore, the aim of this study was to investigate the cephalometric features of DS subjects and to compare these findings with normal control subjects. The results of this study are expected to enhance the orthodontic diagnosis and management of individuals with DS.
MATERIALS AND METHODS
Sample
Sixty Saudi DS patients of both genders (33 female, 27 male) with an age range from 12–22 years (mean age 15.8 years) were included in this study. After obtaining approval from the ethics committee at the College of Dentistry Research Center in King Saud University, different hospitals, DS care centers, and schools in Riyadh city (capital city of Saudi Arabia) were visited. Families were contacted and the study was explained to them. Those who agreed to participate in the study were included.
All patients selected were proven to be affected by a genetic abnormality based on chromosomal analysis by karyotype test. This was found in the medical or school files of each individual. The DS subjects were in good general health, with the typical body characteristics of DS individuals. All subjects in the study were living with their families and not institutionalized. Once a consent form was signed by the parents, lateral cephalometric radiographs were taken at the College of Dentistry at King Saud University using the Planmeca Proline EC machine. The parameters for the machine were standardized and routinely calibrated at a regular and fixed schedule. The procedure for obtaining the cephalometric radiographs was carried out by a well-trained technician and the orthodontic resident.
In order to compare the DS subjects with a normal group of subjects, 60 cephalometric radiographs of normal controls matching the DS subjects in age and gender (with specific inclusion criteria) were obtained from the archives of the College of Dentistry.
The selection criteria for the control group were based on the following:
Subjects should be nonsyndromic.
Subjects should have Class I skeletal relation, average facial height, average overjet and overbite, no extraction or congenital missing teeth, and no history of orthodontic treatment.
Subjects should have no known medical problems such as growth, ear-nose-throat infections, or cervical or back problems.
Methods
M Pro Scanner, (Epson perfection V750-M ProScanner, Seiko Epson Corp, Tokyo, Japan) then digitized and traced by one examiner using an orthodontic imaging and management solutions software (Dolphin 11 imaging and management solutions software, Chatsworth, Calif). The linear measurements were adjusted by entering the first two ruler points; this allowed the software to adjust for magnification.13 Angular and linear measurements were obtained for the hard and soft tissue. For intraexaminer reliability, 30 cephalometric radiographs (15 DS, 15 controls) were randomly selected and analyzed twice within a 2-week interval. Figure 1 shows the cephalometric landmarks chosen. Table 1 displays the angular and linear measurements that were used with their corresponding definitions, and Figures 2 through 4 show the cephalometric measurements of the craniofacial complex.14–19 Figure 5a,b shows the cephalometric tracing of a Down syndrome and a control subject, respectively.
Figure 1.
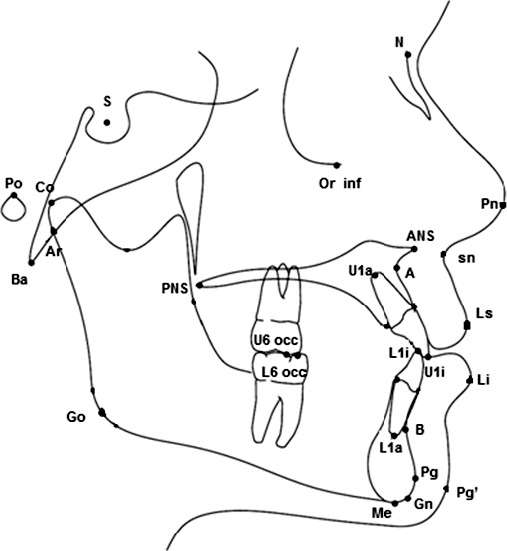
Cephalometric landmarks used in the study. Po indicates porion; S, sella; Orb inf, orbita inferior; N, nasion; Ba, basion; B, supramentale; pg, pogonion; Gn, gnathion; Me, menton; Ar, articulare; Go, gonion; A, subspinale; ANS, anterior nasal spine; Co, condylion; L1a, lower central root apex; L1i, lower central incisal tip; U1i, upper central incisal tip; U1a, upper central root apex; sn, subnasale; Pn, pronasale; Ls, labia superioris; Li, labia inferioris; Pg′, soft tissue pogonion; U6 occ, occlusal surface of upper first molar; L6 occ, occlusal surface of lower first molar; and PNS, posterior nasal spine.
Table 1.
Angular and Linear Cephalometric Measurements and Their Definitions

Figure 2.
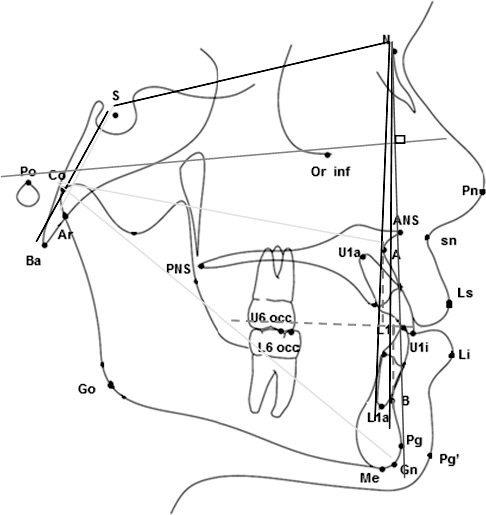
Cranial base measurements: (SN length, SBa length, and NSBa angle). Sagittal skeletal measurements: (SNA angle, SNB angle, ANB angle, Wits appraisal, Co-A length, Co- Gn length, A-Na perp, and Pg-Na perp).
Figure 3.
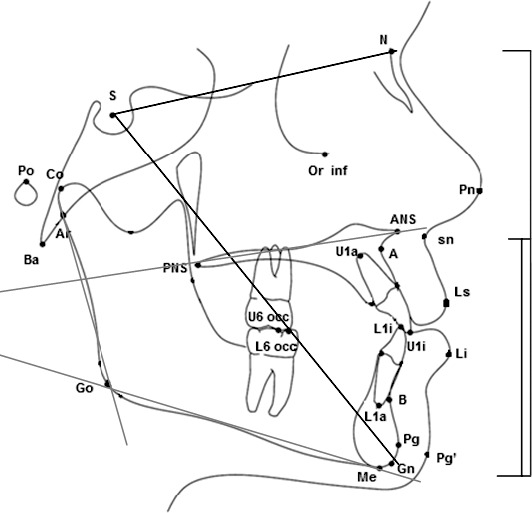
Vertical skeletal measurements: (PP-MP angle, SN-MP angle, ANS-Me/N-Me [%], Y-axis [SGn-SN] angle, and Ar-Go-Me angle).
Figure 4.

Dental measurements: (UI-NA angle and distance, LI-NB angle and distance, and Ui-Li angles). Soft tissue measurements: (NLA angle, UL-E line distance, and LL-E line distance).
Figure 5.
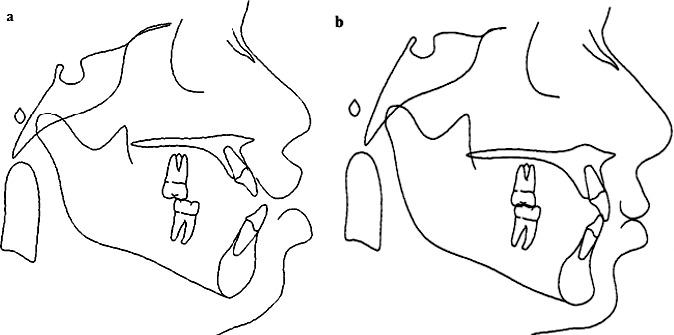
(a) Cephalometric tracing of a 15-year old girl with DS. (b) Cephalometric tracing of a control of similar age and gender.
Statistical Analysis
The data were entered in MS Excel and analyzed using the SPSS Pc+ version 18.0 statistical software. Descriptive statistics (mean, standard deviation, and percentages) were used to describe the quantitative and categorical variables. Student's t-test for two independent samples was used to compare the mean values of quantitative variables when the distribution of the data was symmetric. The Mann-Whitney U-test was used to compare the mean ranks of quantitative variables when the distribution of the data was skewed. The reliability of the readings of all study variables was measured 2 weeks apart by the same examiner for a random sample of 15 DS subjects and 15 controls. A P value of ≤.05 and 95% confidence intervals were used to assess statistical significance and precision of the estimates.
RESULTS
Reliability of Measurements
The Cronbach alpha was calculated to assess the consistency between the two sets of measurements of cranial base, sagittal skeletal, vertical skeletal, dental, and soft tissue. The values obtained ranged from 0.80 to 0.95, which indicate a highly statistically significant reliability of measurements.
Comparisons of the Craniofacial Analysis of DS Subjects and Controls
In order to analyze the results that were obtained, the cephalometric measurements were divided into five separate entities: cranial base, sagittal skeletal, vertical skeletal, dental, and soft tissue measurements.
Cranial base measurements: There was a highly statistically significant difference in the values of the cranial base measurements SBa length, SN length, and NSBa angle between DS subjects and controls (Table 2). The values of SBa (P = .001) and SN (P < .0001) were statistically significantly larger in controls than in the DS subjects, whereas NSBa values of DS cases were significantly larger than those of the controls (P < .0001).
Sagittal skeletal measurements: A highly statistically significant difference in sagittal skeletal measurements Co-A, ANB, and A-Na perp (P < .0001), and SNA (P = .002) of DS subjects and controls was observed, where the measurements of the controls were significantly larger than those of the DS subjects (Table 3). In addition, the Wits appraisal proved to be significantly different in the DS subjects when compared to the controls (P = .006).The Co-Gn, SNB, and Pg-Na perp showed no significant differences between DS subjects and controls.
Vertical skeletal measurements: There was a highly statistically significant difference in the vertical skeletal measurements SN-MP (P = .008), PP-MP (P = .037), ANS-Me/N-Me (P = .002), Y-axis (SGn-SN) (P < .001), and Ar-Go-Me (P < .0001) of DS subjects and controls, where the measurements of the DS subjects were larger than those of the controls (Table 4).
Dental measurements: Highly statistically significant differences in U1-NA (P = .005), U1-NA mm, L1-NB, and L1-NB mm (P < .0001) were noted where the measurements of the DS subjects were larger than those of the controls (Table 5). However, the U1-L1 measurement of the controls was statistically significantly larger than that of the DS subjects (P < .0001).
Soft tissue measurements: The control subjects exhibited a highly statistically significant difference in the NLA, where the control values were significantly larger than the DS subjects (P < .0001) (Table 6). On the other hand, a statistically significant difference was observed between the control and the DS group with LL-E and UL-E, where the values of the DS subjects were significantly larger than those of the controls (P < .0001).
Table 2.
Comparison of Mean Values of Cranial Base Measurements Between Down Syndrome (DS) Cases and Controlsa

Table 3.
Comparison of Mean Values and Median Values of Sagittal Skeletal Measurements Between Down Syndrome (DS) Cases and Controlsa

Table 4.
Comparison of Mean Values of Vertical Skeletal Measurements Between Down Syndrome (DS) Cases and Controlsa

Table 5.
Comparison of Mean Values of Dental Measurements Between Down Syndrome (DS) Cases and Controlsa

Table 6.
Comparison of Mean Values and Median Values of Soft Tissue Measurements Between Down Syndrome (DS) Cases and Controls

DISCUSSION
Down syndrome is the most common of all malformation syndromes.1 It is the most recognized cause of physical and intellectual disability with the highest birth rate of all chromosomal abnormalities. In this study, DS subjects were chosen in particular since there is a relatively high incidence in Saudi Arabia with 1 in every 554 live births being affected.11 According to Kumar et al.20 and Horbelt,21 the life expectancy of these patients has increased significantly over the past few years. With this decreased mortality rate and increased incidence, the overall effect is a growing population of DS individuals.
The results of the present research proved that there were significant differences in the cephalometric findings in all the studied areas between the two groups. The first part of the analysis concentrated on measuring the length of the anterior (SN) and posterior cranial base (SBa), and the inclination of the posterior cranial base (SNBa) of the two study groups. Our findings revealed that the angle of the cranial base was more obtuse, and the length of the anterior and posterior cranial bases was more reduced in DS subjects when compared with normal subjects. This is in agreement with Frostad et al.4 who found that the overall size of the craniofacial complex was smaller in the DS group at 4 years of age and remained smaller into adulthood. Similarly, Fink et al.5 concluded that the sagittal area of the endocranium is significantly smaller than normal. More recently, Suri et al.9 found that the angle of the cranial base was more obtuse, and the anterior and posterior cranial base lengths were reduced in DS subjects in comparison to the norm. Alió et al.10 reported that growth in the cranial base of DS patients is less than that in the general population. They also found that the cranial base in DS patients is flatter and shorter, which is in agreement with the results presented here.
The second part of the analysis represents the sagittal measurements of the maxilla and mandible of both groups. The findings of the study revealed significant differences regarding all measurements of the maxilla (Co-A, SNA, A-Na perp) between the two groups. The maxilla was found to be significantly smaller and retrognathic in DS subjects in comparison to controls. In addition, both the ANB angle and the Wits appraisal illustrated significant differences as well, with the tendency of DS subjects toward a Class III skeletal relation. On the other hand, the mandibular measurements did not show any significant differences (Co-Gn, SNB, Pg-Na perp). Frostad et al.4 showed supporting results regarding the maxilla. Their study concluded that the overall size of the young DS craniofacial complex was smaller, with the maxilla being more retrognathic. Moreover, Fink et al.5 in their investigation concluded that the area of the midfacial region in subjects with DS was significantly smaller than normal subjects. Fischer-Brandies7 and Suri et al.9 found that the maxilla was smaller in Down subjects similar to the present study. Finally, Alió et al.10 concluded that the maxilla in DS subjects showed hypoplasia in both the vertical and sagittal planes, which is in agreement with the current study. In contrast to the studies mentioned above, a study performed by Quintanilla et al.8 found that the craniofacial parameters for facial and maxillary depths indicated average values within the clinical norm.
Regarding mandibular development, Quintanilla et al.8 found similar results to our study in which the mandible was not found to be affected by the syndrome. However, Fink et al.5 and Suri et al.9 found the mandible—although not to the extent of the maxilla—was smaller in DS subjects.
When the vertical measurements (SN-MP, PP-MP, ANS-Me/N-Me,Y-axis, Ar-Go-Me) were analyzed, significant differences between the two groups were found. A hyperdivergent mandible and increased lower facial height with a skeletal open bite tendency can be expected in DS subjects. This is contrary to the results shown by Quintanilla et al.8 who revealed in their analysis that DS subjects have a tendency toward a normal mandibular growth pattern rather than vertical growth. However, their study did not compare DS subjects to matching controls. In addition, this difference could be related to a population dissimilarity.
When comparing the dental measurements of DS subjects with the control group, significant differences were found. Protruded and proclined upper and lower incisors and hence, a decreased upper to lower incisor angle was noted in the Down subjects when compared to the normal controls. This is in agreement with Suri et al.9 who found in their cephalometric analysis that DS subjects have severely proclined upper incisors and Quintanilla et al.8 who found that the lower incisors in the Down subjects were protruded and proclined. Several studies22–24 hypothesized that proclination of the anterior teeth in DS subjects is related to the anterior position of the tongue.18,19 Macroglossia has been reported previously, which in turn could have led to the increased dental protrusion found in ours and other studies.12,25–28
Soft tissue comparative measurements of the present study showed significant differences as well. A significantly smaller nasolabial angle and protruded upper and lower lips were noted in Down subjects when compared to controls. Ferrario et al.29 found similar results in which the nasolabial angle was more acute, and both upper and lower lips were more protruded and prominent in Down subjects. A study performed by Quintanilla et al.8 showed the same with regard to the lips in which they were found to be more prominent in DS subjects. However, Sforza et al.30 reported that the nasolabial angle in DS subjects was actually increased, with a more obtuse angle. This difference could be due to the ethnic background of the subjects since this was done on a Northern Sudanese sample.
CONCLUSIONS
It can be concluded from this study that:
DS subjects present with a shorter anterior and posterior cranial base length and a backward rotation of the posterior cranial base.
The maxilla of DS subjects is usually deficient, which predisposes them to a Class III pattern.
Lower facial height is usually increased in DS patients with an increase in the mandibular plane angle and a tendency to skeletal open bite.
Bimaxillary dental protrusion is evident in DS subjects with protruded and proclined upper and lower incisors. Hence, an acute nasolabial angle with protruded upper and lower lips can be expected in these subjects.
ACKNOWLEDGMENTS
The authors would like to thank the College of Dentistry Research Center and the Deanship of Scientific Research at King Saud University, Saudi Arabia for funding this research project (NF2257).
REFERENCES
- 1.Gorlin R, Cohen M, Hennekam R. Syndromes of the Head and Neck 4th ed. New York, NY: Oxford University Press; 2001. [Google Scholar]
- 2.Desai S. Down syndrome: a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:279–285. doi: 10.1016/s1079-2104(97)90343-7. [DOI] [PubMed] [Google Scholar]
- 3.Limbrock G, Fischer-Brandies H, Avalle C. Castillo-Morales' orofacial therapy: treatment of 67 children with Down syndrome. Dev Med Child Neurol. 1991;33:296–303. doi: 10.1111/j.1469-8749.1991.tb14880.x. [DOI] [PubMed] [Google Scholar]
- 4.Frostad W, Cleall J, Melosky L. The craniofacial complex in the trisomy 21 syndrome (Down's syndrome) Arch Oral Biol. 1971;16:707–722. doi: 10.1016/0003-9969(71)90116-6. [DOI] [PubMed] [Google Scholar]
- 5.Fink G, Madaus W, Walker G. A quantitative study of the face in Down's syndrome. Am J Orthod Dentofacial Orthop. 1975;67:540–553. doi: 10.1016/0002-9416(75)90299-7. [DOI] [PubMed] [Google Scholar]
- 6.Fischer-Brandies H, Schmid R, Fischer-Brandies E. Craniofacial development in patients with Down's syndrome from birth to 14 years of age. Eur J Orthod. 1986;8:35–42. doi: 10.1093/ejo/8.1.35. [DOI] [PubMed] [Google Scholar]
- 7.Fischer-Brandies H. Cephalometric comparison between children with and without Down's syndrome. Eur J Orthod. 1988;10:255–263. doi: 10.1093/ejo/10.3.255. [DOI] [PubMed] [Google Scholar]
- 8.Quintanilla J, Biedma B, Rodriguez M, Mora MT, Cunqueiro MM, Pazos MA. Cephalometries in children with Down's syndrome. Pediatr Radiol. 2002;32:635–643. doi: 10.1007/s00247-002-0703-x. [DOI] [PubMed] [Google Scholar]
- 9.Suri S, Tompson B, Cornfoot L. Cranial base, maxillary and mandibular morphology in Down syndrome. Angle Orthod. 2010;80:861–869. doi: 10.2319/111709-650.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Alió J, Lorenzo J, Iglesias M, Manso FJ, Ramírez EM. Longitudinal maxillary growth in Down syndrome patients. Angle Orthod. 2011;81:253–259. doi: 10.2319/040510-189.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Niazi M, Al-Mazyad A, Al-Husain M, et al. Down's syndrome in Saudi Arabia: incidence and cytogenetics. Hum Hered. 1995;45:65–69. doi: 10.1159/000154261. [DOI] [PubMed] [Google Scholar]
- 12.Al-Shawaf R, Al-Faleh W. Craniofacial characteristics in Saudi Down's syndrome. King Saud University J Dent Science. 2011(1–2);2:17–22. [Google Scholar]
- 13.Cohen JM. Comparing digital and conventional cephalometric radiographs. Am J Orthod Dentofacial Orthop. 2005;128:157–160. doi: 10.1016/j.ajodo.2005.03.017. [DOI] [PubMed] [Google Scholar]
- 14.McNamara JA., Jr A method of cephalometric evaluation. Am J Orthod Dentofacial Orthop. 1984;86:449–469. doi: 10.1016/s0002-9416(84)90352-x. [DOI] [PubMed] [Google Scholar]
- 15.Stiener C. Cephalometrics for you and me. Am J Orthod Dentofacial Orthop. 1953;39:729–755. [Google Scholar]
- 16.Ricketts R. Foundation for cephalometric communication. Am J Orthod. 1960;46:330–357. [Google Scholar]
- 17.Jarabak J, Fizzell J. Technique and Treatment With Lightwire Edgewise Appliance. St Louis, Mo: CV Mosby; 1972. [Google Scholar]
- 18.Holdaway R. A soft-tissue cephalometric analysis and its use in orthodontic treatment planning. Part I. Am J Orthod Dentofacial Orthop. 1983;84:1–28. doi: 10.1016/0002-9416(83)90144-6. [DOI] [PubMed] [Google Scholar]
- 19.Jacobson A, Jacobson R. Radiographic Cephalometry From Basic to 3D Imaging 2nd ed. Hanover Park, IL: Quintessence Publishing Co; 2006. [Google Scholar]
- 20.Kumar V, Cotran R, Robbins S. Basic Pathology 6th ed. Philadelphia, Pa: Saunders; 1997. [Google Scholar]
- 21.Horbelt C. Down syndrome: a review of common physical and oral characteristics. Gen Dent. 2007;55:399–402. [PubMed] [Google Scholar]
- 22.Jensen G, Cleall J, Yip A. Dentoalveolar morphology and developmental changes in Down's syndrome (trisomy 21) Am J Orthod. 1973;64:607–618. doi: 10.1016/0002-9416(73)90291-1. [DOI] [PubMed] [Google Scholar]
- 23.Ashok P, Boghani C. Dental manifestations of Down's syndrome. J Indian Dent Assoc. 1985;57:97–99. [PubMed] [Google Scholar]
- 24.Maclaurin ET, Shaw L, Foster TD. Dental caries and periodontal disease in children with Down's syndrome and other mentally handicapping conditions. J Paediatr Dent. 1985;1:15–19. [PubMed] [Google Scholar]
- 25.Cohen MM, Sr, Cohen MM., Jr The oral manifestations of trisomy G-1 (Down syndrome) Birth Defects Orig Artic Ser. 1971;7:241–251. [PubMed] [Google Scholar]
- 26.Gullikson J. Oral findings in children with Down's syndrome. ASDC J Dent Child. 1973;40:293–297. [PubMed] [Google Scholar]
- 27.Smith D. Health care management of adults with Down syndrome. Am Fam Physician. 2001;64:1031–1038. [PubMed] [Google Scholar]
- 28.Asokan S, Muthu M, Sivakumar N. Oral findings of Down syndrome children in Chennai city, India. Indian J Dent Res. 2008;19:230–235. doi: 10.4103/0970-9290.42956. [DOI] [PubMed] [Google Scholar]
- 29.Ferrario V, Dellavia C, Serrao G, Sforza C. Soft tissue facial angles in Down's syndrome subjects: a three-dimensional non-invasive study. The Eur J Orthod. 2005;27:355–362. doi: 10.1093/ejo/cji017. [DOI] [PubMed] [Google Scholar]
- 30.Sforza C, Elamin F, Rosati R, Lucchini MA, Tommasi DG, Ferrario VF. Three-dimensional assessment of nose and lip morphology in North Sudanese subjects with Down syndrome. Angle Orthod. 2011;81:107–114. doi: 10.2319/042510-222.1. [DOI] [PMC free article] [PubMed] [Google Scholar]