

Abstract
Primary pulmonary artery sarcoma (PAS) is an extremely rare malignant disorder that presents like pulmonary thromboembolism (PE). Primary osteogenic sarcoma in the pulmonary artery (PA) is even rarer and can produce osteoid or cartilaginous matrix. Few studies have described the radiographic characteristics of osteosarcoma of the PA. We there report a case of a 78‐year‐old male patient with osteosarcoma in the PA where the patient went through surgical treatment after careful multimodalityimaging assessment. The patient was admitted to our hospital with the nonspecific symptom of heart failure. Multimodality imaging showed the primary lesion adhering to the arterial wall but without invading into surrounding tissues. PET/CT showed signs of hypometabolic activity within the lumen of the main PA. Cardiac MRI showed preserved left ventricular systolic function. CT showed distinctive features of PA osteosarcoma (a slightly hyperdense mass with calcification in pulmonary trunk).
Keywords: Pulmonary artery, Osteosarcoma, Dyspnoea, Magnetic resonance imaging, Computed tomography
Introduction
Pulmonary artery osteosarcoma, a subtype of pulmonary artery sarcoma (PAS), has been rarely reported, with a prevalence of about 4% in the literature. 1 Here, we present a case of a 78‐year‐old male patient admitted to our hospital due to progressive heart failure symptoms.
Case Report
A previously healthy 78‐year‐old male patient presented with progressive dyspnoea on exertion (New York Heart Association Class III), wheezing, and dry cough of 3 months duration. His physical examination demonstrated unremarkable results. Heart sounds were normal on cardiac auscultation except for a loud pulmonic component (P2) of the second heart sound. The majority of biochemical assays including BNP were normal, except for mildly increased fasting blood glucose concentration (6.40 mmol/mL, reference values <6.05) and slightly increased CA‐19‐9 in the serum (32.86 U/mL, reference values <31.3). The electrocardiography was normal. Transthoracic echocardiography at local hospital showed left ventricular mild diastolic dysfunction. Pulmonary thromboembolism (PTE) was highly suspected according to subsequent contrast‐enhanced chest computed tomography (CT) and PET/CT scan. After a 2 month anticoagulation therapy, the symptoms did not relieve, and the patient was readmitted to our hospital. Our CT scan (Figure 1 ) depicted a large filling defect (8.5 × 3 cm) in the main pulmonary artery with polyploid ossification, patchy ground‐glass opacification in the right middle and lower lobes. Cardiac MRI revealed right heart dilatation, left ventricular ejection fraction of 59%, right ventricular ejection fraction of 41%, and T2‐weighted dark blood sequence showed a slightly hyperintense soft tissue‐filled mass (Figure 2 ). Steady‐state free precession cine demonstrated a mass with beaded periphery distal to the pulmonic valve, moving with cardiac cycle and obstructing pulmonary trunk (Figure 3 , Supporting Information, Video S1 ). Post‐gadolinium delayed enhancement sequence showed peripheral hyperenhancement consistent with neoplasm (Figure 4 ). PET/CT showed hypometabolic activity in the pulmonary trunk without metastases in other organs, such as the liver and the lungs (Figure 5 ). Pulmonary angiography further revealed neovascularity in the mass (Figure 6 , Supporting Information, Video S2 ). The patient underwent surgery with pulmonary endarterectomy through median sternotomy and cardiopulmonary bypass. Pathologic examination revealed a pulmonary artery low‐grade osteosarcoma.
Figure 1.
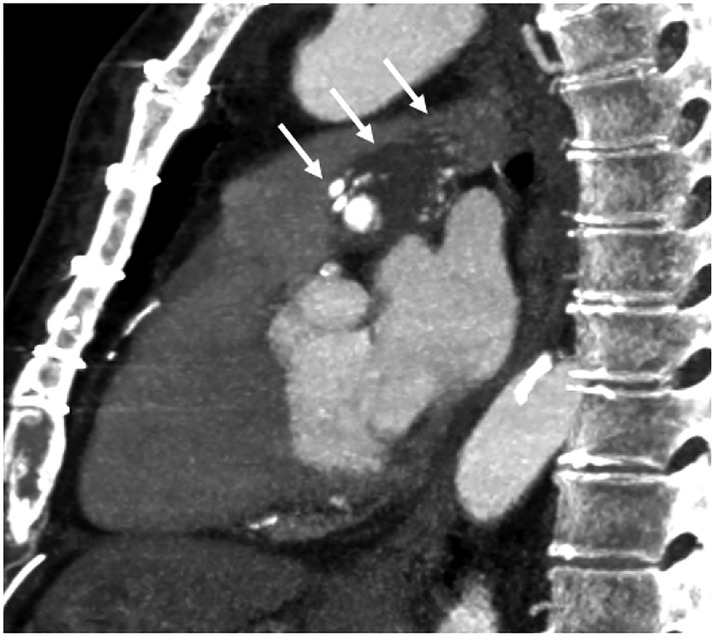
Contrast‐enhanced chest computed tomography scan.
Figure 2.
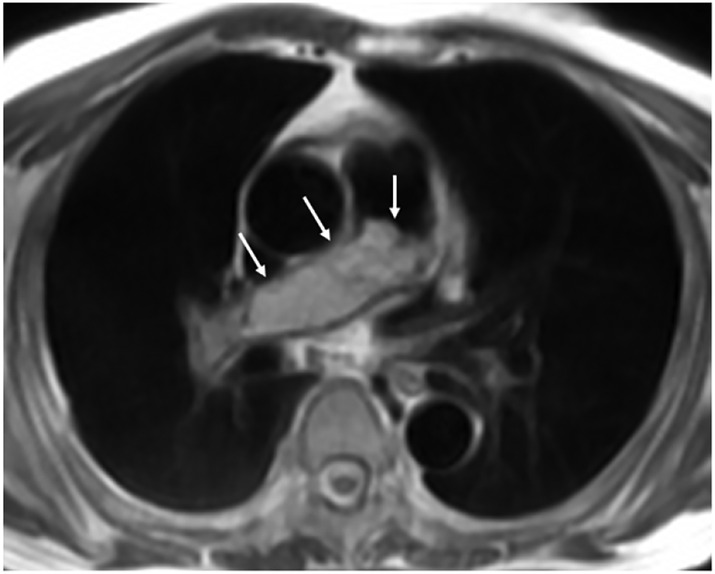
Dark‐blood T2‐weighted cardiac MR scan.
Figure 3.
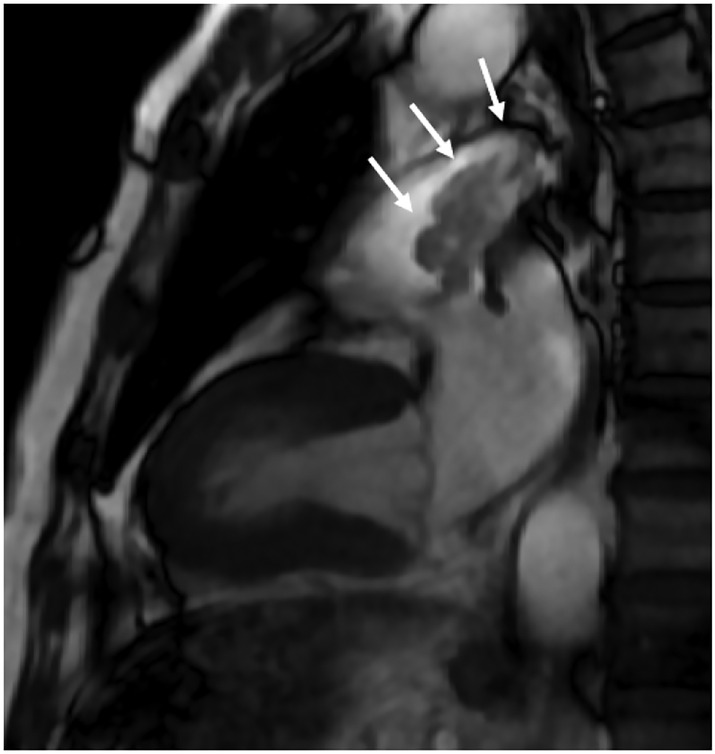
Steady‐state free‐precession (SSFP) cine cardiac MR scan.
Figure 4.
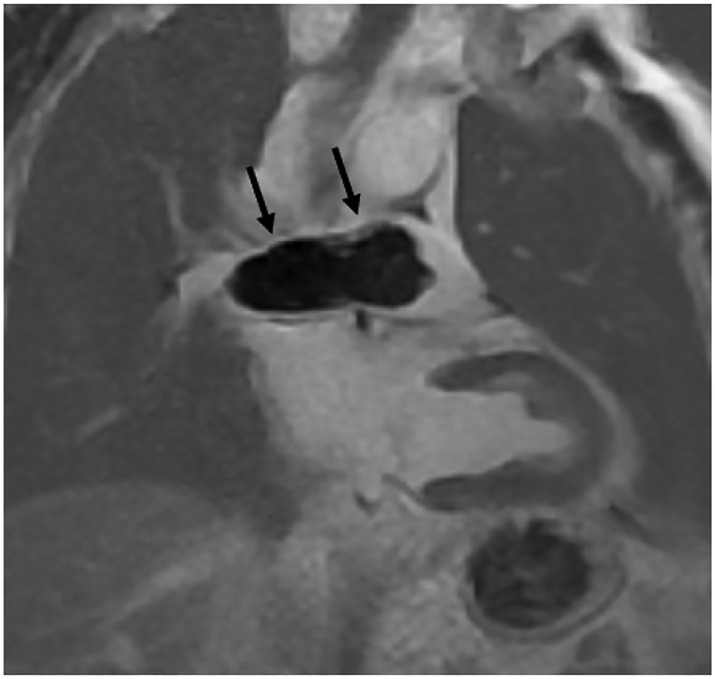
Delay enhancement cardiac MR scan by phase‐sensitive inversion recovery (PSIR) sequence.
Figure 5.

Whole‐body positron emission tomography (PET/CT).
Figure 6.
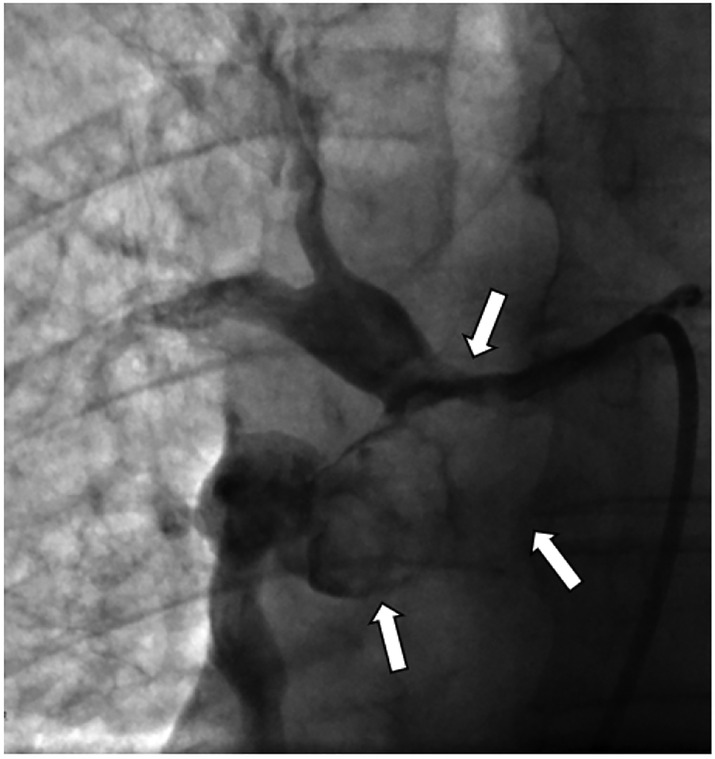
Pulmonary angiography.
Discussion
Different histological subtypes of pulmonary artery sarcoma (PAS) have been reported in the literature. To our knowledge, the current case of pulmonary artery osteosarcoma has not been reported in detail. 2 We found several imaging features of this subtype PAS, including ossification within the mass, acute angles between mass and the vessel wall, hypometabolic activity of FDG‐PET scan, and absence or occurrence of distant metastasis, all consistent with the low‐grade osteosarcoma. The clinical presentation of PAS is usually nonspecific, 3 and its radiologic appearances often lead to the misdiagnosis of PTE. 4 However, the treatments for both diseases are quite different. An accurate and timely diagnosis is often challenging. Aggressive surgery resection is the primary treatment for the localized lesion. The pathophysiology of PAS is unclear, but many predisposing risk factors are linked to the occurrence of PAS. 5 In this case, the pathogenic factor may be his professional exposure to vinyl chloride. 6 In the diagnosis of pulmonary artery osteosarcoma, multimodality imaging should be underscored to avoid inappropriate diagnosis and a delayed intervention. Clinicians should be aware of the key clinical and radiographic characteristics that differentiate this disease from PTE, because timely diagnosis coupled with surgical resection can improve the prognosis of the disease.
Conflict of interest
None declared.
Funding
This work was supported by grant No. 81930044 and No. 81620108015 from the key projects of National Natural Science Foundation of China.
Supporting information
Video S1. Supporting Information.
Video S2. Supporting Information.
Zheng, Y. , Duan, X. , Wang, H. , and Zhao, S. (2021) Pulmonary artery osteosarcoma masquerading as pulmonary thromboembolism: the role of multimodality imaging. ESC Heart Failure, 8: 5565–5567. 10.1002/ehf2.13625.
References
- 1. Buderi S, Theologou T, Gosney J, Shackcloth M. Pulmonary artery tumor embolism in a patient with previous fibroblastic osteosarcoma. Ann Thorac Surg 2013; 6: 2155–2157. [DOI] [PubMed] [Google Scholar]
- 2. Bandyopadhyay D, Panchabhai TS, Bajaj NS, Patil PD, Bunte MC. Primary pulmonary artery sarcoma: a close associate of pulmonary embolism‐20‐year observational analysis. J Thorac Dis 2016; 8: 2592–2601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Luo R, Xu H, Zhang P, Ye F, Wang F. Rare solitary fibrous tumor in the pulmonary artery mimicking pulmonary embolism. Circ Cardiovasc Imaging. 2017; 10: e005933. [DOI] [PubMed] [Google Scholar]
- 4. Rajaram S, Swift AJ, Davies C, Hill C, Jenkins D, Goddard M, Condliffe R, Elliot CA, Wild JM, Kiely DG. Primary pulmonary artery sarcoma and coexisting chronic thromboembolic pulmonary hypertension. Am J Respir Crit Care Med 2013; 188: e7–e8. [DOI] [PubMed] [Google Scholar]
- 5. Desmarais P, Laskine M, Caporuscio C. Primary pulmonary artery angiosarcoma mimicking pulmonary embolism in a 66‐year‐old man with dyspnea. CMAJ 2016; 188: E509–E512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Young RJ, Brown NJ, Reed MW, Hughes D, Woll PJ. Angiosarcoma. Lancet Oncol 2010; 11: 983–991. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Video S1. Supporting Information.
Video S2. Supporting Information.