

Abstract
Odontomas are the most commonly occurring odontogenic tumor, and earlier they were considered developmental anomaly as the morphodifferentiation of ameloblast does not occur in odontomas. Odontomas are considered hamartoma rather than true neoplasms as histologically they contain odontogenic tissues which are native to the oral cavity. These odontomas are usually asymptomatic and are revealed in radiographic examination but can also present with over-retained deciduous teeth and malocclusion and with other local complications such as infection. Etiology of odontomas is considered to be from genetic, local environmental, and systemic factors. Broadly based on their radiologic and clinical features, they are classified into two types: compound composite odontomas and complex composite odontomas. The odontomas which resemble teeth are called compound composite odontomas and which do not resemble teeth are called complex composite odontomas. Odontomas are called composite odontomas as they contain both epithelial and mesenchymal derivatives. Here, we report two cases of compound composite odontoma, and a case of complex composite odontoma with relevant review of literature.
KEYWORDS: Complex composite odontoma, compound composite odontoma, surgical excision
INTRODUCTION
The odontomas were introduced by Paul Braco in 1867 referred it as tumors formed by overgrowth of dental tissues.[1] It consists of both epithelial and connective tissue component both exhibiting the complete differentiation to ameloblast and odontoblast.[2] Histologically, the enamel and dentin found in odontomas are not laid down in normal fashion as the organization of odontogenic cells fail to occur, the ameloblast and odontoblast do not undergo morphodifferentiation. Thus, odontomas are considered to be developmental anomaly than odontogenic tumor.[3] The incidence of odontomas is as high as 22% of all the odontogenic tumors where compound odontomas comprises 9% of odontogenic tumors.[4] Odontomas occur mostly in permanent dentition and are very rarely found in deciduous dentition.[5]
THE ETIOLOGY OF ODONTOMAS HAS BEEN RELATED TO VARIOUS FACTORS
Growth pressure of the developing tooth germ as per Hitchin et al.[6]
Infection of deciduous predecessor[7]
Mature ameloblast[8]
Epithelial remnants the cell rest of series[9]
Extraneous odontogenic epithelium as the tooth germ divides or conglomerate to form odontoma[10]
Trauma to the predecessor can cause odontoma formation[11]
Genetic factors according to Papagerakis et al.[12]
Lack of gene control over tooth development is a causative factor, gene mutation, inheritance of mutated gene, and manifest in various syndromes such as Gardner syndrome, familial colonic adenomatosis, Gorlin syndrome, Tangier disease, or Hermann syndrome.[13]
Here, we report three cases of odontomas, one being multiple compound composite odontoma of maxilla, second being compound composite odontoma of maxilla, and other complex composite odontoma of mandible.
CASE REPORT
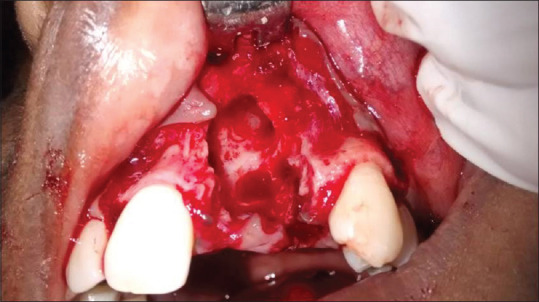
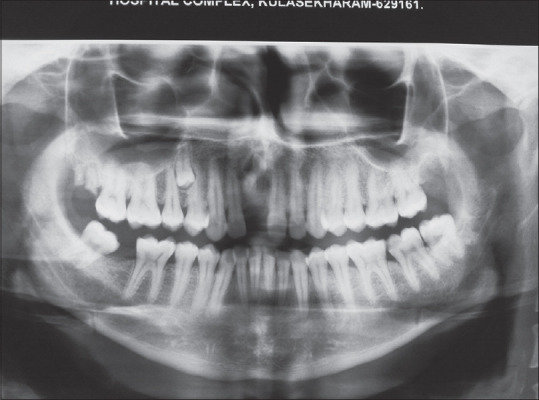
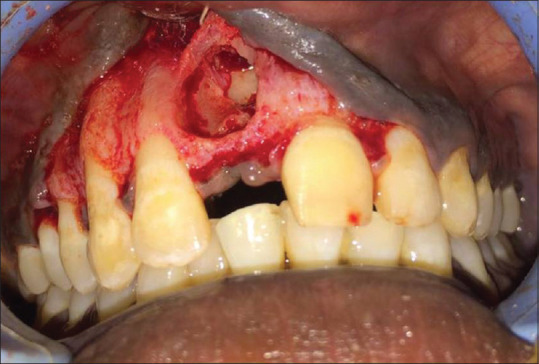
A 21-year-old female had a complaint of retained primary teeth and wanted its prosthetic rehabilitation in left upper front region of jaw. Intraoral examination showed missing 21, decayed 22, and retained 61, 62. The orthopantamogram [Figure 1] showed multiple teeth such as structures in relation to retained deciduous 61, 62, and impacted 21. After diagnosing the swelling as multiple compound composite odontoma radiographically, the treatment plan of extraction of decayed 22, surgical excision of odontomas, and surgical extraction of 21 under local anesthesia was proposed. Under aseptic precaution and under local anesthesia, a crevicular incision was placed extending from 12 to 23 was made. After the extraction of retained deciduous 61, 62, and 22, a buccal bone window was created to expose the odontomas [Figure 2], and after adequate bone removal, nine odontomas were luxated and extracted into along with impacted 21 [Figures 3 and 4]. The incision was closed after achieving hemostasis. The patient's postoperative period was uneventful and histopathological examination confirmed lesion to be odontomas
A 32-year-old male patient came with the complaint of missing tooth 11 which was extracted due to decay 1-year before, and the patient was asymptomatic. On radiographic examination of edentulous ridge, a tooth like radioopacity surrounded by a radiolucent halo was seen, suggesting of a compound composite odontoma and the patient also had impacted supernumerary supplementary premolar in relation to 14 [Figure 5]. After a thorough systemic examination, the treatment plan of surgical excision was proposed. Under local anesthesia and aseptic precautions, a vestibular incision extending from 13 to 22 was made, and the flap was reflected, a bone window was created in the labial side to expose the odontoma [Figure 6] after adequate bone removal, the odontoma was extracted [Figure 7]. The supernumerary premolar was surgically extracted by palatal approach [Figure 8] through a separate palatal incision from 13 to 16. After achieving hemostasis, the wound was closed. The patient's postoperative phase was uneventful
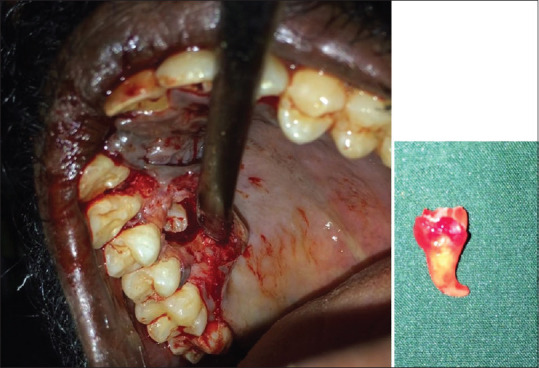
A 28-year-old female reported with a small swelling in relation to buccal vestibule of the 46 [Figure 9]. The patient was asymptomatic except for the radiopaque ill-defined mass in the orthopantamogram [Figure 10]. As the patient had no systemic illness, treatment plan of surgical excision under local anesthesia was proposed. Under aseptic precaution, under local anesthesia, a crevicular incision was placed from 44 to 47, and a bone window was created to expose the odontoma; after adequate bone removal, the odontoma was extracted and the incision was closed after achieving hemostasis [Figure 11]. The postoperative phase of the patient was uneventful and histopathological examination confirmed the lesion to be a complex composite odontoma.
Figure 1.

Orthopantamogram showing multiple compound composite odontoma
Figure 2.

Exposure of the denticles by crevicular incision
Figure 3.
After surgical excision of the denticles
Figure 4.
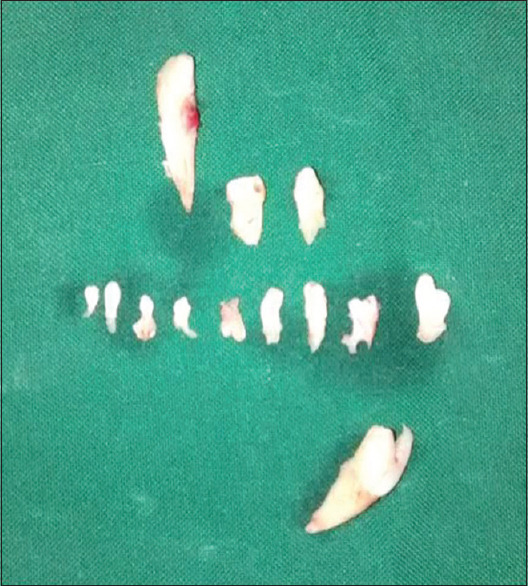
Nine denticles along with extracted teeth 61, 62, 22, and 21
Figure 5.
Orthopantonogram showing compound composite odontoma and impacted supernumerary premolar
Figure 6.
After adequate exposure, the compound odontoma
Figure 7.

Compound composite odontoma
Figure 8.
Supernumerary premolar extracted through palatal approach
Figure 9.

Swelling in the buccal attached gingiva in relation to 46
Figure 10.
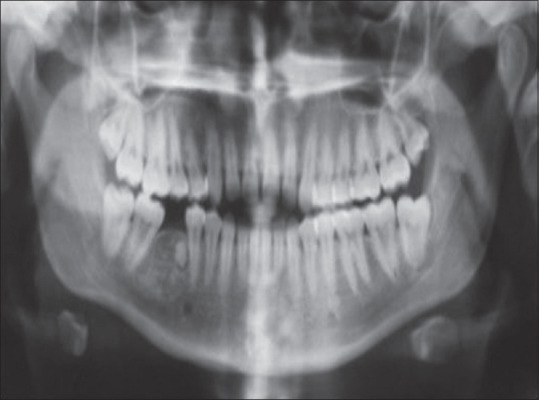
Orthopantomogram showing complex composite odontome
Figure 11.
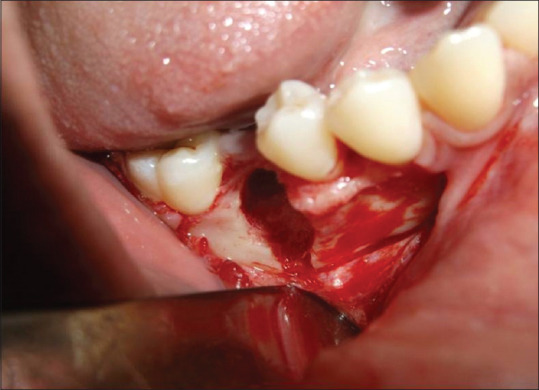
Image of surgical site after extraction of odontome present
REVIEW OF LITERATURE
According to Robinson 1952, odontomas are tumors originating from odontogenic tissues, i.e. it includes all the odontogenic tumors but later the term was restricted to the tumors which had dental hard-tissue formation.[14] Odontomas are considered hamartomas rather than a true neoplasm.[15] Based on gross, microscopic, and radiographic appearance, the odontomas can be classified as complex composite odontomas and compound composite odontoma.[16]
The WHO classified odontomas as ameloblastic fibro- odontoma, ameloblastic odontoma, complex odontoma, and compound odontoma. Ameloblastic odontoma and ameloblastic fibro-odontoma consist of ameloblastic and fibrous tissue, respectively, apart from tooth-like structure.[17] According to Gabel, James, and Payne, the odontomas are classified based on origin as epithelial, composite, and connective tissue.[18] According to Vengal et al., the odontomas can be classified based on their position as intraosseous and extraosseous.[19] According to Thoma and Goldman, the odontomas can be classified into geminated composite odontomas, compound composite odontomas, dilated odontomas, and cystic odontomas. Geminated composite odontomas are well-defined odontomas called as denticles fused together, compound composite odontomas resemble teeth, while complex composite odontomas do not resemble teeth, dilated odontomas have dilated root canal and cystic odontomas have fibrous encapsulation around them.[20] Mostly the odontomas are asymptomatic and only few shows delayed eruption, swelling, and infection.[21] Compound odontomas show bony expansion than composite odontomas. The other manifestations include aplasia, malposition, retention, impaction, malformation, and devitalization of adjacent teeth.[22]
Table 1 enumerates the differences between the complex composite and compound composite odontomas.
Table 1.
Differences between the complex composite and complex composite odontomas
| Compound odontoma | Complex odontoma | |
|---|---|---|
| Shape | Regular | Amorphous[23] |
| Number | Single or multiple | Single[24] |
| Incidence | 9%-37% | 5%-30%[25] |
| Sex predilection | Female | Female[5] |
| Mean age | 14.8-20.3 | 14.8-20.3[26] |
| Site | Maxillary anterior | Mandibular posteriors[27] |
| Radiologically | Well defined tooth like structure | Irregular calcified structure[28] |
| Histologically | Layers of dentin and enamel around pulp like tissue | Haphazardly arranged enamel, dentin, cementum and pulpal tissue[29] |
Multiple odontomas are associated with cleidocranial dysostosis, Gardner's syndrome.[30] According to Bader and Schimidser, other manifestations include pulmonary or aortic stenosis, esophageal stenosis, pneumonia, and bronchiectasis.[31] Apart from systemic signs, local signs such as swelling, delayed eruption, widespread involvement of other facial bones, and eruption of odontomas into oral cavity.[32]
Table 2 shows the incidence of multiple compound composite odontoma with their relation to systemic symptoms.
Table 2.
Incidence of multiple compound composite odontoma with their relation to systemic symptoms
Multiple compound odontomas occur predominantly in the cuspids and incisors as seen in the above case report, followed by mandibular ramus where there are reports with more than 300 denticles.[35] The multiple compound odontomas case reported here shows nine denticles in one jaw maxilla without any systemic symptoms. Lopez-Areal L et al. reported the highest number of 2000 denticles found bilaterally in both jaws.[36] The other regions involved are hard palate, mental foramen, subcondyle region, and middle ear.[37]
CONCLUSION
Although the odontomas are asymptomatic and have limited growth, potential, early diagnosis, and surgical excision are necessary to avoid complications such as cystic changes and malocclusion resulting from the displacement of adjacent permanent teeth. Even though recurrence is rare, complete excision in the case of complex composite odontoma is critical.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient (s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
The study was self-funded.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Sprawson E. Odontomas. Br Dent J. 1937;62:177–201. [Google Scholar]
- 2.Amado Cuesta S, Gargallo Albiol J, Berini Aytés L, Gay Escoda C. Review of 61 cases of odontoma. Presentation of an erupted complex odontoma. Med Oral. 2003;8:366–73. [PubMed] [Google Scholar]
- 3.Shafer GW, Hine MK, Levy BM. A Textbook of Oral Pathology. 4th ed. Philadelphia: WB Saunders; 1983. pp. 308–11. [Google Scholar]
- 4.Bhaskar SN. Odontogenic Tumors of Jaws in Synopsis of Oral Pathology. 7th ed. New York: Mosby; 1986. pp. 292–303. [Google Scholar]
- 5.Malik SA. Odontomatosis (multiple odontomas) – A case report. Br J Oral Surg. 1974;11:262–4. doi: 10.1016/0007-117x(74)90112-7. [DOI] [PubMed] [Google Scholar]
- 6.Hitchin AD, Ferguson HW. Odontome: A breif overview. Dent Rec. 1958;78:309. [Google Scholar]
- 7.Hitchin AD. The aetiology of the calcified composite odontomas. Br Dent J. 1971;130:475–82. doi: 10.1038/sj.bdj.4802682. [DOI] [PubMed] [Google Scholar]
- 8.Torreti EF, Carrel R. Compound odontoma in a 12-year-old child. J Dent Child. 1983;50:376–8. [PubMed] [Google Scholar]
- 9.Fijerskov O. Odontogenesis. In: Mjor IA, Fejerskov O, editors. Histology of the Human Tooth. Copenhagen: Munksgaard; 1979. pp. 21–31. [Google Scholar]
- 10.Smith RM, Tuner JE, Ribbins ML. Atlas of Oral Pathology. St. Louis: CV Mosby; 1981. pp. 54–6. [Google Scholar]
- 11.Andreasen JO. Injuries to developing teeth. In: Andreasen JO, Andreasen FM, editors. Textbook and Color Atlas of Traumatic Injuries to the Teeth. 3rd ed. Copenhagem: Mosby; 1994. pp. 457–94. [Google Scholar]
- 12.Papagerakis P, Peuchmaur M, Hotton D, Ferkdadji L, Delmas P, Sasaki S, et al. Aberrant gene expression in epithelial cells of mixed odontogenic tumors. J Dent Res. 1999;78:20–30. doi: 10.1177/00220345990780010201. [DOI] [PubMed] [Google Scholar]
- 13.Hidalgo-Sánchez O, Leco-Berrocal MI, Martínez-González JM. Metaanalysis of the epidemiology and clinical manifestations of odontomas. Med Oral Patol Oral Cir Bucal. 2008;13:E730–4. [PubMed] [Google Scholar]
- 14.Robinson HB. Proceedings of the 5th Annual Meeting of the American Academy of Oral Pathology. Oral Surg. 1952;5:177. [Google Scholar]
- 15.Shekar SE, Roopa SR, Gunasheela B, Supriya N. Erupted compound odontoma. J Oral Maxillofac Pathol. 2009;13:47–50. doi: 10.4103/0973-029X.48758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kramer IR, Pindborg JJ, Shear M. International Histological Classification of Tumors. 2nd ed. Berlin: Springer; 1992. Histological Typing of Odontogenic Tumor. WHO; pp. 16–21. [Google Scholar]
- 17.Pindborg JJ, Kramer IR, Torloni H. International Histological Classification of Tumors. Vol. 5. Geneva: World Health Organization; 1970. Histological typing of odontogenic tumors, jaw cysts and allied lesions; pp. 29–30. [Google Scholar]
- 18.Singh S, Singh M, Singh I, Khandelwal D. Compound composite odontomaassociated with an unerupted deciduous incisor – A rarity. J Indian Soc Pedod Prev Dent. 2005;23:146–50. doi: 10.4103/0970-4388.16889. [DOI] [PubMed] [Google Scholar]
- 19.Vengal M, Arora H, Ghosh S, Pai KM. Large erupting complex odontoma: A case report. J Can Dent Assoc. 2007;73:169–73. [PubMed] [Google Scholar]
- 20.Thoma KM, Goldmn HM. Oral Pathology. 5th ed. St. Louis: The CV Mosby Company; 1960. pp. 1221–2. [Google Scholar]
- 21.Miki Y, Oda Y, Iwaya N, Hirota M, Yamada N, Aisaki K, et al. Clinicopathological studies of odontoma in 47 patients. J Oral Sci. 1999;41:173–6. doi: 10.2334/josnusd.41.173. [DOI] [PubMed] [Google Scholar]
- 22.Owens BM, Schuman NJ, Mincer HH, Turner JE, Oliver FM. Dental odontomas: A retrospective study of 104 cases. J Clin Pediatr Dent. 1997;21:261–4. [PubMed] [Google Scholar]
- 23.Cawson RA, Binnie WH, Eveson JW. Hong Kong: Mosby-Wolfe; 1993. Color Atlas of Oral Disease Clinical and Pathological Correlations; pp. 6–19. [Google Scholar]
- 24.Tomizawa M, Otsuka Y, Noda T. Clinical observations of odontomas in Japanese children: 39 cases including one recurrent case. Int J Paediatr Dent. 2005;15:37–43. doi: 10.1111/j.1365-263X.2005.00607.x. [DOI] [PubMed] [Google Scholar]
- 25.Philpsen HP, Reichert PA, Ractorious F. Mixed odontogenic tumors and odontomas. Considerations on interrelationship. Review of literature and presentation of 134 new cases of odontomas. Oral Onocol. 1997;33:86–87. doi: 10.1016/s0964-1955(96)00067-x. [DOI] [PubMed] [Google Scholar]
- 26.Slootweg PJ. An analysis of the interrelationship of the mixed odontogenic tumors – ameloblastic fibroma, ameloblastic fibro-odontoma, and the odontomas. Oral Surg Oral Med Oral Pathol. 1981;51:266–76. doi: 10.1016/0030-4220(81)90056-6. [DOI] [PubMed] [Google Scholar]
- 27.Cobos L, Brzovic F, Ladron de Guevara R. Compound and complex odontomas: Clinical study of 65 cases, Odont. Chile. 1966;15:33–9. [PubMed] [Google Scholar]
- 28.Stafne EC, Giblisco JA. Oral Roentgenographic Diagnosis. 4th ed. Philadelphia: WB Sunders; 1975. pp. 78–80. [Google Scholar]
- 29.Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology. Philadelphia: Saunders; 1995. pp. 531–3. [Google Scholar]
- 30.Iwamoto O, Harada H, Kusukawa J, Kameyama T. Multiple odontomas of the mandible: A case report. J Oral Maxillofac Surg. 1999;57:338–41. doi: 10.1016/s0278-2391(99)90685-7. [DOI] [PubMed] [Google Scholar]
- 31.Schimidseder R, Hausamen JE. Multiple odontogenic tumors and other anomalies. Oral Surg Oral Med Oral Pathol. 1975;39:249. doi: 10.1016/0030-4220(75)90226-1. [DOI] [PubMed] [Google Scholar]
- 32.Ajike SO, Adekeye EO. Multiple compound odontomas in the facial bones: A case report. Int J Oral Maxillofac Surg. 2000;29:443. [PubMed] [Google Scholar]
- 33.Mani NJ. Odontoma syndrome: Report of an unusual case with multiple multiform odontomas of both jaws. J Dent. 1974;2:149–52. doi: 10.1016/0300-5712(74)90043-8. [DOI] [PubMed] [Google Scholar]
- 34.Bordini J, Jr, Contar CM, Sarot JR, Fernandes A, Machado MA. Multiple compound odontomas in the jaw: Case report and analysis of the literature. J Oral Maxillofac Surg. 2008;66:2617–20. doi: 10.1016/j.joms.2007.08.027. [DOI] [PubMed] [Google Scholar]
- 35.Pindborg JJ, Hjortiy-Hansen E. Atlas of diseases of the jaws. Copenhagen: Munksgaard; 1974. pp. 98–101. [Google Scholar]
- 36.López-Areal L, Silvestre Donat F, Gil Lozano J. Compound odontoma erupting in the mouth: 4-year follow-up of a clinical case. J Oral Pathol Med. 1992;21:285–8. doi: 10.1111/j.1600-0714.1992.tb01012.x. [DOI] [PubMed] [Google Scholar]
- 37.Kharbanda OP, Saimbi CS, Renu K. Odontome: A case report. JIDA. 1986;58:269–71. [PubMed] [Google Scholar]