

Abstract
The problem:
Policy, systems, and environmental (PSE) approaches have been shown to be effective in increasing rates of healthy behaviors in the overall population, but are not always effective in reaching racial and ethnic minority groups, including Korean Americans (KAs), who may be socially and linguistically isolated from mainstream campaigns and programs. Targeted and tailored PSE strategies are needed to reach these groups.
Purpose:
To describe the process and lessons learned in implementing a targeted and culturally tailored PSE strategy to increase access to healthy foods for KAs.
Key points:
A Korean community-based organization (CBO) used its inherent understanding of cultural context, and social and historical viewpoints of KAs to develop PSE strategies to reach more than 13,000 KAs.
Conclusions:
Local CBOs can play a significant role in complementing population-level strategies with more tailored and targeted approaches to reach racial and ethnic minority groups.
Keywords: Asian American, nutrition, policy, culture, chronic disease
The Asian American population is rapidly increasing. From 2000 to 2010, Asian Americans (AA) had the fastest population growth of any other racial ethnic group1 and are projected to comprise over 8% of the US population by 2060.2 New Jersey is home to a large portion of the AA population, making up 9% of the state’s residents. In particular, Korean Americans (KA) account for 13% of New Jersey’s state’s Asian population. The majority of the New Jersey AA population is foreign-born with high levels of limited English proficiency.3
The AA population is also disproportionately affected by certain chronic diseases, such as diabetes and cardiovascular disease. Diabetes is the fifth leading cause of death for AAs4,5 and AAs are 30–50% more likely to have Type 2 diabetes compared to non-Hispanic whites.6,7 For KAs in particular, diabetes prevalence ranges from 4–10%.8 Moreover, Asian Americans have a higher prevalence of type 2 diabetes at relatively lower BMI cut points than whites.9 Population-based strategies, including policy, systems, and environmental (PSE) approaches have been shown to be effective in preventing chronic diseases by increasing rates of healthy behaviors in the overall population.10 PSE improvements move away from focusing on individual behavior to improve health and instead focus on changing policies, systems, and the physical environment.11 These approaches, however, are not always effective in reaching AA communities and other racial and ethnic minority groups who may be socially and linguistically isolated from mainstream campaigns and programs. Reasons for this include insufficient adaptation of PSE approaches12 that can lead to a “mismatch”13 between the mainstream group for whom the intervention was developed and validated for, and the AA community.14 If strategies are not adapted to account for important differences in culture, language and socioeconomic status, their successful implementation can be impeded.15,16 For example, a New York City study found that barriers such as language and cultural norms prevented AA communities from benefiting from city-wide smoking bans in the same way as the broader population.17 Similarly, although diabetes prevention programs have been shown to be an effective method of preventing the disease,18,19 there continues to be a lack of culturally-adapted programs to prevent diabetes or promote healthful behavioral changes in certain AA ethnic subgroups.20 What are needed are targeted and tailored PSE level strategies to complement broad-based approaches so that comparable results can be achieved in AA communities.
PURPOSE
To this end, the Asian & Pacific Islander and American Health Forum, and the NYU Center for the Study of Asian American Health formed a community-academic partnership to develop the Strategies to Reach and Implement the Vision of Health Equity (STRIVE) Project. Funded through a Racial and Ethnic Approaches to Community Health (REACH) cooperative agreement award from the Centers for Disease Control and Prevention, the STRIVE Project distributed 3 million dollars and provided technical assistance and training to 15 community-based organizations (CBOs) across the United States to implement targeted and tailored evidence and practice-based PSE strategies using a community-engaged approach to reduce health disparities related to chronic disease related risk factors.21 These risk factors included lack of physical activity, poor nutrition, access to healthy food options, and/or issues related to weight management. CBOs were selected as lead organizations for implementing PSE strategies due to their established role as trusted community gatekeepers and inherent knowledge of the communities. These qualities helped facilitate the implementation of relevant and sustainable strategies. All CBOs were required by the grant to carry out the following activities: enhance multisector partnerships to engage multiple stakeholders across sectors to help plan and implement the overall project; conduct a community health assessment and policy scan to gather and organize data on assets and areas for improvement before deciding on critical issues; and develop and implement a community action plan with PSE improvements. This process is further described in an earlier manuscript.21 CBOs were also required to target and tailor their strategies on deep and surface structures as described in Resnicow’s framework.22 Surface structure refers to matching to superficial (or, observable) characteristics (e.g., language, images); and 2) deep structure refers to incorporating cultural, social, and historical influences on health behaviors of the target population. Further description of the process CBOs used to culturally tailor PSE strategies are also described in an earlier manuscript.23 See Figure 1 for example of model for developing and implementing targeted and culturally-tailored PSE strategies following this process.
Figure 1.
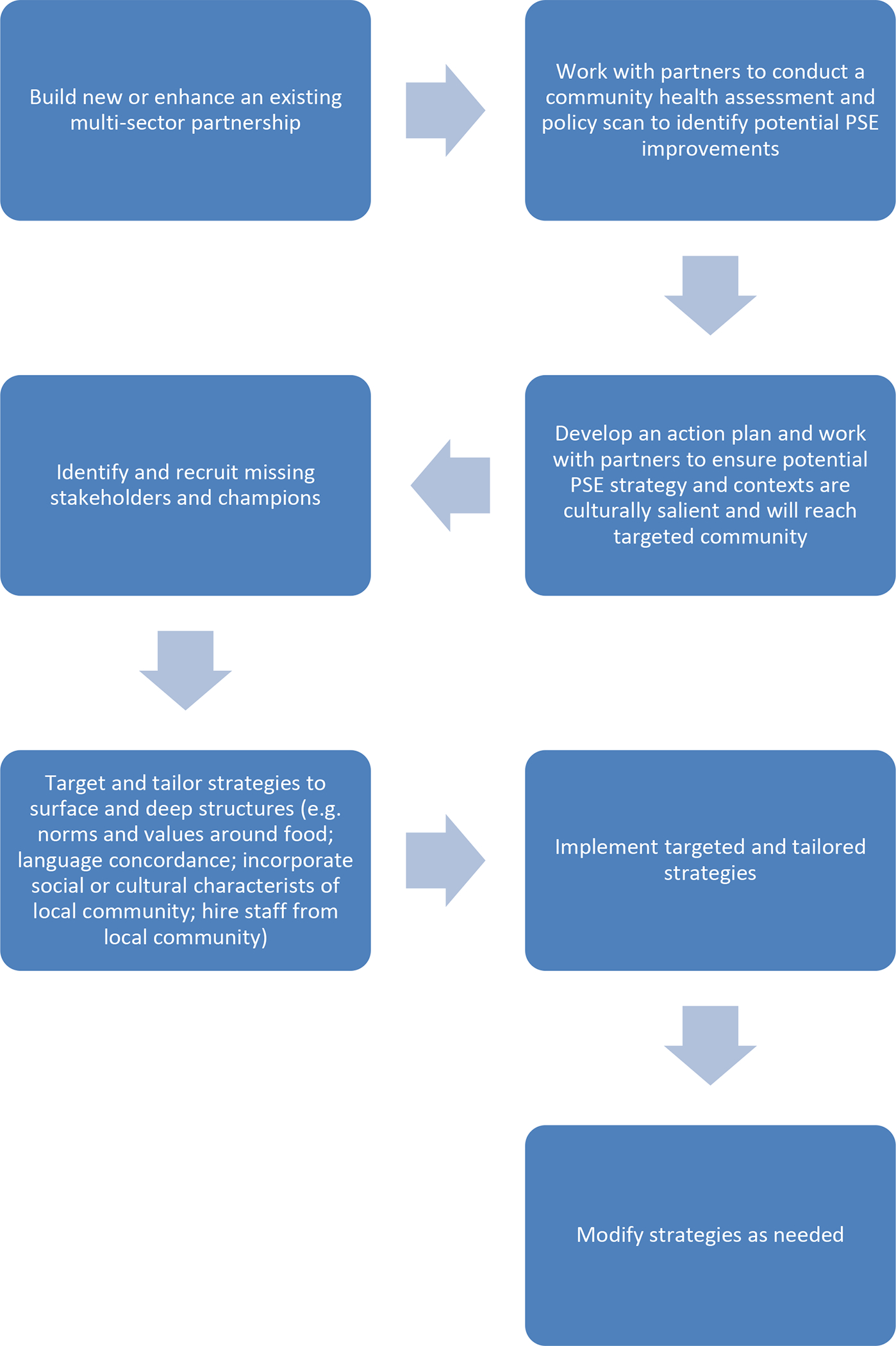
Model for developing and implementing targeted and culturally tailored PSE strategy.
Korean Community Services of Metropolitan NY (KCS) was awarded 1 of the 15 STRIVE grants through a competitive request for proposals to lead the development and implementation of a PSE strategy targeting Korean Americans (Figure 2 illustrates the partnership structure). As a more than 40-year old organization, and the first KA-serving organization in the New York metropolitan area, KCS holds a distinguished reputation in the community as a trusted social service, research, and advocacy organization that aims to improve the health of Korean immigrants and eliminate health disparities. KCS also maintains a strong multi-sector network (including hospitals, government, churches, ethnic media, and universities) that was leveraged to accelerate implementation of the STRIVE Project. KCS increased access to healthy foods at the level of the environment by undertaking a multi-pronged approach which included 1) increasing the number of KA churches that adopted an organizational nutrition policy to provide healthy food options, and 2) increasing the number of Korean mass media campaigns that raised awareness and educated the KA community on choosing healthy foods. Number of people reached by PSE strategy was the key evaluation metric tracked by the Centers for Disease Control and Prevention. Using church attendance logs and circulation numbers of media channels, KCS calculated they had reached more than 8,000 KAs. A further description of the STRIVE evaluation can be found elsewhere.24 The purpose of this article is to describe the process that KCS used and to share lessons learned in implementing a targeted and culturally-tailored PSE strategy to increase access to healthy foods in the KA community in New Jersey. Additionally, this paper presents a possible model for other organizations to follow.
Figure 2.
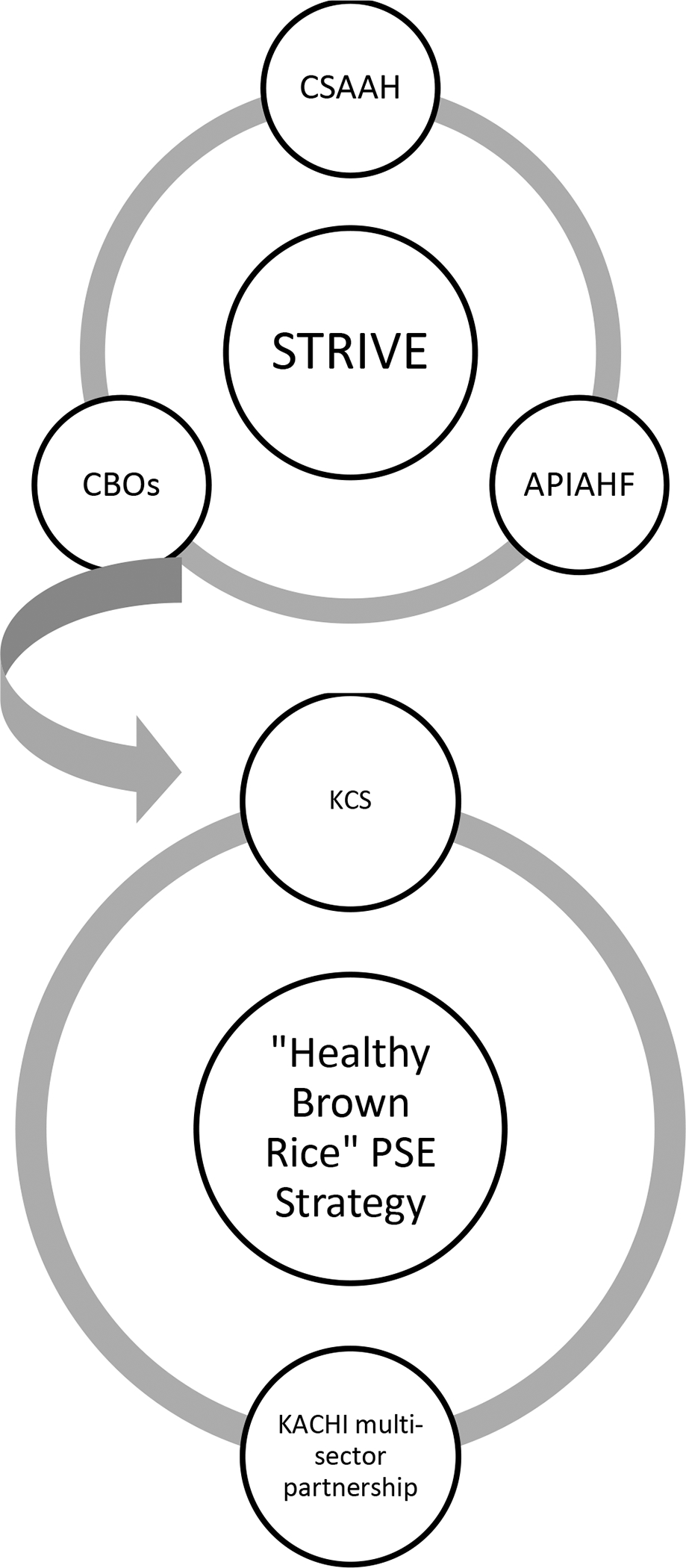
Partnership structure of the Strategies to Reach and Implement the Vision of Health Equity (STRIVE) project.
KEY POINTS
Developing the “Healthy Brown Rice Sunday” PSE Strategy
Following the conduct of their community health assessment and policy scan, KCS identified increasing healthier food options in KA churches as an area for improvement. KCS created the “Healthy Brown Rice Sunday” PSE strategy with the objective of increasing the availability of healthier food options (i.e. brown rice/multigrain rice instead of white rice) in KA churches in the Borough of Palisades Park in Bergen County, New Jersey and the neighboring townships. Bergen County was chosen as it has the highest KA population in New Jersey.3 The “Healthy Brown Rice Sunday” strategy was modeled off of the “Meatless Monday” campaign,25 which aimed to decrease meat consumption by using an idea that was simple to understand (i.e. avoiding meat 1 day a week to reduce chronic disease related risk factors). In the same spirit, the “Healthy Brown Rice Sunday” initiative aimed to encourage KAs to choose brown rice instead of white rice on Sundays.
A Tailored and Targeted Strategy: Understanding Cultural Context
Choosing a faith-based PSE strategy.
As the number of KA immigrants has increased in New Jersey, so too have the number of KA churches, numbering approximately 150 at present.26 Korean churches serve as a center of health, legal, social, and financial information for KAs and are seen as a cultural institution and supportive network system for the KA community.27,28 For many Korean immigrants who face linguistic and cultural barriers in American mainstream society, the church plays an important role in meeting needs for a sense of belonging, maintenance of ethnic identity and native traditions, and social status.29 A study on Korean churches in the United States reported that KA churches and church leaders seek to meet a variety of social and health needs of their congregation and the surrounding community.30 Similar to the successes seen in African American and Latino communities collaborating with faith-based organizations to implement health promotion programs and health education interventions, KA churches have also moved beyond their spiritual and religious roles in the community to provide hepatitis B screening, diabetes prevention programs, and colorectal cancer programs.31,32,33 Given the focal point that KA churches play in the community, and the fact that a large proportion of KAs in New Jersey attend church on a regular basis, KCS identified churches as the target venue for implementing the “Healthy Brown Rice Sunday” PSE strategy. None of the churches that KCS recruited had nutrition standards, guidelines or policies in place at the outset.
Addressing community perceptions of participating in a ‘coalition.’
When the work began, the New Jersey KA community did not have a history of working together in a coalition framework to address health issues. The STRIVE project however, required that grantees utilize a multi-sector partnership model to implement PSE strategies. As KCS worked to identify and bring relevant organizations together, it learned that leaders of four CBOs in New Jersey were already holding monthly meetings to address social and political issues in the KA community. KCS was able to leverage these meetings to introduce the project and to successfully create the Korean American Community Health Initiative (KACHI; Figure 3) with the four CBO leaders, as well as new members recruited from additional sectors. Importantly, KCS decided to refrain from using the term “coalition” when creating KACHI. KCS understood that for many KAs the term was either unfamiliar, or had a negative association with government coalitions in Korea during the military dictatorships from the 1960s to the 1980s. KCS tailored the intervention and terminology to the community, using the terms “partnership” or “teams,” which have a more positive tone for KAs. Additionally, in early meetings, members generally participated as active listeners instead of as active speakers given that they were unfamiliar with the customs of a partnership and the practice of adding their voices to the discussion. It took several meetings for members to become more comfortable in voicing their opinions, and with time the members solidified as a partnership and became invested in the process of collaborative decision making.
Figure 3.

Community-based organizational and other stakeholder partners representing the Korean American Community Health Initiative (KACHI).
Key also to the success of KACHI was KCS’s investment in attending and participating in meetings and events held by the CBOs represented on KACHI. Showing up and supporting other KACHI members helped to strengthen the rapport with these members and helped KCS become better integrated into other partnerships working in the KA community.
Understanding social and historical context of brown rice/multigrain rice.
Rice was targeted as the central focus of KCS’s PSE strategy given that it is the staple food of the Korean diet – typically eaten with each meal - and a main source of carbohydrates. KAs’ rate of carbohydrate consumption is higher than Americans as a whole - 64.5%, compared 51.7%.34 In addition, Korean adults’ high carbohydrate intake and refined-grain consumption are related to metabolic syndrome.35 Substituting brown rice for white has also been shown to decrease the risk for chronic diseases, such as type 2 diabetes.36
Focusing on brown rice/multigrain rice, however, raised some cultural challenges. Many of the older KA generation - who are considered a “product of war” - view white rice as a “luxury good” owing to the fact that generally only brown rice was available and eaten during the war. Historically, white rice was an indicator of affluence, while brown rice was associated with poverty.37 In addition, diabetes is known as a “rich person’s disease” and a natural part of aging. Adding to these challenges was the fact that many KAs complained that brown rice was more expensive, harder to digest because of its tough texture, and more difficult to cook than white rice.
KCS addressed these challenges through several coordinated efforts. First, media was used to frame the message in a culturally-tailored way. Working closely with the marketing director of a Korean local radio station, as well as KACHI members, KCS developed a media concept related to Koreans’ enthusiasm for vitamins as an important part of a healthy lifestyle. The message, “brown rice: rice with color and an abundance of vitamins” was created to appeal to this notion. In particular, this slogan helped KCS change the popular image of brown rice as a “poor” food to a healthy food by emphasizing the color brown as a sign of greater nutritional value. The partnership felt confident that this message would appeal to the KA community as it promoted brown rice as being more abundant in vitamins, fibers and other minerals, and evoked an image of health and nutrition. The media campaign also helped raise awareness of the prevalence of diabetes and other chronic diseases in the KA community, and promoted the benefits of eating brown rice/multigrain rice as a means to help prevent chronic disease related risk factors. The media campaign was also tied into KCS’s “Healthy Brown Rice Sundays” strategy, encouraging KAs to commit to eating brown rice at least once a week.
Second, to address concerns related to the perceived inferior taste of brown rice and its longer cooking time, KCS coordinated and hosted two “Brown Rice Cook-Off Demonstrations.” These events showcased the tasty and creative ways to incorporate brown rice into people’s diets. Creative recipes included brown rice cakes, brown rice vinegar, brown rice risotto, fermented brown rice punch (‘Kikhye’), and brown rice salad. Demonstrations were limited to 20 participants to allow for hands-on experiential learning and taste testing. Participants learned practical tips for cooking brown rice for large group meals and for their families. The two-hour classes were offered once during the week and once more on the weekend to accommodate both homemakers and church kitchen staff members. These events were important in gaining support from church kitchen staff for the PSE strategy.
Finally, to address concerns of the higher cost of brown rice, KCS developed an innovative public-private partnership with H&Y Mart, a large Korean supermarket in New Jersey. H&Y Mart was an ideal partner given that they already had a health-focused aspect to their mission, with the slogan “Eat Healthy! Stay Young!” KCS was able to secure a meeting with the chief operating officer of the supermarket to describe the project. The project was seen as complementary to the company’s goals and they were willing to create a brown rice/multigrain recipe as a promotional item. This opportunity allowed the supermarket to promote its corporate image of its commitment to the health of the Korean community, as well as increase sales of brown rice/multigrain rice. The new product was called “Golden Ratio Brown Rice with Multigrains” (Figure 4) and contained regular brown rice, sweet brown rice, black rice, and black beans. According to the golden ratio developed by the supermarket, the four grains were combined to be palatable to Koreans’ taste. In addition to creating a new promotional brown rice product, H&Y Mart also agreed to sell the product at a discounted price to Korean churches interested in implementing the PSE strategy. H&Y Mart also promoted KCS and the PSE strategy by adding the KCS logo and project information to the packaging. In addition, they were a key collaborative partner in several events including “8/25 Brown Rice Sunday Celebration.” In the Korean language 8/25 or August 25th sounds like, “Hurry Up!”, and this reference was used to kick-off the project.
Figure 4.

Newly created brown rice product (“Golden Ratio Brown Rice with Multigrains”) developed through KCS’s successful community-business partnership.
Addressing the cultural viewpoint of individual responsibility: Introducing PSE to the KA community.
When the project began, KA churches were not acquainted with population-wide health initiatives. This was due in part to mainstream, city-wide campaigns often not reaching ethnic and linguistically isolated communities such as KAs. In addition, KA community members may be more conditioned to understanding health to be an individual and family responsibility. Kitchen staff at the churches shared with KCS that while they ate brown rice/multigrain rice at home for their individual health and the health of their family, the idea of promoting community-wide healthy behaviors in a church setting was an unfamiliar approach. Some church members emphasized that the church was not responsible for the provision of healthy meals to its members, and argued that eating a healthy diet was a personal choice and responsibility. Church meals are seen as a means to promote church fellowship, but not necessarily as a means to promote nutrition. While awareness of the importance of eating a healthy diet was relatively high at the individual level, awareness of increasing access to healthy food options at the community level was initially low. Securing buy-in for a PSE approach at the church level required first raising awareness of the importance of population-wide approaches in improving the health of the KA community.
KCS addressed this challenge through several approaches. First, it secured buy-in from influential stakeholders in KA churches. To gain access to church leaders, KCS approached the Council of Korean Church of New Jersey (the Council), which has more than 180 churches in its membership. KCS was able to successfully build a relationship with the Council who endorsed the project and who gave KCS the opportunity to present and showcase the project at a large community event of over 300 pastors and their families. KCS also built alliances with other key stakeholders including, pastors and pastors’ wives, Deacons, elders, Board Committee members, and kitchen staff members who were responsible for purchasing and preparing the food for church meals.
Overtime, KCS was able to identify champions who had a strong interest in health and nutrition and leverage these relationships to support implementation. For example, the head pastors from partnering churches were asked to talk about healthy eating in their sermons and to tie healthy eating into a biblical context to help support the idea of eating healthy in church. In addition, the president of the Council of Churches was instrumental in recruiting smaller churches in Bergen County, New Jersey, who expressed an interest in implementing the PSE strategy.
An additional strategy used to secure buy-in at the church level was to create culturally-tailored materials built on the spiritual and religious aims of Korean churches. Bible passages were identified and used to support the idea of improving the health of the KA community. KCS also created church “pledge forms” citing biblical verses related to community health and love, as well as individual health and love. Using Christian terminology as a part of the PSE strategy helped to secure buy-in from church leaders and kitchen personnel. By the end of the project period, KCS had collected nine signed pledge forms, representing seven KA churches and two Korean senior centers.
Next Steps and Future Directions
“Healthy Brown Rice Sunday” helped to create momentum in the KA community for addressing health disparities at a population-wide level. KCS was successful in partnering with large churches to implement nutritional policies through several key strategies, including engaging key stakeholders; empowering church staff members (e.g., the kitchen staff) to initiate change; and importantly culturally-adapting the approach, messages, and materials. To this end, KCS was able to apply for and receive additional supplemental funding through the STRIVE Project to implement a train-the-trainer model whereby 40 church staff, representing 26 churches, were trained to implement “Healthy Brown Rice Sunday” within their own churches. These additional efforts reached 5,000 more KAs bringing the total reach to more than 13,000. Lessons learned from the project will also be leveraged for opportunities to expand the initiative to further re-enforce and enhance access to healthy foods using the created infrastructure.
CONCLUSIONS
As a trusted CBO serving the KA community for over 40 years, KCS was well-poised to implement an impactful PSE targeted and tailored PSE strategy that would reach KAs where they work, live, play, and pray. KCS’s success demonstrates that with funding and technical assistance, local CBOs can play a significant role in complementing population-level strategies with more tailored and targeted approaches. This model can potentially be applied to a wide spectrum of CBOs that serve racial and ethnic minority groups who may be socially and linguistically isolated from mainstream campaigns and programs.
ACKNOWLEDGMENTS
This study was funded by the Centers for Disease Control and Prevention grant award numbers U58 DP004685 and U58 DP005621. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agency. We gratefully acknowledge the support and partnership of our colleagues at the Asian & Pacific Islander American Health Forum.
Contributor Information
Soonsik Sara Kim, Korean Community Services of Metropolitan New York, Inc, New York, NY.
Catlin Rideout, Department of Population Health, NYU School of Medicine, New York, NY.
Hee Won Han, Johns Hopkins University, Baltimore, MD.
Linda Lee, Korean Community Services of Metropolitan New York, Inc, New York, NY.
Simona C. Kwon, Department of Population Health, NYU School of Medicine, New York, NY.
REFERENCES
- 1.U.S. Census Bureau. 2010 Census Briefs: The Asian Population. Available at: https://www.census.gov/prod/cen2010/briefs/c2010br-11.pdf. Accessed 11/16/2016.
- 2.U.S. Census Newsroom. U.S. Census Bureau Projections Show a Slower Growing, Older, More Diverse Nation a Half Century from Now. Available at: https://www.census.gov/newsroom/releases/archives/population/cb12-243.html. Accessed 11/16/2016.
- 3.Asian American Federation of New York Census Information Center. Census Profile: New Jersey’s Asian American Population. Available at: http://www.aafny.org/cic/briefs/newjersey.pdf. Accessed 11/16/2016.
- 4.Centers for Disease Control and Prevention. National Vital Statistics Report. Available at: http://www.cdc.gov/nchs/data/nvsr/nvsr65/nvsr65_05.pdf. Accessed on 11/16/2016.
- 5.Office on Women’s Health, U.S. Department of Health and Human Services. Womenshealth.gov. Available at: https://www.womenshealth.gov/publications/our-publications/fact-sheet/diabetes.html. Accessed on 11/16/2016 [Google Scholar]
- 6.Lee J, Brancati F, Yeh HC. Trends in the prevalence of type 2 diabetes in Asians versus Whites. Diabetes Care. 2011; 34(2): 353–357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Joslin Diabetes Center. Asian American and Diabetes. Available at: http://www.joslin.org/info/Asian_Americans_and_Diabetes.html Accessed on 11/16/16 [Google Scholar]
- 8.Islam N, Wyatt L, Kapadia S, Rey M, Trinh-Shevrin C, Kwon S. Diabetes and associated risk factors among Asian Americans subgroups in New York City. Diabetes Care. 2013; 36(1): e5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hsu W, Araneta M, Kanaya A, Chiang J, Fujimoto W. BMI cut points to identify at-risk Asian Americans for type 2 diabetes screening. Diabetes Care. 2015;38:150–158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Brownson R, Haire-Joshu D, Luke D. Shaping the context of health: a review of environmental and policy approaches in the prevention of chronic diseases. Annu Rev Public Health. 2006; 27:341–70. [DOI] [PubMed] [Google Scholar]
- 11.Cook County Department of Public Health and the Public Health Institute of Metropolitan Chicago. What is “policy, systems and environmental change”? Available at: http://www.cookcountypublichealth.org/files/CPPW/PSE%20Change.pdf. Accessed October 10, 2014.
- 12.Merzel C, D’afflitti J Reconsidering community-based health promotion: promise, performance, and potential. Am J Public Health. 2003; 93(4):557–574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Castro F, Barrera M, Martinez C. The cultural adaptation of prevention interventions: resolving tensions between fidelity and fit. Prevention Science. 2004; 5(1): 41–45. [DOI] [PubMed] [Google Scholar]
- 14.Kim M, Han H-R, Kim B. A community-based, culturally tailored behavioral intervention for Korean American with Type 2 diabetes. Diabetes Educ. 2009; 35(6):986–994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Kreuter M, Lukwago S, Bucholtz D, et al. Achieving cultural appropriateness in health promotion programs: targeted and tailored approaches. Health Edu & Behavior. 2002; 30(2):133–146. [DOI] [PubMed] [Google Scholar]
- 16.Chin M, Walters A, Huang E. Interventions to reduce racial and ethnic disparities in health care. Med Car Res Rev. 2007; 64(5 Suppl):7S–28S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Li S, Trinh-Shevrin C, Weerasinghe I, Rey M, Kwon S. Smoking among Asian Americans: Acculturation and Gender in the Context of Tobacco Control Policies in New York City. Health Promotion and Practice. 2013; 4(5 Suppl):18S–28S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Knowler W Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Eng J Med. 2002; 346(6):393–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ramachandran A, Snehalatha C, Mary S, et al. Indian diabetes prevention programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance. Diabetologia. 2006; 49:289–297. [DOI] [PubMed] [Google Scholar]
- 20.Islam N, Wyatt L, Trinh-Shevrin C. Evaluation of a community health worker pilot intervention to improve diabetes management in Bangladesh immigrants with type 2 diabetes in New York City. The Diabetes Educ. 2013; 39(4):478–493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Arista P, Tepporn E, Kwon S, Rideout C, Patel S, Chung M, Bautista R, Trinh-Shevrin C, Ko-Chin K. Recommendations for Implementing Policy, Systems, and Environmental Improvements to Address Chronic Diseases in Asian Americans, Native Hawaiians, and Pacific Islanders. Prev. Chronic Disease 2014; 11(E202):. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.US Department of Health and Human Services. Obesity and Asian Americans. 2009. http://wwwomhrcgov/templates/contentaspx?ID=6458.
- 23.Kwon S, Rideout C, Patel S, Arista P, Tepporn E, Lipman J, Kunkel S, Le D, Ko-Chin K, Trinh-Shevrin C. Improving Access to Healthy Food for Asian Americans, Native Hawaiians, and Pacific Islanders: Lessons learned from the STRIVE Program. Journal of Healthcare for the Poor and Underserved. 2015; 26(20):116–136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Patel S, Kwon S, Arista P, Tepporn E, Chung M, Ko-Chin K, Rideout C, Islam N, Trinh-Shevrin C. Using evidence based policy, systems, and environmental strategies to increase access to healthy food and opportunities for physical activity among Asian Americans, Native Hawaiians, and Pacific Islanders. Am J Public Health. 2015; 105 (Suppl 3):S455–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Meatless Monday. Available at: http://www.meatlessmonday.com/. Accessed on 11/17/16
- 26.The Council of New Jersey Korean American Churches. Directory of NJ Korean Churches; 2014. [Google Scholar]
- 27.Jo A, Maxwell A, Yang B, et al. Conducting Health Research in Korean American Churches: Perspectives from Church Leaders. Journal of Community Health. 2009; 35(2): 156–164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Boddie S, Hong P, Im H, et al. Korean American churches as partners in community development. Social Work & Christianity. 2011; 38(4): 395–416 [Google Scholar]
- 29.Community Toolbox. Understanding culture, social organizations, and leadership to enhance engagement. Available at: http://ctb.ku.edu/en/table-of-contents/culture/cultural-competence/understand-culture-social-organization/main. Accessed on 11/16/2016.
- 30.Jo A, Maxwell A, Choi S, et al. Interest in health promotion among Korean American Seventh-Day Adventists attending a religious retreat. Asian Pacific J Cancer Prev. 2012; 13(6):2923–2930. [DOI] [PubMed] [Google Scholar]
- 31.Ma G, Shive S, Tan Y, et al. Community-based colorectal cancer intervention in underserved Korean Americans. Cancer Epidemiology. 2009; 33: 381–386. [DOI] [PubMed] [Google Scholar]
- 32.Islam N, Zanowiak J, Wyatt L, et al. A Randomized-Controlled, Pilot Intervention on Diabetes Prevention and Healthy Lifestyles in the New York City Korean Community. J Community Health. 2013; 38(6): 1030–1041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bastani R, Glenn B, Maxwell A. Cluster-Randomized Trial to Increase Hepatitis B Testing among Koreans in Los Angeles. Cancer Epidemiol Biomarkers Prev. 2015; 24(9):1341–1349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ahn H-J, Eom Y-K, Han K-A, et al. The effects of small sized rice bowl on carbohydrate intake and dietary patterns in women with type 2 diabetes. Korean Diabetes J. 2010; 34(3):166–173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Song S, Lee J, Song W, et al. Carbohydrate intake and refined-grain consumption are associated with metabolic syndrome in the Korean adult population. J Acad Nutr Diet. 2014; 114(1):54–62. [DOI] [PubMed] [Google Scholar]
- 36.Zhang G, Malik V, Pan A, et al. Substituting brown rice for white rice to lower diabetes risk: a focus-group study in Chinese adults. J Am Diet Assoc. 2010; 110:1216–1221. [DOI] [PubMed] [Google Scholar]
- 37.Kim S Cultural perspectives and current consumption changes of cooked rice in Korean diet. Nutr Res Pract. 2007; 1(1): 8–13. [DOI] [PMC free article] [PubMed] [Google Scholar]