

Abstract
Prognosis of hepatocellular carcinoma (HCC) could be affected by lack of or delayed therapy. We aimed to characterize the prevalence, correlates, and clinical impact of therapeutic underuse and delay in patients with HCC. Patients with HCC diagnosed between 2010 and 2017 were analyzed from the United States National Cancer Database. Logistic regression analysis identified factors associated with no and delayed (>90 days after diagnosis) HCC treatment. Cox proportional hazards regression with landmark analysis assessed the association between therapeutic delay and overall survival (OS), accounting for immortal time bias. Of 116,299 patients with HCC, 24.2% received no treatment and 18.4% of treated patients had delayed treatment. Older age, Black, Hispanic, lower socioeconomic status, earlier year of diagnosis, treatment at nonacademic centers, Northeast region, increased medical comorbidity, worse liver dysfunction, and higher tumor burden were associated with no treatment. Among treated patients, younger age, Hispanic, Black, treatment at academic centers, West region, earlier tumor stage, and receipt of noncurative treatment were associated with treatment delays. In multivariable Cox regression with a landmark of 150 days, patients with and without treatment delays had similar OS (adjusted hazard ratio [aHR], 1.01; 95% confidence interval [CI], 0.98‐1.04) with a median survival of 33.7 vs. 32.1 months, respectively. However, therapeutic delay was associated with worse OS in patients who had tumor, nodes, and metastases (TNM) stage 1 (aHR, 1.06; 95% CI, 1.01‐1.11) or received curative treatment (aHR, 1.12; 95% CI, 1.05‐1.18). Conclusion: One‐fourth of patients with HCC receive no therapy and one‐fifth of treated patients experience treatment delays. Both were associated with demographic, socioeconomic, and clinical characteristics of patients as well as facility type and region. The association between therapeutic delay and survival was stage and treatment dependent.
One‐fourth of HCC patients receive no therapy and one‐fifth of treated patients experience treatment delays. Both were associated with demographic, socioeconomic, clinical characteristics of patients, facility type, and regions. The association between therapeutic delay and survival was stage‐ and treatment‐dependent. Therapeutic delay was associated with worse OS in patients who had early‐stage HCC or received curative treatment.

Abbreviations
- AFP
alpha‐fetoprotein
- aHR
adjusted hazard ratio
- CI
confidence interval
- CoC
Commission on Cancer
- HCC
hepatocellular carcinoma
- IQR
interquartile ratio
- MELD
Model for End‐Stage Liver Disease
- NCDB
National Cancer Database
- OS
overall survival
- SES
socioeconomic class
- TNM
tumor, nodes, and metastases
- US
United States
Hepatocellular carcinoma (HCC) continues to be one of the fastest rising cancers globally and locally, with increasing mortality rates.( 1 , 2 ) Patients diagnosed at an early stage are eligible for curative treatment options, with 5‐year survival exceeding 60%.( 3 , 4 , 5 ) Increasing efforts, therefore, have focused on improving surveillance to detect HCC at an early stage.( 6 , 7 ) While timely guideline‐concordant follow‐up and treatment are required for early cancer detection to translate into improved overall survival (OS),( 8 ) single‐center studies suggest pervasive downstream failures in the HCC care continuum.( 9 )
Underuse and therapeutic delays in cancer care are in part attributable to interrelated disparities in health care use and access to therapy, including racial and ethnic inequities in the delivery of appropriate care, with lower rates of treatment among elderly, Black individuals, and those of lower socioeconomic class (SES).( 10 ) In addition, cancer care is a complex and multistep process influenced by several patient factors (fear of treatment, adherence rates, access to resources, cultural preferences, clinical factors), provider factors (knowledge, coordination of care, timely references to specialists), and systemic factors (logistics, national and regional policies, multidisciplinary team). If the care continuum is disrupted at any of these levels, it can lead to suboptimal and delayed therapy, with an enormous economic burden.10
Given the rapid tumor doubling time of HCC, there is a concern that even brief therapeutic delays could lead to tumor progression, stage migration, and poor survival outcomes.( 11 ) However, studies in other malignancies have demonstrated mixed results, with delayed treatment being associated with worse survival in some but not others.( 12 , 13 , 14 , 15 , 16 ) Understanding the clinical impact of HCC therapeutic delays is highly relevant and timely considering the ongoing coronavirus disease 2019 (COVID‐19) pandemic and its impact on health care delivery and outcome.( 17 , 18 , 19 ) A recent international survey from 76 centers found most centers reported delays in HCC treatments related to the COVID‐19 pandemic.( 20 ) Although single‐center studies have evaluated HCC treatment underuse and delays,( 9 , 21 , 22 , 23 ) no large‐scale study has characterized no therapy and therapeutic delays in a national cohort of United States (US) patients. Therefore, our study investigated the nationwide prevalence, correlates, and clinical impact of no therapy and delayed therapy among patients with HCC in the United States.
Patients and Methods
Database
The National Cancer Database (NCDB) is a large, comprehensive, nationwide clinical oncology database containing more than 70% of newly diagnosed cancer cases in the United States.( 24 ) It is a joint project of the Commission on Cancer (CoC) of the American College of Surgeons and the American Cancer Society. It is sourced from hospital registry data collected in more than 1,500 CoC‐accredited cancer facilities in the United States and Puerto Rico. The NCDB contains approximately 34 million records from hospital cancer registries across the United States and Puerto Rico. Data elements are collected and submitted to the NCDB from CoC‐accredited cancer program registries using nationally standardized data item and coding definitions, as specified in the CoC's Facility Oncology Registry Data Standards, and nationally standardized data transmission format specifications coordinated by the North American Association of Central Cancer Registries.
Patients and Variables
All patients with HCC diagnosed between 2010 and 2017 were identified from the NCDB. HCC diagnosis was based on the International Classification of Disease Oncology, Third Edition, code C22.0 and the histology codes 8170‐8175. Patients with missing treatment information, including time to treatment initiation, were excluded (Supporting Fig. S1).
Demographic, socioeconomic, reporting medical facilities, and clinical information of patients were extracted from the NCDB. Patient demographic information included age, sex, and race/ethnicity. The extracted socioeconomic data included insurance status, income (median household income for patient zip code based on the 2016 American Community Survey data, in quartiles), education (median percentage of adults age 25 years or older in the patient's zip code with a high school degree based on 2016 American Community Survey data), and living community type (metropolitan, urban, rural). The treatment facilities data included the facility type and their geographic location. The facility type was categorized into academic (>500 new cancer diagnoses annually and at least four postgraduate training programs), comprehensive community (>500 new cancer diagnoses annually), integrated network (no minimum caseload, joint venture with multiple facilities providing integrated cancer care and comprehensive services, with at least one facility in the category being a hospital and a CoC‐accredited cancer program), and community (100‐500 new cancer diagnoses annually). The collected clinical data included Charlson/Deyo comorbidity index (0, 1, 2, ≥3), alpha‐fetoprotein (AFP) (normal vs. elevated), Model for End‐Stage Liver Disease (MELD) score, tumor size, and treatment modality. Tumor, nodes, and metastases (TNM) staging was based on the seventh edition of the American Joint Committee on Cancer. Curative treatment included tumor ablation, liver resection, and liver transplantation. For patients who received multiple courses of treatments, NCDB reports the most curative treatment (i.e., liver transplantation > resection > ablation > noncurative treatment) as the type of treatment.
In contrast, time to treatment was defined by date of the first treatment that the patient received. The number of days between the date of HCC diagnosis and date of first treatment that patients received at any facility, including treatment received from non‐CoC‐accredited cancer programs, was calculated. For instance, a patient who underwent bridging therapy with transarterial chemoembolization (TACE) and then underwent liver transplantation would have days from diagnosis to first TACE recorded. Treatment delay was defined as time from diagnosis to treatment exceeding 90 days based on HCC doubling time and as used in prior publications.( 9 , 21 , 25 ) Institutional review board review was exempted as the study involved the analysis of the de‐identified data set.
Statistical Analysis
Baseline and demographic characteristics were summarized by standard descriptive measures (frequency and percentage for categorical variables and mean ± SD or median with interquartile range [IQR] for continuous variables). These characteristics were then compared by receipt of treatment and treatment delay using the Pearson’s chi‐squared test for categorical variables and the Welch’s t test or the Mann‐Whitney‐Wilcoxon test for continuous variables, as appropriate. Survival probabilities were estimated using the Kaplan‐Meier method and compared using the log‐rank test. Median survival was estimated using the reverse Kaplan‐Meier method.
All multivariable analyses were performed on the full respective cohort with missing data imputed using the multivariate imputation by chained equation approach.( 26 ) Missing data rates were assessed for all covariates included in the multivariable model and were as follows: race/ethnicity (0.28%), insurance (1.3%), education (7.8%), income (7.9%), community (2.6%), facility type (1.0%), region (1.0%), TNM stage (7.4%), MELD (28.5%), tumor size (24.2%), and AFP (13.2%). Multiple imputations replace missing data with estimates based on a multivariable model that follows the same distribution of the missing data. We generated five complete data sets with five iterations using the predictive mean‐matching method among missing covariates to account for the uncertainty around the true value of the missing data and to obtain approximately unbiased estimates. The multivariable estimates from the fitted model were the aggregated averages of the results of fitting the model among the five independent data sets, with variance equal to the imputation‐corrected variance/covariance matrix.
Factors associated with no receipt and delay in cancer treatment were identified using univariable and multivariable logistic regression. Factors associated with OS were estimated using univariable and multivariable Cox proportional hazards regression with time to event defined as the time from diagnosis to last follow‐up or death. Immortal time bias refers to a bias attributed to the period of follow‐up time where a patient is “immortal,” i.e., the patient needs to survive long enough to receive the exposure of interest (treatment delay in this study). This may select for more indolent tumors, with more favorable prognosis, thereby mitigating risk of stage migration and worse survival from treatment delays. In order to address the issue of immortal time bias, a landmark analysis was performed to evaluate the association between treatment delays and OS, with a designated landmark date of 150 days after HCC diagnosis.( 27 ) In this analysis, patients who died before the designated landmark time and those who received HCC treatment after the landmark were excluded, thus eliminating immortal time bias in the treatment‐delay group. Sensitivity analysis was further conducted with landmark dates of 120 and 180 days after HCC diagnosis.
All statistical analyses were performed using R statistical software (version 4.0.3; R Foundation, Vienna, Austria) with two‐sided tests and a significance level of 0.05.
Results
Patient Characteristics
Patient characteristics of the 116,299 patients with HCC are summarized in Table 1. The mean age of the population was 64 years, and the majority were men (76%). The cohort was racially diverse, with the greatest proportion being White (62%), followed by Black (15%), Hispanic (15%), and Asian/others (8.5%). More than half of the patients were treated at academic centers. In terms of their clinical status, half of the patients had no comorbidity and median MELD score was 12. Over one third (39%) had TNM stage 1 HCC, and median tumor size was 4.2 cm (IQR, 2.5‐7.2).
Table 1.
Patient characteristics by treatment status
| Characteristic | Treatment | Treatment delay | |||||
|---|---|---|---|---|---|---|---|
| Overall, n = 116,299 | No Treatment n = 28,147 | Treatment n = 88,152 | P Value | No Delay n = 71,845 | Treatment Delay n = 16,307 | P Value | |
| Age | <0.001 | <0.001 | |||||
| Mean (SD) | 64 (10) | 65 (11) | 64 (10) | 64 (10) | 63 (9) | ||
| Sex | 0.675 | 0.924 | |||||
| Male | 88,754 (76%) | 21,507 (76%) | 67,247 (76%) | 54,802 (76%) | 12,445 (76%) | ||
| Female | 27,545 (24%) | 6,640 (24%) | 20,905 (24%) | 17,043 (24%) | 3,862 (24%) | ||
| Race | <0.001 | <0.001 | |||||
| White | 71,444 (62%) | 16,463 (59%) | 54,981 (63%) | 45,477 (64%) | 9,504 (58%) | ||
| Hispanic | 17,103 (15%) | 4,802 (17%) | 12,301 (14%) | 9,572 (13%) | 2,729 (17%) | ||
| Black | 17,518 (15%) | 4,675 (17%) | 12,843 (15%) | 10,158 (14%) | 2,685 (17%) | ||
| Asian + others | 9,790 (8.5%) | 2,094 (7.5%) | 7,696 (8.8%) | 6,361 (8.9%) | 1,335 (8.2%) | ||
| Insurance status | <0.001 | <0.001 | |||||
| Not insured | 6,121 (5.4%) | 2,564 (9.3%) | 3,557 (4.1%) | 2,843 (4.0%) | 714 (4.4%) | ||
| Private | 34,705 (30%) | 6,290 (23%) | 28,415 (33%) | 23,405 (33%) | 5,010 (31%) | ||
| Medicaid/Medicare | 71,033 (62%) | 18,255 (66%) | 52,778 (61%) | 42,878 (61%) | 9,900 (62%) | ||
| Other | 2,345 (2.1%) | 461 (1.7%) | 1,884 (2.2%) | 1,458 (2.1%) | 426 (2.7%) | ||
| High school degree | <0.001 | <0.001 | |||||
| 82.4% or less | 31,981 (30%) | 9,119 (35%) | 22,862 (29%) | 18,216 (28%) | 4,646 (32%) | ||
| 82.5%‐89.1% | 28,793 (27%) | 7,329 (28%) | 21,464 (27%) | 17,497 (27%) | 3,967 (28%) | ||
| 89.2%‐93.7% | 25,844 (25%) | 6,032 (23%) | 19,812 (25%) | 16,372 (25%) | 3,440 (24%) | ||
| More than 93.7% | 18,612 (18%) | 3,724 (14%) | 14,888 (19%) | 12,543 (19%) | 2,345 (16%) | ||
| Median income | <0.001 | <0.001 | |||||
| Less than $40,227 | 26,430 (25%) | 7,498 (29%) | 18,932 (24%) | 15,199 (24%) | 3,733 (26%) | ||
| $40,227‐$50,353 | 24,247 (23%) | 6,332 (24%) | 17,915 (23%) | 14,633 (23%) | 3,282 (23%) | ||
| $50,354‐$63,332 | 23,722 (23%) | 5,743 (22%) | 17,979 (23%) | 14,672 (23%) | 3,307 (23%) | ||
| $63,333+ | 30,631 (29%) | 6,581 (25%) | 24,050 (30%) | 20,006 (31%) | 4,044 (28%) | ||
| Community type | 0.035 | 0.035 | |||||
| Metro | 97,915 (87%) | 23,878 (87%) | 74,037 (87%) | 60,197 (87%) | 13,840 (88%) | ||
| Urban | 13,227 (12%) | 3,250 (12%) | 9,977 (12%) | 8,207 (12%) | 1,770 (11%) | ||
| Rural | 1,520 (1.3%) | 414 (1.5%) | 1,106 (1.3%) | 916 (1.3%) | 190 (1.2%) | ||
| Facility type | <0.001 | <0.001 | |||||
| Academic | 65,963 (57%) | 10,946 (39%) | 55,017 (63%) | 43,801 (62%) | 11,216 (69%) | ||
| Community cancer program | 5,335 (4.6%) | 2,695 (9.7%) | 2,640 (3.0%) | 2,224 (3.1%) | 416 (2.6%) | ||
| Comprehensive community cancer program | 29,071 (25%) | 10,498 (38%) | 18,573 (21%) | 15,759 (22%) | 2,814 (17%) | ||
| Integrated network | 14,511 (13%) | 3,758 (13%) | 10,753 (12%) | 8,993 (13%) | 1,760 (11%) | ||
| Region | <0.001 | <0.001 | |||||
| Northeast | 23,119 (20%) | 5,178 (19%) | 17,941 (21%) | 14,522 (21%) | 3,419 (21%) | ||
| Midwest | 23,039 (20%) | 4,855 (17%) | 18,184 (21%) | 15,350 (22%) | 2,834 (17%) | ||
| South | 46,323 (40%) | 12,089 (43%) | 34,234 (39%) | 28,283 (40%) | 5,951 (37%) | ||
| West | 22,399 (19%) | 5,775 (21%) | 16,624 (19%) | 12,622 (18%) | 4,002 (25%) | ||
| Charlson comorbidity index | <0.001 | <0.001 | |||||
| 0 | 58,602 (50%) | 14,187 (50%) | 44,415 (50%) | 36,434 (51%) | 7,981 (49%) | ||
| 1 | 26,693 (23%) | 5,952 (21%) | 20,741 (24%) | 16,958 (24%) | 3,783 (23%) | ||
| 2 | 10,910(9.4%) | 2,375 (8.4%) | 8,535 (9.7%) | 6,863 (9.6%) | 1,672 (10%) | ||
| ≥3 | 20,094 (17%) | 5,633 (20%) | 14,461 (16%) | 11,590 (16%) | 2,871 (18%) | ||
| TNM stage | <0.001 | <0.001 | |||||
| Stage 1 | 40,233 (39%) | 5,900 (26%) | 34,333 (43%) | 26,798 (42%) | 7,535 (50%) | ||
| Stage 2 | 21,952 (21%) | 3,091 (14%) | 18,861 (24%) | 14,526 (23%) | 4,335 (29%) | ||
| Stage 3 | 21,336 (21%) | 6,179 (27%) | 15,157 (19%) | 12,912 (20%) | 2,245 (15%) | ||
| Stage 4 | 18,639 (18%) | 7,491 (33%) | 11,148 (14%) | 10,134 (16%) | 1,014 (6.7%) | ||
| MELD | <0.001 | 0.154 | |||||
| Median [IQR] | 12 [8, 19] | 16 [11, 24] | 11 [8, 16] | 11 [8, 17] | 11 [8, 16] | ||
| Tumor size, cm | <0.001 | <0.001 | |||||
| Median [IQR] | 4.2 [2.5, 7.2] | 5.7 [3.2, 9.2] | 3.9 [2.5, 6.7] | 4.0 [2.5, 7.0] | 3.2 [2.2, 5.0] | ||
| AFP | <0.001 | <0.001 | |||||
| Negative | 26,931 (29%) | 4,315 (21%) | 22,616 (31%) | 17,946 (30%) | 4,670 (34%) | ||
| Positive | 66,722 (71%) | 16,552 (79%) | 50,170 (69%) | 41,060 (70%) | 9,110 (66%) | ||
| Treatment | <0.001 | <0.001 | |||||
| Noncurative treatment | 55,095 (62%) | ‐ | 55,095 (62%) | 44,580 (62%) | 10,515 (64%) | ||
| Curative | 33,057 (38%) | ‐ | 33,057 (38%) | 27,265 (38%) | 5,792 (36%) | ||
| Liver transplant | 7,995 (24%) | 7,995 (24%) | 6,299 (23%) | 1,696 (29%) | |||
| Resection | 11,746 (36%) | 11,746 (36%) | 10,459 (38%) | 1,287 (22%) | |||
| Ablation | 13,316 (40%) | 13,316 (40%) | 10,507 (39%) | 2,809 (49%) | |||
There were 28,147 (24.2%) patients who received no HCC treatment; among those who were treated, 16,307 (18.4%) patients had a therapeutic delay. Between 2010 and 2017, the proportion of untreated patients decreased from 26.8% to 22.8% (P < 0.001); however, the proportion of those with treatment delays was stable between 17% and 19% (Fig. 1).
FIG. 1.
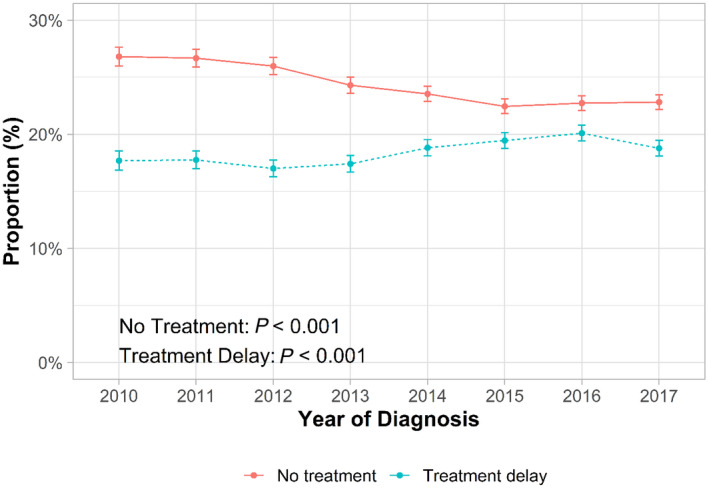
Trends in HCC treatment underuse and delay in treatment between 2010 and 2017. Error bars represent 95% CI.
Among patients who received HCC treatments, 38% received potentially curative treatment. Ablation was the most commonly used potentially curative treatment modality (40%), while 36% received surgical resection (36%) and 24% received liver transplant.
Factors Associated With No HCC Treatment
Patient demographics and SES, diagnosis year, medical facility type, region, and patient clinical characteristics were significantly associated with not receiving HCC treatment (Table 2 ). Demographic factors that increased the likelihood of no treatment included older age, Hispanic ethnicity or Black race compared to White race, and measures of lower SES (no insurance, living in a zip code area with lower income, and lower education). Several clinical characteristics were associated with higher odds of no HCC treatment, including increased medical comorbidity (Charlson comorbidity index ≥3), worse liver dysfunction (higher MELD score), and increased tumor burden (higher AFP and TNM stage). Finally, there were geographic and temporal variations in receipt of HCC treatment; receiving care at nonacademic programs, Northeast region (compared to Midwest/South), and early years of diagnosis were associated with higher odds of no HCC treatment. For every 1 year increase in the year of diagnosis, the odds of no HCC treatment decreased by 4%.
Table 2.
Factors associated with no receipt of HCC treatment
| Characteristic | Univariate | Multivariable | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | P Value | OR | 95% CI | P Value | |
| Age (10‐year change) | 1.17 | 1.16, 1.19 | <0.001 | 1.19 | 1.17, 1.22 | <0.001 |
| Sex | ||||||
| Male | — | — | — | — | ||
| Female | 0.99 | 0.96, 1.02 | 0.669 | 1.03 | 0.99,1.07 | 0.134 |
| Race | ||||||
| White | — | — | — | — | ||
| Hispanic | 1.30 | 1.26, 1.35 | <0.001 | 1.18 | 1.13, 1.23 | <0.001 |
| Black | 1.22 | 1.17, 1.26 | <0.001 | 1.16 | 1.11, 1.21 | <0.001 |
| Asian + others | 0.91 | 0.86, 0.96 | <0.001 | 0.94 | 0.89, 0.99 | 0.023 |
| Insurance status | ||||||
| Not insured | — | — | — | — | ||
| Private | 0.31 | 0.29, 0.33 | <0.001 | 0.37 | 0.35, 0.40 | <0.001 |
| Medicaid/Medicare | 0.48 | 0.45, 0.51 | <0.001 | 0.49 | 0.46, 0.52 | <0.001 |
| Other | 0.34 | 0.30, 0.38 | <0.001 | 0.40 | 0.35, 0.44 | <0.001 |
| High school | ||||||
| 82.4% or less | — | — | — | — | ||
| 82.5%‐89.1% | 0.86 | 0.83, 0.89 | <0.001 | 0.90 | 0.86, 0.93 | <0.001 |
| 89.2%‐93.7% | 0.76 | 0.74, 0.79 | <0.001 | 0.86 | 0.82, 0.91 | <0.001 |
| More than 93.7% | 0.63 | 0.60, 0.65 | <0.001 | 0.76 | 0.71, 0.80 | <0.001 |
| Median Income | ||||||
| Less than $40,227 | — | — | — | — | ||
| $40,227‐$50,353 | 0.89 | 0.86, 0.93 | <0.001 | 0.94 | 0.91, 0.99 | 0.007 |
| $50,354‐$63,332 | 0.81 | 0.77, 0.84 | <0.001 | 0.89 | 0.86, 0.94 | <0.001 |
| $63,333+ | 0.69 | 0.67, 0.72 | <0.001 | 0.87 | 0.83, 0.93 | <0.001 |
| Community type | ||||||
| Metro | — | — | — | — | ||
| Urban | 1.01 | 0.97, 1.05 | 0.643 | 0.91 | 0.87, 0.96 | <0.001 |
| Rural | 1.16 | 1.03, 1.30 | 0.010 | 0.96 | 0.83, 1.07 | 0.560 |
| Year of diagnosis | 0.96 | 0.96, 0.97 | <0.001 | 0.96 | 0.95, 0.96 | <0.001 |
| Facility type | ||||||
| Academic | — | — | — | — | ||
| Community cancer program | 5.13 | 4.84, 5.43 | <0.001 | 3.85 | 3.51, 3.96 | <0.001 |
| Comprehensive community cancer program | 2.84 | 2.75, 2.93 | <0.001 | 2.42 | 2.31, 2.48 | <0.001 |
| Integrated network | 1.76 | 1.68, 1.83 | <0.001 | 1.60 | 1.52, 1.66 | <0.001 |
| Region | ||||||
| Northeast | — | — | — | — | ||
| Midwest | 0.93 | 0.89, 0.97 | <0.001 | 0.82 | 0.79, 0.86 | <0.001 |
| South | 1.22 | 1.18, 1.27 | <0.001 | 0.93 | 0.89, 0.97 | <0.001 |
| West | 1.20 | 1.15, 1.26 | <0.001 | 1.02 | 0.97, 1.07 | 0.515 |
| Charlson comorbidity | ||||||
| 0 | — | — | — | — | ||
| 1 | 0.90 | 0.87, 0.93 | <0.001 | 0.91 | 0.88, 0.95 | <0.001 |
| 2 | 0.87 | 0.83, 0.91 | <0.001 | 0.93 | 0.89, 0.99 | 0.007 |
| ≥3 | 1.22 | 1.18, 1.26 | <0.001 | 1.33 | 1.29, 1.39 | <0.001 |
| TNM stage | ||||||
| Stage 1 | — | — | — | — | ||
| Stage 2 | 0.95 | 0.91, 1.00 | 0.048 | 0.97 | 0.93, 1.02 | 0.201 |
| Stage 3 | 2.37 | 2.28, 2.47 | <0.001 | 1.80 | 1.78, 1.92 | <0.001 |
| Stage 4 | 3.91 | 3.76, 4.07 | <0.001 | 2.59 | 2.57, 2.79 | <0.001 |
| AFP | ||||||
| Negative | — | — | — | — | ||
| Positive | 1.73 | 1.67, 1.79 | <0.001 | 1.22 | 1.16, 1.24 | <0.001 |
| MELD (10‐unit change) | 1.78 | 1.74, 1.81 | <0.001 | 1.33 | 1.31, 1.35 | <0.001 |
| Tumor size (1‐cm change) | 1.16 | 1.14, 1.18 | <0.001 | 1.00 | 1.00, 1.01 | <0.001 |
Abbreviation: OR, odds ratio.
Factors Associated With Delayed HCC Treatment
Among those who underwent HCC treatment, predictors of treatment delay are summarized in Table 3. There continued to be racial/ethnic disparities, with Hispanic ethnicity and Black race both associated with higher odds of HCC treatment delay, similar to their association with no HCC treatment. However, the association between age and treatment delay was discrepant, with younger patients having increased odds of treatment delays. Among clinical characteristics, poor prognostic factors, including higher tumor burden (positive AFP, higher TNM stage), were associated with decreased odds of treatment delay. We noted geographic differences in HCC treatment delays; receiving care at nonacademic programs and Midwest/South regions was associated with a decreased likelihood of treatment delays, while the West region was associated with increased odds of treatment delay. Finally, receipt of curative treatment was inversely associated with HCC treatment delay.
Table 3.
Factors associated with HCC treatment delay
| Characteristic | Univariate | Multivariable | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | P Value | OR | 95% CI | P Value | |
| Age (10‐year change) | 0.91 | 0.89, 0.92 | <0.001 | 0.85 | 0.83, 0.88 | <0.001 |
| Sex | ||||||
| Male | — | — | — | — | ||
| Female | 1.00 | 0.96, 1.04 | 0.916 | 1.02 | 0.96, 1.08 | 0.594 |
| Race | ||||||
| White | — | — | — | — | ||
| Hispanic | 1.36 | 1.30, 1.43 | <0.001 | 1.19 | 1.10, 1.28 | <0.001 |
| Black | 1.26 | 1.21, 1.33 | <0.001 | 1.26 | 1.16, 1.36 | <0.001 |
| Asian + others | 1.00 | 0.94, 1.07 | 0.895 | 0.90 | 0.81, 0.98 | 0.024 |
| Insurance status | ||||||
| Not insured | — | — | — | — | ||
| Private | 0.85 | 0.78, 0.93 | <0.001 | 0.89 | 0.77, 1.00 | 0.086 |
| Medicaid/Medicare | 0.92 | 0.85, 1.00 | 0.052 | 1.02 | 0.89, 1.15 | 0.764 |
| Other | 1.16 | 1.02, 1.33 | 0.029 | 1.21 | 0.98, 1.49 | 0.079 |
| High school degree | ||||||
| 82.4% or less | — | — | — | — | ||
| 82.5%‐89.1% | 0.89 | 0.85, 0.93 | <0.001 | 1.01 | 0.93, 1.07 | 0.796 |
| 89.2%‐93.7% | 0.82 | 0.78, 0.87 | <0.001 | 0.97 | 0.89, 1.05 | 0.489 |
| More than 93.7% | 0.73 | 0.69, 0.77 | <0.001 | 0.90 | 0.80, 0.98 | 0.037 |
| Median income | ||||||
| Less than $40,227 | — | — | — | — | ||
| $40,227‐$50,353 | 0.91 | 0.87, 0.96 | <0.001 | 0.95 | 0.86, 1.01 | 0.184 |
| $50,354‐$63,332 | 0.92 | 0.87, 0.97 | 0.001 | 0.94 | 0.87, 1.02 | 0.169 |
| $63,333+ | 0.82 | 0.78, 0.86 | <0.001 | 0.91 | 0.84, 1.01 | 0.055 |
| Community type | ||||||
| Metro | — | — | — | — | ||
| Urban | 0.94 | 0.89, 0.99 | 0.022 | 1.04 | 0.95, 1.13 | 0.362 |
| Rural | 0.90 | 0.77, 1.05 | 0.200 | 1.04 | 0.79, 1.27 | 0.763 |
| Year of diagnosis | 1.02 | 1.02, 1.03 | <0.001 | 1.02 | 1.00, 1.03 | 0.008 |
| Facility type | ||||||
| Academic | — | — | — | — | ||
| Community cancer program | 0.73 | 0.66, 0.81 | <0.001 | 0.74 | 0.61, 0.89 | 0.001 |
| Comprehensive community cancer program | 0.70 | 0.67, 0.73 | <0.001 | 0.67 | 0.63, 0.72 | <0.001 |
| Integrated network | 0.76 | 0.72, 0.81 | <0.001 | 0.79 | 0.72, 0.86 | <0.001 |
| Region | ||||||
| Northeast | — | — | — | — | ||
| Midwest | 0.78 | 0.74, 0.83 | <0.001 | 0.72 | 0.66, 0.78 | <0.001 |
| South | 0.89 | 0.85, 0.94 | <0.001 | 0.83 | 0.78, 0.90 | <0.001 |
| West | 1.35 | 1.28, 1.42 | <0.001 | 1.29 | 1.19, 1.39 | <0.001 |
| Charlson comorbidity index | ||||||
| 0 | — | — | — | — | ||
| 1 | 1.02 | 0.98, 1.06 | 0.404 | 1.01 | 0.94, 1.07 | 0.812 |
| 2 | 1.11 | 1.05, 1.18 | <0.001 | 1.08 | 0.99, 1.18 | 0.078 |
| ≥3 | 1.13 | 1.08, 1.19 | <0.001 | 1.04 | 0.97, 1.12 | 0.235 |
| TNM stage | ||||||
| Stage 1 | — | — | — | — | ||
| Stage 2 | 1.06 | 1.02, 1.11 | 0.006 | 1.01 | 0.93, 1.05 | 0.755 |
| Stage 3 | 0.62 | 0.59, 0.65 | <0.001 | 0.65 | 0.60, 0.69 | <0.001 |
| Stage 4 | 0.36 | 0.33, 0.38 | <0.001 | 0.47 | 0.42, 0.51 | <0.001 |
| AFP | ||||||
| Negative | — | — | — | — | ||
| Positive | 0.85 | 0.82, 0.89 | <0.001 | 0.90 | 0.84, 0.94 | <0.001 |
| MELD (10‐unit change) | 0.95 | 0.92, 0.97 | <0.001 | 0.99 | 0.97, 1.03 | 0.490 |
| Tumor size (1‐cm change) | 0.73 | 0.69, 0.76 | <0.001 | 0.99 | 0.99, 1.00 | <0.001 |
| Treatment type | ||||||
| Noncurative | — | — | — | — | ||
| Curative | 0.90 | 0.87, 0.93 | <0.001 | 0.82 | 0.77, 0.87 | <0.001 |
Abbreviation: OR, odds ratio.
Impact of Treatment Delay on OS
As expected, no treatment was associated with worse OS in univariable (adjusted hazard ratio [aHR], 3.38; 95% confidence interval [CI], 3.32‐3.44) and multivariable (aHR, 2.71; 95% CI, 2.62‐2.80) analysis. With a landmark of 150 days, patients with therapeutic delay had similar OS compared to those without delay in HCC therapy, with median survival of 33.7 months versus 32.1 months, respectively (Fig. 2). Patients with HCC treatment delay had similar OS compared to those without delay in univariable and multivariable analysis, with a landmark date of 150 after HCC diagnosis (Table 4). Results were consistent in sensitivity analyses using different landmarks of 120 and 180 days (Fig. 2).
FIG. 2.
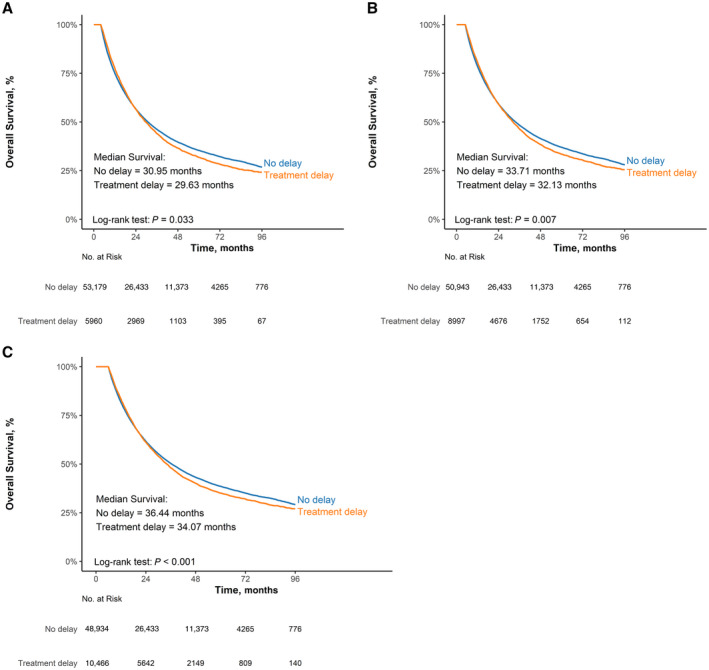
Kaplan‐Meier curve showing estimated OS in patients with no delay versus delay in treatment (landmark analysis). (A) 120 days landmark, (B) 150 days landmark, and (C) 180 days landmark. Overall median survivals are comparable between the two groups, although there is a statistically significant difference in median survival due to the large sample size.
Table 4.
Association between HCC treatment delay and OS among patients who received HCC treatment
| Characteristic | Univariate | Multivariable* | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | P Value | HR | 95% CI | P Value | |
| Landmark at 120 days | 1.04 | 1.00, 1.07 | 0.033 | 1.01 | 0.98, 1.05 | 0.522 |
| Landmark at 150 days | 1.04 | 1.01, 1.07 | 0.007 | 1.01 | 0.98, 1.04 | 0.399 |
| Landmark at 180 days | 1.05 | 1.02, 1.08 | <0.001 | 1.03 | 1.00, 1.06 | 0.078 |
Adjusted by demographic, socioeconomic, center, regions, and clinical characteristic variables included in Table 3.
Subgroup analysis showed lack of association between HCC treatment delay and OS for most subgroups stratified by demography, SES, severity of liver dysfunction (MELD), and treating facility type. However, there was a significant interaction between tumor stage, curative treatment, and treatment delay in predicting OS (all P < 0.001). Therapeutic delay was associated with worse OS in patients with an earlier stage of HCC reflected by TNM stage 1 (aHR, 1.06; 95% CI, 1.01‐1.11), tumor size <4 cm (aHR, 1.06; 95% CI, 1.02‐1.11), or receipt of curative treatment (aHR, 1.12; 95% CI, 1.05‐1.18). When curative treatment was further stratified, the association between treatment delay and OS was similar among those who underwent ablation (aHR, 1.05; 95% CI, 0.97‐1.13), resection (aHR, 1.12; 95% CI, 0.99‐1.12), or liver transplantation (aHR, 1.11; 95% CI, 0.95‐1.31). However, HCC treatment delay had no association with OS in patients with TNM stage 2 (aHR, 1.03; 95% CI, 0.97‐1.09), stage 3 (aHR, 0.95; 95% CI, 0.89‐1.01), stage 4 (aHR, 0.95; 95% CI, 0.87‐1.05), tumor size ≥4 cm (aHR, 0.98; 95% CI, 0.94‐1.02), or noncurative treatment receipt (aHR, 0.98; 95% CI, 0.95‐1.02).
Discussion
Our study investigated the nationwide prevalence, correlates, and clinical significance of no receipt or delay in HCC treatment. About one quarter of patients did not receive HCC treatment, although the proportion of patients without treatment decreased over time. Among treated patients, therapy was delayed in 18% of patients. In light of the transition from diagnosis to treatment being a complex and multistep process, particularly in early stage patients with HCC, we found multiple factors at different levels were associated with no and delayed treatment. Finally, we found delay in treatment was not associated with shorter OS in landmark analyses, although it showed a mild association with worse OS in patients who had earlier stage HCC and received curative treatment.
Underuse of cancer treatment has been reported for several other cancers in the United States, with this issue being more prevalent for low‐grade non‐Hodgkin lymphoma and less prevalent for germ cell, renal, and colorectal cancers.( 28 , 29 ) There have been older smaller studies evaluating this question in patients with HCC. A meta‐analysis of 24 studies from January 1989 to March 2013 showed 47% of patients with HCC had not received any HCC treatment.( 30 ) Subsequent retrospective cohort studies from an urban safety‐net hospital and the Department of Veterans Affairs both reported approximately one‐third of patients with HCC failed to receive cancer treatment.( 9 , 30 , 31 ) In our study, we found this to be true in a smaller proportion of patients, consistent with observed trends, suggesting increased treatment use over time. The improved treatment use may reflect increasing treatment options with higher efficacy, particularly for those with advanced‐stage HCC. Despite this encouraging trend, treatment use remains far lower than other cancers, which might be attributed to 1) higher HCC burden in racial/ethnic minorities who have limited access to medical care, 2) increased medical comorbidities, particularly underlying cirrhosis and hepatic dysfunction precluding cancer treatment, and 3) lower familiarity of providers with HCC treatment algorithms. Indeed, we found Hispanics and Blacks and patients with higher MELD scores were less likely to receive HCC treatment. This is consistent with a recent Surveillance, Epidemiology and End Results registry analysis that showed racial disparities in HCC treatment use among Hispanics and Blacks.( 32 ) Racial/ethnic disparities in the receipt of cancer treatment are well known in multiple other solid organ cancers, with a negative impact on the health outcomes in racial/ethnic minorities.( 33 ) This disparity in treatment are often due to nonclinical factors, and developing strategies to facilitate appropriate cancer care for racial/ethnic minorities may provide an essential means of reducing disparities in cancer treatment.( 33 ) In addition to race/ethnicity, prior studies in other solid organ cancers investigated socioeconomic variations in cancer treatment and patient outcome.( 34 , 35 ) Our results also highlight the impact of socioeconomic status on HCC treatment receipt, which might stem from variation in access to care (primary care, ambulatory care visits, subspecialist referrals) and quality of cancer treatment.
Clinical characteristics of patients, medical facility type, and geographic region were associated with treatment delay in HCC. Unexpectedly, we found that patient care at academic centers was associated with an increased likelihood of having treatment delays. This finding may be related to time for initial referral and consultation, particularly for patients who live remotely; involvement of multidisciplinary teams and subspecialties; and access to advanced multimodal treatment options, including liver transplantation at academic centers compared to community hospitals.( 21 , 30 ) We also observed that clinical factors, such as larger tumor size, elevated AFP, and advanced tumor stages were less likely to experience treatment delays. This could be explained by the “triage effect” where aggressive tumors with inherently worse prognosis were prioritized for treatment while treatment of less severe tumors were reasonably delayed. Our speculation of “case prioritization” is supported by similar investigations in lung,( 36 , 37 ) colon,( 38 ) and endometrial cancers,( 39 ) where patients with advanced cancer with higher symptom burden received prompt treatment compared to less aggressive tumors. Moreover, treatment decision for advanced HCC is relatively straightforward with primarily systemic therapy, whereas there are various curative treatment options for early stage HCC (e.g., ablation, resection, transplant), selection of which is dependent on several factors, including the severity of liver dysfunction, SES, and the location of tumor, contributing to the delay.( 3 )
Although it is evident that HCC treatment delays are prevalent, available data on their impact on survival outcomes are conflicting.( 21 , 22 , 23 , 40 , 41 , 42 , 43 , 44 , 45 , 46 ) Most earlier studies concluded that delay in treatment was associated with poorer survival.( 21 , 22 , 40 , 41 , 42 , 44 ) However, more recent studies showed no significant impact of treatment delay on survival.( 23 , 43 , 45 , 46 ) Our landmark analysis, which accounts for immortal bias from delayed treatment, suggests that treatment delay was not associated with patient survival. This finding was consistently observed when the analysis was repeated at different landmark points (120, 150, and 180 days). However, our subgroup analysis showed that treatment delay was associated with worse OS in patients who had earlier stage HCC and received curative treatment. HCC is typically regarded as an aggressive tumor with short tumor‐doubling times, and recent data suggest that about 35% of HCCs have tumor‐volume doubling time <3 months.( 11 , 25 ) Further, tumor‐doubling times are typically shorter among smaller tumors, suggesting that delays at an early stage might be particularly problematic. Tumor growth among these patients may increase the risk of microvascular invasion and decrease the likelihood of complete response to curative treatment.
The results of our study need to be interpreted in the context of its limitations. First, as it is a retrospective analysis, it cannot determine causation; thus, we are only able to report associations between variables, particularly between therapeutic delay and OS. Second, even though the database contains comprehensive cancer‐specific information, we were unable to adjust certain important clinical factors, including liver disease etiology and presence of cirrhosis, presence of hepatic encephalopathy or ascites, number of HCC nodules, and Barcelona Clinic Liver Cancer staging. Alternatively, we used tumor size and TNM staging as measures of tumor burden and MELD score as a measure of liver dysfunction. Third, the database lacked information on how patient and provider preference, hospital resources, and other factors may affect treatment decisions. Fourth, NCBD does not have data on referrals to a tertiary center for cancer management, which could have led to treatment delay, especially in patients who received care at academic cancer programs. However, any treatment delay from referral would need to be considered in light of high‐volume clinical expertise; availability of specialty services, such as liver transplantation; and multidisciplinary care, all of which have been associated with improved clinical outcomes among patients with HCC.( 47 , 48 ) The NCDB does not capture a detailed longitudinal course of HCC treatment, and so we were unable to examine if receipt of a specific type of noncurative treatment before curative treatment would affect treatment delay or OS. Finally, many covariates were associated with outcomes despite small effect size due to large sample size; therefore, some associations reported in this study might not be clinically relevant. We feel these limitations are outweighed by the strengths of this study. This is the largest cohort study evaluating treatment receipt and delays in a contemporary cohort encompassing a broad range of all patients with HCC, with diversity across age, race/ethnicity, tumor stage, and treatment type.
In conclusion, no treatment and delayed HCC treatment are widely prevalent in the United States. There were racial/ethnic and socioeconomic disparities in HCC treatment underuse and delay. The association between therapeutic delay and OS appears to be stage and treatment dependent, with worse survival noted among patients with early stage HCC or curative treatment receipt who experienced therapeutic delays. Future studies are warranted to further characterize the underlying cause of health care disparities in HCC treatment receipt and therapeutic delays.
Supporting information
Supplementary Material
Supported by the American College of Gastroenterology (Junior Faculty Development Award), United States Department of Defense (CA191051), Cedars‐Sinai Medical Center (Clinical Scholar award), Huiying Foundation, and National Institutes of Health (R01 MD12565 and U01 CA230694).
The American College of Gastroenterology, United States Department of Defense, Cedars‐Sinai Medical Center, Huiying Foundation, and National Institutes of Health had no role in the collection of data; the design and conduct of the study; management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Potential conflict of interest: Dr. Singal consults for Genentech, Bayer, Eisai, Exelixis, AstraZeneca, and TARGET RWE. Dr. Roberts consults for AstraZeneca, MJH Life Sciences, and Clinical care options; he advises and received grants from Bayer, Exact Sciences, and Gilead; he advises GRAIL, Tavec, QED Therapeutics, Genentech, Envision, and Eisai and received grants from Ariad, BTG International, GylcoTest, RedHill, Ltd Pharma, and Wako Diagnostics. Dr. Yang provides a consulting service for Exact Sciences, Gilead Sciences, and Eisai. The other authors have nothing to report.
References
- 1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394‐424. Erratum in: CA Cancer J Clin 2020;70:313. [DOI] [PubMed] [Google Scholar]
- 2. Yang JD, Hainaut P, Gores GJ, Amadou A, Plymoth A, Roberts LR. A global view of hepatocellular carcinoma: trends, risk, prevention and management. Nat Rev Gastroenterol Hepatol 2019;16:589‐604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Bruix J, Sherman M; American Association for the Study of Liver Diseases . Management of hepatocellular carcinoma: an update. Hepatology 2011;53:1020‐1022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Singal AG, Marrero JA. Recent advances in the treatment of hepatocellular carcinoma. Curr Opin Gastroenterol 2010;26:189‐195. [DOI] [PubMed] [Google Scholar]
- 5. Singal AG, Pillai A, Tiro J. Early detection, curative treatment, and survival rates for hepatocellular carcinoma surveillance in patients with cirrhosis: a meta‐analysis. PLoS Med 2014;11:e1001624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Marrero JA, Kulik LM, Sirlin CB, Zhu AX, Finn RS, Abecassis MM, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018;68:723‐750. [DOI] [PubMed] [Google Scholar]
- 7. Wolf E, Rich NE, Marrero JA, Parikh ND, Singal AG. Use of hepatocellular carcinoma surveillance in patients with cirrhosis: a systematic review and meta‐analysis. Hepatology 2021;73:713‐725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Singal AG, Lok AS, Feng Z, Kanwal F, Parikh ND. Conceptual model for the hepatocellular carcinoma screening continuum: current status and research agenda. Clin Gastroenterol Hepatol 2020; 10.1016/j.cgh.2020.09.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Rao A, Rich NE, Marrero JA, Yopp AC, Singal AG. Diagnostic and therapeutic delays in patients with hepatocellular carcinoma. J Natl Compr Canc Netw 2021. May 28:1‐14. [DOI] [PubMed] [Google Scholar]
- 10. Kim AK, Singal AG. Health disparities in diagnosis and treatment of hepatocellular carcinoma. Clin Liver Dis (Hoboken) 2015;4:143‐145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Rich NE, John BV, Parikh ND, Rowe I, Mehta N, Khatri G, et al. Hepatocellular carcinoma demonstrates heterogeneous growth patterns in a multicenter cohort of patients with cirrhosis. Hepatology 2020;72:1654‐1665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Tørring ML, Frydenberg M, Hansen RP, Olesen F, Vedsted P. Evidence of increasing mortality with longer diagnostic intervals for five common cancers: a cohort study in primary care. Eur J Cancer 2013;49:2187‐2198. [DOI] [PubMed] [Google Scholar]
- 13. Richards MA, Westcombe AM, Love SB, Littlejohns P, Ramirez AJ. Influence of delay on survival in patients with breast cancer: a systematic review. Lancet 1999;353:1119‐1126. [DOI] [PubMed] [Google Scholar]
- 14. Bleicher RJ. Timing and delays in breast cancer evaluation and treatment. Ann Surg Oncol 2018;25:2829‐2838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Ramos M, Esteva M, Cabeza E, Llobera J, Ruiz A. Lack of association between diagnostic and therapeutic delay and stage of colorectal cancer. Eur J Cancer 2008;44:510‐521. [DOI] [PubMed] [Google Scholar]
- 16. Fisher DA, Zullig LL, Grambow SC, Abbott DH, Sandler RS, Fletcher RH, et al. Determinants of medical system delay in the diagnosis of colorectal cancer within the Veteran Affairs Health System. Dig Dis Sci 2010;55:1434‐1441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Jazieh AR, Chan SL, Curigliano G, Dickson N, Eaton V, Garcia‐Foncillas J, et al. Delivering cancer care during the COVID‐19 pandemic: recommendations and lessons learned from ASCO global webinars. JCO Glob Oncol 2020;6:1461‐1471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Fix OK, Hameed B, Fontana RJ, Kwok RM, McGuire BM, Mulligan DC, et al. Clinical best practice advice for hepatology and liver transplant providers during the COVID‐19 pandemic: AASLD expert panel consensus statement. Hepatology 2020;72:287‐304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Network ACSCA . COVID‐19 Pandemic Early Effects on Cancer Patients and Survivors: April 2020. American Cancer Society; 2020. [Google Scholar]
- 20. Muñoz‐Martínez S, Sapena V, Forner A, Nault J‐C, Sapisochin G, Rimassa L, et al. Assessing the impact of COVID‐19 on liver cancer management (CERO‐19). JHEP Rep 2021;3:100260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Singal AG, Waljee AK, Patel N, Chen EY, Tiro JA, Marrero JA, et al. Therapeutic delays lead to worse survival among patients with hepatocellular carcinoma. J Natl Compr Canc Netw 2013;11:1101‐1108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Chen WT, Fernandes ML, Lin CC, Lin SM. Delay in treatment of early‐stage hepatocellular carcinoma using radiofrequency ablation may impact survival of cirrhotic patients in a surveillance program. J Surg Oncol 2011;103:133‐139. [DOI] [PubMed] [Google Scholar]
- 23. Lim C, Bhangui P, Salloum C, Gómez‐Gavara C, Lahat E, Luciani A, et al. Impact of time to surgery in the outcome of patients with liver resection for BCLC 0‐A stage hepatocellular carcinoma. J Hepatol 2017; 10.1016/j.jhep.2017.09.017. [DOI] [PubMed] [Google Scholar]
- 24. American College of Surgeons National cancer database. https://www.facs.org/quality‐programs/cancer/ncdb. Published 2021. Accessed February 2021.
- 25. Nathani P, Gopal P, Rich N, Yopp A, Yokoo T, John B, et al. Hepatocellular carcinoma tumour volume doubling time: a systematic review and meta‐analysis. Gut 2021;70:401‐407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. White IR, Royston P, Wood AM. Multiple imputation using chained equations: Issues and guidance for practice. Stat Med 2011;30:377‐399. [DOI] [PubMed] [Google Scholar]
- 27. Farr AM, Foley K. Landmark analysis to adjust for immortal time bias in oncology studies using claims data linked to death data. Value Health 2013;16:A50. [Google Scholar]
- 28. Ward MM, Ullrich F, Matthews K, Rushton G, Goldstein MA, Bajorin DF, et al. Who does not receive treatment for cancer? J Oncol Pract 2013;9:20‐26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Miller KD, Nogueira L, Mariotto AB, Rowland JH, Yabroff KR, Alfano CM, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin 2019;69:363‐385. [DOI] [PubMed] [Google Scholar]
- 30. Tan D, Yopp A, Beg MS, Gopal P, Singal AG. Meta‐analysis: underutilisation and disparities of treatment among patients with hepatocellular carcinoma in the United States. Aliment Pharmacol Ther 2013;38:703‐712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Khalaf N, Ying J, Mittal S, Temple S, Kanwal F, Davila J, et al. Natural history of untreated hepatocellular carcinoma in a US cohort and the role of cancer surveillance. Clin Gastroenterol Hepatol 2017;15:273‐281.e271. [DOI] [PubMed] [Google Scholar]
- 32. Franco RA, Fan Y, Jarosek S, Bae S, Galbraith J. Racial and geographic disparities in hepatocellular carcinoma outcomes. Am J Prev Med 2018;55(Suppl. 1):S40‐S48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Shavers VL, Brown ML. Racial and ethnic disparities in the receipt of cancer treatment. J Natl Cancer Inst 2002;94:334‐357. [DOI] [PubMed] [Google Scholar]
- 34. Lam MB, Phelan J, Orav EJ, Jha AK, Keating NL. Medicaid expansion and mortality among patients with breast, lung, and colorectal cancer. JAMA Netw Open 2020;3:e2024366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Sommers BD, Gawande AA, Baicker K. Health insurance coverage and health ‐ what the recent evidence tells us. N Engl J Med 2017;377:586‐593. [DOI] [PubMed] [Google Scholar]
- 36. Diaconescu R, Lafond C, Whittom R. Treatment delays in non‐small cell lung cancer and their prognostic implications. J Thorac Oncol 2011;6:1254‐1259. [DOI] [PubMed] [Google Scholar]
- 37. González‐Barcala FJ, García‐Prim JM, Alvarez‐Dobaño JM, Moldes‐Rodríguez M, García‐Sanz MT, Pose‐Reino A, et al. Effect of delays on survival in patients with lung cancer. Clin Transl Oncol 2010;12:836‐842. [DOI] [PubMed] [Google Scholar]
- 38. Amri R, Bordeianou LG, Sylla P, Berger DL. Treatment delay in surgically‐treated colon cancer: does it affect outcomes? Ann Surg Oncol 2014;21:3909‐3916. [DOI] [PubMed] [Google Scholar]
- 39. Crawford SC, Davis JA, Siddiqui NA, de Caestecker L, Gillis CR, Hole D, et al. The waiting time paradox: population based retrospective study of treatment delay and survival of women with endometrial cancer in Scotland. BMJ 2002;325:196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Huo TI, Huang YH, Chiang JH, Wu JC, Lee PC, Chi CW, et al. Survival impact of delayed treatment in patients with hepatocellular carcinoma undergoing locoregional therapy: is there a lead‐time bias? Scand J Gastroenterol 2007;42:485‐492. [DOI] [PubMed] [Google Scholar]
- 41. Croome KP, Chudzinski R, Hanto DW. Increasing time delay from presentation until surgical referral for hepatobiliary malignancies. HPB (Oxford) 2010;12:644‐648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Brahmania M, Ahmed O, Kelley M, Kowgier M, Khalili K, Beecroft R, et al. Wait time for curative intent radio frequency ablation is associated with increased mortality in patients with early stage hepatocellular carcinoma. Ann Hepatol 2017;16:765‐771. [DOI] [PubMed] [Google Scholar]
- 43. Akce M, Sansgiry S, Temple SL, Davila J, Sada Y. The effect of treatment delay on survival in patients with hepatocellular cancer. J Clin Oncol 2017;35(Suppl.):e15645. [Google Scholar]
- 44. Tsai WC, Kung PT, Wang YH, Kuo WY, Li YH. Influence of the time interval from diagnosis to treatment on survival for early‐stage liver cancer. PLoS One 2018;13:e0199532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Xu K, Watanabe‐Galloway S, Rochling FA, Farazi PA, Monirul Islam KM, Wang H, et al. Surgical delay is associated with improved survival in hepatocellular carcinoma: results of the National Cancer Database. J Gastrointest Surg 2019;23:933‐943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Kabir T, Syn N, Ramkumar M, Yeo EYJ, Teo JY, Koh YX, et al. Effect of surgical delay on survival outcomes in patients undergoing curative resection for primary hepatocellular carcinoma: Inverse probability of treatment weighting using propensity scores and propensity score adjustment. Surgery 2020;167:417‐424. [DOI] [PubMed] [Google Scholar]
- 47. Yopp AC, Mansour JC, Beg MS, Arenas J, Trimmer C, Reddick M, et al. Establishment of a multidisciplinary hepatocellular carcinoma clinic is associated with improved clinical outcome. Ann Surg Oncol 2014;21:1287‐1295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Mokdad AA, Zhu H, Marrero JA, Mansour JC, Singal AG, Yopp AC. Hospital volume and survival after hepatocellular carcinoma diagnosis. Am J Gastroenterol 2016;111:967‐975. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material