

Despite effective treatment with coronary artery bypass grafting (CABG), patients with coronary artery disease face an elevated risk of heart failure (HF) and cardiovascular (CV) death. Left atrial (LA) strain has previously been shown to be an important determinant of outcomes, including atrial fibrillation in patients with CABG (1). We hypothesized that LA reservoir strain predicts HF and CV death in patients undergoing CABG, even in patients with a normal LA size.
We included 782 patients scheduled for CABG in a retrospective cohort study. Patients with known significant valvular disease, CABG performed as rescue treatment, inadequate image quality for speckle-tracking echocardiography, and patients in atrial fibrillation rhythm during the echocardiogram were excluded. In total, 555 patients with echocardiography a median 14 days (interquartile range: 8 to 30 days) before surgery were studied. Demographic and clinical data were collected from hospital charts. The endpoint was defined as a composite of incident HF and/or CV death. Follow-up data on incident HF were obtained from the National Patient Registry and defined as new hospitalizations; data on CV deaths were obtained from the National Causes of Death Registry. All endpoints were validated through review of the hospital charts. Under Danish law, retrospective studies do not require approval from Health Research Ethics Committee.
Echocardiographic analyses were performed according to guidelines (2). LA speckle-tracking analysis was performed as biplane analysis to acquire LA reservoir (εs), conduit, and contraction (εa) strain.
Cox proportional hazards regression and Harrell’s C-statistics were used to assess the prognostic value of LA strain. Adjustment was made for: age, sex, hypertension, diabetes mellitus, peripheral artery disease, creatinine, left ventricular ejection fraction, ratio between early mitral inflow velocity and mitral annular early diastolic velocity >14, and global longitudinal strain. Cumulative incidence curves were created for high versus low εs (cutoff 27.4%).
Of 555 patients, 53 (10%) developed incident HF and/or CV death (29 developed HF, 24 developed CV death, and 6 developed both) during a median follow-up time of 3.7 years (interquartile range: 2.7 to 4.8 years). Overall, 83% were men, mean age was 67 years, LVEF was 51%, and mean EuroSCORE II was 1.31% (interquartile range: 0.94% to 1.96%). Patients developing the outcome had impaired LA function (εs: 22% vs. 28%; εa: 12% vs. 15%; LA conduit strain: 10% vs. 12%). No difference in occurrence of postoperative atrial fibrillation between the outcome groups was found. Postoperative atrial fibrillation was defined as any length of either symptomatic or asymptomatic episodes of atrial fibrillation detected and reported in the hospital chart during the postoperative in-hospital stay.
Atrial strain measures were univariable predictors of outcome (Figure 1). εs provided the highest C-statistic of 0.66. After adjusting for confounding variables, εs and εa remained independent predictors of outcome. Patients with low atrial strains had >2-fold increased risk of the outcome. In patients with LA volume <34 ml/m2, εs remained an independent predictor of outcome (hazard ratio of 1.06 [1.01 to 1.11; p = 0.021] per 1% decrease).
FIGURE 1. Cumulative Incidence Curve and Forest Plot.
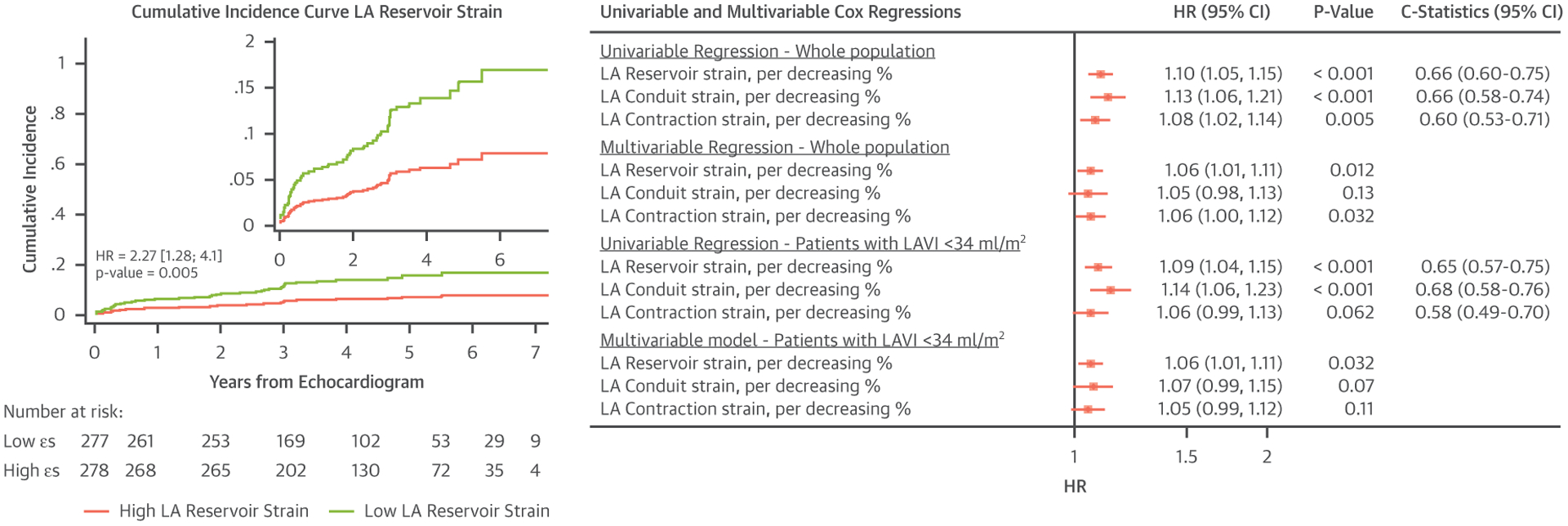
Cumulative incidence curve for left atrial (LA) reservoir showing the estimated incidence of heart failure and/or cardiovascular death between the high and low LA reservoir (εs) strain group (cutoff 27.4%). Forest plot for univariable and multivariable Cox regressions. Multivariable adjustments included age, sex, hypertension, diabetes mellitus, peripheral artery disease, creatinine, left ventricular ejection fraction, ratio between early mitral inflow velocity and mitral annular early diastolic velocity >14, and global longitudinal strain. HR = hazard ratio; LAVI = left ventricular volume index; x-axis = time from echocardiography examination; y-axis = cumulative incidence of the endpoint.
This study showed the strong association between LA mechanics and the development of the outcome in patients with CABG. All findings were adjusted for global longitudinal strain and show potential value irrespective of this measurement. In patients with normal LA volume, εs remained a significant predictor of the outcome. Changes in LA deformation appearing before any increase in LA volume are underlining the value of looking beyond LA size. A previous study (3) found εs and εa to be strongly impaired in patients with HF with reduced ejection fraction, independent of changes in global longitudinal strain and LA volume, which suggests that atrial strain is a more sensitive marker of atrial dysfunction than LA size. More so, they found that LA reservoir function had the potential to recover in weeks if decongestive therapy was performed. Impaired εs after decongestion was shown to be associated with higher risk of HF and all-cause death.
In conclusion, εs and εa are independent predictors of HF and CV death after CABG and add prognostic information, even in patients with normal LA size.
Footnotes
Please note: The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The authors attest they are in compliance with human studies committees and animal welfare regulations of the authors’ institutions and Food and Drug Administration guidelines, including patient consent where appropriate. For more information, visit the JACC: Cardiovascular Imaging author instructions page.
REFERENCES
- 1.Gabrielli L, Corbalan R, Córdova S, et al. Left atrial dysfunction is a predictor of postcoronary artery bypass atrial fibrillation: association of left atrial strain and strain rate assessed by speckle tracking: left atrial strain and postoperative atrial fibrillation. Echocardiography 2011;28: 1104–8. [DOI] [PubMed] [Google Scholar]
- 2.Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging 2015; 16:233–71. [DOI] [PubMed] [Google Scholar]
- 3.Deferm S, Martens P, Verbrugge FH, et al. LA mechanics in decompensated heart failure: insights from strain echocardiography with invasive hemodynamics. J Am Coll Cardiol Img 2020;13:1107–15. [DOI] [PubMed] [Google Scholar]