

Abstract
Background
This review is one in a series of reviews of interventions for lateral elbow pain. Lateral elbow pain, or tennis elbow, is a common condition causing pain in the elbow and forearm and lack of strength and function of the elbow and wrist. Acupuncture has long been used to treat lateral elbow pain in China and in Western countries practitioners and consumers are increasingly exploring acupuncture as a first line treatment for musculoskeletal disorders. No previous systematic review of the available evidence has been conducted to determine whether acupuncture is efficacious in the treatment lateral elbow pain.
Objectives
To determine the effectiveness of acupuncture in the treatment of adults with lateral elbow pain with respect to pain reduction, improvement in function, grip strength and adverse effects.
Search methods
We searched MEDLINE, CINAHL, EMBASE and SCISEARCH and the Cochrane Clinical Trials Register and the Musculoskeletal Review Group's specialist trial database from 1966 to June 2001. Identified keywords and authors were searched in an effort to retrieve as many trials as possible.
Selection criteria
Two independent reviewers assessed all identified trials against pre‐determined inclusion criteria. Randomised and pseudo randomised trials in all languages were included in the review provided they were testing acupuncture compared to placebo or another intervention in adults with lateral elbow pain (tennis elbow). Outcomes of interest were pain, function, disability, quality of life, strength, participant satisfaction with treatment and adverse effect.
Data collection and analysis
For continuous variables means and standard deviations were extracted or imputed to allow the analysis of weighted mean difference, while for binary data numbers of events and total population were analysed and interpreted as relative risks. Trial results were combined only in the absence of clinical and statistical heterogeneity.
Main results
Four small randomized controlled trials were included but due to flaws in study designs (particularly small populations, uncertain allocation concealment and substantial loss to follow up) and clinical differences between trials, data from trials could not be combined in a meta‐analysis. One randomised controlled trial found that needle acupuncture results in relief of pain for significantly longer than placebo (WMD = 18.8 hours, 95%CI 10.1 to 27.5) and is more likely to result in a 50% or greater reduction in pain after 1 treatment (RR 0.33, 95%CI 0.16 to 0.69) (Molsberger 1994) . A second randomized controlled trial demonstrated needle acupuncture to be more likely to result in overall participant reported improvement than placebo in the short term (RR = 0.09 95% CI 0.01 to 0.64) (Haker 1990a) . No significant differences were found in the longer term (after 3 or 12 months). A randomized controlled trial of laser acupuncture versus placebo demonstrated no differences between laser acupuncture and placebo with respect to overall benefit (Haker 1990b). A fourth included trial published in Chinese demonstrated no difference between Vitamin B12 injection plus acupuncture, and Vitamin B12 injection alone (Wang 1997).
Authors' conclusions
There is insufficient evidence to either support or refute the use of acupuncture (either needle or laser) in the treatment of lateral elbow pain. This review has demonstrated needle acupuncture to be of short term benefit with respect to pain, but this finding is based on the results of 2 small trials, the results of which were not able to be combined in meta‐analysis. No benefit lasting more than 24 hours following treatment has been demonstrated. No trial assessed or commented on potential adverse effect. Further trials, utilising appropriate methods and adequate sample sizes, are needed before conclusions can be drawn regarding the effect of acupuncture on tennis elbow.
Keywords: Adult, Humans, Acupuncture Therapy, Acupuncture Therapy/methods, Randomized Controlled Trials as Topic, Tennis Elbow, Tennis Elbow/therapy
Plain language summary
Acupuncture for elbow pain
Acupuncture might be able to provide short‐term relief from tennis elbow, but more research is needed.
Background
This Cochrane review is one of a series of Cochrane reviews of interventions for lateral elbow pain in adults.
Lateral elbow pain is common (population prevalence 1‐3%) (Allender 1974) and causes considerable morbidity and financial cost. Peak incidence is 40‐50 years and for women between 42 and 46 years of age the incidence increases to 10% (Chard 1989, Verhaar 1994). While lateral elbow pain is generally self‐limiting, symptoms often persist for 18 months to two years (Hudak 1996b) . The cost is therefore high, both in terms of loss of productivity, and health care utilisation. The incidence of lateral elbow pain in general practice is four to seven per 1000 patients per year (Verhaar 1994, Hamilton 1986, Kivi 1983).
"Lateral elbow pain" is described by many analogous terms in the literature, including "tennis elbow", "lateral epicondylitis", "rowing elbow", "tendonitis of the common extensor origin", and peritendonitis of the elbow". For the purposes of this review the term "lateral elbow pain" will be used as it best describes the site of the pain, and will allow for greater clarity of inclusion.
Lateral elbow pain is characterised by pain over the lateral epicondyle of the humerus and pain on resisted dorsi‐flexion of the wrist. It is considered an overload injury typically following minor and often unrecognised trauma of the extensor muscles of the forearm (Murtagh 1988).
Three systematic reviews specifically addressing the effect of interventions for lateral elbow pain have been published (Labelle 1992, Hudak 1996, Assendelft 1996). All report little demonstrable evidence for efficacy of any of the studied interventions. No trials of acupuncture were included in any of these reviews.
Acupuncture for the treatment of musculoskeletal pain is growing in acceptance, by both clinicians and consumers of health care. Approximately one million consumers utilise acupuncture annually in the United States (Paramore 1997), and a large percentage of these suffer musculoskeletal disorders (Diehl 1997).
Acupuncture is thought to confer an analgesic effect and several hypotheses as to the chain of events resulting in analgesia from acupuncture have been proposed. Some authors attribute the analgesic effects to the release of b‐endorphins in the lumbar spine and increased 5‐Hydroxy tryptophan level in the cerebrum. Other explanations include the overriding of the pain stimulus by the biochemical lines of acupuncture in the transmitting process of the central nervous system, and the more traditional explanation of the freeing of a blockage of "Qi" or energy flow by acupuncture (Viola 1998).
Although acupuncture is often recommended for the treatment of lateral elbow pain, few studies have investigated the efficacy of this intervention, and to our knowledge, no systematic review has been published specifically addressing the effectiveness of acupuncture for relief of pain and dysfunction associated with lateral elbow pain.
Objectives
To determine the effectiveness of acupuncture in the treatment of patients with lateral elbow pain with respect to symptom reduction including pain, improvement in function, grip strength, and adverse effect.
Methods
Criteria for considering studies for this review
Types of studies
Studies were included following blinded review (author, year and journal concealed) by two independent reviewers (SH, LB). Criteria for inclusion were: a) randomised controlled trials b) outcome assessor blind or not blind to allocated group (a sensitivity analysis was planned both including and excluding unblinded studies since foreknowledge of treatment allocation may lead to biased assessment of outcome). c) all languages were considered, and a translator was if necessary. A second sensitivity analysis was planned including and excluding foreign language publications.
Types of participants
Inclusion in this review was restricted to trials with participants meeting the following criteria:
a) Adults >16 years of age. b) Lateral elbow pain for greater than three weeks duration. c) No history of significant trauma or systemic inflammatory conditions such as rheumatoid arthritis. d) Studies which included various soft tissue diseases and tendinopathies at other sites were included provided that the lateral elbow pain results were presented separately or > 90% of patients in the study had lateral elbow pain.
A full description of all inclusion criteria used to describe lateral elbow pain forms part of the table of included studies.
Types of interventions
All randomised, controlled comparisons of acupuncture versus placebo or acupuncture versus another modality were included. For the purposes of meta‐analysis, comparisons were established according to intervention.
Types of outcome measures
The outcomes of interest include pain (at night, at rest and on movement), function, disability and quality of life (including surrogate measures such as return to work), grip strength, participant perception of overall effect or global preference, range of motion (active and passive) and adverse effects.
Search methods for identification of studies
We searched MEDLINE, EMBASE, CINAHL (includes all major physiotherapy and occupational therapy journals from U.S.A., Canada, England, Australia and New Zealand), and Science Citation Index (SCISEARCH) from 1966 to June 2001 using the Cochrane Musculoskeletal Review Group's "optimally sensitive search strategy" to identify all possible randomised controlled trials. Keywords gained from previous reviews and all relevant articles were searched. Any additional keyword identified from subsequent articles was searched again. As this review is one of a series of interventions for lateral elbow pain, various interventions were included in the search strategy.
1 RANDOMIZED‐CONTROLLED TRIAL in PT 2 RANDOMIZED‐CONTROLLED‐TRIALS 3 RANDOM‐ALLOCATION 4 DOUBLE‐BLIND‐METHOD 5 SINGLE‐BLIND‐METHOD 6 CLINICAL‐TRIAL in PT 7 explode CLINICAL‐TRIALS 8 (clin* near trial*) in TI 9 (clin* near trial*) in AB 10 (singl* or doubl* or trebl* or tripl*) near (blind* or mask*) 11 (#10 in TI) or (#10 in AB) 12 PLACEBOS 13 placebo * in TI 14 placebo in AB 15 random * in TI 16 random * in AB 17 RESEARCH DESIGN 18 #1 #2 #3 #4 #5 #6 #7 #8 #9 #10 #11 #12 #13 #14 #15 #16 #17 19 EXPLODE (* see note ) 20 EXPLODE (* see note) 21 EXPLODE (see* note) 22 TEXT WORDS for all SYNONYMS or / 23 #19 or #20 or # 21 or #22 24 #18 AND # 23 25 TG=ANIMAL not ( TG=HUMAN and TG=ANIMAL) 26 #24 not 25 27 acupuncture* 28 analgesics* 29 anti‐inflammatory drugs* 30 N.S.A.I.D.S.* 31 NSAID* 32 extra corporeal shock wave therapy* 33 non steroidal anti‐inflammatory drugs* 34 orthopaedic surgery* 35 surgery* 36 Ultrasound* 37 LLLT* 38 Laser* 39 Shortwave* 40 TENS* 41 #27 or #28 or #29 or #30 or #31 or #32 or #33 or #34 or #35 or #36 or #37 or #38 or #39 or #40 42 common extensor origin* 43 epicondylitis* 44 lateral epicondylitis* 45 lateral elbow pain* 46 tendonitis* 47 tennis elbow* 48 #42 or #43 or #44 or #45 or #46 or #47 49 #26 and #41 and #48
Further electronic searches for key authors identified were made, and a record of these searches kept. Print outs of all search strategies were compiled and stored for future reproduction and review if required.
i) The Cochrane Controlled Trials Register (CCTR) This is an electronic database and is published on the Cochrane Library. The search for relevant trials was conducted on Issue 1, 2001.
All articles were coded and details of source, intervention, population and funding recorded. The investigator compiling the references (SG) decided on potentially relevant trials (based on the article being a trial of an intervention for tennis elbow), and collated these trials for first round inclusion. The methods sections of these trials were then blinded of all reference to journal, author or country of origin, and sent to the blinded reviewers (LB & SH) for inclusion assessment.
Data collection and analysis
Following identification of potential trials for inclusion by the previously outlined search strategy (SG), the blinded methods sections of all identified trials were reviewed independently according to predetermined criteria (see selection criteria), by two of three investigators (LB, SH, RB). Decisions regarding the inclusion of trials were be made independently and any disagreements resolved by consensus where possible, or arbitration by the third reviewer.
DESCRIPTION OF VALIDITY The blinded methods and results sections of each included trial was assessed by the same two independent reviewers and the following key methodological criteria were extracted.
Allocation concealment Blinded assessment of outcome Numbers lost to follow up Appropriate statistical analysis
A descriptive approach to validity assessment was chosen rather than use of a scale due to concerns regarding the consistency and validity of available scales. The key methodological criteria were selected based on there being empirical evidence linking failure to meet these criteria with the possibility of a biased trial result.
This information was then collated in the table of included studies, and blinded outcome assessor used as the basis of a sensitivity analysis.
DATA EXTRACTION AND ANALYSIS Data was extracted and recorded onto specially developed data extraction forms. The following characteristics were extracted for each trial and recorded along with the results of trial methodological assessment in the Table of Included Studies.
1. Details of participants including demographic characteristics, source of recruitment and criteria for diagnosis 2. Details of the experimental and control interventions including intervention type, dosage and duration of treatment 3. Outcomes measures used in the trial (outcome, method of measurement and timing)
In order to assess efficacy, raw data (means and standard deviations of change scores) were extracted and entered into Revman 4.1. When trials reported standard error of the mean it was converted to a standard deviation. When data reported in the included trial was converted or imputed details of this were recorded in the notes section of the included studies table. All data transformation and entry was performed by one reviewer and checked by a second (SG, MW).
For trials where the required data was not reported or able to be calculated, further details were requested from first authors. When unsuccessful, the study was included in the review and fully described, but not included in the meta‐analysis. An entry to that effect was made in the notes section of the included studies table.
DATA SYNTHESIS Meta‐analysis was facilitated by RevMan 4.1, using the following choices of summary statistic.
CONTINUOUS OUTCOMES: Weighted mean difference using a random effects model was selected as the summary statistic. A random effects model was used to account for the anticipated large amount of heterogeneity among the primary trials. In the event of significant heterogeneity (p < 0.1), trials results were not pooled.
BINARY OUTCOMES: Relative risk using a random effects model was selected for interpretation of the dichotomous outcome measures in this review as events were not rare (Deeks 1998) . A random effects model was selected to account for the large amount of anticipated heterogeneity among the primary trials. In the event of significant heterogeneity, trial results were not pooled.
Sensitivity analyses were planned to assess the effect of blinding of outcome assessor, and of the inclusion of foreign language trials. It was planned to perform meta‐analysis both including and excluding trials without a blinded assessment of outcome, and including and excluding trials published in languages other than English, and the impact on the summary result assessed. Due to a paucity of trials sensitivity analysis was not possible but may be included in future updates of this review.
Results
Description of studies
Eleven potential studies were identified and five references included. Of these one was a duplicate publication, therefore four trials were included in the review. Of the six excluded studies, four were not randomised (Brattberg 1983, Zhiming 1990, Zhongying 1989, Wu 1997) one was a narrative review (Lee 2000) and one was a trial in a population of general non‐specific tendinopathies where the results of those with lateral elbow pain were not reported separately (Ammer 1994). One of these excluded studies was published in Chinese and translated into English (Wu 1997). The remaining excluded trials were all published in English. All were from the published literature.
Of the included studies, two trials compared needle acupuncture to placebo (Molsberger 1994, Haker 1990a) but used different outcome assessments. One trial compared laser acupuncture to placebo (Haker 1990b), and one compared a combination of acupuncture and vitamin B12 injection to Vitamin B12 injection alone (Wang 1997).
All trials defined lateral elbow pain according to a similar set of diagnostic criteria (pain over the lateral epicondyle with pain produced by grip, resisted wrist and/ or finger dorsiflexion) and excluded participants with cervical spine pathology. Two trials followed participants for 12 months (Haker 1990a, Haker 1990b), while two reported outcome only immediately following treatment (Huang 1998, Molsberger 1994).
Due to the clinical heterogeneity of differing interventions and timing of outcome assessment, no pooling of studies was possible.
Risk of bias in included studies
Trial populations ranged from 48 to 93 participants (see table of included studies). Concealment of allocation was unclear in all trials. All but one trial (Huang 1998) had a blinded outcome assessor. In the two trials following participants for longer than one assessment immediately after treatment, up to 20% of participants were lost to follow up (see table of included studies).
Effects of interventions
Based on the results of two randomised controlled trials which could not be combined, acupuncture results in relief of pain for significantly longer than placebo (WMD = 18.8 hours, 95%CI 10.1 to 27.5) (Molsberger 1994), is more likely to result in a 50% or greater reduction in pain after 1 treatment (RR 0.33, 95%CI 0.16 to 0.69) (Molsberger 1994) , and more likely to result in overall improvement (RR = 0.09 95% CI 0.01 to 0.64) after 10 treatments (Haker 1990a). No significant differences were found in the longer term (after 3 or 12 months).
No differences were demonstrated between laser acupuncture and placebo with respect to overall benefit, and no differences were demonstrated between Vitamin B12 injection plus acupuncture, and Vitamin B12 injection alone.
Discussion
Due to the small number of included trials and problems with methodology of the included trials (particularly small populations, uncertain allocation concealment and substantial loss to follow up), the results of this review are inconclusive and should be interpreted with caution.
Acupuncture is increasingly been used in the treatment of musculoskeletal conditions in Western countries, and has been the treatment of choice in China for centuries. While there is evidence for the use of acupuncture in idiopathic headache (Linde 2001), this review does not provide sufficient evidence to support or oppose the use of acupuncture (needle or laser) in the treatment of lateral elbow pain.
Only four randomised controlled trials meeting the inclusion criteria of this review were identified and no data could be combined due to clinical heterogeneity between trials.
One trial of needle acupuncture demonstrated significantly longer duration of pain relief following acupuncture than placebo, however, while statistically significant, the acupuncture group experienced a mean pain relief following treatment of less than 24 hours which may not be considered clinically significant for a chronic condition. Two trials demonstrated participants felt significantly better in terms of pain and overall improvement immediately following treatment, but this improvement was not sustained at 3 or 12 months. In a self limiting condition however such improvement may be clinically significant if it allows improvement in function while the condition follows its natural history toward recovery. However, such short term improvement needs to be validated by further trials before acupuncture can be recommended for short term and temporary symptom relief.
Authors' conclusions
Implications for practice.
There is insufficient evidence to either support or refute the use of acupuncture (either needle or laser) in the treatment of lateral elbow pain. This review has demonstrated needle acupuncture to be of short term benefit with respect to pain, but this finding is based on the results of 2 small trials, the results of which were not able to be combined in meta‐analysis. No benefit lasting more than 24 hours following treatment has been demonstrated. No trial assessed or commented on potential adverse effect.
Implications for research.
Further randomised controlled trials of both laser and needle acupuncture are needed to assess the efficacy of this increasingly popular intervention for treating lateral elbow pain. Trials should be adequately powered, attempt to blind both participant and outcome assessor, and include outcome measures of pain and function and adverse effect. Outcome measures should be valid, reliable and responsive. Future studies of the benefit of acupuncture should give consideration to the most appropriate dosage, site and method of administration of acupuncture.
What's new
| Date | Event | Description |
|---|---|---|
| 16 June 2008 | Amended | Converted to new review format. A001‐R |
Acknowledgements
This review was supported by a fellowship granted to the first author by the Department of Health and Human Services, Victorian State Government, Victoria, Australia, and a one week visiting fellowship to the Australasian Cochrane Centre granted by the Cochrane Collaboration. The authors extend their gratitude to these two bodies in addition to acknowledging the methodological support and advice of the staff at the Australasian Cochrane Centre. The authors would also like to thank the Cochrane Musculoskeletal Review Group (CMSG) Editorial Team, Arne Gam, Bill Gillespie and Vivian Robinson for their helpful comments and suggestions.
Data and analyses
Comparison 1. ACUPUNCTURE VERSUS PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Duration of pain relief (hours) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Overall improvement (number of patients unchanged or worse) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.1 After 10 treatments | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 After 3 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 After 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Less than 50 % pain relief after 1 treatment | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected |
1.1. Analysis.
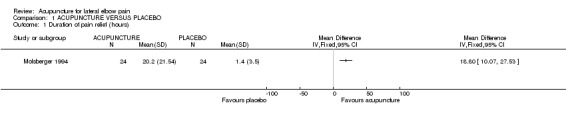
Comparison 1 ACUPUNCTURE VERSUS PLACEBO, Outcome 1 Duration of pain relief (hours).
1.2. Analysis.
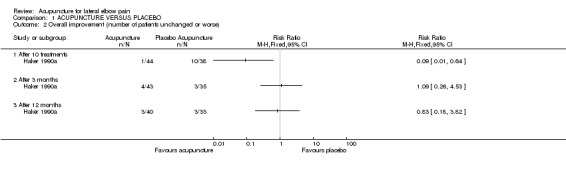
Comparison 1 ACUPUNCTURE VERSUS PLACEBO, Outcome 2 Overall improvement (number of patients unchanged or worse).
1.3. Analysis.
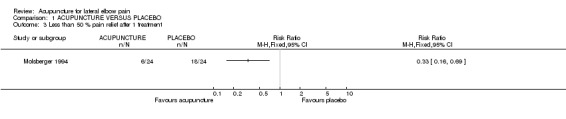
Comparison 1 ACUPUNCTURE VERSUS PLACEBO, Outcome 3 Less than 50 % pain relief after 1 treatment.
Comparison 2. LASER ACUPUNCTURE POINTS VS PLACEBO.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Subjective outcome of no change or worse | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.1 After 10 sessions | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 After 3 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 After 12 months | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
2.1. Analysis.
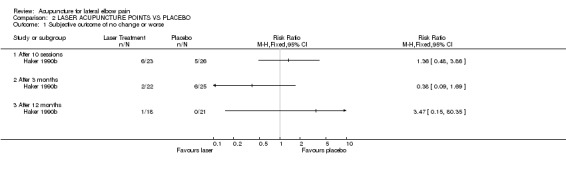
Comparison 2 LASER ACUPUNCTURE POINTS VS PLACEBO, Outcome 1 Subjective outcome of no change or worse.
Comparison 3. ACUPUNCTURE PLUS VITAMIN B12 INJECTION VS INJECTION ALONE.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Still with symptoms after treatment | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected |
3.1. Analysis.
Comparison 3 ACUPUNCTURE PLUS VITAMIN B12 INJECTION VS INJECTION ALONE, Outcome 1 Still with symptoms after treatment.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Haker 1990a.
| Methods | Randomised controlled trial Blinding: double‐blinded, outcome assessor was blind to intervention and placebo used Loss to follow up: 86 enrolled, 6 drop outs in first 2 weeks (time, illness not related to elbow, and one giving no reason). These patients were not followed up. 4 withdrawals (3 in superficial group) withdrew after 3 months due to lack of effect. Appropriate Statistical Analysis: Did not use intention to treat analysis | |
| Participants | 82 participants Inclusion criteria: lateral elbow/ epicondyle pain produced by 2 or more of 4 diagnostic tests; palpation, resisted wrist extension, passive stretching, resisted finger extension Exclusion criteria: shoulder/neck/ thoracic dysfunction local arthritis/ general polyarthritis neurological abnormalities radial nerve entrapment | |
| Interventions | Experimental group : 5 acupuncture points (L1 10, 11,12, Lu 5 & SJ 5) treated 10 times (2‐3 times weekly for 20 weeks control group: placebo: superficial needle insertion only in identical areas & dosage as experimental group | |
| Outcomes | Assessment at baseline, at treatment conclusion, 3 & 12 month followups: 4 diagnostic inclusion criteria (see participants) 4 additional tests; pain reproduction on isometric pronation/ supination, vigorimeter test & lifting test additional subjective question at completion using 5 point scale | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Haker 1990b.
| Methods | Randomised controlled trial Blinding: double blinded, placebo used but unclear who else was blinded Loss to follow up: all 49 completed treatment, afterwards 1 in each group withdrew, 7 withdrew after 3 month follow up (4 in laser group and 3 in placebo) due to ongoing elbow pain and desire to try other treatment options Appropriate Statistical Analysis: The analysis was appropriate for the 40 subjects that completed the assessment, however of note there were 9 subjects lost to follow up | |
| Participants | 49 participants Inclusion criteria: pain over lateral epicondyle for at least 1 month and pain during 2 or more tests as follows 1) palpation lateral epicondyle 2) resisted wrist extension with elbow pronation 3) passive stretching of extensors with elbow extension forearm pronated 4) resisted finger extension with eblow extended, forearm pronated Exclusion criteria: local arthritis, generalised polyarthritis, neurological abnormalities, radial nerve entrapment | |
| Interventions | Experimental group: Mid 1500 IRRADIA laser, Ga‐As laser, wavelength 904 nm, measured mean power outlet 12 mW, peak value 8.3 W, frequency 70 Hz (pulsed) . Control Group: placebo. Laser machine turned off but wand applied to acupuncture points as per control group | |
| Outcomes | Assessment at baseline, 3 months, 1 year 1. measured grip strength but no variance reported so unable to use 2. subjective report of pain on 5 point scale ( 1 = excellent, 2 = good, 3 = better, 4 = slightly improved 5= unchanged or worse |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Molsberger 1994.
| Methods | Randomised placebo controlled trial. Blinding: stated as single blind however subject and outcome assessor were blind to group allocation Loss to follow up: no subjects were reported as lost to follow up or withdrawn Appropriate Statistical Analysis: The study was subjected to an interim analysis and stopped as reported significance had been reached. No subjects were reported to have crossed over treatment groups | |
| Participants | 48 participants Inclusion criteria: subjects with chronic unilateral tennis elbow pain (> 2 months, average 15.4 months) Exclusion criteria: current analgesic therapy systemic joint/bone disorders previous acupuncture treatment overt psychiatric illness inability to speak/read/write German | |
| Interventions | Experimental group: a single non‐segmental acupuncture stimulation treatment on distal points for elbow pain (homolateral leg) control group: a single placebo acupuncture (no insertional needles) | |
| Outcomes | Assessed before and after treatment: pain measurement ‐ 11 point box scale questionnaire (0 = no pain at all, 10 = pain as severe as it could possibly be) duration of pain reduction assessed by following patients for 72 hours | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
Wang 1997.
| Methods | Randomised controlled trial No blinding No participants lost to follow up Intention to treat analysis: Yes | |
| Participants | 60 participants Inclusion criteria: lateral elbow pain from 10 days to 1.5 years | |
| Interventions | Acupuncture plus vitamin B12 injection versus vitamin B12 injection alone | |
| Outcomes | Number cured the only outcome reported. Measured immediately following treatment | |
| Notes | Translated from Chinese. Included in meta‐analysis as a seperate comparison. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | D ‐ Not used |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ammer 1994 | Population not specific to lateral epicondylitis. Included patients with various musculoskeletal conditions and results not reported seperately |
| Brattberg 1983 | Not a randomised controlled trial. |
| Huang 1998 | Randomised controlled trial of 2 different methods of acupunture (floating and classic), demonstrated floating to be significant different to classic with respect to pain at end of treatment. Not included in the review as not comparing acupunture to placebo or another intervention. |
| Lee 2000 | Review |
| Pan 1997 | Randomised controlled trial of 2 different methods of acupuncture. Not blinded. |
| Wu 1997 | Controlled clinical trial, participants selected to treatment or reference group non randomly by trialist |
| Yang 1997 | Randomised controlled trial of 2 slightly different methods of acupuncture. Not blinded. |
| Zhiming 1990 | Not a randomised controlled trial |
| Zhongying 1989 | Not a randomised controlled trial |
Sources of support
Internal sources
Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, Australia.
Australasian Cochrane Centre, Australia.
External sources
No sources of support supplied
Declarations of interest
None known
Edited (no change to conclusions)
References
References to studies included in this review
Haker 1990a {published data only}
- Haker E, Lundeberg T. Acupuncture treatment in epicondylalgia: A comparative study of two treatment techniques. Journal of Musculoskeletal Pain 1994;2(4):126‐8. [DOI] [PubMed] [Google Scholar]
- Haker E, Lundeberg, T. Acupuncture treatment in epicodylalgia: A comparative study of two acupuncture techniques. The Clinical Journal of Pain 1990;6:221‐6. [DOI] [PubMed] [Google Scholar]
Haker 1990b {published data only}
- Haker, E, Lundeberg, T. Laser treatment applied to acupuncture points in lateral humeral epicondylalgia. A double‐blind study. Pain 1990;43(2):243‐7. [DOI] [PubMed] [Google Scholar]
Molsberger 1994 {published data only}
- Molsberger A, Hille E. The analgesic effect of acupuncture in chronic tennis elbow pain. British Journal of Rheumatology 1994;33:1162‐5. [DOI] [PubMed] [Google Scholar]
Wang 1997 {published data only}
- Wang LC. 30 Cases of tennis elbow treated by moxibustion. Shanghai Journal of acupuncture and moxibustion 1997;16(6):20. [Google Scholar]
References to studies excluded from this review
Ammer 1994 {published data only}
- Ammer, K, Kitzinger, E. Thermography of the auricle. Deutsche Zeitschrift Fur Akupunktur 1994;37(6):133‐8. [Google Scholar]
Brattberg 1983 {published data only}
- Brattberg G. Acupuncture therapy for tennis elbow. Pain 1983:258‐88. [DOI] [PubMed] [Google Scholar]
Huang 1998 {published data only}
- Huang, Y, Zhonghua, F, Dongbin, X, Rangke, W. Introduction to floating acupuncture: Clinical study on the treatment of lateral acupuncture. American Journal of Acupuncture 1998;26(1):27‐31. [Google Scholar]
Lee 2000 {published data only}
- Lee, T. Acupuncture and chronic pain management. Annals of the Academy of Medicine 2000;29:17‐21. [PubMed] [Google Scholar]
Pan 1997 {published data only}
- Pan N. 78 cases of tennis elbow treated by raised up needling. Shanghai Journal of acupuncture and moxibustion 1997;16(5):19. [Google Scholar]
Wu 1997 {published data only}
- Wu, ZP. Tennis elbow treated by plum‐blossom needle therapy combined with ginger‐partitioned moxibustion: report of 28 cases. Jiling Journal Traditional Chinese Medicine 1997;17:27. [Google Scholar]
Yang 1997 {published data only}
- Yang JR, Bai JM, Wu LL. 100 cases of tennis elbow treated by acupuncture. Shanghai Journal of Acupuncture 1997;16(5):18. [Google Scholar]
Zhiming 1990 {published data only}
- Zhiming, W. Successful treatment of epicondylitis with chize‐through‐tender point puncturing method. Journal of traditional chinese medicine 1990;10(2):122‐3. [PubMed] [Google Scholar]
Zhongying 1989 {published data only}
- Zhongying, M. 52 cases of external humeral epicondylitis treated by acupuncture and moxibustion. Journal of traditional Chinese Medicine 1989;9(1):3‐4. [PubMed] [Google Scholar]
Additional references
Allender 1974
- Allander E. Prevalence, incidence and remission rates of some common rheumatic diseases and syndromes. Scandinavian Journal of Rheumatology 1974;3:145‐53. [DOI] [PubMed] [Google Scholar]
Assendelft 1996
- Assendelft W. Corticosteroid injections for lateral epicondylitis: a systematic overview. British Journal of General Practice 1996;46:209‐16. [PMC free article] [PubMed] [Google Scholar]
Chard 1989
- Chard MD, Hazlemanand BL. Tennis elbow ‐ a reappraisal. British Journal of Rheumatology 1989;28(3):186‐90. [DOI] [PubMed] [Google Scholar]
Cyriax 1936
- Cyriax JH. The pathology and treatment of tennis elbow. J Bone Joint Surg (A), 1936. 4: p. J Bone Joint Surg (A) 1936;4:p. 921‐40. [Google Scholar]
Deeks 1998
- Deeks, J. Odds ratios should be used only in case‐control studies and logistic regression analysis (letter). BMJ 1998;317:1115. [DOI] [PMC free article] [PubMed] [Google Scholar]
Diehl 1997
- Diehl DL, Kaplan G, Coulter I, Glik D, Huirwitz EL. Use of acupuncture by American Physicians. J Alt Comp Med 1997;3(2):119‐26. [DOI] [PubMed] [Google Scholar]
Hamilton 1986
- Hamilton, P. The prevalence of humeral epicondylitis: a survey in general practice. J Royal College G Practitioners 1986;36:p. 464‐5. [PMC free article] [PubMed] [Google Scholar]
Hudak 1996
- Hudak P, Cole D, Haines A. Understanding Prognosis to Improve Rehabilitation: The Example of Lateral Elbow Pain. Arch Phys Med Rehabil 1996;77:586‐92. [DOI] [PubMed] [Google Scholar]
Hudak 1996b
- Hudak P, Cole D, Haines T. Understanding prognosis to improve rehabilitation: the example of lateral elbow pain. Arch Phys Rehabil 1996;77:568‐93. [DOI] [PubMed] [Google Scholar]
Jadad 1996
- Jadad A, Moore A, Carroll D, Jenkinson C, Reynolds J, Gavaghan D, McQuay H. Assessing the quality of reports of randomised clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17:1‐12. [DOI] [PubMed] [Google Scholar]
Kivi 1983
- Kivi P. The etiology and conservative treatment of lateral epicondylitis. Scand J Rehabil Med 1983;15:37‐41. [PubMed] [Google Scholar]
Labelle 1992
- Labelle H, et al. Lack of scientific evidence for the treatment of lateral epicondylitis of the elbow. The Journal of Bone and Joint Surgery 1992;74:646‐51. [DOI] [PubMed] [Google Scholar]
Linde 2001
- Linde, K, et al. Acupuncture for idiopathic headache (Cochrane Review). Cochrane Database of Systematic Reviews 2001, Issue 2. [DOI: 10.1002/14651858.CD001218.pub2.] [DOI] [PubMed] [Google Scholar]
Murtagh 1988
- Murtagh J. Tennis Elbow. Aust Family Physician 1988;17:90, 91, 94‐5. [PubMed] [Google Scholar]
Paramore 1997
- Paramore LC. The use of alternative therapies: Estimates from the 1994 Robert Wood Johnson Foundation National Access to Health Care Survey. J Pain Sympt Manage 1997;13(2):83‐9. [DOI] [PubMed] [Google Scholar]
Verhaar 1994
- Verhaar, J. Tennis elbow: Anatomical, epidemiological and therapeutic aspects. Int Ortopaedics 1994;18:263‐7. [DOI] [PubMed] [Google Scholar]
Viola 1998
- Viola Leonardo. A critical review of the current conservative therapies for tennis elbow (lateral epicondylitis). ACO 1998;7(2):53‐67. [PMC free article] [PubMed] [Google Scholar]