

Surgical construction of a vagina may be indicated in transgender women and cisgender women with congenital or acquired vaginal absence. It has a positive effect on quality of life and generally enables patients to engage in penetrative sexual intercourse. Different surgical techniques exist for vaginal (re)construction (Colebunders, Brondeel, D'Arpa, Hoebeke, & Monstrey, 2017; Bouman et al., 2014). Genital surgery in transgender women is performed by plastic surgeons, urologists and gynecologists.
In transgender women wishing genital gender affirming surgery, penile inversion or penoscrotal vaginoplasty is the most commonly performed procedure for genital (re)construction (Buncamper et al., 2016). Though multiple surgical techniques exist, essential steps are the same. A neovaginal cavity is created between bladder and rectum and an inverted penile skin and/or scrotal flap, with or without additional skin grafting, is used to line this cavity. Intestinal vaginoplasty is mentioned as surgical alternative for patients with shortage of penile skin and those who need to undergo revision vaginoplasty. A pedicled, isolated intestinal, predominantly ileum or sigmoid colon segment is used as neovaginal lining (Labus et al., 2011; van der Sluis et al., 2018). Satisfactory (long-term) results in terms of complications and patient-reported satisfaction have been published (Bouman et al., 2014, 2016).
Excessive neovaginal discharge may have a negative impact on sexual health and quality of life. It may also be indicative of conditions which need treatment. Since various surgical procedures exist to create a neovagina, as mentioned above, it can be hard to differentiate, diagnose and subsequently treat neovaginal symptoms in transgender women. Especially for health professionals with little experience in the transgender field. In this editorial, we propose a diagnostic and treatment algorithm for transgender women who underwent vaginoplasty surgery and subsequently experience neovaginal discharge.
Proposal for a diagnostic and treatment algorithm
Neovaginal discharge in transgender women after penoscrotal vaginoplasty may be caused by wound healing problems, hypergranulation, infection, postoperative necrosis, recto- or urethroneovaginal fistulas, sexually transmitted diseases and bacterial dysbiosis. When intestinal vaginoplasty is performed, inflammatory bowel disease, other types of colitis, diversion neovaginitis and cancer may cause neovaginal discharge. In Figure 1, an overview is presented of possible causes of neovaginal discharge in transgender women after vaginoplasty. A diagnostic and treatment algorithm is proposed. All causes for neovaginal discharge are exemplified further in the manuscript.
Figure 1.
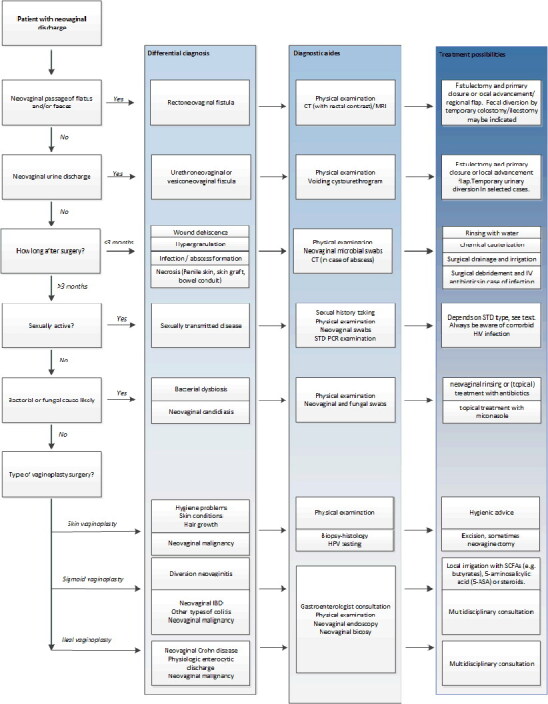
A diagnostic and treatment algorithm of neovaginal discharge in transgender women after vaginoplasty. Differential diagnoses, diagnostic aides and treatment possibilities are provided.
Rectoneovaginal fistula formation
Rectoneovaginal fistulas occur in approximately 1-2% of transgender women after vaginoplasty (van der Sluis et al., 2016a). These are predominantly related to (intra-operative) trauma. Intraoperative rectal perforation, which is more likely to occur during revision vaginoplasty, predisposes for fistula formation (van der Sluis, Bouman, Gijs, & van Bodegraven, 2015). Experienced symptoms comprise foul-smelling, brown, neovaginal discharge with or without neovaginal passage of flatus or feces. Diagnosis is usually based on clinical symptoms and neovaginal examination alone. Though in small fistulas a low-residue diet may be chosen as a first noninvasive treatment option, surgical intervention is frequently necessary. Fistulectomy and subsequent primary closure or closure with a local advancement flap or regional flap may be performed in order to treat the fistula. Fecal diversion by temporary colostomy or ileostomy may be indicated.
Urethroneovaginal fistula formation
Urethroneovaginal fistulas occur in approximately 1% of transgender women after vaginoplasty (van der Sluis et al., 2016a). Meatal stenosis/urethral strictures, which may lead to prestenotic dilation, partial or complete necrosis of the penile-inverted skin flap, and partial or complete neovaginal prolapse may predispose for urethroneovaginal fistula formation. Symptoms comprise neovaginal urine discharge during voiding, a splayed urinary stream, recurrent urinary tract infections and/or position-dependent neovaginal urine discharge. In most patients, fistulectomy and subsequent primary closure or closure with a local advancement flap may be the first line surgical approach for urethroneovaginal fistulas. In selected cases, temporary urinary diversion may be achieved through a suprapubic urinary catheter.
Wound healing problems
Wound dehiscence and hypergranulation
Little is known on the incidence of postoperative wound dehiscence after vaginoplasty surgery. It may arise due to tension on the sutures or secondary to surgical site infection. Generally, expectative treatment is indicated, and the patient is advised to rinse daily with water. Hypergranulation may occur in the early postoperative period, and also -shortly- after secondary corrective surgery. Diagnosis can be made with physical examination. Sometimes, biopsy sampling for histological examination to exclude malignancy may be necessary. Treatment generally consists of chemical cauterization with silver nitrate sticks or topical corticosteroids, which can be performed without anesthesia on an outpatient basis.
Wound infection
The incidence of local wound infections after penile inversion vaginoplasty ranges from 4.0-16.8% in current literature (Bizic, Stojanovic, & Djordjevic, 2017; Buncamper et al., 2016; Horbach et al., 2015). Patients with comorbid diabetes and a history of smoking and illicit substance use have a higher incidence of local wound infections. The incidence of local wound infections after intestinal vaginoplasty is approximately 1-2% (Bouman et al., 2014). When the presence of an abscess is suspected, additional imaging, generally CT scanning, is indicated. Sometimes, neovaginal abcesses can drain spontaneously, however, if not, abscesses should be adequately drained and irrigated.
Neovaginal (graft) necrosis
When full- or partial thickness skin grafts are utilized in the vaginoplasty procedure, partial or no graft take may cause skin graft necrosis. Treatment will consist of revision surgery to remove the necrotized tissue and intravenous antibiotic administration in case of systemic infection. At a second stage, regrafting of the neovaginal cavity may be performed, although a non-surgical approach may be chosen as well (Reed, Yanes, Delto, Omarzai, & Imperatore, 2015; van der Sluis, Bouman, Meijerink, et al., 2016d).
When intestinal vaginoplasty is performed, the intestinal segment used relies on its vascular pedicle for its vascular supply. Intraoperative or postoperative pedicle thrombosis, rupture, or too much tension, may lead to compromised vascularization of the intestinal segment. Neovaginal necrosis is most likely to occur in the early postoperative period. Patients may experience malodorous neovaginal discharge, concomitant abdominal pain and fever. Neovaginal endoscopy to evaluate mucosal ischemia is most accurate, whereas CT-scan with intravenous contrast may be helpful as well.
Sexually transmitted diseases
Although the neovagina is structurally different compared to the vagina of a cisgender woman, sexually transmitted diseases may still be transmitted through unprotected sexual intercourse. Healthcare providers should be ex Wouter tra cautious in patients who exhibit high-risk sexual behavior, for example engaging in sex work (Operario, Soma, & Underhill, 2008; Wilson et al., 2009). Which neovaginal tissue is most susceptible for STD contraction is unknown. Patients with neovaginal gonococcal or chlamydial infection may present with malodorous neovaginal discharge, but infection may also be present in patients without symptoms (Bodsworth, Price, & Davies, 1994; van der Sluis et al., 2015). Neovaginal swabs may be diagnostic for STDs. Treatment may consist of systematic or topical antibiotic administration. When a patient exhibits high-risk sexual behavior whilst having any neovaginal STD, HIV testing should also be considered.
Bacterial dysbiosis
The surgically constructed neovagina is a microbial and fungal niche, which is hardly studied up till now. Common microbial inhabitants of the penile-inverted neovagina are Staphylococcus epidermidis, Streptococcus anginosus, Enterococcus faecalis, Corynebacterium, Mobiluncus curtisii and Bacteroides ureolyticus (Petricevic et al., 2015). Lactobacillus species can also be found (Weyers et al., 2009). The usual microbial inhabitants of the sigmoid neovagina are, as found by culturing techniques, common intestinal bacteria (Toolenaar, Freundt, Wagenvoort, et al., 1993a). Bacterial overgrowth, sometimes described as dysbiosis, may cause neovaginal discharge and discomfort (Jain & Bradbeer, 2007). In these cases, neovaginal swabs may function as a diagnostic aid. When indicated, neovaginal rinsing or (topical) treatment with antibiotics may treat bacterial overgrowth or dysbiosis.
Neovaginal candidiasis
Little is known on the prevalence of neovaginal candidiasis in transgender women. All data on this subject is from one single, retrospective case series (de Haseth et al., 2018). It has only been described in patients after penile-inversion vaginoplasty. Patients may present with white-colored neovaginal, sometimes malodorous discharge and/or with neovaginal itching. In most patients, topical treatment with Miconazole may relief symptoms.
Neovaginal malignancy
Cancer of the neovagina occurs rarely, merely case reports have been published on this subject (Schober, 2007). Cancer of the skin-lined neovagina, frequently HPV-related, is most commonly squamous cell carcinoma. Cancer of the intestine-lined neovagina is usually adenocarcinoma. Diagnosis and staging may be achieved with neovaginoscopy, tumor biopsy, histology and additional imaging to determine the extent of the tumor and lymph node involvement. In case of occurrence of this infrequent type of cancer, oncological, multidisciplinary consultation is warranted. Depending on stadium of the cancer, neovaginectomy according to oncological surgical principles, is most commonly necessary.
Diversion neovaginitis
Luminal nutrients, especially small-chain fatty acids (SCFA), are the primary energy source for colonocytes. Diversion colitis is colonic inflammation caused by a lack of luminal nutrients after surgical diversion of the fecal stream. SCFA deprivation may lead to apoptosis of colonocytes and to an inflammatory mucosal response and epithelial barrier disruption. This has also been observed after sigmoid vaginoplasty (Abbasakoor, Mahon, & Boulos, 2004; Toolenaar, Freundt, Wagenvoort, et al., 1993b). Macroscopically, it is characterized by a diminished vascular pattern, edema, granularity, friability, decreased resilience, and erythema (van der Sluis, Bouman, Meijerink, et al., 2016b). Microscopically, it is characterized by lymphoid aggregates and lymphoplasmacellular infiltrate (van der Sluis, Bouman, Meijerink, et al., 2016c). Symptoms experienced by patients comprise excessive neovaginal discharge and malodor. Noninvasive, medical therapy is the first treatment of choice. These comprise of local irrigation with SCFAs (e.g., butyrates), 5-aminosalicylic acid (5-ASA) or steroids (Luceri et al., 2016). Because of chronic (mild) inflammation of the sigmoid neovagina, long-term follow-up of patients who underwent sigmoid vaginoplasty, seems advisable.
Neovaginal inflammatory bowel disease
Using a bowel segment for a vaginoplasty procedure in patients with comorbid inflammatory bowel disease seems undesirable. However, symptomatic onset of IBD may occur after intestinal vaginoplasty is performed (Froese, Haggitt, & Friend, 1991; Grasman, van der Sluis, & de Boer, 2016; Malka, Anquetil, & Ruszniewski, 2000; Webster et al., 2013). Treatment options comprise topical agents (such as sulfasalazine or mesalamine) or surgical treatment, sometimes even neovaginectomy. However, whether the guidelines for treatment of inflammatory bowel disease may be applicable for diversion vaginitis remains questionable, because neovaginal IBD has only been reported in singular cases.
Discussion
In this article, a proposal for a diagnostic and treatment algorithm for neovaginal discharge in transgender women who underwent vaginoplasty is presented. Neovaginal discharge in transgender women after vaginoplasty may be caused by recto- or urethroneovaginal fistulas, wound healing problems, infection, postoperative necrosis, sexually transmitted diseases, bacterial dysbiosis and malignancy. When intestinal vaginoplasty is performed, inflammatory bowel disease, other types of colitis, diversion neovaginitis and cancer may cause neovaginal discharge. Many aspects must be taken into account, including symptoms, physical examination, type of graft used during surgery and postoperative time. Proper medical history taking, physical examination and knowledge of the surgical procedures, postoperative anatomy, and tissue functionality are critical for a comprehensive and adequate diagnostic process.
A strength of this algorithm is that it is the first of its kind. It may provide useful information for (surgical) health professionals of transgender individuals. As the incidence of transgender people seeking medical and surgical care is increasing significantly, knowledge regarding postoperative medical issues, aiding of the diagnostic process and helping to select proper treatment is important. A weakness of this algorithm is that is primarily based on expert opinion and retrospective case studies. In our center in Amsterdam, the Netherlands, over 1300 vaginoplasty procedures were performed in the period 1990-2019. As we are the only center in the Netherlands offering the full range of surgical treatments for transgender individuals, valuable knowledge of postoperative complications lies within our patient cohort.
Wouter B. van der Sluis
Department of Plastic Reconstructive and Hand Surgery, Amsterdam University Medical Center, Amsterdam, The Netherlands
w.vandersluis@vumc.nl
Kristin B. de Haseth
Department of Plastic Reconstructive and Hand Surgery, Amsterdam University Medical Center, Amsterdam, The Netherlands
Lian Elfering
Department of Plastic Reconstructive and Hand Surgery, Amsterdam University Medical Center, Amsterdam, The Netherlands
Müjde Özer
Department of Plastic Reconstructive and Hand Surgery, Amsterdam University Medical Center, Amsterdam, The Netherlands
Jan Maerten Smit
Department of Plastic Reconstructive and Hand Surgery, Amsterdam University Medical Center, Amsterdam, The Netherlands
Andries E. Budding
Department of Medical Microbiology and Infection Control, Amsterdam University Medical Center, Amsterdam, The Netherlands
Adriaan A. van Bodegraven
Department of Gastroenterology and Hepatology, Amsterdam University Medical Center, Amsterdam, The Netherlands Department of Gastroenterology, Geriatrics, Intensive Care and Internal Medicine, Zuyderland Medical Centre, Geleen, The Netherlands
Marlon E. Buncamper
Department of Plastic Reconstructive and Hand Surgery, Amsterdam University Medical Center, Amsterdam, The Netherlands Department of Plastic Surgery, Ghent University Hospital, Ghent, Belgium
Nanne K. H. de Boer
Department of Gastroenterology and Hepatology, Amsterdam University Medical Center, Amsterdam, The Netherlands
Margriet G. Mullender
Department of Plastic Reconstructive and Hand Surgery, Amsterdam University Medical Center, Amsterdam, The Netherlands
Mark-Bram Bouman
Department of Plastic Reconstructive and Hand Surgery, Amsterdam University Medical Center, Amsterdam, The Netherlands
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Abbasakoor, F., Mahon, C., & Boulos, P.B. (2004). Diversion colitis in sigmoid neovagina. Colorectal Disease, 4, 290–291. doi: 10.1111/j.1463-1318.2004.00653.x [DOI] [PubMed] [Google Scholar]
- Bizic, M. R., Stojanovic, B., & Djordjevic, M. L. (2017). Genital reconstruction for the transgendered individual. Journal of Pediatric Urology, 5, 446–452. doi: 10.1016/j.jpurol.2017.07.015 [DOI] [PubMed] [Google Scholar]
- Bodsworth, N. J., Price, R., & Davies, S. C. (1994). Gonococcal infection of the neovagina in a male-to-female transsexual. Sexually Transmitted Diseases, 4, 211–212. [DOI] [PubMed] [Google Scholar]
- Bouman, M.-B., van Zeijl, M. C. T., Buncamper, M. E., Meijerink, W. J. H. J., van Bodegraven, A. A., & Mullender, M. G. (2014). Intestinal vaginoplasty revisited: A review of surgical techniques, complications, and sexual function. The Journal of Sexual Medicine, 11(7), 1835–1847. doi: 10.1111/jsm.12538 [DOI] [PubMed] [Google Scholar]
- Bouman, M.-B., van der Sluis, W. B., van Woudenberg Hamstra, L. E., Buncamper, M. E., Kreukels, B. P. C., Meijerink, W. J. H. J., & Mullender, M. G. (2016). Patient-reported esthetic and functional outcomes of primary total laparoscopic intestinal vaginoplasty in transgender women with penoscrotal hypoplasia. The Journal of Sexual Medicine, 13(9), 1438–1444. doi: 10.1016/j.jsxm.2016.06.009 [DOI] [PubMed] [Google Scholar]
- Buncamper, M. E., van der Sluis, W. B., van der Pas, R. S. D., Özer, M., Smit, J. M., Witte, B. I., … Mullender, M. G. (2016). Surgical outcome after penile inversion vaginoplasty: A retrospective study of 475 transgender women. Plastic and Reconstructive Surgery, 138(5), 999–1007. doi: 10.1097/PRS.0000000000002684 [DOI] [PubMed] [Google Scholar]
- Colebunders, B., Brondeel, S., D'Arpa, S., Hoebeke, P., & Monstrey, S. (2017). An update on the surgical treatment for transgender patients. Sexual Medicine Reviews, 5(1), 103–109. doi: 10.1016/j.sxmr.2016.08.001 [DOI] [PubMed] [Google Scholar]
- Froese, D. P., Haggitt, R. C., & Friend, W. G. (1991). Ulcerative colitis in the autotransplanted neovagina. Gastroenterology, 100(6), 1749–1752. doi: 10.1016/0016-5085(91)90679-F [DOI] [PubMed] [Google Scholar]
- Grasman, M. E., van der Sluis, W. B., & de Boer, N. K. H. (2016). Neovaginal sparing in a transgender woman with ulcerative colitis. Clinical Gastroenterology and Hepatology, 14(7), e73–74. doi: 10.1016/j.cgh.2016.01.006 [DOI] [PubMed] [Google Scholar]
- Horbach, S. E. R., Bouman, M.-B., Smit, J. M., Özer, M., Buncamper, M. E., & Mullender, M. G. (2015). Outcome of vaginoplasty in male-to-female transgenders: A systematic review of surgical techniques. The Journal of Sexual Medicine, 12(6), 1499–1512. doi: 10.1111/jsm.12868 [DOI] [PubMed] [Google Scholar]
- Jain, A., & Bradbeer, C. (2007). A case of successful management of recurrent bacterial vaginosis of neovagina after male to female gender reassignment surgery. International Journal of STD & AIDS, 18(2), 140–141. doi: 10.1258/095646207779949790 [DOI] [PubMed] [Google Scholar]
- de Haseth, K. B., Buncamper, M. E., Özer, M., Elfering, L., Smit, J. M., Bouman, M.-B., & van der Sluis, W. B. (2018). Symptomatic neovaginal candidiasis in transgender women after penile inversion vaginoplasty: A clinical case series of five consecutive patients. Transgender Health, 3(1), 105–108. doi: 10.1089/trgh.2017.0045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Labus, L. D., Djordjevic, M. L., Stanojevic, D. S., Bizic, M. R., Stojanovic, B. Z., & Cavic, T. M. (2011). Rectosigmoid vaginoplasty in patients with vaginal agenesis: Sexual and psychosocial outcomes. Sexual Health, 8(3), 427–430. doi: 10.1071/SH10105 [DOI] [PubMed] [Google Scholar]
- Luceri, C., Femia, A. P., Fazi, M., Di Martino, C., Zolfanelli, F., Dolara, P., & Tonelli, F. (2016). Effect of butyrate enemas on gene expression profiles and endoscopic/histopathological scores of diverted colorectal mucosa: A randomized trial. Digestive and Liver Disease, 48(1), 27–33. doi: 10.1016/j.dld.2015.09.005 [DOI] [PubMed] [Google Scholar]
- Malka, D., Anquetil, C., & Ruszniewski, P. (2000). Ulcerative colitis in a sigmoid neovagina. New England Journal of Medicine, 343(5), 369–369. doi: 10.1056/NEJM200008033430515 [DOI] [PubMed] [Google Scholar]
- Operario, D., Soma, T., & Underhill, K. (2008). Sex work and HIV status among transgender women: Systematic review and meta-analysis. Jaids Journal of Acquired Immune Deficiency Syndromes, 48(1), 97–103. doi: 10.1097/QAI.0b013e31816e3971 [DOI] [PubMed] [Google Scholar]
- Petricevic, L., Kaufmann, U., Domig, K. J., Kraler, M., Marschalek, J., Kneifel, W., & Kiss, H. (2015). Molecular detection of Lactobacillus species in the neovagina of male-to-female transsexual women. Scientific Reports, 4(1), 3746. doi: 10.1038/srep03746 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reed, H. M., Yanes, R. E., Delto, J. C., Omarzai, Y., & Imperatore, K. (2015). Non-grafted vaginal depth augmentation for transgender atresia, our experience and survey of related procedures. Aesthetic Plastic Surgery, 39(5), 733–744. doi: 10.1007/s00266-015-0523-7 [DOI] [PubMed] [Google Scholar]
- Schober, J. M. (2007). Cancer of the neovagina. Journal of Pediatric Urology, 3(3), 167–170. doi: 10.1016/j.jpurol.2006.07.010 [DOI] [PubMed] [Google Scholar]
- Toolenaar, T. A., Freundt, I., Wagenvoort, J. H., Huikeshoven, F. J., Vogel, M., Jeekel, H., & Drogendijk, A. C. (1993a). Bacterial flora of the sigmoid neovagina. Journal of Clinical Microbiology, 31(12), 3314–3316. doi: 10.1128/JCM.31.12.3314-3316.1993 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toolenaar, T. A., Freundt, I., Huikeshoven, F. J., Drogendijk, A. C., Jeekel, H., & Chadha-Ajwani, S. (1993b). The occurrence of diversion colitis in patients with a sigmoid neovagina. Human Pathology, 24(8), 846–849. doi: 10.1016/0046-8177(93)90134-3 [DOI] [PubMed] [Google Scholar]
- van der Sluis, W. B., Bouman, M.-B., Gijs, L., & van Bodegraven, A. A. (2015). Gonorrhoea of the sigmoid neovagina in a male-to-female transgender. International Journal of STD & AIDS, 26(8), 595–598. doi: 10.1177/0956462414544725 [DOI] [PubMed] [Google Scholar]
- van der Sluis, W. B., Bouman, M.-B., Buncamper, M. E., Pigot, G. L. S., Mullender, M. G., & Meijerink, W. J. H. J. (2016a). Clinical characteristics and management of neovaginal fistulas after vaginoplasty in transgender women. Obstetrics & Gynecology, 127(6), 1118–1126. doi: 10.1097/AOG.0000000000001421 [DOI] [PubMed] [Google Scholar]
- van der Sluis, W. B., Bouman, M. B., Meijerink, W. J., Elfering, L., Mullender, M. G., de Boer, N. K. H., & van Bodegraven, A. A. (2016). Diversion neovaginitis after sigmoid vaginoplasty: Endoscopic and clinical characteristics. Fertility and Sterility, 105(3), 834–839.e1. doi: 10.1016/j.fertnstert.2015.11.013 [DOI] [PubMed] [Google Scholar]
- van der Sluis, W. B., Neefjes-Borst, E. A., Bouman, M.-B., Meijerink, W. J., de Boer, N. K. H., Mullender, M. G., & van Bodegraven, A. A. (2016). Morphological spectrum of neovaginitis in autologous sigmoid transplant patients. Histopathology, 68(7), 1004–1012. doi: 10.1111/his.12894 [DOI] [PubMed] [Google Scholar]
- van der Sluis, W. B., Bouman, M. B., Buncamper, M. E., Mullender, M. G., & Meijerink, W. J. (2016). Revision vaginoplasty: A comparison of surgical outcomes of laparoscopic intestinal versus perineal full-thickness skin graft vaginoplasty. Plastic and Reconstructive Surgery, 138(4), 793–800. doi: 10.1097/PRS.0000000000002598 [DOI] [PubMed] [Google Scholar]
- van der Sluis, W. B., Pavan, N., Liguori, G., Bucci, S., Bizic, M. R., Kojovic, V., … Bouman, M.-B. (2018). Ileal vaginoplasty as vaginal reconstruction in transgender women and patients with disorders of sex development: An international, multicentre, retrospective study on surgical characteristics and outcomes. BJU International, 121(6), 952–958. doi: 10.1111/bju.14155 [DOI] [PubMed] [Google Scholar]
- Webster, T., Appelbaum, H., Weinstein, T. A., Rosen, N., Mitchell, I., & Levine, J. J. (2013). Simultaneous development of ulcerative colitis in the colon and sigmoid neovagina. Journal of Pediatric Surgery, 48(3), 669–672. doi: 10.1016/j.jpedsurg.2012.12.025 [DOI] [PubMed] [Google Scholar]
- Weyers, S., Verstraelen, H., Gerris, J., Monstrey, S., dos Santos Lopes Santiago, G., Saerens, B., … Verhelst, R. (2009). Microflora of the penile skin-lined neovagina of transsexual women. BMC Microbiology, 9(1), 102. doi: 10.1186/1471-2180-9-102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilson, E. C., Garofalo, R., Harris, R. D., Herrick, A., Martinez, M., Martinez, J., Belzer, M., …Transgender Advisory Committee and the Adolescent Medicine Trials Network for HIV/AIDS Interventions. (2009). Transgender female youth and sex work: HIV risk and a comparison of life factors related to engagement in sex work. AIDS and Behavior, 13(5), 902–913. doi: 10.1007/s10461-008-9508-8 [DOI] [PMC free article] [PubMed] [Google Scholar]