

Abstract
Background
Digital interventions offer a solution to address the high demand for mental health promotion, especially when facing physical contact restrictions or lacking accessibility. Engagement with digital interventions is critical for their effectiveness; however, retaining users’ engagement throughout the intervention is challenging. It remains unclear what strategies facilitate engagement with digital interventions that target mental health promotion.
Objective
Our aim is to conduct a scoping review to investigate user engagement strategies and methods to evaluate engagement with digital interventions that target mental health promotion in adults.
Methods
This scoping review adheres to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for scoping reviews. The search was conducted in 7 electronic databases from inception to April 2020. The inclusion criteria for studies were as follows: adult (aged ≥18 years) users of digital interventions for mental health promotion from the general population; any digital intervention for mental health promotion; and user engagement strategies described in the intervention design. We extracted the following data items: study characteristics, digital intervention (type and engagement strategy), evaluation of engagement strategy (method and result specifying whether the strategy was effective at facilitating engagement), and features of engagement (extent of use and subjective experience of users).
Results
A total of 2766 studies were identified, of which 16 (0.58%) met the inclusion criteria. The 16 studies included randomized controlled trials (6/16, 37%), studies analyzing process data (5/16, 31%), observational studies (3/16, 19%), and qualitative studies (2/16, 13%). The digital interventions for mental health promotion were either web based (12/16, 75%) or mobile app based (4/16, 25%). The engagement strategies included personalized feedback about intervention content or users’ mental health status; guidance regarding content and progress through e-coaching; social forums, and interactivity with peers; content gamification; reminders; and flexibility and ease of use. These engagement strategies were deemed effective based on qualitative user feedback or responses on questionnaires or tools (4/16, 25%), usability data (5/16, 31%), or both (7/16, 44%). Most studies identified personalized support in the form of e-coaching, peer support through a social platform, personalized feedback, or joint videoconference sessions as an engaging feature.
Conclusions
Personalized support during the intervention, access to social support, and personalized feedback seem to promote engagement with digital interventions for mental health promotion. These findings need to be interpreted with caution because the included studies were heterogeneous, had small sample sizes, and typically did not address engagement as the primary outcome. Despite the importance of user engagement for the effectiveness of digital interventions, this field has not yet received much attention. Further research is needed on the effectiveness of different strategies required to facilitate user engagement in digital interventions for mental health promotion.
Keywords: digital interventions, mental health promotion, engagement, scoping review, mobile phone
Introduction
Background
Mental health promotion and well-being is a global public health challenge because of the high prevalence of mental disorders [1]. Mental health disorders are among the leading causes of global disability-adjusted life years (DALYs), with depressive disorders responsible for 1.8% of the DALYs and anxiety responsible for 1.1% of the DALYs [2]. As such, mental health disorders carry high costs not only for individuals, but also for families, communities, and societies [3]. In the European Union, the costs of mental disorders are estimated as being more than €600 billion (US $694 billion), which represents more than 4% of the gross domestic product across the European Union [3].
Mental health disorders have increased over time globally [2], highlighting the need for the prevention of mental disorders and promotion of mental well-being and mental health of the general population.
To face the challenge of the increasing burden of mental disorders and to address the demand for mental health promotion, technological approaches provide a solution [1]. Digital interventions offer the potential to overcome availability and accessibility barriers, including geographical location and time [1,4,5]. Furthermore, digital interventions for mental health are accessible to internet users who own PCs or mobile devices. Anonymous use is desired to bypass barriers because of the stigma of seeking help for mental health concerns [4,6,7]. Thus, digital interventions may reach different target groups compared with local mental health services [6].
Digital interventions for mental health are defined as interventions that are delivered through a digital platform such as the web [1,4,8], smartphone apps [4,6], SMS text messaging (on any platform) [1], and virtual reality [1,4] and target the prevention or treatment of mental health disorders. These interventions mostly implement techniques related to cognitive behavioral therapy or positive psychology [7] and, in the context of mental health, have been applied in healthy [4,8] and clinical samples [4,6,7]. The effectiveness of such interventions has been addressed by a number of systematic reviews. For example, Lattie et al [4] investigated digital interventions for college students who were either healthy or showed symptoms of psychological distress, depression, or anxiety. The authors found that some interventions, regardless of the type of digital intervention, were effective in improving mental health outcomes, including depression, anxiety, and psychological well-being in general. Furthermore, a systematic review by Weisel et al [6] examined mobile apps for adults with heightened symptom severity of several mental health disorders. Indeed, some interventions such as apps delivering cognitive behavioral therapy were found to be effective in reducing symptoms of depression but not effective in reducing symptoms of anxiety [6]. Overall, the systematic reviews suggest that an important function of digital interventions is to not only address existing clinical symptoms, but also to target the promotion of mental health; in general, enhance mental health promotion. Thus, this scoping review focuses on the application of digital interventions in studies with nonclinical samples for mental health promotion.
Engagement in digital technologies is critical for their effectiveness; however, retaining users’ engagement in digital interventions is challenging [9]. Digital interventions, in general, are prone to attrition because of their self-help and unguided nature [5]. For example, the systematic review by Lattie et al [4] revealed that many digital interventions that targeted the promotion of mental health in college students were effective, but attrition rates (ie, proportion of participants dropping out from the intervention) were high in the investigated trials. In some trials, most of the participants adhered to the first module but did not complete the subsequent modules [4]. Despite some evidence for the effectiveness and benefits of digital interventions for mental health promotion, problems are further encountered in translating the results from research studies into real-life settings [9]. Attrition is frequently reported in real-life settings when using digital interventions for general health and well-being [9] as well as prevention and treatment for specific conditions such as depression [7]. These findings highlight the need to develop strategies to effectively engage users with digital interventions for mental health promotion.
Engagement with digital interventions can be defined as “(1) the extent (e.g. amount, frequency, duration, depth) of usage and (2) a subjective experience characterized by attention, interest, and affect” [10]. The features frequency, duration, and amount refer to temporal use, with “amount” being defined as “total length of each intervention contact.” “Depth” is defined as a “variety of content used” [10]. Accordingly, engagement is described as a multidimensional construct in which users experience sustained behavioral aspects of engagement.
Objective
A synthesis of evidence on engagement strategies is required for digital interventions that address mental health promotion. Our aim is to collate such evidence using a scoping review approach to obtain a broad understanding of how user engagement is explored, measured, and evaluated in the context of digital interventions for mental health promotion. The research questions are as follows:
What strategies are applied to improve user engagement with digital interventions for mental health promotion?
What type of strategies result in better engagement with digital interventions for mental health promotion, and how is this improvement in engagement measured?
Methods
Methodological Details
This scoping review followed the Joanna Briggs Institute Scoping Review Methodology [11] and is reported based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines [12]. Additional methodological details are reported in the multimedia appendices. The completed PRISMA-ScR checklist is shown in Multimedia Appendix 1.
Protocol and Registration
The protocol for this review was prospectively registered at the Open Science Foundation registries [13].
Eligibility Criteria
Primary studies with any design were eligible for inclusion. The studies had to fulfill the following Population, Intervention, Control, and Outcomes characteristics:
Population: Any users of digital interventions for mental health promotion aged ≥18 years from the general population not in a clinical setting.
Intervention: Digital intervention for mental health promotion.
Control: Any comparator, such as another intervention type, or no comparator;
Outcomes:
Any user engagement strategy used in the design of digital interventions for mental health promotion.
Effectiveness of engagement strategies assessed and evaluated after the intervention.
The exclusion criteria were as follows:
Studies without primary data, including reviews, commentaries, letters to the editor, and study protocols.
Studies with clinical samples or specific subpopulations, for example, high-risk groups.
Studies with digital interventions for mental health treatment or health-related fields other than mental health.
Studies that did not report or recommend engagement strategies in the intervention design.
Information Sources
The information sources were the following electronic databases:
MEDLINE through Ovid
CINAHL through EBSCO
The Social Science Citation Index through Web of Science
The Science Citation Index through Web of Science
The Emerging Sources Citation Index through Web of Science
PsycINFO through Ovid
The Cochrane Central Register of Controlled Trials and the Cochrane Database of Systematic Reviews through the Cochrane Library
Search Strategy
The search strategy was developed by the team assisted by an experienced information specialist who subsequently conducted the search. Databases were searched from inception to April 2020, with no language limits applied. The search results for each database are presented in Multimedia Appendix 2. The search structure combined appropriate keywords and controlled vocabulary terms for 3 concepts: digital health interventions, engagement, and mental health. The search syntax for MEDLINE is presented in Multimedia Appendix 3.
Selection of Sources of Evidence
All results were exported to EndNote (Clarivate) reference management software for deduplication and then imported to Covidence (Veritas Health Innovation Ltd) systematic review management software for title, abstract, and full-text screening. In all, 2 authors (MS and LK) independently selected studies based on title or abstract, and any inconsistencies were resolved by consensus during discussion. A list of articles included and excluded for full-text screening are presented in Multimedia Appendix 4.
Data-Charting Process
A data-charting form was developed and calibrated by the team. The team discussed and agreed upon how data items would be selected and coded. In all, 2 authors (MS and LK) tested and calibrated self-developed data-charting forms for each study design until all relevant data were captured. The full data charting was conducted independently by 2 authors (MS and LK), and any discrepancies were discussed until consensus was reached.
Data Items
For each article, the data extracted included the following:
Bibliographic information: title, first author, year of publication, and country.
Study and participant characteristics: study design, aim of the study, sample size, age, and gender of participants.
Characteristics of the digital intervention: mode or type, aim, and content.
Engagement measures: user engagement rate for the intervention, type of tool used to measure user engagement, and features of engagement measured.
Engagement strategies: strategies for user engagement used in the design and effective evaluated user engagement strategy.
Effective engagement strategies were identified for each article based on the authors' analysis of subjective user experience obtained through qualitative methodologies or questionnaires or, if available, based on the percentage of participants engaging with the intervention for a specific duration as determined by objective measures of intervention use.
Study Quality
Consistent with the PRISMA-ScR [12] guidelines, Joanna Briggs Institute Scoping Review Methodology guidance, and the framework proposed by Arksey and O’Malley [14], a quality appraisal was not conducted.
Data Synthesis
The data were divided into groups based on study design. The outcomes were narratively synthesized for each study design.
Results
Selection of Sources of Evidence
A total of 4585 articles were identified across all databases. Of the 4585 articles, 1819 (39.67%) duplicates were removed. On screening of the titles and abstracts of the remaining 2766 studies, 2654 (95.95%) were excluded, and the full texts of 112 (4.05%) articles were downloaded and screened against the inclusion and exclusion criteria. Of these 112 articles, 96 (85.7%) were excluded, and a total of 16 (14.3%) articles were included in this review. Figure 1 provides an overview of the selection process of the articles.
Figure 1.
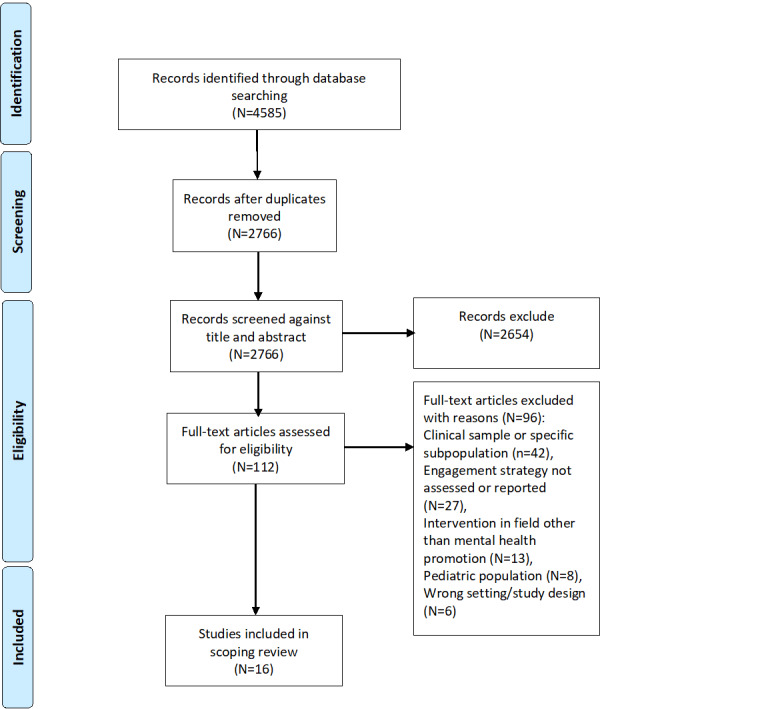
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram.
Study Characteristics
Table 1 presents the general description of the studies. Of the 16 studies, 16 (100%) were published between 2013 and 2020 and originated from Europe (6/16, 37%), North America (6/16, 37%), and Australia (4/16, 25%). The study designs included randomized controlled trials (6/16, 37%), process data studies (5/16, 31%), observational studies (3/16, 19%), and qualitative studies (2/16, 13%). A process data study is a study conducting a secondary analysis on the primary data sets. The digital interventions for mental health promotion were mostly web based (12/16, 75%) or mobile app based (4/16, 25%).
Table 1.
General characteristics of studies (N=16).
| Author, year of publication; countrya | Study design | Type of study | Intervention type (intervention name) |
| Lappalainen et al, 2013 [15]; Finland | RCTb | Feasibility | Web portal (P4 Well) |
| Todkill and Powell, 2013 [16]; United Kingdom | Qualitative study | Evaluation of design | Web based (MoodGym) |
| Morris et al, 2015 [17]; United States | RCT | Efficacy | Web based (Panoply) |
| Clarke et al, 2016 [18]; Australia | Process data study | Evaluation of usability engagement and efficacy | Web based (myCompass) |
| Laurie and Blandford, 2016 [19]; United Kingdom | Qualitative study | Gain insight into user experience | Mobile app (Headspace) |
| Zarski et al, 2016 [20]; Germany | Process data study | Evaluation of use in 3 intervention groups of RCTs | Web based and mobile app (GET.ON Stress) |
| Chou et al, 2017 [21]; United States | Process data study | Evaluation of design | Web based and mobile app (SuperBetter) |
| Dryman et al, 2017 [22]; United States | Process data study | Evaluation of use, engagement, and efficacy | Web based (Joyable) |
| Ly et al, 2017 [23]; Sweden | RCT | Feasibility | Mobile app (Shim) |
| Bakker et al, 2018 [24]; Australia | Cross-sectional | Evaluation of usability and feasibility | Mobile app (MoodMission) |
| Morrison et al, 2018 [25]; United Kingdom | Observational study | Efficacy | Web based and mobile app (Healthy Paths and Healthy Mind) |
| Song et al, 2018 [26]; Canada | Process data study | Evaluation of use and engagement | Web based (Walk Along) |
| Birk and Mandryk, 2019 [27]; United States | RCT | Efficacy | Web based (NRc) |
| Carter et al, 2019 [28]; United States | Cross-sectional | Evaluation of design | Mobile app (NewCope) |
| Przybylko et al, 2019 [29]; Australia | RCT | Efficacy | Web based (The Lift Project) |
| Renfrew et al, 2020 [30]; Australia | RCT | Comparison of 3 modes of engagement strategies | Web based and mobile app (MyWellness) |
aCountry of the corresponding author.
bRCT: randomized controlled trial.
cNR: not reported.
Qualitative Studies
Overview
Of the 16 included studies, 2 (13%) were qualitative studies (36 participants). Both studies reported effective engagement strategies based on user feedback.
Engagement Strategies Used in the Design
Todkill and Powel [16], conducted a qualitative study with 20 participants who used the intervention for 12 weeks. The intervention included of a total of five modules that taught relaxation and meditation techniques, one module per week, web-based workbooks with 29 web-based exercises. No engagement strategy was reported.
Laurie and Blandford [19], conducted a qualitative study with 16 participants who used the intervention for 30 days. The intervention consisted of one audio file for daily guided meditation exercises for 10-15 minutes and a supplementary videos every 3-4 days. The researchers reported following engagement strategies used in intervention design (1) primary task support (audio and video content for meditation); (2) guidance (meditation guided by audio content); (3) third-party endorsement (during sign-up, users read quotes from journalists and celebrities); (4) social support (built-in buddy feature, allowing users to team up with others); (5) trust in provider.
Recommended Engagement Strategies
Both studies recommended the provision of daily challenging content and flexibility and ease of use as useful engagement strategies.
Observational and Process Data Studies
Overview
Of the 16 included studies, 3 (19%) were observational studies (592 participants) and 5 (31%) were process data studies (7000 participants). Table 2 presents the findings of these studies.
Table 2.
Overview of observational and process data studies (n=8).
| Study | Number of participants |
Intervention (duration) | Engagement strategy in intervention design |
Recommended engagement strategy (author conclusion based on engagement rate) |
| Clarke et al, 2016 [18] | 90 | Assessment of users’ self-reported symptoms followed by 24×7 access to a personalized intervention that includes real-time self-monitoring of moods and interactive psychotherapeutic modules (7 weeks) | 1. Reminders to facilitate self-monitoring by SMS text messaging or email as scheduled by the user; 2. Graphical feedback about self-monitoring | 1. Personalized feedback incorporating program content; 2. Alerts and reminders; 3. Flexibility in agenda and use |
| Zarski et al, 2016 [20] | 395 | A total of 7 modules composed of psychoeducation and exercises for every module (4-7 weeks) | CGa: Received intervention; IGb1: Personalized written feedback from e-coach on the completed exercises and reminder by e-coach once in 7 days (content-focused guidance); IG2: Personalized feedback and adherence monitoring on demand of participants (adherence-focused guidance) | Content-focused guidance |
| Chou et al, 2017 [21] | —c | Gamified challenges in browser-based community forum; players can invite other players to browser-based community to form allies (4 weeks) | 1. Gaming language; 2. Social forum; 3. Bright graphics | NRd |
| Dryman et al, 2017 [22] | 3439 | A total of 5 modules: learning through psychoeducation, core skill development by cognitive restructuring, 2 exposure modules, and final graduation module (12 weeks) | 1. Coaches paired with users to provide feedback and support through weekly calls; 2. Coach-initiated and automated emails to encourage participation and progress | Guidance and support through coaching |
| Bakker et al, 2018 [24] | 44 | Assessment of user inputs on distress, followed by daily coping activities or games (30 days) |
1. Games designed with real-time coping strategies; 2. Rewards for daily completed games; 3. Push notifications of incomplete games; 4. Bright graphics | NR |
| Morrison et al, 2018 [25] | 543 | Tools to improve awareness of participants’ thoughts or behaviors and support change in thinking patterns and behaviors (NR) | IG1: web based; IG2: mobile app; 1. Simple and reduced content; 2. Easy accessibility; 3. Push notifications for incomplete tool | IG2: 1. Simple and reduced content; 2. Easy accessibility; 3. Push notifications for incomplete tool |
| Song et al, 2018 [26] | 3076 | Self-help tools and a secure account with access to additional resources and links (NR) | NR | Personal email invitations to visit the site |
| Carter et al, 2019 [28] | 5 | Daily task, user-specific feedback, informational resources, self-assessment page, journal page (NR) | 1. Self-monitoring tools for stress; 2. Goal setting with daily task; 3. User-specific feedback on stress level; 4. Reminders and progress summary | Task with user-specific feedback and self-monitoring |
aCG: control group.
bIG: intervention group.
cNot available.
cNR: not reported.
Engagement Strategies Used in the Design
Of the 16 studies, 4 (25%) integrated personalized feedback about intervention content and users’ stress level as an engagement strategy in the intervention design and used reminder SMS text messaging or email according to users’ demand and progress as an engagement strategy. Moreover, of the 16 studies, 3 (19%) used bright colors and neat graphics as an engagement strategy in the intervention design. Guidance regarding content and progress through e-coaching was used in the intervention design of 13% (2/16) of the studies. Gamification of the content was used as an engagement strategy in the intervention design of 13% (2/16) of the studies. Goal setting and providing rewards were engagement strategies integrated into the intervention design of 13% (2/16) of the studies. Push notifications were identified in 13% (2/16) of the studies, whereas a social forum and interactivity with peers, simple content, and flexibility and ease of use were identified as the engagement strategies used in 6% (1/16) of the studies, separately.
Recommended Engagement Strategies
Effective engagement strategies were identified by the authors based on usability data and user feedback. The engagement measures of these studies are presented in Multimedia Appendix 5 [18,20-22,24-26,28]. Personalized feedback about intervention content and users’ stress level was identified as an effective engagement strategy in 50% (4/8) of the studies. For example, Clarke et al [18] reported on the myCompass program that assessed users’ self-reported symptoms on registration and provided personalized intervention with real-time self-monitoring of moods and behaviors and sent graphical feedback about users’ self-monitoring history alongside contextual information to their phone or PC as an engagement strategy and concluded that it directly enhanced users’ engagement with the program.
In 25% (2/8) of the studies, guidance regarding content and progress through e-coaching was reported as a strategy with the potential to increase engagement. In 25% (2/8) of the studies, implementing reminders according to users’ demand and progress was identified as a beneficial engagement strategy. For example, Zarski et al [19] analyzed 3 forms of guidance through human support and compared the effects on engagement with a stress-management intervention that involved content-focused guidance, adherence-focused guidance, and administrative guidance. Participants in the content-focused guidance group received personalized feedback after completion of every exercise. Participants in the adherence-focused guidance group received a personalized reminder by an e-coach in case of incomplete exercises. Participants in the administrative guidance group were provided with contact information during the study period. Participants in the content-focused guidance group showed the highest engagement, followed by participants in the adherence-focused guidance group and the sample that received administrative guidance. However, content-focused guidance was not significantly associated with higher adherence compared with adherence-focused guidance, indicating that guidance regarding content and progress through e-coaching improved engagement. Flexibility and ease of use was recommended in 25% (2/8) of the studies as an engaging strategy.
Randomized Controlled Trials
Overview
Of the 16 included studies, 6 (37%) were experimental studies (15 arms). Table 3 presents the findings of these studies.
Table 3.
Overview of randomized controlled trials (n=6).
| Study | Participants, n (% female) | Age in years, mean (SD) | Intervention (duration) | Engagement strategy in intervention design by group | Recommended engagement strategy (author conclusion based on the usability of study arms) |
| Lappalainen et al, 2013 [15] | 24 (0) | 47 (7) | A total of 3 group meetings and personal use of web portal, apps, and devices (3 months) | CGa: No intervention; IGb: Personalized feedback | IG: Personalized feedback |
| Morris et al, 2015 [17] | 166 (72) | 24 (5) | Peer-to-peer platform for cognitive reappraisal and socioaffective support and supportive reappraisals from web-based crowd helpers (3 weeks) | CG: Expressive writing, web based; IG: 1. Short content; 2. Positive support messages from peers; 3. Quick feedback any time; 4. Repeated reminders; 5. Accessibility any time | IG: 1. Personalized feedback; 2. Support messages from peers; 3. Flexibility in use |
| Ly et al, 2017 [23] | 28 (54) | 26 (7) | Learn strategies of positive psychology through fully automated conversation, daily check-ins, and weekly summaries (2 weeks) | CG: No intervention; IG: Fully automated chatbot (conversational agent) | IG: Fully automated chatbot |
| Birk and Mandryk, 2019 [27] | 259 (51) | 35 (11) | Customization of avatar, ABMTc, and negative mood induction (3 weeks) | IG1: Customized avatar and ABMT; IG2: Customized avatar and no ABMT; IG3: Generic avatar and ABMT; IG4: Generic avatar and no ABMT | IG1: Avatar customization and personalization |
| Przybylko et al, 2019 [29] | 426 (69) | 47 (16) | Video presenting evidence-based strategies for promoting mental health and emotional wellness, daily and weekly challenges, gamification, and social forum (12 weeks) | CG: No intervention; IG: 1. Real-time coping strategies for daily mission; 2. Social forum with interactive component; 3. Rewards for completing missions; 4. Mission history available; 5. Push notifications alert for incomplete mission; 6. Bright graphics | IG: Interactive components in the social forum |
| Renfrew et al, 2020 [30] | 458 (78) | 46 (1) | Videos, workbook, reading materials related to the topic, and daily and weekly challenges (10 weeks) | CG: Automated email support; IG1: Automated email support and reminder SMS text messaging; IG2: Automated email support and videoconference session per week and 1 reminder SMS text message for videoconference per week | None (Videoconference mode had no effect on intervention engagement, and getting the chosen support style did not result in better engagement or outcomes) |
aCG: control group.
bIG: intervention group.
cABMT: attention bias modification training.
Engagement Strategies Used in the Design
In all, 4 intervention arms in 50% (3/6) of the studies used reminder SMS text messaging or email according to users’ demand and progress as an engagement strategy. Personalized feedback about intervention content and users’ stress level was used as an engagement strategy in 2 intervention arms in 33% (2/6) of the studies. A social forum and interactivity with peers was an engagement strategy in 2 intervention arms in 33% (2/6) of the studies. Easy accessibility and flexibility was used as an engagement strategy in 1 intervention arm. Personalization of content was used as an engagement strategy in 3 intervention arms in 33% (2/6) of the studies. Videoconference sessions with an e-coach were used as an engagement strategy in an intervention arm in 17% (1/6) of the studies. Push notifications were integrated as an engagement strategy in the intervention arm in 17% (1/6) of the studies. Gamification of content was used as an engagement strategy in an intervention arm in 17% (1/6) of the studies.
Renfrew et al [30] compared 3 modes of support differing in resource requirements on the effectiveness of the intervention, that is, automated emails, personalized SMS text messaging, and facilitated videoconference. Participants in the email group received a weekly email before every session with a 20- to 25-second video motivating users to engage. The personalized SMS text messaging group received an automated email and a personalized SMS text message, with the participant’s first name, to prompt engagement, and signature of a research team member, thrice weekly for the first 3 weeks and then twice weekly for the remaining 7 weeks. The reduction in messages was carried out with the perception that support has a threshold and a surfeit of messages may reduce engagement. The members of the videoconference group received automated email support and were invited to attend a videoconference session once a week. User engagement was not significantly different among the 3 groups, although notable variability in responses within the groups was indicated by a large SD.
Recommended Engagement Strategies
Engagement strategies were reported by authors based on usability data of different study arms. Engagement measures are presented in Multimedia Appendix 6 [15,17,23,27,29,30]. Of the 6 studies, 2 (33%) identified personalized feedback about intervention content and users’ stress level as an effective engagement strategy, and a social forum and interactivity with peers was identified as a useful engagement strategy in 2 (33%) studies. For example, Przybylko et al [29] included a social forum in the intervention design, where the participants could comment and post pictures regarding daily content. It was concluded that this strategy was highly engaging for users.
Of the 6 studies, 2 (33%) identified content personalization as an effective engagement strategy. For example, Ly et al [23] reported that content personalization through a fully automated chatbot intervention, Shim, which made users learn, reflect, and practice positive psychology through adequate responses and feedback to user’s statements, was found to be highly engaging for users. Birk and Mandryk [27] reported that avatar personalization for the intervention content greatly improved task-specific user engagement.
Features of Engagement and Tools Used
Table 4 and Figure 2 present the features of engagement explored in the different studies and the tools used to measure these features. Of the 16 studies, 13 (81%) measured frequency; 8 (50%) measured duration; 7 (44%) measured amount, attention, affect, and interest; and 3 (19%) measured depth. Of the 16 studies, 12 (75%) used automatic measures, 7 (44%) used self-administered questionnaires, and 5 (31%) used qualitative interviews to evaluate engagement.
Table 4.
Features of engagement and measuring methods (N=16).
| Study | Theory of engagement | Features of engagement | Tool used to measure engagement |
| Lappalainen et al, 2013 [15] | Technology tools | Affect | Questionnaire on perceived utility and acceptance |
| Lappalainen et al, 2013 [15] | Technology tools | Frequency | Automatic+questionnaire and number of log-ins |
| Todkill and Powell, 2013 [16] | —a | Affect, attention, and interest | Interviews on content, medium, functionalities, and experience |
| Morris et al, 2015 [17] | Technological interaction and consumption | Attention, interest, and depth | UEQb+interview |
| Morris et al, 2015 [17] | Technological interaction and consumption | Amount, duration, and frequency | Automatic; time per session, time of intervention use total, and number of log-ins |
| Clarke et al, 2016 [18] | — | Affect | Interview |
| Clarke et al, 2016 [18] | — | Frequency | Automatic; number of log-ins, number of modules completed, frequency of self-monitoring, and interviews |
| Laurie and Blandford, 2016 [19] | — | Affect, attention, and interest | Interview and qualitative interviews |
| Laurie and Blandford, 2016 [19] | — | Frequency | Automatic; frequency of app use over study period |
| Zarski et al, 2016 [20] | — | Duration and frequency | Automatic; number of completed modules |
| Chou et al, 2017 [21] | — | Interest, depth, duration, and frequency | Automatic; completion rate of intervention |
| Dryman et al, 2017 [22] | Motivational techniques delivered by coaches | Frequency and duration | Automatic; average number of days in the program, average activities per participant, and completion rate of all modules |
| Ly et al, 2017 [23] | Fully automated conversational agent | Affect, attention, and interest | Interview |
| Ly et al, 2017 [23] | Fully automated conversational agent | Frequency | Automatic; number of reflections completed, number of active days, open app ratio, and interviews on content, medium, and functionalities |
| Bakker et al, 2018 [24] | Recommendations by Bakker et al [31] (2016) | Affect, attention, interest, depth, and frequency | Questionnaire, uMARSc, text-entry questions, and HRS-MAd |
| Morrison et al, 2018 [25] | Recommendation by Dennison et al [32] (2013) | Affect and attention | Questionnaire on satisfaction with the intervention, PEIe, and TAM-2f |
| Morrison et al, 2018 [25] | Recommendation by Dennison et al [32] (2013) | Duration and frequency | Automatic; total time of intervention use, time per log-in, and number of log-ins |
| Song et al, 2018 [26] | — | Interest, amount, duration, and frequency | Automatic; number of pages accessed per session, time per session, goal conversion rate, number of returning users, bounce rate, and number of pages accessed per session |
| Birk and Mandryk, 2019 [27] | Self-determination theory | Attention | Questionnaire and Player Identification Scale |
| Carter et al, 2019 [28] | Patient engagement framework | Frequency, attention, and interest | Automatic+questionnaire; percentage of task completion per user, average completion time of tasks, average CSATg scale score, Nielsen–Shneiderman heuristics, and SUSh |
| Przybylko et al, 2019 [29] | Experiential pedagogical framework | Duration | Automatic; attrition rate |
| Renfrew et al, 2020 [30] | SAMi | Duration Frequency |
Automatic; total duration of videos viewed, number of videoconference sessions attended, and challenge score |
aNot available.
bUEQ: User Experience Questionnaire.
cuMARS: Mobile Application Rating Scale, user version.
dHRS-MA: Homework Rating Scale-Mobile Application.
ePEI: Patient Enablement Instrument.
fTAM-2: Technology Acceptance Model-2.
gCSAT: Customer Satisfaction.
hSUS: System Usability Scale.
iSAM: Supportive Accountability Model.
Figure 2.
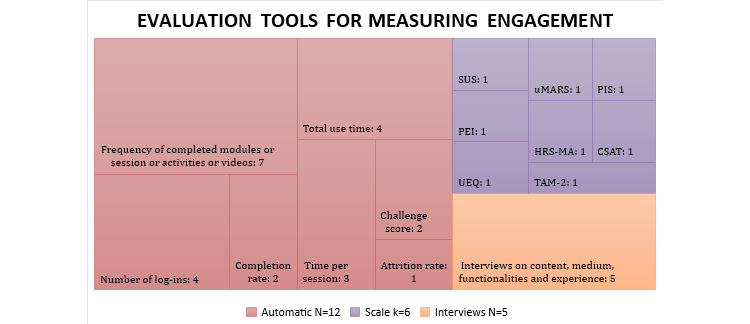
Evaluation tools for measuring engagement used in included studies. (Tool used for engagement measurement: number of studies using it). CSAT: Customer Satisfaction Scale; HRS-MA: Homework Rating Scale-Mobile Application; PEI: Patient Enablement Instrument; PIS: Player Identification Scale; SUS: System Usability Scale; TAM-2: Technology Acceptance Model-2; UEQ: User Experience Questionnaire; uMARS: Mobile Application Rating Scale, user version.
Discussion
Principal Findings
This scoping review aims to identify the strategies that improve user engagement and explore how the engagement is evaluated in the context of digital interventions for mental health promotion. The findings from this scoping review suggest that there are 6 strategies that can positively influence engagement, with various design features to implement them. The methods to measure engagement included objective measures of technology use and subjective measures of user experience through questionnaires or qualitative interviews.
The key finding of our review is that strategies such as personalization, e-coaching, social forums, reminders, gamification, and flexibility and ease of use seem to promote engagement with digital interventions for mental health promotion.
Comparison With Prior Work
Our review corresponds to previous findings in the broader literature of digital health well-being interventions and digital behavior change interventions, which concluded that personalization, support, and guidance through the intervention’s duration can increase user engagement and uptake [9,10]. Similar to previous studies, one of the most recommended strategies for increasing engagement identified in this review is e-coaching and human support [9,10,33]. Another interesting finding of this review is that personalization of intervention content or advanced design features that mimic human support, such as an automated chatbot or avatar customization, can increase engagement. This was also recently demonstrated in an experimental study on a smoking cessation app: users who were provided support through an automated chatbot were found to have higher engagement than users without the automated chatbot [34]. Other engagement strategies identified in this review include reminders, gamification (goals and rewards), and flexibility and ease of use. Likewise, Perski et al [10] identified reminders and incentives as engaging strategies in digital behavior change interventions. The authors also reported certain delivery features that they hypothesized to positively influence engagement. These included an esthetic design, ease of use, and the right message tone.
In general, digital interventions for mental health need to adopt some suitable strategies to motivate users to take up and continue use as well as use the full potential of the intervention [9]. In the following section, each of the identified engagement strategies and design features to tailor them are discussed in turn.
Engagement Strategies
Personalization
Engagement strategies that incorporate personalization and allow customizing to user requirements and needs seem to enhance engagement [15-18,23,26-28]. The included studies used various design features to tailor personalization, including feedback on content, feedback on stress level, and personalization of intervention content. Personalized feedback and personalization of content were identified as strategies with the potential to increase user engagement.
The results here are comparable to those across mental health [35] and other areas of health promotion, such as in smoking cessation [36], physical activity promotion [37], and suicide prevention [38]. In the initial stage, the intervention can be tailored to user expectations on autonomy versus support. Accordingly, the level and kind of support provided during the intervention can be adapted to the user’s preference [5]. Examples of individualized support are personalized feedback and reminders [5].
e-Coaching
Guidance through e-coaching is another engagement strategy identified in this scoping review. The included studies [20,22,30] have used content-focused guidance and adherence-focused guidance design features, and evaluation has found them to greatly increase user engagement.
Previous research has demonstrated that e-coaching led to better engagement with digital interventions for mental health. Persuasive e-coaching and guidance have been associated with better treatment outcome, engagement, and retention in psychological web-based interventions for the treatment of depression according to a systematic review [33]. Although a recent scoping review concluded that providing structured support improved engagement with an internet-based psychological intervention, the variability in the provision of human support, such as delivery mode, intensity, and type, resulted in heterogeneous outcomes, making comparisons difficult [39].
Social Forum
Social forums and interactivity with peers has been identified as a strategy to increase user engagement with digital interventions for mental health promotion [17,21,29]. This has also been supported by recent studies that found that human interaction of any kind is greatly valued by users of digital interventions for mental health [6]. Therefore, human influence should be accorded the same priority as the technology itself [1]. A narrative review recommended that social forums and social media should be harnessed to provide mental health services for youth to increase access to, and engagement with, digital therapeutic solutions for their mental health [40].
Reminders
Reminders have been identified as an engagement strategy in various included studies [17,18,22,25,28-30]. Different design features have been used to tailor reminders: push notifications, personalized SMS text messaging, personalized email, reminder SMS text messaging or email by an e-coach according to the use pattern of the user, and passive reminder SMS text message or email. Personalized SMS text messaging and reminder SMS text messaging or email by an e-coach according to the use pattern of the user have the potential to greatly increase engagement.
Consistent with this finding, a factorial screening experiment explored the impact of 4 different types of SMS text messages on a behavior change smoking cessation intervention and demonstrated that reminders through SMS text messaging based on users’ use pattern of content can boost overall levels of engagement with the intervention [41].
Gamification
Gamification of content has been identified as an engagement strategy in this scoping review [19,21,24,28,29]. Various design features have been used in the intervention designs of the included studies to tailor gamification. These include gamification of content, goal setting, rewards or badges for a completed mission, and provision of new content daily.
A systematic review examining the effect of gamification on adherence to web-based interventions for mental health treatment concluded that various gamification features have been incorporated in the design of web-based interventions. The effect of gamification on user engagement and adherence remains inconclusive because this has not been explored explicitly [42].
Flexibility and Ease of Use
Flexibility and ease of use was identified as an engagement strategy in this review. Various design features such as flexibility of content use, offline availability of content, bright graphics, big colorful icons, easy-to-understand content, and web-based and mobile app options have been used in the included studies to tailor this strategy. In line with this, the latest literature review analyzed users’ public reviews for mental health apps to gain insights into user perceptions and concluded that ease of use was a feature both liked and recommended by users of mental health apps [35].
Methods to Evaluate Engagement
The methods to evaluate engagement in the included studies can be broadly described as objective users’ use measures and subjective experience measures. The result demonstrates heterogeneous reporting of engagement measures and a wide range of assessment measures and reporting data. The heterogeneity of engagement data makes the result incomparable and hinders the understanding of the effectiveness of engagement strategies. Consistent with this finding, other reviews examining engagement with health and well-being apps also reported heterogeneity of data and incomparable results [9]. In addition, the reviews examining the effectiveness of different design features of a single engagement strategy reported inconclusive findings because of the heterogeneity of data [39,42].
Similarly, a recent systematic review investigating measurement and reporting methods of user engagement with mental health apps concluded that high heterogeneity of the measuring and reporting methods and different methodologies used to assess mental health apps, such as user satisfaction, acceptability, feasibility, and usability, make it difficult to report actual engagement with these apps. In addition, there is a need for careful understanding of engagement before claiming engagement strategies used by these apps as effective engagement strategies [43].
Recommendation for Future Design and Research
First, the engagement strategies identified and recommended in this scoping review were primarily explored as a by-product in the included studies and were not evaluated systematically. Of the 16 studies, only 2 (13%) [20,30] were identified that methodologically explored the effectiveness of different engagement strategies for user engagement. The remaining studies merely recommended strategies based on the authors’ analysis of user feedback or participant use data for the intervention. This shows that, so far, the focus has only been on effectiveness, acceptability, feasibility, or use of digital technologies for mental health promotion and there is a lack of interest in the effectiveness of engagement strategies because the interventions address healthy people rather than clinical samples. Thus, more experimental studies are required to investigate the effectiveness of engagement strategies for digital technologies for mental health promotion based on the percentage of participants who report their engagement with such technologies.
In addition, the identified engagement strategies are presented as a separate component in this scoping review. However, these strategies have been used in combination in the intervention designs of the included studies. A review of digital mental health interventions recommended the incorporation of different persuasive technological features that can result in different synergies compared with their use [44]. Therefore, future studies should focus on exploring and evaluating various engagement strategies, their dosage, and different combinations to identify the most effective set of strategies for use and engagement.
Second, engagement was explored and measured heterogeneously. Even among studies with the same designs, the reported engagement data were heterogeneous, making it impossible to determine the most effective engagement strategy. The approach to implementing engagement strategies for digital health interventions is relatively new and highly varied. There is a need for harmonization of research, evaluation, and reporting standards to produce high-quality evidence for engagement. This could be achieved with the development and adoption of guidelines or a minimum set of indicators to measure engagement. Furthermore, digital technologies allow for the creation of large data sets that may be used to assess outcomes based on engagement with specific intervention components [45]. More research is required to identify what characteristics or correlates of engagement can be consistently recorded over time to investigate how engagement changes over time and how engagement is related to the intervention’s duration, as well as to develop new statistical approaches for analyzing these large and complex data sets. Future research should also report attrition rates to explore possible relationships between engagement and attrition.
Third, research is required on the healthy level of engagement to achieve the desired outcomes and reduce attrition. In general, the optimal dose of engagement is still unclear in the field of digital health interventions. Yardley et al [46] propose that establishing and promoting “effective engagement” rather than merely “more engagement” may be more useful for digital interventions for behavior change, with “effective engagement” defined as “sufficient participation with the intervention to accomplish desired effects.” The findings of Zhang et al [47] suggest that digital apps addressing mental health should follow the Goldilocks concept of just right. Like many other digital technologies, mental health apps do not ensure that the more the engagement, the better the results. The benefits of using an app can only be achieved when the dosages of various sorts of intervention features are just right. Exhaustion can result from too much engagement, whereas inefficiency might result from too little engagement. As a result, mental health technology should be designed in such a way that it encourages optimal use [47]. Fourth, engagement was not explored in depth. Most of the studies explored the objective measures of technology use, including frequency, duration, and amount, whereas subjective measures of user experience, such as affect, attention, and interest, were explored less commonly. Engagement with digital interventions for behavior change can be described as the extent of use and subjective experience [10]. Perski et al [10] conceptualized engagement with digital behavior change interventions and proposed a framework through a systematic interdisciplinary approach to assess different features of engagement. The authors emphasized that the future research avenue should include assessment of all features of engagement to reduce the fragmentation in digital health research and establish standard optimal procedures to achieve engagement across different kinds of digital behavior change interventions [10]. Although objective measures of technology use can provide data on user engagement, the exploration of subjective measures of user experience can help in identifying correlates of engagement. Therefore, future studies should explore engagement features in depth, that is, both objective use and subjective experience measures, to generate better evidence for engagement with digital interventions.
Limitations
To our knowledge, this is the first scoping review to explore engagement strategies for digital interventions for mental health promotion. The findings have been summarized taking into consideration the authors’ recommendations based on user engagement data or user feedback. Nevertheless, this review includes a few limitations. It focuses on digital interventions for mental health promotion for the nonclinical population; thus, the findings may not be applicable to other settings. Another limitation is that our inclusion criteria were very narrow for a scoping review, and it cannot be ruled out that studies with clinical samples included healthy control groups that could have been included in this scoping review. This review included only published data and excluded gray literature; therefore, some relevant literature may have been missed.
Conclusions
Various engagement strategies have been reported in digital interventions for mental health promotion, including personalization, human and social support, gamification, personalized feedback, and reminders. User engagement was predominantly reported in terms of frequency, duration, and amount, as well as subjectively (affect, attention, and interest). Human support and e-coaching during the intervention, access to social support, human support–mimicking design features, and personalized feedback or reminders may work best to promote engagement. The findings need to be interpreted with caution because the included studies were heterogeneous, had small sample sizes, and typically explored engagement strategies only as a by-product. All studies were from high-income, nonclinical settings that may not be applicable to other contexts. Despite the importance of user engagement for the effectiveness of digital interventions, this area has not yet received much attention; therefore, conclusions cannot be drawn regarding the most effective engagement strategy because of the heterogeneity of data. Further experimental research is needed on the effectiveness of different types of engagement strategies to facilitate user engagement with digital interventions for mental health promotion.
Acknowledgments
The authors gratefully acknowledge the support of the Leibniz ScienceCampus Digital Public Health Bremen, which is jointly funded by the Leibniz Association (W4/2018), the Federal State of Bremen, and the Leibniz Institute for Prevention Research and Epidemiology–BIPS. The publication of this article was funded by the Open Access Fund of the Leibniz Association.
Abbreviations
- DALY
disability-adjusted life year
- PRISMA-ScR
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) Extension for Scoping Reviews checklist.
Systematic searches of electronic databases.
Search syntax for primary studies in MEDLINE.
Full-text assessment and list of excluded studies.
Overview of observational and process data studies.
Overview of experimental studies.
Footnotes
Authors' Contributions: MS, HB, and TB conceived and planned the study. MS developed the protocol. LC assisted in the development of the search strategy and conducted the literature search for this review. HB and TB verified the analytic methodology for the scoping review and were responsible for overall supervision. MS and LK conducted title and abstract screening and full-text screening. HB resolved conflicts during the screening. MS developed data charts for extraction in consultation with HB. MS and LK extracted data. MS, LK, and KKDS wrote the manuscript. All authors discussed the results and commented on, and approved, the final manuscript.
Conflicts of Interest: None declared.
References
- 1.Rudd BN, Beidas RS. Digital mental health: the answer to the global mental health crisis? JMIR Ment Health. 2020 Jun 02;7(6):e18472. doi: 10.2196/18472. https://mental.jmir.org/2020/6/e18472/ v7i6e18472 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.GBD 2019 DiseasesInjuries Collaborators Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020 Oct 17;396(10258):1204–22. doi: 10.1016/S0140-6736(20)30925-9. https://linkinghub.elsevier.com/retrieve/pii/S0140-6736(20)30925-9 .S0140-6736(20)30925-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Health at a Glance: Europe 2018 (Summary in Greek) / Health at a Glance: Europe 2018. Online: OECD Library; 2018. [Google Scholar]
- 4.Lattie EG, Adkins EC, Winquist N, Stiles-Shields C, Wafford QE, Graham AK. Digital mental health interventions for depression, anxiety, and enhancement of psychological well-being among college students: systematic review. J Med Internet Res. 2019 Jul 22;21(7):e12869. doi: 10.2196/12869. https://www.jmir.org/2019/7/e12869/ v21i7e12869 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Patel S, Akhtar A, Malins S, Wright N, Rowley E, Young E, Sampson S, Morriss R. The acceptability and usability of digital health interventions for adults with depression, anxiety, and somatoform disorders: qualitative systematic review and meta-synthesis. J Med Internet Res. 2020 Jul 06;22(7):e16228. doi: 10.2196/16228. https://www.jmir.org/2020/7/e16228/ v22i7e16228 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Weisel KK, Fuhrmann LM, Berking M, Baumeister H, Cuijpers P, Ebert DD. Standalone smartphone apps for mental health-a systematic review and meta-analysis. NPJ Digit Med. 2019 Dec 2;2:118. doi: 10.1038/s41746-019-0188-8. doi: 10.1038/s41746-019-0188-8.188 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Burger F, Neerincx MA, Brinkman W. Technological state of the art of electronic mental health interventions for major depressive disorder: systematic literature review. J Med Internet Res. 2020 Jan 20;22(1):e12599. doi: 10.2196/12599. https://www.jmir.org/2020/1/e12599/ v22i1e12599 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Powell J, Williams V, Atherton H, Bennett K, Yang Y, Davoudianfar M, Hellsing A, Martin A, Mollison J, Shanyinde M, Yu L, Griffiths KM. Effectiveness and cost-effectiveness of a self-guided internet intervention for social anxiety symptoms in a general population sample: randomized controlled trial. J Med Internet Res. 2020 Jan 10;22(1):e16804. doi: 10.2196/16804. https://www.jmir.org/2020/1/e16804/ v22i1e16804 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Szinay D, Jones A, Chadborn T, Brown J, Naughton F. Influences on the uptake of and engagement with health and well-being smartphone apps: systematic review. J Med Internet Res. 2020 May 29;22(5):e17572. doi: 10.2196/17572. https://www.jmir.org/2020/5/e17572/ v22i5e17572 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Perski O, Blandford A, West R, Michie S. Conceptualising engagement with digital behaviour change interventions: a systematic review using principles from critical interpretive synthesis. Transl Behav Med. 2017 Jun;7(2):254–67. doi: 10.1007/s13142-016-0453-1. http://europepmc.org/abstract/MED/27966189 .10.1007/s13142-016-0453-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.11.2.7 Data extraction. JBI Manual for Evidence Synthesis. 2020. [2021-11-11]. https://jbi-global-wiki.refined.site/space/MANUAL/3283910928 .
- 12.Tricco AC, Lillie E, Zarin W, O'Brien KK, Colquhoun H, Levac D, Moher D, Peters MD, Horsley T, Weeks L, Hempel S, Akl EA, Chang C, McGowan J, Stewart L, Hartling L, Aldcroft A, Wilson MG, Garritty C, Lewin S, Godfrey CM, Macdonald MT, Langlois EV, Soares-Weiser K, Moriarty J, Clifford T, Tunçalp Ö, Straus SE. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018 Oct 02;169(7):467–73. doi: 10.7326/M18-0850. https://www.acpjournals.org/doi/abs/10.7326/M18-0850?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed .2700389 [DOI] [PubMed] [Google Scholar]
- 13.Effective user’s engagement strategies for digital mental health interventions: a scoping review protocol. OSF Registries. 2020. [2021-11-09]. https://osf.io/9xyg7 .
- 14.Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005 Feb;8(1):19–32. doi: 10.1080/1364557032000119616. [DOI] [Google Scholar]
- 15.Lappalainen P, Kaipainen K, Lappalainen R, Hoffrén H, Myllymäki T, Kinnunen M, Mattila E, Happonen AP, Rusko H, Korhonen I. Feasibility of a personal health technology-based psychological intervention for men with stress and mood problems: randomized controlled pilot trial. JMIR Res Protoc. 2013 Jan 09;2(1):e1. doi: 10.2196/resprot.2389. https://www.researchprotocols.org/2013/1/e1/ v2i1e1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Todkill D, Powell J. Participant experiences of an internet-based intervention and randomised control trial: interview study. BMC Public Health. 2013 Oct 28;13:1017. doi: 10.1186/1471-2458-13-1017. https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-13-1017 .1471-2458-13-1017 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Morris RR, Schueller SM, Picard RW. Efficacy of a web-based, crowdsourced peer-to-peer cognitive reappraisal platform for depression: randomized controlled trial. J Med Internet Res. 2015 Mar 30;17(3):e72. doi: 10.2196/jmir.4167. https://www.jmir.org/2015/3/e72/ v17i3e72 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Clarke J, Proudfoot J, Whitton A, Birch M, Boyd M, Parker G, Manicavasagar V, Hadzi-Pavlovic D, Fogarty A. Therapeutic alliance with a fully automated mobile phone and web-based intervention: secondary analysis of a randomized controlled trial. JMIR Ment Health. 2016 Feb 25;3(1):e10. doi: 10.2196/mental.4656. https://mental.jmir.org/2016/1/e10/ v3i1e10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Laurie J, Blandford A. Making time for mindfulness. Int J Med Inform. 2016 Dec;96:38–50. doi: 10.1016/j.ijmedinf.2016.02.010.S1386-5056(16)30030-2 [DOI] [PubMed] [Google Scholar]
- 20.Zarski A, Lehr D, Berking M, Riper H, Cuijpers P, Ebert DD. Adherence to Internet-Based Mobile-Supported Stress Management: A Pooled Analysis of Individual Participant Data From Three Randomized Controlled Trials. J Med Internet Res. 2016 Jun 29;18(6):e146. doi: 10.2196/jmir.4493. https://www.jmir.org/2016/6/e146/ v18i6e146 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Chou T, Bry LJ, Comer JS. Multimedia field test: evaluating the creative ambitions of SuperBetter and its quest to gamify mental health. Cognit Behav Pract. 2017 Feb;24(1):115–20. doi: 10.1016/j.cbpra.2016.10.002. [DOI] [Google Scholar]
- 22.Dryman MT, McTeague LM, Olino TM, Heimberg RG. Evaluation of an open-access CBT-based Internet program for social anxiety: patterns of use, retention, and outcomes. J Consult Clin Psychol. 2017 Oct;85(10):988–99. doi: 10.1037/ccp0000232.2017-27625-001 [DOI] [PubMed] [Google Scholar]
- 23.Ly KH, Ly A, Andersson G. A fully automated conversational agent for promoting mental well-being: a pilot RCT using mixed methods. Internet Interv. 2017 Dec;10:39–46. doi: 10.1016/j.invent.2017.10.002. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(17)30091-X .S2214-7829(17)30091-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bakker D, Kazantzis N, Rickwood D, Rickard N. Development and pilot evaluation of smartphone-delivered cognitive behavior therapy strategies for mood- and anxiety-related problems: MoodMission. Cognit Behav Pract. 2018 Nov;25(4):496–514. doi: 10.1016/j.cbpra.2018.07.002. [DOI] [Google Scholar]
- 25.Morrison LG, Geraghty AW, Lloyd S, Goodman N, Michaelides DT, Hargood C, Weal M, Yardley L. Comparing usage of a web and app stress management intervention: an observational study. Internet Interv. 2018 Jun;12:74–82. doi: 10.1016/j.invent.2018.03.006. https://linkinghub.elsevier.com/retrieve/pii/S2214-7829(18)30006-X .S2214-7829(18)30006-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Song MJ, Ward J, Choi F, Nikoo M, Frank A, Shams F, Tabi K, Vigo D, Krausz M. A process evaluation of a web-based mental health portal (WalkAlong) using Google Analytics. JMIR Ment Health. 2018 Aug 20;5(3):e50. doi: 10.2196/mental.8594. https://mental.jmir.org/2018/3/e50/ v5i3e50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Birk MV, Mandryk RL. Improving the efficacy of cognitive training for digital mental health interventions through avatar customization: crowdsourced quasi-experimental study. J Med Internet Res. 2019 Jan 08;21(1):e10133. doi: 10.2196/10133. https://www.jmir.org/2019/1/e10133/ v21i1e10133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Carter L, Rogith D, Franklin A, Myneni S. NewCope: a theory-linked mobile application for stress education and management. Stud Health Technol Inform. 2019 Aug 21;264:1150–4. doi: 10.3233/SHTI190406. http://europepmc.org/abstract/MED/31438105 .SHTI190406 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Przybylko G, Morton D, Kent L, Morton J, Hinze J, Beamish P, Renfrew M. The effectiveness of an online multimodal intervention for mental health promotion: a randomised controlled trial - 2020:-. doi: 10.21203/rs.2.12991/v1. (forthcoming) https://www.researchgate.net/publication/340856931_The_effectiveness_of_an_online_multimodal_intervention_for_mental_health_promotion_A_randomised_controlled_trial. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Renfrew ME, Morton DP, Morton JK, Hinze JS, Przybylko G, Craig BA. The influence of three modes of human support on attrition and adherence to a web- and mobile app-based mental health promotion intervention in a nonclinical cohort: randomized comparative study. J Med Internet Res. 2020 Sep 29;22(9):e19945. doi: 10.2196/19945. https://www.jmir.org/2020/9/e19945/ v22i9e19945 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Bakker D, Kazantzis N, Rickwood D, Rickard N. Mental health smartphone apps: review and evidence-based recommendations for future developments. JMIR Ment Health. 2016 Mar 01;3(1):e7. doi: 10.2196/mental.4984. https://mental.jmir.org/2016/1/e7/ v3i1e7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Dennison L, Morrison L, Conway G, Yardley L. Opportunities and challenges for smartphone applications in supporting health behavior change: qualitative study. J Med Internet Res. 2013 Apr 18;15(4):e86. doi: 10.2196/jmir.2583. https://www.jmir.org/2013/4/e86/ v15i4e86 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Richards D, Richardson T. Computer-based psychological treatments for depression: a systematic review and meta-analysis. Clin Psychol Rev. 2012 Jun;32(4):329–42. doi: 10.1016/j.cpr.2012.02.004.S0272-7358(12)00027-X [DOI] [PubMed] [Google Scholar]
- 34.Perski O, Crane D, Beard E, Brown J. Does the addition of a supportive chatbot promote user engagement with a smoking cessation app? An experimental study. Digit Health. 2019 Sep 30;5:2055207619880676. doi: 10.1177/2055207619880676. https://journals.sagepub.com/doi/10.1177/2055207619880676?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed .10.1177_2055207619880676 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Alqahtani F, Orji R. Insights from user reviews to improve mental health apps. Health Informatics J. 2020 Sep;26(3):2042–66. doi: 10.1177/1460458219896492. https://journals.sagepub.com/doi/10.1177/1460458219896492?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed . [DOI] [PubMed] [Google Scholar]
- 36.McClure JB, Shortreed SM, Bogart A, Derry H, Riggs K, St John J, Nair V, An L. The effect of program design on engagement with an internet-based smoking intervention: randomized factorial trial. J Med Internet Res. 2013 Mar 25;15(3):e69. doi: 10.2196/jmir.2508. https://www.jmir.org/2013/3/e69/ v15i3e69 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Carter DD, Robinson K, Forbes J, Hayes S. Experiences of mobile health in promoting physical activity: a qualitative systematic review and meta-ethnography. PLoS One. 2018 Dec 17;13(12):e0208759. doi: 10.1371/journal.pone.0208759. https://dx.plos.org/10.1371/journal.pone.0208759 .PONE-D-18-20417 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Whiteside U, Lungu A, Richards J, Simon GE, Clingan S, Siler J, Snyder L, Ludman E. Designing messaging to engage patients in an online suicide prevention intervention: survey results from patients with current suicidal ideation. J Med Internet Res. 2014 Feb 07;16(2):e42. doi: 10.2196/jmir.3173. https://www.jmir.org/2014/2/e42/ v16i2e42 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Shim M, Mahaffey B, Bleidistel M, Gonzalez A. A scoping review of human-support factors in the context of internet-based psychological interventions (IPIs) for depression and anxiety disorders. Clin Psychol Rev. 2017 Nov;57:129–40. doi: 10.1016/j.cpr.2017.09.003.S0272-7358(17)30097-1 [DOI] [PubMed] [Google Scholar]
- 40.Valentine L, McEnery C, D’Alfonso S, Phillips J, Bailey E, Alvarez-Jimenez M. Harnessing the potential of social media to develop the next generation of digital health treatments in youth mental health. Curr Treat Options Psych. 2019 Sep 11;6(4):325–36. doi: 10.1007/s40501-019-00184-w. [DOI] [Google Scholar]
- 41.Graham AL, Papandonatos GD, Jacobs MA, Amato MS, Cha S, Cohn AM, Abroms LC, Whittaker R. Optimizing text messages to promote engagement with internet smoking cessation treatment: results from a factorial screening experiment. J Med Internet Res. 2020 Apr 02;22(4):e17734. doi: 10.2196/17734. https://www.jmir.org/2020/4/e17734/ v22i4e17734 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Brown M, O'Neill N, van Woerden H, Eslambolchilar P, Jones M, John A. Gamification and adherence to web-based mental health interventions: a systematic review. JMIR Ment Health. 2016 Aug 24;3(3):e39. doi: 10.2196/mental.5710. https://mental.jmir.org/2016/3/e39/ v3i3e39 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ng MM, Firth J, Minen M, Torous J. User engagement in mental health apps: a review of measurement, reporting, and validity. Psychiatr Serv. 2019 Jul 01;70(7):538–44. doi: 10.1176/appi.ps.201800519. http://europepmc.org/abstract/MED/30914003 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Wildeboer G, Kelders SM, van Gemert-Pijnen JE. The relationship between persuasive technology principles, adherence and effect of web-based interventions for mental health: a meta-analysis. Int J Med Inform. 2016 Dec;96:71–85. doi: 10.1016/j.ijmedinf.2016.04.005.S1386-5056(16)30054-5 [DOI] [PubMed] [Google Scholar]
- 45.Murray E, Hekler EB, Andersson G, Collins LM, Doherty A, Hollis C, Rivera DE, West R, Wyatt JC. Evaluating digital health interventions: key questions and approaches. Am J Prev Med. 2016 Nov;51(5):843–51. doi: 10.1016/j.amepre.2016.06.008. http://europepmc.org/abstract/MED/27745684 .S0749-3797(16)30229-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Yardley L, Spring BJ, Riper H, Morrison LG, Crane DH, Curtis K, Merchant GC, Naughton F, Blandford A. Understanding and promoting effective engagement with digital behavior change interventions. Am J Prev Med. 2016 Nov;51(5):833–42. doi: 10.1016/j.amepre.2016.06.015.S0749-3797(16)30243-4 [DOI] [PubMed] [Google Scholar]
- 47.Zhang R, Nicholas J, Knapp AA, Graham AK, Gray E, Kwasny MJ, Reddy M, Mohr DC. Clinically meaningful use of mental health apps and its effects on depression: mixed methods study. J Med Internet Res. 2019 Dec 20;21(12):e15644. doi: 10.2196/15644. https://www.jmir.org/2019/12/e15644/ v21i12e15644 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) Extension for Scoping Reviews checklist.
Systematic searches of electronic databases.
Search syntax for primary studies in MEDLINE.
Full-text assessment and list of excluded studies.
Overview of observational and process data studies.
Overview of experimental studies.