

Abstract
We aim to present a case with bilateral sequential paracentral acute middle maculopathy (PAMM). A 57-year-old man presented with paracentral scotoma in the left eye. The patient’s multimodal imaging findings were consistent with PAMM in the left eye. Extensive systemic work-up revealed hypertension and a history of cerebrovascular event. One year after initial presentation, the patient had a subsequent decrease in visual acuity in the right eye and developed optical coherence tomography findings consistent with PAMM, whereas the left eye showed resolved PAMM findings. Although rare, PAMM can occur bilaterally. Clinicians should monitor unilateral PAMM patients with systemic vasculopathy for involvement in the fellow eye.
Keywords: PAMM, paracentral acute middle maculopathy, hypertension, cerebrovascular event
Introduction
Paracentral acute middle maculopathy (PAMM) is a recently defined retinal entity characterized by a hyperreflective parafoveal band at the level of the inner nuclear layer (INL) on spectral-domain optical coherence tomography (SD-OCT) corresponding to ischemia in the deep retinal capillary plexus.1
PAMM can be isolated or associated with several retinovascular and systemic diseases such as retinal artery or vein occlusion (RVO), diabetic retinopathy, Purtscher retinopathy, and sickle-cell retinopathy.2,3,4 Despite the substantial number of unilateral PAMM cases in the literature, there is little information on the bilateral involvement of PAMM. Herein, we aim to report a patient who presented with acute PAMM in one eye and subsequently developed PAMM in the fellow eye during follow-up.
Case Report
A 57-year-old man presented complaining of a black spot in his left eye for 2 months. At presentation, his best corrected visual acuity (BCVA) was 20/200 in the left eye and 20/20 in the right eye. Biomicroscopic slit-lamp and dilated fundus examinations were within normal limits except for the presence of grade 2 nuclear sclerosis in both eyes. Fundus fluorescein angiography (FA) showed normal perfusion of the retinal vessels with no abnormal fluorescence or leakage in both eyes (Figure 1A, B). SD-OCT showed a hyperreflective band pattern at the level of the INL and inner plexiform layer (IPL) in the left eye and apparently normal retinal structures in the right eye (Figure 1C, D). His medical history included hypertension for the last 5 years and a previous cerebrovascular event. He was taking 160 mg valsartan, 12.5 mg hydrochlorothiazide, and 100 mg acetylsalicylic acid. At presentation, his blood pressure was 140/90 mmHg. The patient’s SD-OCT findings were consistent with PAMM in the left eye. Accordingly, the patient underwent an extensive systemic work-up including carotid artery Doppler and orbital color Doppler imaging, metabolic panel, blood count, and cardiology and hematology consultations for underlying disease. The systemic work-up was unremarkable.
Figure 1.
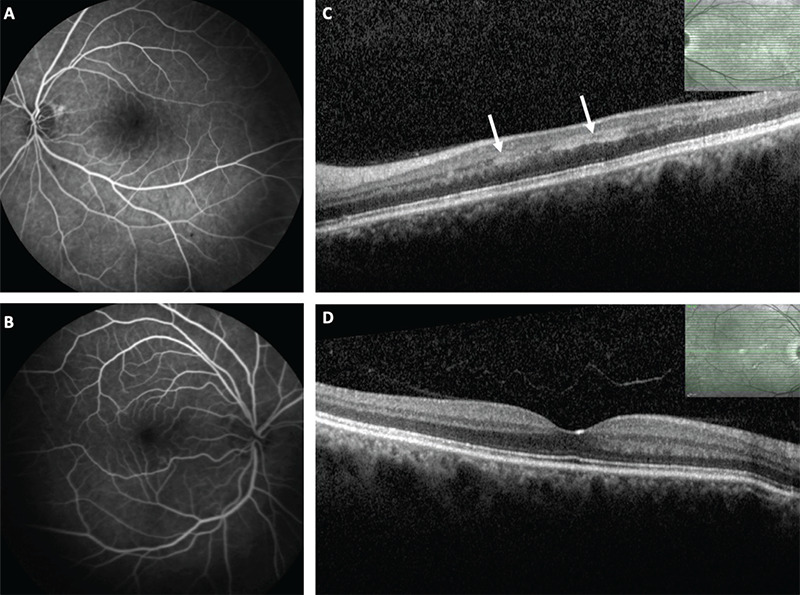
Fundus fluorescein angiography shows complete perfusion of the retinal vessels without abnormal leakage in both eyes at initial visit (A, B). Spectral domain optical coherence tomography (SD-OCT) scans of the left eye demonstrate a hyperreflective parafoveal band at the level of the inner nuclear and inner plexiform layers (C). The right eye of the patient shows no abnormality on SD-OCT (D)
The patient missed several follow-up visits, then returned 1 year after his initial presentation with complaints of a black spot in the fellow eye for 1 month. Visual acuity was 20/25 in the left eye and 20/60 in the right eye. No retinal lesion was seen in dilated fundus examination. FA was within normal limits in both eyes (Figure 2A, B). On SD-OCT, a hyperreflective lesion was noted at the INL and IPL level in the right eye with signs of chronic PAMM in the left eye (Figure 2C, D). OCT angiography showed decreased perfusion of the deep capillary plexus with normal perfusion of the superficial capillary plexus in the right eye (Figure 2E-H). Microperimetry showed paracentral scotomas corresponding to the retinal lesions seen on SD-OCT in both eyes (Figure 3). In light of his previous retinal findings in the left eye, patient was diagnosed as bilateral PAMM. His BCVA was 20/25 in both eyes at final visit.
Figure 2.
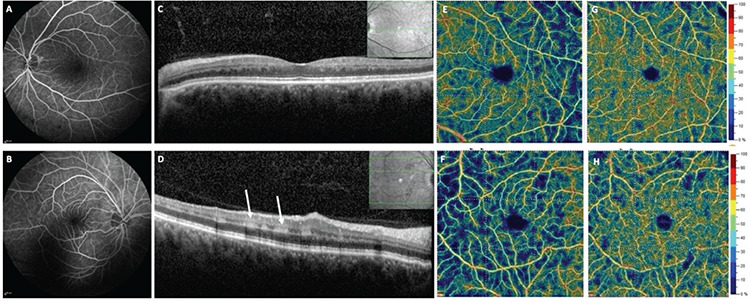
Fundus fluorescein angiography shows complete perfusion of the retinal vessels in both eyes (A, B). Spectral domain optical coherence tomography (SD-OCT) scan of the left eye shows inner nuclear layer thinning associated with outer plexiform layer elevation consistent with resolved paracentral acute middle maculopathy (PAMM) (C). SD-OCT scan of the right eye reveals a hyperreflective parafoveal band at the level of the inner nuclear and inner plexiform layers corresponding to acute PAMM (D). OCT angiography shows normal perfusion of the deep and superficial capillary plexuses in the left eye (E, G) and decreased perfusion of the deep capillary plexus but normal perfusion of the superficial capillary plexus in the right eye (F, H)
Figure 3.
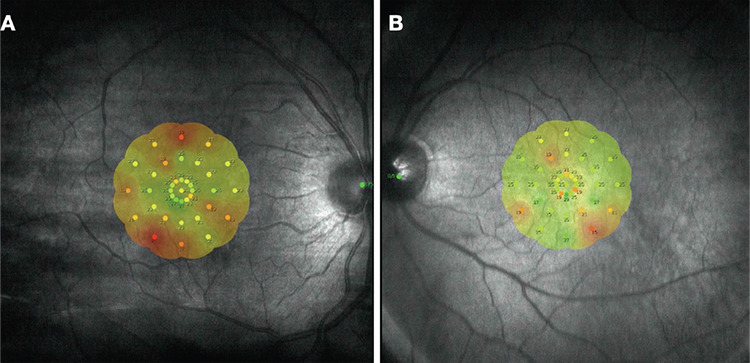
Retinal sensitivity maps containing interpolated retinal sensitivity measures. Microperimetry images show decreased retinal sensitivity in red (A, B)
Discussion
Herein, we document a patient with a history of hypertension and cerebrovascular event who presented with PAMM in one eye and later developed PAMM in the fellow eye. Initially, the first eye showed characteristic acute PAMM findings, then had signs of chronic (resolved) PAMM in the form of INL thinning associated with outer plexiform layer disruption/elevation. The subsequent development of INL thinning corresponding to the original PAMM lesion suggests that ischemia of the intermediate and deep capillary plexuses may be the primary etiology.
Though PAMM has been associated with various ocular and systemic conditions, a recent study reported that the condition may occur even in asymptomatic patients with unknown systemic disease.5 In a recent study, chronic PAMM lesions were detected in 89.9% of hypertensive patients and 16.7% of healthy individuals.5 Moreover, the likelihood of developing chronic PAMM lesions was significantly higher in patients with mild hypertension, which may suggest that these lesions are the earliest changes in retinal microcirculation before changes in OCTA parameters become apparent. In another study, the prevalence of resolved PAMM lesions in the fellow eyes of patients with unilateral RVO was found to be as high as 71.2%, whereas 19.3% of age-matched healthy individuals displayed similar findings.6
In conclusion, patients with systemic vascular pathologies are at risk for developing bilateral PAMM, which may occur sequentially. These patients should be monitored closely for involvement of the fellow eye.
Footnotes
Ethics
Informed Consent: Obtained.
Peer-review: Externally peer reviewed.
Authorship Contributions
Surgical and Medical Practices: İ.K.M., E.Ö.T., V.L.K., Concept: İ.K.M., E.Ö.T., V.L.K., Design: İ.K.M., E.Ö.T., V.L.K., Data Collection or Processing: İ.K.M., E.Ö.T., V.L.K., Analysis or Interpretation: İ.K.M., E.Ö.T., V.L.K., Literature Search: İ.K.M., E.Ö.T., V.L.K., Writing: İ.K.M., E.Ö.T., V.L.K.,
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study received no financial support.
References
- 1.Sarraf D, Rahimy E, Fawzi AA, Sohn E, Barbazetto I, Zacks DN, Mittra RA, Klancnik JM Jr, Mrejen S, Goldberg NR, Beardsley R, Sorenson JA, Freund KB. Paracentral acute middle maculopathy: a new variant of acute macular neuroretinopathy associated with retinal capillary ischemia. JAMA Ophthalmol. 2013;131:1275–1287. doi: 10.1001/jamaophthalmol.2013.4056. [DOI] [PubMed] [Google Scholar]
- 2.Iafe NA, Onclinx T, Tsui I, Sarraf D. Paracentral acute middle maculopathy and deep retinal capillary plexus infarction secondary to reperfused central retinal artery occlusion. Retina Cases Brief Rep. 2017;11(Suppl1):S90–S93. doi: 10.1097/ICB.0000000000000424. [DOI] [PubMed] [Google Scholar]
- 3.Rahimy E, Kuehlewein L, Sadda SR, Sarraf D. Paracentral acute middle maculopathy: What we knew then and what we know now. Retina. 2015;35:1921–1930. doi: 10.1097/IAE.0000000000000785. [DOI] [PubMed] [Google Scholar]
- 4.Kıyat P, Değirmenci C, Nalçacı S, Afrashi F, Akkın C. Paracentral acute middle maculopathy. Turk J Ophthalmol. 2020;50:193–196. doi: 10.4274/tjo.galenos.2020.92972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Maltsev DS, Kulikov AN, Burnasheva MA, Chhablani J. Prevalence of resolved paracentral acute middle maculopathy lesions in fellow eyes of patients with unilateral retinal vein occlusion. Acta Ophthalmol. 2020;98:e22–e28. doi: 10.1111/aos.14196. [DOI] [PubMed] [Google Scholar]
- 6.Burnasheva MA, Maltsev DS, Kulikov AN, Sherbakova KA, Barsukov AV. Association of chronic paracentral acute middle maculopathy lesions with hypertension. Ophthalmol Retina. 2020;4:504–509. doi: 10.1016/j.oret.2019.12.001. [DOI] [PubMed] [Google Scholar]