

Abstract
Background/Aims
The current study evaluates the efficacy and safety of the stand-alone implantation of the MINIject (iSTAR Medical, Wavre, Belgium) supraciliary, microinvasive glaucoma drainage device in patients with medically uncontrolled open-angle glaucoma.
Methods
This prospective, multicentre, first-in-human, single-arm interventional study evaluated stand-alone, ab interno implantation in 25 patients of a 5 mm long uveoscleral device made of STAR biocompatible material, which is a soft, microporous, flexible silicone. The primary outcome was the reduction of intraocular pressure (IOP) at 6 months compared with baseline, and follow-up continued until 2 years for 21 patients. Secondary outcomes included success defined as diurnal IOP of ≤21 mmHg and >5 mmHg with an IOP reduction of 20% without (complete) or with/without (qualified) glaucoma medication.
Results
Mean baseline IOP was 23.2±2.9 mmHg on 2.0±1.1 glaucoma medication ingredients and decreased to 13.8±3.5 mmHg (−40.7% reduction) on 1.0±1.3 medications 2 years after implantation. Complete success was achieved in 47.6% of patients (10/21) and qualified success in 100% of patients (21/21) at the 2-year follow-up. All patients achieved a 20% IOP reduction with 48% of patients medication-free. No serious ocular adverse events or additional glaucoma surgery were reported. Mean central endothelial cell density (ECD) mildly decreased from 2411 cells/mm2 (n=26) to 2341 cells/mm2 (n=21) at 24 months, which represents a 5% decrease for matched eyes. No patient had a ≥30% decrease in central ECD.
Conclusion
This first-in-human study on the stand-alone implantation of the MINIject supraciliary drainage system shows promising IOP-lowering results and medication reduction over 24 months with few adverse events.
Trial registration number
Keywords: Glaucoma, Intraocular pressure, Treatment surgery, Aqueous humour, Anterior chamber
Glaucomatous vision loss remains one of the main reasons for blindness across the world. 1 Traditionally, glaucoma is initially treated with topical drops, lasers and surgery as a last resort. All treatments are geared towards intraocular pressure (IOP) lowering. Given the significant morbidities associated with conventional glaucoma surgeries such as trabeculectomy and tube shunt procedures, minimally invasive glaucoma surgery (MIGS) was developed to help bridge the gap between topical/laser therapy and traditional filters. The ideal MIGS procedure allows for moderate IOP lowering and a good safety profile, while causing minimal tissue disruption. 2 There are a variety of MIGS options available, which can be classified into different subtypes either targeting Schlemm’s canal, supraciliary space or subconjunctival space.
The uveoscleral pathway accounts for 10–60% of aqueous outflow typically decreasing with age as extracellular fibrillar material accumulates in the ciliary muscle impeding aqueous drainage. 3–5 Renewed interest in this space has led to the development of devices that help enhance outflow through the uveoscleral pathway. The CyPass Microstent (Alcon, Vernier-Geneva, Switzerland) and the iStent Supra (Glaukos Corporation, San Clemente, CA, USA) have both been designed to stent the suprachoroidal space using tubular implants delivered through an ab interno approach. 6 7 The CyPass Microstent has recently been voluntarily withdrawn from the market due to concerns of endothelial cell loss as shown by the results of the COMPASS-XT trial, which was a 5-year extension of the initial pivotal COMPASS trial. 6 8 Several studies have shown promising IOP-lowering results with these suprachoroidal devices. 7 9
A novel implant has been developed targeting the suprachoroidal space: the MINIjectTM glaucoma drainage device (iSTAR Medical SA, Wavre, Belgium). 10 The device is inserted into the nasal quadrant of the eye through a 2 mm clear corneal incision. The MINIject implant is composed of a biocompatible porous silicone STAR® material. The unique flexible design conforms to the shape of the eye, and the micropores allow for enhanced aqueous outflow through the device. The STAR material has been shown to provide minimal tissue reaction, which is a promising feature of the implant given the risk of fibrosis. 11 The MINIject is 5 mm in length with an oblong cross-sectional design measuring 1.1×0.6 mm (figure 1). A green ring positioned at 0.5 mm from the tip of the device allows for accurate positioning in the anterior chamber. Preliminary 6-month results have been published previously. 10 The purpose of the current study is to evaluate the efficacy and adverse events of the stand-alone implantation of the MINIject glaucoma drainage device with a 2-year follow-up, and final study results are reported in this manuscript.
Figure 1.
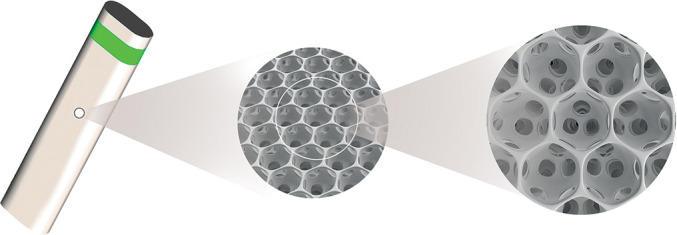
MINIject implant (iSTAR Medical, Wavre, Belgium) made of STAR material. Reprinted from Denis et al, 10 copyright (2019), with permission from Elsevier and the American Academy of Ophthalmology.
METHODS
This paper reports 2-year outcomes of a multicentre, prospective, open-label, single-arm trial, in which patients were implanted with the MINIject glaucoma drainage device between June and October 2017 by three surgeons (PD, CH, IKA) in Panama and India. The study adhered to the tenets of the Declaration of Helsinki, and institutional review board approval was obtained from all concerned hospitals (Maxivision Super Speciality Eye Hospital, Hyderabad, India; Panama Eye Centre, formerly Clinica de Ojos Orillac-Calvo, Panama City, Panama). Written informed consent was provided by all participants of the study.
Patients included were at least 18 years old, had primary open-angle glaucoma (POAG) with an angle grading of Schaffer 3 or 4 and IOP between 21 mmHg and 35 mmHg on one or more glaucoma medication classes. The main exclusion criteria were other types of glaucoma (angle closure, neovascular, uveitic), corneal or retinal disease, prior filtering glaucoma surgery and visual field (VF) defect within the central 10°. Methods were fully described in the previous preliminary paper. 10
A comprehensive slit-lamp exam was performed to ascertain study eligibility with one eye per patient enrolled. In summary, the implantation consists of injecting the device through a 2 mm clear corneal incision in the nasal suprachoroidal space while using a direct view gonioprism and viscoelastic. The implant was advanced until the middle of the green ring coincided with the level of the scleral spur. No antimetabolites were used during or after implantation.
Postoperatively corticosteroid drops and antibiotic drops were used as per the investigator’s discretion (25 of 26 eyes received topical antibiotics). Patients were seen following surgery at postoperative day 1, weeks 1 and 2 and months 1, 3, 6, 12, 18 and 24. All glaucoma medications were discontinued after the procedure. Glaucoma medications were re-introduced if IOP decreased <20%, or if IOP was at an unsafe level for the patient as per investigator discretion, or if glaucoma progression was noted on VF testing. IOP was measured at every visit with two readings obtained (a third was used if the two first readings differed by >2 mmHg). Diurnal IOP (08:00, 12:00 and 16:00) was measured at baseline, 6, 12, 18 and 24 months. Preoperative baseline data including demographics (age, gender, ethnicity), as well as ocular characteristics and history (glaucoma medications; glaucoma diagnosis and severity; cup-to-disc ratio; best-corrected visual acuity (BCVA) using ETDRS chart at 4 m; perimetry mean deviation (MD); history of laser trabeculoplasty, cataract surgery) were collected. VF testing using Humphrey Field Analyser (Carl Zeiss Meditec AG, Jena, Germany) was performed at baseline and months 1, 3, 6, 12, 18 and 24 with progression qualified as a loss of 3 dB or more from baseline MD. Other testing included optic nerve examination and photography, ultrasound biomicroscopy (UBM) assessing implant position, and specular microscopy at multiple time points. Adverse events were recorded for each patient, specific ocular symptoms were questioned at each visit (blurred vision, glare, halos, dryness and foreign-body sensation) and patients were asked to complete seven questions from the Collaborative Initiative Glaucoma Treatment Study (CIGTS) quality of life patient questionnaire at baseline and at the 6-, 12-, 18- and 24-month follow-up visits (online supplemental appendix 1). 12
bjophthalmol-2020-316888supp001.pdf (129.3KB, pdf)
The primary outcome of the study was reduction of IOP at 6 months. Secondary outcomes included success defined as diurnal IOP of ≤21 mmHg and >5 mmHg with an IOP reduction of 20% without the use of glaucoma medication (complete success) or regardless of the use of glaucoma medication (qualified success). Other secondary outcomes included reduction of IOP at other follow-up time points, reduction in glaucoma medication and adverse events. Results were reported based upon the intention-to-treat population. These results were further confirmed in a separate analysis of the per-protocol population. Data analysis was performed using SAS version 9.3, concomitant medications were classified using the WHO Drug Dictionary (2017 V1) and adverse events coded using the Medical Dictionary for Regulatory Activities (MedDRA Version 20.0).
RESULTS
There were 43 patients screened for enrolment with 26 meeting all inclusion criteria and included in the safety population. One enrolled patient did not receive the implant due to anatomical concerns at the time of implantation in a myopic eye. Thus, 25 eyes were implanted with the device. Twenty-one patients completed the 24-month follow-up, two patients died (unrelated to the study implant), one was lost to follow-up and one withdrew from the study without providing a reason.
In the safety population, patients had a mean age±SD of 69.4±11.1 years with 50% (n=13) pseudophakic and 58% (n=15) were using two or more glaucoma medication ingredients. Glaucoma severity was assessed as mild or moderate in 88.4% (n=23) with an MD of −8.9±6.9 dB. All patients had primary POAG with no history of laser trabeculoplasty. Baseline mean logMAR BCVA was 1.1±0.2. Additional demographic variables can be found in the previously published report. 10 Mean baseline IOP was 23.2±2.9 mmHg using a mean of 2.0±1.1 glaucoma medications. The primary endpoint at 6 months was met, with a signification reduction in IOP of 9.0 mmHg. 10
Results at 24 months
The mean reduction in IOP 24 months after surgery was 40.7% compared with baseline, to a mean diurnal IOP of 13.8±3.5 mmHg at 24 months. At months 6, 12 and 18, postoperative IOP decreased to 14.2±4.7 mmHg, 16.0±4.8 mmHg and 14.7±3.5 mmHg, respectively. Glaucoma medications decreased to a mean of 1.0±1.3 at 24 months, with 47.6% of patients (10/21 patients) medication-free. IOP and medication use throughout the follow-up period can be found in table 1 and figure 2. Qualified success was reached by 100% of patients (21/21) and complete success by 47.6% of patients (10/21). If applying a lower IOP cut-off of ≤18 mmHg in these definitions, qualified success would be 95.2% of patients (20/21) and complete success would be 42.9% (9/21) at the 24-month follow-up visit. Example UBM images can be found in figure 3. Furthermore, no additional glaucoma surgery was performed up to 24 months after MINIject implantation.
Table 1.
Baseline and postoperative intraocular pressure (IOP) values and number of medications used in the intention-to-treat population
| Baseline | 6 months | 12 months | 18 months | 24 months | |
|---|---|---|---|---|---|
| n | 25 | 24 | 24 | 22 | 21 |
| IOP (mmHg), mean (SD) | 23.17 (2.91) | 14.23 (4.74) | 16.00 (4.8) | 14.74 (3.49) | 13.76 (3.46) |
| IOP reduction (mmHg), mean (SD) | NA | 8.95 (3.69) | 7.17 (4.63) | 8.51 (3.79) | 9.55 (3.84) |
| IOP reduction (%), mean | NA | 39.07 | 30.83 | 36.24 | 40.65 |
| Medication-free eyes, number (%) | 0 | 21 (87.5) | 19 (79.1) | 14 (63.6) | 10 (47.6) |
| Medications per eye, mean (SD) | 2.0 (1.06) | 0.3 (0.74) | 0.4 (0.88) | 0.7 (1.09) | 1.0 (1.3) |
Figure 2.
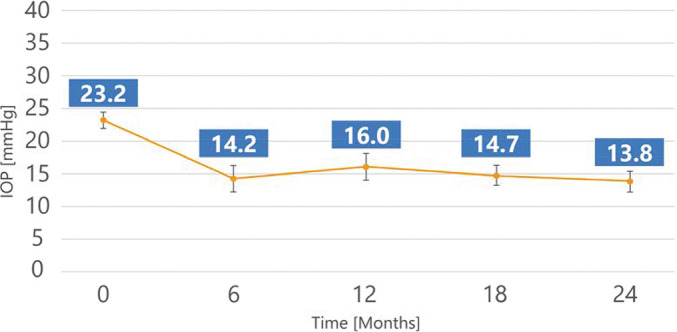
Mean intraocular pressure (mmHg) with 95% CI error bars from baseline to 24-month follow-up in the intention-to-treat population.
Figure 3.

Example ultrasound biomicroscopy images at week 1 (left) and 24-month (right) follow-up.
Quality of life
The results of the quality of life questionnaire show an absence or reduction in incidence for all symptoms at 24 months compared with those reported at baseline, indicating an improvement in patient quality of life. In particular, there were significant reductions (75–100%) in eye irritation/burning, eye pain, and skin sensitivity or irritation around the eye. There were also reductions (39–67%) in excessive tearing, red eyes and the sensation of a foreign presence in the eye. Outcomes from the quality of life questionnaire can be found in table 2.
Table 2.
Results of the quality of life patient questionnaire: whether the listed symptom was experienced in the last 7 days
| Symptom | Baseline (n=26) | 24 months (n=21) |
|---|---|---|
| Eye irritation/burning, n (%) | 5 (19) | 0 (0) |
| Eye pain, n (%) | 5 (19) | 1 (5) |
| Excessive tearing, n (%) | 8 (31) | 4 (19) |
| Droopy eyelid, n (%) | 0 (0) | 0 (0) |
| Red eye, n (%) | 5 (19) | 2 (10) |
| Feeling like something is in the eye, n (%) | 4 (15) | 1 (5) |
| Skin sensitivity or irritation around the eye, n (%) | 3 (12) | 0 (0) |
Adverse events
A complete list of ocular adverse events in the study eye can be found in table 3. The most frequent adverse events were anterior chamber reaction (8/26 patients, 30.8%), visual acuity reduced (8/26, 30.8%), VF defect (7/26, 26.9%), IOP elevation (5/26, 19.2%) and lenticular opacities (5/26, 19.2%). Visual acuity decreased nine times in eight patients with five events qualified as unrelated to the procedure and four possibly/probably related to the procedure (none related to the device). Two-thirds (6/9) of visual acuity reduction events resolved with cataract surgery, medications or spontaneously. Three patients had ongoing visual acuity reduction at the conclusion of the study of which two were related to cataracts (reduction of 20 letters and counting fingers) and one related to corneal oedema (counting fingers). The patient with corneal oedema had a preoperative endothelial cell density (ECD) count of 792 cells/mm2 due to a complicated cataract surgery several years prior causing endothelial trauma. The investigator expected corneal decompensation to continue over time. Corneal oedema developed in the central area (away from the MINIject implantation site) 24 months post-surgery, and the investigator assessed oedema as being unrelated to the study device. Mean VF was unchanged between baseline (MD: −8.9 dB, pattern SD (PSD): 5.0) and 24-month follow-up (MD: −8.7 dB, PSD: 5.5). VF loss of ≥3 dB was reported in seven patients varying from mild to moderate with 4/7 patients subsequently regaining the loss reported in their prior VF tests. Of these four patients, two had gains from cataract surgery and two patients were given medication or had spontaneous gains in VF. At the conclusion of the study, 3/7 patients had an ongoing VF loss: one patient with corneal oedema could not complete VF testing at 24 months and two patients had cataract progression with no surgery performed by study completion. Only one patient had IOP elevation ≥10 mmHg from baseline (after the 1-month follow-up visit), which met the protocol definition of substantial IOP increase. All IOP elevations resolved. One patient developed mild, transient hypotony on postoperative day 2, which resolved within 7 days. There were no changes in mean refraction in the study eye. There were no suprachoroidal haemorrhages and no additional glaucoma surgeries were required.
Table 3.
Number of patients in the safety population experiencing adverse ocular events in the study eye from post-surgery until study completion
| Adverse event | n (%) |
|---|---|
| Anterior chamber inflammation | 8 (30.8) |
| Visual acuity reduced | 8 (30.8) |
| Visual field defect | 7 (26.9) |
| Intraocular pressure increased* | 5 (19.2) |
| Lenticular opacities | 5 (19.2) |
| Hyphaema | 3 (11.5) |
| Conjunctival haemorrhage | 2 (7.7) |
| Eye pain | 2 (7.7) |
| Eye pruritus | 2 (7.7) |
| Cataract | 1 (3.8) |
| Cataract subcapsular | 1 (3.8) |
| Conjunctival oedema | 1 (3.8) |
| Corneal disorder | 1 (3.8) |
| Corneal oedema | 1 (3.8) |
| Cystoid macular oedema | 1 (3.8) |
| Detached Descemet’s membrane | 1 (3.8) |
| Glare | 1 (3.8) |
| Hypotony of eye | 1 (3.8) |
| Iatrogenic corectopia | 1 (3.8) |
| Macular fibrosis | 1 (3.8) |
| Posterior capsular opacification | 1 (3.8) |
| Punctate keratitis | 1 (3.8) |
| Vitreous haemorrhage | 1 (3.8) |
| Corneal abrasion | 1 (3.8) |
| Conjunctival foreign body | 1 (3.8) |
*Only one patient had a mean intraocular pressure (IOP) increase, which fulfilled the protocol definition of substantial IOP increase (≥10 mmHg higher than screening IOP after the 1-month postoperative visit).
n= number of patients.
Mean central ECD decreased from 2411 cells/mm2 (n=26) at baseline to 2341 cells/mm2 (n=21) at 24 months, representing a 5% decrease for matched patients. At 24-month follow-up, there were no patients with a central ECD loss of >=30% from baseline. BCVA and mean refraction remained the same throughout the study (mean logMAR BCVA change of 0.02±0.3 and mean change in refraction of −0.21±1.03 D). Two patient deaths during the follow-up period were deemed unrelated to the study (one died during sleep and one died as a result of pancreatic cancer). This was confirmed by the study’s independent Safety Monitoring Committee. Overall, there were no untoward safety concerns related to the device during the 24-month study.
DISCUSSION
This prospective, first-in-human, multicentre, single-arm study examined the efficacy, success, adverse events and the safety profile of a novel supraciliary implant, MINIject. At 24 months, the patients in this study had a mean reduction in IOP of 40.7% (9.6 mmHg), from medicated mean diurnal IOP of 23.2±2.9 mmHg at baseline to 13.8±3.5 mmHg at 24 months. A reduction of glaucoma medications was also shown from a mean of 2.0±1.1 to 1.0±1.3, with 47.6% of patients being medication free. Success, as defined by an IOP of ≤21 mmHg and >5 mmHg with an IOP reduction of 20%, was 47.6% for complete success (no glaucoma medications) and 100% for qualified success (with and without glaucoma medications). Studies have shown that when IOP has been significantly reduced to levels ≤18 mmHg, glaucoma progression could potentially be stopped and further damage to the optic nerve prevented. 13 14 In addition, the CIGTS showed that IOP reductions of 35% and 48% in a 5-year study were able to slow the progression of glaucoma. 15 In this study, 95.2% of patients had IOP ≤18 mmHg at 24-month follow-up and there was a mean reduction in IOP of 40.7%.
The IOP reduction and success rates in this study are considerable compared with other stand-alone MIGS devices targeting Schlemm’s canal or the supraciliary space. As MINIject was implanted in a stand-alone procedure, it is more appropriate to compare these results with other stand-alone studies. Cataract surgery is a potential confounder. Supraciliary devices provide the best comparators given the similar implantation location. Stand-alone CyPass (Alcon) implantation (n=65) was shown at 2 years in the DUETTE study to decrease IOP from a mean of 24.5±2.8 mmHg to 16.8±3.9 mmHg (−31% reduction) (n=32) with 56.3% having a 20% reduction of IOP from baseline and a mean medication reduction from 2.2±1.1 at baseline to 1.5±1.2 at 2 years. 16 At 2 years, 12 eyes (18.5%) required additional glaucoma surgery. 17 Success was defined as IOP between 6 and 21 mmHg on no medications (complete success: 29.2%) or on same or fewer medications (qualified success: 62.5%). The 2-year results are limited by a significant loss to follow-up (>50%). Another multicentre study examining real-world results for CyPass in the CyCLE trial (n=224) found a baseline IOP of 22.6±6.7 mmHg on a mean of 2.2±1.2 medications decreasing to 16.7±3.8 mmHg (-18% reduction) on 1.8±1.2 medications at 2 years (n=120) with 58% achieving 20% decrease in IOP from baseline. At 3 years, 32% required secondary glaucoma surgery. 18
Trabecular bypass stents can also serve as comparators although they target the conventional outflow pathway. The recent COMPARE trial 19 compared stand-alone 12-month outcomes of two iStent Trabecular Micro Bypass devices (Glaukos, San Clemente, CA, USA) with one Hydrus Microstent (Ivantis, Irvine, CA, USA). At baseline, mean medicated IOP was 19.0±3.9 (Hydrus, n=77) and 19.1±3.6 mmHg (2-iStent, n=77) on a mean of 2.5±0.7 (Hydrus) and 2.7±0.8 (2-iStent) medications. At 12 months, mean IOP decreased to 17.3±3.7 (Hydrus) and 18.1±3.7 mmHg (2-iStent) on 1.0±0.3 (Hydrus) and 1.7±0.3 (2-iStent) medications, and these results were sustained to 24 months. At 24 months, the unpublished data made available on the company website states that 63% of of patients in the Hydrus group compared to 40% of of patients in the 2-iStent group obtained a 20% IOP reduction. Also, medication use decreased by a mean of 1.3 medications (52%) with 38% of patients medication-free in the Hydrus group, compared to a reduction of 0.8 medications (29%) with 19% of patients medication-free in the 2-iStent group. No patients in the Hydrus group required reoperation as opposed to 9% in the 2-iStent group. 20 There are many iStent studies that have shown varied amounts of IOP and medication reduction with stand-alone implantation. 21–26
Another stand-alone study comparing Hydrus to selective laser trabeculoplasty up to 1 year found similar results with stand-alone Hydrus implantation (n=31) with a reduction of IOP from 23.1±5.1 mmHg on 2.3±0.8 medications at baseline to 16.5±2.6 mmHg (26% reduction) on 0.9±1.0 medications, although at only 12-month follow-up, with 47% remaining medication free. 27
In comparison to these supraciliary and trabecular bypass studies, in our sample, mean baseline IOP was 23.2±2.9 mmHg on 2.0±1.1 glaucoma medications and decreased to 13.8±3.5 mmHg (40.7% reduction) on 1.0±1.3 glaucoma medications. All patients achieved at least 20% IOP reduction with 48% of patients medication-free at the 2-year follow-up. In addition, no patients required further glaucoma surgery. Our study results show a trend towards considerably greater IOP reduction sustained up to a follow-up period of 24 months, with similar medication reduction, compared to the studies listed earlier.
Aside from stenting procedures, trabeculotomies have also shown similar IOP-lowering capabilities using devices such as the Trabectome (MicroSurgical Technology, Redmond, WA, USA) and the Kahook Dual Blade (KDB) (New World Medical, Rancho Cucamonga, CA, USA). A review article of the Trabectome literature has shown that the stand-alone procedure decreased IOP by a weighted mean difference of −9.8±0.9 mmHg with −1.1±0.5 less glaucoma medications at 2 years. 28 The overall success rates using final IOP ≤21 mmHg and 20% decrease in IOP from baseline were 61±17% at 1 year and 46±34% at 2 years. There was no indication of medication use to qualify success in these studies. Another stand-alone KDB study (n=16) with only 12-month follow-up was shown to decrease IOP and medications from a baseline 20.4±1.3 mmHg on 3.1±0.2 medications to 14.1±0.9 mmHg on 2.3±0.4 medications. 29 Complications such as hyphemas (up to 100% in Trabectome studies) and sustainability concerns are potential drawbacks to these procedures.
Finally, subconjunctival MIGS have also been studied as a stand-alone procedure. A prospective 2-year, multicentre series on the Xen gel stent (Allergan, Dublin, Ireland) has shown in stand-alone implantation (n=106) a reduction of IOP from a baseline of 21.7±3.8 mmHg on 2.7±0.9 medications to 15.4±5.2 mmHg (28.2% reduction) on 1.2±1.2 medications. 30 Of note, subconjunctival MIGS have several significant differences compared with other ab interno MIGS, as they completely bypass the conventional and uveoscleral pathways of aqueous humour drainage by creating a filtering bleb with mitomycin use and potential risks of infection and hypotony. They also require a more intensive postoperative follow-up and potential needling (41%). 30
Investigators from the CIGTS have suggested that quality-of-life perception may be even more important for patients than small differences in treatment results, even if those differences are statistically or clinically significant. The quality of life questionnaire completed by patients in this study showed an improvement or absence in all areas measured. 12 In particular, there were marked reductions (50–100%) in eye irritation/burning, eye pain and excessive tearing, which could be attributed to the reduction in medication burden with around half of the patients on no medications at final follow-up. Also, a reduction in foreign-body sensation (75%), and skin sensitivity or irritation around the eye (100%) were noted.
There were few adverse events during the study. The most common ones were transient inflammation and IOP elevations. These are quite common after MIGSs and resolved with conservative therapy or spontaneously. Cataract surgery is often anticipated when performing MIGS in a phakic patient, particularly since some patients had pre-existing cataracts at baseline, and considering the mean age of patients and the duration of the study. Indeed, 3/13 phakic patients (23%) in our study had cataract surgery in the study eye during the study period. Of these three eyes, two had pre-existing mild/moderate cataracts at baseline. In comparison, Grisanti et al reported 19/75 phakic patients (25%) had cataract surgery up to 2 years after CyPass implantation. 18 The DUETTE study found 11/41 phakic patients (27%) had cataract surgery up to 24-month follow-up. 17 Another potential concern is ECD loss, as seen with the CyPass device, which ultimately led to its withdrawal from the market. 31 ECD results after MINIject implantation have shown minimal ECD loss at 2 years, which is encouraging. This could be due to MINIject’s soft and conforming material, as well as its design which minimises the amount of material in the anterior chamber (0.5 mm). ECD results in this study will continue to be monitored up to 5 years. Being an ab interno, bleb-free, supraciliary procedure, there were no adverse events associated with blebs, needling or revision surgery, and no MMC-related complications due to the prohibition of MMC use per study protocol.
Despite the fact that a direct comparison is challenging, these data indicate that MINIject has shown a trend towards greater IOP and medication reduction compared to current MIGS options, with results sustained out to 24 months. These promising results were achieved alongside improved quality of life indicators, with no untoward safety concerns, and with minimal reduction in ECD levels.
Limitations of this study include its non-comparative design. Overall, it is difficult to compare all these different procedures by simply looking at IOP and medication reduction, due to many different factors that affect surgical success including age, disease severity, glaucoma type, surgical technique, preoperative IOP, preoperative medication use, etc. The small sample size and limited sites/surgeons decrease the generalisability of the results, which is common in first-in-human trials. There were no untoward safety concerns throughout the study. As is the case with many glaucoma trials, IOP is an imperfect measure of glaucoma control. VF testing was performed to assess progression during the trial, but there was a significant learning curve for patients, and testing was not systematically repeated in case of significant VF changes.
This first-in-human study on the MINIject drainage system shows significant IOP and medication reduction over 24 months with few adverse events. The risk of fibrosis and device failure is an ongoing concern with any glaucoma surgery. The proprietary STAR material has shown a minimal inflammatory response in rabbits 11 , supported clinically by the results in this study which show sustained IOP lowering up to 24 months. As with any MIGS device, these results need to be confirmed with a larger sample of patients and long-term studies.
Acknowledgments
The study investigators would like to thank the independent members of the Safety Monitoring Committee: A.G. Jünemann MD (Rostock University, Rostock, Germany); R.D. Fechtner MD (SUNY Upstate Medical University, NY, USA); R.A. Eiferman MD (University of Louisville, Louisville, USA); L.H. Silver PhD (Silver Pharma Consulting Inc., El Paso, Texas, USA). The authors acknowledge statistical analyses by Nicolas Dubois, MSc, and Koenraad D’Hollander, MD, MSc (IDDI, Louvain-la-Neuve, Belgium), clinical operations support by Ljubomir Manola, PhD (iSTAR Medical, Wavre, Belgium), and writing and editorial assistance provided by Katherin Awad, BSc, MBA.
Footnotes
Funding: iSTAR Medical (Wavre, Belgium) has directly sponsored the STAR-I study. The sponsor participated in the design of the study, conducting the study and review of the manuscript. There is no grant number.
Competing interests: PD: iSTAR Medical, Alcon, Allergan, Glaukos, Santen, Thea; CH: iSTAR Medical, Thea Pharma; GMD: Alcon, Allergan, Bausch & Lomb, Glaukos, Labtician, Novartis, MST, Santen, Sight Sciences; KPR, AK, EC: no financial interests; ZH: Vice President of Regulatory and Clinical at iSTAR Medical; IKA: Aequus, Aerie Pharmaceuticals, Alcon, Allergan, ArcScan, Bausch & Lomb, Beaver Visitec, Camras Vision, Carl Zeiss Meditec, CorNeat Vision, Ellex, ElutiMed, Equinox, Genentech, Glaukos, Gore, Iantech, InjectSense, Iridex, iSTAR Medical, Ivantis, Johnson & Johnson Vision, KeLoTec, LayerBio, Leica Microsystems, MicroOptx, New World Medical, Omega Ophthalmics, PolyActiva, Sanoculis, Santen, Science Based Health, Sight Sciences, Stroma, TrueVision, Vizzari.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data are available upon reasonable request. Data may be obtained from a third party and are not publicly available.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
REFERENCES
- 1. Tham YC, Li X, Wong TY, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology 2014;121:2081–90. 10.1016/j.ophtha.2014.05.013 [DOI] [PubMed] [Google Scholar]
- 2. Saheb H, Ahmed II. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol 2012;23:96–104. 10.1097/ICU.0b013e32834ff1e7 [DOI] [PubMed] [Google Scholar]
- 3. Becker B, Neufeld A. Pressure dependence of uveoscleral outflow. J Glaucoma 2002;11:545. 10.1097/00061198-200210000-00017 [DOI] [PubMed] [Google Scholar]
- 4. Bill A. Some aspects of aqueous humour drainage. Eye 1993;7:14–19. 10.1038/eye.1993.4 [DOI] [PubMed] [Google Scholar]
- 5. Alm A, Nilsson SF. Uveoscleral outflow: a review. Exp Eye Res 2009;88:760–8. 10.1016/j.exer.2008.12.012 [DOI] [PubMed] [Google Scholar]
- 6. Vold S, Ahmed II, Craven ER, et al. Two-year COMPASS trial results: supraciliary microstenting with phacoemulsification in patients with open-angle glaucoma and cataracts. Ophthalmology 2016;123:2103–12. 10.1016/j.ophtha.2016.06.032 [DOI] [PubMed] [Google Scholar]
- 7. Myers JS, Masood I, Hornbeak DM, et al. Prospective evaluation of two iStent((R)) trabecular stents, one istent supra((R)) suprachoroidal stent, and postoperative prostaglandin in refractory glaucoma: 4-year outcomes. Adv Ther 2018;35:395–407. 10.1007/s12325-018-0666-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Ianchulev T, Lane S, Masis M, et al. Corneal endothelial cell density and morphology after phacoemulsification in patients with primary open-angle glaucoma and cataracts: 2-year results of a randomized multicenter trial. Cornea 2019;38:325–31. 10.1097/ICO.0000000000001826 [DOI] [PubMed] [Google Scholar]
- 9. Vinod K. Suprachoroidal shunts. Curr Opin Ophthalmol 2018;29:155–61. 10.1097/ICU.0000000000000458 [DOI] [PubMed] [Google Scholar]
- 10. Denis P, Hirneiss C, Reddy K, et al. A first-in-human study of the efficacy and safety of MINIject in patients with medically uncontrolled open angle glaucoma (STAR-I). Ophthalmol Glaucoma 2019;2:290–7. 10.1016/j.ogla.2019.06.001 [DOI] [PubMed] [Google Scholar]
- 11. Grierson I, Minckler D, Rippy MK, et al. Pre-clinical experience of STAR material. European Society of Cataract and Refractive Surgery Annual Meeting . Vienna: Austria. 2018. [Google Scholar]
- 12. Janz N, Wren P, Lichter P, et al. The collaborative initial glaucoma treatment study: interim quality of life findings after initial medical or surgical treatment of glaucoma. Ophthalmology 2001;108:1954–65. 10.1016/S0161-6420(01)00874-0 [DOI] [PubMed] [Google Scholar]
- 13. The Advanced Glaucoma Intervention Study (AGIS) . 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS Investigators. Am J Ophthalmol 2000;130:429–40. 10.1016/S0002-9394(00)00538-9 [DOI] [PubMed] [Google Scholar]
- 14. Vogel R, Crick R, Newson R, et al. Association between intraocular pressure and loss of visual field in chronic simple glaucoma. Br J Ophthalmol 1990;74:3–6. 10.1136/bjo.74.1.3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Lichter PR, Musch DC, Gillespie BW, et al. Interim clinical outcomes in the collaborative initial glaucoma treatment study comparing initial treatment randomized to medications or surgery. Ophthalmology 2001;108:1943–53. 10.1016/S0161-6420(01)00873-9 [DOI] [PubMed] [Google Scholar]
- 16. Garcia-Feijoo J, Hoh H, Uzunov R, et al. Supraciliary microstent in refractory open-angle glaucoma: two-year outcomes from the DUETTE trial. J Ocul Pharmacol Ther 2018;34:538–42. 10.1089/jop.2018.0036 [DOI] [PubMed] [Google Scholar]
- 17. García-Feijoo J, Rau M, Grisanti S, et al. Supraciliary micro-stent implantation for open-angle glaucoma failing topical therapy: 1-year results of a multicenter study. Am J Ophthalmol 2015;159:1075–81. 10.1016/j.ajo.2015.02.018 [DOI] [PubMed] [Google Scholar]
- 18. Grisanti S, Grisanti S, Garcia-Feijoo J, et al. Supraciliary microstent implantation for open-angle glaucoma: multicentre 3-year outcomes. BMJ Open Ophthalmol 2018;3:e000183. 10.1136/bmjophth-2018-000183 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Ahmed IIK, Fea A, Au L, et al. A prospective randomized trial comparing Hydrus and iStent microinvasive glaucoma surgery implants for standalone treatment of open-angle glaucoma: the COMPARE study. Ophthalmology 2020;127:52–61. 10.1016/j.ophtha.2019.04.034 [DOI] [PubMed] [Google Scholar]
- 20. Ivantis announces 24-month results of landmark prospective, randomized comparative MIGS clinical trial. 2019. Available https://www.ivantisinc.com/newsroom/ivantis-announces-24-month-results/
- 21. Chang DF, Donnenfeld ED, Katz LJ, et al. Efficacy of two trabecular micro-bypass stents combined with topical travoprost in open-angle glaucoma not controlled on two preoperative medications: 3-year follow-up. Clin Ophthalmol 2017;11:523–8. 10.2147/OPTH.S121041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Lindstrom R, Lewis R, Hornbeak DM, et al. Outcomes following implantation of two second-generation trabecular micro-bypass stents in patients with open-angle glaucoma on one medication: 18-month follow-up. Adv Ther 2016;33:2082–90. 10.1007/s12325-016-0420-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Berdahl J, Voskanyan L, Myers JS, et al. Implantation of two second-generation trabecular micro-bypass stents and topical travoprost in open-angle glaucoma not controlled on two preoperative medications: 18-month follow-up. Clin Exp Ophthalmol 2017;45:797–802. 10.1111/ceo.12958 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Fea AM, Belda JI, Rekas M, et al. Prospective unmasked randomized evaluation of the iStent inject ((R)) versus two ocular hypotensive agents in patients with primary open-angle glaucoma. Clin Ophthalmol 2014;8:875–82. 10.2147/OPTH.S59932 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Ahmed II, Katz LJ, Chang DF, et al. Prospective evaluation of microinvasive glaucoma surgery with trabecular microbypass stents and prostaglandin in open-angle glaucoma. J Cataract Refract Surg 2014;40:1295–300. 10.1016/j.jcrs.2014.07.004 [DOI] [PubMed] [Google Scholar]
- 26. Vold SD, Voskanyan L, Tetz M, et al. Newly diagnosed primary open-angle glaucoma randomized to 2 trabecular bypass stents or prostaglandin: outcomes through 36 months. Ophthalmol Ther 2016;5:161–72. 10.1007/s40123-016-0065-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Fea AM, Ahmed II, Lavia C, et al. Hydrus microstent compared to selective laser trabeculoplasty in primary open angle glaucoma: One year results. Clin Exp Ophthalmol 2017;45:120–7 10.1111/ceo.12805. [DOI] [PubMed] [Google Scholar]
- 28. Kaplowitz K, Bussel II, Honkanen R, et al. Review and meta-analysis of ab-interno trabeculectomy outcomes. Br J Ophthalmol 2016;100:594–600. 10.1136/bjophthalmol-2015-307131 [DOI] [PubMed] [Google Scholar]
- 29. Sieck E, Epstein R, Kennedy J, et al. Outcomes of Kahook Dual Blade goniotomy with and without phacoemulsification cataract extraction. Ophthalmol Glaucoma 2018;1:75–81. 10.1016/j.ogla.2018.06.006 [DOI] [PubMed] [Google Scholar]
- 30. Reitsamer H, Sng C, Vera V, et al. Two-year results of a multicenter study of the ab interno gelatin implant in medically uncontrolled primary open-angle glaucoma. Graefes Arch Clin Exp Ophthalmol 2019;257:983–96. 10.1007/s00417-019-04251-z [DOI] [PubMed] [Google Scholar]
- 31. Alcon announces voluntary global market withdrawal of CyPass Micro-Stent for surgical glaucoma. 2018. Available https://www.alcon.com/media-release/alcon-announces-voluntary-global-market-withdrawal-cypass-micro-stent-surgical
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bjophthalmol-2020-316888supp001.pdf (129.3KB, pdf)