

Abstract
Beard and moustache reconstruction has gained more popularity and acceptance over the last decade. The procedure is done for the correction of facial areas with hair density deficit and also for the cosmetic enhancement of pre-existing facial hair. The surgical technique includes the harvesting of grafts from the scalp by the follicular unit excision (FUE) or follicular unit transplantation (FUT) technique and then placing them in either premade slits or by stick and place method. The advancement and refinement of procedure over the years has aided in achieving the optimal aesthetic results, with minimal side effects.
Keywords: beard reconstruction, moustache reconstruction, sideburn reconstruction, follicular unit excision
Introduction
Facial hair in men has been a sign of masculinity. The reconstruction or cosmetic enhancement of beard and moustache has been trending as men have become more conscious about their looks. There have been several techniques used by various surgeons in the past for the reconstruction of beard and moustache. 1 2 3 4 5 6 Back in 1972, Vallis transplanted hair to the upper lip to create a moustache using a full thickness strip graft from the parietal scalp. 1 Reed performed single follicular unit transplantation (FUT) in 1999 to repair a cleft lip moustache alopecia. 5 Over the last two decades, there have been various advancements and the technique has been refined to achieve cosmetically pleasing results. As per the 2020 International Society of Hair Restoration Surgeons (ISHRS) practice consensus, almost 15% of procedures in men targeted nonscalp areas of the body, of which beard/moustache accounted for 5% of procedures. 7 The percentage of targeted nonscalp areas is almost double of what it was in 2012 (7.1%) ( Fig. 1 ). 8 The acceptance and demand of the procedure have also elevated drastically for indications secondary to decreased follicular density in facial areas and in patients who want to enhance the already existing facial features.
Fig. 1.
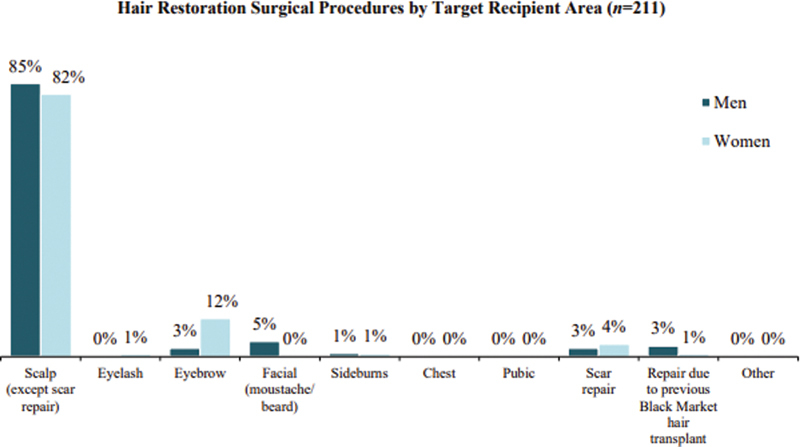
Percentage of hair restoration surgical procedures by target recipient area as per 2020 ISHRS practice consensus. The results show the distribution of 15% of the nonscalp targeted areas of the body in males and females over different nonscalp regions, where eyebrow transplant accounted for the maximum procedures in females (12%) and beard and moustache reconstruction accounted for maximum procedures in males (5%). 7
Table 1 depicts the percentage of importance of the targeted recipient site with beard restoration procedures as per the 2020 ISHRS practice consensus. Most respondents rated strong goatee and strong cheek beards higher than the prominent moustache and strong sideburns. 7
Table 1. Percentage of importance of the targeted recipient site with beard restoration procedures as per 2020 ISHRS practice consensus a .
| Very important (1) | Important (2) | Moderately important (3) | Slightly important (4) | Not important (5) | Mean | |
|---|---|---|---|---|---|---|
| Strong sideburns | 10.4% | 37.0% | 34.7% | 12.2% | 5.7% | 2.7 |
| Strong goatee | 15.8% | 38.2% | 27.7% | 8.7% | 9.8% | 2.6 |
| Strong cheek beard | 15.4% | 34.6% | 31.2% | 12.0% | 6.9% | 2.6 |
| Prominent moustache | 12.2% | 35.4% | 33.6% | 12.5% | 6.3% | 2.7 |
2020 ISHRS practice census offers key insights on hair restoration practices and procedures.
Most respondents rated strong goatee and strong cheek beards higher than the prominent moustache and strong sideburns. 7
Anatomy
The face can be divided into frontal and lateral aspects with different zones for the purpose of facial hair restoration.
The moustache, the goatee, and the central portion of the upper part of the neck comprise the frontal aspect, out of which the former two are the most prominent features with comparatively higher density. The follicular units in these areas are mainly single-haired. The lateral aspect of the face includes the sideburns, the cheek beard, the jawline beard, the submandibular beard, and the lateral portion of the upper part of the neck. The highest point of the cheek beard lies on the intersection of two lines: (a) the line joining the glabella to the angle of the mandible and (b) the line joining the angle of the mouth to the tragus. The upper border of the cheek beard should lie below the second line with upward convexity through the highest point. However, the points may vary as per the individual facial proportions.
While all components of a beard were considered important by men, the highest ranked “very important” features included “strong goatee” (15.8%) and “strong cheek beards” (15.4%) ( Table 2 ). The neck-beard extending below the jawline in the submandibular region can have whorls and is rarely reconstructed unless asked for. It has a high degree of variability in angles and directions and poses a great challenge for the surgeon when the restoration is needed ( Fig. 2 ).
Table 2. Subdivision of face for the purpose of facial hair restoration 9 .
| Zone | Subdivision | |
|---|---|---|
| Frontal zone | 1 | Moustache |
| 2 | Goatee | |
| 3 | Central portion of upper part of neck | |
| Lateral zone | 4 | Sideburns |
| 5 | Cheek beard | |
| 6 | Jaw beard | |
| 7 | Submandibular beard extending up to the neck | |
| 8 | Lateral portion of upper part of neck | |
Fig. 2.
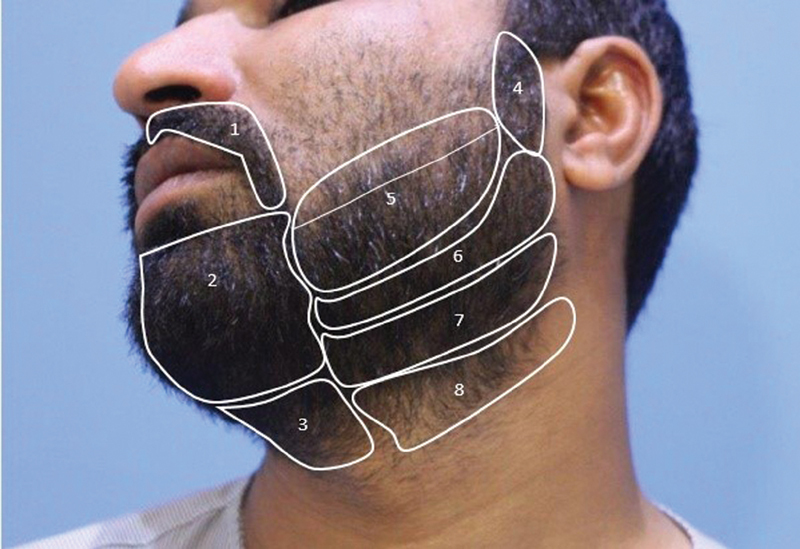
Different zones over the face for the purpose of beard hair restoration as enumerated in Table 2 .
At puberty, androgenic hair, specifically in the beard, transitions to become terminal hair and continues to increase in density until midthirties. The beard hair is coarser than the scalp, and has a larger root and a blunter tip, making it typically triangular in shape. 10 The density of hair is less over the beard as compared to that on the scalp. Dr. Chiara Inasalaca, in her study, determined that the average number of hair per graft in the beard was one, average follicular unit density was 65, and average hair density was 70. 11 However, the author observed the density to be very high, from 45 to 50 FU/cm 2 over the cheek area and 75 to 80 FU/cm 2 over the chin area. Moustache hairs were of even higher density, of about 85 to 90 FU/cm 2 laterally and 150 to 160 FU/cm 2 in the central area, pertaining to the fact that Middle Easterners and Southeast Asians have the highest beard densities of all ethnicities. 12
Indications
Beard or moustache reconstruction is needed if there is an absence of the same in case of congenital atrichia or in cases where the follicular density is less than desired. Few such indications are as follows:
Scars due to trauma, burns, or surgery 13 14 ( Figs. 3 and 4 ).
Traction alopecia, most commonly observed in the Sikh community in India due to the tradition of tying their beard as it grows longer ( Fig. 5 ).
Long-standing alopecia areata.
Stable cicatricial alopecia in the beard region: lichen planopilaris, frontal fibrosing alopecia in the sideburn area, and so forth.
Postfolliculitis scarring.
Correction of previously transplanted beard.
Cosmetic enhancement of already existing beard or moustache to attain certain desired styling.
Moustache reconstruction in cases of cleft lip repair.
Fig. 3.
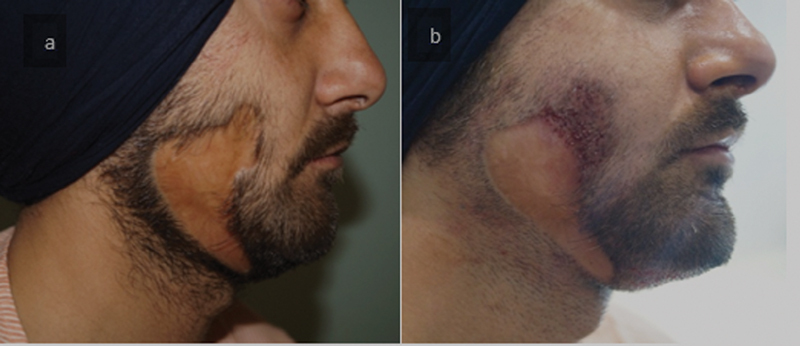
( a ) Scar due to burn and ( b ) the test patch done to check the viability of tissue and subsequent survival of grafts.
Fig. 4.
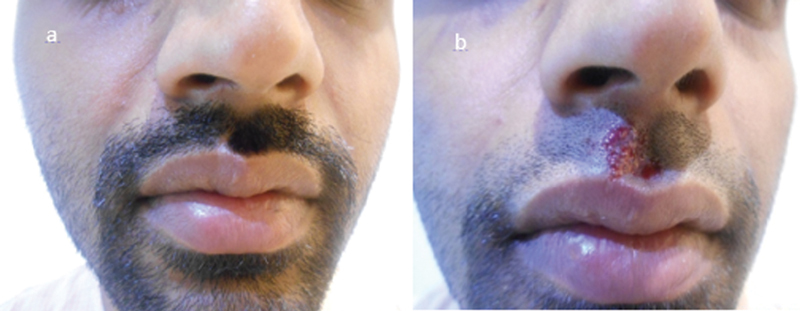
( a ) Traumatic scar. ( b ) After scar revision with single follicular units.
Fig. 5.

(a) Traction alopecia. (b) Results after 1 year.
Fig. 6.

(a) Congenital hypotrichia. (b) Immediate postoperative picture with grafts.
Fig. 7.

(a) Congenital atrichia. (b) Results after 1 year.
Preoperative Considerations
A detailed medical history of the patient along with examination of the face with the anatomical landmarks is mandatory to plan the requirement and distribution of grafts as per the patient's expectations.
Any history of bleeding tendencies, diabetes, hypertension, any relevant drug history, allergies, and scarring tendencies should be taken just like any other surgery. In case of any pre-existing skin pathology, biopsy should be taken to confirm the diagnosis and to determine the activity of the disease, specifically in cases of cicatricial alopecia.
Counseling
Counseling plays a major role in achieving satisfactory result from any aesthetic procedure. Understanding the patient's expectations from the procedure and discussing the surgical limitations beforehand can enhance the patient's experience and also prevent any discrepancy in future.
The most common indication that is encountered for facial hair reconstruction is congenital hypotrichia or atrichia. 15 In such cases, 2,000 to 2,500 grafts are required to attain the desired density. The primary goal of any facial hair restoration procedure is to provide good density, but patients should always be forewarned that the single procedure may not be enough to attain the desired look and sometimes a second sitting is needed to attain the best possible outcome.
The diameter of hair over scalp is anywhere between 25 to 125 µm. 10 It has relatively smaller root, tapered tip, and is usually medullated. Beard hair is coarser than scalp hair, and has a larger root and a blunter tip. 16 The difference in the characteristics of scalp hair and beard hair can provide near to natural results and same should be explained to patient. The midoccipital region of the scalp donor area is preferred as the hair in this region has caliber and texture almost equivalent to hair in beard and moustache area. The patient must be informed about the long hours of the surgery and a detailed plan of execution should be made. He should be prepared for frequent changing of position and multiple pricks during anesthesia.
Detailed planning sheet with patient details, time required for each step of surgery, and the team members responsible for each step minimizes the total duration of the procedure helps to make the surgery smooth for both the patient as well as the doctor's own team.
Operative Considerations
Local Anesthesia
The authors give nerve blocks to limit the pain from multiple injections as the infiltration of the local anesthesia can be very painful over face. Using a vibrator and 26 gauge × 1.5 in hypodermic needle can minimize the number of pricks and make the procedure more comfortable ( Fig. 8 ).
Fig. 8.
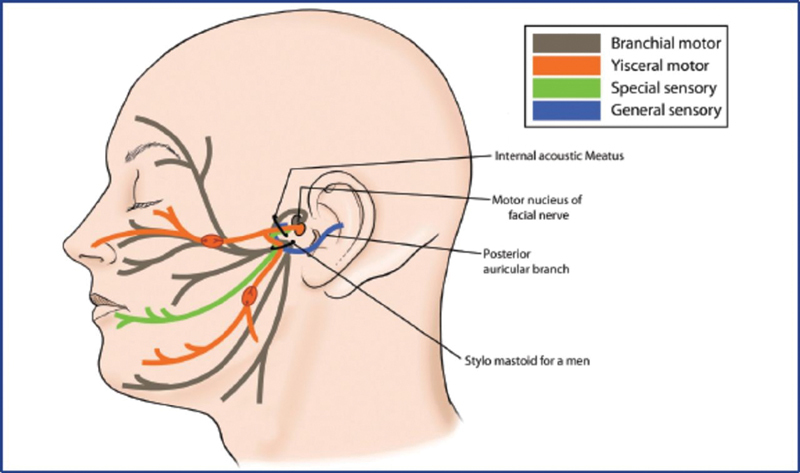
Nerve supply of the face.
Auriculotemporal nerve block: The auriculotemporal nerve is a branch of the mandibular nerve that runs with the superficial temporal artery and vein and supplies the skin over the parotid gland, the external ear. It is blocked by inserting needle 1.5 cm anterior to the ear, at the level of tragus behind the superficial artery pulsations, and injecting around 1 mL of 2% lidocaine with 1:200,000 adrenaline. 15
Infraorbital nerve block: Infraorbital nerve is a branch of maxillary nerve which emerges from the infraorbital foramen, located 6 to 10 mm below the infraorbital margin in the midpupillary line. The block is achieved by giving 2 mL of 2% lignocaine with 1:100,000 adrenaline via intraoral route and aids in anesthetizing the infraorbital area, the upper lip, and the moustache area.
Mental nerve block: Mental nerve is a branch of mandibular nerve which emerges through the mental foramen located on the anterior surface of mandible on the midpupillary line. This can be achieved by injecting 2 mL of 2% lignocaine with 1:100,000 adrenaline into the mental foramen, either via intraoral route or transcutaneous route.
Field blocks: After the nerve blocks, field anesthesia is given into deep dermal subcutaneous tissue as the needle is withdrawn slowly as it minimizes the pain due to anesthesia. 16 It can be achieved in the overall field by starting in front of the tragus and going downward along the posterior border of the ramus toward the angle of mandible, and then along the inferior border toward the midline. Once the lower border of the area is anesthetized, anesthesia can be injected along the upper border of the designed beard, starting from tragus going downward and anteriorly to the angle of the mouth.
Donor Area Harvesting
The midoccipital area of the scalp is preferred as the donor area where grafts can be taken from either by follicular unit transplantation (FUT) or follicular unit excision (FUE) technique. During excision, mostly single or two hair grafts are selectively excised. Wherever the caliber of scalp hair is less as compared to beard, two follicular unit grafts or paired FUs can be used. If the grafts requirement is around 300 to 400, as seen in cases of small scars and moustache reconstruction, and wherever patient finds it convenient, grafts can be taken from the undersurface of the beard by FUE technique ( Fig. 9 ).
Fig. 9.
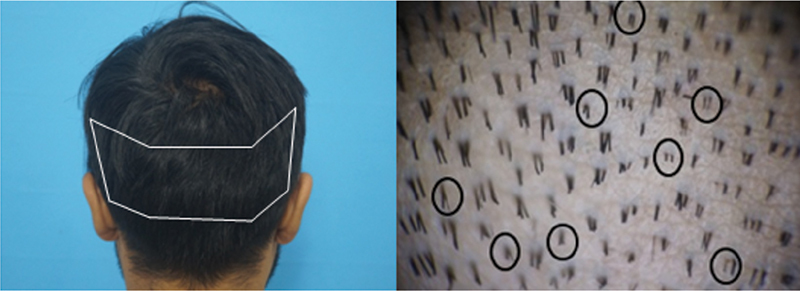
Midoccipital region on the scalp provides the most optimal grafts which match the caliber and texture of the beard hair. Selecting single and double unit grafts during extraction provides much better yield for maximal coverage.
Recipient Area Slit Making
Ideally, a 0.8 to 0.9 mm cut-to-size (CTS) chisel-shaped blade can be used to create the coronal slits so as to minimize the difficulties during implantation, while some surgeons still prefer to use hypodermic needle to give the slits. Coronal slits are much better because of the smaller size comparatively. Superficial tumescence is given all over the facial area to minimize the laxity of facial skin and to create the slits with the appropriate direction and angulation. The slits are directed at the angle of 10° to 20° along the plane of the skin. The traction provided by the assistant also aids in making slits into loose facial skin but can cause distortion of angulation at certain sites.
Frontal Zone Planning for Beard Hair Reconstruction
The frontal aspect of the face includes mainly moustache and goatee which play an important role in enhancing the secondary sexual characteristics attained with beard in men. Hence, it requires more number of grafts comparatively. Around 1,000 to 1,100 grafts are needed to reconstruct moustache and a dense goatee.
Moustache : The natural direction of the hair in the moustache area is slightly outward and downward, so the direction of the slits should be made in alignment with the pre-existing hair or to mimic the natural look. The authors earlier preferred to give the sagittal slits in this area but now prefer to give the coronal slits as the size of the slit is smaller and is better aligned to prevent cobblestoning. This gives much satisfactory results in this area where the density is kept higher on the upper edge as compared to the lower half. This provides a layering effect that gives an illusion of density with a minimal number of grafts. Also, giving higher density in the philtrum provides much better aesthetic results. Placement of single unit grafts on the upper edge provides much natural results. Around 300 to 400 grafts on each side are required with a density of around 35 to 40 grafts/cm 2 to attain desirable results. 15
Goatee : The moustache on both sides runs along the lateral border of the mouth downward where it reaches the chin area to become the lateral goatee. The goatee area requires slits with acute angulation which are parallel to the skin. The slits are directed downward and are made as flat as possible. Excessive caution is needed while making slits in this area as the excessive traction to make slits in the area joining lips to the goatee can cause tears across the inner labial surface and can touch teeth as well. It may require 600 to 700 grafts alone at the density of 35 to 40 grafts/cm 2 .
Lateral Zone Planning for Beard Hair Reconstruction
Sideburns : While creating the sideburns and the cheek portion of the beard, coronal slits are preferred as it ensures proper alignment of the hair keeping the angle acute and directed downward and parallel to existing hair. The number of grafts required may be 200 on each side. The upper part of the sideburns can be made denser to achieve a fuller look as the hair will grow longer in the downward direction and provide an overlapping effect and better coverage.
Cheek beard : It is advised to make slits in the skewed pattern over the area of the cheek as the hair runs laterally and downward. It is quite big a zone which can be further divided into two parts: the border and the body. In the cheek border, it is advised to give less density with single hair grafts to attain the soft, feathering look whereas in the body of the cheek, maximum density is obtained as to achieve the fuller look of the beard.
Jawline beard : The cheek beard, sideburns, and goatee are the areas that are majorly targeted during the reconstruction of the beard. The jawline beard is reconstructed with minimal grafts as it gets coverage from the overlapping effect of the grafts placed in the cheek beard. The conservative approach includes transplanting the grafts in cheek area first as much as possible and then targeting the submandibular or jaw beard if needed so as to achieve the dense look in the most visible areas. The shadow area, that is, the submandibular area gets concealed anyway on keeping the hair on the cheek beard longer.
Implantation
Implantation is a challenging task for the team and requires skilled placers due to the laxity and the movability of the facial skin. There is an increased risk of bleeding as the face is quite vascular. It can be a daunting task ergonomically as only one placer can implant at one go, thus increasing the time duration of the entire procedure. Excessive trauma to the superficial nerves can also result in transient paralysis of the facial muscles.
The single hair grafts are placed using Jeweller's forceps at the border of the cheek beard to give a natural look, as done during hairline designing over the scalp. This enhances the cosmetic look of the beard and provides a softer look at the edges. Single and two follicular unit grafts can be placed in the body of the cheek beard and jaw beard to achieve a fuller and dense look ( Fig. 10 ). Premade slits can be made to minimize the out-of-body time of grafts but it can also pose a challenge as the slits can get closed by the time of implantation. The same can be reopened by applying counter traction and stretching the skin simultaneously. This can aggravate the bleeding or oozing at the local site. Alternatively, implanters or stick and place methods can be used to minimize the bleeding.
Fig. 10.

Image demonstrating placement of grafts for achieving better aesthetic look from beard hair transplant.
Postoperative Considerations
The patient might have numbness in the treated area and may find it difficult to chew food and may have drooling due to local anesthesia. Therefore, patient is advised to take either fluids or semisolid diet on the day of the surgery. This can be followed by semisolid food on the second day. For the first 5 days, the transplanted area should be kept moist. This helps to decrease the scab formation and allows the hair to set properly. Antibiotics and analgesics are given for 7 days and shaving can be done from eighth day onwards. Tumescence can result in facial edema and ecchymosis which disappears eventually over a week's duration. The results from the transplant start to become visible as early as 3 months and keep improvising over the span of one year. The transplanted hair may sometimes not have the desired angulation or direction as the follicles may shift during the healing process due to the laxity of the skin.
Complications
The following complications may occur:
Bumpiness or irregularity of skin can happen in the transplanted area, especially the goatee and moustache area ( Fig. 11 ).
Improper direction of grafts when not placed in ultra-acute angles. However, with proper technique and usage of the smallest slits, these complications can be minimised.
Mild redness and slight swelling in the facial area for a few days after the procedure, is common and will reduce in 2 to 3 days.
The patient may also have some cobblestoning, mainly in the central part right below the lower lip comprising of soul patch and chin mound. 17 This can be avoided by de-epithelization of grafts before implantation or doing microdermabrasion after few months of the procedure ( Fig.12 ).
Fig. 11.

Bumpiness and redness of skin seen 5 days after the hair.
Fig. 12.

Cobblestoning.
Conclusion
Beard and moustache transplantation is in vogue now with the ever increasing demand among men. A skilled surgeon with his trained team can achieve near natural results by refining the technique further. Recent advancements in the facial hair restoration has also provided base to the novice surgeons to gain the skill while providing satisfactory results to the patient ( Figs. 13 ).
Fig. 13.

Results for the case of hypotrichia where 1,800 grafts were implanted using the FUE technique.
Footnotes
Conflict of Interest None declared.
References
- 1.Vallis C P. Hair transplantation to the upper lip to create a moustache. Case report. Plast Reconstr Surg. 1974;54(05):606–608. doi: 10.1097/00006534-197411000-00018. [DOI] [PubMed] [Google Scholar]
- 2.Kumar P. L-shaped scalp flap for moustache reconstruction in a patient with an acid burn of the face. Burns. 1996;22(05):413–416. doi: 10.1016/0305-4179(95)00158-1. [DOI] [PubMed] [Google Scholar]
- 3.Brandy D A. Chest hair used as donor material in hair restoration surgery. Dermatol Surg. 1997;23(09):841–844. doi: 10.1111/j.1524-4725.1997.tb00428.x. [DOI] [PubMed] [Google Scholar]
- 4.Agrawal K, Panda K N. Moustache reconstruction using an extended midline forehead flap. Br J Plast Surg. 2001;54(02):159–161. doi: 10.1054/bjps.2000.3517. [DOI] [PubMed] [Google Scholar]
- 5.Reed M L, Grayson B H. Single-follicular-unit hair transplantation to correct cleft lip moustache alopecia. Cleft Palate Craniofac J. 2001;38(05):538–540. doi: 10.1597/1545-1569_2001_038_0538_sfuhtt_2.0.co_2. [DOI] [PubMed] [Google Scholar]
- 6.Barrera A. Hair transplantation. St. Louis (MO): Quality Medical Publishing, Inc.; 2002. Restoration of the eyebrows, mustache and beard; p. 158. [Google Scholar]
- 7.Keene S A, Ceh V, Sideris K. 2020 ISHRS practice census offers key insights on hair restoration practices and procedures. Hair Transplant Forum Int. 2020;30(03):97. [Google Scholar]
- 8.Leonard R T, Sideris K. Practice census finds robust growth in hair restoration surgery over the years. Hair Transplant Forum Int. 2013;23(06):214–215. [Google Scholar]
- 9.Dua K.102: Focused Session—Eyebrows, Beard, and Body HairIn: Virtual 2020 ISHRS 28th World Congress.2020 [Google Scholar]
- 10.Garn S M. Types and distribution of the hair in man. Ann N Y Acad Sci. 1951;53(03):498–507. doi: 10.1111/j.1749-6632.1951.tb31952.x. [DOI] [PubMed] [Google Scholar]
- 11.Sethi P, Bansal A, Kumar A. New Delhi, India: Jaypee Brothers Medical Publishers (P) Ltd; 2019. Body hair transplant; p. 110. [Google Scholar]
- 12.True R, Dua K, Akaki T. Beard chat. Hair Transplant Forum Int. 2015;25:156. [Google Scholar]
- 13.Barr L, Barrera A. Use of hair grafting in scar camouflage. Facial Plast Surg Clin North Am. 2011;19(03):559–568. doi: 10.1016/j.fsc.2011.06.010. [DOI] [PubMed] [Google Scholar]
- 14.Rajput R. Postburns hair restoration of eyebrow, eyelash, moustache, beard and scalp areas. Ind J Burn. 2015;23(01):26–31. [Google Scholar]
- 15.Dua K, Chahar M. New Delhi, India: Jaypee Brothers Medical Publishers Ltd.; 2016. Facial hair transplantation; pp. 313–320. [Google Scholar]
- 16.Arndt K A, Burton C, Noe J M. Minimizing the pain of local anesthesia. Plast Reconstr Surg. 1983;72(05):676–679. doi: 10.1097/00006534-198311000-00017. [DOI] [PubMed] [Google Scholar]
- 17.Epstein J. Facial hair restoration: hair transplantation to eyebrows, beard, sideburns, and eyelashes. Facial Plast Surg Clin North Am. 2013;21(03):457–467. doi: 10.1016/j.fsc.2013.05.004. [DOI] [PubMed] [Google Scholar]