

Abstract
Objective:
To evaluate the periodontal health and tooth vitality of palatally impacted and buccal ectopic maxillary canines after completion of orthodontic treatment.
Materials and Methods:
Fifteen patients who had unilateral, palatally impacted canines and 15 patients who had unilateral, buccal ectopic canines comprised the subjects of the study. Clinical and radiographic data was collected by recalling the patients in both groups after a mean period of 3.82 ± 1.54 years following completion of their orthodontic treatment. In both groups, the contralateral, normally placed canines served as controls.
Results:
Palatally impacted canines had greater pocket depths, higher gingival levels, higher electric pulp testing scores, and reduced bone levels compared to their contralaterals. Buccal ectopic canines had increased plaque and gingival bleeding index, greater pocket depths, reduced attached gingival width, higher gingival levels, increased clinical crown lengths, and higher electric pulp testing scores compared to their contralaterals. Buccal ectopic canines had lower electric pulp testing scores and higher bone levels compared to palatally impacted canines.
Conclusion:
All ectopic canines had increased plaque and gingival bleeding index, greater pocket depths, reduced attached gingival width, higher gingival levels, increased crown lengths, higher electric pulp testing scores, and reduced bone levels compared to their contralaterals.
Keywords: Periodontal health, Tooth vitality, Long term, Ectopic canines, Palatally impacted canines
INTRODUCTION
The prevalence of impacted maxillary canines is reported to vary between 0.9% and 2.2%, and in most cases, the impacted canines are ectopically positioned.1 Eighty-five percent of ectopic canines are located palatal to the dental arch.2
The proper localization of the impacted tooth plays a crucial role in determining the feasibility of, as well as the proper access for, the surgical approach and the proper direction for the application of orthodontic forces.3,4
The two techniques for surgically exposing and bringing the palatally impacted canine into occlusion are the open approach (OA) and the closed approach (CA). The advantages of the OA include the orthodontist's ability to observe the impacted tooth and have a continuing access to the impacted tooth as it is moved to its normal position in the dental arch,5,6 as well as faster eruption.5 However, this method is often associated with multiple periodontal problems, such as gingival recession,5,7–9 bone loss,5 decreased width of keratinized gingiva,9,10 delayed periodontal healing,11 and gingival inflamation.9 Periodontal health may be also compromised when the CA is performed.12,13
Labial impaction of the maxillary canine is less frequent than palatal impaction and is often caused by insufficient arch length. The canine is often positioned high in the alveolar bone and erupts through the alveolar mucosa. When detected early, prevention may be achieved by the extraction of the deciduous canine.14
Earlier methods of uncovering impacted canines advocated radical bone removal to expose the crown of the impacted tooth so as to remove all bony obstacles and to provide an easier path for tooth movement. McDonald and Yap15 evaluated the relationship between the amount of bone removed during surgical exposure and the subsequent bone loss around the impacted tooth. They found that the more bone removed initially, the greater the bone loss after orthodontic treatment. Kohavi et al.16 concluded that extensive bone removal that might inadvertently involve the cementoenamel junction (CEJ) should be avoided. Patients treated with more extensive bone removal had on average 5.4% less bony support than those patients treated with less extensive bone removal.
Since during the treatment of impacted canines both surgical and orthodontic procedures are used, tooth vitality could be influenced as well.1,17
In our retrospective study we assessed the periodontal status and tooth vitality of palatally impacted canine cases that were exposed with CA and ectopic buccal canines that were treated with conventional orthodontic techniques, and we compared them with the contralateral canines that served as control teeth and also compared them with each other. By determining to what extent we had been successful in preserving the periodontal health of our treated ectopic canine cases, we will have a chance to evaluate our treatment strategies and consider some modifications if needed.
MATERIALS AND METHODS
In order to be able to include a sufficient number of patients in the study groups, we examined the archive files of two separate orthodontic departments in İstanbul. Selection criteria were as follows: presence of unilateral palatally impacted or buccal ectopic canines at the beginning of the treatment, having received orthodontic treatment with fixed appliances, active treatment completed at least 6 months ago, good oral hygiene, and no systemic disease. A total of 52 patients who met these criteria were identified. Thirty of these 52 patients, 15 patients who had unilateral palatally impacted canines and 15 patients who had unilateral buccal ectopic canines at the beginning of their orthodontic treatment, agreed to come to the recall appointments. Twenty-one of them were girls and nine of them were boys. Mean age of the patients at the beginning of the treatment was 11.43 ± 1.45 years. Mean treatment duration was found to be 3.71 ± 1.32 years (3.52 ± 1.43 years for buccal, 3.90 ± 1.21 years for palatal canines). Mean recall period was 3.82 ± 1.54 years.
In the first group of patients, palatally impacted canines had been exposed with a CA technique with minimal bone removal in the Departments of Dental Surgery of Marmara and Yeditepe Universities. Attachments had been bonded to the impacted canines at the time of surgical exposure.
In the second group of patients, who had buccal ectopic maxillary canines, orthodontic treatment for alignment of these teeth was completed by conventional orthodontic techniques, with or without the extraction of permanent teeth. In two patients from this group, electro surgery was performed for the canine exposure.
Patients in both groups were recalled for collection of the clinical data. The periodontal status of the canines was evaluated clinically and radiographically. In both groups, the contralateral, normally placed canines served as control. The study was approved by the Ethical Committee of the Medical Faculty of Marmara University, İstanbul, Turkey.
Clinical Evaluation
Periodontal examination
The following measurements of the involved canines were made to evaluate their periodontal health status:
Plaque index (PI): The mesial, distal, buccal, and palatal surfaces were scored on a scale of 0 to 3, according to the method described by Silness and Löe.18
Gingival bleeding index (GBI): The same surfaces were scored as for the plaque index on a scale of 0 to 3, according to the method of Löe and Silness.19
Pocket depth (PD): The depths of the mesial, distal, buccal, and palatal gingival pockets were measured as the distance from the free gingival margin to the bottom of the pocket with a standard periodontal probe.
Attached gingival width (AGW): The width of attached gingiva was measured by subtracting the pocket depth from the distance between the gingival margin and the mucogingival junction.
Gingival level (GL): Gingival level on the buccal and palatal aspects was measured with a divider from the most apical extent of the CEJ to the most apical extent of the gingival margin.
Crown length (CL): Clinical crown length was measured as the distance between the canine cusp tip and the most apical extent of the gingival margin.
Electric pulp testing score (EPTS)
Tooth vitality was assessed with Parkell Pulp Vitality Tester (Parkell Inc, Edgwood, NY), grading from 1 to 10 (10 being nonvital).
Radiographic Evaluation
For measurements of bone level and root resorption, two periapical radiographs were obtained using a long-cone paralleling technique. All radiographs were scanned. The measurements on these images were made using Dental Studio NX 2006 Version 6.0 software (Nemotec, Madrid, Spain). Bone level was measured by calipers as the distance from the CEJ to the alveolar crest on both the mesial and distal sides (Figure 1). Root length was measured as the distance from a line connecting the mesial and distal CEJ to the root apex using a ruler (Figure 2).
Figure 1.
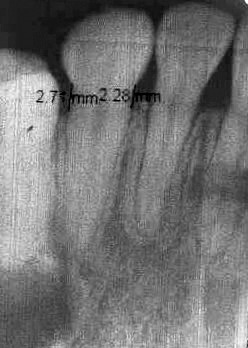
Bone level.
Figure 2.
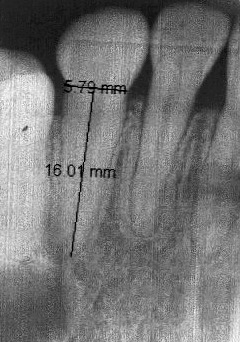
Root length.
Reliability of the Method
In order to determine operator reliability and reproducibility, all the bone-level and root-length measurements of 60 teeth were repeated 2 weeks later by the same observer. Correlation between these two sets of measurements was assessed with Pearson correlation analysis.
Statistical Method
The paired-samples t-test was used to compare parametric data (pocket depth, attached gingival width, gingival level, crown length, bone level, and root length), and the Wilcoxon signed rank test was applied to compare nonparametric data (plaque index, gingival bleeding index, and electric pulp testing score [EPTS]) between the ectopic canines and their contralateral controls. To make comparisons between impacted palatal and buccal ectopic canines, the Mann-Whitney U-test was used for nonparametric data, and Student's t-test was used for parametric data. Level of significance was selected as P < .05 for all tests. All statistical tests were made using SPSS 12.0 software (SPSS Inc, Chicago, Ill).
RESULTS
Comparison showed statistically significant differences in plaque index and gingival bleeding index scores, pocket depth, attached gingival width, gingival level, crown length, EPTS, and bone level.
Palatally impacted canines had greater pocket depths (P < .01), higher gingival levels (P < .01), higher EPTS (P < .01), and reduced bone levels (P < .01) compared to their contralaterals (Table 1).
Table 1.
Comparison of the Palatally Impacted Canines and Their Contralateral After Orthodontic Treatmenta

Buccal ectopic canines had increased plaque index (P < .01), increased gingival bleeding index (P < .01), greater PD (P < .05), reduced attached gingival width (P < .001), higher gingival levels (P < .001), increased crown lengths (P < .001), and higher EPTS (P < .05) compared to their contralaterals. Bone level was reduced as well, but this reduction was not statistically significant (Table 2).
Table 2.
Comparison of the Buccal Ectopic Canines and Their Contralaterals After Orthodontic Treatmenta

Buccal ectopic canines had lower EPTS (P < .05) and higher bone levels (P < .01) compared to palatally impacted canines (Table 3).
Table 3.
Comparison of the Buccal Ectopic and Palatally Impacted Canines After Orthodontic Treatmenta

The correlation between the first and second measurements, which was done in order to evaluate the method error, was established to be high. Findings suggest that bone level and root length measurements are reliable (r = 1.000; P = .01).
DISCUSSION
The orthodontic treatment aims at moving the corresponding tooth into its correct position in the dental arch without causing periodontal problems and tooth vitality loss. However, the periodontal condition and sensitivity of treated impacted canines were reported to be affected by the surgical and orthodontic procedures used. There are studies6,10,13,16 that have previously illustrated the potential periodontal problems associated with surgical exposure and orthodontic alignment of ectopic canines. On the other hand, it must be remembered that orthodontic treatment itself carries a risk of tooth morbidity.20 In both situations, the role of increased difficulty in maintaining adequate oral hygiene during appliance therapy may be significant.
When we look at the previous studies in the literature, we see that there is conflicting evidence as to how the periodontal condition and vitality of the impacted canines were affected by treatment procedures. Woloshyn et al.12 observed greater pocket depths and significantly lower crestal bone height in the impacted canines compared to contralateral controls. On the other hand, Crescini et al.21 found no attachment loss, no recession, and no significant differences in keratinized tissue width in a follow-up examination of eight cases with impacted canines when compared to the contralateral canines. Vermette et al.22 observed reduced width of attached gingiva and reduced bone levels of treated buccal ectopic canines compared to their contralaterals. On the other hand, Tegsjö et al.9 found no significant differences in the periodontal status between treated impacted canines and the nontreated controls.
The aim of our study was to assess the periodontal status and vitality of the palatally impacted and buccal ectopic canines after orthodontic treatment and compare them with the contralateral canines that served as control teeth and also compare them with each other.
In the first group of patients, palatally impacted canines had been exposed using a CA technique with minimal bone removal. It can be said that the periodontal condition of treated impacted canines is almost always affected, independent of the surgical or orthodontic procedures used. However, it seems that less damaging effects on the periodontium should be anticipated when using the CA technique.5–9
In the second group of patients, who had buccal ectopic maxillary canines, orthodontic treatment for alignment of these teeth was completed by conventional orthodontic techniques. After enough space was created for ectopic canines by the clinician, the teeth erupted spontaneously except in two cases. Since the position of these two canines was coronal to the mucogingival junction, the gingival tissue around the crowns was removed with electro surgery in order to place a bracket; the remainder of the group was treated without any surgical procedure. In the patients who had electro surgery, no bone was removed around the crown.
In this study, six periodontal parameters were used. These were chosen from among the most commonly used periodontal parameters so as to cover all dental and gingival landmarks. Many of the authors used two, three, or five of them.1,17,23
In our study, we measured the bone loss on periapical radiographs. In the literature, many of the authors used these films as well, such as Kokich and Mathews,24 Kohavi et al.,16 Woloshyn et al.,12 Hansson and Rindler,25 and Becker.26
We compared buccal ectopic and palatally impacted canines with their contralateral controls.
We found that palatally impacted canines had greater pocket depth, higher gingival levels, higher EPTS, and reduced bone levels compared to their contralaterals.
The results of Burden et al.27 in their study group of 18 patients with unilateral palatal impaction of a maxillary canine were greater pocket depth and reduced bone levels, which are similar to our results. A good gingival and periodontal status with slight differences between treated and untreated sides was reported by Hansson and Rindler,25 though increased pocket depth and lower marginal bone level were registered.
Since our study was a retrospective study, it was not possible to obtain sound information on how much bone was removed during the surgical procedure. Of course the volume of bone removal is a very important variable influencing long-term periodontal health. The increases in the pocket depth and gingival level and decrease in the bone level of the palatally impacted canines after treatment may be related to the more extensive bone removal during the closed flap surgical approach.
Another finding of the present study was that although surgical intervention was performed in only two of the buccal ectopic canines, the mean plaque index and gingival bleeding index scores, pocket depth and crown level increased compared to their contralaterals. Reduced attached gingival width with higher gingival levels and higher EPTS were also among the findings in this group.
According to Kohavi et al.,10 attached gingival width was significantly reduced following the alignment of buccal ectopic maxillary canines, which is in parallel with our results. The reasons for this deterioration in periodontal health could not be elucidated; however, we can speculate that it is related to the emergence of the buccal ectopic canines through the alveolar mucosa and the insufficient buccal bone support.
Comparison of the buccal ectopic and palatally impacted canines revealed that buccal ectopic canines had lower EPTS and higher bone levels compared to palatally impacted canines. The shorter treatment duration of buccal ectopic canines and the fact that there was no need for bone removal during (except in two cases) their treatment period might have accounted for this difference. In the literature there are only a few studies about the vitality of impacted maxillary canines after active orthodontic treatment. Blair et al.17 reported on the tooth vitality loss from the treatment of palatally impacted maxillary canines. In another study, D'Amico et al.1 followed up on a total of 61 children who had received treatment for impacted maxillary canines on average 3.5 years earlier in order to evaluate the long-term results of the treatments. As a result they found that the vital response of two canines was reduced. Thus, both orthodontic and surgical procedures can influence sensitivity of the treated impacted teeth. In our study, the long treatment duration, in addition to the orthodontic forces applied to these teeth, might have influenced tooth vitality.
The findings of this study should be interpreted with caution due to the following limitations: the sample size was small, and the severity of the ectopia and the distance the tooth has to travel until it reaches its final place were not taken into account. They both may have an impact on periodontal health. On the other hand, it would not be wrong to say that the changes observed in the periodontal status and vitality of the ectopic teeth, though statistically significant, did not reach clinical significance.
CONCLUSIONS
The alterations in the periodontal health of palatally ectopic canines, compared to their contralaterals, were in the form of alveolar bone loss, increased probing depth, higher gingival levels, and higher EPTS.
The periodontal health parameters of buccal ectopic canines pointed to a situation of gingival deficiency. They had increased plaque index and gingival bleeding index, greater pocket depths, reduced attached gingival width, higher gingival levels, increased crown lengths, and higher EPTS compared to their contralaterals.
Buccal ectopic canines had lower EPTS and higher bone levels compared to the palatally impacted canines.
REFERENCES
- 1.D'Amico RM, Bjerklin K, Kurol J, Falahat B. Long-term results of orthodontic treatment of impacted maxillary canines. Angle Orthod. 2003;73:231–238. doi: 10.1043/0003-3219(2003)073<0231:LROOTO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Ericson S, Kurol J. Radiographic examination of ectopically erupting maxillary canines. Am J Orthod Dentofacial Orthop. 1987;91:483–492. doi: 10.1016/0889-5406(87)90005-9. [DOI] [PubMed] [Google Scholar]
- 3.Bishara SE. Impacted maxillary canines: a review. Am J Orthod Dentofacial Orthop. 1992;101:159–171. doi: 10.1016/0889-5406(92)70008-X. [DOI] [PubMed] [Google Scholar]
- 4.Ericson S, Kurol PJ. Resorption of incisors after ectopic eruption of maxillary canines: a CT study. Angle Orthod. 2000;70:415–423. doi: 10.1043/0003-3219(2000)070<0415:ROIAEE>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 5.Vanarsdall RL, Corn H. Soft-tissue management of labially positioned unerupted teeth. Am J Orthod. 1977;72:53–64. doi: 10.1016/0002-9416(77)90124-5. [DOI] [PubMed] [Google Scholar]
- 6.Wisth PJ, Norderval K, Boe OE. Comparison of two surgical methods in combined surgical-orthodontic correction of impacted maxillary canines. Acta Odontol Scand. 1976;34:52–57. doi: 10.3109/00016357609026558. [DOI] [PubMed] [Google Scholar]
- 7.Boyd RL. Clinical assessment of injuries in orthodontic movement of impacted teeth. II. Surgical recommendations. Am J Orthod. 1984;86:407–418. doi: 10.1016/s0002-9416(84)90034-4. [DOI] [PubMed] [Google Scholar]
- 8.Melkos AB, Papadopoulos MA. Periodontal aspects associated with the surgical and orthodontic treatment of impacted canines. Hellenic Orthod Rev. 2004;7:9–24. [Google Scholar]
- 9.Tegsjö U, Valerius-Olsson H, Andersson L. Periodontal conditions following surgical exposure of unerupted maxillary canines—a long term follow-up study of two surgical techniques. Swed Dent J. 1984;8:257–263. [PubMed] [Google Scholar]
- 10.Kohavi D, Zilberman Y, Becker A. Periodontal status following the alignment of buccally ectopic maxillary canine teeth. Am J Orthod. 1984;85:78–82. doi: 10.1016/0002-9416(84)90125-8. [DOI] [PubMed] [Google Scholar]
- 11.Becker A, Shpack N, Shteyer A. Attachment bonding to impacted teeth at the time of surgical exposure. Eur J Orthod. 1996;18:457–463. doi: 10.1093/ejo/18.5.457. [DOI] [PubMed] [Google Scholar]
- 12.Woloshyn H, Årtun J, Kennedy DB, Joondeph DR. Pulpal and periodontal reactions to orthodontic alignment of palatally impacted canines. Angle Orthod. 1994;64:257–264. doi: 10.1043/0003-3219(1994)064<0257:PAPRTO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.Becker A, Kohavi D, Zilberman Y. Periodontal status following the alignment of palatally impacted canine teeth. Am J Orthod. 1983;84:332–336. doi: 10.1016/s0002-9416(83)90349-4. [DOI] [PubMed] [Google Scholar]
- 14.Power SM, Short MB. An investigation into the response of palatally displaced canines to the removal of deciduous canines and an assessment of factors contributing to favourable eruption. Br J Orthod. 1993;20:215–223. doi: 10.1179/bjo.20.3.215. [DOI] [PubMed] [Google Scholar]
- 15.McDonald F, Yap WL. The surgical exposure and application of direct traction of unerupted teeth. Am J Orthod. 1986;89:331–340. doi: 10.1016/0002-9416(86)90056-4. [DOI] [PubMed] [Google Scholar]
- 16.Kohavi D, Becker A, Zilberman Y. Surgical exposure, orthodontic movement, and final tooth position as factors in periodontal breakdown of treated palatally impacted canines. Am J Orthod. 1984;85:72–77. doi: 10.1016/0002-9416(84)90124-6. [DOI] [PubMed] [Google Scholar]
- 17.Blair GS, Hobson RS, Leggat TG. Posttreatment assessment of surgically exposed and orthodontically aligned impacted maxillary canines. Am J Orthod Dentofacial Orthop. 1998;113:329–332. doi: 10.1016/s0889-5406(98)70305-1. [DOI] [PubMed] [Google Scholar]
- 18.Silness J, Löe H. Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand. 1964;22:121–135. doi: 10.3109/00016356408993968. [DOI] [PubMed] [Google Scholar]
- 19.Löe H, Silness J. Periodontal disease in pregnancy. I. Prevalence and severity. Acta Odontol Scand. 1963;21:533–551. doi: 10.3109/00016356309011240. [DOI] [PubMed] [Google Scholar]
- 20.Lewis PD. Preorthodontic surgery in the treatment of impacted canines. Am J Orthod. 1971;60:382–397. doi: 10.1016/0002-9416(71)90150-3. [DOI] [PubMed] [Google Scholar]
- 21.Crescini A, Clauser C, Giorgetti R, Cortellini P, Pini Prato GP. Tunnel traction of infraosseous impacted maxillary canines. A three-year periodontal follow-up. Am J Orthod Dentofacial Orthop. 1994;105:61–72. doi: 10.1016/S0889-5406(94)70100-8. [DOI] [PubMed] [Google Scholar]
- 22.Vermette ME, Kokich VG, Kennedy DB. Uncovering labially impacted teeth: apically positioned flap and closed-eruption techniques. Angle Orthod. 1995;65:23–32. doi: 10.1043/0003-3219(1995)065<0023:ULITAP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 23.Crescini A, Nieri M, Buti J, Baccetti T, Pini Prato GP. Orthodontic and periodontal outcomes of treated impacted maxillary canines. Angle Orthod. 2007;77:571–577. doi: 10.2319/080406-318.1. [DOI] [PubMed] [Google Scholar]
- 24.Kokich VG, Mathews DP. Surgical and orthodontic management of impacted teeth. Dent Clin North Am. 1993;37:181–214. [PubMed] [Google Scholar]
- 25.Hansson C, Rindler A. Periodontal conditions following surgical and orthodontic treatment of palatally impacted maxillary canines—a follow-up study. Angle Orthod. 1998;68:167–172. doi: 10.1043/0003-3219(1998)068<0167:PCFSAO>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 26.Becker A. Ectopic eruption of maxillary canines. Eur J Orthod. 1993;15:425. doi: 10.1093/ejo/15.5.425. [DOI] [PubMed] [Google Scholar]
- 27.Burden DJ, Mullally BH, Robinson SN. Palatally ectopic canines: closed eruption versus open eruption. Am J Orthod Dentofacial Orthop. 1999;115:640–644. doi: 10.1016/s0889-5406(99)70289-1. [DOI] [PubMed] [Google Scholar]