

Abstract
This randomized controlled trial evaluated the effect of a 5‐week daily skin‐to‐skin contact (SSC) intervention between mothers and their full‐term infants, compared with care‐as‐usual, on exclusive and continued breastfeeding duration during the first post‐natal year. Healthy pregnant women (n = 116) from a community sample were enrolled and randomly allocated to the SSC or care‐as‐usual condition. SSC mothers were requested to provide one daily hour of SSC for the first five post‐natal weeks. Twelve months post‐partum, mothers indicated the number of exclusive and continued breastfeeding months. Multiple regression analyses were conducted using intention‐to‐treat, per‐protocol and exploratory dose–response frameworks. In intention‐to‐treat analyses, exclusive and continued breastfeeding duration was not different between groups (exclusive: 3.61 ± 1.99 vs. 3.16 ± 1.77 months; adjusted mean difference 0.28, 95% confidence interval [CI] −0.33 to 0.89; p = 0.36; continued: 7.98 ± 4.20 vs. 6.75 ± 4.06 months; adjusted mean difference 0.81, 95% CI −0.46 to 2.08; p = 0.21). In per‐protocol analyses, exclusive and continued breastfeeding duration was longer for SSC than care‐as‐usual dyads (exclusive: 4.89 ± 1.26 vs. 3.25 ± 1.80 months; adjusted mean difference 1.28, 95% CI 0.31–2.24; p = 0.01; continued: 10.81 ± 1.97 vs. 6.98 ± 4.08 months; adjusted mean difference 2.33, 95% CI 0.13–4.54; p = 0.04). Exploratory dose–response effects indicated that more SSC hours predicted longer exclusive and continued breastfeeding duration. This study demonstrates that for the total group, the 5‐week daily SSC intervention did not extend exclusive and continued breastfeeding duration. However, for mothers performing a regular daily hour of SSC, this simple and accessible intervention may extend exclusive and continued breastfeeding duration by months. Future studies are required to confirm these promising findings. Trial registration: Netherlands Trial Register (NTR5697).
Keywords: breastfeeding, kangaroo‐mother care method, term birth, touch
Key messages.
Benefits of breastfeeding are well‐established but breastfeeding rates are suboptimal worldwide. Daily skin‐to‐skin contact in mothers and their full‐term infants is a potential intervention that may increase breastfeeding rates.
Daily skin‐to‐skin contact during the first five post‐natal weeks between mothers and full‐term infants, compared with care‐as‐usual, did not extend exclusive and continued breastfeeding duration during the first post‐natal year for the total group.
When only mothers who adhered to the skin‐to‐skin contact protocol were examined, daily skin‐to‐skin contact, compared with care‐as‐usual, extended exclusive breastfeeding duration with 1.28 months and continued breastfeeding duration with 2.33 months in the first post‐natal year.
1. INTRODUCTION
Breastfeeding has extensive, long‐lasting health benefits for children and mothers (Victora et al., 2016; World Health Organization, 2013a, 2013b). The World Health Organization recommends exclusive breastfeeding for up to 6 months and continued breastfeeding up to 2 years or beyond (Kramer & Kakuma, 2012; World Health Organization, 2021). However, worldwide, just 80% of all neonates receive breastfeeding after birth, and exclusive breastfeeding rates at 6 months post‐partum are below 50% (Peeters et al., 2015; Victora et al., 2016). At 12 months post‐partum, less than 60% of all infants in middle–upper income and less than 30% in high‐income countries receive breastfeeding (Victora et al., 2016). Interventions, including breastfeeding education, support and increasing awareness on breastfeeding benefits, can lengthen breastfeeding duration but are costly and burdensome to the health care system (Haroon et al., 2013; McFadden et al., 2017; Sinha et al., 2015). Despite these interventions, global improvements in breastfeeding rates are limited. This indicates a need for simple, low‐cost interventions to increase breastfeeding rates.
Skin‐to‐skin contact (SSC), placing a naked infant onto their mother's bare chest, holds promise in this regard (World Health Organization, 2003). In preterm infants, SSC is related to any and exclusive breastfeeding at discharge, earlier establishment of breastfeeding and longer continuation during the first six post‐natal months (Conde‐Agudelo & Díaz‐Rossello, 2016; Flacking et al., 2011; Maastrup et al., 2014). Currently, SSC is encouraged immediately after birth for healthy full‐term infants and is related to higher breastfeeding rates 1 to 4 months post‐partum and an older age at weaning (Moore et al., 2016; UNICEF, 2017). Only one study examines the effects of 1‐month daily SSC in mothers and full‐term infants. Results indicated that breastfeeding rates did not decline over the first three post‐natal months in the SSC group, whereas in the control group they did (Bigelow et al., 2014). These results are promising, but the lack of a randomized controlled design may have affected the accuracy of results.
The current randomized controlled trial (RCT) examines the effect of a 5‐week daily hour of SSC between mothers and full‐term infants, compared with care‐as‐usual (CAU), on exclusive and continued breastfeeding duration (as secondary outcomes) until 12 months post‐partum. The daily hour of SSC was considered achievable because Dutch mothers receive 10 to 12 weeks of paid post‐natal maternity leave. We hypothesized that SSC dyads would show longer exclusive and continued breastfeeding duration, compared with CAU dyads (Bigelow et al., 2014; Moore et al., 2016).
2. METHODS
2.1. Trial design and setting
In this RCT with two parallel groups (intervention vs. passive control), we recruited healthy pregnant women from the community in Nijmegen, The Netherlands, and surrounding areas. Ethics approval was granted by the ethics committee of the Social Science faculty of the Raboud University (ECSW2015‐2311‐358). The primary outcome was maternal depressive symptoms (not presented in this study), which SSC did not improve over the first post‐natal year (Cooijmans et al., 2021). This trial was registered with the Netherlands Trial Register (NTR5697), followed CONSORT guidelines (see Supporting Information), and the protocol, unchanged after trial commencement except for the analyses, was published (Cooijmans et al., 2017).
2.2. Participants
Pregnant women were eligible if they were aged ≥18, had a singleton pregnancy, reported no drug use, had no severe health problems, were not participating in other research and understood the Dutch language. Inclusion criteria for the infant were born at ≥37 weeks, no congenital anomalies, birthweight ≥2500 g and 5‐min Apgar score ≥7. Women were recruited via a database of pregnant women interested in research participation, social media and flyers. Interested and eligible women provided written informed consent. Baseline characteristics are presented in Table 1.
Table 1.
Baseline characteristics
| Intention‐to‐treat | Per‐protocol | |||
|---|---|---|---|---|
| SSC (n = 56) | CAU (n = 60) | SSC (n = 18) | CAU (n = 60) | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Maternal age (years) | 32.36 (3.85) | 32.48 (3.05) | 32.90 (3.80) | 32.48 (3.05) |
| Maternal educational level a | 6.82 (1.55) | 6.87 (1.79) | 6.78 (1.48) | 6.87 (1.79) |
| Smoking, n (%) | ||||
| No | 54 (96%) | 60 (100%) | 17 (94%) | 60 (100%) |
| Yes | 2 (4%) | 0 (0%) | 1 (6%) | 0 (0%) |
| Alcohol, n (%) | ||||
| No | 55 (98%) | 60 (100%) | 17 (94%) | 60 (100%) |
| Yes | 1 (2%) | 0 (0%) | 1 (6%) | 0 (0%) |
| C‐section, n (%) | ||||
| No | 51 (91%) | 55 (92%) | 17 (94%) | 55 (92%) |
| Yes | 5 (9%) | 5 (8%) | 1 (6%) | 5 (8%) |
| Birth order, n (%) | ||||
| First | 27 (48%) | 28 (47%) | 6 (33%) | 28 (47%) |
| Second | 18 (32%) | 23 (38%) | 7 (39%) | 23 (38%) |
| Third | 11 (20%) | 9 (15%) | 5 (28%) | 9 (15%) |
| Apgar score | 9.84 (0.42) | 9.70 (0.62) | 9.72 (0.58) | 9.70 (0.62) |
| Child sex, n (%) | ||||
| Male | 23 (61%) | 34 (57%) | 7 (39%) | 34 (57%) |
| Female | 33 (59%) | 26 (43%) | 11 (61%) | 26 (43%) |
| Gestational age at birth (weeks) | 40.08 (1.01) | 40.02 (1.10) | 40.16 (1.03) | 40.02 (1.10) |
| Birthweight (g) | 3650.05 (414.93) | 3567.47 (385.77) | 3760.56 (454.59) | 3567.47 (385.77) |
| Breastfeeding intention, n (%) | ||||
| No | 4 (7%) | 2 (3%) | 0 (0%) | 2 (3%) |
| Yes | 51 (91%) | 58 (97%) | 17 (94%) | 58 (97%) |
| Do not know yet | 1 (2%) | 0 (0%) | 1 (6%) | 0 (0%) |
| Intended breastfeeding duration known, n (%) | ||||
| Yes | 36 (71%) | 43 (74%) | 13 (72%) | 43 (74%) |
| Do not know yet | 15 (29%) | 15 (26%) | 4 (22%) | 15 (26%) |
| Intended breastfeeding duration (months) | 10.25 (6.44) | 8.03 (5.63) | 11.00 (6.74) | 8.03 (5.63) |
Abbreviations: CAU, care‐as‐usual; SSC, skin‐to‐skin contact.
Maternal educational level: 1, primary education; 2–6, secondary education; and 7–8, higher education.
2.3. Randomization and masking
An independent researcher prepared a computer‐generated random allocation sequence (1:1) with random permuted blocks (four and six) stratified by parity (primiparae/multiparae) and created opaque sealed envelopes. The principal investigator assigned women to their condition after enrolment. During the recruitment phase, women were told that the study was about infant sleep and feeding, maternal and infant health, and mother–infant contact and that some participants would be asked to include a 5‐week daily mother–infant contact period. SSC mothers received SSC instructions. CAU mothers received no additional instructions.
2.4. Procedure
Interested and eligible women were visited at home in late pregnancy (Weeks 34–36) and given study information. Participants signed the informed consent form, were assigned to a condition and completed baseline questionnaires. SSC women were asked to spend at least one daily uninterrupted hour in mother–infant SSC for the first five post‐natal weeks, starting immediately after birth (adapted from previous research to promote adherence; Bigelow et al., 2012). Besides daily SSC, both conditions underwent the same procedures.
After birth, mothers retrospectively filled out a simple daily logbook every 2 to 3 h during daytime. During natural breaks in their day, such as for feeding, they registered holding (i.e., physical contact with clothes), SSC and no contact in 15‐min intervals during the 5‐week intervention period. Note that also CAU mothers registered SSC. Prior to randomization, when all mothers were explained the logbook, SSC was described as having the naked infant (wearing only a diaper) on the mother's bare chest, just as is done immediately after birth according to current delivery guidelines. CAU mothers were given no additional information about SSC. The logbook was based on a widely used similar logbook to register infant behaviour in 5‐min intervals (Barr et al., 1988). All mothers were contacted weekly to remind them to fill out the logbook, to ask them about adverse events and, for SSC mothers, to discuss SSC implementation problems.
One year after birth, all mothers filled out a digital follow‐up questionnaire, including questions on infant feeding, and were visited at home for debriefing.
2.5. Outcomes
Feeding data on breastfeeding and formula feeding for the first 12 months were collected when the infant turned 1 by means of a table. This table had columns for breastfeeding and formula feeding for the 12 months. The mother indicated with crosses the type of fluid feeding the child received each month. With additional questions, the mother reported in which month solids were introduced (i.e., fruit, vegetables and porridge). From these data, the following variables were calculated for the current study: (1) exclusive breastfeeding duration, which was defined as the number of months the infant received only breastfeeding (no formula, solids), and (2) continued breastfeeding duration, which was defined as the number of months the infant received any breastfeeding (combined with formula and/or solids).
2.6. Statistical analyses
Sample size calculations, based on the primary outcome not examined in this paper (Cooijmans et al., 2017), indicated that 84 mother–infant dyads were required to detect an effect size of Cohen's f = 0.24 in maternal depressive symptoms, derived from a prior study (Bigelow et al., 2012), at 0.05 significance level with 80% power. Comparable effect sizes were expected for breastfeeding duration, based on risk ratios from the review on early SSC of Moore et al. (2016). An effect size of 0.24 is considered a medium effect size. This is considered clinically relevant because of the positive health effects of longer breastfeeding durations for both mother and infant and the low breastfeeding rates in medium‐ and high‐income countries (Victora et al., 2016).
The linearity, multicollinearity and homoscedasticity assumptions were checked. After the analyses, the normality of residuals was checked. Additionally, outliers were examined and winsorized (replaced with a value of 3 SDs above or below the mean; Tukey, 1977). Missingness was investigated using Little's missing completely at random (MCAR) test and by correlating missingness to baseline characteristics using Pearson correlation coefficients to check if missingness was random.
Analyses were completed using multiple regressions. Intended breastfeeding duration reported in late pregnancy was controlled for following recommendations of Moore et al. (2016) on SSC and breastfeeding research. The regression coefficient represents the adjusted mean difference presented with 95% confidence intervals (CIs). Three statistical approaches were used: (1) intention‐to‐treat (ITT), (2) per‐protocol (PP) and (3) exploratory dose–response (DR) analyses. In ITT analyses, mother–infant dyads were analysed according to condition, irrespective of compliance or withdrawal. Missing values in the outcome (exclusive and continued breastfeeding duration) and covariate (intended breastfeeding duration) data were imputed with the expectation–maximization method when missing data were <20% and when missingness was at random (Liu & Brown, 2013). In PP analyses, SSC dyads without missing data who adhered to the SSC protocol were compared with CAU dyads without missing data. Protocol adherence derived from the contact logbook. Logbook data were only used when at least 80% of each day for ≥21 out of 35 days was completed. Of the total sample, 90 adequately filled out the logbook (27: no missing days; 39: 1 or 2 missing days; 16: 3–7 missing days; and 8: 8–14 missing days). Missing days were replaced with the mean SSC duration 2 days before and after the missing day (Beijers et al., 2013). Data from remaining logbooks were not used. SSC dyads with ≥28 out of 35 days (80%) with ≥60 min of SSC were included in PP analyses. Data for the exploratory DR analyses, including only SSC mothers from the ITT selection with valid logbooks, derived from the imputation were used for the ITT analyses. Total duration of SSC during the intervention was the independent variable.
Although the protocol prespecified ITT analyses, we added PP and exploratory DR analyses, as recommended (Hernán & Hernández‐Díaz, 2012). Additionally, we used multiple regression analyses instead of prespecified multivariate analyses of covariance to retain consistency between ITT, PP and DR analyses. All analyses were completed in SPSS Statistics for Mac OS (Version 26.0).
3. RESULTS
Recruitment was between 29 April 2016 and 18 September 2017, and follow‐up was between 18 May 2017 and 17 October 2018. Figure 1 shows the participant flow. Initially, 116 mother–infant dyads were recruited; four women were excluded due to medication use after enrolment, and seven infants did not meet eligibility criteria after birth. Eleven additional pregnant women were recruited. No adverse events were reported.
Figure 1.
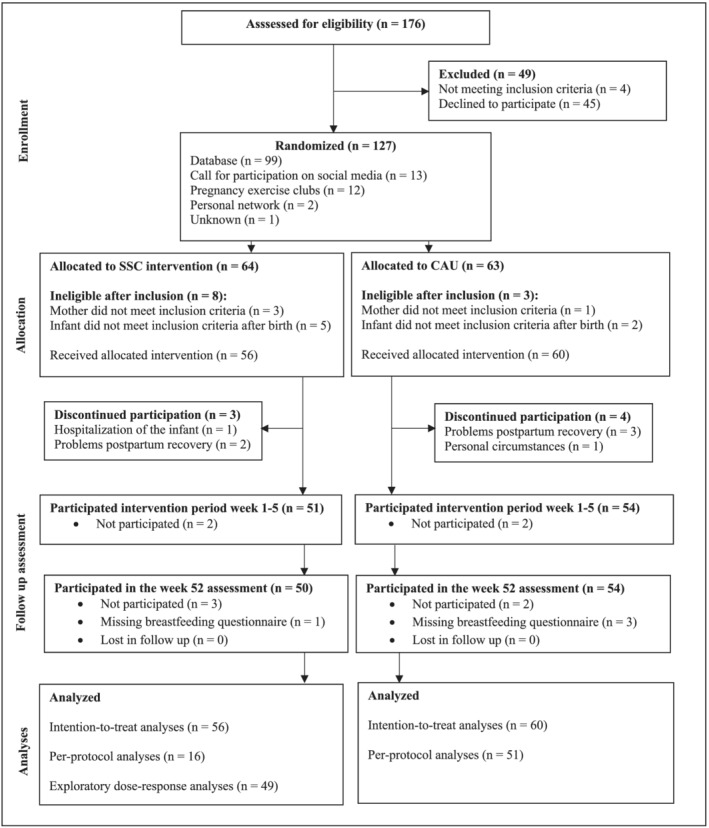
Trial profile. Numbers represent mothers that participated in the measurement round but do not define the number of mothers that actually provided breastfeeding information at 1‐year follow‐up. CAU, care‐as‐usual; SSC, skin‐to‐skin contact
Across all variables, 3% of values were missing. Missingness was not completely at random (Little's MCAR test: χ 2 = 38.40, df = 22, p = 0.02). Missing pattern analyses showed that missingness in the outcomes was negatively correlated with maternal educational level (r = −0.32, p < 0.001). No outliers were detected.
Baseline characteristics were balanced between conditions for ITT and PP samples, except for intended breastfeeding duration (Table 1). For SSC mothers, intended breastfeeding duration tended to be longer than for CAU mothers in the ITT and PP samples.
Independent sample t‐tests revealed a longer total SSC duration (min) during the intervention period in the SSC group (ITT: 2067.68 ± 850.65; PP: 2905.90 ± 497.52) than the CAU group (ITT: 308.17 ± 442.41; PP: 308.17 ± 442.41) in ITT (p < 0.001, effect size 1.97, 95% CI 1.54–2.43) and PP analyses (p < 0.001, effect size 5.52, 95% CI 4.47–6.82; Figure 2). For the SSC group, 16 out of 56 mothers reported ≥28 of 35 days with ≥60 SSC minutes and had no missing outcome data. Baseline characteristics were not significantly different between SSC mothers who did and did not adhere to the SSC protocol.
Figure 2.
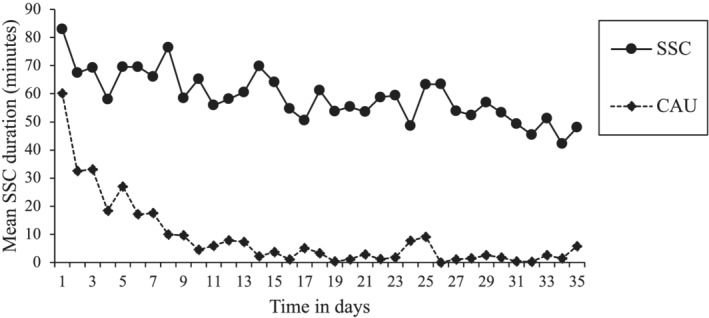
Mean daily skin‐to‐skin contact (SSC) duration in the SSC and care‐as‐usual (CAU) condition based on data derived from the intention‐to‐treat selection
The ITT and PP models are presented in Table 2. The ITT analyses revealed that mothers reported equally long exclusive and continued breastfeeding duration in both groups. The PP analyses indicated that exclusive and continued breastfeeding duration was longer in the SSC group than the CAU group.
Table 2.
Effects of skin‐to‐skin contact vs. care‐as‐usual on exclusive and continued breastfeeding duration
| Intention‐to‐treat | Per‐protocol | |||||||
|---|---|---|---|---|---|---|---|---|
| SSC (n = 56) | CAU (n = 60) | Adjusted mean difference (95% CI) a | Adjusted p value a | SSC (n = 16) | CAU (n = 51) | Adjusted mean difference (95% CI) a | Adjusted p value a | |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |||||
| Exclusive breastfeeding duration (months) | 3.61 (1.99) | 3.16 (1.77) | 0.28 (−0.33 to 0.89) | 0.36 | 4.88 (1.26) | 3.25 (1.80) | 1.28 (0.31–2.24) | 0.01 |
| Continued breastfeeding duration (months) | 7.98 (4.20) | 6.75 (4.06) | 0.81 (−0.46 to 2.08) | 0.21 | 10.81 (1.97) | 6.98 (4.08) | 2.33 (0.13–4.54) | 0.04 |
Abbreviations: CAU, care‐as‐usual; CI, confidence interval; SD, standard deviation; SSC, skin‐to‐skin contact.
SSC group minus CAU group, adjusted for intended breastfeeding duration.
The exploratory DR models are presented in Table 3. The mean duration of total SSC during the intervention period in SSC mothers from the ITT selection with valid logbooks was 34.46 ± 14.18 h, range 2.25–65.75. The findings showed that exclusive and continued breastfeeding was longer in SSC mothers who reported more SSC hours than in SSC mothers who reported fewer hours.
Table 3.
Exploratory effects of skin‐to‐skin contact dose on exclusive and continued breastfeeding duration
| Exclusive breastfeeding duration | Continued breastfeeding duration | |||||||
|---|---|---|---|---|---|---|---|---|
| B | β | 95% CI | p value | B | β | 95% CI | p value | |
| Intended breastfeeding duration pregnancy | 0.14 | 0.49 | 0.08–0.21 | <0.001 | 0.35 | 0.56 | 0.22–0.48 | <0.001 |
| SSC doses in hours | 0.06 | 0.40 | 0.03–0.09 | <0.001 | 0.12 | 0.42 | 0.06–0.18 | <0.001 |
| R 2 | 0.42 | <0.001 | 0.52 | <0.001 | ||||
| Cohen's f 2 | 0.72 | 0.28–1.60 | 1.08 | 0.51–2.34 | ||||
Abbreviations: B, regression coefficient; CI, confidence interval; Cohen's f 2, effect size for regression model; R 2, total explained variance by the model; SSC, skin‐to‐skin contact; β, standardized regression coefficient.
All effects emerged after adjusting for intended breastfeeding duration (as reported in late pregnancy).
4. DISCUSSION
This RCT with mothers and full‐term infants investigated the effects of a 5‐week daily 1‐h SSC intervention, above and beyond CAU, on exclusive and continued breastfeeding duration. ITT analyses revealed that daily SSC did not extend exclusive or continued breastfeeding duration during the first post‐natal year. However, PP analyses including only SSC mothers who adhered to the protocol revealed differences. Compared with CAU mothers, SSC mothers reported approximately 1.28 months longer exclusive breastfeeding and 2.33 months longer continued breastfeeding durations in the first post‐natal year. Additionally, exploratory dose–response effects were found. More hours of SSC were related to both longer exclusive and continued breastfeeding durations. Notably, effects emerged after adjusting for intended breastfeeding duration. These results provide preliminary support for daily SSC benefits on exclusive and continued breastfeeding duration in the first post‐natal year but only when SSC is consistently delivered.
Contrary to expectations, it was not feasible for most SSC mothers to incorporate daily SSC into their daily routine. Despite weekly contact to discuss SSC implementation and paid maternity leave, only 18 out of 56 SSC mothers adhered to the prescribed daily hour (note that only 16 also had complete outcome data and could be included in the PP analyses). Low adherence rates in behavioural change interventions are not uncommon. A meta‐analysis including 669 studies showed that the average retention rate in psychotherapy and behavioural change interventions was 20% (Swift & Greenberg, 2012). Potentially, adherence rates are even lower post‐partum. A recent RCT on e‐health in mothers during the post‐partum period reported adherence rates comparable with the current study (Gilmore et al., 2017). Our lower adherence rate may be a result of mothers being unmotivated or unaware of possible SSC benefits. Greater adherence might be expected if women are made aware of potential benefits of SSC evidenced by scientific research. However, we expect that our results would have been different had all SSC mothers adhered to the SSC guidelines because baseline characteristics in SSC mothers who adhered were not different from SSC mothers who did not. Future trials focusing on SSC protocol adherence are warranted.
The results of the PP and exploratory DR analyses are consistent with prior research. A systematic review on SSC immediately after birth in full‐term infants showed higher breastfeeding rates and longer continued breastfeeding in SSC vs. control dyads (Moore et al., 2016). Similarly, prior research on SSC dose–response effects found more SSC to be related to higher exclusive breastfeeding rates during maternity hospitalization (Bramson et al., 2010). Moreover, the only study on daily SSC in full‐term infants found that SSC mothers provided longer breastfeeding than control mothers (Bigelow et al., 2014). The present study found comparable benefits when comparing CAU dyads with SSC dyads who adhered to the daily hour of SSC. Moreover, as most CAU mothers also performed some SSC (largely during the first post‐natal days; Figure 2), these results suggest that the beneficial effects of this intervention add to the beneficial effects of SSC during the first post‐natal hours. More research is needed to confirm this notion. Additionally, dose–response effects suggest that the benefits for breastfeeding duration increase with increasing total SSC duration over the 5‐week intervention period. Because these results were derived from exploratory analyses, future studies are required to confirm these promising findings.
Difference from previous studies is that the present study found no effects of SSC on breastfeeding when including all dyads irrespective of compliance or withdrawal. The only prior study on daily SSC and breastfeeding in full‐term infants used a quasi‐experimental design instead of a randomized controlled design (Bigelow et al., 2014). In Bigelow's study, SSC mothers were informed about SSC before consent, which may have led to a sampling bias and the inclusion of only highly motivated SSC mothers. Indeed, although a much more time‐intensive SSC protocol was requested (Week 1: six daily SSC hours; Weeks 2–4: two daily SSC hours; and SSC inclusion criteria: ≥4000 min of SSC in the first month), most mothers adhered to it despite no actions to promote adherence. In contrast, the present study included a randomized controlled design and allocated mothers irrespective of their motivation to perform SSC. Possibly due to the study design, low adherence rates were observed in the current trial. As a result, the promising PP findings are likely underpowered. Effects may have been stronger and detected in the ITT framework as well had greater adherence rates been achieved. However, we also acknowledge the possibility that the differences between the groups in the PP analyses might not have been due to daily SSC.
The underlying working mechanisms that relate daily SSC to longer breastfeeding duration are largely unknown. One possible underlying mechanism is breastfeeding frequency. Potentially, SSC provides extra opportunities for breastfeeding and, in turn, may extend exclusive and continued breastfeeding duration. We examined this explanation post hoc by using weekly breastfeeding frequency data during the 5‐week intervention period. Daily breastfeeding frequency was comparable in the SSC group vs. the CAU group for the PP selection (7.99 ± 2.36 vs. 7.20 ± 2.92; adjusted mean difference −0.79, 95% CI −2.30 to 0.73; p = 0.30). As such, this explanation is less likely. Another possible underlying mechanism is that SSC may stimulate optimal infant breastfeeding behaviour. Early SSC promotes better coordinated suckling (Srivastava et al., 2014). As such, a mother who engages in regular SSC may experience fewer breastfeeding problems and feel improved breastfeeding self‐efficacy, or confidence in her ability to breastfeed her infant (Aghdas et al., 2014; Nimbalkar et al., 2016). In turn, these factors are crucial predictors for breastfeeding duration (Meedya et al., 2010; Odom et al., 2013). A third potential underlying mechanism is the hormone oxytocin. During SSC, nerve fibres related to touch are stimulated. This contributes to the activation of the oxytocinergic system, releasing oxytocin into the maternal body (UvnäsMoberg et al., 2020; Uvnäs‐Moberg et al., 2015). Prior research shows that elevated oxytocin concentrations are related to milk ejection and production (Uvnäs‐Moberg et al., 2020); this may in turn facilitate longer exclusive and continued breastfeeding duration. Future research on potential underlying mechanisms is needed to deepen the understanding of the effects of SSC on breastfeeding duration.
The current study has several major strengths. First, it was an RCT that was preregistered, which improves transparency and reproducibility of the findings. Second, we employed a relatively long follow‐up period after the intervention, and retention rates were high for a time‐intensive intervention study. Although the study has strengths, it also has some limitations. First, the baseline characteristics indicate a sampling bias. Almost all mothers were highly educated, had the intention to breastfeed their infant and were mostly recruited from a group interested in research participation, which compromises the generalizability of the results. Second, the percentage of missingness was small, but missingness was not completely at random and could only partly explained by maternal educational level. This may have affected the results. Third, breastfeeding information was based on a 1‐year recall, which could lead to a recall bias. However, prior research shows that maternal recall for breastfeeding duration is reliable, even up to 20 years, especially if the recalled period is shorter than 3 years (Li et al., 2005; Natland et al., 2012). Finally, mothers reported their intended breastfeeding duration during the late pregnancy home visit, minutes after the randomization had taken place. Adjusting for a postrandomization outcome that is on the causal pathway to the outcome is not optimal. Nonetheless, we controlled for intended breastfeeding duration in our analyses because it is recommended in the literature (see review by Moore et al., 2016) and because despite randomization, there were significant differences in intended breastfeeding duration between the SSC and CAU mothers in the ITT and PP samples. Controlling for intended breastfeeding duration did not affect our results. Future studies in more heterogeneous samples are essential to examine the effectiveness of daily SSC on breastfeeding duration.
5. CONCLUSION
To our knowledge, this is the first study that examined the effectiveness of a daily SSC intervention in healthy mothers and full‐term infants on exclusive and continued breastfeeding duration using an RCT. For the total group, this study indicates that daily SSC did not extend exclusive and continued breastfeeding duration. However, the findings based on only mothers who adhered to the SSC protocol are promising. The findings from the current trial provide preliminary scientific support that daily SSC in the first 5 weeks post‐partum may be a simple and cost‐effective way to extend the period of exclusive and continued breastfeeding duration in mothers and full‐term infants. These findings suggest that it may be important to encourage new mothers to engage in a daily hour of SSC to increase breastfeeding duration in the first post‐natal year. Hopefully, given the importance of breastfeeding and its long‐lasting benefits for children and mothers, this study will inspire replication attempts in more heterogeneous samples with more focus on protocol adherence.
CONFLICTS OF INTEREST
The authors declare that they have no conflicts of interest.
CONTRIBUTIONS
KHMC conceptualized and designed the study, collected the data, carried out the initial analyses, drafted the initial manuscript and revised the manuscript. RB and CdW conceptualized and designed the study, contributed to the interpretation of the data, and critically reviewed and revised the manuscript for important intellectual content. BEB contributed to the interpretation of the data, and critically reviewed and revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Supporting information
Table S1. CONSORT 2010 checklist of information to include when reporting a randomised trial*
ACKNOWLEDGEMENTS
We would like to thank the families who participated in the SKIPPY study and all research assistants and students for their assistance with data collection and data processing. This study was supported by the graduate school of the Behavioural Science institute, Radboud University; the Jacobs Foundation (Advanced Research Fellowship to CdW); and the Netherlands Organization for Scientific Research (Nederlandse Organisatie voor Wetenschappelijk Onderzoek) (VENI Grant 016.195.197 to RB; VICI Grant 016.Vici.185.038 to CdW). The funders had no role in study design, data collection, analysis, interpretation of data, writing of the report or the decision to submit the manuscript for publication.
Cooijmans, K. H. M. , Beijers, R. , Brett, B. E. , & de Weerth, C. (2021). Daily skin‐to‐skin contact in full‐term infants and breastfeeding: Secondary outcomes from a randomized controlled trial. Maternal & Child Nutrition, 18:e13241. 10.1111/mcn.13241
DATA AVAILABILITY STATEMENT
The data are not freely available, as we did not ask participants to consent to store deidentified data in an online depository. Deidentified individual participant data that underlie the results reported in this article will be made available upon publication (no end date) to researchers with a methodologically sound proposal for reuse of the data. The proposal should be directed to carolina.deweerth@radboudumc.nl. Upon approval, data requestors will need to sign a data transfer agreement. Researchers are asked to analyse the data and/or publish the results within 2 years.
REFERENCES
- Aghdas, K. , Talat, K. , & Sepideh, B. (2014). Effect of immediate and continuous mother infant skin‐to‐skin contact on breastfeeding self‐efficacy of primiparous women: A randomized control trial. Women and Birth, 27(1), 37–40. 10.1016/j.wombi.2013.09.004 [DOI] [PubMed] [Google Scholar]
- Barr, R. G. , Kramer, M. S. , Boisjoly, C. , McVey‐White, L. , & Pless, I. B. (1988). Parental diary of infant cry and fuss behaviour. Archives of Disease in Childhood, 63, 380–387. 10.1136/adc.63.4.380 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beijers, R. , Riksen‐Walraven, J. M. , & de Weerth, C. (2013). Cortisol regulation in 12‐month‐old human infants: Associations with the infants' early history of breastfeeding and co‐sleeping. Stress, 16(3), 267–277. 10.3109/10253890.2012.742057 [DOI] [PubMed] [Google Scholar]
- Bigelow, A. E. , Power, M. , Gillis, D. E. , Maclellan‐Peters, J. , Alex, M. , & MacDonald, C. (2014). Breastfeeding, skin‐to‐skin contact, and mother–infant interactions over infants' first three months. Infant Mental Health Journal, 35(1), 51–62. 10.1002/imhj.21424 [DOI] [PubMed] [Google Scholar]
- Bigelow, A. E. , Power, M. , MacLellan‐Peters, J. , Alex, M. , & McDonald, C. (2012). Effect of mother/infant skin‐to‐skin contact on postpartum depressive symptoms and maternal physiological stress. Journal of Obstetric, Gynecologic & Neonatal Nursing, 41(3), 369–382. 10.1111/j.1552-6909.2012.01350.x [DOI] [PubMed] [Google Scholar]
- Bramson, L. , Lee, J. W. , Moore, E. , Montgomery, S. , Neish, C. , Bahjri, K. , & Melcher, C. L. (2010). Effect of early skin‐to‐skin mother–infant contact during the first 3 hours following birth on exclusive breastfeeding during the maternity hospital stay. Journal of Human Lactation, 26(2), 130–137. 10.1177/0890334409355779 [DOI] [PubMed] [Google Scholar]
- Conde‐Agudelo, A. , & Díaz‐Rossello, J. L. (2016). Kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Cochrane Database of Systematic Reviews, 8, CD002771. 10.1002/14651858.CD002771.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooijmans, K. H. M. , Beijers, R. , Brett, B. E. , & De Weerth, C. (2021). Daily skin‐to‐skin contact and mental health in mothers of full‐term infants: A randomized controlled trial. Manuscript submitted for publication.
- Cooijmans, K. H. M. , Beijers, R. , Rovers, A. C. , & de Weerth, C. (2017). Effectiveness of skin‐to‐skin contact versus care‐as‐usual in mothers and their full‐term infants: Study protocol for a parallel‐group randomized controlled trial. BMC Pediatrics, 17(1), 154. 10.1186/s12887-017-0906-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flacking, R. , Ewald, U. , & Wallin, L. (2011). Positive effect of kangaroo mother care on long‐term breastfeeding in very preterm infants. Journal of Obstetric, Gynecologic, and Neonatal Nursing, 40(2), 190–197. 10.1111/j.1552-6909.2011.01226.x [DOI] [PubMed] [Google Scholar]
- Gilmore, L. A. , Klempel, M. C. , Martin, C. K. , Myers, C. A. , Burton, J. H. , Sutton, E. F. , & Redman, L. M. (2017). Personalized mobile health intervention for health and weight loss in postpartum women receiving women, infants, and children benefit: A randomized controlled pilot study. Journal of Women's Health, 26(7), 719–727. 10.1089/jwh.2016.5947 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haroon, S. , Das, J. K. , Salam, R. A. , Imdad, A. , & Bhutta, Z. A. (2013). Breastfeeding promotion interventions and breastfeeding practices: A systematic review. BMC Public Health, 13, S20. 10.1186/1471-2458-13-S3-S20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hernán, M. A. , & Hernández‐Díaz, S. (2012). Beyond the intention‐to‐treat in comparative effectiveness research. Clinical Trials, 9(1), 48–55. 10.1177/1740774511420743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kramer, M. S. , & Kakuma, R. (2012). Optimal duration of exclusive breastfeeding. Cochrane Database of Systematic Reviews, 8, CD003517. 10.1002/14651858.CD003517.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li, R. , Scanlon, K. S. , & Serdula, M. K. (2005). The validity and reliability of maternal recall of breastfeeding practice. Nutrition Reviews, 63(4), 103–110. 10.1111/j.1753-4887.2005.tb00128.x [DOI] [PubMed] [Google Scholar]
- Liu, Y. , & Brown, S. D. (2013). Comparison of five iterative imputation methods for multivariate classification. Chemometrics and Intelligent Laboratory Systems, 120, 106–115. 10.1016/j.chemolab.2012.11.010 [DOI] [Google Scholar]
- Maastrup, R. , Hansen, B. M. , Kronborg, H. , Bojessen, S. N. , Hallum, K. , Frandsen, A. , Kyhnaeb, A. , Svarer, I. , & Hallström, I. (2014). Breastfeeding progression in preterm infants is influenced by factors in infants, mothers and clinical practice: The results of a national cohort study with high breastfeeding initiation rates. PLoS ONE, 9(9), e108208. 10.1371/journal.pone.0108208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- McFadden, A. , Gavine, S. , Renfrew, M. J. , Wade, A. , Buchanan, P. , Taylor, J. L. , Veitch, E. , Renni, A. M. , Crowther, S. A. , Neiman, S. , & MacGillivray, S. (2017). Support for healthy breastfeeding mothers with healthy term babies. Cochrane Database of Systematic Reviews, 5, CD001141. 10.1002/14651858.CD001141.pub5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meedya, S. , Fahy, K. , & Kable, A. (2010). Factors that positively influence breastfeeding duration to 6 months: A literature review. Women and Birth, 23(4), 135–145. 10.1016/j.wombi.2010.02.002 [DOI] [PubMed] [Google Scholar]
- Moore, E. R. , Bergman, N. , Anderson, G. C. , & Medley, N. (2016). Early skin‐to‐skin contact for mothers and their healthy newborn infants. Cochrane Database of Systematic Reviews, 11, CD003519. 10.1002/14651858.CD003519.pub4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Natland, S. T. , Andersen, L. F. , Nilsen, T. I. L. , Forsmo, S. , & Jacobsen, G. W. (2012). Maternal recall of breastfeeding duration twenty years after delivery. BMC Medical Research Methodology, 12, 179. 10.1186/1471-2288-12-179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nimbalkar, A. S. , Patel, D. V. , Nimbalkar, S. M. , Patel, V. K. , Patel, D. N. , & Phatak, A. G. (2016). Infant and young child feeding practices in infants receiving skin to skin care at birth: Follow‐up of randomized cohort. Journal of Clinical and Diagnostic Research, 10(12), SC09–SC12. 10.7860/jcdr/2016/22930.9003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odom, E. C. , Li, R. , Scanlon, K. S. , Perrine, C. G. , & Grummer‐Strawn, L. (2013). Reasons for earlier than desired cessation of breastfeeding. Pediatrics, 131(3), e726–e732. 10.1542/peds.2012-1295 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peeters, D. , Lanting, C. I. , & van Wouwe, J. P. (2015). Peiling melkvoeding van zuigelingen 2015. https://www.tno.nl/media/5248/peiling-melkvoeding-van-zuigelingen-2015.pdf
- Sinha, B. , Chowdhury, R. , Sankar, M. J. , Martines, J. , Taneja, S. , Mazumder, S. , Rollins, N. , Bahl, R. , & Bhandari, N. (2015). Interventions to improve breastfeeding outcomes: A systematic review and meta‐analysis. Acta Paediatrica, 104(s467), 114–135. 10.1111/apa.13127 [DOI] [PubMed] [Google Scholar]
- Srivastava, S. , Gupta, A. , Bhatnagar, A. , & Dutta, S. (2014). Effect of very early skin to skin contact on success at breastfeeding and preventing early hypothermia in neonates. Indian Journal of Public Health, 58(1), 22–26. 10.4103/0019-557X.128160 [DOI] [PubMed] [Google Scholar]
- Swift, J. K. , & Greenberg, R. P. (2012). Premature discontinuation in adult psychotherapy: A meta‐analysis. Journal of Consulting and Clinical Psychology, 80(4), 547–559. 10.1037/a0028226 [DOI] [PubMed] [Google Scholar]
- Tukey, J. W. (1977). Exploratory data analysis. Reading: Addison Wesley. [Google Scholar]
- UNICEF . (2017). Guide to the Unicef UK Baby Friendly Initiative standards. https://www.unicef.org.uk/babyfriendly/wp-content/uploads/sites/2/2014/02/Guide-to-the-Unicef-UK-Baby-Friendly-Initiative-Standards.pdf
- UvnäsMoberg, K. , Ekström‐Bergström, A. , Buckley, S. , Massarotti, C. , Pajalic, Z. , Luegmair, K. , Kotlowska, A. , Lengler, L. , Olza, I. , Grylka‐Baeschlin, S. , Leahy‐Warren, P. , Hadjigeorgiu, E. , Villarmea, S. , & Dencker, A. (2020). Maternal plasma levels of oxytocin during breastfeeding—A systematic review. PLoS ONE, 15(8), e0235806. 10.1371/journal.pone.0235806 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uvnäs‐Moberg, K. , Handlin, L. , & Petersson, M. (2015). Self‐soothing behaviors with particular reference to oxytocin release induced by non‐noxious sensory stimulation. Frontiers in Psychology, 5, 1529. 10.3389/fpsyg.2014.01529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uvnäs‐Moberg, K. , Handlin, L. , & Petersson, M. (2020). Neuroendocrine mechanisms involved in the physiological effects caused by skin‐to‐skin contact—With a particular focus on the oxytocinergic system. Infant Behavior and Development, 61, 101482. 10.1016/j.infbeh.2020.101482 [DOI] [PubMed] [Google Scholar]
- Victora, C. G. , Bahl, R. , Barros, A. J. , França, G. V. , Horton, S. , Krasevec, J. , Murch, S. , Sankar, M. J. , Walker, N. , & Rollins, N. C. (2016). Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. The Lancet, 387, 475–490. 10.1016/S0140-6736(15)01024-7 [DOI] [PubMed] [Google Scholar]
- World Health Organization . (2003). Kangaroo mother care: A practical guide. http://www.who.int/maternal_child_adolescent/documents/9241590351/en/
- World Health Organization . (2013a.) Long‐term effects of breastfeeding: A systematic review. https://apps.who.int/iris/bitstream/handle/10665/79198/9789241505307eng.pdf;jsessionid=42DEFC1D08049476184ED3A41685C07B?sequence=1
- World Health Organization . (2013b). Short‐term effects of breastfeeding: A systematic review of the benefits of breastfeeding on diarrhea and pneumonia mortality. https://apps.who.int/iris/bitstream/handle/10665/95585/9789241506120_eng.pdf?sequence=1&isAllowed=y
- World Health Organization . (2021). Breastfeeding. https://www.who.int/health-topics/breastfeeding#tab=tab_1
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. CONSORT 2010 checklist of information to include when reporting a randomised trial*
Data Availability Statement
The data are not freely available, as we did not ask participants to consent to store deidentified data in an online depository. Deidentified individual participant data that underlie the results reported in this article will be made available upon publication (no end date) to researchers with a methodologically sound proposal for reuse of the data. The proposal should be directed to carolina.deweerth@radboudumc.nl. Upon approval, data requestors will need to sign a data transfer agreement. Researchers are asked to analyse the data and/or publish the results within 2 years.