

Abstract
We sought to analyze all high-quality studies available regarding the possible differences in contained and uncontained techniques for morcellation of fibroids and uteri. We systematically searched PubMed, Cochrane Central, Scopus, ClinicalTrials.Gov, MEDLINE and Web of Science from September 2010 to September 2020 for our search terms. We included studies that specifically enrolled patients undergoing power morcellation myomectomy or power morcellation hysterectomy procedures. In our search, we had no restriction to age, country, or publication date.
We extracted data related to study design, baseline characteristics of patients, and perioperative outcomes such as total operative time, total blood loss, and duration of hospital stay. We found no substantial difference in total operative time between contained power morcellation and uncontained manual morcellation myomectomy (p=0.52), but contained power morcellation had a significantly longer total operative time than uncontained power morcellation for hysterectomy and myomectomy [135.50 vs. 93.33 minutes, (p=0.003)]. Total blood loss was comparable for contained power morcellation versus uncontained manual morcellation myomectomy (p=0.32) and contained power morcellation versus uncontained power morcellation myomectomy or hysterectomy (p=0.91). Contained power morcellation and uncontained manual morcellation myomectomy had comparable hospital stay periods (p=0.5). Contained power morcellation leads to a longer operating time than uncontained power morcellation for both hysterectomy and myomectomy. No differences were found in comparisons of blood loss, operative time, or comparison to manual methods of morcellation.
Keywords: Power morcellation, manual morcellation, myomectomy, meta-analysis
Introduction
Uterine fibroids or myomas are some of the most common benign tumors of premenopausal women(1). Patients may present with pain, abnormal uterine bleeding, pressure symptoms, or infertility(2,3). The traditional approach to treat large uterine myomas involved abdominal myomectomy or hysterectomy. With the advent of minimally invasive laparoscopic techniques, there is a need for analysis of the different techniques for performing laparoscopic hysterectomy and myomectomy in the presence of large fibroids requiring some form of morcellation for removal(4). Some studies have shown that laparoscopic myomectomy, versus open myomectomy, may have higher success rates and fewer complications when performed on appropriately selected patients(5). Further described advantages of laparoscopic myomectomy include less postoperative pain, faster recovery time, shorter hospital stay, and higher probability of maintaining reproductive function(6).
In an attempt to solve the problems of specimen removal in laparoscopy, several techniques have been developed to break apart these tissues in order to deliver them through the small incisions that characterize laparoscopy, also known as morcellation. As a result, various techniques, such as laparoscopic power morcellation and manual morcellation have been developed for laparoscopic, vaginal, or mini-laparotomy (ML) use. These procedures can be performed with or without a specially designed bag to contain the shredded pieces which may result(7). In unexpected malignancies, power morcellation can lead to the unintended spread of malignant cells. This has become of particular interest in recent years, as the contained power morcellation of unexpected leiomyosarcoma can result in spreading of the leiomyosarcoma and worsening of the patient’s prognosis. This culminated in an Food and Drug Administration (FDA)-issued statement discouraging the use of power morcellation for myomectomy or hysterectomy in 2014, but this statement was later updated to allow the their usage only in a contained environment(8). The FDA decision may have been a factor in pushing manufacturers of power morcellation devices to develop containment systems for avoiding cell spillage and unintentional implantation of malignant cells(9,10).
Prior to these events, contained laparoscopies in gynecology were mainly performed in ovarian cystectomy or oophorectomy to reduce the risk of dissemination of undetected malignant cells(11). Currently, many studies have investigated the different outcomes of in-bag manual or power uterine morcellation and assessed new techniques to address the general drawbacks of morcellation(12,13,14).
In this analysis, we aimed at evaluating the contained power morcellation technique and compare its perioperative outcomes with the uncontained power and manual morcellation procedures. Unfortunately, at this time, there is insufficient follow-up data to support the aim of this study, including the discovery of future occult malignancy outcomes. Therefore, our aim at this time is limited to the analysis of the perioperative outcomes of these procedures. Moreover, we were unable to consider the effects of differences in morcellation techniques, closure methods, or the effects of administered intraoperative medications, such as vasopressin.
Materials and Methods
We conducted and drafted this study according to the steps described in “Cochrane handbook for systematic reviews of interventions” and the “Preferred reporting items for systematic reviews and meta-analyses (PRISMA)” guidelines(15,16).
Search Strategy and Data Collection
We searched the following electronic databases: PubMed, Cochrane Central, Web of Science, ClinicalTrials.Gov, MEDLINE and Scopus for all published studies up to September 1, 2020, published within the last 10 years (from September 1, 2011). We conducted our search using the following key terms: “Laparoscopy,” “Celioscopy,” “Peritoneoscopy,” “Morcellation,” “Fibroidectomy,” “Myomectomy,” and “Uterine Myomectomy.”
After removing duplicates using Endnote software, we screened all remaining citations for eligibility through two steps: First, screening the titles and abstracts and second, screening the full texts. We then included the studies matching our selection criteria. Moreover, we manually screened the references of the included studies for other related papers.
Selection Criteria
We included all studies that enrolled patients specifically undergoing power morcellation myomectomy or power morcellation hysterectomy. In our search, we had no restriction to age, country, or publication date. We excluded non-English studies, non-available studies, thesis, reviews, and individual case reports. We did not further sort included studies by selected techniques, closure methods, or intraoperative medications administered. All techniques of power morcellation or manual morcellation were assumed to be performed to the best of the ability of the surgeon, and other differences of technique, (with the exception of power vs. manual morcellation), were ignored.
Data Extraction
The following data was extracted:
1. Summary of the included studies and their elements such as study design, study arms, duration, number of patients, and conclusion.
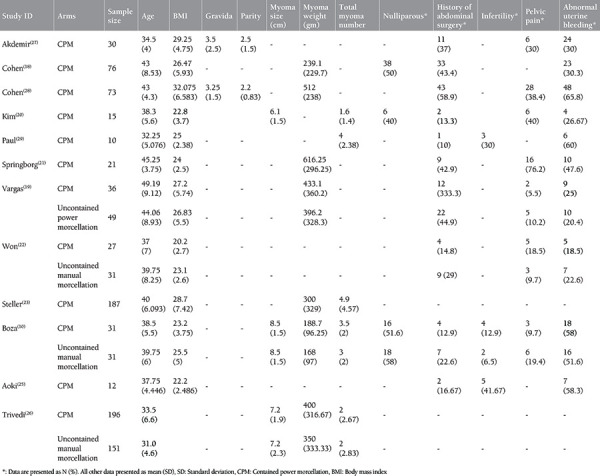
2. Baseline characteristics of the enrolled patients including age, body mass index (BMI), gravidity and parity, number of nulliparous participants, history of abdominal surgeries, myoma characteristics, and myoma symptoms of pain, infertility, or abnormal uterine bleeding.
3. Perioperative outcomes including total operative time (defined as initial incision to skin closure), morcellation preparation time (defined as any time delegated by the surgeon to prepare in order to perform morcellation), total morcellation time (defined as the total time declared by the surgeon as needed to perform the morcellation portion of the procedure), total blood loss, and duration of hospital stay.
4. Data required to complete our quality assessment (assessment of bias).
Quality Assessment
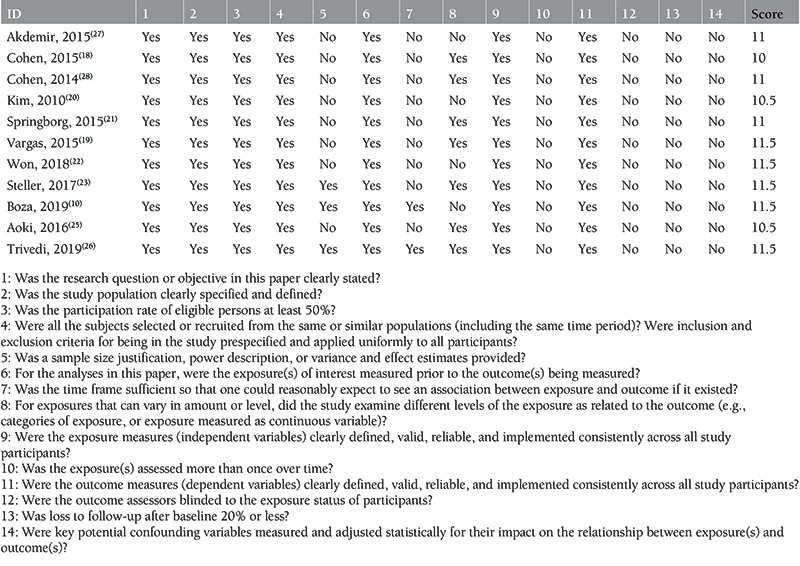
We assessed the quality of the included studies using the National Institute of Health (NIH) quality assessment tools(17). The tool for observational cohort studies composed of 14 questions to assess the risk of bias and confounders, while the tool for case series composed of 9 assessment questions. Assessment questions included the judgment of the clarity of the study question, the definition of the study population, the participation rate, the specification of the study inclusion and exclusion criteria, the sample size justification, the outcome measurement process, the sufficiency of timeframe and follow-up period, the precise definition and validity of the exposure and outcome measures, multiple measurements of the exposure, blinding of the outcome assessor, the loss of follow-up rate, and the potential confounding variables. These questions were answered by “yes,” “no,” “not applicable,” “cannot determine,” or “not reported.” Then, each study was attributed a score to judge the overall quality as either “good,” “fair,” or “poor.”
Data Synthesis and Analysis
Statistical analyses were performed using the RevMan version 5.4 software. Continuous outcomes were analyzed as mean difference (MD) and standard error. Pooled results were reported as MD and 95% confidence interval (CI) using the generic inverse-variance method under the random-effects model. We used I-squared and chi-squared statistics to assess heterogeneity among the studies. Indications of heterogeneity included I2 values of ≥50% with chi-square p-values <0.10. In the case of heterogeneity, we resolved by performing a sensitivity analysis using the “leave-one-out” test. Some studies reported the results of myomectomy and hysterectomy patients as a single group, so the data from these studies were pooled and reported in a separate analysis.
Results
Literature Search and Characteristics of the Included Trials
Our search obtained 525 studies (232 from PubMed, 184 from Scopus, 100 from WOS, and 9 from Cochrane). After removing 49 duplicates and 452 citations by title and abstract screening, there were 24 papers that entered full-text screening and were further refined according to our criteria to eventually reach 12 articles (Figure 1)(10,18,19,20,21,22,23,24,25,26,27,28). We ultimately included one case series and 11 cohort studies with 976 patients total. Among these, 714 patients underwent contained power morcellation, 213 underwent uncontained manual morcellation, and 49 underwent uncontained power morcellation. The mean age of the patients ranged from 31 to 49 years, and the mean BMI ranged from 22.2 to 32.1 across studies. A mean of 10% to 59% of patients among the studies had previous abdominal surgery and 18.5% to 65% of then had abnormal uterine bleeding. Summary of the included studies and baseline characteristics of the enrolled patients are found in Tables 1 and 2 respectively.
Figure 1.
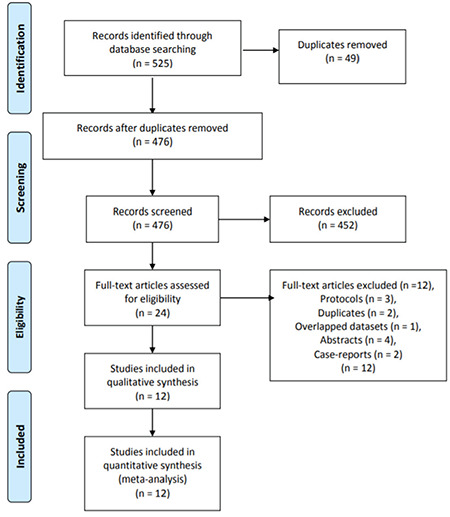
The PRISMA flow chart summarizing the literature search and including studies from each database
PRISMA: Preferred reporting items for systematic reviews and meta-analyses
Table 1. Summary of the included studies.
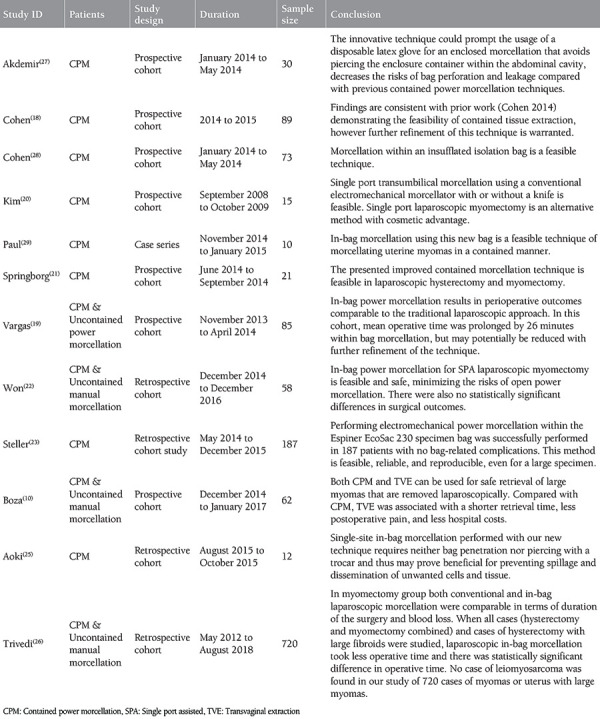
Table 2. Baseline characteristics of the included studies.
Results of Quality Assessment
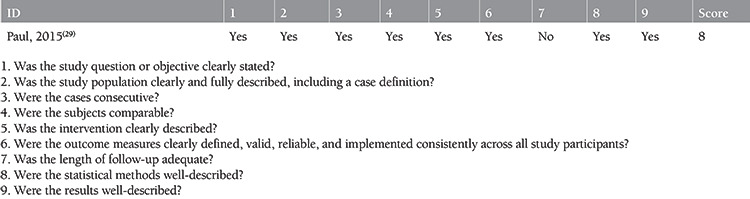
According to the NIH quality assessment tool for observational cohort studies, all 11 included cohort studies were of fair quality(10,18,19,20,21,22,23,25,26,27,28). According to the NIH quality assessment tool for case series, the included case series was of good quality(29). For more details on all assessment questions of each study, refer to Supplementary Table S1 for cohort studies and Supplementary Table S2 for the case series study.
Supplementary Table 1. Risk of bias assessment of the included cohort studies.
Supplementary Table 2. Risk of bias assessment of the included case series study.
Study Outcomes
1. Total Operative Time (Min.)
1.1 Myomectomy-only data
Six studies(10,22,26,27,29,30) with analyzable data reported this outcome, with a total of 522 myomectomy patients; 309 patients underwent contained power morcellation, and 213 patients underwent uncontained manual morcellation. The pooled data showed an increase in total operative time in the contained power morcellation group [MD=116.66, 95% CI (102.38, 130.93)] compared to the uncontained manual morcellation group [MD=104.81, 95% CI (71.23, 138.40)]. There was no substantial differences in operative time between the two groups (p=0.52) (Figure 2).
Figure 2.
Forest plot of the total operative time (min.) comparison between contained power morcellation versus uncontained manual morcellation myomectomy
CI: Confidence interval
The pooled results for both contained power morcellation (p<0.00001, I2=90%) and uncontained manual morcellation (p<0.00001, I2=97%) were heterogeneous, and could not be resolved.
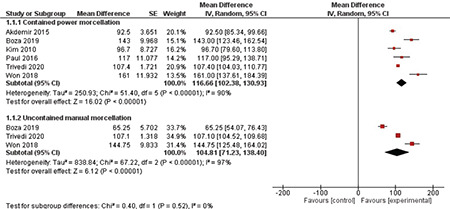
1.2 Hysterectomy and myomectomy data
Five studies(18,19,21,25,28) with analyzable data reported this outcome, with a total of 485 myomectomy or hysterectomy patients; 436 patients underwent contained power morcellation, and 49 patients underwent uncontained power morcellation. The pooled data showed an increase in total operative time for contained power morcellation [MD=135.50, 95% CI (110.23, 160.76)], over the uncontained power morcellation groups [MD=93.33, 95% CI (80.76, 105.90)]. The test for subgroup difference confirmed a statistically shorter operation time with the uncontained power morcellation (p=0.003) (Figure 3). The contained power morcellation subgroup was heterogeneous (p<0.00001, I2=92%), could not be solved and was not applicable to the other subgroup since it represented a single study arm.
Figure 3.
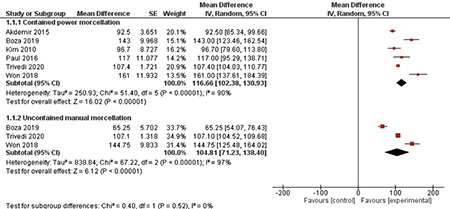
Forest plot of the total operative time (min.) comparison between contained power morcellation versus uncontained power morcellation myomectomy or hysterectomy
CI: Confidence interval
2. Morcellation Preparation Time (Min.)
2.1 Myomectomy-only data
Two studies(27,29) with analyzable data reported this outcome, with a total of 40 myomectomy patients all undergoing contained power morcellation. The results showed an average morcellation preparation time of 9.89 minutes [95% CI (5.12, 14.65)] (Supplementary Figure S1). Pooled data were heterogeneous (p<0.0008, I2=91%), and could not be resolved.
Suplemental Figure 1.
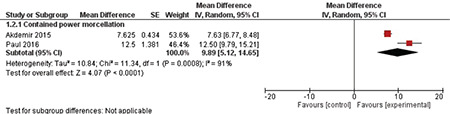
Forest plot of the morcellation preparation time (min.) for contained power morcellation myomectomy
CI: Confidence interval
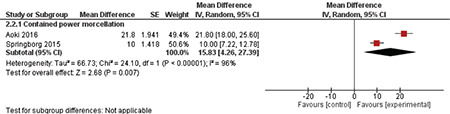
2.2 Hysterectomy and myomectomy data
Two studies(21,25) with analyzable data reported this outcome, with 51 myomectomy or hysterectomy patients all undergoing contained power morcellation surgery. The results showed an average morcellation preparation time of 15.83 minutes [95% CI (4.26, 27.39)] (Supplementary Figure S2). Pooled data were heterogeneous (p<0.00001, I2=96%), and we could not solve the heterogeneity.
Suplemental Figure 2.
Forest plot of the morcellation preparation time (min.) for contained power morcellation hysterectomy or myomectomy
CI: Confidence interval
3. Total Morcellation Time (Min.)
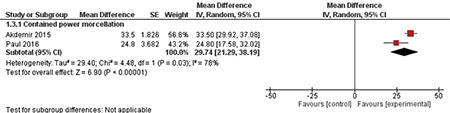
3.1 Myomectomy-only data
Two studies(27,29) with analyzable data reported this outcome, with 40 myomectomy patients who underwent contained power morcellation. The results showed an average morcellation time of 29.74 minutes, [95% CI (21.29, 38.19)] (Supplementary Figure S3). The data were heterogeneous (p<0.03, I2=78%), and we could not solve the heterogeneity.
Suplemental Figure 3.
Forest plot of the total morcellation time (min.) for contained power morcellation myomectomy
CI: Confidence interval
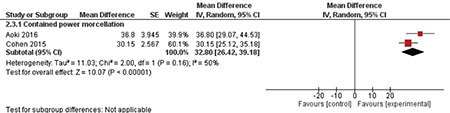
3.2 Hysterectomy and myomectomy data
Two studies(18,25) with analyzable data reported this outcome, with 119 myomectomy or hysterectomy patients who underwent contained power morcellation. The results showed an average morcellation time of 32.80 minutes, [95% CI (26.42, 39.18)] (Supplementary Figure S4). Pooled data were homogenous (p<0.16, I2=50%).
Suplemental Figure 4.
Forest plot of the total morcellation time (min.) for contained power morcellation hysterectomy or myomectomy
4. Total Blood Loss (mL)
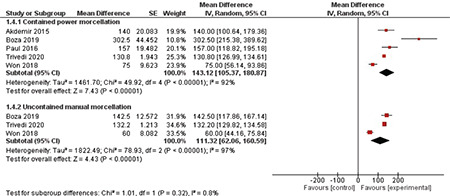
4.1 Myomectomy-only data
Five studies(10,22,26,27,29) with analyzable data reported this outcome, with 507 myomectomy patients; 294 patients underwent contained power morcellation, and 213 patients underwent uncontained manual morcellation. The pooled data showed an increase in total blood loss in the contained power morcellation group [MD=143.12, 95% CI (105.37, 180.87)] compared to the uncontained manual morcellation group [MD=111.32, 95% CI (62.06, 160.59)]. There was no difference in this outcome between the two groups (p=0.32) (Figure 4). Pooled data were heterogeneous for both contained power morcellation (p<0.00001, I2=92%) and uncontained manual morcellation (p<0.00001, I2=97%), and we could not solve the heterogeneity.
Figure 4.
Forest plot of the total blood loss (mL) comparison between contained power morcellation versus uncontained manual morcellation myomectomy
CI: Confidence interval
4.2 Hysterectomy and myomectomy data
Six studies(18,19,21,23,25,28) with analyzable data reported this outcome, with 485 myomectomy or hysterectomy patients; 436 patients underwent contained power morcellation, and 49 patients underwent uncontained power morcellation. The pooled data showed an increase in total blood loss in the contained power morcellation group [MD=119.62, 95% CI (85.28, 153.96)] compared to the uncontained power morcellation group [MD=116.10, 95% CI (62.14, 170.06)]. The test for subgroup difference showed no difference between the two groups (p=0.91) (Figure 5). The data for the contained power morcellation subgroup was heterogeneous (p<0.00001, I2=85%), and we could not solve the heterogeneity, while heterogeneity did not apply to the uncontained power morcellation subgroup because it represented a single study arm.
Figure 5.
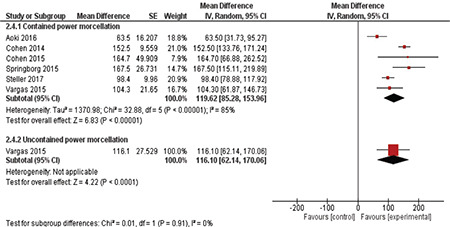
Forest plot of the total blood loss (mL) comparison between contained power morcellation versus uncontained power morcellation myomectomy or hysterectomy
CI: Confidence interval
5. Duration of Hospital Stay (Days)
5.1 Myomectomy-only data
Five studies(10,20,22,27,29) with analyzable data reported this outcome, with 175 myomectomy patients; 113 patients underwent contained power morcellation, and 62 patients underwent uncontained manual morcellation. The pooled data showed an increase in the duration of hospital stay in the contained power morcellation [MD=1.86, 95% CI (1.17, 2.54)] over the uncontained manual morcellation groups [MD=2.10, 95% CI (1.86, 2.35)]. Both groups had comparable hospital stay duration (p=0.5) (Figure 6). Pooled data were heterogeneous for contained power morcellation (p<0.00001, I2=97%) and uncontained manual morcellation (p<0.12, I2=58%), and we could not solve the heterogeneity.
Figure 6.
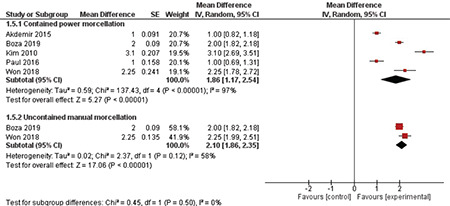
Forest plot of the duration of hospital stay (days) comparison between contained power morcellation versus uncontained manual morcellation myomectomy
CI: Confidence interval
5.2 Hysterectomy and myomectomy data
Two studies(21,28) with analyzable data reported this outcome, with 94 myomectomy or hysterectomy patients who underwent contained power morcellation. Pooled data showed an average hospital stay duration of 0.74 days, [95% CI (0.25, 1.23)] (Figure 7). Pooled data were also heterogeneous (p<0.00001, I2=95%), and this could not be solved.
Figure 7.
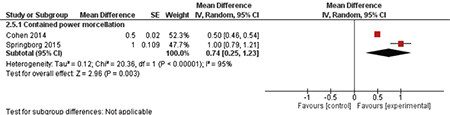
Forest plot of the duration of hospital stay (days) for contained power morcellation myomectomy or hysterectomy
CI: Confidence interval
Discussion
Contained power morcellation and uncontained power morcellation for myomectomy and hysterectomy had similar total blood loss, but uncontained power morcellation had a shorter total operative time for both procedures. Contained power morcellation and uncontained manual morcellation myomectomy had similar total operation time, total blood loss, and hospital stay duration. These findings confirm that contained power morcellation is a feasible procedure, but likely does involve an increase in operation time.
In 1979, Semm(30) reported the first laparoscopic myomectomy (LM), which aimed to minimize complications due to abdominal myomectomy or hysterectomy. Laparoscopy enabled surgeons to remove multiple myomas during one procedure(31,32). Then morcellation emerged to overcome the limitations related to myoma size, making it possible to extract myomas reaching 20 cm or greater laparoscopically(33). Morcellation approaches varied over time and several studies investigated different techniques, including in situ as well as incisional morcellation techniques(34,35,36,37,38).
A retrospective cohort study compared perioperative outcomes associated with electronic power morcellation (PM), manual vaginal morcellation, and manual morcellation via ML in 297 cases, including 137 myomectomies(7). They reported no significant differences between the techniques of the three morcellation methods, but the operative time was longer with the ML. Therefore, the three techniques are considered feasible options for LM.
The FDA statement largely precludes morcellation that is both uncontained and uses a power source, but it does not specifically discourage the use of techniques that exclude one or the other(8). Therefore, there are confounding views as to whether PM should be used with containment or rather simply replaced with a manual method. A recent review concluded that different factors could correlate with sarcoma dissemination and also recommended PM use only in premenopausal women undergoing myomectomy, only after an endometrial biopsy was obtained(39). A meta-analysis of 176 premenopausal women who underwent LM compared intraoperative and postoperative outcomes between in-bag PM and uncontained manual morcellation but no significant difference was found between the methods due to the low-quality evidence used(40). Although PM is often criticized for possible injuries, it is worth mentioning that no intraoperative complications were reported in most of our included studies(21,22,23,25,26,27,29). Also, the advantages of PM regarding cosmetic effect(20) and easier management of large myoma(23) are worth noting. Only two of the included studies reported no intraoperative complications with manual morcellation(22,26). Three intraoperative complications were reported in the included studies for contained(18,19) and uncontained PM myomectomy or hysterectomy(19).
Given that PM is discouraged without a containment system, different techniques are emerging to cope with available resources in low-income countries. For example, Akdemir et al.(27) described the feasibility of using a surgical glove instead of an expensive bag for laparoscopic morcellation in Turkey.
Strengths
Our study is the first meta-analysis to compare contained PM with uncontained manual morcellation. We extracted all analyzable data and included all available observational studies with variations in sample sizes. The Cochrane handbook and PRISMA guidelines were followed throughout this manuscript. According to quality assessment tools, most included studies were of moderate quality.
Study Limitations
These include the observational design of included studies, the high heterogeneity that could not be solved in most outcomes, and the small sample size of some included studies. As a result, we were forced to perform an indirect analysis due to insufficient data for direct comparison. In addition, variations in surgical techniques, which could vary from surgeon to surgeon if not surgery to surgery, could introduce some error into our analysis. This could include the injection of vasoconstricting agents, or differences in tissue closure techniques. This would likely have the largest effect on the surgeon’s operating time.
There is a critical need for more well-designed randomized controlled trials with larger samples and more accurate measurements in order to determine the efficacy and safety of contained PM, in relation to various perioperative and postoperative outcomes. It would be particularly useful if future studies could investigate novel techniques used to practice contained morcellation and manage large myomas, and could include comparisons of intraoperative medications, such as vasopressin, which has the potential to significantly decrease blood loss and operative times.
Conclusion
Contained PM myomectomy has similar total operation time, total blood loss, and hospital stay duration compared with uncontained manual morcellation myomectomy. Also, it has similar total blood loss as uncontained PM for myomectomy or hysterectomy. However, contained PM seems to have a longer total operation time than uncontained PM.
Footnotes
Ethics
Peer-review: Internally peer-reviewed.
Authorship Contributions
Concept: A.K., G.M., A.M., A.C., G.B., K.S., Data Collection or Processing: A.C., G.B., H.U., A.A., S.G., J.P., C.C., Analysis or Interpretation: A.M., Tables: A.C., Figures: A.A., H.U., Supervision: S.R.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study received no financial support.
References
- 1.Agdi M, Tulandi T. Minimally invasive approach for myomectomy. Semin Reprod Med. 2010;28:228–34. doi: 10.1055/s-0030-1251479. [DOI] [PubMed] [Google Scholar]
- 2.Acién P, Quereda F. Abdominal myomectomy: results of a simple operative technique. Fertil Steril. 1996;65:41–51. doi: 10.1016/s0015-0282(16)58025-x. [DOI] [PubMed] [Google Scholar]
- 3.Pritts EA, Parker WH, Olive DL. Fibroids and infertility: an updated systematic review of the evidence. Fertil Steril. 2009;91:1215–23. doi: 10.1016/j.fertnstert.2008.01.051. [DOI] [PubMed] [Google Scholar]
- 4.Stringer NH, Walker JC, Meyer PM. Comparison of 49 laparoscopic myomectomies with 49 open myomectomies. J Am Assoc Gynecol Laparosc. 1997;4:457–64. doi: 10.1016/s1074-3804(05)80039-8. [DOI] [PubMed] [Google Scholar]
- 5.Bean EM, Cutner A, Holland T, Vashisht A, Jurkovic D, Saridogan E. Laparoscopic myomectomy: a single-center retrospective review of 514 patients. J Minim Invasive Gynecol. 2017;24:485–93. doi: 10.1016/j.jmig.2017.01.008. [DOI] [PubMed] [Google Scholar]
- 6.Falcone T, Parker WH. Surgical management of leiomyomas for fertility or uterine preservation. Obstet Gynecol. 2013;121:856–68. doi: 10.1097/AOG.0b013e3182888478. [DOI] [PubMed] [Google Scholar]
- 7.Meurs E, Brito LG, Ajao MO, Goggins ER, Vitonis AF, Einarsson JI, et al. Comparison of morcellation techniques at the time of laparoscopic hysterectomy and myomectomy. J Minim Invasive Gynecol. 2017;24:843–9. doi: 10.1016/j.jmig.2017.04.023. [DOI] [PubMed] [Google Scholar]
- 8.(FDA) TUSFaDA. UPDATE: The FDA recommends performing contained morcellation in women when laparoscopic power morcellation is appropriate. Last Accessed Date: 25.02.2020. Available from: [Internet] https://www.fda.gov/medical-devices/safety-communications/update-fda-recommends-performing-contained-morcellation-women-when-laparoscopic-power-morcellation.
- 9.Cheung VY, Pun TC. Contained morcellation for laparoscopic myomectomy within a specially designed bag. J Minim Invasive Gynecol. 2016;23:139–40. doi: 10.1016/j.jmig.2015.08.889. [DOI] [PubMed] [Google Scholar]
- 10.Boza A, Misirlioglu S, Taskiran C, Urman B. Contained power morcellation versus transvaginal extraction for retrieval of laparoscopically removed myomas: a comparison of perioperative outcomes. Surg Innov. 2019;26:72–6. doi: 10.1177/1553350618790710. [DOI] [PubMed] [Google Scholar]
- 11.Smorgick N. Laparoscopic specimen retrieval bags. J Obstet Gynaecol India. 2014;64:370–2. doi: 10.1007/s13224-014-0598-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kho KA, Nezhat CH. Evaluating the risks of electric uterine morcellation. JAMA. 2014;311:905–6. doi: 10.1001/jama.2014.1093. [DOI] [PubMed] [Google Scholar]
- 13.Rimbach S, Holzknecht A, Schmedler C, Nemes C, Offner F. First clinical experiences using a new in-bag morcellation system during laparoscopic hysterectomy. Arch Gynecol Obstet. 2016;294:83–93. doi: 10.1007/s00404-015-3986-5. [DOI] [PubMed] [Google Scholar]
- 14.AAGL Practice Report: morcellation during uterine tissue extraction. J Minim Invasive Gynecol 2014;21:517-30. [Internet] [DOI] [PubMed]
- 15.Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions. New York: John Wiley & Sons; 2019. doi: 10.1002/14651858.ED000142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. 2009;6:e1000100. doi: 10.1371/journal.pmed.1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.National Institute of Health National Heart, Lung and Blood Institute Quality Assessment Tools. Available from: [Internet] https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools.
- 18.Cohen SL, Morris SN, Brown DN, Greenberg JA, Walsh BW, Gargiulo AR, et al. Contained tissue extraction using power morcellation: prospective evaluation of leakage parameters. Am J Obstet Gynecol. 2016;214:257.e1–.e6. doi: 10.1016/j.ajog.2015.08.076. [DOI] [PubMed] [Google Scholar]
- 19.Vargas MV, Cohen SL, Fuchs-Weizman N, Wang KC, Manoucheri E, Vitonis AF, et al. Open power morcellation versus contained power morcellation within an insufflated isolation bag: comparison of perioperative outcomes. J Minim Invasive Gynecol. 2015;22:433–8. doi: 10.1016/j.jmig.2014.11.010. [DOI] [PubMed] [Google Scholar]
- 20.Kim YW, Park BJ, Ro DY, Kim TE. Single-port laparoscopic myomectomy using a new single-port transumbilical morcellation system: initial clinical study. J Minim Invasive Gynecol. 2010;17:587–92. doi: 10.1016/j.jmig.2010.04.009. [DOI] [PubMed] [Google Scholar]
- 21.Springborg HH, Istre O. Complete plastic lining of the abdominal cavity during laparoscopic electromechanical morcellation—a promising technique. Gynecol Surg. 2015;12:133–7. [Google Scholar]
- 22.Won YB, Lee HJ, Eoh KJ, Chung YS, Lee YJ, Park SH, et al. In-bag power morcellation technique in single-port laparoscopic myomectomy. Obstet Gynecol Sci. 2018;61:267–73. doi: 10.5468/ogs.2018.61.2.267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Steller C, Cholkeri-Singh A, Sasaki K, Miller CE. Power morcellation using a contained bag system. JSLS. 2017;21:e2016–00095. doi: 10.4293/JSLS.2016.00095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Paul PG, Khurd AS, Radhika KT, Bulusu S, Paul G. techniques for laparoscopic contained tissue extraction. Curr Obstet Gynecol Rep. 2016;5:325–32. [Google Scholar]
- 25.Aoki Y, Matsuura M, Matsuno T, Yamamoto T. Single-site in-bag morcellation achieved via direct puncture of the pneumoperitoneum cap, a cordless electric morcellator, and a 5-mm flexible scope. Eur J Obstet Gynecol Reprod Biol. 2016;201:126–30. doi: 10.1016/j.ejogrb.2016.04.012. [DOI] [PubMed] [Google Scholar]
- 26.Trivedi PH, Trivedi S, Patil S. Laparoscopic in-bag morcellation compared with conventional morcellation of myomas and uterus with myomas. J Obstet Gynaecol India. 2020;70:69–77. doi: 10.1007/s13224-019-01273-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Akdemir A, Taylan E, Zeybek B, Ergenoglu AM, Sendag F. Innovative technique for enclosed morcellation using a surgical glove. Obstet Gynecol. 2015;125:1145–9. doi: 10.1097/AOG.0000000000000823. [DOI] [PubMed] [Google Scholar]
- 28.Cohen SL, Einarsson JI, Wang KC, Brown D, Boruta D, Scheib SA, et al. Contained power morcellation within an insufflated isolation bag. Obstet Gynecol. 2014;124:491–7. doi: 10.1097/AOG.0000000000000421. [DOI] [PubMed] [Google Scholar]
- 29.Paul PG, Thomas M, Das T, Patil S, Garg R. Contained morcellation for laparoscopic myomectomy within a specially designed bag. J Minim Invasive Gynecol. 2016;23:257–60. doi: 10.1016/j.jmig.2015.08.004. [DOI] [PubMed] [Google Scholar]
- 30.Semm K. Tissue-puncher and loop-ligation--new aids for surgical-therapeutic pelviscopy (laparoscopy) = endoscopic intraabdominal surgery. Endoscopy. 1978;10:119–24. doi: 10.1055/s-0028-1098278. [DOI] [PubMed] [Google Scholar]
- 31.Palomba S, Zupi E, Russo T, Falbo A, Marconi D, Tolino A, et al. A multicenter randomized, controlled study comparing laparoscopic versus minilaparotomic myomectomy: short-term outcomes. Fertil Steril. 2007;88:942–51. doi: 10.1016/j.fertnstert.2006.12.048. [DOI] [PubMed] [Google Scholar]
- 32.Seracchioli R, Rossi S, Govoni F, Rossi E, Venturoli S, Bulletti C, et al. fertility and obstetric outcome after laparoscopic myomectomy of large myomata: a randomized comparison with abdominal myomectomy. Hum Reprod. 2000;15:2663–8. doi: 10.1093/humrep/15.12.2663. [DOI] [PubMed] [Google Scholar]
- 33.Sinha R, Hegde A, Warty N, Patil N. Laparoscopic excision of very large myomas. J Am Assoc Gynecol Laparosc. 2003;10:461–8. doi: 10.1016/s1074-3804(05)60145-4. [DOI] [PubMed] [Google Scholar]
- 34.Sinha R, Hegde A, Warty N, Mahajan C. Laparoscopic myomectomy: enucleation of the myoma by morcellation while it is attached to the uterus. J Minim Invasive Gynecol. 2005;12:284–9. doi: 10.1016/j.jmig.2005.03.018. [DOI] [PubMed] [Google Scholar]
- 35.Torng PL, Hwang JS, Huang SC, Chang WC, Chen SY, Chang DY, et al. effect of simultaneous morcellation in situ on operative time during laparoscopic myomectomy. Hum Reprod. 2008;23:2220–6. doi: 10.1093/humrep/den256. [DOI] [PubMed] [Google Scholar]
- 36.Chen SY, Chang DY, Sheu BC, Torng PL, Huang SC, Hsu WC, et al. Laparoscopic-assisted vaginal hysterectomy with in situ morcellation for large uteri. J Minim Invasive Gynecol. 2008;15:559–65. doi: 10.1016/j.jmig.2008.06.002. [DOI] [PubMed] [Google Scholar]
- 37.Zhang P, Song K, Li L, Yukuwa K, Kong B. Application of simultaneous morcellation in situ in laparoscopic myomectomy of larger uterine leiomyomas. Med Princ Pract. 2011;20:455–8. doi: 10.1159/000327671. [DOI] [PubMed] [Google Scholar]
- 38.Tsai HW, Ocampo EJ, Huang BS, Twu NF, Wang PH, Yen MS, et al. effect of semisimultaneous morcellation in situ during laparoscopic myomectomy. Gynecol Minim Invasive Ther. 2015;4:132–136. [Google Scholar]
- 39.Halaska MJ, Gracia M, Laky R, Zapardiel I. Morcellation of the uterus: is there any place? Curr Oncol Rep. 2020;22:68. doi: 10.1007/s11912-020-00927-6. [DOI] [PubMed] [Google Scholar]
- 40.Zullo F, Venturella R, Raffone A, Saccone G. In-bag manual versus uncontained power morcellation for laparoscopic myomectomy. Cochrane Database Syst Rev. 2020;5:CD013352. doi: 10.1002/14651858.CD013352.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]