

Abstract
Background
Supernumerary sex chromosome aneuploidies (SCA) are common genetic conditions characterized by additional X or Y chromosome, affecting ~1/500 individuals, with the most frequent karyotypes of 47,XXY (Klinefelter syndrome), 47,XXX (Trisomy X), and 47,XYY (Jacob syndrome). Although there is considerable phenotypic variation among these diagnoses, these conditions are characterized by the presence of overlapping physical, medical, developmental, and psychological features. Our interdisciplinary clinic’s experience anecdotally supports previous published findings of atopic conditions, feeding difficulties, and gastroesophageal reflux to be more prevalent in SCAs (Bardsley et al., Journal of Pediatrics, 2013, 163, 1085; Samango‐Sprouse et al., The Application of Clinical Genetics, 2019, 12, 191; Tartaglia et al., Acta Paediatrica, 2008, 100, 851). Furthermore, we observed that many of these patients have also been diagnosed with eosinophilic esophagitis (EoE), an association not currently reported in the literature.
Methods
We conducted a retrospective chart review of all 667 patients with SCA seen at a large tertiary care center to investigate the prevalence and presenting features of EoE.
Results
Four percent of children with SCAs had a biopsy‐confirmed diagnosis of EoE, which represents an odds ratio of 32 (95% CI 6–185) when compared to the prevalence rates reported in the general population.
Conclusion
Routine screening for EoE symptoms may be warranted for individuals with SCA and atopic conditions.
Keywords: eosinophilic esophagitis, Klinefelter, sex chromosome aneuploidies
Sex chromosome aneuploidies (SCA) are common genetic conditions that may be associated with atopic conditions, including eosinophilic esophagitis (EoE). Confirmed EoE was found in 29/650 (4.5%) of youth with SCA, 32 (95% CI 6–185) greater risk than the general pediatric population. Patients with SCA are at risk and should be screened for EoE with age‐appropriate symptoms on a routine basis, as earlier diagnosis and treatment may minimize the severity of disease.

1. INTRODUCTION
Supernumerary sex chromosome aneuploidies (SCA) are common genetic conditions characterized by additional X or Y chromosome, affecting ~1/500 live births collectively, including the karyotypes 47,XXY (Klinefelter syndrome); 47,XXX (Trisomy X); 47,XYY (Jacob’s syndrome); 48,XXXY and 48,XXYY. Despite the high prevalence of these conditions, the majority of individuals with SCAs remain undiagnosed within their lifetime (Abramsky & Chapple, 1997; Bojesen et al., 2003), with ascertainment during childhood heavily dependent upon the severity of clinical presentation leading to genetic evaluation. With cell‐free fetal DNA (cffDNA) prenatal screening becoming an obstetric standard of care, infants are now being incidentally identified (Gregg et al., 2016).
Although there is considerable phenotypic variation among these diagnoses, these conditions collectively are characterized by the presence of physical, medical, developmental, and psychological features. The eXtraordinarY Kids Clinic at Children’s Hospital Colorado is an interdisciplinary clinical and research program dedicated to addressing manifestations of SCAs from infancy to young adulthood. With over 650 individual clinical patients and hundreds more participating in research studies, we have observed higher than the expected rates of atopic conditions, feeding difficulties, and gastroesophageal reflux, which is consistent with previous reports (Bardsley et al., 2013; Samango‐Sprouse et al., 2019). Furthermore, we observed that a higher than expected number of these patients have also been diagnosed with eosinophilic esophagitis (EoE). EoE is an immune‐mediated esophageal disease characterized by an increased number of eosinophils in the esophagus and symptoms of esophageal dysfunction (Furuta et al., 2007; Rothenberg, 2015). EoE was first recognized as an independent clinical diagnosis in 1993, but the first clinical guidelines for EoE were not published until 2007 (Furuta et al., 2007; Philpott et al., 2014; Rothenberg, 2015). A diagnosis of EoE requires symptoms of esophageal dysfunction and histological esophageal eosinophilia (≥15 eosinophils per high‐power field) from a mucosal biopsy obtained from upper intestinal endoscopy, with other causes of esophageal eosinophilia being ruled out (Dellon et al., 2018; Furuta et al., 2007; Rothenberg, 2015).
The incidence of EoE varies widely among geographies, with an average of seven new cases per 100,000 persons per year (range: 1–20/100,000). Prevalence rates range between 13 and 49 cases per 100,000 persons, with pediatric populations ranging from 0.2 to 43 cases per 100,000 persons (Iuliano et al., 2018; Lucendo et al., 2017). Several studies support increasing incidence rates of EoE overall, likely attributed to an increasing awareness of EoE and symptoms referred for evaluation (Dellon et al., 2015; Giriens et al., 2015; Liacouras et al., 2005; Maradey‐Romero et al., 2015; Prasad et al., 2009; van Rhijn et al., 2013; Shaheen et al., 2018; Syed et al., 2012; Warners et al., 2018). EoE affects predominantly Caucasian males with a 3:1 increased male prevalence. Although the reasons for this sex difference are not yet well understood, there is speculation of this male predilection associated with genetic factors including single nucleotide polymorphisms (SNPs) in the thymic stromal lymphopoietin (TSLP) gene, the TSLP receptor gene, and estrogen‐responsive gene expression differences in subjects with EoE (Sleiman et al., 2014; Wheeler et al., 2019).
Presenting symptoms of EoE can differ greatly based on the age of the individual. Children with EoE typically have a history of feeding difficulty, vomiting, and abdominal pain, while adolescents and adults are more likely to present with dysphagia and food impaction (Furuta & Katzka, 2015). Over time, individuals with EoE may adapt their eating habits and develop coping strategies to ameliorate some of these symptoms, such as drinking a lot of water while eating, taking a long time to eat, and using sauces during meal times to help lubricate food (Furuta & Katzka, 2015). These coping strategies may also mask the underlying problem, therefore a high index of suspicion is needed to identify these behaviors and symptoms as EoE (Hirano & Furuta, 2020; Lee et al., 2018). In children with developmental disabilities, such as those associated with SCAs, the non‐specific symptoms of EoE may be even more likely to go unrecognized. Left untreated, EoE can progress to cause strictures in the esophagus or food impaction. Treatment of EoE can include eliminating potential allergens from the diet, topical swallowed steroids, proton pump inhibitors, and endoscopic dilation of esophageal strictures if present. The goals of treatment of EoE aim to relieve symptoms, improve the histologic findings, and prevent further complications of EoE (Dellon et al., 2018; Hirano & Furuta, 2020).
This study aims to quantify the prevalence of EoE among a clinical population of youth with SCA and describe the presenting symptoms in order to bring attention to (a) the co‐existence of these conditions and (b) the importance of recognizing EoE symptoms early in this patient population to initiate appropriate referrals for diagnostic evaluation and treatment in an attempt to prevent long‐term complications of EoE.
2. MATERIALS AND METHODS
This is a retrospective study reviewing the electronic medical records of 667 clinical patients between the ages of 1 month and 30 years with confirmed SCA [47,XXX (n = 101); 47,XXY (n = 372); 47,XYY (n = 71); 48,XXXY (n = 14); 48,XXYY (n = 88); and other/mosaic (n = 21)] seen in the Children’s Hospital Colorado (CHCO) eXtraordinarY Kids Clinic between 2005 and 2020. Medical records were searched for a diagnosis of or past medical history consistent with EoE and 46 cases were further reviewed to corroborate a confirmed diagnosis of EoE as defined by ≥15 eosinophils per high‐power field on esophageal biopsy. Pathology reports and medical records were obtained from outside institutions if the EoE diagnosis was made outside of CHCO and were reviewed by a board‐certified pediatric gastroenterologist (NN). For those 29 cases with a biopsy‐confirmed diagnosis of EoE, clinical data including symptoms related to gastrointestinal dysfunction, co‐existing atopic diseases, height and BMI at the time of EoE diagnosis, karyotype, reason for genetic testing, and developmental histories were abstracted from the medical record. This study was approved by the local institutional review board (COMIRB # 08‐0513) and all parents provided written informed consent and patients provided assent, as age appropriate for inclusion of clinical records in this research study.
The prevalence of EoE among clinical patients with SCA was obtained by dividing the total number of biopsy‐confirmed cases over the total number of patients seen during that time period. Records retrieved in the initial search from individuals with a clinical history consistent with EoE but did not meet criteria for a biopsy‐confirmed diagnosis of EoE were excluded (n = 17). The prevalence of EoE in the SCA cohort was compared to previous reports of EoE prevalence in the general pediatric population with the Fisher’s exact test with relative risk and 95% confidence interval (CI) calculated with the Koopman asymptotic score method using Prism GraphPad v9.1.0 for Mac GraphPad Software, www.graphpad.com. For the most conservative estimate, we used the reported population prevalence in males in the United States (as high as 140 in 100,000; Dellon et al., 2014) as a conservative comparison, recognizing the actual prevalence in an age‐matched sample would likely be much lower. Measures of central tendency and variability were used to summarize the outcomes of interests. Due to variability in presenting symptoms by age, the cohort was stratified into younger children (1–9 years of age) and older children/adults (>9 years of age) groups. For illustration purposes, select case reports were presented.
3. RESULTS
Summary data for patients with co‐existing SCA and EoE are presented in Table 1 and patient‐level data are available in Table S1. Twenty‐nine patients (4.5%) with non‐mosaic SCA and a confirmed diagnosis of EoE were identified (Figure 1). This conservatively represents a relative risk of EoE of 32 (95% CI 6–185) times greater in children with SCA than would be expected in the general population. The risk of EoE was significantly greater than expected in all SCA karyotypes (p < .006 for all). A higher proportion of patients with tetrasomy conditions had EoE (48,XXYY 8% and 48,XXXY 15%) compared to trisomy conditions (3%–6%; Fisher’s exact test p = .03).
TABLE 1.
Patients with SCA and EoE (n = 29)
| n (%) or median (IQR) | |
|---|---|
| Karyotype | |
| 47,XXY | 13 (45%) |
| 47,XYY | 4 (14%) |
| 47,XXX | 3 (10%) |
| 48,XXYY | 7 (24%) |
| 48,XXXY | 2 (7%) |
| Male sex | 26 (90%) |
| Race/ethnicity | |
| Non‐Hispanic White | 26 (90%) |
| Hispanic White | 2 (7%) |
| Non‐Hispanic Asian | 1 (3%) |
| Gestational age (weeks) | 40 (38–40) |
| Timing of SCA diagnosis | |
| Prenatal | 9 (31%) |
| Postnatal | 20 (69%) |
| Neurodevelopmental phenotype | |
| Normal/no diagnoses | 4 (14%) |
| Autism spectrum disorder | 14 (48%) |
| Developmental delay | 25 (86%) |
| Intellectual disability | 7 (24%) |
| Atopic conditions | |
| Eczema | 12 (41%) |
| Food allergies | 23 (79%) |
| Environmental allergies | 17 (59%) |
| Asthma | 18 (62%) |
| EoE characteristics | |
| Age of EoE diagnosis (yrs) | 11 (5–15) |
| Delay in diagnosis (yrs) | 2 (1–3) |
| Peak eosinophils/HPF at diagnosis | 41 (27–92) |
FIGURE 1.
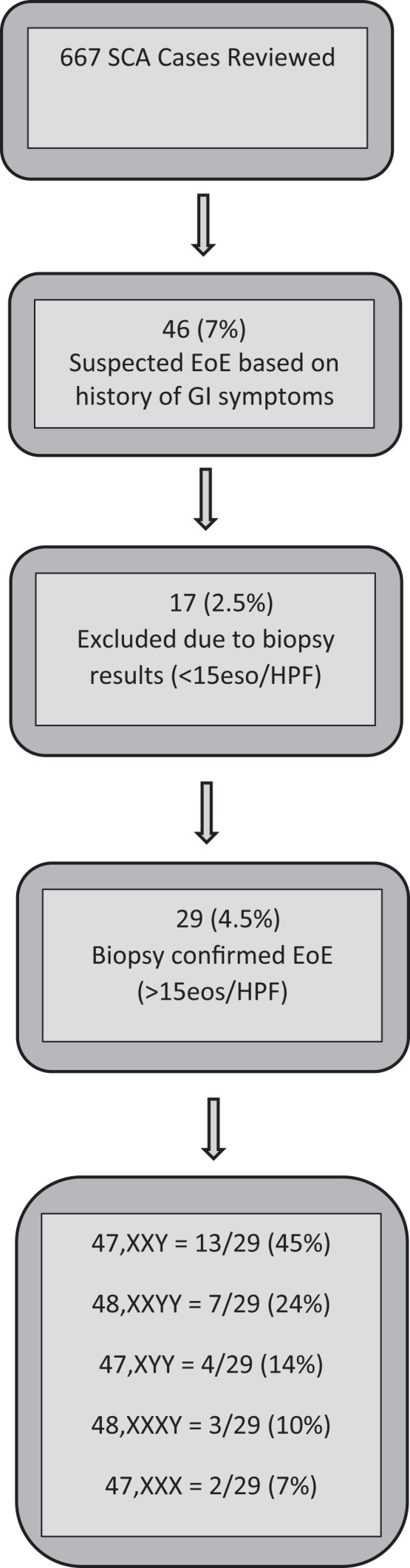
SCA cases initially reviewed and confirmed with EoE by pathology report review
Nine patients (31%) were prenatally diagnosed with SCA either due to advanced maternal age (n = 7) or abnormal ultrasound findings (n = 2). Twenty patients (69%) were diagnosed postnatally (median age: 7 years, range: 13 months–17 years) with SCA, the majority of whom received genetic testing due to developmental delays, hypotonia, or specific physical exam findings suggesting hypogonadism. The majority of patients had developmental delays affecting both motor and speech/language development from mild to moderate severity, and almost half had a diagnosis of autism spectrum disorder (ASD). Two of the patients with ASD had very limited expressive language. All 29 patients reported at least one atopic disease. Of the 23 patients with known food allergies, the average number of food allergies was to 5 different foods (range 1–12 different food allergies) with the most common reported food allergies being dairy products (15/23, 65%), eggs (9/23, 39%), peanuts (9/23, 39%), tree nuts (8/23, 35%), and soy (6/23, 26%). Other food allergies that were reported included wheat, sesame, legumes, tomato, fish, and lentils, among others. Sleeping problems were also present in four of the cases at the time of EoE diagnosis.
The most common presenting symptoms leading to a diagnostic endoscopy are shown in Figure 2. Dysphagia and reflux were the most common presenting signs in both younger and older children. Younger children were more likely to present with feeding difficulties and gagging, whereas only children >10 years were presented with food impaction. While height did not seem to be impacted, eight patients (28%) had a body mass index (BMI) <5% ile at the time of EoE diagnosis. Symptoms were present for a median of 2 years prior to EoE diagnosis.
FIGURE 2.
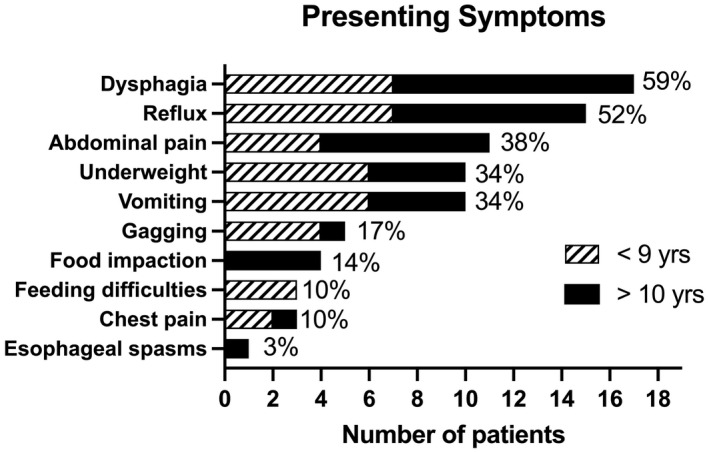
EoE presenting symptoms stratified by age group
To highlight EoE histories and presentations, six cases are selected and described in Table 2. These six cases and their associated patient numbers correspond in Table S1, with additional information about each patient provided.
TABLE 2.
Six Case Histories Demonstrating Variable Presentations of EoE in Patients with SCA
| Patient 2 | Patient 2 is a 14‐year‐old female with 47,XXX and had a complicated medical history. She was born full term at 6lbs 5oz and 18.5in by induced vaginal delivery. She had a long‐standing history of failure to thrive (average BMI, 0.24% ile from age 5 to 10 years; prior BMI data not available). At 3 years of age, she started to experience abdominal pain, chest pain, and reflux. Her symptoms worsened with time to include chronic vomiting and dysphagia. She also had food allergies, environmental allergies, and eczema. At 6 years of age, an upper endoscopy was performed, with pathology showing 12 and 2 eos/HPF in the distal and proximal esophagus, respectively, which was not diagnostic for EoE. She started omeprazole (20 mg/day) following this initial endoscopy. Due to continuous and progressive GI symptoms, another upper endoscopy was performed at age 8, with pathology showing 110 eos/HPF in the distal esophagus, diagnostic for EoE. Following the diagnosis of EoE, she was continued on omeprazole and also started on swallowing topical corticosteroid, fluticasone 110 mcg, 2 puffs swallowed twice daily. She continued to avoid known IgE‐mediated food allergies including dairy, egg, peanut, tree nut, fish, sesame, tomato, and soy. At age 12, she was evaluated by chromosomal microarray (CMA) for developmental delays, learning difficulties, ADHD, anxiety, and joint hypermobility, which identified non‐mosaic 47,XXX. |
| Patient 4 | Patient 4 is a 5‐year‐old male with 47,XYY identified prenatally by cell‐free fetal DNA (cffDNA) screening due to advanced maternal age, confirmed postnatally by chromosomal microarray. He was born at 38 weeks and noted to have hypotonia, and motor delays led to initiation of physical therapy at 7 months of age. At 11 months of age, symptoms of gagging with stage 3 baby foods led to feeding evaluation and a diagnosis of delayed oral motor skills. Developmental evaluation at 16 months of age led to diagnoses of global developmental delays and autism spectrum disorder (ASD), and feeding at that time included stage 2 and some stage 3 foods as well as ongoing bottle feeding. He had a febrile seizure at 22 months of age, after which he showed regression of feeding and began refusing purees or other foods beyond formula from the bottle. This improved slowly with feeding therapy until a lip requiring sutures at age 3 again led to a refusal of all feedings beyond bottle foods. He received various therapies including feeding, speech, occupational, physical, and autism behavioral therapies since prior to 2 years of age. He was seen by developmental pediatrics at age 4 years and 2 months and referred for additional feeding and gastroenterology (GI) evaluation due to poor weight gain and ongoing feeding problems. Communication at that time was limited with no use of words, occasional vocalizations, and a few signs. The feeding evaluation attributed his feeding difficulties to autism‐related sensory issues and the GI evaluation was not pursued by parents at that time. At age 5 with ongoing feeding struggles, he was evaluated by GI in the GEDP clinic at the CHCO for refusal to eat solid foods and malnutrition (BMI 0.7% ile). An upper endoscopy was performed and pathology revealed 45 eos/HPF in both the proximal and distal esophagus; diagnostic for EoE. The endoscopy visually showed edema and exudate (collections of eosinophils). He started treatment by swallowing topical corticosteroids of oral viscous budesonide (0.5 mg twice daily). Treatment is ongoing with sustained feeding and developmental therapies, transition to elemental formula, and follow‐up endoscopy pending. |
| Patient 7 | Patient 7 is a 9‐year‐old male with 47,XYY syndrome diagnosed at 3 years of age by chromosomal microarray due to developmental delays and abnormal white matter hyperintensities on brain MRI. He was born full term, 5lbs 5oz and 18.5in by spontaneous vaginal delivery. He has an atopic disease history of eczema, asthma, food allergies, and seasonal allergies. At 12 months of age, he had significant reflux and chronic vomiting, treated with high‐dose PPI (omeprazole 40 mg), yet symptoms persisted. At 3 years of age he was evaluated with an upper endoscopy, and pathology revealed 90 and 35 eos/HPF in the distal and proximal esophagus, respectively; diagnostic for EoE. Visually, the endoscopy showed exudate and edema. He started swallowing topical corticosteroid, fluticasone (44 mcg, 2 puffs swallowed twice daily). Six months after starting treatment for EoE, his symptoms of reflux and vomiting had resolved. |
| Patient 13 | Patient 13 is a 14‐year‐old male with 47,XXY syndrome diagnosed prenatally by amniocentesis secondary to increased nuchal translucency on fetal ultrasound, as well as postnatal confirmatory karyotype. He was born at 39 weeks by spontaneous vaginal delivery, weighing 5lbs 4oz. He was presented in the GI clinic at 10 years of age due to dysphagia. At the time he had a history of seasonal allergies and poor weight gain, with a low BMI (3rd percentile; prior BMI data not available). History during this initial GI evaluation revealed that he had always been a slow eater, drank a lot of liquids during mealtime, and frequently used sauces with most foods. In addition, he had presented to the emergency department on two separate occasions due to feelings of food stuck in his esophagus (food impactions that both resolved without endoscopic intervention). After this evaluation, he underwent an upper GI series to assess for esophageal stricture which showed mild narrowing of the proximal third of the esophagus with mucosal irregularities seen. He then started omeprazole (40 mg) with a plan to undergo an upper endoscopy. However, the family did not follow‐up for 2.5 years. At 13 years of age, he returned to care and underwent an upper endoscopy, with pathology showing 130 and 47 eos/HPF in the distal and proximal esophagus, respectively; diagnostic for EoE. His visual endoscopy findings included edema, exudate, and linear furrows. After the endoscopy, he started swallowing topical corticosteroids, fluticasone (110 mcg, 2 puffs swallowed twice daily), for treatment of EoE and continued taking omeprazole (40 mg), and symptoms of dysphagia resolved. |
| Patient 16 | Patient 16 is a 9‐year‐old male with 48,XXYY syndrome diagnosed at 5 years of age by chromosomal microarray ordered due to developmental delays. He was born full term at 8lbs 4oz. At 12 months of age, he was noted to have reflux and episodes of spitting up blood. It is unclear if he underwent further evaluation for these symptoms at that age, but these symptoms resolved over time without intervention. At age 8, he was evaluated by the GEDP at CHCO for concerns of dysphagia and behaviors of self‐pounding on his chest when eating; symptoms which began around 7 years of age. Upon further history, he was noted to always be a slow eater, drink excessive amounts of water during mealtime, and use sauces liberally to lubricate his foods. He also had a history of significant atopic disease including, eczema, asthma, food allergies, and seasonal allergies. Due to suspicion of EoE, an upper endoscopy was performed and pathology showed 16 and 18 eos/HPF in the distal and proximal esophagus, respectively; diagnostic for EoE. His visual endoscopic findings included exudate (collections of eosinophils) and edema. After he was diagnosed with EoE, he started omeprazole (40 mg) daily and eliminated dairy from his diet, with improved symptoms. |
| Patient 19 | Patient 19 is a 24‐year‐old male diagnosed with 48,XXYY at 22 months of age by karyotype ordered due to significant developmental delays and hypotonia. He was born full term at 6lbs 3oz and 20in. He has atopic diagnoses including, asthma, food allergies, and seasonal allergies. At age 16, he was evaluated by GI due to dysphagia, abdominal pain, and an unexplained 15 pound weight loss in the prior 6 month period. He started omeprazole (30 mg, twice daily) without relief of GI symptoms. At age 17, he underwent upper endoscopy due to dysphagia with food impactions. Pathology demonstrated 68 and 103 eos/HPF in the distal and proximal esophagus, respectively; diagnostic for EoE. In addition, pathology identified candida esophagitis, unrelated to his diagnosis of EoE. He started on a 21‐day treatment for the candida esophagitis as well as lansoprazole (30 mg twice daily). A repeat upper endoscopy, at age 18, showed persistent eosinophils as well as persistent candida esophagitis, which was treated again. He remains on lansoprazole (30 mg, twice daily), but has not returned for a follow‐up appointment in GI for further assessment of his EoE at this time. |
4. DISCUSSION
This is the first study to report the co‐existence of EoE in individuals with SCA, with 4.5% of patients with SCA found to have EoE. While the true prevalence of EoE among individuals with SCA will require additional prospective research, this suggests a much higher risk than would be expected in the general pediatric population. Furthermore, due to the developmental features in SCA, symptoms of EoE may go unrecognized. However, the presenting features, association with other atopic conditions, and predominance of non‐Hispanic White males are similar to what has been reported for pediatric EoE in general. Based on our findings in this study, children with SCAs who have at least one atopic condition should be specifically screened for age‐appropriate symptoms of EoE and if symptoms are present, referred to a pediatric gastroenterologist.
Studies evaluating the clinical presentations of EoE in children and adults have shown that younger children are more likely to present with feeding difficulties, gagging, nausea, vomiting, failure to thrive, and abdominal pain; while teenagers and adults are more likely to present with dysphagia and food impactions (Falk, 2014; Liacouras et al., 2014). Our findings are largely similar with the exception that 54% (7/13) of the children <9 years also had a history of dysphagia, a symptom more commonly thought to occur in older patients. The dysphagia identified in the SCA population could be attributed to various factors, including comorbidities in SCA that may make dysphagia more evident or potentially a delay in diagnosis leading to more severe disease. Low oral motor tone, a common finding in SCAs, can contribute to swallowing difficulties, therefore it is possible dysphagia may present earlier in the setting of EoE. Other developmental and social‐emotional delays may limit the child’s ability to exercise coping strategies described above leading to symptomatic dysphagia sooner. Although these reasons are speculative, dysphagia in an individual with SCA of any age should prompt the evaluation for EoE. In addition, poor weight gain, feeding difficulties, and reflux were commonly identified in our SCA cohort, therefore clinicians and families should consider gastroenterology evaluation in these settings. Screening tools such as the Pediatric Eosinophilic Esophagitis Symptom Severity Module, Version 2.0 (PEESS V2.0), is a validated instrument for assessing symptoms of EoE over time and can be used for patients with SCA (Franciosi et al., 2011; Martin et al., 2015).
In addition to presenting symptoms, several children adopted specific coping strategies surrounding eating in order to alleviate EoE symptoms and discomfort, a finding previously described by others (Furuta & Katzka, 2015; Iuliano et al., 2018). The history from Patient 12 highlights behaviors consistent with common coping strategies when EoE is present, including eating slowly, drinking excess water during mealtimes, and using sauces. Although the symptoms may be masked with these coping strategies, the underlying esophageal disease persists potentially resulting in progressive symptoms, food impaction, and/or esophageal strictures. One study found that 85% of adults who had untreated EoE symptoms for 20 years eventually experienced an esophageal stricture (Schoepfer et al., 2013). Therefore, a high index of clinical suspicion is necessary for recognition of sometimes subtle symptoms or coping habits that children with EoE may display. Children in this study had symptoms for a median of 2 years, with one having symptoms for 12 years prior to diagnosis. By identifying a diagnosis of EoE early, medical management can be guided to halt progression of worsening symptoms such as esophageal strictures, improve quality of life, and provide answers to the patient and their families for their persistent gastrointestinal symptoms.
While EoE is currently thought to be caused by a combination of environmental and genetic factors, food antigens are currently thought to be the most likely cause of the pathogenesis of EoE (Dellon et al., 2018; Furuta & Katzka, 2015; Philpott et al., 2014). Atopic disease, such as food and environmental allergies, asthma, and eczema, are commonly associated with EoE (Lucendo et al., 2017). One study concluded that about 63% of all patients with EoE have at least one atopic diagnosis, while only 3% have all four atopic diagnoses (Benninger et al., 2017). Some additional environmental factors that have been found to increase an individual’s risk for EoE include living in arid/temperate environments, early exposure to certain food antigens, breastfeeding, antibiotic use in infancy, and preterm birth (Philpott et al., 2014). Individuals with SCA have an increased risk for atopic disease, such as asthma, food allergies, and seasonal allergies (Tartaglia et al., 2008, 2011). All 29 patients in this chart review had at least one atopic disease, and many with multiple atopies (3 atopic diagnoses in 13/29; 4 atopic diagnoses in 3/29), suggesting even higher rates of atopy than anticipated from the EoE literature alone. This finding could be attributed to culminating factors including individuals with SCA already at higher risk for atopic diagnoses, an ascertainment bias, or possibly suggest an underlying etiology to link these findings. Given the universal finding of atopy in the patients with SCA and EoE in this cohort, we strongly recommend screening for EoE symptoms among children with SCA and atopic disease.
In addition to atopy, neurodevelopmental disabilities were present in the majority of our children in this series, including 14 (48%) who had a confirmed diagnosis of ASD, 2 of whom were nonverbal. SCAs are associated with a higher prevalence of developmental delays and ASD, so this is not surprising in and of itself, however neurodevelopmental concerns can further complicate the clinical picture of EoE. The relationship between EoE and ASD has been described before, with the prevalence of ASD among children with EoE as high as 7.5%, and children with ASD seeming to have a higher prevalence of EoE than expected as well (Capucilli et al., 2018; Heifert et al., 2016). In this context, these children may develop adverse eating behaviors secondary to EoE‐associated discomfort, especially in lower functioning children who cannot communicate their symptoms or utilize coping mechanisms. Furthermore, presenting symptoms of EoE such as food refusal, gagging, or somatic symptoms, may be inadvertently attributed to ASD‐ or SCA‐associated symptoms such as oral sensitivities, delayed oral motor skills, extreme food selectivity, ritualistic eating behaviors, or difficulties with communication rather than considering GI pathology. In these settings, EoE symptoms may be exacerbated to episodes of dysphagia before coming to clinical attention. In the setting of neurodevelopmental disabilities, it seems likely that the risk of missing the diagnosis of EoE is higher than for neurotypical children, although additional research is still needed in this area.
The current understanding of the pathophysiology of EoE includes possible genetic factors that influence an individual’s risk for developing EoE. Information about the genetics of EoE includes altered esophageal epithelial expression of estrogen receptors (ERs) and estrogen‐responsive genes as well as sex‐independent disease‐associated single nucleotide polymorphisms (SNPs). Esophageal epithelium differential expression of ER genes, ESR1 (Estrogen Receptor 1) gene (OMIM 133430) and ESR2 (Estrogen Receptor 2) gene (OMIM 601663), coupled with altered expression of other estrogen‐responsive genes, is proposed to protect females against the development of EoE due to estrogen hormone signaling pathways and suppression of IL‐13‐induced esophageal epithelial barrier dysfunction, thereby contributing to male propensity of EoE presentation (Wheeler et al., 2019). Disease‐associated SNPs are thought to disrupt immune pathways, leading to a recruitment of eosinophils to the esophagus, causing inflammation, and the other visual esophageal findings in EoE (Kottyan et al., 2020; Kottyan & Rothenberg, 2017; Rothenberg, 2015). While the male predilection for EoE is likely multifactorial, the suspected and possibly associated SNPs are in the thymic stromal lymphopoietin (TSLP) gene (OMIM 607003) and the TSLP receptor gene (CRLF2, cytokine receptor‐like factor 2 gene, OMIM 300357 and OMIM 400023 for Y‐linked). It is important to note that the TSLP receptor gene is located in the pseudoautosomal region of Xp22.3/Yp11.3 (Sherrill et al., 2010), in which all SCA cases in this chart review would likely overexpress these genes as the pseudoautosomal regions escape X‐inactivation. This overexpression of pseudoautosomal region genes, including the TSLP receptor gene, could possibly have epigenetic impacts and may contribute to the development of EoE in both male and female SCA patients. In a 2020 study by Kottyan et al, 31 reported independent EoE risk loci were identified to be primarily located either between genes or within gene introns, and only 3 of 31 loci resulted in an amino acid change, suggesting genetic risk to be derived from changes in DNA regulatory activity leading to a genotype‐dependent expression. While it is important to note that no risk loci were located on the X nor Y chromosome, the risk variants identified within genes are suggested to have allele‐specific expression (e.g., TSLP gene) that may influence the physiology of epithelial cells in the esophagus, predisposing to the development of EoE (Kottyan et al., 2020). Future research should evaluate gene expression profiles of ERs and estrogen‐responsive genes in SCA patients as well as SNPs within the TSLP receptor gene and other genes on the sex chromosomes that may provide generalizable information for the etiology of EoE and contribution to the sex differences observed (Wheeler et al., 2019).
In addition to some of the known immune‐related SNPs and genes that may influence EoE risk, there are also a number of described genetic syndromes that show an increased prevalence of EoE compared to the general population. For example, an individual with a connective tissue disorder (CTD), such as, Ehlers–Danlos syndrome, Marfan syndrome, or Loeys–Dietz syndrome, has an eight‐fold increased risk of EoE when compared to individuals without a CTD (Philpott et al., 2014). Studies looking at twins with EoE have found that there is a 40% concordance between monozygotic twins and a 30% concordance between dizygotic twins, which is about 10‐fold higher than non‐twin siblings (Rothenberg, 2015). These studies demonstrate that there are some genetic factors that play a role in the pathophysiology of EoE, but more so, environmental exposures seem to be the driving factor of concordance (Rothenberg, 2015). Further research is needed to better understand if individuals with these syndromes, including SCAs, represent a more vulnerable population for exposures to contributing environmental factors versus genetic/epigenetic impact leading to risks for developing EoE.
Strengths of this study include a relatively large clinical cohort of over 650 individuals with SCA, confirmation of the EoE diagnosis from examination of pathology reports, and availability of a detailed clinical history for confirmed cases. Furthermore, although we did not have a control group, we assumed the highest reported prevalence of EoE in the general population, therefore biasing toward a type II error. Limitations of this retrospective report include the relatively small total number of confirmed EoE cases (n = 29), patient sampling bias from a specialty clinic with potential overrepresentation of severity, the inability to accurately identify the specific age of onset of EoE symptoms for all patients, and potential bias imbedded within retrospective chart reviews, including the potential for omitted or inaccurate data. Furthermore, there was variability in clinical approach to GI symptoms throughout the study period, as EoE screening questions and GI referrals to the GEDP increased as the high frequency of EoE diagnosis was recognized. Despite these limitations, the recognition of a probable association between SCA and EoE is an important contribution to the current literature. Additional research is needed to understand the true prevalence, natural history, and etiology of EoE in the SCA population.
The findings of this chart review demonstrate the importance for the community affected by SCA conditions to have an increased awareness of the variable presentations of eosinophilic esophagitis (including coping strategies), especially among different age groups and in the context of neurodevelopmental problems, the need for specific screening for EoE symptoms, and referral to GI for evaluation and treatment. Such clinical knowledge and action can facilitate diagnosing EoE as early as possible and improve quality of life, symptom management, and limit progression of severity for patients. Appendix A provides a printable handout that can be distributed to families of patients with SCA as a source of information regarding EoE.
CONFLICT OF INTEREST
The authors have declared no conflicts of interest.
AUTHOR CONTRIBUTION
Susan Howell, Shanlee M. Davis, Glenn T. Furuta, Nicole R. Tartaglia, and Nathalie Nguyen conceived and designed the project. Catherine Buchanan, Heather Miyazawa, and Susan Howell acquired the data. All authors analyzed the data, interpreted the results, and revised the manuscript. All authors read and approved the final manuscript.
Supporting information
Table S1
ACKNOWLEDGMENTS
The authors thank the study participants in the eXtraordinarY Kids Clinic and their families. This work was also supported by NIH/NCATS Colorado CTSA Grant Number UL1 TR002535, NIH/NINDS K23NS070337, NIH/NICHD K23HD092588, and NIH 2RO1‐HD42974 and the LaCache Chair for Allergic and Immunological GI Diseases (GTF). Contents are the authors’ sole responsibility and do not necessarily represent official NIH views.
APPENDIX A. Eosinophilic Esophagitis (EoE) in Patients with Sex Chromosome Aneuploidies (SCA)
Sex chromosome aneuploidy (SCA)
→What is it?
Typically, humans have 46 chromosomes in total. The only difference between a male’s and a female’s chromosomes is their sex chromosomes (X and Y). Females have two X chromosomes (46,XX), while males have an X and an Y chromosomes (46,XY). A sex chromosome aneuploidy means that a person has an atypical number of sex chromosomes. Depending on the type of SCA, an individual can have too many or too few. The prevalence of SCA is about 1/500 children, with Klinefelter syndrome (47,XXY) being the most common.
→How is it diagnosed?
More commonly today, many individuals with SCA are being identified in the prenatal period. Non‐invasive prenatal screening (NIPS) now allows a baby’s chromosomes to be studied before they are born thorough a maternal blood sample. Some pregnancies are then tested by chorionic villus sampling (CVS) or amniocentesis to make a diagnosis. However, many cases of SCA are diagnosed later, when an individual starts to experience symptoms, which prompt testing, such as developmental concerns in childhood, or infertility in adulthood. The diagnosis of SCA is made by a blood test called a karyotype or a chromosomal microarray (CMA).
→What are some findings in SCA?
Each type of SCA is different from another. The most common symptoms of SCAs may include developmental delays, learning disabilities, social/emotional problems, tall stature, as well as hypogonadism and infertility in males with extra X chromosomes, such as 47,XXY. Individuals with SCA can also experience symptoms such as feeding difficulties, reflux, and abdominal pain. However, SCAs are highly variable and many individuals who do not experience any symptoms may go undiagnosed.
→Recent study of individuals with SCA?
A recent study performed at the eXtraordinarY Kids Clinic at Children’s Hospital Colorado reported 19 out of 619 (3%) individuals with a diagnosis of SCA and eosinophilic esophagitis (EoE).
Eosinophilic Esophagitis (EoE)
→What is it?
Eosinophilic esophagitis (EoE) is a rare immune‐mediated esophageal disease characterized by an abnormal collection of eosinophils throughout the esophagus. An eosinophil is a type of white blood cell that commonly responds to infection or allergic reaction. In the case of EoE, the eosinophils are thought to be driven by certain foods.
→What are the symptoms of EoE?
The most common symptoms of EoE are listed below. Interestingly, these symptoms can differ greatly depending on the age of the individual. For example, young children are more likely to experience reflux and vomiting, while teenagers and adults are more likely to experience swallowing difficulties (dysphagia) and food impaction.
| Most common symptoms | |
|---|---|
| Young children (ages 1–9 years) | Older children (ages 10–18 years) |
| Reflux | Dysphagia (swallowing difficulties) |
| Vomiting | Food impaction |
| Dysphagia (swallowing difficulties) | Weight loss |
| Failure to thrive | Chronic abdominal pain |
| Chronic abdominal pain | |
| Chest pains | |
| Feeding difficulties | |
| Gagging | |
| Sleep issues | |
→Other common findings in EoE?
Other clinical findings commonly reported in individuals with EoE include diagnosed atopies, such as food allergies, seasonal allergies, asthma, and eczema. As shown below, individuals with SCA and EoE in the recent study performed at the eXtraordinarY Kids Clinic at Children’s Hospital Colorado were also found to experience many of these atopies. This study found the most common food allergies in these individuals included milk, soy, egg, and peanuts/tree nuts.
| Atopy diagnoses in SCA and EoE | ||
|---|---|---|
| Food allergies | 79% | |
| Asthma | 62% | |
| Seasonal allergies | 59% | |
| Eczema | 41% | |
→Individual coping strategies?
Individuals with EoE, especially children, are known to develop somewhat specific coping strategies surrounding eating in order to alleviate their chronic GI symptoms. The most common coping strategies include drinking a lot of water during mealtimes, eating slowly, chewing foods for long periods of time, avoiding certain types of foods, and using excess amounts of sauces, such as ketchup or BBQ sauce. These coping strategies can help to improve an individual’s symptoms, which can make the diagnosis more difficult to make.
→How is EoE diagnosed?
EoE is diagnosed from a procedure called an upper endoscopy, which takes a biopsy of the esophagus. This biopsy is then studied under a microscope and the number of eosinophils are counted. If there are ≥15 eosinophils present in a specific size area of the esophagus tissue biopsied, a diagnosis of EoE is made.
→How is EoE treated?
EoE is commonly treated in three ways: diet, medications, and sometimes surgical intervention. EoE symptoms may improve by eliminating certain foods that may be triggering the eosinophil immune response. For example, the six food elimination diet (avoiding milk, egg, soy, wheat, peanuts/tree nuts, and seafood) could help to reduce symptoms. The use of acid blocking medications (proton pump inhibitors, PPI) and/or swallowed topical corticosteroids can also reduce the number of eosinophils and help to improve symptoms. Lastly, individuals with EoE can sometimes experience a narrowing of their esophagus, called a stricture, which may improve from a surgical procedure to dilate the esophagus.
→Suspecting the diagnosis?
EoE should be considered when an individual is experiencing any of the common symptoms, such as swallowing difficulties, chronic vomiting, and food impaction, especially when any number of the atopy symptoms is also present. It is important to ask about possible EoE and be aware of the different coping strategies that are sometimes used to help an individual reduce his/her GI symptoms. If a child is consistently using coping strategies during mealtimes, struggles from any described GI symptoms, and has atopy diagnoses, consider talking with the doctor about an evaluation for EoE.
→What to do next?
If you are a parent and are suspicious of EoE in your child, consider talking to your child’s primary care physician about your concerns. A child who is experiencing symptoms of EoE or who has unique mealtime coping habits should be considered for a referral and evaluation by a gastroenterologist (GI doctor). A GI doctor can evaluate for possible underlying causes of these symptoms and help to address your concerns. A gastroenterologist may want to perform an upper endoscopy to biopsy the esophagus in order to determine if EoE is present.
Howell, S. , Buchanan, C. , Davis, S. M. , Miyazawa, H. , Furuta, G. T. , Tartaglia, N. R. , & Nguyen, N. (2021). Eosinophilic esophagitis in individuals with sex chromosome aneuploidies: Clinical presentations and management implications. Molecular Genetics & Genomic Medicine, 9, e1833. 10.1002/mgg3.1833
Nicole R. Tartaglia and Nathalie Nguyen are co‐author.
Funding information
This study was supported by National Institute of Child Health and Human Development (NIH/NICHD) (K23HD092588), National Institute of Neurological Disorders and Stroke (NIH/NINDS) (K23NS070337), and National Center for Advancing Translational Sciences (NIH/NCATS) (Colorado CTSA UL1TR002535).
DATA AVAILABILITY STATEMENT
Deidentified data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- Abramsky, L. , & Chapple, J. (1997). 47, XXY (Klinefelter syndrome) and 47, XYY: Estimated rates of and indication for postnatal diagnosis with implications for prenatal counselling. Prenatal Diagnosis, 17(4), 363–368. 10.1002/(SICI)1097-0223(199704)17:4<363:AID-PD79>3.0.CO;2-O [DOI] [PubMed] [Google Scholar]
- Bardsley, M. Z. , Kowal, K. , Levy, C. , Gosek, A. , Ayari, N. , Tartaglia, N. , Lahlou, N. , Winder, B. , Grimes, S. , & Ross, J. L. (2013). 47, XYY syndrome: clinical phenotype and timing of ascertainment. Journal of Pediatrics, 163(4), 1085–1094. 10.1016/j.jpeds.2013.05.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benninger, M. S. , Strohl, M. , Holy, C. E. , Hanick, A. L. , & Bryson, P. C. (2017). Prevalence of atopic disease in patients with eosinophilic esophagitis. International Forum of Allergy & Rhinology, 7(8), 757–762. 10.1002/alr.21968 [DOI] [PubMed] [Google Scholar]
- Bojesen, A. , Juul, S. , & Gravholt, C. H. (2003). Prenatal and postnatal prevalence of Klinefelter syndrome: A national registry study. Journal of Clinical Endocrinology and Metabolism, 88(2), 622–626. 10.1210/jc.2002-021491 [DOI] [PubMed] [Google Scholar]
- Capucilli, P. , Cianferoni, A. , Grundmeier, R. W. , & Spergel, J. M. (2018). Comparison of comorbid diagnoses in children with and without eosinophilic esophagitis in a large population. Annals of Allergy, Asthma & Immunology, 121(6), 711–716. 10.1016/j.anai.2018.08.022 [DOI] [PubMed] [Google Scholar]
- Dellon, E. S. , Erichsen, R. , Baron, J. A. , Shaheen, N. J. , Vyberg, M. , Sorensen, H. T. , & Pedersen, L. (2015). The increasing incidence and prevalence of eosinophilic oesophagitis outpaces changes in endoscopic and biopsy practice: national population‐based estimates from Denmark. Alimentary Pharmacology & Therapeutics, 41(7), 662–670. 10.1111/apt.13129 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dellon, E. S. , Jensen, E. T. , Martin, C. F. , Shaheen, N. J. , & Kappelman, M. D. (2014). Prevalence of eosinophilic esophagitis in the United States. Clinical Gastroenterology and Hepatology, 12(4), 589–596 e581. 10.1016/j.cgh.2013.09.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dellon, E. S. , Liacouras, C. A. , Molina‐Infante, J. , Furuta, G. T. , Spergel, J. M. , Zevit, N. , Spechler, S. J. , Attwood, S. E. , Straumann, A. , Aceves, S. S. , Alexander, J. A. , Atkins, D. , Arva, N. C. , Blanchard, C. , Bonis, P. A. , Book, W. M. , Capocelli, K. E. , Chehade, M. , Cheng, E. , … Bredenoord, A. J. (2018). Updated international consensus diagnostic criteria for eosinophilic esophagitis: Proceedings of the AGREE conference. Gastroenterology, 155(4), 1022–1033.e10. 10.1053/j.gastro.2018.07.009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Falk, G. W. (2014). Clinical presentation of eosinophilic esophagitis in adults. Gastroenterology Clinics of North America, 43(2), 231–242. 10.1016/j.gtc.2014.02.009 [DOI] [PubMed] [Google Scholar]
- Franciosi, J. P. , Hommel, K. A. , DeBrosse, C. W. , Greenberg, A. B. , Greenler, A. J. , Abonia, J. P. , Rothenberg, M. E. , & Varni, J. W. (2011). Development of a validated patient‐reported symptom metric for pediatric eosinophilic esophagitis: Qualitative methods. BMC Gastroenterology, 11, 126. 10.1186/1471-230X-11-126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furuta, G. T. , & Katzka, D. A. (2015). Eosinophilic esophagitis. New England Journal of Medicine, 373(17), 1640–1648. 10.1056/NEJMra1502863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furuta, G. T. , Liacouras, C. A. , Collins, M. H. , Gupta, S. K. , Justinich, C. , Putnam, P. E. , Bonis, P. , Hassall, E. , Straumann, A. , & Rothenberg, M. E. (2007). Eosinophilic esophagitis in children and adults: A systematic review and consensus recommendations for diagnosis and treatment. Gastroenterology, 133(4), 1342–1363. 10.1053/j.gastro.2007.08.017 [DOI] [PubMed] [Google Scholar]
- Giriens, B. , Yan, P. , Safroneeva, E. , Zwahlen, M. , Reinhard, A. , Nydegger, A. , Vavricka, S. , Sempoux, C. , Straumann, A. , & Schoepfer, A. M. (2015). Escalating incidence of eosinophilic esophagitis in Canton of Vaud, Switzerland, 1993–2013: a population‐based study. Allergy, 70(12), 1633–1639. 10.1111/all.12733 [DOI] [PubMed] [Google Scholar]
- Gregg, A. R. , Skotko, B. G. , Benkendorf, J. L. , Monaghan, K. G. , Bajaj, K. , Best, R. G. , Klugman, S. , & Watson, M. S. (2016). Noninvasive prenatal screening for fetal aneuploidy, 2016 update: A position statement of the American College of Medical Genetics and Genomics. Genetics in Medicine, 18(10), 1056–1065. 10.1038/gim.2016.97 [DOI] [PubMed] [Google Scholar]
- Heifert, T. A. , Susi, A. , Hisle‐Gorman, E. , Erdie‐Lalena, C. R. , Gorman, G. , Min, S. B. , & Nylund, C. M. (2016). Feeding disorders in children with autism spectrum disorders are associated with eosinophilic esophagitis. Journal of Pediatric Gastroenterology and Nutrition, 63(4), e69–e73. 10.1097/MPG.0000000000001282 [DOI] [PubMed] [Google Scholar]
- Hirano, I. , & Furuta, G. T. (2020). Approaches and challenges to management of pediatric and adult patients with eosinophilic esophagitis. Gastroenterology, 158(4), 840–851. 10.1053/j.gastro.2019.09.052 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iuliano, S. , Minelli, R. , Vincenzi, F. , Gaiani, F. , Ruberto, C. , Leandro, G. , & De’Angelis, G. L. (2018). Eosinophilic esophagitis in pediatric age, state of the art and review of the literature. Acta Biomed, 89(8‐S), 20–26. 10.23750/abm.v89i8-S.7866 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kottyan, L. C. , Parameswaran, S. , Weirauch, M. T. , Rothenberg, M. E. , & Martin, L. J. (2020). The genetic etiology of eosinophilic esophagitis. The Journal of Allergy and Clinical Immunology, 145(1), 9–15. 10.1016/j.jaci.2019.11.013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kottyan, L. C. , & Rothenberg, M. E. (2017). Genetics of eosinophilic esophagitis. Mucosal Immunology, 10(3), 580–588. 10.1038/mi.2017.4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, K. , Furuta, G. T. , & Nguyen, N. (2018). Eosinophilic esophagitis is an underlying cause for gastrointestinal concerns in children. Frontiers in Pediatrics, 6, 113. 10.3389/fped.2018.00113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liacouras, C. A. , Spergel, J. , & Gober, L. M. (2014). Eosinophilic esophagitis: clinical presentation in children. Gastroenterology Clinics of North America, 43(2), 219–229. 10.1016/j.gtc.2014.02.012 [DOI] [PubMed] [Google Scholar]
- Liacouras, C. A. , Spergel, J. M. , Ruchelli, E. , Verma, R. , Mascarenhas, M. , Semeao, E. , Flick, J. , Kelly, J. , Brown–Whitehorn, T. , Mamula, P. , & Markowitz, J. E. (2005). Eosinophilic esophagitis: a 10‐year experience in 381 children. Clinical Gastroenterology and Hepatology, 3(12), 1198–1206. 10.1016/s1542-3565(05)00885-2 [DOI] [PubMed] [Google Scholar]
- Lucendo, A. J. , Molina‐Infante, J. , Arias, Á. , Arnim, U. , Bredenoord, A. J. , Bussmann, C. , Amil Dias, J. , Bove, M. , González‐Cervera, J. , Larsson, H. , Miehlke, S. , Papadopoulou, A. , Rodríguez‐Sánchez, J. , Ravelli, A. , Ronkainen, J. , Santander, C. , Schoepfer, A. M. , Storr, M. A. , Terreehorst, I. , … Attwood, S. E. (2017). Guidelines on eosinophilic esophagitis: evidence‐based statements and recommendations for diagnosis and management in children and adults. United European Gastroenterology Journal, 5(3), 335–358. 10.1177/2050640616689525 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maradey‐Romero, C. , Prakash, R. , Lewis, S. , Perzynski, A. , & Fass, R. (2015). The 2011–2014 prevalence of eosinophilic oesophagitis in the elderly amongst 10 million patients in the United States. Alimentary Pharmacology & Therapeutics, 41(10), 1016–1022. 10.1111/apt.13171 [DOI] [PubMed] [Google Scholar]
- Martin, L. J. , Franciosi, J. P. , Collins, M. H. , Abonia, J. P. , Lee, J. J. , Hommel, K. A. , Varni, J. W. , Grotjan, J. T. , Eby, M. , He, H. , Marsolo, K. , Putnam, P. E. , Garza, J. M. , Kaul, A. , Wen, T. , & Rothenberg, M. E. (2015). Pediatric eosinophilic esophagitis symptom scores (PEESS v2.0) identify histologic and molecular correlates of the key clinical features of disease. The Journal of Allergy and Clinical Immunology, 135(6), 1519–1528 e1518. 10.1016/j.jaci.2015.03.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Philpott, H. , Nandurkar, S. , Royce, S. G. , Thien, F. , & Gibson, P. R. (2014). Risk factors for eosinophilic esophagitis. Clinical and Experimental Allergy, 44(8), 1012–1019. 10.1111/cea.12363 [DOI] [PubMed] [Google Scholar]
- Prasad, G. A. , Alexander, J. A. , Schleck, C. D. , Zinsmeister, A. R. , Smyrk, T. C. , Elias, R. M. , Locke, G. R. , & Talley, N. J. (2009). Epidemiology of eosinophilic esophagitis over three decades in Olmsted County, Minnesota. Clinical Gastroenterology and Hepatology, 7(10), 1055–1061. 10.1016/j.cgh.2009.06.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rothenberg, M. E. (2015). Molecular, genetic, and cellular bases for treating eosinophilic esophagitis. Gastroenterology, 148(6), 1143–1157. 10.1053/j.gastro.2015.02.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Samango‐Sprouse, C. A. , Counts, D. R. , Tran, S. L. , Lasutschinkow, P. C. , Porter, G. F. , & Gropman, A. L. (2019). Update on the clinical perspectives and care of the child with 47, XXY (Klinefelter Syndrome). The Application of Clinical Genetics, 12, 191–202. 10.2147/TACG.S180450 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schoepfer, A. M. , Safroneeva, E. , Bussmann, C. , Kuchen, T. , Portmann, S. , Simon, H. U. , & Straumann, A. (2013). Delay in diagnosis of eosinophilic esophagitis increases risk for stricture formation in a time‐dependent manner. Gastroenterology, 145(6), 1230–1236.e2. 10.1053/j.gastro.2013.08.015 [DOI] [PubMed] [Google Scholar]
- Shaheen, N. J. , Mukkada, V. , Eichinger, C. S. , Schofield, H. , Todorova, L. , & Falk, G. W. (2018). Natural history of eosinophilic esophagitis: A systematic review of epidemiology and disease course. Diseases of the Esophagus, 31(8), 15. 10.1093/dote/doy015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sherrill, J. D. , Gao, P.‐S. , Stucke, E. M. , Blanchard, C. , Collins, M. H. , Putnam, P. E. , Franciosi, J. P. , Kushner, J. P. , Abonia, J. P. , Assa’ad, A. H. , Kovacic, M. B. , Biagini Myers, J. M. , Bochner, B. S. , He, H. , Hershey, G. K. , Martin, L. J. , & Rothenberg, M. E. (2010). Variants of thymic stromal lymphopoietin and its receptor associate with eosinophilic esophagitis. The Journal of Allergy and Clinical Immunology, 126(1), 160–165.e3. 10.1016/j.jaci.2010.04.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sleiman, P. M. A. , Wang, M.‐L. , Cianferoni, A. , Aceves, S. , Gonsalves, N. , Nadeau, K. , Bredenoord, A. J. , Furuta, G. T. , Spergel, J. M. , & Hakonarson, H. (2014). GWAS identifies four novel eosinophilic esophagitis loci. Nature Communications, 5, 5593. 10.1038/ncomms6593 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Syed, A. A. , Andrews, C. N. , Shaffer, E. , Urbanski, S. J. , Beck, P. , & Storr, M. (2012). The rising incidence of eosinophilic oesophagitis is associated with increasing biopsy rates: A population‐based study. Alimentary Pharmacology & Therapeutics, 36(10), 950–958. 10.1111/apt.12053 [DOI] [PubMed] [Google Scholar]
- Tartaglia, N. , Ayari, N. , Howell, S. , D’Epagnier, C. , & Zeitler, P. (2011). 48, XXYY, 48, XXXY and 49, XXXXY syndromes: Not just variants of Klinefelter syndrome. Acta Paediatrica, 100(6), 851–860. 10.1111/j.1651-2227.2011.02235.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tartaglia, N. , Davis, S. , Hench, A. , Nimishakavi, S. , Beauregard, R. , Reynolds, A. , Fenton, L. , Albrecht, L. , Ross, J. , Visootsak, J. , Hansen, R. , & Hagerman, R. (2008). A new look at XXYY syndrome: Medical and psychological features. American Journal of Medical Genetics Part A, 146A(12), 1509–1522. 10.1002/ajmg.a.32366 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Rhijn, B. D. , Verheij, J. , Smout, A. J. , & Bredenoord, A. J. (2013). Rapidly increasing incidence of eosinophilic esophagitis in a large cohort. Neurogastroenterology and Motility, 25(1), 47–52.e45. 10.1111/nmo.12009 [DOI] [PubMed] [Google Scholar]
- Warners, M. J. , de Rooij, W. , van Rhijn, B. D. , Verheij, J. , Bruggink, A. H. , Smout, A. , & Bredenoord, A. J. (2018). Incidence of eosinophilic esophagitis in the Netherlands continues to rise: 20‐year results from a nationwide pathology database. Neurogastroenterology and Motility, 30(1), 13165. 10.1111/nmo.13165 [DOI] [PubMed] [Google Scholar]
- Wheeler, J. C. , Vanoni, S. , Zeng, C. , Waggoner, L. , Yang, Y. , Wu, D. , & Hogan, S. P. (2019). 17beta‐Estradiol protects the esophageal epithelium from IL‐13‐induced barrier dysfunction and remodeling. The Journal of Allergy and Clinical Immunology, 143(6), 2131–2146. 10.1016/j.jaci.2018.10.070 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1
Data Availability Statement
Deidentified data that support the findings of this study are available from the corresponding author upon reasonable request.