

Abstract
Objectives
The coronavirus disease 2019 (COVID-19) pandemic has set a precedent for the fastest-produced vaccine as a result of global collaboration and outreach. This study explored Malaysians’ acceptance of the COVID-19 vaccine and its associated factors.
Methods
A cross-sectional anonymous web-based survey was disseminated to Malaysian adults aged ≥18 years old via social media platforms between July 10, 2020 and August 31, 2020.
Results
In the analysis of 4,164 complete responses, 93.2% of participants indicated that they would accept the COVID-19 vaccine if it was offered for free by the Malaysian government. The median out-of-pocket cost that participants were willing to pay for a COVID-19 vaccine was Malaysian ringgit (MYR) 100 (interquartile range [IQR], 100) if it was readily available and MYR 150 (IQR, 200) if the supply was limited. Respondents with a low likelihood of vaccine hesitancy had 13 times higher odds of accepting the COVID-19 vaccine (95% confidence interval [CI], 8.69 to 19.13). High perceived risk and severity were also associated with willingness to be vaccinated, with adjusted odds ratios of 2.22 (95% CI, 1.44 to 3.41) and 2.76 (95% CI, 1.87 to 4.09), respectively. Age and ethnicity were the only independent demographic characteristics that predicted vaccine uptake.
Conclusion
Public health strategies targeting perceived risk, perceived susceptibility and vaccine hesitancy could be effective in enhancing vaccine uptake.
Keywords: COVID-19, COVID-19 vaccines, SARS-CoV-2 vaccine, Surveys and questionnaires
Introduction
It has been over a year since coronavirus disease 2019 (COVID-19) emerged as the greatest global health crisis of the century, with wide-reaching economic, social, and environmental impacts. From its humble origins as a novel cluster of pneumonia cases in China, the number of current infections worldwide as of May 10, 2021 stands at 157.9 million, with a global death toll of nearly 3.3 million [1]. In Malaysia, the first reported case of COVID-19 occurred on January 25, 2020, marking the beginning of the first wave of COVID-19 infections in Malaysia [2]. Buoyed by the emergence of several clusters, the rate of infections began to escalate rapidly. Since then, the country has undergone 2 additional waves; the second started on February 27, 2020 and an ongoing third wave started on September 8, 2020. Various stages of movement control orders (MCOs) have since been implemented by the Malaysian government in an attempt to contain the outbreak. Thus far, the third wave has proved to be the most severe, with daily infections reaching a record high of 5,725 on January 29, 2021 [3]. Only with the reintroduction of the MCO restrictions on January 11 did the rate of infections start to show a gradual decline. As of May 8, 2021, the number of cumulative infections in Malaysia reached 444,484, with 1,700 deaths [4].
Since the announcement in early November 2020 by Pfizer-BioNTech that the COVID-19 vaccine was 90% effective [5], the United Kingdom and United States (US) responded swiftly by authorising the emergency use of this vaccine, which is also known as the Comirnaty COVID-19 mRNA vaccine. This was followed by approval for emergency use by the World Health Organization (WHO) a month later [6]. The Malaysian government similarly mounted a prompt response with the implementation of the national COVID-19 immunisation plan across 3 phases, with the first beginning on February 24, 2021 and lasting until April [7]. The target population for the first phase are front-liners, particularly those in the medical profession. Subsequently, the second phase (April to August 2021) involved senior citizens aged 65 and above, high-risk groups, and disabled, and the third phase (May to February 2022) will cover both citizens and non-citizens aged 18 years and above. Based on latest estimates, it is predicted that approximately 60% to 75% of the population needs to be vaccinated in order to confer effective herd immunity against COVID-19 transmission [8,9]. Our national target is 80% of the population [10]. Hence, public acceptance and the role of the public will be of great consequence for achieving the intended goal of herd immunity. Nevertheless, polls on COVID-19 vaccine acceptance have exposed a perturbing trend in Malaysia. During the first wave in April 2020, a relatively high acceptance rate of 85% to 94% was demonstrated in polls conducted by an international market research company and a research team from Malaysia, respectively [11,12]. However, by December 2020, in the midst of the third wave and impending vaccination rollout, acceptance levels declined to 67%, a stark contrast from the earlier values [13].
Despite having standard monitoring mechanisms in place, uncertainties regarding safety profile and effectiveness remain the primary concerns. Extensive publicity highlighting adverse events in the early stages [14,15] and during the initial vaccination rollout [16] may have triggered negative perceptions and unfounded fears, ultimately contributing to reduced vaccine uptake. Several studies during previous influenza pandemics had adopted health behavioural theories to examine predictors of vaccination intent [17–19]. During the influenza pandemic in 2009, post-pandemic public polls reported poor uptake of the pandemic influenza vaccine in the general public, high-risk groups, and healthcare workers [20,21]. These failures stemmed from a breakdown in perceptions of risk, susceptibility, and vulnerability in the population. Therefore, this study aimed to provide a pre-emptive understanding of factors influencing acceptance of the COVID-19 vaccine amongst the Malaysian population. This will serve to guide interventions for future pandemic preparedness planning.
Materials and Methods
Study Population and Sampling
We conducted a cross-sectional anonymous survey using the Research Electronic Data Capture platform to disseminate a web-based self-administered questionnaire. This survey was done between July 10, 2020 and August 31, 2020. The survey was disseminated via various social media platforms such as Instagram, Twitter, LinkedIn, Facebook, WhatsApp, and Telegram. The target population was Malaysian adults aged 18 years old and above. All respondents were informed that their participation was anonymous and voluntary at the beginning of the survey. Consent was implied if the participants started answering the questionnaire.
Study Instrument
The questionnaire in this study was adapted from published literature during the previous H1N1 pandemic [22]. Questions were modified to fit the context of COVID-19 pandemic in accordance with the objective of this study. Furthermore, a few additional questions were adopted from the SAGE Working Group on Vaccine Hesitancy to assess the possibility of vaccine hesitancy [23].
During the process of questionnaire development, local experts, including healthcare professionals and academicians, proofread and validated the content. The questionnaire was developed in English and subsequently translated into Bahasa Malaysia and Mandarin. Pilot testing was done before study commencement, and the questionnaire was modified according to the feedback until no more amendments were needed. The final version of the questionnaire can be found in Supplementary Material 1. The questionnaire comprised questions that assessed (1) sociodemographic characteristics and COVID-19 experience; (2) vaccine hesitancy; (3) perceptions of risk and seriousness; (4) acceptability of the COVID-19 vaccine; (5) willingness to pay; and (6) attitudes towards the COVID-19 vaccine.
Sociodemographic characteristics and COVID-19 experience
The first part of the questionnaire collected basic sociodemographic data on age, sex, ethnicity, education level, monthly household income, occupation, and living arrangements (e.g., living with elderly individuals, children, and/or pregnant women). The respondents were also asked to indicate whether they or their family and friends had been infected with COVID-19 previously.
Vaccine hesitancy
All respondents were asked 4 items to assess vaccine hesitancy. Three items were assessed on a 5-point Likert-type scale. For the fourth item, respondents were asked to respond to the following statement “Have you ever declined vaccination for your child?” A simplified option of yes/no/not applicable was used for this item. Responses suggestive of vaccine hesitancy are shown in Table 1. These responses are given a score of 1 for each item, with a maximum score of 4. A score of 2 or more is considered to indicate a likelihood of vaccine hesitancy.
Table 1.
Responses suggestive of vaccine hesitancy
| Statement | Responses suggestive of vaccine hesitancy |
|---|---|
| My religion/physiology/culture recommends against vaccination. | Agree or strongly agree |
| Some groups or influential people are against vaccination for different reasons. Do you agree or disagree with these groups of people? | Agree or strongly agree |
| It is important for me to get recommended vaccines for myself and my children. | Disagree or strongly disagree |
| Have you ever declined vaccination for your children? | Yes |
Perceptions of risk and seriousness
Perceptions of risk and seriousness were measured using 3 items with responses on a 5-point Likert-type scale. Participants were asked about the risk level they perceived for themselves, the perceived risk for the general community in Malaysia, and the perceived seriousness of the disease if they contracted the infection.
Acceptability of the COVID-19 vaccine
One item assessed respondents’ perceived acceptability of the COVID-19 vaccine. The respondents were asked to choose yes, no, or unsure to describe their intention if a COVID-19 vaccine was made available to Malaysians for free. Respondents who answered no or unsure were prompted for reasons for refusal, while respondents who answered yes were asked about the maximum acceptable number of doses.
Willingness to pay
The willingness to pay for a COVID-19 vaccine under the circumstances of sufficient and limited supply was measured using 2 items. Both items were open-ended questions, where participants were allowed to input any amount between Malaysian ringgit (MYR) 0 and MYR 1,500 (approximately USD 360).
Attitudes towards the COVID-19 vaccine
The last part of the questionnaire contained 7 items assessing the attitudes of respondents towards a COVID-19 vaccine. All items were measured on a 5-point Likert-type scale.
Statistical Analysis
The responses were analysed using descriptive and inferential statistics. All categorical variables were expressed as frequencies and percentages, while continuous variables were expressed as means with standard deviations or medians with interquartile ranges (IQRs) depending on the distribution of data. For inferential analysis, we studied the factors associated with acceptance of COVID-19 vaccination. Logistic regression was used to assess statistical associations in univariate and multivariate analyses. Variables with a p-value<0.05 in the univariate analyses were included in the multivariate logistic regression analysis to identify independent predictors of COVID-19 vaccine uptake. Odds ratio (ORs) and 95% confidence intervals (95% CIs) were calculated. All statistical analyses were performed using R version 3.6.3, with the level of significance set at 5%.
In the analysis, responses regarding the level of agreement or risk level were collapsed into 3 levels (agree, not sure, disagree or low risk, medium risk, high risk). Under the vaccine hesitancy section, the level of agreement was dichotomised into agree (consisting of strongly agree and agree) or disagree (consisting of strongly disagree, disagree, and not sure) due to the small number of responses for not sure. Respondents who answered at least 2 out of the 4 questions pointing towards vaccine hesitancy were considered more likely to be vaccine-hesitant.
Results
Background Characteristics
In total, 4,164 complete responses were received during the survey period. Demographic profiles and COVID-19 experiences of the respondents are summarised in Table 2. The majority of the respondents were women (71.2%), with a median age of 37.0 years (IQR, 14 years), of Malay ethnicity (54.7%) and possessed at least tertiary education (74.5%). Slightly over half of respondents had an average monthly household income of over MYR 5,000 (58.4%), while the remainder earned less than MYR 5,000 (41.6%). Approximately one-third (31.2%) of the respondents were healthcare workers with the remainder being the general public (68.8%). A total of 61.7% lived with elderly individuals, children, and/or pregnant women. Nearly all respondents (99.6%) did not have a previous COVID-19 infection, whereas a small fraction of the respondents (6.5%) reported having family members or friends who had contracted COVID-19.
Table 2.
Background characteristics and their associations with COVID-19 vaccine acceptance
| Characteristic | Results (n=4,164) |
|---|---|
| Demographic profile | |
| Age (y) | 37.0 (31.0–45.0) |
| Sex | |
| Male | 1,200 (28.8) |
| Female | 2,964 (71.2) |
| Ethnicity | |
| Malay | 2,276 (54.7) |
| Chinese | 1,309 (31.4) |
| Indian | 285 (6.8) |
| Others | 294 (7.1) |
| Highest education level | |
| Up to high school education/technical skills/diploma or equivalent | 1,061 (25.5) |
| Tertiary education | 3,103 (74.5) |
| Average monthly household income | |
| <MYR 5,000 | 1,731 (41.6) |
| ≥MYR 5,000 | 2,433 (58.4) |
| Live with elderly/children/pregnant woman | |
| Yes | 2,570 (61.7) |
| No | 1,594 (38.2) |
| Occupation | |
| Healthcare workers | 1,298 (31.2) |
| Non-healthcare workers | 2,866 (68.8) |
| COVID-19 experience | |
| History of contracting COVID-19 infection | |
| Yes | 16 (0.4) |
| No | 4,148 (99.6) |
| Known any family members or friends infected with COVID-19 | |
| Yes | 272 (6.5) |
| No | 3,892 (93.5) |
Data are presented as median (interquartile range) or n (%).
COVID-19, coronavirus disease 2019; MYR, Malaysian ringgit.
Vaccine Hesitancy
In total, 137 (3.3%) respondents were identified as being more likely to have vaccine hesitancy sentiments. Although Malaysia is a multicultural and multi-ethnic country, most respondents (91.6%) did not think that their religion, philosophy, or culture was against vaccination. The majority (94.1%) agreed with the importance of receiving the recommended vaccination for themselves and their children. Among 2,809 respondents with children, only a minority stated that they would refuse vaccination for their children. Furthermore, only 7% of the respondents agreed with the views of the vaccine-hesitant population (Table 3).
Table 3.
Determinants of vaccine hesitancy among the respondents
| Statement | Result (n=4,164) |
|---|---|
| My religion/philosophy/culture recommends against vaccination | |
| Agree | 348 (8.4) |
| Disagree | 3,816 (91.6) |
| Some groups or influential people are against vaccination for different reasons. Do you agree or disagree with these groups of people? | |
| Agree | 290 (7.0) |
| Disagree | 3,874 (93.0) |
| It is important for me to get recommended vaccines for myself and my children | |
| Agree | 3,917 (94.1) |
| Disagree | 247 (5.9) |
| Have you ever declined vaccination for your children? | |
| Yes | 21 (0.5) |
| No | 2,788 (67.0) |
| Not applicable | 1,355 (32.5) |
| Vaccine hesitancy | |
| Probable | 137 (3.3) |
| Not likely | 4,027 (96.7) |
Data are presented as n (%).
Perceptions of Risk and Seriousness
The respondents perceived that there was a higher risk of COVID-19 infection among the general Malaysian population than for themselves (Table 4). Nearly half (49.5%) of the respondents ranked Malaysian residents to be at high risk of becoming infected with COVID-19 during this pandemic. However, the self-perceived risk of contracting COVID-19 was more evenly distributed across the different risk levels. Interestingly, the respondents had high perceptions of severity. Almost two-thirds of the respondents perceived that their health would be seriously affected if they were infected with COVID-19.
Table 4.
Respondents’ perceived risk and severity
| Perception of risk and severity | Result (n=4,164) | |
|---|---|---|
| How likely is it for a Malaysian resident to get infected by COVID-19 during this pandemic? | ||
| High | 2,061 (49.5) | |
| Medium | 1,615 (38.8) | |
| Low | 488 (11.7) | |
| What is the risk for you to get infected by COVID-19 during this pandemic? | ||
| High | 1,491 (35.8) | |
| Medium | 1,448 (34.8) | |
| Low | 1,225 (29.4) | |
| If you were infected with COVID-19, how seriously do you think it would affect your health? | ||
| Severe | 2,768 (66.5) | |
| Moderate | 1,052 (25.3) | |
| Mild | 344 (8.3) |
Data are presented as n (%).
COVID-19, coronavirus disease 2019.
Acceptability of the COVID-19 Vaccine and Willingness to Pay
The acceptance rate of the COVID-19 vaccine was generally high at 93.2%, while the remaining respondents answered either no (2.1%) or unsure (4.7%) if they were offered the COVID-19 vaccine for free by the Malaysian government. The median willingness to pay for a COVID-19 vaccine was 50% higher if the supply was limited than if it was readily available, with values of MYR 150 (IQR, 200) and MYR 100 (IQR, 100), respectively.
Among the 3,882 participants who responded yes for COVID-19 vaccine intent, 1,702 (43.8%) felt that the number of doses did not matter to them. The proportion of participants who would accept more than a single dose of the COVID-19 vaccine was rather high, with only 262 of them (6.7%) choosing 1 dose as the maximum acceptable dose. However, very few (n=36, 0.9%) would accept a maximum of 4 doses. As for the others, the maximum number of acceptable doses for the COVID-19 vaccine ranged between 2 (n=1,023, 26.4%) and 3 (n=859, 22.1%) doses (Figure 1).
Figure 1.
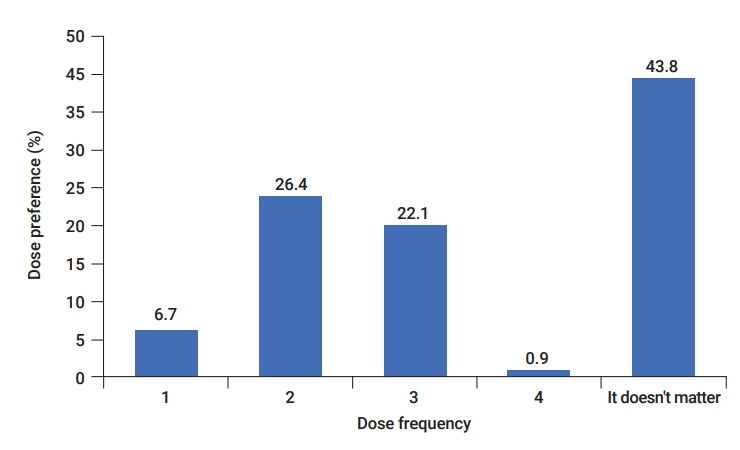
Maximum acceptable number of doses if the vaccination needs to be received in stages for those who accepted the coronavirus disease 2019 (COVID-19) vaccine.
For the respondents who had negative responses or were unsure of their COVID-19 vaccine intent, the top 3 concerns were the adequacy of vaccine testing (77.7%), its effectiveness (63.8%), and side effects (57.1%) (Table 5).
Table 5.
Reasons for refusing the COVID-19 vaccine
| Reason | Result (n=282) |
|---|---|
| I am concerned that the vaccine has not been tested adequately | 219 (77.7) |
| I am concerned regarding the effectiveness of the vaccine | 180 (63.8) |
| I am afraid of the side effects | 161 (57.1) |
| I am concerned that taking the COVID-19 vaccine will cause me to get the disease | 47 (16.7) |
| I think my chances of being infected are low | 42 (14.9) |
| I am afraid of pain | 21 (7.4) |
| COVID-19 will only cause a mild illness | 21 (7.4) |
Data are presented as n (%).
COVID-19, coronavirus disease 2019.
Factors Associated with Acceptance of the COVID-19 Vaccine
Table 6 summarises the univariate and multivariate analyses of factors associated with acceptance of the COVID-19 vaccine. Stepwise multivariate regression analysis (backward method) was performed, and the variables selected were age, race, vaccine hesitancy sentiments, perceived population risk of contracting COVID-19 and risk to health. In the final model, variables that were important indicators of vaccine acceptance were added to the multivariate regression model. The Hosmer-Lemeshow test was used to test the goodness of fit of the model (p=0.582, χ2=4.702). All variables were checked for interaction and multicollinearity. The variance inflation factor (VIF), which was used for collinearity analysis, indicated low correlations among the investigated variables (VIF<2). Older participants were less likely to accept the COVID-19 vaccine. With every 1-year increase in age, there was a 3% lower likelihood of accepting the vaccine (0.97; 95% CI, 0.96 to 0.98). In terms of ethnicity, the odds of being willing to accept the COVID-19 vaccine among Malays was 2.4 and 1.9 times higher than that among Chinese and Indians, respectively. The associations between COVID-19 vaccination intent and other sociodemographic factors (e.g., sex, education level, monthly household income, occupation, and living arrangement) were not statistically significant. A low likelihood of vaccine hesitancy sentiments (adjusted odds ratio [AOR], 12.89; 95% CI, 8.69 to 19.13) showed the strongest association with acceptance of the COVID-19 vaccine. Additionally, respondents who perceived a high risk for the general community to contract COVID-19 were more than 2 times as likely to be willing to receive the COVID-19 vaccine than those with a low-risk perception (AOR, 2.22; 95% CI, 1.44 to 3.41). Although the self-perceived risk of COVID-19 infection was associated with COVID-19 vaccination intent in the univariate analysis, it was not significant when adjusted for other variables. Participants who perceived their health would be seriously affected if they were infected with COVID-19 had significantly higher odds of accepting the COVID-19 vaccine than those who perceived a low level of severity (AOR, 2.76; 95% CI, 1.87 to 4.09). However, previous COVID-19 experience did not influence the acceptance of COVID-19 vaccination.
Table 6.
Univariate and multivariate logistic regression of factors associated with acceptance of the COVID-19 vaccine
| Characteristic | Univariate analysis |
Multivariate analysis |
||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | AOR | 95% CI | p | |
| Age (y) | 0.96 | 0.95–0.97 | <0.001 | 0.97 | 0.96–0.98 | <0.001* |
| Sex | ||||||
| Female | 1 (reference) | 1 (reference) | ||||
| Male | 0.74 | 0.58–0.96 | 0.023* | 1.10 | 0.82–1.49 | 0.633 |
| Ethnicity | ||||||
| Malay | 1 (reference) | 1 (reference) | ||||
| Chinese | 0.42 | 0.33–0.55 | <0.001* | 0.39 | 0.29–0.52 | <0.001* |
| Indian | 0.40 | 0.27–0.62 | <0.001* | 0.47 | 0.29–0.77 | 0.004* |
| Others | 1.00 | 0.58–1.89 | 0.706 | 1.05 | 0.57–2.07 | 0.808 |
| Education level | ||||||
| Secondary education and below | 1 (reference) | |||||
| Tertiary education | 0.85 | 0.64–1.13 | 0.27 | |||
| Average monthly household income | ||||||
| <MYR 5,000 | 1 (reference) | |||||
| ≥MYR 5,000 | 0.86 | 0.67–1.11 | 0.248 | |||
| Live with elderly, children, or pregnant woman | ||||||
| No | 1 (reference) | |||||
| Yes | 1.21 | 0.95–1.54 | 0.126 | |||
| Occupation | ||||||
| Non-healthcare workers | 1 (reference) | |||||
| Healthcare workers | 1.25 | 0.95–1.64 | 0.113 | |||
| History of contracted COVID-19 | ||||||
| No | 1 (reference) | |||||
| Yes | 0.51 | 0.14–3.24 | 0.296 | |||
| Known any family members of friends infected with COVID-19 | ||||||
| No | 1 (reference) | |||||
| Yes | 1.26 | 0.76–2.25 | 0.394 | |||
| Likelihood of vaccine hesitancy sentiments | ||||||
| High | 1 (reference) | 1 (reference) | ||||
| Low | 15.8 | 12.2–20.64 | <0.001* | 12.92 | 8.70–19.18 | <0.001* |
| How likely it is for a Malaysian resident to get infected by COVID-19 during this pandemic | ||||||
| Low | 1 (reference) | 1 (reference) | ||||
| Medium | 2.17 | 1.59–2.95 | <0.001* | 1.38 | 0.93–2.04 | 0.028 |
| High | 3.94 | 2.84–5.47 | <0.001* | 2.02 | 1.29–3.14 | <0.001* |
| What level of risk do you think you have of catching COVID-19 during this pandemic? | ||||||
| Low | 1 (reference) | 1 (reference) | ||||
| Medium | 1.81 | 1.36–2.41 | <0.001* | 1.27 | 0.90–1.79 | 0.248 |
| High | 2.42 | 1.79–3.30 | <0.001* | 1.20 | 0.81–1.78 | 0.433 |
| If you were infected with COVID-19, how seriously do you think it would affect your health? | ||||||
| Low | 1 (reference) | 1 (reference) | ||||
| Medium | 1.88 | 1.30–2.69 | <0.001* | 1.26 | 0.82–1.92 | 0.023 |
| High | 3.52 | 2.49–4.92 | <0.001* | 2.28 | 1.50–3.41 | <0.001* |
COVID-19, coronavirus disease 2019; OR, odds ratio; CI, confidence interval; AOR, adjusted odds ratio; MYR, Malaysian ringgit.
R2=0.140, variance inflation factor<2, No interactions among covariates. Hosmer-Lemeshow goodness of fit test: χ2=4.7023, df=6, p=0.5825.
p<0.05.
Attitude towards the COVID-19 Vaccine
The participants were asked if they were concerned about adverse events, and 68.9% reported that they could readily accept the mild side effects of the COVID-19 vaccine. The respondents agreed that cost of the COVID-19 vaccine (53.9%) and halal certification (43.7%) were important considerations. Comparatively, only 1,285 (30.9%) felt that the country of origin was important when deciding whether to receive the COVID-19 vaccine. The majority (57.6%) believed that the vaccine will stop virus transmission, and 2,646 (63.5%) disagreed with the statement that only high-risk populations require vaccination. On a positive note, the participants had strong trust in the Malaysian government, with 88.2% expressing confidence in receiving the COVID-19 vaccine if the government advocated doing so (Table 7).
Table 7.
Attitude towards the COVID-19 vaccine
| Statement | Result (n=4,164) |
|---|---|
| I can readily accept the mild side effects of the COVID-19 vaccine. | |
| Agree | 2,867 (68.9) |
| Not sure | 714 (17.1) |
| Disagree | 583 (14.0) |
| The COVID-19 vaccine will stop the virus transmission. | |
| Agree | 2,397 (57.6) |
| Not sure | 1,230 (29.5) |
| Disagree | 537 (12.9) |
| Only high-risk groups such as children, pregnant women, elderly and those with underlying medical conditions need to be vaccinated with the COVID-19 vaccine. | |
| Agree | 1,069 (25.7) |
| Not sure | 449 (10.8) |
| Disagree | 2,646 (63.5) |
| I am confident in taking the COVID-19 vaccine if it is advocated by the Malaysian government. | |
| Agree | 3,674 (88.2) |
| Not sure | 333 (8.0) |
| Disagree | 157 (3.8) |
| The country of origin of the COVID-19 vaccine will influence my decision to take it. | |
| Agree | 1,285 (30.9) |
| Not sure | 1,031 (24.8) |
| Disagree | 1,848 (44.4) |
| The COVID-19 vaccine needs to be certified halal before I will take it. | |
| Agree | 1,818 (43.7) |
| Not sure | 516 (12.4) |
| Disagree | 1,830 (43.9) |
| The cost of the vaccine will affect my decision to take it. | |
| Agree | 2,245 (53.9) |
| Not sure | 807 (19.4) |
| Disagree | 1,112 (26.7) |
Data are presented as n (%).
COVID-19, coronavirus disease 2019.
Discussion
Our study showed that Malaysians generally had higher levels of acceptance of the COVID-19 vaccine than respondents from many countries [24–27]. This finding is further supported by Wong et al. [11], who reported a 94.3% rate of COVID-19 vaccination intent among Malaysians. According to a global survey involving 13,426 respondents from 19 countries, country-specific acceptance rates ranged between 54.9% and 88.6% [26]. However, these studies were done during the peak of the pandemic period. Hence, the acceptance rate would be likely to change if this study is repeated at a different stage of the pandemic [28]. This could likely be attributed to factors modulating vaccine hesitancy, including confidence in the healthcare system, health professionals, and policy-makers [23]. During the period when this survey was conducted, Malaysia had just entered the recovery movement control order phase, with the reopening of various economic sectors. The daily number of cases reported was trending towards single digits, with a general positive view on how the Malaysian government had tackled the COVID-19 pandemic [29]. Thus, vaccine acceptance rates were relatively high with government advocacy. This is consistent with several published studies reporting a significant positive association between trust in the government and vaccine uptake [23,30,31]. Several months later, in December, a public survey by the Ministry of Health Malaysia reported that the vaccine acceptance rate was 67%, in significant contrast to previous results [32]. By then, Malaysia had entered its third wave and was rife with pandemic fatigue, with palpable strain on the healthcare system and economy. Daily infections surged to 4 digits and continued on an upwards trend. Therefore, this highlights the need to capitalise on positive momentum to retain public confidence for a smooth and successful vaccination rollout in the future.
Vaccine hesitancy was named by the WHO as one of the top 10 threats to global health [33]. It is defined as delay or refusal of vaccinations despite availability and is influenced by complacency, convenience, and confidence. Similar to many countries, Malaysia has seen a rise in vaccine hesitancy in recent years [34,35]. As a Southeast Asian country, Malaysia has rich social, cultural, traditional, and religious elements that play a prominent role in influencing health behaviours. The vaccine hesitancy survey questions focused primarily on contextual, individual, and group influences, taking into account local literature highlighting the importance of religious and socio-cultural influences on vaccine hesitancy in Malaysia [36–38]. Nevertheless, only a small proportion of the study participants agreed that their religion and culture were against vaccination. In the National Health and Morbidity Survey 2016, concerns that the vaccines were not halal were cited as one of the reasons for vaccine hesitancy [39]. Nearly half of our study respondents wanted the COVID-19 vaccine to be certified as halal before agreeing to take it. This highlights the central role of religious authorities in promoting COVID-19 vaccination. After the influenza pandemic of 2008, few studies were done in Malaysia regarding vaccination hesitancy and uptake during the pandemic. Our findings showed that those whose answers implied vaccine hesitancy had a lower likelihood of accepting the vaccine. This is consistent with findings from many studies showing vaccine hesitancy to be a main contributor to poor vaccine uptake [40–42]. This is especially relevant in the midst of the COVID-19 pandemic fuelled with uncertainties, which are further accentuated by social media misinformation. Conspiracy theories have dominated social media, ranging from assertions that the COVID-19 pandemic is a hoax, that COVID-19 was spread on purpose [43] or more recently, that the COVID vaccine contains a microchip [44]. A study by Mohd Azizi et al. [38] found that the internet was the main source of information about vaccines in Malaysia and that misinformation contributed to vaccine reluctance. To put these findings into perspective, a week into the launch of the national COVID-19 immunisation plan in Malaysia, only 6.1% of the targeted 80% of the population had registered for the vaccine [45].
Multiple health behavioural theories and published studies have indicated individuals with high perceived risk and perceived seriousness had a higher likelihood of accepting the vaccine [46–48]. Recent studies on acceptance of the COVID-19 vaccine also found positive associations between vaccination intent and perceived susceptibility or perceived severity [24,25,49–51]. Although our study showed similar findings, the association between perceived personal risk level and acceptance of the COVID-19 vaccine was not statistically significant in the multivariate analysis. Interestingly, it was the perceived risk of the general community to be infected with COVID-19 that predicted vaccine acceptance among the participants. A cross-sectional survey of 1,159 Malaysians on their intent to receive the COVID-19 vaccine found that the majority (85.4%) were worried about the possibility of contracting COVID-19, but only 59.3% perceived their risk of infected with COVID-19 to be high [11]. These connections may be complex. For instance, individuals who are healthy or adhere to preventive measures (i.e., wearing a mask and physical distancing) may perceive their risk of contracting COVID-19 infection to be low, but still prefer to be vaccinated in view of the risk of community transmission. Nevertheless, we found that participants with high perceived severity were more likely to obtain the COVID-19 vaccine. Our findings highlighted the importance of increasing perceived risk and severity for COVID-19 among the public, as these beliefs may result in higher vaccine uptake. Some past public health programs targeting these beliefs have been successful in increasing vaccine uptake [52–54].
Published studies have suggested that COVID-19 vaccine acceptance can be predicted by various sociodemographic factors [24,25,27,49–51]. In our study, only age and ethnicity were found to be significant predictors of acceptance. Both Malik et al. [27] and Al-Mohaithef and Padhi [24] found that older individuals were more likely to accept the COVID-19 vaccine. However, our findings showed otherwise. This is a cause for concern considering the current evidence indicating that the elderly population is at higher risk of severe infections [55–57]. With the WHO and Malaysian government recommending the elderly population as a priority group to receive the COVID-19 vaccine [58,59], strategies need to be in place to ensure good vaccine uptake among the elderly. Interestingly, our study showed no significant difference in vaccine acceptance between the healthcare and non-healthcare worker groups, unlike in other studies [60]. This could be attributed to the study period, since the questionnaire was administered at a time when public fear was still predominant with no indication of a cure or vaccine. However, with more information available in tandem with the global COVID-19 vaccination rollout, acceptance levels will change. This may be particularly true among healthcare workers who depend on published scientific evidence to determine their intent to vaccinate. A study by Shekhar et al. [61] on COVID-19 vaccine acceptance among healthcare workers in the US in October to November 2020 found only one-third (36.0%) of respondents to be agreeable for vaccination immediately. In contrast, non-healthcare workers may be influenced by widely available information—be it misinformation, disinformation, or accurate information—that is easily accessible via social media. According to the report of the SAGE Working Group in Vaccine Hesitancy, religion and culture were identified as a determinant influencing vaccine uptake [23]. This may explain the difference in vaccine acceptance between the ethnic groups in our study. It is important to note that the population reflected by our respondents differs from the general Malaysian population. Based on statistics compiled by the Department of Statistics Malaysia, the median age of the Malaysian population is 29.2 years, with a slight male predominance (51.5% vs. 48.5%) [62]. Furthermore, the racial distribution of the Malaysian population is predominantly Malay (69.6%), followed by Chinese (22.6%), Indian (6.8%), and others (1.0%).
Over the past year, the pandemic has taken a considerable toll on the economic welfare of nations and their inhabitants. While high-income countries are able to procure excess doses for their citizens, this is inversely seen in lower- to middle-income countries [63]. Therefore, willingness to pay may be a strategic advantage for health systems facing budget constraints. Our study results imply that with limited availability, people may be more inclined to pay a higher price for the vaccine. Healthcare in Malaysia is divided into the government-funded system and the private sector. Perhaps, this could be a positive indicator that the private healthcare sector could play a greater role in the later parts of the national COVID-19 immunisation program. This situation is reminiscent of the influenza vaccine, which is readily available at private clinics and hospitals in Malaysia for a fee depending on the type [64]. Among numerous elements driving public confidence in vaccines, copious significance is placed on the safety and effectiveness of vaccines [49,50]. The recent information surrounding adverse events in the ongoing COVID-19 vaccine rollout may have a further impact on vaccine acceptance. Although only 14% of the study participants were unable to accept mild side effects of the COVID-19 vaccine, concerns about the adequacy of vaccine testing, vaccine effectiveness, and vaccine safety were the top reasons for participants who refused or were unsure about receiving the COVID-19 vaccine. While 57.6% of the study participants believed that the COVID-19 vaccine would help stop the virus transmission, some participants also were concerned about the cost and halal status of the COVID-19 vaccine. In adjunct to various concerns regarding the prospective vaccine, we asked respondents about the maximum number of acceptable doses to understand whether the number of doses would be a potential deterrent. Many of the respondents felt that the number of doses did not matter, likely due to their heightened perceived susceptibility and severity. Other studies centred on non-pandemic vaccines such as hepatitis B found that fewer doses were associated with better completion rates. It was also reported that an accelerated dosing schedule increased adherence. A study during the early stages of the COVID-19 pandemic in China similarly showed that there was a preference for fewer doses. With the current COVID-19 vaccination being mostly a 2-dose schedule, this may be one less problem affecting vaccine acceptance. Unfortunately, our study did not explore how additional vaccine characteristics would affect the public’s COVID-19 vaccination intent. It is recommended that future research should explore the key attributes influencing the public’s willingness to be vaccinated.
This study has a few limitations. Firstly, the study employed convenience sampling, and the nature of a web-based online survey also limits the participation of those without internet access or low digital literacy. Hence, we acknowledge limitations in replicating the demographic distribution to reflect the broader Malaysian population. Secondly, as participation in this survey was voluntary, there may have been some level of self-selection bias since the survey may have received more attention from those who were concerned about the COVID-19 pandemic and vaccine. Thirdly, this was a cross-sectional study collecting the public’s responses during a specific time frame. Therefore, the responses are only reflective of the information available during that time. The study did not explore other details (e.g., vaccine attributes and disease determinants) that could affect vaccine acceptance among the public. Next, our study assessed the COVID-19 vaccination intent with the assumption that the vaccine would be free. The acceptance level might be lower if out-of-pocket payments are incurred. Additionally, as this survey was conducted anonymously, we were unable to rule out the possibility of multiple entries from the same respondent. Last but not least, the use of a 5-point Likert scale for responses to survey questions may have resulted in some form of response bias. Merging the responses into 2 or 3 groups (whichever is applicable) could have resulted in some loss in the statistical interpretation of the findings on an ordinal scale.
Conclusion
In conclusion, most participants were willing to receive the COVID-19 vaccine. Willingness to receive the COVID-19 vaccine was affected by factors including age, race, perceived community risk to COVID-19 infection, perceived severity, and the absence of vaccine hesitancy sentiments. If the real-world acceptance level is similar to the findings of this study, Malaysia will be able to achieve herd immunity through its COVID-19 vaccination program. Further studies are warranted to explore the relative importance of various vaccine-related, contextual, and individual or group determinants associated with acceptance of the COVID-19 vaccine. Future public health strategies targeting these factors could help to increase vaccine uptake.
Footnotes
Ethics Approval
This study was registered with the National Medical Research Registry (NMRR-20-1089-55153). Ethical approval for this study was obtained from the Medical Research and Ethics Committee (MREC), Ministry of Health Malaysia (KKM/NIHSEC/ P20-1333 (4)). Participation in this survey was voluntary. All methods were performed in accordance with the Declaration of Helsinki. No personal identifiers were collected in the survey. Informed consent of the participants was implied when the participants started answering the questionnaire, as participation in the study was voluntary. The study was conducted anonymously; hence no personal identifiers were collected. Before answering the survey, all respondents were informed regarding the need to publish the results. We have obtained permission from the Director General of Health Malaysia to publish this article.
Conflicts of Interest
The authors have no conflicts of interest to declare.
Funding
None.
Availability of Data
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Authors’ Contributions
Conceptualization: JFWL,YLW; Data curation: JFWL, YLW; Data curation: JFWL, CTL; Formal analysis: JFWL, CTL, HST; Investigation: JFWL; Methodology: JFWL, YLW; Project administration: JFWL; Writing–original draft: JFWL; Writing–review & editing: all authors.
Additional Contributions
We would like to thank the Director General of Health, Ministry of Health (MOH) Malaysia for his permission to publish this study. We would also like to acknowledge the Director of the Institute for Clinical Research, MOH Malaysia for support throughout the study. We are grateful to Professor Dr. Liew Su May (University Malaya), Associate Professor Dr. Lim Lee Ling (University Malaya), Professor Dr. Philip Clarke (Oxford University), Dr. Laurence Roope (Oxford University) and Dr. Frauke Becker (Oxford University) for proofreading and validating the questionnaire. The authors also wish to thank those who participated in the survey and promoted the survey to their social networks.
Supplementary Material
Supplementary Material 1. Acceptance and perception on the COVID-19 vaccination (immunization) in the general population of Malaysia. Supplementary data are available at https://doi.org/10.24171/j.phrp.2021.0085.
Acceptance and perception on the Covid-19 vaccination (immunization) in the general population of Malaysia
References
- 1.John Hopkins University (JHU) COVID-19 dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU) [Internet] Baltimore: JHU; 2020 [cited 2021 May 10]. Available from: https://coronavirus.jhu.edu/map.html.
- 2.DG of Health KPK Press statement 25 January 2020-Detection of new cases confirmed infected with 2019 novel coronavirus (2019-nCoV) in Malaysia [Internet] General of Health Malaysia; 2020 [cited 2021 Jan 5]. Available from: https://kpkesihatan.com/2020/01/25/kenyataan-akhbar-kpk-25-januari-2020-pengesanan-kes-baharu-yang-disahkan-dijangkiti-2019-novel-coronavirus-2019-ncov-di-malaysia/
- 3.DG of Health KPK Press statement 29 January 2021-Current situation of coronavirus infection 2019 (COVID-19) in Malaysia [Internet] General of Health Malaysia; 2021 [cited 2021 Mar 7]. Available from: https://kpkesihatan.com/2021/01/29/kenyataan-akhbar-kpk-29-januari-2021-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/
- 4.DG of Health KPK Press statement 10 May 2021-Current situation of coronavirus infection 2019 (COVID-19) in Malaysia [Internet] General of Health Malaysia; 2021 [cited 2021 May 28]. Available from: https://kpkesihatan.com/2021/05/10/kenyataan-akhbar-kpk-10-mei-2021-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/
- 5.Pfizer Pfizer and BioNTech announce vaccine candidate against covid-19 achieved success in first interim analysis from phase 3 study [Internet] New York: Pfizer; 2020 [cited 2021 Mar 8]. Available from: https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-announce-vaccine-candidate-against.
- 6.World Health Organization (WHO) WHO issues its first emergency use validation for a COVID-19 vaccine and emphasizes need for equitable global access [Internet] Geneva: WHO; 2020 [cited 2021 Mar 11]. Available from: https://www.who.int/news/item/31-12-2020-who-issues-its-first-emergency-use-validation-for-a-covid-19-vaccine-and-emphasizes-need-for-equitable-global-access.
- 7.The special committee for ensuring access to COVID-19 vaccine supply (JKJAV). National COVID-19 immunisation programme [Internet] Putrajaya, Malaysia: JKJAV; 2021 [cited 2021 Nov 8]. Available from: https://www.vaksincovid.gov.my/pdf/Program_Imunisasi_COVID-19_Kebangsaan_Versi_Bahasa_Inggeris.pdf.
- 8.Billah MA, Miah MM, Khan MN. Reproductive number of coronavirus: a systematic review and meta-analysis based on global level evidence. PLoS One. 2020;15:e0242128. doi: 10.1371/journal.pone.0242128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Anderson RM, Vegvari C, Truscott J, et al. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet. 2020;396:1614–6. doi: 10.1016/S0140-6736(20)32318-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.PM: vaccination vital for herd immunity. The Star [Internet] 2021 Feb 22 [cied 2021 Mar 8]. Available from: https://www.thestar.com.my/news/nation/2021/02/22/pm-vaccination-vital-for-herd-immunity.
- 11.Wong LP, Alias H, Wong PF, et al. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum Vaccin Immunother. 2020;16:2204–14. doi: 10.1080/21645515.2020.1790279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ipsos Global attitudes : COVID-19 vaccines [Internet] Sarajevo: Ipsos; 2021 [cited 2021 Apr 5]. Available from: https://www.ipsos.com/en-ba/global-attitudes-covid-19-vaccine-january-2021.
- 13.World Health Organization (WHO) COVID-19 in Malaysia situation report 30 [Internet] Geneva: WHO; 2021 [cited 2021 May 28]. Available from: https://www.who.int/malaysia/internal-publications-detail/covid-19-in-malaysia-situation-report-30.
- 14.Visontay E. Oxford University Covid vaccine trial put on hold due to possible adverse reaction in participant. The Guardian [Inernet] 2020 Sep 9 [cited 2021 Jan 25]. Available from: https://www.theguardian.com/world/2020/sep/09/oxford-university-astrazeneca-covid-vaccine-trial-put-on-hold-due-to-adverse-reaction-in-participant.
- 15.Herper M. Johnson & Johnson Covid-19 vaccine study paused due to unexplained illness in participant. STAT [Internet] 2020 Oct 12 [cited 2021 Apr 5]. Available from: https://www.statnews.com/2020/10/12/johnson-johnson-covid-19-vaccine-study-paused-due-to-unexplained-illness-in-participant/
- 16.Glover RE, Urquhart R, Lukawska J, et al. Vaccinating against covid-19 in people who report allergies. BMJ. 2021;372:n120. doi: 10.1136/bmj.n120. [DOI] [PubMed] [Google Scholar]
- 17.Shahrabani S, Benzion U, Yom Din G. Factors affecting nurses' decision to get the flu vaccine. Eur J Health Econ. 2009;10:227–31. doi: 10.1007/s10198-008-0124-3. [DOI] [PubMed] [Google Scholar]
- 18.Allison MA, Reyes M, Young P, et al. Parental attitudes about influenza immunization and school-based immunization for school-aged children. Pediatr Infect Dis J. 2010;29:751–5. doi: 10.1097/INF.0b013e3181d8562c. [DOI] [PubMed] [Google Scholar]
- 19.Hu Y, Wang Y, Liang H, et al. Seasonal influenza vaccine acceptance among pregnant women in Zhejiang province, China: evidence based on health belief model. Int J Environ Res Public Health. 2017;14:1551. doi: 10.3390/ijerph14121551. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jimenez-Garcia R, Rodriguez-Rieiro C, Hernandez-Barrera V, et al. Negative trends from 2008/9 to 2011/12 seasons in influenza vaccination coverages among high risk subjects and health care workers in Spain. Vaccine. 2014;32:350–4. doi: 10.1016/j.vaccine.2013.11.040. [DOI] [PubMed] [Google Scholar]
- 21.Chor JS, Ngai KL, Goggins WB, et al. Willingness of Hong Kong healthcare workers to accept pre-pandemic influenza vaccination at different WHO alert levels: two questionnaire surveys. BMJ. 2009;339:b3391. doi: 10.1136/bmj.b3391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Seale H, Heywood AE, McLaws ML, et al. Why do I need it? I am not at risk! Public perceptions towards the pandemic (H1N1) 2009 vaccine. BMC Infect Dis. 2010;10:99. doi: 10.1186/1471-2334-10-99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.World Health Organisation (WHO) Report of the SAGE Working Group on Vaccine Hesitancy [Internet] Geneva: WHO; 2014 [cited 2021 Apr 5]. Available from: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf.
- 24.Al-Mohaithef M, Padhi BK. Determinants of COVID-19 vaccine acceptance in Saudi Arabia: a web-based national survey. J Multidiscip Healthc. 2020;13:1657–63. doi: 10.2147/JMDH.S276771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Fu C, Wei Z, Pei S, et al. Acceptance and preference for COVID-19 vaccination in health-care workers (HCWs) [Preprint] doi: 10.1101/2020.04.09.20060103. Posted 2020 Apr 14. medRxiv 2020.04.09.20060103. [DOI] [Google Scholar]
- 26.Lazarus JV, Ratzan SC, Palayew A, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2020;27:225–8. doi: 10.1038/s41591-020-1124-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Malik AA, McFadden SM, Elharake J, et al. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine. 2020;26:100495. doi: 10.1016/j.eclinm.2020.100495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.SteelFisher GK, Blendon RJ, Ward JR, et al. Public response to the 2009 influenza A H1N1 pandemic: a polling study in five countries. Lancet Infect Dis. 2012;12:845–50. doi: 10.1016/S1473-3099(12)70206-2. [DOI] [PubMed] [Google Scholar]
- 29.Malaysia ranks 4th in global survey on public approval of Covid-19 crisis management. FMT [Internet] 2020 May 8 [cited 2021 Jan 25]. Available from: https://www.freemalaysiatoday.com/category/nation/2020/05/08/malaysia-ranks-4th-in-global-survey-on-public-approval-of-covid-19-crisis-management/
- 30.Fu LY, Zimet GD, Latkin CA, et al. Associations of trust and healthcare provider advice with HPV vaccine acceptance among African American parents. Vaccine. 2017;35:802–7. doi: 10.1016/j.vaccine.2016.12.045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lee C, Whetten K, Omer S, et al. Hurdles to herd immunity: distrust of government and vaccine refusal in the US, 2002-2003. Vaccine. 2016;34:3972–8. doi: 10.1016/j.vaccine.2016.06.048. [DOI] [PubMed] [Google Scholar]
- 32.Zahiid SJ. Health Ministry survey shows a third of Malaysians still fear, doubt Covid-19 vaccine. Malay Mail [Internet] 2020 Dec 31 [cited 2021 Mar 9]. Available from: https://www.malaymail.com/news/malaysia/2020/12/31/health-ministry-survey-shows-a-third-of-malaysians-still-fear-doubt-covid-1/1936319.
- 33.World Health Organisation (WHO) Ten threats to global health in 2019 [Internet] Geneva: WHO; 2019 [cited 2021 Jan 25]. Available from: https://www.who.int/vietnam/news/feature-stories/detail/ten-threats-to-global-health-in-2019.
- 34.Arikiah P. Why childhood vaccination continues to be a divisive issue in Malaysia. cna [Internet] 2019 Apr 14 [cited 2021 Jan 5]. Available from: https://www.channelnewsasia.com/news/asia/malaysia-childhood-vaccination-immunisation-debatable-11389462.
- 35.Wong LP, Wong PF, AbuBakar S. Vaccine hesitancy and the resurgence of vaccine preventable diseases: the way forward for Malaysia, a Southeast Asian country. Hum Vaccin Immunother. 2020;16:1511–20. doi: 10.1080/21645515.2019.1706935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Zainal Abidin Z, Hanafiah Juni M, Ibrahim F, et al. Adherence towards different vaccines of childhood immunization of under five year old children. Malays J Med Health Sci. 2017;13:43–50. [Google Scholar]
- 37.Ahmad NA, Jahis R, Kuay LK, et al. Primary immunization among children in Malaysia: reasons for incomplete vaccination. J Vaccines Vaccin. 2017;8:358. [Google Scholar]
- 38.Mohd Azizi FS, Kew Y, Moy FM. Vaccine hesitancy among parents in a multi-ethnic country, Malaysia. Vaccine. 2017;35:2955–61. doi: 10.1016/j.vaccine.2017.04.010. [DOI] [PubMed] [Google Scholar]
- 39.Institute for Public Health, National Institutes of Health National health and morbidity survey 2016: maternal and child health. Volume two: maternal and child health findings [Internet] Kuala Lumpur, Malaysia: Ministry of Health Malaysia; 2016 [cited 2021 Apr 5]. Available from: https://iku.moh.gov.my/images/IKU/Document/REPORT/2016/NHMS2016ReportVolumeII-MaternalChildHealthFindingsv2.pdf.
- 40.de Figueiredo A, Simas C, Karafillakis E, et al. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: a large-scale retrospective temporal modelling study. Lancet. 2020;396:898–908. doi: 10.1016/S0140-6736(20)31558-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Quinn SC, Jamison AM, An J, et al. Measuring vaccine hesitancy, confidence, trust and flu vaccine uptake: results of a national survey of White and African American adults. Vaccine. 2019;37:1168–73. doi: 10.1016/j.vaccine.2019.01.033. [DOI] [PubMed] [Google Scholar]
- 42.Kohl S. Vaccine confidence and vaccination delivery in the European Union. Eur J Hosp Pharm. 2019;26:51–4. doi: 10.1136/ejhpharm-2018-001829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Uscinski JE, Enders AM, Klofstad C, et al. Why do people believe COVID-19 conspiracy theories? Harvard Kennedy Sch Misinformation Rev [Internet] 2020 Apr [cited 2021 Apr 5]. Available from: [DOI]
- 44.Ball P, Maxmen A. The epic battle against coronavirus misinformation and conspiracy theories. Nature. 2020;581:371–4. doi: 10.1038/d41586-020-01452-z. [DOI] [PubMed] [Google Scholar]
- 45.Carvalho M. Only 6.1% of target 80% have registered for Covid-19 vaccine so far, says Khairy. The Star [Internet] 2021 Mar 1 [cited 2021 Mar 9]. Available from: https://www.thestar.com.my/news/nation/2021/03/01/only-61-of-target-80-have-registered-for-covid-19-vaccine-so-far-says-khairy. [Google Scholar]
- 46.Ling M, Kothe EJ, Mullan BA. Predicting intention to receive a seasonal influenza vaccination using Protection Motivation Theory. Soc Sci Med. 2019;233:87–92. doi: 10.1016/j.socscimed.2019.06.002. [DOI] [PubMed] [Google Scholar]
- 47.Rajamoorthy Y, Radam A, Taib NM, et al. Willingness to pay for hepatitis B vaccination in Selangor, Malaysia: a cross-sectional household survey. PLoS One. 2019;14:e0215125. doi: 10.1371/journal.pone.0215125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Rajamoorthy Y, Radam A, Taib NM, et al. The relationship between perceptions and self-paid hepatitis B vaccination: a structural equation modeling approach. PLoS One. 2018;13:e0208402. doi: 10.1371/journal.pone.0208402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Reiter PL, Pennell ML, Katz ML. Acceptability of a COVID-19 vaccine among adults in the United States: how many people would get vaccinated? Vaccine. 2020;38:6500–7. doi: 10.1016/j.vaccine.2020.08.043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Harapan H, Wagner AL, Yufika A, et al. Acceptance of a COVID-19 vaccine in Southeast Asia: a cross-sectional study in Indonesia. Front Public Health. 2020;8:381. doi: 10.3389/fpubh.2020.00381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Harapan H, Wagner AL, Yufika A, et al. Willingness-to-pay for a COVID-19 vaccine and its associated determinants in Indonesia. Hum Vaccin Immunother. 2020;16:3074–80. doi: 10.1080/21645515.2020.1819741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Reiter PL, Katz ML, Bauermeister JA, et al. Increasing human papillomavirus vaccination among young gay and bisexual men: a randomized pilot trial of the outsmart HPV intervention. LGBT Health. 2018;5:325–9. doi: 10.1089/lgbt.2018.0059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.McRee AL, Shoben A, Bauermeister JA, et al. Outsmart HPV: acceptability and short-term effects of a web-based HPV vaccination intervention for young adult gay and bisexual men. Vaccine. 2018;36:8158–64. doi: 10.1016/j.vaccine.2018.01.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Graffigna G, Palamenghi L, Boccia S, et al. Relationship between citizens' health engagement and intention to take the COVID-19 vaccine in Italy: a mediation analysis. Vaccines (Basel) 2020;8:576. doi: 10.3390/vaccines8040576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Sim BLH, Chidambaram SK, Wong XC, et al. Clinical characteristics and risk factors for severe COVID-19 infections in Malaysia: a nationwide observational study. Lancet Reg Health West Pac. 2020;4:100055. doi: 10.1016/j.lanwpc.2020.100055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Li J, Huang DQ, Zou B, et al. Epidemiology of COVID-19: a systematic review and meta-analysis of clinical characteristics, risk factors, and outcomes. J Med Virol. 2021;93:1449–58. doi: 10.1002/jmv.26424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Chidambaram V, Tun NL, Haque WZ, et al. Factors associated with disease severity and mortality among patients with COVID-19: a systematic review and meta-analysis. PLoS One. 2020;15:e0241541. doi: 10.1371/journal.pone.0241541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Malaysia agrees to buy 12.8 million doses of Pfizer's COVID-19 vaccine. cna [Internet] 2020 Nov 27 [cited 2021 Jan 25]. Available from: https://www.channelnewsasia.com/news/asia/malaysia-covid-19-pfizer-vaccine-coronavirus-13651672.
- 59.World Health Organization (WHO) Roadmap for prioritizing population groups for vaccines against COVID-19 [Internet] Geneva: WHO; 2020 [cited 2021 Nov 8]. Available from: https://www.who.int/immunization/sage/meetings/2020/october/Session03_Roadmap_Prioritization_Covid-19_vaccine.pdf.
- 60.Dror AA, Eisenbach N, Taiber S, et al. Vaccine hesitancy: the next challenge in the fight against COVID-19. Eur J Epidemiol. 2020;35:775–9. doi: 10.1007/s10654-020-00671-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Shekhar R, Sheikh AB, Upadhyay S, et al. COVID-19 vaccine acceptance among health care workers in the United States. Vaccines (Basel) 2021;9:119. doi: 10.3390/vaccines9020119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Department of Statistics Malaysia Current population estimates, Malaysia, 2020 [Internet] Putrajaya, Malaysia: Department of Statistics Malaysia; 2020 [cited 2021 Jan 15]. Available from: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=155&bul_id=OVByWjg5YkQ3MWFZRTN5bDJiaEVhZz09&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09.
- 63.Collins K, Holder J. See how rich countries got to the front of the vaccine line. The New York Times [Internet] 2021 Mar 31 [cited 2021 May 18]. Available from: https://www.nytimes.com/interactive/2021/03/31/world/global-vaccine-supply-inequity.html.
- 64.Yusof TA. 200,000 influenza vaccines available within the next two months. New Straits Times [Internet] 2020 Jan 18 [cited 2021 May 18]. Available from: https://www.nst.com.my/news/nation/2020/01/557596/200000-influenza-vaccines-available-within-next-two-months.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Acceptance and perception on the Covid-19 vaccination (immunization) in the general population of Malaysia