

ABSTRACT
Objective:
To compare lower incisor dentoalveolar compensation and mandible symphysis morphology among Class I and Class III malocclusion patients with different facial vertical skeletal patterns.
Materials and Methods:
Lower incisor extrusion and inclination, as well as buccal (LA) and lingual (LP) cortex depth, and mandibular symphysis height (LH) were measured in 107 lateral cephalometric x-rays of adult patients without prior orthodontic treatment. In addition, malocclusion type (Class I or III) and facial vertical skeletal pattern were considered. Through a principal component analysis (PCA) related variables were reduced. Simple regression equation and multivariate analyses of variance were also used.
Results:
Incisor mandibular plane angle (P < .001) and extrusion (P = .03) values showed significant differences between the sagittal malocclusion groups. Variations in the mandibular plane have a negative correlation with LA (Class I P = .03 and Class III P = .01) and a positive correlation with LH (Class I P = .01 and Class III P = .02) in both groups. Within the Class III group, there was a negative correlation between the mandibular plane and LP (P = .02). PCA showed that the tendency toward a long face causes the symphysis to elongate and narrow. In Class III, alveolar narrowing is also found in normal faces.
Conclusions:
Vertical facial pattern is a significant factor in mandibular symphysis alveolar morphology and lower incisor positioning, both for Class I and Class III patients. Short-faced Class III patients have a widened alveolar bone. However, for long-faced and normal-faced Class III, natural compensation elongates the symphysis and influences lower incisor position.
Keywords: Lower incisor, Dentoalveolar compensation, Symphysis, Class I, Class III, Vertical skeletal pattern
INTRODUCTION
It has been noted that within the dentofacial complex a compensatory mechanism exists that tries to preserve a proportional and harmonious facial pattern. When either basal bone, whether maxilla or mandible, deviates from its expected growth pattern, the remaining craniofacial structures react in an attempt to mask this discrepancy.1 Related to this, dental compensation acts to camouflage anterior-posterior and vertical basal bone discrepancies in an attempt to establish a normal incisor relationship.2,3 In a Class III malocclusion, the upper incisor typically is proclined, whereas the lower incisors are retroclined. In the vertical dimension, the compensation is attained by varying the symphysis length and through incisor eruption.4
Once craniofacial growth of a Class III malocclusion patient has slowed significantly, therapeutic options decrease to two possibilities: orthodontic camouflage or orthognathic surgery.5 For the first option, it is necessary to further increase the degree of compensation which could go over accepted tooth movement boundaries; while for the second, the already expressed compensation must be eliminated to facilitate meaningful surgical movements. In both cases, orthodontics must move the teeth through the alveolus that holds them. Consequently, these changes must be considered in the treatment plan since they limit or condition our therapeutic possibilities.5 Several studies have addressed the need of respecting anatomic limits in order to prevent iatrogenic phenomena such as bone loss, alveolar dehiscence, gingival recession, dental mobility, and other negative effects.6–12
In the study by Handelman,6 107 Class I, II, and III skeletal malocclusions were evaluated. A decrease in the alveolar width was noted in all patients with malocclusions and long facial patterns and in Class III patients with normal faces. However, when dividing the subjects into nine subgroups, the sample sizes were small and heterogeneous, showing fewer significant differences. Outside of Handelman's study,6 there are a few other studies that had explored the relationship between the alveolar bone and the behavior of the incisors as related to vertical and sagittal skeletal patterns.7–10 The purpose of our study was to evaluate the relationship between possible compensation of the lower incisors and the mandibular symphyseal dimensions in a sample of Class I and Class III skeletal malocclusions with different vertical facial patterns.
MATERIALS AND METHODS
Institutional ethical board approval was granted. Consecutive orthodontic records of Class III and Class I malocclusion patients treated between 2009 and 2010 were reviewed from three private orthodontic clinics. The final sample consisted of 107 lateral cephalometric x-rays of white subjects between 18 and 45 years of age with complete permanent dentition. Patients who had received prior orthodontic treatment or maxillofacial surgery, were syndromic, or had craniofacial malformations or root resorption were excluded.
Cephalometric measurements
The x-rays were calibrated with the NemoCeph computer program (Software Nemotec, Madrid, Spain) in order to compensate the different magnifications of the x-rays. The same examiner performed all tracings by hand using a negatoscope (Mobiclinic, Seville, Spain), with acetate paper and a fine-point pencil (0.5 mm).
Class III and Class I subjects
ANB angle13 was used in the sagittal classification of the malocclusions (ANB ≤ −1° in Class III and ANB = 2° ± 2 in Class I). In order to eliminate any degree of confounding by the vertical pattern, an essential requirement was that Class III subjects had Wits14 ≤ −1 mm and Class I subjects had Wits between 0 and 2 mm. The Class III sample was further segregated according to the incisor relationship in three subgroups: positive overjet, negative overjet, and edge-to-edge.
Vertical facial type
Through the mandibular plane (Go-Gn a SN line), Class I and Class III patients were classified into long (>35°), average (30–35°), or short faces (<29°)13 (Table 1).
Table 1.
Sample Segregation in Class I and Class III

Lower incisor position
The incisor mandibular plane angle (IMPA) was obtained from the angle between the long axis of the lower incisor and the Downs mandibular plane.15 The amount of extrusion from the edge of the incisor was calculated on the functional occlusal plane16 (Figure 1).
Figure 1.
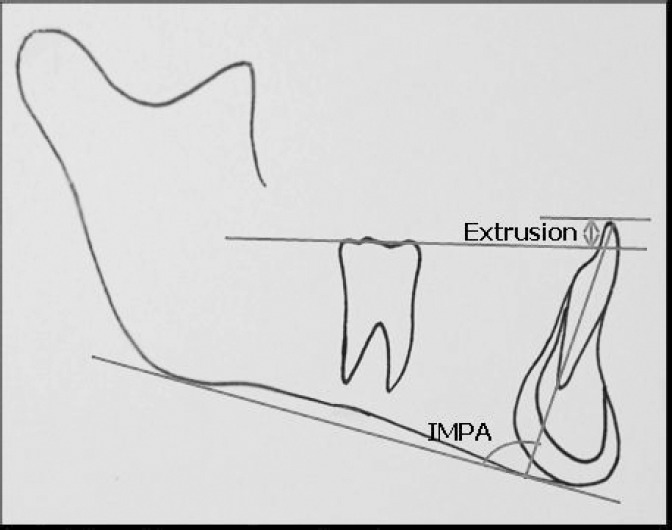
The position of the lower incisor: IMPA and extrusion.
Symphysis dimensions
The dimensions of the mandibular symphysis were quantified following Handelman's criteria6: LP, bone posterior to the apex of the incisor; LA, bone anterior to the apex of the incisor; and LH, bone inferior to the apex of the incisor (Figure 2).
Figure 2.
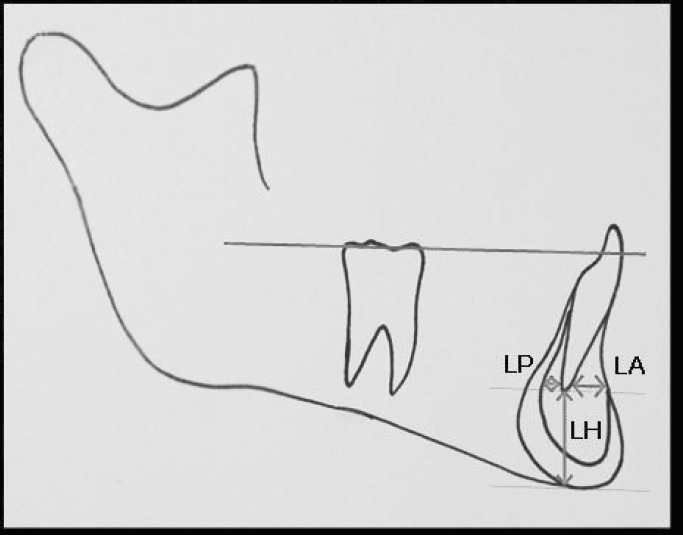
The dimensions of the symphysis: LP, LA, and LH.
Reliability Analysis
To calculate intrarater reliability, new tracings and complete cephalometric analysis were repeated for 25 randomly chosen radiographs.
Statistical Analysis
Differences between the lower incisor position and symphysis dimensions were evaluated with an analysis of variance (ANOVA) considering the three Class III malocclusion subgroups and with a Student's t-test considering the Class I and Class III malocclusion groups.
A simple regression analysis was used to determine the correlation coefficients between the mandibular plane and the variables corresponding to incisor position and symphysis dimensions.
A principal component analysis17 (PCA) was used to evaluate if the five variables related to incisor position and symphysis dimensions could be reduced in order to reduce data variability and strengthen the statistical analysis. After completing the PCA, an ANOVA was performed to evaluate significant differences within the sagittal and vertical skeletal facial patterns. Finally, a multivariate analysis of variance (MANOVA) was performed to evaluate the studied variables and their interactions and associations.
RESULTS
A kappa value of 0.84 was attained, CI (0.76, 0.89). The confidence interval (CI 95%) for each variable was: IMPA (−0.6, 7.7), extrusion (−0.97, 0.74), LP (−0.55, 1.31), LA (−0.19, 1.14), and LH (−2.08, 2.78).
Normality of data was confirmed with the test of Shapiro-Wilk (P > .05). Descriptive data for the included sample can be found in Table 2.
Table 2.
Sample Descriptive Statistics in Class I and III: Overjet Subgroups: (a) Positive, (b) Negative and (c) Edge-to-Edge. Vertical Facial Type Subgroups: (LF) Long, (NF) Normal or Average and (SF) Short

Among the three Class III subgroups, no significant differences were observed for IMPA values (P = .31), while there were differences for the extrusion values (P = .05) (Figure 3). The MANOVA, with a Wilks lambda of P = .003, confirms that marginal differences exist in the extrusion between the edge-to-edge relationship and other relationships.
Figure 3.
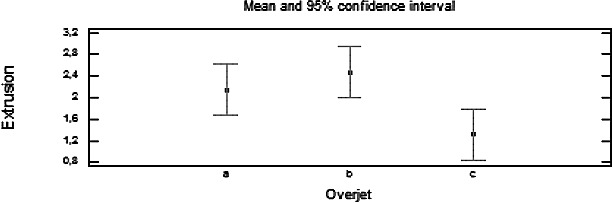
Extrusion value in three types of Class III overjets. (a) Positive. (b) Negative. (c) Edge-to-edge.
The IMPA (P < .001) and extrusion (P = .03) values show significant differences between the sagittal malocclusion groups. The lower incisor is more protruded in Class I and more extruded in Class III malocclusion patients (Figures 4 and 5). In Class III malocclusion patients, the IMPA has a negative correlation with the mandibular plane (P = .002) (Table 3). Nevertheless, there is no significant correlation between extrusion and the mandibular plane for either group.
Figure 4.
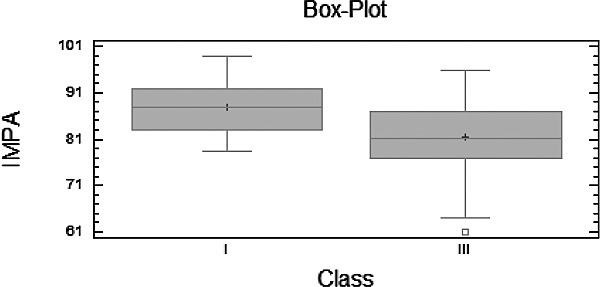
IMPA variation in Class I and Class III.
Figure 5.
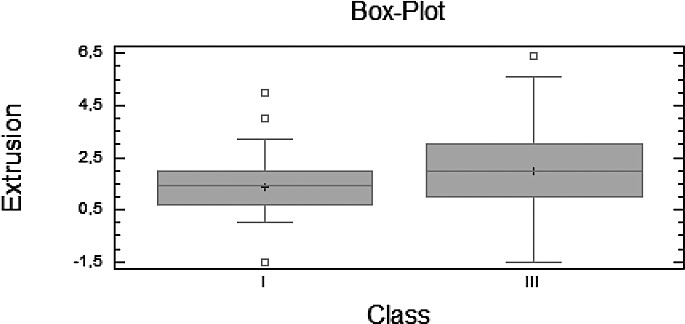
Extrusion variation in Class I and Class III.
Table 3.
Correlations Between the Mandibular Plane and Lower Incisor in Class I and Class III

When the symphysis dimensions (LP, LA, and LH) among the two malocclusions and the three Class III subgroups are evaluated, there are no significant or marginal differences (all P > .05).
The relationship between symphysis dimension and the mandibular plane is shown in Table 4. Variations in the mandibular plane have a negative correlation with LA (Class I P = .03 and Class III P = .01) and a positive correlation with LH (Class I P = .01 and Class III P = .02) in both groups. Within the Class III group, there is a negative correlation between the mandibular plane and LP (P = .02).
Table 4.
Correlations Between the Mandibular Plane and the Mandibular Symphysis in Class I and Class III

When performing the PCA, a reduction to three linear combinations was possible (all with an eigenvalue greater than 1.0). These three components explain 71.03% of the variability in the original data (Table 5).
Table 5.
Principal Component Analysis

Component 1 (CP1): IMPA and LA, the greater the incisor inclination, the greater the amount of bone between the apex and cortex of the symphysis.
Component 2 (CP2): Extrusion and LH, the greater the extrusion, the greater the basal apex distance from the symphysis.
Component 3 (CP3): LP is the variable with greater weight and is not related to the other variables (Table 5).
The principal component analysis between the Class III subgroups did not show any significance (CP1, P = .6; CP2, P = .2; CP3, P = .4) and Wilks lambda (P = .38).
Between the malocclusion groups, the analysis showed a statistically significant difference in CP1, (P = .005) and CP2 (P = .006) averages (Figure 6). However, CP3 (P = .12) did not contribute to any statistical differences.
Figure 6.
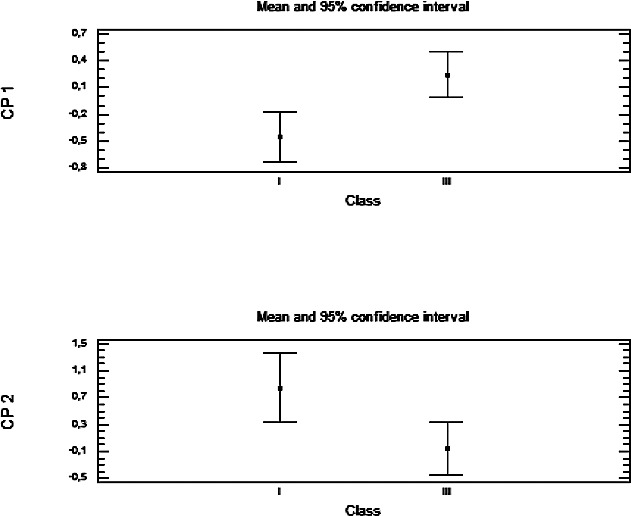
Average value for principal components 1 (CP1) and 2 (CP2) in Classes I and III.
In Figure 7, the dispersion of Class I malocclusion subjects placed them toward negative CP1 values (greater IMPA and LA) and toward positive CP2 values (less extrusion and LH). On the contrary, in Class III malocclusions, extrusions and LH are increased and IMPA and LA decreased.
Figure 7.
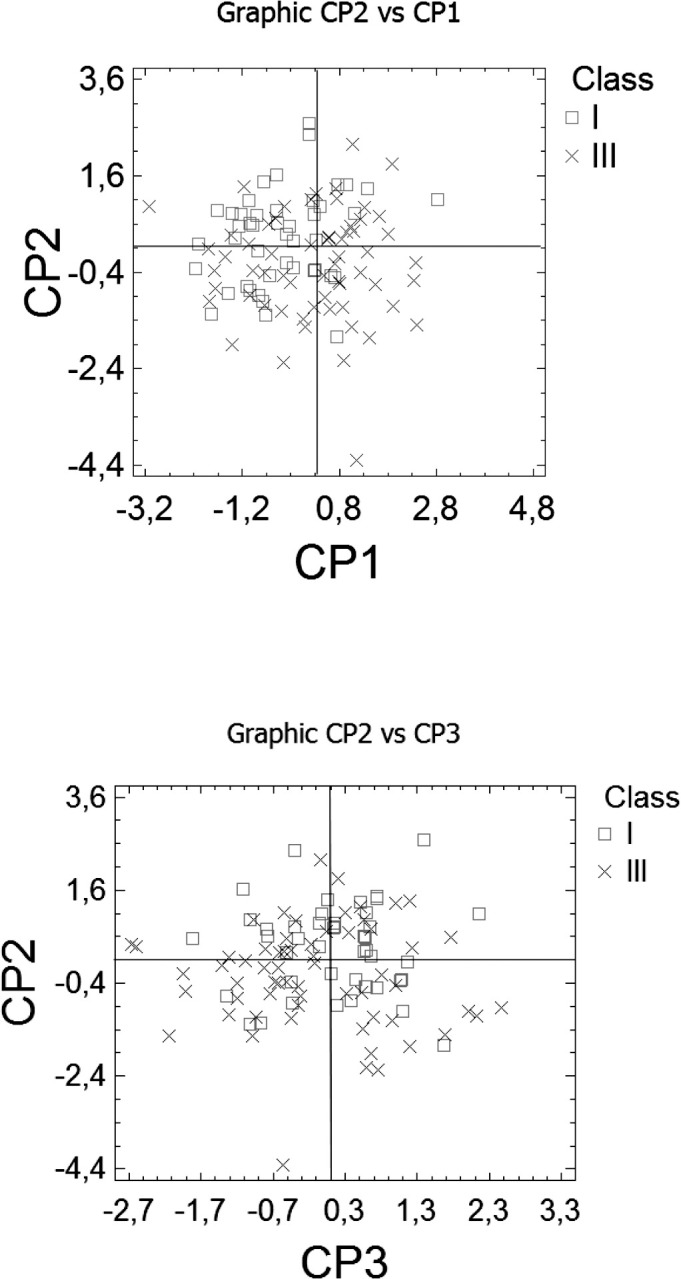
Principal components 1 (CP1), 2 (CP2), and 3 (CP3) in Classes I and III.
The MANOVA analysis, with a Wilks lambda P = .001, showed marginal differences in CP1 between long faces and all other patterns within Class III, and in CP3 between long faces and short faces.
DISCUSSION
A comparative study between a Class I and a Class III sample group with different vertical patterns was done in order to evaluate the dentoalveolar compensation of the lower incisor and the concomitant changes in the mandibular symphysis. In prior related publications,18–20 sample sizes were heterogeneous and small. Additionally, their statistical analyses sought differences between different malocclusion types but did not concurrently evaluate to what extent the symphysis dimensions were related to variations in the position of the incisor and the skeletal pattern.
Evaluation of Inclination and Extrusion of Lower Incisor
Within Class III, with IMPA values less than 84° and increased extrusion above 1.7 mm, discrepancies were observed when compared to the Class I sample. The differences against the Class I sample were further emphasized, increasing retroclination in such a manner that the mandibular plane increases in Class III subjects. This relationship has been previously described in several cephalometric patterns.10,21,22
However, no significant differences were found in the amount of retroclination between our three Class III subgroups. These results were in contrast with previous studies,23,24 which did indeed find less retroclination in Class III patients with negative overjet. In one case,23 a heterogeneous Class III sample of 48 subjects from 6 to 34 years of age with mixed and permanent occlusion was used, while in the other case24 incisor inclination was measured in respect to the NB line, which may be subject to mandibular rotation. Vertical facial patterns had to be taken into consideration.25,26 In our sample, all 62 of the Class III subjects were adults and had permanent dentition; the measurements of the incisor were performed with respect to their bone base in order to prevent any facial pattern masking.
As opposed to previous studies, extrusion of the lower incisor with respect to the occlusal plane was also evaluated, observing the fact that in Class III patients, the lower incisor is extruded in comparison with the Class I sample. Within the Class III sample, the group with an edge-to-edge incisor relationship showed a lesser degree of extrusion, which varies between 0.8 and 1.6 mm, showing these values to be even lower than the Class I average. On the other hand, in the negative overjet group, we found greater extrusion of the lower incisor with respect to its bone base.
Evaluation of Symphysis Dimensions
No significant differences were found with regard to the symphyseal dimensions between the Class I and Class III samples and within the Class III subgroups. These results partially coincided with Handelman's conclusions.6 However, when segregating the sample according to mandibular plane divergence, it can be observed that in both Class I and Class III patients, the increase in the mandibular plane involved a decrease in LA and an increase in LH. These data coincide with that of Handelman,5 who found a decrease in LA and LH in all long-faced and Class III normal-faced patients. Additionally, according to our results, in Class III patients there was a negative correlation between the mandibular plane and cortical LP, to such an extent that the width of the lingual cortex of the symphysis decreased as mandibular plane divergence increased. In a previous study27 in subjects with Class III, the root apex was closer to the buccal cortical due to the fact that the incisor is more lingually inclined. However, vertical facial growth pattern was not considered.
Evaluation of Changes in the Position of the Lower Incisor and Symphysis Dimensions With the Principal Component Analysis
When applying the PCA, the variables representing the position of the incisor showed a clear difference between Class I and Class III samples, also confirmed by the Student's t-test. Unlike Handelman's5 research, principal components have demonstrated that the distances from the apex to LA are directly related to the grade of inclination of the incisor, while the distance to the LH is related to incisor extrusion. In Class I, the lower incisor was not found to be extruded very much with respect to the occlusal plane. The distance from the apex to LH is shorter with respect to the Class III incisor, which is extruded, and the LH increased. Therefore, in Class I patients with protruding incisors, as the incisor edge is advanced, the apex rotates toward the lingual side. As such, LA increases, while in Class III patients with a retroclined incisor, as the apex nears the buccal cortex, LA decreases.
PCs have allowed for differences to be shown between normal- and short-faced patients that were not evident in the previous comparative analyses. Comparing these groups, alveolar bone remodeling does not respond to changes in the extrusion and inclination of the lower incisor. Normal-faced patients, in comparison with short-faced patients, present with lesser extrusion and greater IMPA. The symphysis is much more remodeled and elongated, the LA and LP cortices are elongated to a lesser extent and the LH are elongated to a greater extent. In short-faced patients with a more extruded and less proclined incisor, we find increased thickness in the cortices (LA and LP) and a decrease in LH height, presenting a thick, shortened symphysis. In comparison with the two other groups, an extruded and retroclined incisor is often found in long-faced patients, which causes the LH increase and the LA decrease. The LP cortex, which is decreased in long-faced subjects, lies outside the dentoalveolar compensation mechanism of the lower incisor and responds to the more intense reformation process that takes place in these subjects. Class III patients with normodivergent and hyperdivergent patterns show a much more marked dentoalveolar compensation mechanism: the incisor retroclines and extrudes even more, affecting the reformation of the symphysis, giving rise to the narrowing and elongation of all of its alveolar walls: LP, LA, and LH.
In long-faced and normal-faced Class III patients with mandibular prognathism, natural compensation elongates the symphysis, which could condition orthodontic movements, limiting presurgical decompensation and increasing the risk of damage to periodontal tissues. According to the results of our study, the vertical facial pattern is a determining factor for mandibular anterior alveolar remodeling both in Class I and Class III patients, and this likely conditions orthodontic movement. Class III short-faced patients have a thickened alveolar bone, which should allow for more significant teeth movements without a concomitant periodontal risk.
Limitations
Various researchers are currently studying how the morphology of the alveolar bone is affected by lower incisor proclination through three-dimensional (3D) cone-beam computed tomography.12,28 There is no doubt that our results will have to be contrasted in the future with data obtained from 3D imaging.
Although the total sample is larger than previous samples, some subgroups were still small, making it difficult to draw properly powered conclusions. As the sample was taken from the files of private offices, the number of patients in the different subgroups reflects the population that seeks orthodontic treatment. This likely may have implied that less extreme vertical patterns are shown.
CONCLUSIONS
Vertical facial pattern is a significant factor in mandibular symphysis alveolar morphology and lower incisor positioning, both for Class I and Class III patients.
Short-faced Class III patients have a widened alveolar bone.
However, for long-faced and normal-faced Class III patients, natural compensation elongates the symphysis and influences lower incisor position.
REFERENCES
- 1.Goldsman S. The variations in skeletal and denture patterns in excellent adult facial types. Angle Orthod. 1959;29:63–92. [Google Scholar]
- 2.Bibby RE. Incisor relationships in different skeletofacial patterns. Angle Orthod. 1980;50:41–44. doi: 10.1043/0003-3219(1980)050<0041:IRISP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.Jacobson A, Evans WG, Preston CG, Sadowsky PL. Mandibular prognathism. Am J Orthod. 1974;66:140–171. doi: 10.1016/0002-9416(74)90233-4. [DOI] [PubMed] [Google Scholar]
- 4.Nielsen IL. Vertical malocclusions: etiology, development, diagnosis and some aspects of treatment. Angle Orthod. 1991;61:247–260. doi: 10.1043/0003-3219(1991)061<0247:VMEDDA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 5.Burns NR, Musich DR, Martin C, Razmus T, Gunel E, Ngan P. Class III camouflage treatment: what are the limits. Am J Orthod Dentofacial Orthop. 2010;137:9. doi: 10.1016/j.ajodo.2009.05.017. [DOI] [PubMed] [Google Scholar]
- 6.Handelman CS. The anterior alveolus: its importance in limiting orthodontic treatment and its influence on the occurrence of iatrogenic sequelae. Angle Orthod. 1996;66:95–110. doi: 10.1043/0003-3219(1996)066<0095:TAAIII>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 7.Chung CJ, Jung S, Baik HS. Morphological characteristics of the symphyseal region in adult skeletal Class III crossbite and openbite malocclusions. Angle Orthod. 2008;78:38–43. doi: 10.2319/101606-427.1. [DOI] [PubMed] [Google Scholar]
- 8.Troy BA, Shanker S, Fields HW, Vig K, Johnston W. Comparison of incisor inclination in patients with Class III malocclusion treated with orthognathic surgery or orthodontic camouflage. Am J Orthod Dentofacial Orthop. 2009;135:146.e1–9. doi: 10.1016/j.ajodo.2008.07.012. [DOI] [PubMed] [Google Scholar]
- 9.Ishikawa H, Nakamura S, Iwasaki H, Kitazawa S, Tsukada H, Sato Y. Dentoalveolar compensation related to variations in sagittal jaw relationships. Angle Orthod. 1999;69:534–538. doi: 10.1043/0003-3219(1999)069<0534:DCRTVI>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 10.Tang N, Zhao ZH, Liao CH, Zhao MY. Morphological characteristics of mandibular symphysis in adult skeletal class II and Class III malocclusions with abnormal vertical skeletal patterns [in Chinese] Hua Xi Kou Qiang Yi Xue Za Zhi. 2010;28:395–398. [PubMed] [Google Scholar]
- 11.Lee KM, Kim YI, Park SB, Son WS. Alveolar bone loss around lower incisors during surgical orthodontic treatment in mandibular prognathism. Angle Orthod. 2012;82:637–644. doi: 10.2319/081711-526.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kook YA, Kim G, Kim Y. Comparison of alveolar bone loss around incisors in normal occlusion samples and surgical skeletal class III patients. Angle Orthod. 2012;82:645–652. doi: 10.2319/070111-424.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Steiner CC. Cephalometrics for you and me. Am J Orthod. 1953;39:729–755. [Google Scholar]
- 14.Jacobson A. The Wits appraisal of jaw disharmony. Am J Orthod. 1975;67:125–138. doi: 10.1016/0002-9416(75)90065-2. [DOI] [PubMed] [Google Scholar]
- 15.Tweed TH. The Frankfort-mandibular plane angle in orthodontic diagnosis, Classification, treatment planning and prognosis. Am J Orthod Oral Surg. 1946;32:175–221. doi: 10.1016/0096-6347(46)90001-4. [DOI] [PubMed] [Google Scholar]
- 16.Ricketts RM. Cephalometric analysis and synthesis. Angle Orthod. 1961;31:141–156. [Google Scholar]
- 17.Foguet JM. Análisis Multivariante Análisis de Componentes Principales (Colección ESADE) Barcelona, Spain: Ed Hispano Europea SA; 1989. [Google Scholar]
- 18.Sandborn RT. Differences between the facial skeletal patterns of Class III malocclusion and normal occlusion. Angle Orthod. 1955;25:208–222. [Google Scholar]
- 19.Ten Hoeve A, Mulie RM. The effect of anterio-posterior incisor repositioning on the palatal cortex as studied with laminography. J Clin Orthod. 1976;10:804–822. [PubMed] [Google Scholar]
- 20.Solow B. The dentoalveolar compensatory mechanism: background and clinical implications. Br J Orthod. 1980;7:145–161. doi: 10.1179/bjo.7.3.145. [DOI] [PubMed] [Google Scholar]
- 21.Fastlight J. Tetragon: a visual cephalometric analysis. J Clin Orthod. 2000;34:353–360. [Google Scholar]
- 22.Anwar N, Fida M. Compensation for vertical dysplasia and its clinical application. Eur J Orthod. 2009;31:516–522. doi: 10.1093/ejo/cjp010. [DOI] [PubMed] [Google Scholar]
- 23.Baca A. Mecanismos incisales de compensación de las desarmonías esqueléticas sagitales: resultados de un estudio sobre 500 pacientes maloclusivos. Rev Esp Ortod. 1992;22:36–52. [Google Scholar]
- 24.Ishikawa H, Nakamura S, Iwasaki H, Kitazawa S, Tsukada H, Chu S. Dentoalveolar compensation in negative overjet cases. Angle Orthod. 2000;70:145–148. doi: 10.1043/0003-3219(2000)070<0145:DCINOC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 25.Behrents RG. Growth in the Aging Craniofacial Skeleton Monograph 17 Craniofacial Growth Series. Ann Arbor, Mich: Center for Human Growth and Development. The University of Michigan; 1985. [Google Scholar]
- 26.Bishara SE, Fahl JA, Peterson LC. Longitudinal changes in the ANB angle and Wits appraisal: clinical implications. Am J Orthod. 1983;84:133–139. doi: 10.1016/0002-9416(83)90177-x. [DOI] [PubMed] [Google Scholar]
- 27.Yamada C, Kitai N, Kakimoto N, Murakami S, Furukawa S, Takada K. Spatial relationships between the mandibular central incisor and associated alveolar bone in adults with mandibular prognathism. Angle Orthod. 2007;77:766–772. doi: 10.2319/072906-309. [DOI] [PubMed] [Google Scholar]
- 28.Yu Q, Pan XG, Ji GP, Shen G. The association between lower incisal inclination and morphology of the supporting alveolar bone—a cone-beam CT study. Int J Oral Sci. 2009;1:217–223. doi: 10.4248/IJOS09047. [DOI] [PMC free article] [PubMed] [Google Scholar]