

Abstract
Adolescent and young adult health, development and behavior lay a foundation for future population health. Increasing rates of young adult homelessness mean there is a need for research which generates evidence to support a stronger focus on population-level prevention. Using longitudinal data from a population-based sample of young adults participating in the cross-nationally matched International Youth Development Study, we examined adolescent antecedents of young adult homelessness in Washington State in the USA and in Victoria, Australia. Participants were surveyed using a modified version of the Communities That Care youth survey. Analyses of prospective, longitudinal data from 1,945 participants, recruited as state-representative secondary school samples at Grade 7 (average age 13, 2002) and longitudinally compared at young adulthood (average age 25, 2014), showed that young adults in Washington State reported higher rates of past year homelessness (5.24%) compared to those in Victoria (3.25%). Path modelling showed less positive family management strategies at age 13 uniquely increased risk for age 25 homelessness. This effect remained after accounting for age 15 antecedents in peer-group, school, and community environments. Friends’ drug use, school suspension, academic failure, and low neighborhood attachment at age 15 mediated the association between less positive family management strategies at age 13 and age 25 homelessness. Despite observing some cross-national differences in levels of family, peer-group, school, and community antecedents, we found that these factors equally increased risk for age 25 homelessness in both states, suggesting similar cross-national influences for young adult homelessness. The findings indicate cross-nationally common adolescent antecedents for young adult homelessness that could be targeted by prevention strategies across international settings.
Keywords: Homelessness, Adolescents, Young adults, Cross-state study, Risk factors, Prevention
Introduction
Young adulthood lays an important foundation for health across the life-course and for future population health (Patton et al. 2018; Patton et al. 2016; Sawyer et al. 2012). Internationally, reducing homelessness among adolescents and young adults remains a major challenge. Slowing its rise and minimizing its impact are crucial for individuals and society. National prevalence estimates from the USA suggest approximately 567,000 people were homeless in 2019, of those, 8.4% were aged 18–24 years (Statista 2020). An estimated 290,400 persons experienced homelessness in Australia in 2019, of whom 14.2% were between ages 18–24 (Australian Institute of Health & Welfare 2020). Young adult homelessness is a significant driver of poor health outcomes, reduced educational opportunities and social inequality, severely disrupting the attainment of adult developmental milestones that set the stage for later economic stability, psychological and physical health, and social well-being (e.g., Koegel et al. 1995; van den Bree et al. 2009). Identifying malleable life-course antecedents that increase risk for or protect against homelessness, and the social context in which they arise, is critical to identifying points of intervention that will affect young adult homelessness at the population level.
Despite evidence of profound health and social inequalities experienced by the homeless efforts to address these inequalities have been inadequate in health and social policy. We do not have a current evidence base that is adequate to inform primary homelessness prevention at the population-level (Heerde and Patton 2020). A lack of robust evidence on life-course antecedents of homelessness among population-based samples severely limits system-wide capacity to develop evidenced-based prevention and intervention strategies for reducing risks for homelessness. A stronger focus on population-level prevention holds promise for reducing the number of young adults entering homelessness. In this context, studies that have adequately measured antecedents of homelessness across the formative years from adolescence to young adulthood are needed to further understanding of the developmental course of homelessness. As we will generate here, such studies are needed to enable development and refinement of evidence-based approaches seeking to reduce homelessness and understand what the gains from effective primary prevention interventions might be.
Population-Based Studies of Young Adult Homelessness
Prevention science approaches, which call for understanding early developmental (life-course) predictors (antecedents) and their effect on later health and behavior (Catalano et al. 2012), are likely to provide valuable information for developing prevention programming or adapting existing programs that better respond to antecedents of young adult homelessness. Despite repeated calls for longitudinal studies, few exist (e.g., Brakenhoff et al. 2015; Tyler and Bersani 2008; van den Bree et al. 2009; Shelton et al. 2009; Heerde et al. 2020). One reason lies in the difficulty of obtaining reliable, robust longitudinal data on a population group, who are difficult to engage and retain in descriptive or intervention studies (Aldridge et al. 2018; Heerde and Patton 2020; van den Bree et al. 2009). Consequently, most prior studies have used retrospective study designs with data collected from purposefully recruited community-based samples of homeless participants without a comparison group of non-homeless participants (van den Bree et al. 2009). While such studies provide an indication of correlates of homelessness, they do not provide sufficient data for etiological purposes of identifying developmental antecedents of homelessness.
Across the few studies that have analyzed data from population-based samples various antecedents of homelessness have been specified. However, these studies were limited either by their cross-sectional nature (Bearsley-Smith et al. 2008; Shelton et al. 2009), or, where longitudinal studies were conducted, a shortage of data spanning key developmental periods (e.g., adolescence to adulthood; Brakenhoff et al. 2015; Tyler and Bersani 2008; van den Bree et al. 2009). Across these studies, less positive family management practices (e.g., permissive parenting styles, lower relationship quality), childhood abuse and removal from the family by child protective services increased risk for homelessness (Brakenhoff et al. 2015; Shelton et al. 2009; Tyler and Bersani 2008; van den Bree et al. 2009; Bearsley-Smith et al. 2008). Having been suspended from school and academic underachievement were associated with young adult homelessness (Heerde et al. 2020; Brakenhoff et al. 2015; Tyler and Bersani 2008; van den Bree et al. 2009) as was associating with peers engaged in problem behavior (Bearsley-Smith et al. 2008). Residing in a community with higher levels of poverty, victimization, and lower attachment to ones’ neighborhood increased risk for young adult homelessness (Shelton et al. 2009; Tyler and Bersani 2008).
Applying Life-Course and Social-Ecological Theories to Young Adult Homelessness
Few prior studies on young adult homelessness have been embedded within life-course theory (e.g., Whitbeck et al. 2000). This study draws on two complementary theoretical frameworks, life-course theory (Hser et al. 2007; Elder et al. 2003) and the social development model (SDM; Catalano and Hawkins 1996). Life-course theory is commonly used in longitudinal studies investigating how exposure to risk and protective factors at specific points in development influence subsequent health and social outcomes (Elder et al. 2003).
The SDM hypothesizes that individuals form social bonds within multiple socializing contexts (e.g., family, peer-group, school and community; Catalano and Hawkins 1996; Cambron et al. 2019) and the development of these bonds can be an important promotive influence on health and social outcomes. For example, early positive socialization experiences within the family set foundations for later bonding with pro-social peers, and for avoiding bonding with antisocial peers (Cambron et al. 2019). Both life-course theory and the SDM detail that (1) early development experiences influence later development; (2) stages of development have cumulative effects; and (3) development occurs in the context of multiple and interacting socializing contexts and as a result of exposure to both risk and protective factors (Cambron et al. 2019; Catalano and Hawkins 1996; Elder et al. 2003; Hser et al. 2007).
Longitudinal Cross-national Studies of Young Adult Homelessness
Cross-national comparisons of longitudinal study findings offer benefits as they (1) promote understanding of the comparability of etiologic processes across nations, and (2) permit testing of whether mean levels of potential antecedents are similar or different, which may reflect differences in macro-level policy and the socio-ecological contexts that affect mean levels of risk (or protection). The observation of cross-national differences in antecedents across two countries can identify those that may have a culturally specific influence (Jessor 2008; Segall et al. 1998). The analysis of data from two-country samples also permits the testing of hypotheses in one country to be confirmed in the second country (McMorris et al. 2007) allowing within-study replication of findings. Such studies are rare, despite their utility to inform policy and test theories of the etiology of homelessness and other problem behaviors.
A prior longitudinal study using the current sample, sought to examine longitudinal associations between a wide range of individual, family, peer-group, school, and community antecedents measured in grades 7–9 (ages 13–15 years) and age 25 homelessness. Results from multivariable logistic regression analyses found that only academic failure and school suspension increased risk for later homelessness (Heerde et al. 2020). The strength of association between these antecedents and homelessness was similar in Australia and the USA. A notable limitation of this study, and prior longitudinal studies examining antecedents of later homelessness (e.g., adolescence to adulthood; Brakenhoff et al. 2015; Tyler and Bersani 2008; van den Bree et al. 2009), is that it merely identified those adolescent factors that were uniquely associated with homelessness, but did not examine temporal or mediational relationships among variables. As a consequence, capacity for understanding the complex and potentially interacting risk relationships between modifiable antecedents and homelessness across adolescence and into young adulthood in these studies was restricted.
In this prior study, it was recommended that further research modelling and testing unique risk relationships across a broad range of malleable antecedents and across multiple interacting social-ecological contexts, congruent with the SDM, be undertaken (Heerde et al. 2020). To this end, in the current study, we employed longitudinal path modelling to examine early antecedents of homelessness more comprehensively across adolescence and into young adulthood. Specifically, this modelling approach permited us to not only examine the direct effect of adolescent antecedents on young adult homelessness, but also indirect effects and relationships between antecedents. That is, the goal of the current study was to provide a more detailed map of longitudinal pathways to homelessness. Congruent with life-course theory (Elder et al. 2003) and the SDM (Catalano and Hawkins 1996), we expected that risk within the family environment would increase risk across other adolescent social contexts (e.g., peer-group, school and community contexts). For example, prior analyses of data from the International Youth Development Study have shown family risk (e.g., conflict) in adolescence is associated with later peer, school, and community risk factors for socially disruptive behaviors such as substance use (Kelly et al. 2012; Scholes-Balog et al. 2020).
In the current study, we built upon our previous findings by analyzing data from the same population-based state representative cohort to delve into whether and how family, peer-group, school, and community antecedents during adolescence (~ages 13–15 years) are associated with risk of homelessness in young adulthood (~age 25 years) in Washington State and Victoria. We hypothesized that (1) family antecedents in early adolescence (~age 13) will increase risk for young adult homelessness (~age 25); and (2) antecedents in peer-group, school, and community settings in mid-adolescence (~age 15) will mediate the expected association between family risk factors and later homelessness. An important validity check in cross-national studies is to make sure these risk relationships are the same across countries. Hence, we tested whether associations between family, peer-group, school, and community antecedents during adolescence and young adult homelessness were moderated by State.
Methods
Sample
Data were drawn from a population-based sample of young adults participating in the International Youth Development Study (IYDS). The IYDS is an ongoing longitudinal study examining the epidemiology and etiology of health risk and socially disruptive behaviors among participants from Victoria, Australia and Washington State, in the United States . Participants were initially recruited as adolescents in state-representative secondary school samples in 2002 at age 12 years and have been followed to 2014–15 at age 25 years.
To ensure cross-national validity and to reduce method differences, the study design was subjected to several processes in 2001, including matching sampling, recruitment, surveys and survey administration procedures. The survey underwent cognitive pretesting and piloting, including language review and cross-national item adaptation to ensure content validity across the two states (for full details see McMorris et al. 2007). These processes reduced methodological problems identified in many prior international comparison studies (Segall et al. 1998). To achieve state-representative samples, participants were recruited using a two-stage cluster sampling approach in 2002: (1) public and private schools with Grades 5, 7 and 9 were randomly selected for recruitment into the study using a probability proportionate to grade-level size sampling procedure and (2) one class at the appropriate grade level was randomly selected within each school (McMorris et al. 2007).
The original IYDS sampling and recruitment methods have been described in detail elsewhere (McMorris et al. 2007). In sum, across all Grade levels, 7782 eligible students (3926 in Victoria) were approached to participate. Of these students, 2885 (74.8%) in Washington State and 2884 (73.5%) in Victoria consented to and took part in the 2002 survey. At the time of recruitment, both states were similar in demographic and economic characteristics including: population size and urbanicity, higher than national levels of educational participation, and low proportions of residents living in poverty (McMorris et al. 2007). The current study uses data from the cohort in Grade 7 (average age 13, 2002), as well as follow-up data collected from these individuals in Grade 9 (average age 15, 2004) and at young adulthood (average age 25, 2014) in both states. Retention rates in both states were 83% or higher at all follow-up surveys.
The analysis sample includes 1945 young adults (51% female; n = 984 in Victoria), ranging between 12 and 16 years of age (mean (M) = 13.01 years, standard deviation (SD) = .43) at study outset. Race and ethnicity are conceptualized differently in Australia and the USA. In Australian policy and culture, identity is conceptualized as Australian rather than based on ancestry. Therefore, most of the Victorian sample identified as Australian (91%) and the Washington State sample had a majority identifying as white (65%). In Washington State, 16% of the sample identified as Hispanic/Latinx, 4% African/American, 6% Native American and 6% as Asian/Pacific Islander. Participants self-reported their sexual identity at age 25 only. Most of the sample identified as completely heterosexual (straight; 81% in Victoria, 79% in Washington State). In Victoria, 13% identified as mostly heterosexual (straight, but somewhat attracted to people of their own sex; 14% in Washington State), 2% as bisexual (attracted to men and women equally; 3% in Washington State), 1% as mostly homosexual (gay or lesbian, but somewhat attracted to people of the opposite sex; 1% in Washington State), 2% as completely homosexual (gay or lesbian; 0.8% in Washington State), and 0.5% as asexual (0.1% in Washington State). At the age 25 survey, the sample ranged in age between 23 and 27 years (M = 25.14, SD = .84; 53% female).
Procedure
Ethics approval.
The University of Melbourne Human Ethics in Research Committee and the Royal Children’s Hospital Ethics in Human Research Committee approved the study in Australia. In Washington State, the University of Washington Human Subjects Institutional Review Board approved the study. Written parental consent and participant assent was obtained for all participants at study outset; participant consent was obtained at age 25. During adolescence, relevant educational authorities for public and private schools in Victoria and Washington State provided permission to conduct the research in schools.
Survey administration.
A single survey administration protocol was used by trained survey staff in both states. At ages 13 and 15, surveys were administered to class groupings within schools. The age 25 survey was administered online. During adolescence Victorian participants received a small gift (e.g., stress ball) and Washington State participants received USD$10, at the completion of each survey. At age 25, participants in both states received a USD/AUD$40 gift voucher as reimbursement for their time.
Measures
Self-report measures of adolescent risk factors (antecedents) and young adult homelessness were adapted from the Communities That Care youth survey (Arthur et al. 2002; Glaser et al. 2005; Hemphill et al. 2011) and were selected based on the SDM, prior research (Bearsley-Smith et al. 2008; Brakenhoff et al. 2015; Shelton et al. 2009; van den Bree et al. 2009) and availability of measures in the IYDS dataset. All measures have demonstrated longitudinal validity and reliability for adolescents in Victoria (Hemphill et al. 2011) and Washington State (Arthur et al. 2002; Glaser et al. 2005).
Young adult (age 25) homelessness (dependent variable).
The item, “In the past year, have you been homeless (i.e., not had a regular place to live?)” was used to measure homelessness at age 25 years. Response options were dichotomous, ‘Yes’ (1) and ‘No’ (0).
Demographic antecedents.
Participants reported their age (date of birth), gender (male [0] or female [1]) and the state in which they lived (Washington State [0] or Victoria [1]). A measure of family socio-economic status (Family SES) was created using parent (mother and father) reported level of annual family income (ranging from ‘less than $10 000’ through to ‘$200 000 and above’) and highest level of education (e.g., less than secondary school, completed secondary school, and completed post-secondary school). Parents self-reported levels of income and education were obtained in phone interviews conducted around the time when their adolescent child took part in the 2002 (age 13) survey.
Age 13 family antecedents.
Poor family management strategies (e.g., family rules, monitoring, negative reinforcement) were measured using nine items (Cronbach’s α = .80); “Would your parents know if you did not come home on time?” is an example item. Family conflict was measured using three items (Cronbach’s α = .81) such as “People in my family have serious arguments.” Four items were used to examine low attachment to parent(s) (Cronbach’s α = .77). “Do you share your thoughts and feelings with your mother?” is an example item. For each of these measures’ response options ranged from ‘definitely no’ (1) through to ‘definitely yes’ (4). The scale measuring attachment to parent(s) was reverse coded so that lower levels of attachment were indicated by a higher score.
Age 15 peer-group antecedents.
Interaction with antisocial peers consisted of eight items (Cronbach’s α = .85). “In the past year, how many of your best friends have attacked someone with the idea of seriously hurting them?” is an example item. Four items including “In the past year, how many of your best friends have tried alcohol (like beer, wine, or liquor/spirits) when their parents didn’t know about it?” were used to examine friends’ use of drugs (Cronbach’s α = .79). Response options for both scales ranged from ‘none of my friends’ (0) through to ‘4 of my friends’ (4).
Age 15 school antecedents.
Academic failure was measured using two items. “Putting them all together, what were your grades/marks like last year?” is an example item. Response options ranged from ‘very good’ (1) through to ‘very poor’ (4). School suspension was assessed using the item, “How many times in the past year have you been suspended from school?” Response options ranged from ‘never’ (1) through to ‘40+ times’ (8). The item “How important do you think the things you are learning in school are going to be for your later life?” is one of seven items (Cronbach’s α = .80) used to measure low commitment to school. Response options ranged from ‘very important’ (1) through to ‘not at all important’ (5). Four items were used to measure low recognition for prosocial involvement (Cronbach’s α = .73). “My teacher(s) notices when I am doing a good job and lets me know about it” is an example item. Response options ranged from ‘definitely no’ (1) through to ‘definitely yes’ (4) and were reverse coded so that lower levels of recognition were indicated by a higher score.
Age 15 community antecedents.
Low neighborhood attachment was measured using three items (Cronbach’s α = .83) including “I’d like to get out of my neighborhood.” Five items, such as “How much do each of the following statements describe your neighborhood: lots of empty or abandoned buildings.” were used to assess community disorganization (Cronbach’s α = .85). Response options for both scales ranged from ‘definitely no’ (1) through to ‘definitely yes’ (4).
Survey response accuracy was examined at ages 13 and 15. Responses were coded as questionable if participants reported (1) “I was not honest all of the time” when asked how honest they were when completing the survey; (2) use of a fictitious drug (included in the survey for accuracy checking) in the past month; and (3) drug use on >120 occasions in the past month.
Statistical Analysis
Descriptive analyses were performed using Stata SE software for Windows Version 15.1 (StataCorp LLC 2017). Fifteen participants at age 13 and 27 at age 15 met the criteria for questionable responses (e.g., use of a fictious drug), and were excluded from the analyses. The percentage of missing data on the analyzed variables ranged from 0 – 4% (M = 2.4%).
Tests of differences in means and frequencies for age 13 family, age 15 peer-group, school and community antecedents, and age 25 homelessness between the two states, and by homelessness status (for antecedents), were conducted using t tests and chi-square analyses. Pooled standard deviations were used to calculate effect sizes (Cohen 1977). Zero-order correlations were examined to show highly correlated pairs or sets of variables that might result in collinearity in the subsequent path analyses.
Two longitudinal path models (see Figure 1) were estimated using Mplus, version 8.2 (Muthén and Muthén 2017). Full information maximum likelihood estimation was used in all analyses to minimize potential bias due to missing data (Muthén and Muthén 2017; Schafer and Graham 2002). Model estimation proceeded as follows. We first estimated associations between age 13 family antecedents and age 25 homelessness (Step 1; Figure 1A). Building on results from this first model, we then estimated pathways from age 13 poor family management through age 15 peer-group, school, and community antecedents to age 25 homelessness (Step 2; Figure 1B). Indirect (i.e., mediated) effects of age 13 poor family management on age 25 homelessness via age 15 variables were estimated in model 2 using the modelindirect function. Demographic factors (age 13) were included in the analyses. Model fit indices were examined in accordance with current recommendations (Cangur and Ercan 2015). The results presented are fully standardized.
Figure 1.
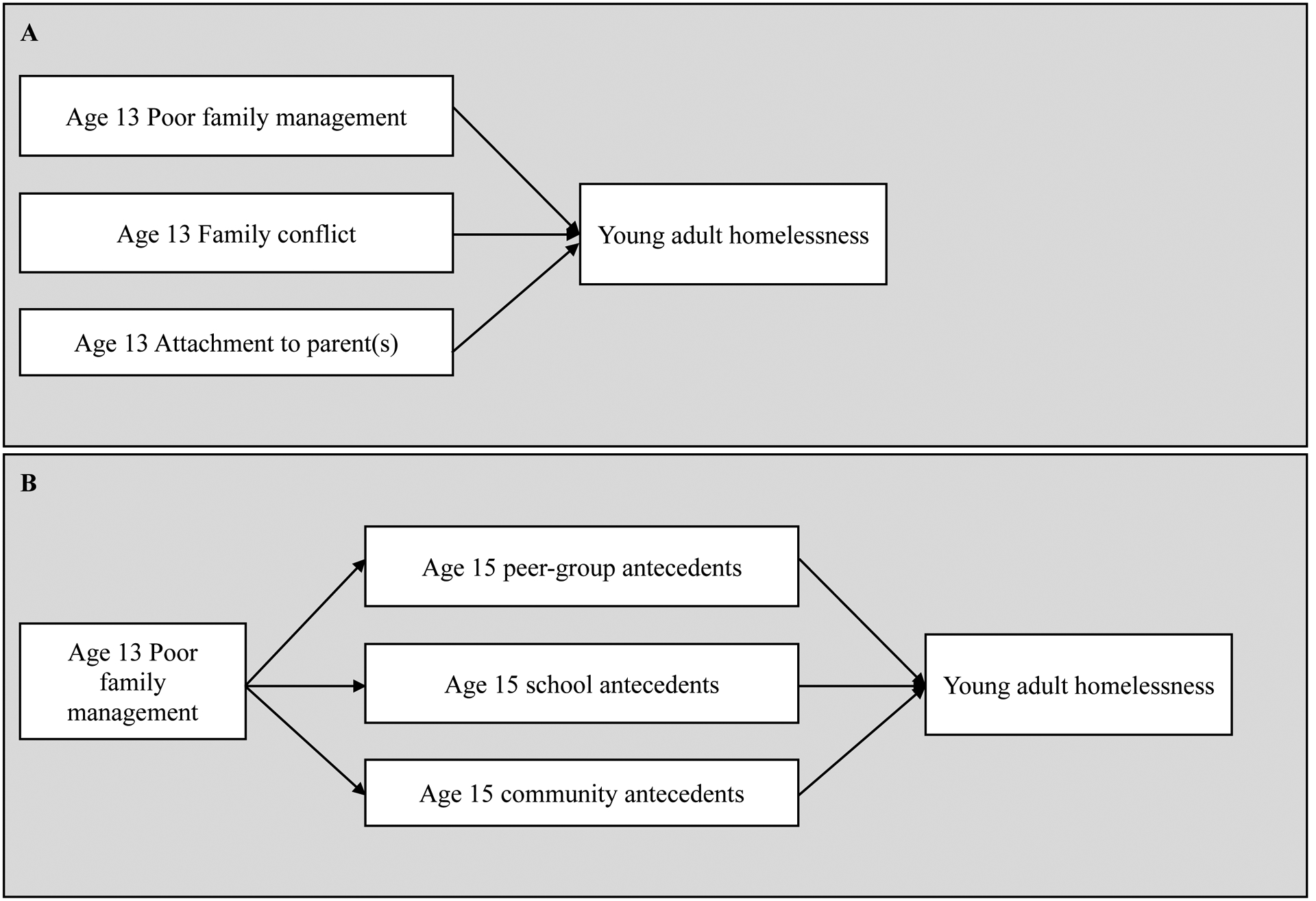
Hypothesized models for young adult homelessness.
Multiple-group modeling and chi-square difference testing in Mplus (Muthén and Muthén 2017) were used to test whether the identified relationships differed across the two states. Differences in model fit between a model constraining parameters to be equal in the two states, and an unconstrained model were tested using the difftest function.
Results
State Comparisons of Adolescent Risk Factors and Young Adult Homelessness
Table 1 in the online supplementary material shows adolescents in Washington State were slightly older than those in Victoria at baseline and reported slightly higher family socio-economic status. At age 13, Victorian participants reported less positive family management practices compared to those in Washington State. Significantly lower attachment to parents was found for Washington State compared to Victorian adolescents. Washington State compared to Victorian participants showed significantly higher levels of interacting with antisocial peers, academic failure, and significantly lower attachment to their neighborhood at age 15. Victorian compared to Washington State adolescents were less committed to school. Young adults in Washington State reported significantly higher rates of past year homelessness compared to those in Victoria (5.24% [95% CI 3.92, 6.97] vs. 3.25% [95% CI = 2.25, 4.67]).
Correlations and Comparisons of Adolescent Antecedents by Homelessness Status
Intercorrelations among study variables were low-moderate and in the expected direction (range r = .01 to r = .64; see online supplementary material Table 2). Table 3 in the online supplementary material shows means and frequencies for age 13 and 15 antecedents by age 25 homelessness status. Overall, compared to young adults who were not homeless, those who reported experiencing homelessness at age 25 generally reported higher levels of antecedent risk factors in family (age 13), peer-group, school, and community (age 15) social contexts.
Step 1: Path Model of Family Antecedents of Young Adult Homelessness
Results showed being female was uniquely associated with more positive family management practices, higher levels of family conflict and lower attachment to parents at age 13 (see Figure 2). Living in Victoria uniquely increased risk for poor family management practices and lower attachment to parents. Less positive family management practices uniquely increased risk for age 25 homelessness. Family conflict and low attachment to parents were not uniquely related to age 25 homelessness and were dropped from further modeling. Living in Victoria was uniquely associated with a lower likelihood of age 25 homelessness. Full results for the Step 1 model are included in the online supplementary material (Table 4).
Figure 2.
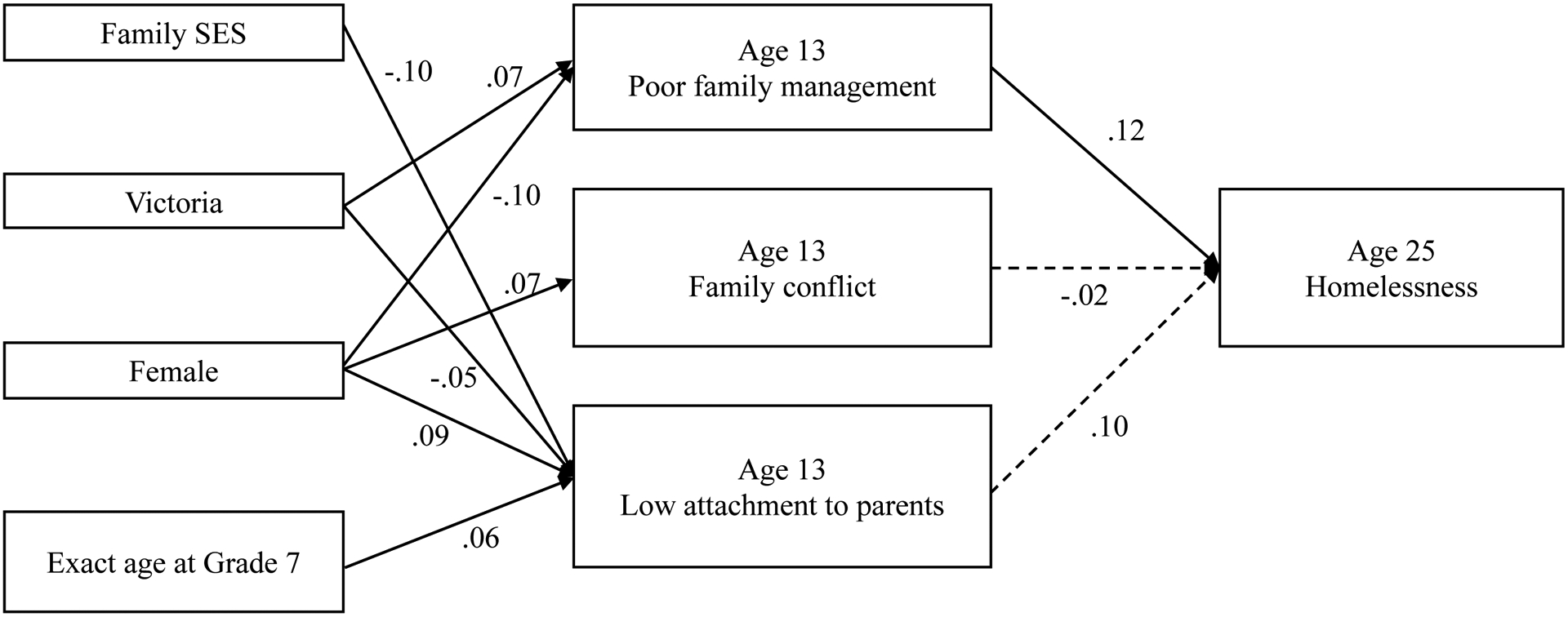
Results from the path model: early adolescent family antecedents of young adult homelessness
Note. Model fit statistics: χ2(22, N = 1874) = 736.48, p < .0001, comparative fit index (CFI) = 1.00, Tucker-Lewis index (TLI) = 1.00, root-mean-square error of approximation (RMSEA estimate) = 0.00. Dashes indicate non-significant paths. Solid lines indicate paths significant at p < .05. For ease of viewing, paths from demographic variables to each of the Age 13 family antecedents are not included in the Figure, however, they were included in the model.
Step 2: Modelling Associations among Family, Peer-Group School, and Community Antecedents of Young Adult Homelessness
Less positive family management practices at age 13 uniquely increased risk for age 15 peer-group, school, and community antecedents (see Figure 3). Family socio-economic status, gender, age, and state were associated with age 15 peer-group, school, and community antecedents. In this model, the direct effect of age 13 family management practices on age 25 homelessness was no longer significant, however, a small, but statistically significant total indirect effect was observed (standardized parameter estimate .09). Friends’ use of drugs, school suspension, academic failure, and low neighborhood attachment at age 15 significantly mediated the association between less positive family management practices at age 13 and age 25 homelessness. Living in Victoria continued to reduce the likelihood of homelessness at age 25 after all variables were included in the model. Full results for the Step 2 model are included in the online supplementary material (Table 5).
Figure 3.
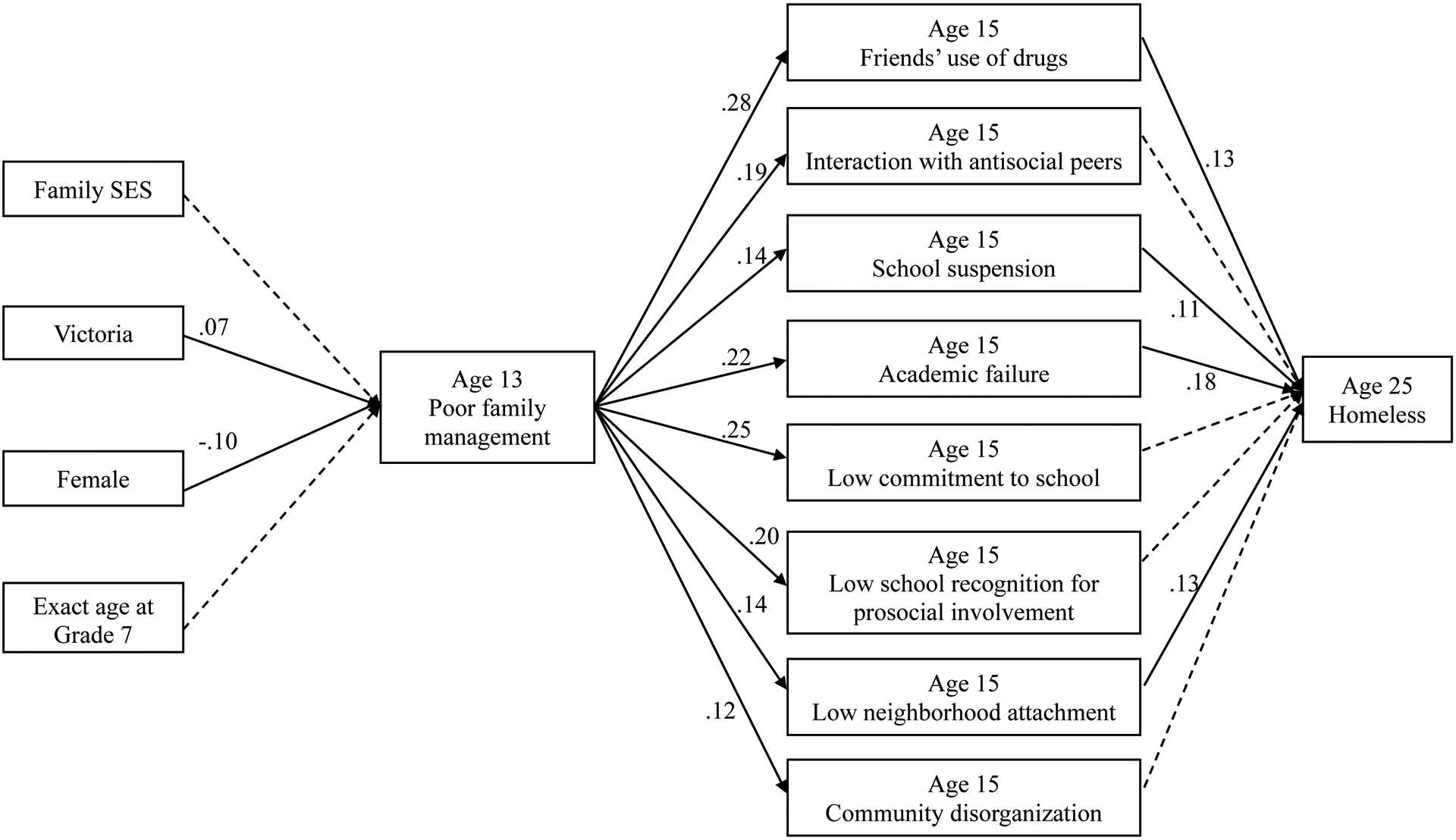
Results from the path model: family, peer-group, school, and community antecedents of young adult homelessness.
Note. Model fit statistics: χ2(22, N = 1878) = 6329.76, p < .0001, CFI = 1.00, TLI = 1.00, RMSEA estimate = 0.00. Dashes indicate non-significant paths. Solid lines indicate paths significant at p < .05. For ease of viewing, paths from demographic variables to each of the Grade 9 antecedents are not included in the Figure, however, they were included in the model.
Cross-State Equivalence of Associations among Adolescent Antecedents of Young Adult Homelessness
Tests of model equivalence by state showed poor fit of the constrained model. To achieve acceptable fit, we released constraints on the association between family SES and other model variables, as well as constraints on the intercorrelations among mediators. No cross-state differences in structural pathways between adolescent antecedents and young adult homelessness were found. Full results for the multiple group model are included in the online supplementary material (Table 6).
Discussion
Reducing young adult homelessness remains a major challenge. Research that generates evidence to support a stronger focus on population-level prevention efforts to target risk in individuals before they are at high risk of homelessness is needed. The current study, using longitudinal data collected from a state representative population-based sample, demonstrates it is possible to identify adolescent antecedents of young adult homelessness, and interrelationships among them, at a population level. Cross-national differences in associations between these antecedents and young adult homelessness are also identifiable. The findings suggest that intervention points targeting antecedents across the formative years from adolescence to young adulthood may reduce risk for later homelessness at a population level and may have application in both Australia and the USA.
Understanding risk within adolescent social contexts is essential to identifying individuals who may be at higher risk of homelessness and intervening early to reduce this risk. Our findings suggest that broader indicators of early adolescent family dysfunction (e.g., less positive family management strategies) are important antecedents to young adult homelessness and are important in prevention efforts targeting the adolescent family milieu. Findings from the few prior population-based studies of homelessness antecedents support this notion, and indicate permissive parenting styles, lower parent-adolescent relationship quality and nontraditional family structures are also indicators of family functioning associated with homelessness (Brakenhoff et al. 2015; Shelton et al. 2009; Tyler and Bersani 2008; van den Bree et al. 2009).
In line with life-course and SDM theories (Catalano and Hawkins 1996; Cambron et al. 2019) we examined the longitudinal influence of several indicators of family dysfunction (i.e. less positive family management strategies, low attachment to parents and family conflict) from early in adolescence into young adulthood. There appears to be a complex relationship between antecedents within the family environment, broader socializing contexts and homelessness into young adulthood. We found that less positive family management strategies (including a lack of clear rules, low parenting monitoring and supervision) in early adolescence (age 13) increased risk for young adult homelessness at age 25 years. Congruent with life-course theory (Elder et al. 2003) and the SDM (Catalano and Hawkins 1996), our findings suggest antecedents within the family environment uniquely increased risk within peer-group, school and community contexts in mid-adolescence (age 15), and that positive social boundaries in the early adolescent family milieu set a foundation for healthy social relationships outside of the family unit, including those related to schooling, peer-group affiliations and community connection. Our findings highlight the importance of family management as a potential marker for later homelessness while also suggesting that prevention and intervention within other important adolescent social contexts, particularly peer-group, school, and community settings, is warranted. Where adolescents experience poor family management, averting or delaying engagement with substance-using peers, suspension from school and academic underachievement, may be important targets for prevention strategies. Relationships with prosocial peers and supportive adults may help to counteract poor management within the family (Kelly et al. 2016; Kelly et al. 2012) and later homelessness. Programming and intervention efforts that support these aspects of family and broader social functioning may help in addressing young adult homelessness.
Our findings illustrate the potential of longitudinal population-based studies to identify modifiable antecedents of homelessness and potential intervention points for preventing the transition into homelessness. Existing multi-sectoral tested-effective universal prevention programs have successfully addressed many of these antecedents in the USA (e.g., Blueprints for Healthy Youth Development 2019). For example, Communities That Care (CTC) has demonstrated success in reducing life-course antecedents of a range of adolescent and young adult health risk and socially disruptive behaviors, including those identified here as increasing risk for young adult homelessness (e.g., peer drug use; Hawkins et al. 2014; Toumbourou et al. 2019). Where decreases in rates of young adult homelessness are shown to result from the implementation of intervention strategies within CTC communities, findings will provide further guidance to system-wide homelessness prevention policy and programming. A key area for future longitudinal studies is to further understand developmental antecedents of homelessness, and antecedents and mechanisms of persistence and desistence of homelessness across socializing contexts. Testing the effectiveness of prevention frameworks such as CTC is warranted.
Distinctive from prior population-based studies, we examined cross-national differences in antecedents that increase risk for young adult homelessness. Although there were some cross-national differences in inter-concept correlations in mid adolescence, we found a similar cross-national profile of adolescent antecedents in our multi-group analysis. These results support the generality of estimating the unique effects of a broad range of malleable antecedents grounded in the SDM and life-course theory across two Western countries. That is, despite observed level differences in the mean or prevalence of multiple antecedents, the developmental processes leading to increased risk for young adult homelessness were the same in both Victoria and Washington State.
The findings further suggest that common intervention points targeting similar antecedents within family, peer-group, school, and community contexts, may reduce risk for young adult homelessness in both states (Victoria and Washington State). Notably, although our samples were state-representative and similar in economic characteristics (McMorris et al. 2007) at the time of study commencement in 2002, our findings showed a common cross-national effect for early adolescent family socioeconomic deprivation and young adult homelessness. Further cross-national research investigating developmental antecedents across the multiple socializing contexts in which children, adolescents, and young adults interact should seek to confirm the current findings and identify antecedents in other potential spheres of influence.
Study strengths and limitations.
This is one of few prospective, longitudinal studies that has examined antecedents of homelessness, using data collected from a population-based sample, across the formative years from adolescence to young adulthood, and where data on the antecedents analyzed was collected prior to the transition to homelessness. The study is unique in examining two cross-state samples, which were state-representative at the time of study commencement in 2002. The study has used identical methods in recruitment, surveying and longitudinal follow-up, and demonstrates consistently high retention rates (McMorris et al. 2007; Heerde et al. 2020). Thus, the study presents a unique opportunity to examine cross-national antecedents of homelessness prospectively over multiple periods of development, using detailed data on a wide range of factors, relative to prior studies. The ability of this study to maximize the available data to investigate the research questions, is a notable strength.
We acknowledge several study limitations. The study found rates of young adult homelessness below the respective national average in both states. While national prevalence estimates provide valuable information on rates of homelessness across age groups, it is generally acknowledged these rates are likely underestimates of homelessness (Hall et al. 2020; Morton et al. 2018). Rates of homelessness in the current study are likely subject to underestimation. Despite participants being provided with assurances of confidentiality and anonymity when completing the survey, it is possible perceived stigma associated with experiencing homelessness may be intensified in a longitudinal survey where participants know they will be surveyed again. Although retention rates are high in the current study, it may be that individuals experiencing homelessness were less likely to participate at age 25. Owing to the low rate of young adult homelessness (72 cases), our analyses may have been underpowered to detect very small effects as significant. Notwithstanding, we were able to detect significant path model parameters as small as .11 (linking age 15 school suspension and age 25 homelessness) and a small, statistically significant indirect effect of age 13 family management on age 25 homelessness (0.09). Single item measures of homelessness such as that used here are common in prior studies (Heerde et al. 2014; Heerde et al. 2015), however, the use of a single item measure has limited our capacity to examine the variety of conditions that may represent young adult homelessness (e.g., rough sleeping, couch surfing, family homelessness).
Several limitations regarding the measures analyzed in this study are noted. During adolescence, participants were not asked about their sexual identity or orientation, nor their gender identity beyond the binary question of male or female. Given the high proportions of young adults identifying as being Australian (in Victoria) and White (in Washington State) or identifying as heterosexual (>90% in both states), our analyses did not control for, or examine differences in associations by, ethnicity or sexual identity. Prior research has noted childhood trauma, abuse, and out-of-home care placement as key factors influencing homelessness (e.g., Bearsley-Smith et al. 2008; Koegel et al. 1995). These measures were not available in the current study; thus, we were unable to control for or test these potential associations. All measures analyzed are based on self-report data. The use of self-report data in studies of adolescents and young adults and for the antecedents examined here is considered reliable (e.g., Jolliffe et al. 2003). Our analyses focused exclusively on antecedents that increase risk for young adult homelessness. The potential role of antecedents that decrease or moderate the effect of risk for young adult homelessness requires detailed study. Last, our findings are generalizable only to the state and cohort samples analyzed.
Conclusions
This study is unique in its identification of developmental antecedents of young adult homelessness, and points of intervention, within cross-nationally matched population-based cohorts. Findings suggested that less positive family environment characteristics in early adolescence increase risk for young adult homelessness by increasing risk across peer-group, school, and community settings in mid-adolescence. Our findings showed a similar set of cross-national adolescent antecedents for later homelessness suggesting that there are similar developmental influences on young adult homelessness in both states. The analysis of cross-national population-level longitudinal data is needed to continue modelling antecedents of homelessness and points of intervention that ensure young adults make a successful transition into stable housing. Understanding developmental risks and mechanisms that influence persistence and desistence of young adult homelessness is an area for future inquiry. The effectiveness of prevention frameworks such as CTC, which are used to implement universal level tested and effective preventive strategies, for reducing young adult homelessness requires detailed investigation. Such studies are vital for establishing an evidence base that is adequate to inform population-level homelessness prevention.
Supplementary Material
Acknowledgements:
The authors express their appreciation to project staff and participants.
Funding sources:
Dr Heerde is currently supported by funding from a Melbourne Research Fellowship and is grateful for support from the Westpac Scholars Trust (Research Fellowship, 2017-2020). The authors are grateful for the financial support of the National Institute on Drug Abuse (R01DA012140), National Institute on Alcoholism and Alcohol Abuse (R01AA017188), Australian National Health and Medical Research Council (NHMRC; 491241, 594793, 1047902) and Australian Research Council (DP109574, DPO663371, DPO877359). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders. The funding agencies did not have any involvement in the analysis and interpretation of data, the writing of the article or the submission of the article for publication.
Footnotes
Ethical approval: The University of Melbourne Human Ethics in Research Committee and the Royal Children’s Hospital Ethics in Human Research Committee in Victoria and the University of Washington Human Subjects Institutional Review Board in Washington State approved the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of these institutions and the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent: Informed consent was obtained from all individual study participants.
Conflicts of interest: The authors declare that they have no conflict of interest.
References
- Aldridge RW, Story A, Hwang SW, Nordentoft M, Luchenski SA, Hartwell G, et al. (2018). Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: a systematic review and meta-analysis. The Lancet, 391(10117), 241–250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arthur M, Hawkins JD, Pollard JA, Catalano RF, & Baglioni A Jr (2002). Measuring risk and protective factors for use, delinquency, and other adolescent problem behaviors: The Communities That Care Youth Survey. Evaluation Review, 26(6), 575–601. [DOI] [PubMed] [Google Scholar]
- Australian Institute of Health & Welfare (2020). Specialist homelessness services annual report 2019. Cat. no. HOU 322 Canberra: Australian Institute of Health & Welfare. [Google Scholar]
- Bearsley-Smith CA, Bond LM, Littlefield L, & Thomas LR (2008). The psychosocial profile of adolescent risk of homelesssness. European Child & Adolescent Psychiatry, 17(4), 226–234, doi: 10.1007/s00787-007-0657-5. [DOI] [PubMed] [Google Scholar]
- Blueprints for Healthy Youth Development (2019). Registry of Experimentally Proven Programs. https://www.blueprintsprograms.org. Accessed 14/92020.
- Brakenhoff B, Jang B, Slesnick N, & Snyder A (2015). Longitudinal predictors of homelessness: findings from the National Longitudinal Survey of Youth-97. Journal of Youth Studies, 18(8), 1015–1034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cambron C, Catalano RF, & Hawkins JD (2019). The Social Development Model. In Farrington DP, Kazemian L, & Piquero AR (Eds.), The Oxford Handbook of Developmental and Life-Course Criminology. New York: Oxford University Press. [Google Scholar]
- Cangur S, & Ercan I (2015). Comparison of model fit indices used in structural equation modeling under multivariate normality. Journal of Modern Applied Statistical Methods, 14(1), 14. [Google Scholar]
- Catalano RF, Fagan AA, Gavin LE, Greenberg MT, Irwin CE Jr, Ross DA, et al. (2012). Worldwide application of prevention science in adolescent health. The Lancet, 379(9826), 1653–1664, doi: 10.1016/S0140-6736(12)60238-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Catalano RF, & Hawkins JD (1996). The Social Development Model: A Theory of Antisocial Behavior. In Hawkins JD (Ed.), Delinquency and Crime: Current theories (pp. 149–197). New York: Cambridge. [Google Scholar]
- Cohen J (1977). Statistical power analysis for the behavioural sciences (Revised edition). New York: Academic Press. [Google Scholar]
- Elder GH, Johnson MK, & Crosnoe R (2003). The emergence and development of life course theory. In Mortimer J, & Shanahan M (Eds.) Handbook of the life course (pp. 3–19): Springer: Boston, MA. [Google Scholar]
- Glaser RR, Horn MLV, Arthur MW, Hawkins JD, & Catalano RF (2005). Measurement properties of the Communities That Care® Youth Survey across demographic groups. Journal of Quantitative Criminology, 21(1), 73–102. [Google Scholar]
- Hall S, Fildes J, Liyanarachchi D, Hicking V, Plummer J, & Tiller E (2020). Staying home: A youth survey report on young people’s experience of homelessness. Sydney, NSW: Mission Australia. [Google Scholar]
- Hawkins JD, Oesterle S, Brown EC, Abbott RD, & Catalano RF (2014). Youth problem behaviors 8 years after implementing the Communities That Care prevention system: A community-randomized trial. JAMA Pediatrics, 168(2), 122–129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heerde J, Bailey JA, Toumbourou JW, Rowland B, & Catalano R (2020). Longitudinal associations between early-mid adolescent risk and protective factors and young adult homelessness in Australia and the United States. Prevention Science, 21(4), 557–567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heerde JA, Hemphill SA, & Scholes-Balog KE (2014). ‘Fighting’ for survival: A systematic review of physically violent behavior perpetrated and experienced by homeless young people. Aggression and Violent Behavior, 19(1), 50–66. [Google Scholar]
- Heerde JA, & Patton GC (2020). The vulnerability of young homeless people. The Lancet Public Health, 5(e302-e303). [DOI] [PubMed] [Google Scholar]
- Heerde JA, Scholes-Balog KE, & Hemphill SA (2015). Associations between youth homelessness, sexual offenses, sexual victimization, and sexual risk behaviors: A systematic literature review. Archives of Sexual Behavior, 44(1), 181–212. [DOI] [PubMed] [Google Scholar]
- Hemphill SA, Heerde JA, Herrenkohl TI, Patton GC, Toumbourou JW, & Catalano RF (2011). Risk and protective factors for adolescent substance use in Washington State, the United States and Victoria, Australia: A longitudinal study. Journal of Adolescent Health, 49(3), 312–320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hser Y-I, Longshore D, & Anglin MD (2007). The life course perspective on drug use: A conceptual framework for understanding drug use trajectories. Evaluation Review, 31(6), 515–547. [DOI] [PubMed] [Google Scholar]
- Jessor R (2008). Description versus explanation in cross-national research on adolescence. Journal of Adolescent Health, 43(6), 527–528, doi: 10.1016/j.jadohealth.2008.09.010. [DOI] [PubMed] [Google Scholar]
- Jolliffe D, Farrington DP, Hawkins JD, Catalano RF, Hill KG, & Kosterman R (2003). Predictive, concurrent, prospective and retrospective validity of self-reported delinquency. Criminal Behaviour and Mental Health, 13(3), 179–197. [DOI] [PubMed] [Google Scholar]
- Kelly A, Mason W, Chmelka M, Herrenkohl T, Kim M, Patton G, et al. (2016). Depressed mood during early to middle adolescence: A bi-national longitudinal study of the unique impact of family conflict. Journal of Youth and Adolescence, 45(8), 1604–1613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelly AB, O’Flaherty M, Toumbourou JW, Homel R, Patton GC, White A, et al. (2012). The influence of families on early adolescent school connectedness: Evidence that this association varies with adolescent involvement in peer drinking networks. Journal of Abnormal Child Psychology, 40(3), 437–447. [DOI] [PubMed] [Google Scholar]
- Koegel P, Melamid E, & Burnam M (1995). Childhood risk factors for homelessness among homeless adults. American Journal of Public Health, 85(12), 1642–1649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McMorris B, Hemphill S, Toumbourou J, Catalano RF, & Patton GC (2007). Prevalence of substance use and delinquent behavior in adolescents from Victoria, Australia and Washington State, United States. Health Education & Behavior, 34(4), 634–650. [DOI] [PubMed] [Google Scholar]
- Morton M, Dworsky A, Matjasko J, Curry S, Schlueter D, Chávez R, et al. (2018). Prevalence and correlates of youth homelessness in the United States. Journal of Adolescent Health, 62(1), 14–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2017). Mplus Version 8 user’s guide. (8 ed.). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Patton GC, Olsson CA, Skirbekk V, Saffery R, Wlodek ME, Azzopardi PS, et al. (2018). Adolescence and the next generation. Nature, 554(7693), 458. [DOI] [PubMed] [Google Scholar]
- Patton GC, Sawyer SM, Santelli JS, Ross DA, Afifi R, Allen NB, et al. (2016). Our future: a Lancet commission on adolescent health and wellbeing. The Lancet, 387(10036), 2423–2478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sawyer SM, Afifi RA, Bearinger LH, Blakemore S-J, Dick B, Ezeh AC, et al. (2012). Adolescence: a foundation for future health. The Lancet, 379(9826), 1630–1640. [DOI] [PubMed] [Google Scholar]
- Schafer JL, & Graham JW (2002). Missing data: our view of the state of the art. Psychological Methods, 7(2), 147–177. [PubMed] [Google Scholar]
- Scholes-Balog K, Hemphill S, Heerde JA, Toumbourou JW, & Patton GC (2020). Childhood social environmental and behavioural predictors of early adolescent onset cannabis use. Drug & Alcohol Review, 399, 384–393, doi: 10.1111/dar.13077. [DOI] [PubMed] [Google Scholar]
- Segall MH, Lonner WJ, & Berry JW (1998). Cross-cultural psychology as a scholarly discipline: On the flowering of culture in behavioral research. American Psychologist, 53(10), 1101–1110. [Google Scholar]
- Shelton KH, Taylor PJ, Bonner A, & van den Bree M (2009). Risk factors for homelessness: evidence from a population-based study. Psychiatric Services, 60(4), 465–472. [DOI] [PubMed] [Google Scholar]
- StataCorp LLC (2017). Stata: Statistics/data analysis. (15:1 IC edition ed.). College Station, TX: StataCorp LLC. [Google Scholar]
- Statista (2020). Estimated number of homeless people in the United States from 2007 to 2020. https://www.statista.com/statistics/555795/estimated-number-of-homeless-people-in-the-us/2020.
- Toumbourou JW, Rowland B, Williams J, Smith R, & Patton GC (2019). Community intervention to prevent adolescent health behavior problems: Evaluation of communities that care in Australia. Health Psychology, 38(6), 536. [DOI] [PubMed] [Google Scholar]
- Tyler KA, & Bersani BE (2008). A longitudinal study of early adolescent precursors to running away. The Journal of Early Adolescence, 28(2), 230–251. [Google Scholar]
- van den Bree MB, Shelton K, Bonner A, Moss S, Thomas H, & Taylor PJ (2009). A longitudinal population-based study of factors in adolescence predicting homelessness in young adulthood. Journal of Adolescent Health, 45(6), 571–578. [DOI] [PubMed] [Google Scholar]
- Whitbeck LB, Hoyt DR, & Bao WN (2000). Depressive symptoms and co-occurring depressive symptoms, substance abuse, and conduct problems among runaway and homeless adolescents. Child Development, 71(3), 721–732. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.