

Abstract
Objective:
To investigate the extent, experience, and trends associated with digital model use, as well as the advantages of using a particular study model type (digital or plaster) in postgraduate orthodontic programs in the United States and Canada.
Materials and Methods:
An electronic survey consisting of 14 questions was sent to 72 program directors or chairpersons of accredited orthodontic postgraduate programs in the United States and Canada.
Results:
Fifty-one responded for a 71% response rate. Sixty-five percent of the schools use plaster study models compared with 35% that use digital models. The most common advantages of plaster models were a three-dimensional feel and the ability for them to be mounted on an articulator. The most common advantages of digital models were the ease of storage and retrieval, and the residents' exposure to new technology. About one third of the plaster model users reported that they wanted to switch to digital models in the future, with 12% planning to do so within 1 year.
Conclusions:
Based on our study, 35% of accredited orthodontic postgraduate programs in the United States and Canada are using digital study models in most cases treated in their programs, and the trend is for increased digital model use in the future.
Keywords: Digital models, Study models, Postgraduate orthodontic programs
INTRODUCTION
Orthodontics is a progressive field that has embraced new technologies. Several orthodontic practices have made the leap to a paperless setup, and with the advent of digital models over a decade ago, there is a growing trend toward being plasterless.1
Orthodontic study models are the cornerstone of diagnosis and treatment planning. Additionally, study models are essential for didactic purposes, assessing progress, and documenting cases and research. Plaster study models are the gold standard in orthodontic diagnosis and treatment planning; however, digital models are gaining popularity due to their advantages over plaster in storing, retrieving, and sharing of information.2–6 Currently, digital models can be used successfully for orthodontic diagnosis and treatment planning cases.7,8 Advances in virtual study model systems have tremendously expanded the utility of digital models, and digital models can now be used for the production of laboratory appliances and computer-aided bracket placement as well as for virtual treatment simulations.4 However, lack of tactile input; increased expense; longer turnaround time; inability to mount them on an articulator; and the need for additional equipment, skill, and information technology support are some of the disadvantages that may discourage orthodontists from switching to digital models.9–11 Digital model use is not limited to private orthodontic offices but is currently being used in several orthodontic postgraduate programs.
Studies assessing the accuracy of measurements obtained from digital models such as tooth size,11–13 arch width,12–14 arch length,14 space analysis,2,15 overjet,11,13 overbite,11,13 midline discrepancy,13 Bolton tooth-size analysis,16,17 and molar and canine relationships13 have shown these models to be valid, clinically acceptable, and more quickly obtainable.17–20 Digital models made from alginate impressions21 as well as with intraoral scanners22 have been proven to be reliable and accurate. A systematic review of digital models by Fleming et al.18 compared tooth size, arch length, irregularity index, arch width, and crowding measurements in patients with and without malocclusions with measurements made using digital calipers on plaster models. There was a high degree of correlation between the two methods, and the results were clinically acceptable. Another systematic review by Luu et al.23 found intrarater assessments of selected linear measurements between virtual and plaster models to be valid and reliable.
Currently, the American Board of Orthodontics (ABO) accepts pretreatment, presurgical, and interim digital models between phase I and II orthodontic treatment in OrthoCAD (Cadent, Carlstadt, NJ) version 3.25 or later, emodel (Geodigm Corporation, Chanhassen, Minn), and SureSmile (Orametrix Inc, Richardson, Tex) formats for the clinical part of the ABO certification exam.24 However, only manually scored final posttreatment plaster casts are presently being accepted due to discrepancies found in measurements with digital models among the parameters of the ABO's objective grading system.9,25 With improvements in software accuracy and usage as well as adequate calibration of examiners, digital models may become an acceptable record for the ABO clinical exam in the future.26
To our knowledge, no study has investigated the type of study models currently being used in postgraduate orthodontic programs in the United States and Canada. Therefore, the aim of our study was to investigate (1) the extent of digital model use and the experience of using digital models for diagnosis and treatment planning and as a didactic medium in postgraduate orthodontic programs in the United States and Canada, (2) the advantages of using one type (digital or plaster) of study model over the other, and (3) trends in the type of study model that will be used in the future in postgraduate programs in the United States and Canada.
MATERIALS AND METHODS
After receiving approval from the AT Still University Institutional Review Board, the survey instrument was submitted to the American Association of Orthodontics (AAO) Survey Review Committee of the AAO Board of Trustees. An electronic survey (SurveyMonkey, Portland, Ore) was administered by the AAO's “Partners in Research Program” after the board had approved the survey. An anonymous and voluntary survey was sent by a Web link, which was e-mailed to program directors or chairpersons of each of the 72 accredited US and Canadian postgraduate orthodontic programs listed on the AAO website. To improve the response rate, 1 month after the AAO had sent out the initial e-mail, two follow-up reminder e-mails were sent to all the programs requesting participation if they had not already taken the survey.
The survey, consisting of 14 questions, was divided between digital and plaster model questions using a logical sequence format. The questions were presented in a multiple-choice format with some questions having the option of entering additional comments. The data were analyzed and compiled using Excel (Microsoft, Redmond, Wash). Additionally, based on the results of the survey, a flow diagram predicting the percentage of plaster users switching to digital in less than 1 year, 2–3 years, and more than 3 years was calculated using the following mathematical equation: projection equation = [.65(proportion of plaster users)][.37(proportion switching to digital)][proportion in time interval]100.
RESULTS
Of the 72 program directors or chairpersons, 55 opened the survey and 51 completed it, translating to a 71% response rate. The results of the survey indicate that 33 (65%) of US and Canadian postgraduate orthodontic programs are currently using plaster models, while 18 (35%) programs use digital models in more than half of the orthodontic cases treated at their school. The data for the plaster and digital models were organized in flow diagrams illustrating the survey questions and answer options as well as the corresponding results (Figures 1 and 2).
Figure 1.
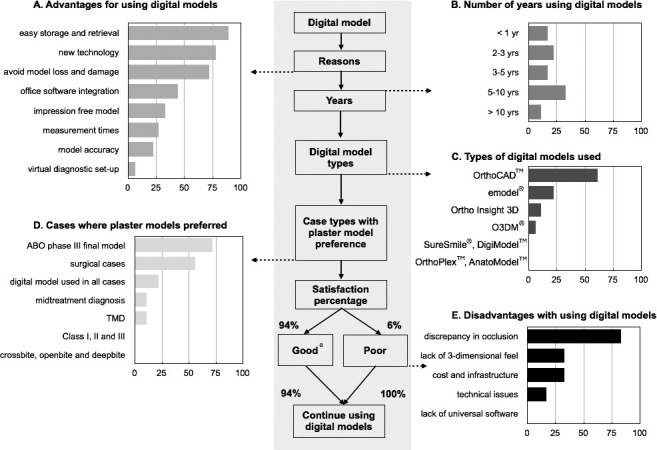
Digital model flow and breakup of results associated with survey question (unit: %). a Good covers excellent, good, and satisfactory.
Figure 2.
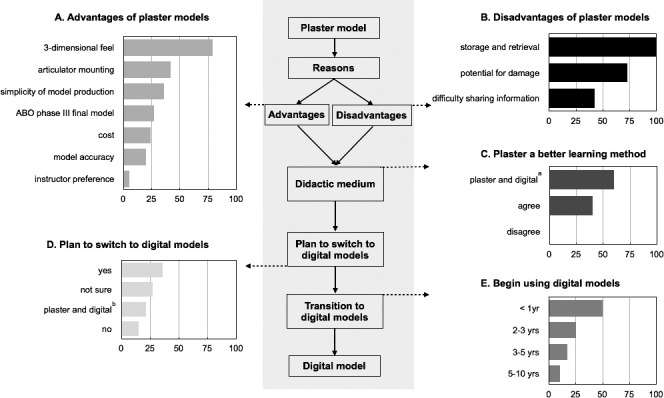
Plaster model flow and breakup of results associated with survey question (unit: %).
a Plaster and digital models are both equally good learning methods. b Some programs use both digital and plaster models, with plaster being the predominant type.
Digital Models
Based on the results of our survey, ease of storage and retrieval (89%, n = 16), exposure to new technology (78%, n = 14), and avoidance of loss and damage to plaster models (72%, n = 13) were the most common reasons for using digital models by educational institutions (Figure 1A). Forty-four percent (n = 8) of the programs reported using digital models for more than 5 years (Figure 1B). OrthoCAD was reported to be the most commonly used digital model software (61%, n = 11), followed emodel used by 22% (n = 4) (Figure 1C).
Digital model users were questioned about clinical situations where plaster models might be preferred over digital models. Plaster models were preferred by 72% (n = 13) for board cases and 56% (n = 10) for surgical cases (Figure 1D). However, 22% (n = 4) of the respondents reported the use of digital models for diagnosing and treating all case types with no preference for plaster models.
Almost all of the current digital model users (94%, n = 17) reported excellent, good, or satisfactory experience with digital models for treating orthodontic cases in their residency programs, while only one (6%) digital model user reported a poor experience. The most commonly reported disadvantage of the digital models was an inconsistency between mounted and correct occlusion (83%, n = 5) (Figure 1E). Of the digital users with excellent, good, and satisfactory experience, 94% (n = 16) reported that they would continue to use digital models in the future, and 100% (n = 1) the digital model user with poor experiences expressed intent to continue using the same medium (Figure 1).
Plaster Models
The plaster model's three-dimensional feel (79%, n = 26), followed by the ability to mount plaster models on an articulator (42%, n = 14), and the simplicity of model production (36%, n = 12) were the most common reasons for continuing to use plaster models (Figure 2A). However, some of the main disadvantages reported with plaster models were the difficulty with storage and retrieval (100%, n = 33), plaster's potential for damage (73%, n = 24), and inconvenience in information sharing (42%, n = 14) (Figure 2B). Of the respondents of the plaster group, 39% (n = 13) agreed plaster was a better learning tool in educational institutions; however 58% (n = 19) reported that both digital and plaster models have benefits as a medium of education (Figure 2C).
Trends
The plaster group was asked if they had plans to switch to digital models for more than half the cases in the future. Of the respondents, 21% (n = 7) reported that they wanted to use both plaster and digital models, but predominantly plaster in more than half the cases and to use digital models on a limited basis (Figure 2D). However, 37% (n = 12) of plaster users had plans to switch to digital models in the future, of which 50% (n = 6) had plans to switch in 1 year or less (Figure 2E).
DISCUSSION
According to our survey results, 65% of schools are currently using plaster models for most of their orthodontic cases. However, a substantial percentage of these programs reported that they would want to switch to digital for the majority of their cases. Considering the results of the projection flow chart, we predict a progressive increase in the number of digital users by 12% within 1 year, 18% in 2 to 3 years, and 24% in more than 3 years (Figure 3).
Figure 3.
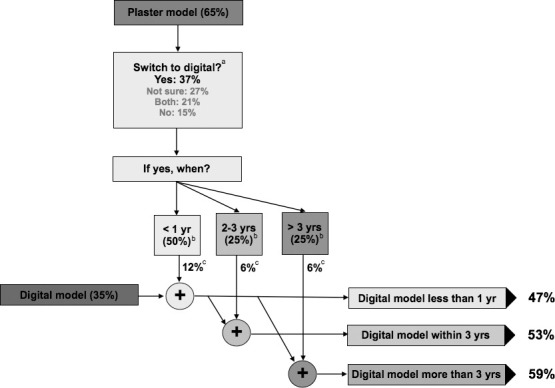
Projection of digital model users at orthodontic programs over the next 1–3 years. a Survey results from Figure 2D. b Survey results from Figure 2E. c Plaster to digital projection equation = [.65(proportion of plaster users)][.37(proportion switching to digital)][proportion in time interval]100. For example, proportion of plaster users switching to digital in less than 1 year, 0.65 × 0.37 × 0.50 = 0.12 × 100 = 12%.
According to the results of our study, the advantages of digital models and the possible reasons for a future increase in digital models are consistent with the current literature available on study models.27 Also, as per our survey results, it was interesting to note that despite the poor experience of one user (6%) with digital models, the program wants to continue using digital models because of their advantages (Figure 1A). Our findings concur with the trend reports in the study by Keim et al.28 that reported the use of digital records is on the rise from 11.0% in 1981 to 58.9% in 2011. Another nationwide survey by Keim et al.1 reported a rapid increase in the use of digital models for pretreatment records from 6.6% to 18.0% from 2002 to 2008. Also, according to the same study, there was an increase in the digital model usage for posttreatment records from 3.2% to 8.9%; however, digital model usage for posttreatment models was much smaller compared to the pretreatment usage. This finding is consistent with the main advantage of plaster models, being that the ABO is currently only accepting plaster posttreatment records for the board certification process (Figure 2A). The introduction of the initial board certification process by the ABO gives recent orthodontic residents the opportunity to submit cases completed during residency,29 and this may have a significant influence on the study model selection process in residency programs. It would be interesting to do a follow-up survey to observe the change in trends of digital model usage after the ABO starts accepting posttreatment digital model records.
Results from several studies measuring tooth size, arch width, space analysis, Bolton's discrepancy, overjet, overbite, and midline discrepancy suggest that digital models are valid and reliable.2,11–17 Also, a study by Bootvong et al.13 reported a substantial agreement between the canine and molar relationships as compared to plaster models. However, the results of our survey found that the majority of the schools predominantly using digital models reported that there was a discrepancy between mounted and correct occlusion (Figure 1E). Further investigation to evaluate the accuracy of the occlusion of digital models may be needed.
In our study, we wanted to investigate the perceptions of program directors or chairpersons on the use of digital models as an educational tool compared to plaster models. Some program directors or chairpersons (39%) reported that plaster models might be a better learning tool; however, 58% of the program directors or chairpersons reported that both types of study models were equally good and had their benefits. OrthoCAD and emodel are two of three digital models currently being accepted by the ABO as pretreatment records for the certification process; and from our study, OrthoCAD was reported to be the most commonly used digital model system followed by emodel. Overall, findings from our study suggest that a majority of the schools are using ABO certification standards in making decisions on the type of digital models to use in their programs.
Similar to most survey-based studies, selection bias was a limitation of our voluntary survey-based research study. The title of the survey instrument was “Digital Model Survey,” and some respondents not using digital models in their respective programs may have chosen not to participate in the survey, whereas there may have been an increased participation of respondents using predominantly digital models to share their views and experiences. With a 71% response rate, the results closely represent the target survey group. However, a higher response rate may more completely represent the current digital model usage in the residency programs in the United States and Canada. Furthermore, including the opinions of orthodontic residents and private practice clinicians, as well as including questions on age, sex, and educational background in future digital model research may provide more insight into the utility of the digital medium in orthodontics. Evaluation and comparison of accuracy, cost effectiveness, and turnaround time between various digital model software systems available today may be another area of future research.
With the introduction of digital models over a decade ago, several programs are currently using digital models. Currently, there are no guidelines for the type of study models that are preferable, and it may be necessary to develop guidelines backed by sound scientific evidence to guide schools in decisions regarding the type of study models to be used in postgraduate residency programs.
CONCLUSIONS
A majority of orthodontic programs are currently using plaster study models, with the main advantages being their three-dimensional feel and the ability to be mounted on an articulator.
Programs using digital models reported the main advantages being favorable experiences during diagnosing and treatment planning, ease of storage and retrieval, and exposure to new technology.
The results of the survey suggest a trend toward increased use of digital models in the future.
ACKNOWLEDGMENT
We thank Dr James D. Seward for assistance with the statistical analysis.
REFERENCES
- 1.Keim RG, Gottlieb EL, Nelson AH. Vogels DS 3rd. 2008 JCO study of orthodontic diagnosis and treatment procedures. Part 1: results and trends. J Clin Orthod. 2008;42:625–640. [PubMed] [Google Scholar]
- 2.Goonewardene RW, Goonewardene MS, Razza JM, Murray K. Accuracy and validity of space analysis and irregularity index measurements using digital models. Aust Orthod J. 2008;24:83–90. [PubMed] [Google Scholar]
- 3.Dalstra M, Melsen B. From alginate impressions to digital virtual models: accuracy and reproducibility. J Orthod. 2009;36:36–41. doi: 10.1179/14653120722905. [DOI] [PubMed] [Google Scholar]
- 4.Favero L, Terrazzani C, Favero V, Stellini E, Cocilovo F. Virtual study models: a comparison of modular application systems. Prog Orthod. 2009;10:16–25. [PubMed] [Google Scholar]
- 5.Peluso M, Josell S, Levine S, Lorei B. Digital models: an introduction. Semin Orthod. 2004;10:226–238. [Google Scholar]
- 6.Bell A, Ayoub AF, Siebert P. Assessment of the accuracy of a three-dimensional imaging system for archiving dental study models. J Orthod. 2003;30:219–223. doi: 10.1093/ortho/30.3.219. [DOI] [PubMed] [Google Scholar]
- 7.Rheude B, Sadowsky PL, Ferriera A, Jacobson A. An evaluation of the use of digital study models in orthodontic diagnosis and treatment planning. Angle Orthod. 2005;75:300–304. doi: 10.1043/0003-3219(2005)75[300:AEOTUO]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Whetten JL, Williamson PC, Heo G, Varnhagen C, Major PW. Variations in orthodontic treatment planning decisions of Class II patients between virtual 3-dimensional models and traditional plaster study models. Am J Orthod Dentofacial Orthop. 2006;130:485–491. doi: 10.1016/j.ajodo.2005.02.022. [DOI] [PubMed] [Google Scholar]
- 9.Okunami TR, Kusnoto B, BeGole E, Evans CA, Sadowsky C, Fadavi S. Assessing the American Board of Orthodontics objective grading system: digital vs plaster dental casts. Am J Orthod Dentofacial Orthop. 2007;131:51–56. doi: 10.1016/j.ajodo.2005.04.042. [DOI] [PubMed] [Google Scholar]
- 10.Mayers M, Firestone AR, Rashid R, Vig KW. Comparison of peer assessment rating (PAR) index scores of plaster and computer-based digital models. Am J Orthod Dentofacial Orthop. 2005;128:431–434. doi: 10.1016/j.ajodo.2004.04.035. [DOI] [PubMed] [Google Scholar]
- 11.Santoro M, Galkin S, Teredesai M, Nicolay OF, Cangialosi TJ. Comparison of measurements made on digital and plaster models. Am J Orthod Dentofacial Orthop. 2003;124:101–105. doi: 10.1016/s0889-5406(03)00152-5. [DOI] [PubMed] [Google Scholar]
- 12.Zilberman O, Huggare JA, Parikakis KA. Evaluation of the validity of tooth size and arch width measurements using conventional and three-dimensional virtual orthodontic models. Angle Orthod. 2003;73:301–306. doi: 10.1043/0003-3219(2003)073<0301:EOTVOT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Bootvong K, Liu Z, McGrath C, et al. et al. Virtual model analysis as an alternative approach to plaster model analysis: reliability and validity. Eur J Orthod. 2010;32:589–595. doi: 10.1093/ejo/cjp159. [DOI] [PubMed] [Google Scholar]
- 14.Sousa MV, Vasconcelos EC, Janson G, Garib D, Pinzan A. Accuracy and reproducibility of 3-dimensional digital model measurements. Am J Orthod Dentofacial Orthop. 2012;142:269–273. doi: 10.1016/j.ajodo.2011.12.028. [DOI] [PubMed] [Google Scholar]
- 15.Leifert MF, Leifert MM, Efstratiadis SS, Cangialosi TJ. Comparison of space analysis evaluations with digital models and plaster dental casts. Am J Orthod Dentofacial Orthop. 2009;136:161–164. doi: 10.1016/j.ajodo.2008.11.019. [DOI] [PubMed] [Google Scholar]
- 16.Tomassetti JJ, Taloumis LJ, Denny JM, Fischer JR., Jr A comparison of 3 computerized Bolton tooth-size analyses with a commonly used method. Angle Orthod. 2001;71:351–357. doi: 10.1043/0003-3219(2001)071<0351:ACOCBT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 17.Mullen SR, Martin CA, Ngan P, Gladwin M. Accuracy of space analysis with emodels and plaster models. Am J Orthod Dentofacial Orthop. 2007;132:346–352. doi: 10.1016/j.ajodo.2005.08.044. [DOI] [PubMed] [Google Scholar]
- 18.Fleming PS, Marinho V, Johal A. Orthodontic measurements on digital study models compared with plaster models: a systematic review. Orthod Craniofac Res. 2011;14:1–16. doi: 10.1111/j.1601-6343.2010.01503.x. [DOI] [PubMed] [Google Scholar]
- 19.Gracco A, Buranello M, Cozzani M, Siciliani G. Digital and plaster models: a comparison of measurements and times. Prog Orthod. 2007;8:252–259. [PubMed] [Google Scholar]
- 20.Quimby ML, Vig KW, Rashid RG, Firestone AR. The accuracy and reliability of measurements made on computer-based digital models. Angle Orthod. 2004;74:298–303. doi: 10.1043/0003-3219(2004)074<0298:TAAROM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 21.Dalstra M, Melsen B. From alginate impressions to digital virtual models: accuracy and reproducibility. J Orthod. 2009;36:36–41. doi: 10.1179/14653120722905. [DOI] [PubMed] [Google Scholar]
- 22.Cuperus AM, Harms MC, Rangel FA, Bronkhorst EM, Schols JG, Breuning KH. Dental models made with an intraoral scanner: a validation study. Am J Orthod Dentofacial Orthop. 2012;142:308–313. doi: 10.1016/j.ajodo.2012.03.031. [DOI] [PubMed] [Google Scholar]
- 23.Luu NS, Nikolcheva LG, Retrouvey JM, et al. Linear measurements using virtual study models. Angle Orthod. 2012;82:1098–1106. doi: 10.2319/110311-681.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.The American Board of Orthodontics. Case Preparation. St Louis: The American Board of Orthodontics; Available at: http://www.americanboardortho.com/professionals/clinicalexam/casereportpresentation/preparation/casts.aspx Accessed December 31, 2012. [Google Scholar]
- 25.Hildebrand JC, Palomo JM, Palomo L, Sivik M, Hans M. Evaluation of a software program for applying the American Board of Orthodontics objective grading system to digital casts. Am J Orthod Dentofacial Orthop. 2008;133:283–289. doi: 10.1016/j.ajodo.2006.03.035. [DOI] [PubMed] [Google Scholar]
- 26.Costalos PA, Sarraf K, Cangialosi TJ, Efstratiadis S. Evaluation of the accuracy of digital model analysis for the American Board of Orthodontics objective grading system for dental casts. Am J Orthod Dentofacial Orthop. 2005;128:624–629. doi: 10.1016/j.ajodo.2004.08.017. [DOI] [PubMed] [Google Scholar]
- 27.Stevens DR, Flores-Mir C, Nebbe B, Raboud DW, Heo G, Major PW. Validity, reliability, and reproducibility of plaster vs digital study models: comparison of peer assessment rating and Bolton analysis and their constituent measurements. Am J Orthod Dentofacial Orthop. 2006;129:794–803. doi: 10.1016/j.ajodo.2004.08.023. [DOI] [PubMed] [Google Scholar]
- 28.Keim RG, Gottlieb EL, Nelson AH. Vogels DS 3rd. 2011 JCO orthodontic practice study. Part 1: trends. J Clin Orthod. 2011;45:535–544. [PubMed] [Google Scholar]
- 29.The American Board of Orthodontics. Examination Process. Available at: http://www.americanboardortho.com/professionals/clinicalexam/examprocess2.aspx - 1. Accessed December 31, 2012. [Google Scholar]