

Abstract
Aims
We aimed to investigate whether sacubitril–valsartan could further improve the prognosis, cardiac function, and left ventricular (LV) remodelling in patients following acute myocardial infarction (AMI).
Methods and results
We searched the PubMed, Embase, Cochrane Library, and China National Knowledge Infrastructure (CNKI) from inception to 10 May 2021 to identify potential articles. Randomized controlled trials (RCTs) meeting the inclusion criteria were included and analysed. Thirteen RCTs, covering 1358 patients, were analysed. Compared with angiotensin‐converting enzyme inhibitors (ACEI)/angiotensin receptor blockers (ARB), sacubitril–valsartan did not significantly reduced the cardiovascular mortality [risk ratio (RR) 0.65, 95% confidence interval (CI) 0.22 to 1.93, P = 0.434] and the rate of myocardial reinfarction (RR 0.65, 95% CI 0.29 to 1.46, P = 0.295) of patients following AMI, but the rate of hospitalization for heart failure (HF) (RR 0.48, 95% CI 0.35 to 0.66, P < 0.001) and the change of LV ejection fraction (LVEF) [weighted mean difference (WMD) 5.49, 95% CI 3.62 to 7.36, P < 0.001] were obviously improved. The N‐terminal pro‐brain natriuretic peptide (NT‐ProBNP) level (WMD −310.23, 95% CI −385.89 to −234.57, P < 0.001) and the LV end‐diastolic dimension (LVEDD) (WMD −3.16, 95% CI −4.59 to −1.73, P < 0.001) were also significantly lower in sacubitril–valsartan group than in ACEI/ARB group. Regarding safety, sacubitril–valsartan did not increase the risk of hypotension, hyperkalaemia, angioedema, and cough.
Conclusions
This meta‐analysis suggests that early administration of sacubitril–valsartan may be superior to conventional ACEI/ARB to decrease the risk of hospitalization for HF, improve the cardiac function, and reverse the LV remodelling in patients following AMI.
Keywords: Sacubitril–valsartan, Angiotensin‐converting enzyme inhibitors, Angiotensin receptor blockers, Heart failure, Acute myocardial infarction, Meta‐analysis
Introduction
Acute myocardial infarction (AMI) is a common and severe type of coronary heart disease with high morbidity and mortality. Although primary percutaneous coronary intervention (pPCI) has been widely performed in patients with AMI to reduce infarct size and preserve ventricular function, almost 25% AMI patients would develop into heart failure (HF). 1 Substantial evidences indicated that β blockers, 2 angiotensin‐converting enzyme inhibitors (ACEI)/angiotensin receptor blockers (ARB), 3 , 4 and mineralocorticoid‐receptor antagonists (MRA) 5 could effectively attenuate the left ventricular (LV) remodelling and reduce the risk of death of AMI patients. However, their risk of re‐hospitalization for HF and mortality remain high. 6
Neuroendocrine hormones activation including the renin angiotensin aldosterone system (RASS) and sympathetic nervous system (SNS) play an important role in the progression of LV remodelling and HF occurrence after AMI. 7 , 8 Therefore, besides timely revascularization, regulating neuroendocrine hormone balance is another pivotal way to improving their prognosis. In addition to blocking the RASS, sacubitril–valsartan is also focused on inhibiting the activity of neprilysin and decreasing the degradation of natriuretic peptides to further counteract the adverse effects of RASS and SNS activation by promoting vasodilation, natriuresis, and diuresis, along with inhibiting myocardial fibrosis and hypertrophy. 9 , 10
Recently, several clinical trials compared the benefits of sacubitril–valsartan and ACEI/ARB in patients following AMI and identified that sacubitril–valsartan could further improve the LV ejection fraction (LVEF) and significantly reduce the major adverse cardiac events (MACE), HF re‐hospitalization risk, as well as LV dimensions. 6 , 11 , 12 However, Docherty et al. 13 found that in comparison with valsartan, sacubitril–valsartan neither effectively improved the LVEF nor significantly reduced the N‐terminal pro‐brain natriuretic peptide (NT‐ProBNP) level, LV volume, and LV mass index in this kind of patients. Hence, compared with ACEI/ARB, the benefits of sacubitril–valsartan in patients following AMI are still controversial. For this purpose, we performed a meta‐analysis to investigate whether sacubitril–valsartan could bring more clinical benefits for patients following AMI than ACEI/ARB drugs.
Methods
This meta‐analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) guidelines. 14
Search strategy and study selection
Literatures were searched in PubMed, Embase, Cochrane Library, and China National Knowledge Infrastructure (CNKI) without any restrictions from inception to 10 May 2021. The search strategy included the following MeSH headings or keywords: angiotensin‐receptor neprilysin inhibitor, sacubitril–valsartan, LCZ696, MI, and AMI (Supporting Information, Table S1 ). Moreover, we manually checked the reference list of retrieved articles to identify the potentially relevant studies. Studies were included if they met the following criteria: (i) randomized controlled trials (RCTs); (ii) adult (age > 18 years) patients following AMI were treated with sacubitril–valsartan vs. ACEI/ARB; and (iii) studies reported the primary or secondary outcomes.
Data extraction and quality assessment
Data extraction was performed by two independent reviewers with discrepancies resolved by discussion. The following data were extracted from each included study: basic characteristics of studies (authors, publication year, journal, country, study design), characteristics of patients (sample size, gender, age, type of MI, time of pPCI, LVEF, medical history), sacubitril–valsartan and ACEI/ARB treatments (initial time, dosage, frequency, duration, mean follow‐up time), primary outcomes (cardiovascular mortality, rate of myocardial reinfarction, rate of hospitalization for HF), and secondary outcomes [NT‐ProBNP level, change of LVEF, change of 6 min walk test (6MWT) distance, change of left ventricular end‐diastolic dimension (LVEDD), and incidence of side effects including hypotension, hyperkalaemia, angioedema, and cough]. The risk of bias of included studies was evaluated by RoB2 tool from Cochrane. 15
Statistical analysis
Statistical methods according to our previous study were used with STATA 14.0 (Stata Corp, College Station, Texas). 16 Heterogeneity was evaluated using I 2 test (0–40%: not important; 30–60%: moderate heterogeneity; 50–90%: substantial heterogeneity; 75–100%: considerable heterogeneity). Risk ratio (RR) and 95% confidence interval (CI) were calculated for cardiovascular mortality, rate of myocardial reinfarction, rate of hospitalization for HF, and incidence of side effects with fixed effect model, if there was no significant heterogeneity. Otherwise, a random effect model was used. Weighted mean difference (WMD) and 95% CI were calculated for NT‐ProBNP level, and changes of LVEF, 6MWT distance, as well as LVEDD with fixed effect model, when there was no significant heterogeneity. Otherwise, a random effect model was used. In addition, sensitivity analysis, funnel plots, and Egger's test were used to assess the stability of estimates and the publication bias, respectively. The P value < 0.05 is considered significant.
Results
Study characteristics
The literature research and selection are shown in Figure 1 . A total of 234 articles were acquired. A total of 212 articles were excluded by title and abstract screening and 22 articles were involved in full text evaluation. Seven articles were excluded for duplication, cohort study, or not reporting associated outcomes and 13 RCTs were finally included in our meta‐analysis. 6 , 11 , 12 , 13 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 The baseline characteristics of included RCTs are summarized in Table 1 . Generally, the 13 RCTs with a total of 1358 patients were published between 2019 and 2021. The baseline characteristics, such as sample size, mean age, and sex ratio of each study, were not significantly different between the two groups. The mean follow‐up duration ranged from 1 to 13 months. The risk of bias analysis indicated that one study was high risk, six studies were some concerns, and six studies were low risk (Figure S1 ).
Figure 1.
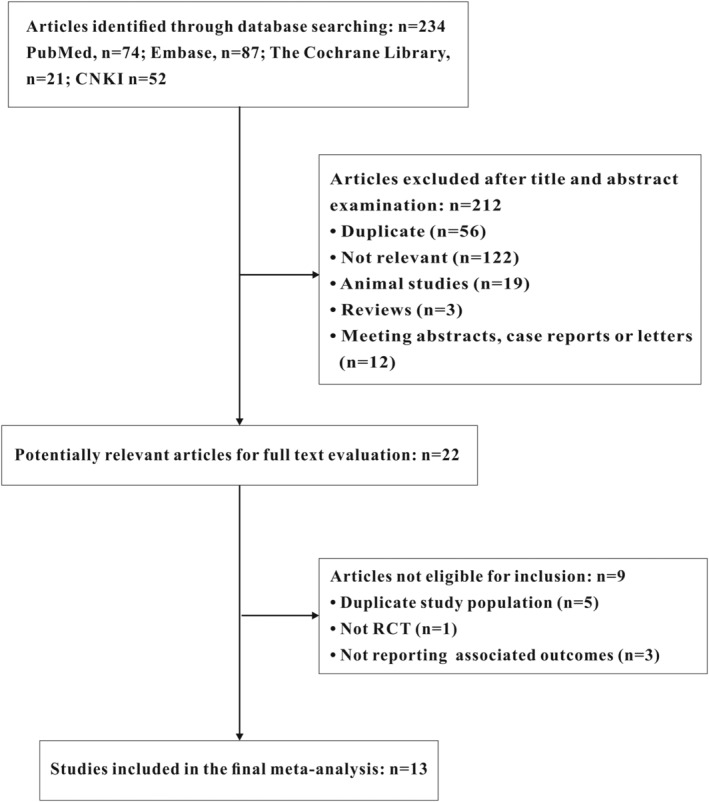
Study selection. CNKI, China National Knowledge Infrastructure; RCT, randomized controlled trial.
Table 1.
Baseline characteristics of included studies
| Study | Type of MI | Sample size | Age (years, mean ± SD) | Male/female | Drugs | Follow‐up (months) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ARNI | Control | ARNI | Control | ARNI | Control | Initial time | ARNI | Control | |||
| Chen C et al., 2019 17 | AMI | 26 | 26 | 56.3 ± 10.1 | 55.7 ± 9.7 | 15/11 | 14/12 | In 2 weeks after AMI | Sacubitril/valsartan 200 mg, bid | Enalapril 5 mg, qd | 6 |
| Zhang et al., 2020 12 | STEMI | 79 | 77 | 60.3 ± 11.7 | 60.0 ± 10.9 | 59/20 | 55/22 | In 24 h after pPCI | Sacubitril/valsartan, MTD | Perindopril, MTD | 6 |
| Wang et al., 2020 6 | STEMI | 68 | 69 | 59.1 ± 7.2 | 60.6 ± 7.6 | 52/16 | 54/15 | After pPCI | Sacubitril/valsartan 100 mg, bid | Enalapril 5 mg, bid | 6 |
| Dong et al., 2020 18 | STEMI | 40 | 40 | 63.9 ± 8.2 | 62.0 ± 7.6 | 23/17 | 26/14 | After pPCI | Sacubitril/valsartan 200 mg, bid | Valsartan 80 mg, qd | 6 |
| Rezq et al., 2020 11 | STEMI | 100 | 100 | 52.0 ± 9.2 | 57.0 ± 11.6 | 86/14 | 88/12 | After pPCI | Sacubitril/valsartan 100 mg, bid | Ramipril 5 mg, bid | 6 |
| Li et al., 2020 19 | AMI | 50 | 50 | 54.4 ± 6.0 | 54.9 ± 6.1 | 28/22 | 27/23 | After pPCI | Sacubitril/valsartan 200 mg, bid | Enalapril 10 mg, bid | 6 |
| Yang et al., 2020 20 | AMI | 42 | 45 | 67.2 ± 4.2 | 67.6 ± 3.8 | 25/17 | 26/19 | NA | Sacubitril/valsartan 100 mg, bid | Valsartan 80 mg, qd | 12 |
| Xiong et al., 2020 21 | AMI | 75 | 71 | 59.0 ± 8.0 | 61.0 ± 9.0 | 55/16 | 46/29 | 1 month after AMI | Sacubitril/valsartan 200 mg, bid | Valsartan 80 mg, qd | 12 |
| Chen H et al., 2020 22 | AMI | 30 | 30 | 55.4 ± 10.1 | 54.6 ± 10.3 | 15/15 | 15/15 | After pPCI | Sacubitril/valsartan, MTD | Enalapril, MTD | 6 |
| Chen L et al., 2021 23 | AMI | 31 | 30 | 56.3 ± 10.1 | 55.7 ± 9.7 | 16/15 | 17/13 | After pPCI | Sacubitril/valsartan 50 mg, bid | Enalapril 5 mg, qd | 1 |
| Chen M et al., 2021 24 | AMI | 48 | 48 | 59.9 ± 13.2 | 60.0 ± 11.7 | 31/17 | 30/18 | NA | Sacubitril/valsartan 200 mg, bid | Benazepril 10 mg, qd | 3 |
| Zhao et al., 2021 25 | AMI | 45 | 45 | 62.8 ± 3.9 | 62.7 ± 6.1 | 25/20 | 27/18 | In 24 h after pPCI | Sacubitril/valsartan 50 mg, bid | Valsartan 80 mg, qd | 3 |
| Docherty et al., 2021 13 | AMI | 47 | 46 | 61.8 ± 10.6 | 59.7 ± 10.1 | 42/5 | 43/3 | 3 months after AMI | Sacubitril/valsartan 200 mg, bid | Valsartan 160 mg bid | 13 |
AMI, acute myocardial infarction; ARNI, angiotensin receptor–neprilysin inhibitor; MTD, maximum tolerated dose; NA, not available; pPCI, primary percutaneous coronary intervention; SD, standard deviation; STEMI, ST segment elevation myocardial infarction.
Primary outcomes
Three studies with a total of 424 patients reported the cardiovascular mortality. No significant heterogeneity was found (I 2 = 0%) and fixed effect model was used. In comparison with ACEI/ARB, the cardiovascular mortality was not significantly improved by sacubitril–valsartan in AMI patients (RR 0.65, 95% CI 0.22 to 1.93, P = 0.434; Figure 2 ). In addition, the rates of myocardial reinfarction (I 2 = 0%) and hospitalization for HF (I 2 = 0%) were investigated in 5 RCTs including 469 and 660 patients, respectively, without significant heterogeneity. The results indicated that compared with ACEI/ARB, sacubitril–valsartan did not significantly lower the rate of myocardial reinfarction (RR 0.65, 95% CI 0.29 to 1.46, P = 0.295; Figure 2 ); the rate of hospitalization for HF (RR 0.48, 95% CI 0.35 to 0.66, P < 0.001; Figure 2 ) was obviously lower in sacubitril–valsartan group than in ACEI/ARB group. In addition, subgroup analysis suggested that sacubitril–valsartan was superior to both ACEI and ARB for decreasing the rate of hospitalization for HF (Figure S2 ).
Figure 2.
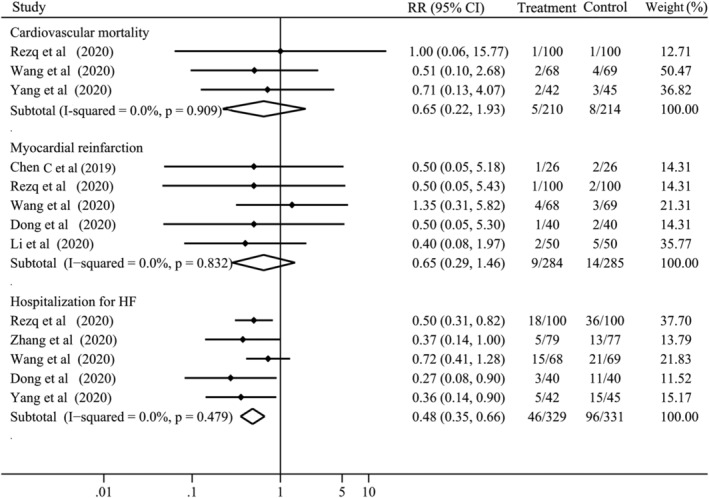
Risks of cardiovascular mortality, myocardial reinfarction, and hospitalization for HF with sacubitril–valsartan vs. angiotensin‐converting enzyme inhibitors/angiotensin receptor blockers. CI, confidence interval; HF, heart failure; RR, risk ratio.
Secondary outcomes
Eleven studies with 1001 patients compared the NT‐ProBNP level at the time of last visit between the two groups. There was considerable heterogeneity (I 2 = 96.7%) and random effect model was used for analysis. The NT‐ProBNP level was significantly lower in sacubitril–valsartan group than in ACEI/ARB group (WMD −310.23, 95% CI −385.89 to −234.57, P < 0.001; Figure 3 ), and this effect was always observed in the subgroup analysis of ACEI and ARB (Figure S3 ). Moreover, the improvement of 6MWT distance was evaluated in 3 studies including 288 patients with considerable heterogeneity (I 2 = 99.8%). Compared with ACEI/ARB, sacubitril–valsartan was inclined to effectively improve the 6MWT distance in patients following AMI, but no significant difference was observed (WMD 73.44, 95% CI −25.81 to 172.69, P = 0.147; Figure 4 ).
Figure 3.
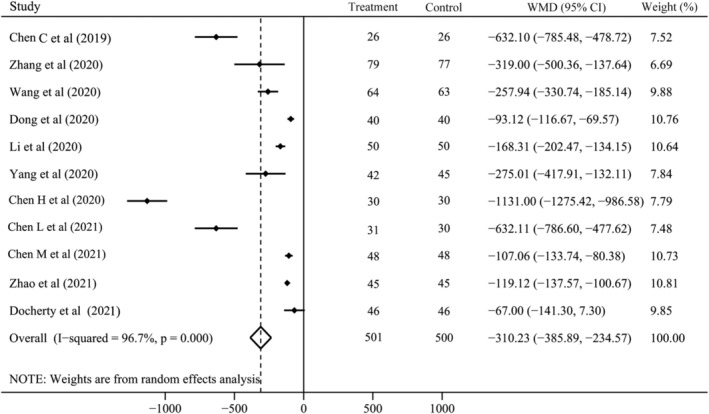
N‐terminal pro‐brain natriuretic peptide with sacubitril–valsartan vs. angiotensin‐converting enzyme inhibitors/angiotensin receptor blockers. CI, confidence interval; WMD, weighted mean difference.
Figure 4.
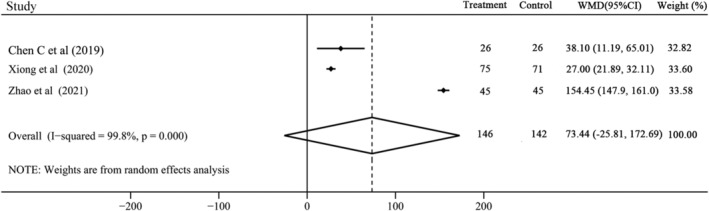
The change of 6 min walk test distance with sacubitril–valsartan vs. angiotensin‐converting enzyme inhibitors/angiotensin receptor blockers. CI, confidence interval; WMD, weighted mean difference.
There were 11 RCTs with 1043 patients and 7 RCTs with 636 patients reported the changes of LVEF and LVEDD, respectively. Both of them had considerable heterogeneity (LVEF: I 2 = 99.8%; LVEF: I 2 = 99.6%) and random effect model was used. Our results showed that sacubitril–valsartan significantly increased the LVEF (WMD 5.49, 95% CI 3.62 to 7.36, P < 0.001; Figure 5 ) and reversed the LVEDD (WMD −3.16, 95% CI −4.59 to −1.73, P < 0.001; Figure 6 ). Subgroup analysis indicated that either compared with ACEI or ARB, sacubitril–valsartan could invariably improve the LVEF (Figure S4 ) and LVEDD (Figure S5 ).
Figure 5.
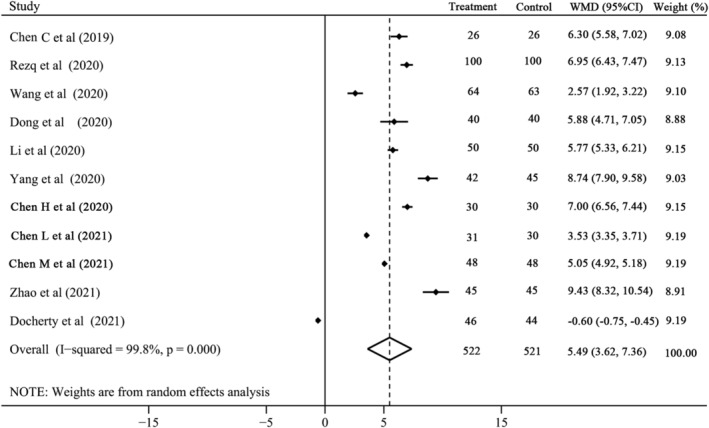
The change of left ventricular ejection fraction with sacubitril–valsartan vs. angiotensin‐converting enzyme inhibitors/angiotensin receptor blockers. CI, confidence interval; WMD, weighted mean difference.
Figure 6.
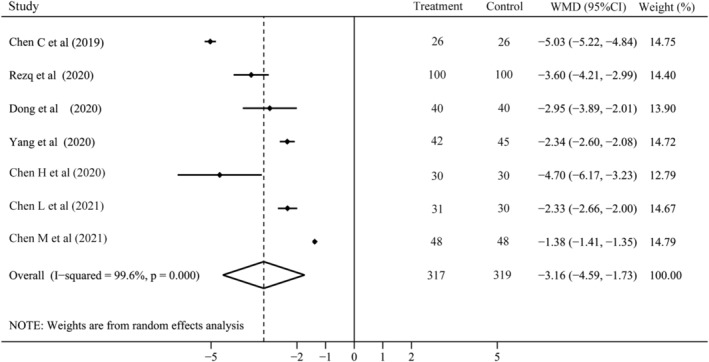
The change of left ventricular end‐diastolic dimension with sacubitril–valsartan vs. angiotensin‐converting enzyme inhibitors/angiotensin receptor blockers. CI, confidence interval; WMD, weighted mean difference.
With regard to the safety, we analysed the most common side effects of sacubitril–valsartan and ACEI/ARB including hypotension (5 RCTs with 439 patients), hyperkalaemia (4 RCTs with 378 patients), angioedema (2 RCTs with 148 patients), and cough (2 RCTs with 198 patients). Except hypotension with moderate heterogeneity, none of them had significant heterogeneity and fixed effect model was used. The incidences of hypotension (RR 1.24, 95% CI 0.74 to 2.08, P = 0.421; Figure S6 ), hyperkalaemia (RR 0.85, 95% CI 0.28 to 2.62, P = 0.783; Figure S6 ), angioedema (RR 0.67, 95% CI 0.12 to 3.85, P = 0.650; Figure S6 ), and cough (RR 0.60, 95% CI 0.15 to 2.41, P = 0.468; Figure S6 ) were all similar between sacubitril–valsartan and ACEI/ARB groups.
Publication bias and sensitivity analysis
We evaluated the publication bias of the rate of myocardial reinfarction, the rate of hospitalization for HF, the NT‐ProBNP, the change of LVEF, the change of LVEDD, and the incidence of hypotension. The funnel plots of all were not symmetric (Figure S7 ), but Egger's test indicated that publication bias was only observed in the NT‐ProBNP (P = 0.009) and there were no significant publication bias in the rate of hospitalization for HF (P = 0.211), the change of LVEF (P = 0.232), the change of LVEDD (P = 0.132), and the incidence of hypotension (P = 0.749). To test the stability of our results, we performed sensitivity analyses for all outcomes and the results indicated that all estimates were stable (Table S2 ).
Discussion
Our meta‐analysis demonstrated that compared with conventional ACEI/ARB, early administration of sacubitril–valsartan neither significantly improved the cardiovascular mortality and the rate of myocardial reinfarction nor increased the 6MWT distance in patients following AMI. But it was able to reduce the rate of hospitalization for HF and NT‐ProBNP level, improve the LVEF, and alleviate the LV remodelling. Moreover, the risk of side effects, including hypotension, hyperkalaemia, angioedema, and cough, was similar between sacubitril–valsartan and ACEI/ARB groups.
Substantial myocardial cells necrosis could decrease myocardial contractility and cardiac output, and compensatory activate several neurohormone pathways including RASS and SNS, which is beneficial to maintain haemodynamic stability in the short term. 6 , 26 However, RASS and SNS long‐term activation could increase cardiac volume and pressure loads, enhance myocardial oxygen consumption, facilitate cardiomyocyte hypertrophy, and finally result in LV remodelling. On the contrary, the natriuretic peptide system, as an important compensation pathway for HF, not only had vasodilatory and diuretic effects but also could suppress the RASS and SNS to facilitate myocardial relaxation and reverse cardiac remodelling. 27 Therefore, suppressing the RAAS and SNS pathways, and augmenting the natriuretic peptide system, may be a promising strategy for the management of patients following AMI, especially, in patients with LV dysfunction or at high risk of developing HF.
Similar with ACEI/ARB, which is able to inhibit RASS, sacubitril–valsartan is also to suppress neprilysin to prevent the degradation of ANP and BNP and elevate the activity of natriuretic peptide system. Several studies have proved that sacubitril–valsartan was a more effective alternative than ACEI/ARB to improve the clinical outcomes of HF with reduced ejection fraction (HFrEF). 28 , 29 But whether early administration of sacubitril–valsartan in patients following AMI could bring more benefits is still unclear. In accordance with most included RCTs, our meta‐analysis found that in comparison with ACEI/ARB, sacubitril–valsartan could significantly decrease the rate of hospitalization for HF, but not cardiovascular mortality and myocardial reinfarction. In fact, for patients following AMI, timely reperfusion, standard antiplatelet, and lipid lowering therapies may be a more pivotal management for lowering the risk factors of coronary heart disease and decreasing the occurrence of myocardial events and reinfarction. 11
The 6MWT distance is an important indicator for the evaluation of cardiac function. In our meta‐analysis, sacubitril–valsartan was inclined to increase the 6MWT distance, but there was no significant difference. Actually, the 6MWT distance from each included RCTs was effectively improved by sacubitril–valsartan. 17 , 21 , 25 The limited sample size and study numbers may decrease the power of our meta‐analysis. NT‐ProBNP is not degraded by neprilysin, and hence, the dynamic levels of NT‐ProBNP could reflect the reduction of LV wall stress in patients treated with sacubitril–valsartan. As with most RCTs, NT‐ProBNP was significantly reduced by sacubitril–valsartan in this meta‐analysis. However, Docherty et al. 13 did not find this difference. It was noteworthy that the initial time of sacubitril–valsartan treatment in this study was 3 months after AMI, and before sacubitril–valsartan administration, the early therapies have made a rapid reduction in NT‐ProBNP to the almost normal level (baseline: 213 pg/mL vs. 242 pg/mL). Therefore, it is hard to further decrease the NT‐ProBNP from the aforementioned baseline by sacubitril–valsartan. In addition, the considerable heterogeneity for NT‐ProBNP and 6MWT may be also partly attributed to the significant variations of baseline cardiac function and sacubitril–valsartan doses of participants in each included RCT.
As the key clinical markers for cardiac function and LV remodelling, both the LVEF and LVEDD were obviously improved by sacubitril–valsartan, but considerable heterogeneity was observed. The heterogeneity may result from the different measuring methods for LVEF and LVEDD. Most RCTs used transthoracic echocardiography; however, the Docherty et al. study used cardiac magnetic resonance imaging (MRI), which is more accurate to assess the cardiac function. Data from the Docherty et al. study 13 suggested that sacubitril–valsartan neither increased LVEF (36.9% vs. 39.1%) nor reduced the left ventricular end‐diastolic volume index (LVEDVI, 111.0 mL/m2 vs. 118.1 mL/m2). As we all known, the cardiac remodelling started at the early stage of AMI and myocardial fibrosis was completed in a few months. 30 Therefore, to inhibit the LV remodelling preferably, sacubitril–valsartan or ACEI/ARB should be used as soon as possible. The initial time of sacubitril–valsartan administration in most included RCTs was in 24 h after the pPCI, except for the Docherty et al. study in which was 3 months after AMI. Hence, the discrepancy between this meta‐analysis and the Docherty et al. study may be mainly attributed to the initial time difference of sacubitril–valsartan use.
With regard to the safety of sacubitril–valsartan, previous studies demonstrated that hypotension was more frequently appeared in patients receiving sacubitril–valsartan. Data from PARAGON‐HF suggested that the mean systolic blood pressure was approximately 5 mmHg lower in sacubitril–valsartan than in valsartan. 31 However, in our meta‐analysis, the incidences of hypotension, hyperkalaemia, angioedema, and cough were similar between sacubitril–valsartan and ACEI/ARB groups. But, due to the limited study numbers, these results about side effects should be interpreted prudently.
There were several limitations in this meta‐analysis. First, the sample size of most included RCTs was small and may make our estimates at risk of bias. Second, about sacubitril–valsartan administration, the initial time, dosage, and duration were variable in each included RCT, which might produce confound bias for the evaluation. Third, Egger's test indicated that publication bias was observed in the NT‐ProBNP, and hence, it should be interpreted prudently. Fourth, the different type and dosage of ACEI/ARB in each study might also influence the accuracy of our estimates. Lastly, the cardiac function of participants in included RCTs was significant variation; this may influence the benefit evaluation. Carefully selecting patients at higher risk of developing HF, or even with early signs of LV dysfunction, may increase the benefits of sacubitril–valsartan for AMI patients.
Conclusions
In summary, this meta‐analysis suggests that early administration of sacubitril–valsartan may be superior to conventional ACEI/ARB to decrease the risk of hospitalization for HF, improve the cardiac function, and reverse the LV remodelling in AMI patients. In the future, PARADISE‐MI study, 32 a well‐designed RCT with large sample size, will confirm our findings and further investigate whether sacubitril–valsartan could improve the long‐term prognosis of patients following AMI.
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
This work was funded by the National Natural Science Foundation of China (No. 81900361).
Supporting information
Table S1. Search strategies of PubMed and the Cochrane Library.
Table S2. Results of sensitivity analysis of all outcomes.
Table S3. DOI number of included Chinese studies.
Figure S1. Risk of bias of included RCTs by RoB2 tool from Cochrane.
Figure S2. The subgroup analysis of hospitalization for HF based on the use of ACEI or ARB in control group. ACEI, angiotensin‐converting enzyme inhibitors; ARB, angiotensin receptor blockers; CI, confidence interval; HF, heart failure; RR, risk ratio.
Figure S3. The subgroup analysis of the NT‐ProBNP based on the use of ACEI or ARB in control group. ACEI, angiotensin‐converting enzyme inhibitors; ARB, angiotensin receptor blockers; CI, confidence interval; WMD, weighted mean difference.
Figure S4. The subgroup analysis of the change of LVEF based on the use of ACEI or ARB in control group. ACEI, angiotensin‐converting enzyme inhibitors; ARB, angiotensin receptor blockers; CI, confidence interval; LVEF, left ventricular ejection fraction; WMD, weighted mean difference.
Figure S5. The subgroup analysis of the change of LVEDD based on the use of ACEI or ARB in control group. ACEI, angiotensin‐converting enzyme inhibitors; ARB, angiotensin receptor blockers; CI, confidence interval; LVEDD, left ventricular end‐diastolic dimension; WMD, weighted mean difference.
Figure S6. The incidence of side effects with sacubitril–valsartan vs. ACEI/ARB. CI, confidence interval; RR, risk ratio.
Figure S7. Funnel plots of the rate of myocardial reinfarction (A), the rate of hospitalization for heart failure (B), the change of LVEF (C), the change of LVEDD (D), the level of NT‐ProBNP (E), the incidence of hypotension (F). LVEF, left ventricular ejection fraction; LVEDD, left ventricular end‐diastolic dimension.
Acknowledgements
We acknowledge all the original authors of the included studies for their excellent work.
Xiong, B. , Nie, D. , Qian, J. , Yao, Y. , Yang, G. , Rong, S. , Zhu, Q. , Du, Y. , Jiang, Y. , and Huang, J. (2021) The benefits of sacubitril–valsartan in patients with acute myocardial infarction: a systematic review and meta‐analysis. ESC Heart Failure, 8: 4852–4862. 10.1002/ehf2.13677.
References
- 1. Kaul P, Ezekowitz JA, Armstrong PW, Leung BK, Savu A, Welsh RC, Quan H, Knudtson ML, McAlister FA. Incidence of heart failure and mortality after acute coronary syndromes. Am Heart J 2013; 165: 379–385.e372. [DOI] [PubMed] [Google Scholar]
- 2. Doughty RN, Whalley GA, Walsh HA, Gamble GD, López‐Sendón J, Sharpe N. Effects of carvedilol on left ventricular remodeling after acute myocardial infarction: the CAPRICORN Echo Substudy. Circulation 2004; 109: 201–206. [DOI] [PubMed] [Google Scholar]
- 3. Investigators TAIREAS . Effect of ramipril on mortality and morbidity of survivors of acute myocardial infarction with clinical evidence of heart failure. The Acute Infarction Ramipril Efficacy (AIRE) Study Investigators. Lancet 1993; 342: 821–828. [PubMed] [Google Scholar]
- 4. Pfeffer MA, McMurray JJ, Velazquez EJ, Rouleau JL, Køber L, Maggioni AP, Solomon SD, Swedberg K, Van de Werf F, White H, Leimberger JD, Henis M, Edwards S, Zelenkofske S, Sellers MA, Califf RM. Valsartan, captopril, or both in myocardial infarction complicated by heart failure, left ventricular dysfunction, or both. N Engl J Med 2003; 349: 1893–1906. [DOI] [PubMed] [Google Scholar]
- 5. Pitt B, Remme W, Zannad F, Neaton J, Martinez F, Roniker B, Bittman R, Hurley S, Kleiman J, Gatlin M. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 2003; 348: 1309–1321. [DOI] [PubMed] [Google Scholar]
- 6. Wang H, Fu X. Effects of sacubitril/valsartan on ventricular remodeling in patents with left ventricular systolic dysfunction following acute anterior wall myocardial infarction. Coron Artery Dis 2021; 32: 418–426. [DOI] [PubMed] [Google Scholar]
- 7. Sigurdsson A, Held P, Swedberg K, Wall B. Neurohormonal effects of early treatment with enalapril after acute myocardial infarction and the impact on left ventricular remodelling. Eur Heart J 1993; 14: 1110–1117. [DOI] [PubMed] [Google Scholar]
- 8. Grosman‐Rimon L, Billia F, Wright E, Carasso S, Elbaz‐Greener G, Kachel E, Rao V, Cherney D. Neurohormones, inflammatory mediators, and cardiovascular injury in the setting of heart failure. Heart Fail Rev 2020; 25: 685–701. [DOI] [PubMed] [Google Scholar]
- 9. Jhund PS, McMurray JJV. The neprilysin pathway in heart failure: a review and guide on the use of sacubitril/valsartan. Heart 2016; 102: 1342–1347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Campbell DJ. Long‐term neprilysin inhibition—implications for ARNIs. Nat Rev Cardiol 2017; 14: 171–186. [DOI] [PubMed] [Google Scholar]
- 11. Rezq A, Saad M, El Nozahi M. Comparison of the efficacy and safety of sacubitril/valsartan versus ramipril in patients with ST‐segment elevation myocardial infarction. Am J Cardiol 2021; 143: 7–13. [DOI] [PubMed] [Google Scholar]
- 12. Zhang Y, Wu Y, Zhang K, Ke Z, Hu P, Jin D. Benefits of early administration of Sacubitril/Valsartan in patients with ST‐elevation myocardial infarction after primary percutaneous coronary intervention. Coron Artery Dis 2021; 32: 427–431. [DOI] [PubMed] [Google Scholar]
- 13. Docherty KF, Campbell RT, Brooksbank KJM, Dreisbach JG, Forsyth P, Godeseth RL, Hopkins T, Jackson AM, Lee MMY, McConnachie A, Roditi G, Squire IB, Stanley B, Welsh P, Jhund PS, Petrie MC, Mcmurray JJV. The effect of neprilysin inhibition on left ventricular remodeling in patients with asymptomatic left ventricular systolic dysfunction late after myocardial infarction. Circulation 2021. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA. Preferred Reporting Items for Systematic Review and Meta‐Analysis Protocols (PRISMA‐P) 2015 statement. Syst Rev 2015; 4: 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge SM, Emberson JR, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 2019; 366: l4898. [DOI] [PubMed] [Google Scholar]
- 16. Xiong B, Huang Y, Tan J, Yao Y, Wang C, Qian J, Rong S, Deng S, Cao Y, Zou Y, Huang J. The short‐term and long‐term effects of tolvaptan in patients with heart failure: a meta‐analysis of randomized controlled trials. Heart Fail Rev 2015; 20: 633–642. [DOI] [PubMed] [Google Scholar]
- 17. Chen C, Qian W, Ding H, Zhou H, Wang W. Effect of sacubitril/valsartan on the short‐term prognosis of patients with acute anterior wall myocardial infarction complicated with cardiac insufficiency after emergency PCI. Progress Modern Biomed 2019; 19: 3720–3725. [Google Scholar]
- 18. Dong Y, Du Q, Yang L, Wang W. Effect of sacubitril/valsartan on patients with acute ST‐segment elevation myocardial infarction and heart failure after emergency percutaneous coronary intervention. Clin J Med Offic 2020; 48: 1248–1252. [Google Scholar]
- 19. Li J, Chen X, Chai Q, Zhang W, Han J, Fang J, Le F. Effect of sacubitril/valsartan on cardiac function after emergency percutaneous coronary intervention in patients with acute myocardial infarction. Chinese J Clin Res 2020; 33: 1200–1203. [Google Scholar]
- 20. Yang H, Sun X, Liu J, Yuan Y, Yang Z. Effect of sacubitril/valsartan for alleviating chronic heart failure in elderly patients after acute myocardial infarction. Chin J Geriat 2020; 39: 38–42. [Google Scholar]
- 21. Xiong Z, Man W, Li Y, Guo W, Wang H, Sun D. Comparison of effects of sacubitril/valsartan versus valsartan on post AMI heart failure. Chin Heart J 2020; 32: 28–32. [Google Scholar]
- 22. Chen H, Li J, Han J, Zhang W, Liu C, Li J. Curative effect of sacubitril/valsartan combined with emergency PCI on acute myocardial infarction complicated by cardiac insufficiency. Chin J Evid Based Cardiovasc Med 2020; 12: 690–693. [Google Scholar]
- 23. Chen L. Comparison of the efficacy of sacubitril/valsartan and enalapril in patients with acute anterior wall myocardial infarction complicated with cardiac insufficiency after emergency PCI. Strait Pharmaceut J 2021; 33: 154–156. [Google Scholar]
- 24. Chen M, Zhong P, Huang C, Yu Y, Luo Z. Short‐term efficacy and safety analysis of sacubitril/valsartan on cardiac function in patients with heart failure after myocardial infarction. Chinese Foreign Med Res 2021; 19: 1–4. [Google Scholar]
- 25. Zhao Y, Dong Z, Lu G, Han L, Xin Y. Effect of sacubitril/valsartan on cardiac function in patients with heart failure after emergency PCI. Northern Pharmaceut J 2020; 17: 11–12. [Google Scholar]
- 26. Prabhu SD, Frangogiannis NG. The biological basis for cardiac repair after myocardial infarction: from inflammation to fibrosis. Circ Res 2016; 119: 91–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Gardner DG, Chen S, Glenn DJ, Grigsby CL. Molecular biology of the natriuretic peptide system: implications for physiology and hypertension. Hypertension 2007; 49: 419–426. [DOI] [PubMed] [Google Scholar]
- 28. McMurray JJV, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, Rouleau JL, Shi VC, Solomon SD, Swedberg K, Zile MR, Investigators P‐H and Committees . Angiotensin‐neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014; 371: 993–1004. [DOI] [PubMed] [Google Scholar]
- 29. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, Falk V, Gonzalez‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GMC, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016; 37: 2129–2200. [DOI] [PubMed] [Google Scholar]
- 30. Mouton AJ, Rivera OJ, Lindsey ML. Myocardial infarction remodeling that progresses to heart failure: a signaling misunderstanding. Am J Physiol Heart Circ Physiol 2018; 315: H71–h79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Solomon SD, McMurray JJV, Anand IS, Ge J, Lam CSP, Maggioni AP, Martinez F, Packer M, Pfeffer MA, Pieske B, Redfield MM, Rouleau JL, van Veldhuisen DJ, Zannad F, Zile MR, Desai AS, Claggett B, Jhund PS, Boytsov SA, Comin‐Colet J, Cleland J, Düngen H‐D, Goncalvesova E, Katova T, Kerr Saraiva JF, Lelonek M, Merkely B, Senni M, Shah SJ, Zhou J, Rizkala AR, Gong J, Shi VC, Lefkowitz MP, Investigators P‐H and Committees . Angiotensin‐neprilysin inhibition in heart failure with preserved ejection fraction. N Engl J Med 2019; 381: 1609–1620. [DOI] [PubMed] [Google Scholar]
- 32. Jering KS, Claggett B, Pfeffer MA, Granger C, Køber L, Lewis EF, Maggioni AP, Mann D, McMurray JJV, Rouleau JL, Solomon SD, Steg PG, van der Meer P, Wernsing M, Carter K, Guo W, Zhou Y, Lefkowitz M, Gong J, Wang Y, Merkely B, Macin SM, Shah U, Nicolau JC, Braunwald E. Prospective ARNI vs. ACE inhibitor trial to DetermIne Superiority in reducing heart failure Events after Myocardial Infarction (PARADISE‐MI): design and baseline characteristics. Eur J Heart Fail 2021; 23: 1040–1048. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Search strategies of PubMed and the Cochrane Library.
Table S2. Results of sensitivity analysis of all outcomes.
Table S3. DOI number of included Chinese studies.
Figure S1. Risk of bias of included RCTs by RoB2 tool from Cochrane.
Figure S2. The subgroup analysis of hospitalization for HF based on the use of ACEI or ARB in control group. ACEI, angiotensin‐converting enzyme inhibitors; ARB, angiotensin receptor blockers; CI, confidence interval; HF, heart failure; RR, risk ratio.
Figure S3. The subgroup analysis of the NT‐ProBNP based on the use of ACEI or ARB in control group. ACEI, angiotensin‐converting enzyme inhibitors; ARB, angiotensin receptor blockers; CI, confidence interval; WMD, weighted mean difference.
Figure S4. The subgroup analysis of the change of LVEF based on the use of ACEI or ARB in control group. ACEI, angiotensin‐converting enzyme inhibitors; ARB, angiotensin receptor blockers; CI, confidence interval; LVEF, left ventricular ejection fraction; WMD, weighted mean difference.
Figure S5. The subgroup analysis of the change of LVEDD based on the use of ACEI or ARB in control group. ACEI, angiotensin‐converting enzyme inhibitors; ARB, angiotensin receptor blockers; CI, confidence interval; LVEDD, left ventricular end‐diastolic dimension; WMD, weighted mean difference.
Figure S6. The incidence of side effects with sacubitril–valsartan vs. ACEI/ARB. CI, confidence interval; RR, risk ratio.
Figure S7. Funnel plots of the rate of myocardial reinfarction (A), the rate of hospitalization for heart failure (B), the change of LVEF (C), the change of LVEDD (D), the level of NT‐ProBNP (E), the incidence of hypotension (F). LVEF, left ventricular ejection fraction; LVEDD, left ventricular end‐diastolic dimension.