

Abstract
Increasing research supports that effective clinician communication with patients and families leads to improved patient outcomes, higher patient satisfaction, and improved clinician experiences. As a result, patient- and family-centered communication is the focus of a 2020 American Academy of Neurology quality measure and part of neurology residency training milestones. Clinicians across training levels can implement strategies for improving patient- and family-centered communication, including optimizing the communication environment, using verbal and nonverbal skills, focusing on the patient's agenda, practicing active listening, demonstrating respect and empathy, individualizing encounters to patient and family needs, and providing clear explanations. These skills can be tailored for specialized encounters (e.g., when wearing masks, telemedicine) and for electronic communication. By purposefully identifying and incorporating key communication skills in everyday practice, clinicians have the opportunity to improve patient care and satisfaction and their own experiences in neurology clinical practice.

Effective patient-centered communication is an increasing focus in neurology clinical practice and training. In 2020, the American Academy of Neurology (AAN) published a Neurology Outcomes Quality Measurement Set including the quality measure, “Patient Communication Experiences for Patients with Neurologic Conditions.” This measure assesses the number of patients or care partners who answered “always” when responding to the query “provider explained things in a way that was easy to understand.” The measure has no allowable exclusions.1 Patient- and family-centered communication is also part of the Interpersonal and Communication Skills competency designated by the Accreditation Council for Graduate Medical Education (ACGME).2 The ACGME Milestones 2.0 workgroup identified 3 fundamental skills relating to this subcompetency: (1) relationship building, (2) approaches to identify and overcome communication barriers, and (3) strategies to elicit patient and family understanding, values, and expectations, with the aim of aligning patient goals and preferences with treatment options.2 In the updated neurology residency milestones (effective July 2021), milestones pertaining to patient- and family-centered communication (the first of 4 skills associated with the Interpersonal and Communication Skills competency) relate to (1) relationship building—including verbal and nonverbal approaches—and (2) shared decision making with individualized and compassionate communication of medical information in the context of patients' and families' values, uncertainty, and conflict.3 The overall intent of this skill is “to deliberately use language and behaviors to form constructive relationships with patients.”4
The increasing focus on patient- and family-centered communication is consistent with research linking effective clinician-patient communication to higher patient satisfaction5 and improved health care outcomes.6 Good communication also benefits clinicians: improved patient satisfaction scores may influence reimbursement and effective communication can decrease litigation.7 Research suggests that strategies to improve communication can improve both patient satisfaction and 3 parts of the quadruple aim of health care: population health, patient experiences, and clinician experiences.8,9
How Is Communication Measured?
In clinical practice, communication is often assessed through patient satisfaction surveys such as the Agency for Healthcare Research and Quality (AHRQ) Consumer Assessment of Healthcare Providers and Systems (CAHPS) or the Press Ganey Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys. The AAN based its communication quality measure on a question from CAHPS because this survey is commonly used, free, and not neurology specific (allowing comparisons with other patient populations), and the AHRQ provides related resources to promote quality improvement.1 In addition to the single question chosen by the AAN for its quality measure (explaining things in a way that is easy to understand), CAHPS queries whether a clinician spends sufficient time, listens carefully, and shows respect. Similarly, the HCAHPS survey has a “communication with doctors” section querying careful listening, treatment with courtesy and respect, and whether clinicians explain things in a way that the patient can understand. Other survey tools, such as the RAND Health Care Patient Satisfaction Questionnaire, also measure communication as 1 aspect of patient satisfaction.
In the ACGME neurology milestones, relationship building is assessed based on whether the resident uses verbal and nonverbal behaviors, active listening, and clear language and establishes a therapeutic relationship through increasingly complex encounters. Skills along the shared decision-making milestone pathway include the resident identifying the need to individualize communication strategies, communicating compassionately to clarify expectations and verify understanding, communicating medical information in the context of the patient's and family's values, uncertainty, and conflict, and using shared decision making.3,4
Improving Clinician-Patient Communication
There are many practical strategies that clinicians at any level can take to improve communication with patients and caregivers (Table 1). Quality communication starts with the right environment, including having a quiet, private space and allowing time for good communication.10 Research suggests that patients feel that clinicians spend more time with them when the clinicians are seated. Patients also report a more positive interaction and better understanding with seated clinicians.11 Patients report higher satisfaction when clinicians focus on the patient's needs rather than time management or clinical issues.12 Ensuring that one has the patient's full agenda at the beginning of the visit by asking “Is there something else you want to address in the visit today?” can eliminate almost 80% of unmet patient concerns.13
Table 1.
Strategies to Improve Clinician-Patient Communication
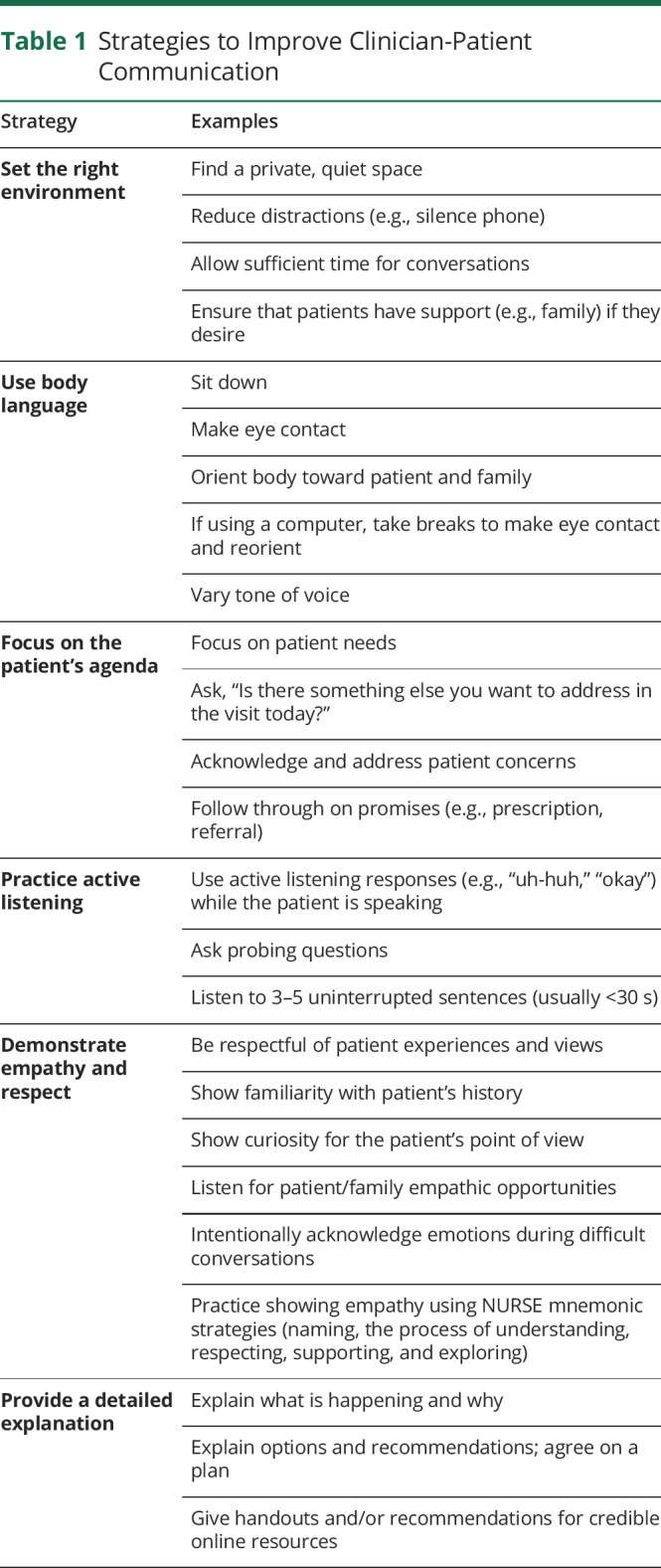
High-quality communication requires the clinician to be an active listener, including using encouraging sounds to demonstrate attention, asking probing questions, allowing the patient to express his or her concerns, and listening without interrupting for at least 3–5 sentences (usually less than 30 seconds).12 Active listening involves both verbal and nonverbal strategies (Table 1).14,15 A critical aspect of the communication skill set is to distinguish between cognitive and emotional communication. Cognitive data refer to discussions about scientific information and logical reasoning, the typical focus of medical training. Clinicians aim to teach patients and families about their diagnosis and the options available to them. At the same time—particularly in difficult conversations—emotional data are an inherent part of communication. This refers to the feelings and associations invoked in the conversation, which may be expressed verbally through tone and pace of speech but often are nonverbal forms of communication such as facial expression and posture. Both of these data streams occur simultaneously during difficult conversations. When clinicians are intentional about bringing emotion to the surface, patients feel a deeper sense of clinician empathy and respect.16
Respect and empathy are paramount to clinician-patient communication,12,14,17 with 1 study showing that respect accounted for more than 4 times as much variance in overall clinician ratings compared with all other aspects of communication.17 Sixty percent of patient-clinician interactions include at least 1 empathic opportunity, which are patient or family statements of emotion, challenge, or progress.18 The NURSE mnemonic (Table 2) outlines several empathic communication tools to respond to such opportunities. These include naming emotions, improving understanding of the patient's journey (focusing on understanding as a process, not as a destination), respecting patients' efforts in the struggle against illness, informing patients of how the clinician will support them along the way, and exploring what patients said with follow-up questions.19 Patients also value when clinicians demonstrate knowledge of the patient and his or her health record, are caring, and respond in a thoughtful way, showing understanding of what the patient described.12 Finally, patients desire clear explanations regarding what is happening and why, the options, and the reasoning behind recommendations.12,14 Both verbal and written education are beneficial.12,14
Table 2.
Sample Mnemonics Supporting Health Care Communication

Communication in Challenging Situations
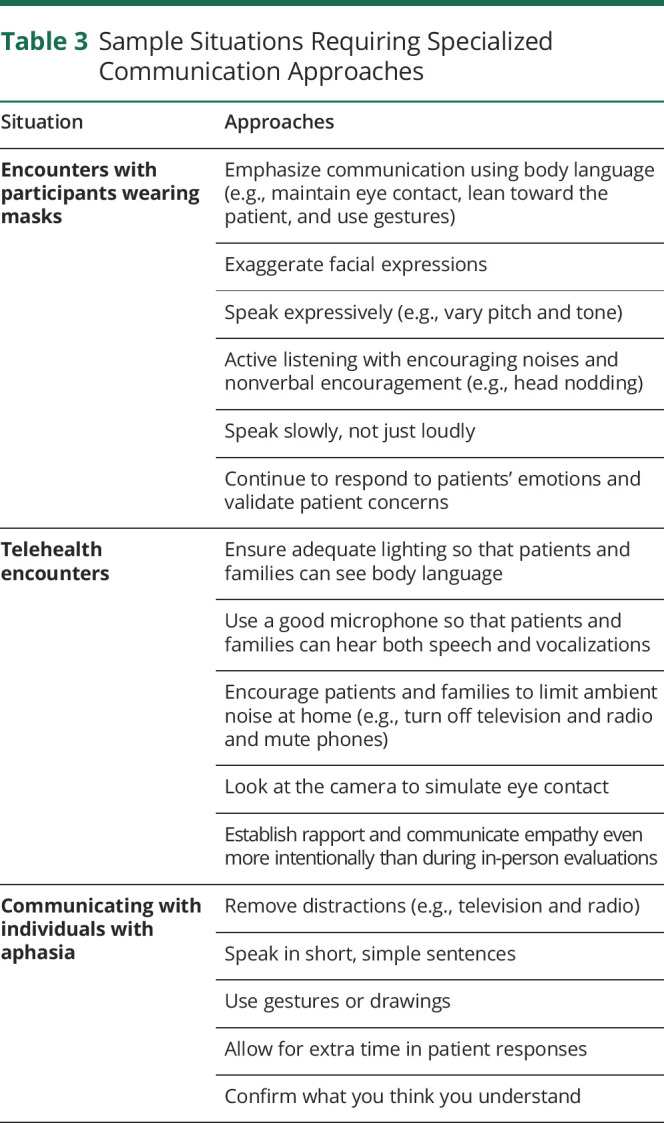
Good communication practices (Table 1) are relevant across clinical encounters. However, scenarios such as encounters in which masks are required,20 telehealth visits, and settings with specific communication barriers (e.g., aphasia21,22) require increased emphasis on certain approaches, such as limiting distractions and using body language (Table 3). Mnemonics can act as cues for clinicians to remember a set of specific communication skills and tasks for various situations, such as diffusing emotionally charged conversations, breaking bad news,10 and navigating communication in cross-cultural encounters23 (Table 2).
Table 3.
Sample Situations Requiring Specialized Communication Approaches
Electronic Communication
Communication with patients via secure messaging through a patient portal has become an integral part of clinician-patient communication. Electronic communication potentially affects patient care as much as in-person communication.24 Patients value the ability to communicate with their care team using secure messaging24 and report that secure messaging improves self-care, communication, and engagement with clinicians.25 Patients also value the support, partnership, and information-giving that they receive through secure messaging, which are all elements of patient-centered communication.26 Strategies for written communication with patients include keeping sentences short, using first and second person (“I” and “you,”respectively), writing in the active voice (“I prescribed” rather than “you were prescribed”), and using noncommittal language when there is uncertainty. Links to reputable online information can be helpful.27
Neurology-Specific Considerations
Optimal communication practices in neurology largely reflect those in health care as a whole. Implementation of neurology resident communication training identified that communication is more successful when allotting adequate time, empathy is critical to successful interactions, and developing approaches to specific challenging scenarios helps facilitate communication.28 Recent research in neurology palliative care identified the need for a systematic approach to communication in neurodegenerative diseases including early discussions of goals and priorities to inform later decision making, preferably with caregivers present.29 Using standardized language and documenting conversations were also recommended strategies.29
Conclusions
Effective clinician communication with patients and families leads to improved patient- and clinician-related outcomes. As a result, it is increasingly emphasized and measured during neurology training and clinical practice. Clinicians across training levels can implement strategies for improving patient- and family-centered communication, ranging from optimizing communication settings, using verbal and nonverbal skills, differentiating between cognitive and emotional communication, using communication tools to demonstrate respect and empathy, individualizing encounters to patient and family needs, and providing clear explanations. These skills can be tailored for specific settings, such as encounters requiring masks, telemedicine, or electronic communication. By purposefully identifying and incorporating key communication skills in everyday practice, clinicians have the opportunity to improve patient care and satisfaction.
Acknowledgment
Work on this article was partially supported by the Florida Department of Health, Public Health Research, Biomedical Research Program.
Appendix. Authors
Study Funding
Work on this article was partially supported by the Florida Department of Health, Public Health Research, Biomedical Research Program. M.J. Armstrong and C.L. Bylund are funded by grant 20A08; N.J. Weisbrod is funded by grant 9AZ18.
Disclosure
M.J. Armstrong serves on the level of evidence editorial board for Neurology® and related publications (uncompensated) and previously received compensation from the AAN for work as an evidence-based medicine methodology consultant. She receives research support from the NIA (R01AG068128, P30AG047266), the Florida Department of Health (grant 20A08), and as the local PI of a Lewy Body Dementia Association Research Center of Excellence. She receives royalties from the publication of the book Parkinson's Disease: Improving Patient Care, and she has received honoraria for presenting at AAN and International Parkinson and Movement Disorder Society annual meetings. N.J. Weisbrod receives research support from the Florida Department of Health (grant 9AZ18). C.L. Bylund receives compensation from The Leukemia & Lymphoma Society as a consultant on caregiver and communication research projects and programming. She receives research support from the NIH (R01CA234030), The Leukemia & Lymphoma Society, and the Florida Department of Health (grant 20A08). She has received compensation from Amgen as a consultant on shared decision-making projects and the Leukemia & Lymphoma Society on caregiver and clinical trial projects. She receives royalties from Oxford for editing the books Oxford Textbook of Communication in Oncology and Palliative Care, 2nd Edition, and Family Communication About Genetics: Theory and Practice. Full disclosure form information provided by the authors is available with the full text of this article at Neurology.org/cp.
References
- 1.Sico JJ, Sarwal A, Benish SM, et al. Quality improvement in neurology: neurology outcomes quality measurement set. Neurology. 2020;94(22):982-990. [DOI] [PubMed] [Google Scholar]
- 2.Edgar L, Roberts S, Holmboe E. Milestones 2.0: a step forward. J Grad Med Educ. 2018;10(3):367-369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Barratt D, Chiota-McCollum N, Dewey J, et al. Neurology Milestones. Accreditation Council for Graduate Medical Education [online]. Accessed December 21, 2020. acgme.org/Portals/0/PDFs/Milestones/NeurologyMilestones2.0.pdf?ver=2020-12-07-155709-570. [Google Scholar]
- 4.The Accreditation Council for Graduate Medical Education. Supplemental guide: neurology [online]. Accessed December 21, 2020. acgme.org/Portals/0/PDFs/Milestones/NeurologySupplementalGuide.pdf?ver=2020-12-07-154812-677.
- 5.Batbaatar E, Dorjdagva J, Luvsannyam A, Savino MM, Amenta P. Determinants of patient satisfaction: a systematic review. Perspect Public Health. 2017;137(2):89-101. [DOI] [PubMed] [Google Scholar]
- 6.Kelley JM, Kraft-Todd G, Schapira L, Kossowsky J, Riess H. The influence of the patient-clinician relationship on healthcare outcomes: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2014;9(4):e94207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Levinson W, Roter DL, Mullooly JP, Dull VT, Frankel RM. Physician-patient communication. The relationship with malpractice claims among primary care physicians and surgeons. JAMA. 1997;277(7):553-559. [DOI] [PubMed] [Google Scholar]
- 8.Boissy A, Windover AK, Bokar D, et al. Communication skills training for physicians improves patient satisfaction. J Gen Intern Med. 2016;31(7):755-761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Haverfield MC, Tierney A, Schwartz R, et al. Can patient-provider interpersonal interventions achieve the quadruple aim of healthcare? A systematic review. J Gen Intern Med. 2020;35(7):2107-2117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP. SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer. Oncologist. 2000;5(4):302-311. [DOI] [PubMed] [Google Scholar]
- 11.Swayden KJ, Anderson KK, Connelly LM, Moran JS, McMahon JK, Arnold PM. Effect of sitting vs. standing on perception of provider time at bedside: a pilot study. Patient Educ Couns. 2012;86(2):166-171. [DOI] [PubMed] [Google Scholar]
- 12.Tallman K, Janisse T, Frankel RM, Sung SH, Krupat E, Hsu JT. Communication practices of physicians with high patient-satisfaction ratings. Perm J. 2007;11(1):19-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Heritage J, Robinson JD, Elliott MN, Beckett M, Wilkes M. Reducing patients' unmet concerns in primary care: the difference one word can make. J Gen Intern Med. 2007;22(10):1429-1433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kee JWY, Khoo HS, Lim I, Koh MYH. Communication skills in patient-doctor interactions: learning from patient complaints. Health Prof Educ. 2018;4(2):97-106. [Google Scholar]
- 15.Henry SG, Fuhrel-Forbis A, Rogers MA, Eggly S. Association between nonverbal communication during clinical interactions and outcomes: a systematic review and meta-analysis. Patient Educ Couns. 2012;86(3):297-315. [DOI] [PubMed] [Google Scholar]
- 16.Back A, Arnold R, Tulsky J. Mastering Communication With Seriously Ill Patients: Balancing Honesty With Empathy and Hope. 1st ed. Cambride University Press;. 2009. [Google Scholar]
- 17.Quigley DD, Elliott MN, Farley DO, Burkhart Q, Skootsky SA, Hays RD. Specialties differ in which aspects of doctor communication predict overall physician ratings. J Gen Intern Med. 2014;29(3):447-454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bylund CL, Makoul G. Examining empathy in medical encounters: an observational study using the empathic communication coding system. Health Commun. 2005;18(2):123-140. [DOI] [PubMed] [Google Scholar]
- 19.VitalTalk. Responding to emotion: articulating empathy using NURSE statements [online]. Accessed January 5, 2021. vitaltalk.org/guides/responding-to-emotion-respecting/.
- 20.Kerr A, Bylund C. 10 ways to improve patient interactions while wearing a mask. In: MedPage Today [online]. Accessed January 8, 2021. medpagetoday.com/publichealthpolicy/generalprofessionalissues/88113. [Google Scholar]
- 21.van Rijssen MN, Veldkamp M, Bryon E, et al. How do healthcare professionals experience communication with people with aphasia and what content should communication partner training entail? Disabil Rehabil. 2021:1-8. [DOI] [PubMed] [Google Scholar]
- 22.American Stroke Association. Aphasia: communicating through barriers [online]. Accessed March 2, 2021. stroke.org/en/about-stroke/effects-of-stroke/cognitive-and-communication-effects-of-stroke/stroke-and-aphasia/aphasia-communicating-through-barriers.
- 23.Berlin EA, Fowkes WC Jr. A teaching framework for cross-cultural health care. Application in family practice. West J Med. 1983;139(6):934-938. [PMC free article] [PubMed] [Google Scholar]
- 24.Alpert JM, Markham MJ, Bjarnadottir RI, Bylund CL. Twenty-first century bedside manner: exploring patient-centered communication in secure messaging with cancer patients. J Cancer Educ. 2021;36(1):16-24. [DOI] [PubMed] [Google Scholar]
- 25.Mold F, Hendy J, Lai YL, de Lusignan S. Electronic consultation in primary care between providers and patients: systematic review. JMIR Med Inform. 2019;7(4):e13042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Alpert JM, Wang S, Bylund CL, et al. Improving secure messaging: a framework for support, partnership & information-giving communicating electronically (SPICE). Patient Educ Couns. 2020;S0738-3991(20)30645-5. [DOI] [PubMed] [Google Scholar]
- 27.Rayner H, Logan I, Rees P, Shah R. Writing outpatient letters to patients. BMJ. 2020;368:m24. [Google Scholar]
- 28.Watling CJ, Brown JB. Education research: communication skills for neurology residents: structured teaching and reflective practice. Neurology. 2007;69(22):E20-E26. [DOI] [PubMed] [Google Scholar]
- 29.Zhem A, Hazeltine AM, Greer JA, et al. Neurology clinicians' views on palliative care communication “How do you frame this?” Neurol Clin Pract. 2020;10(6):527-534. [DOI] [PMC free article] [PubMed] [Google Scholar]