

Abstract
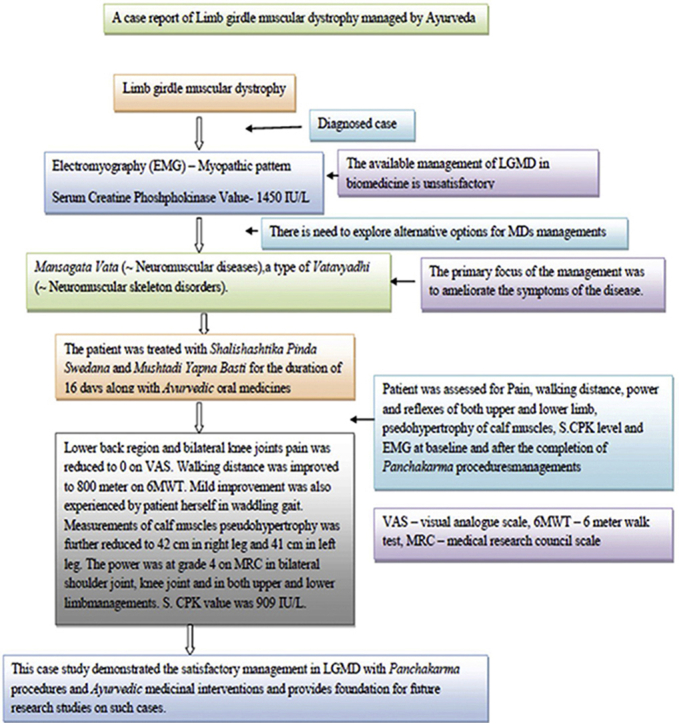
Limb girdle muscular dystrophy (LGMD) is a type of Muscular dystrophy (MD), heterogeneous devastating complex genetic disorders causing progressive weakness and degeneration of muscles. LGMD is hereditary autosomal diseases characterized by weak and wasteful limb girdle muscles. The available management of LGMD in biomedicine is unsatisfactory. Here we present a case of LGMD managed with combinations of Ayurvedic oral medicines and Panchakarma procedures. The Ayurvedic diagnosis of the condition was considered as Mansagata Vata (∼neuromuscular diseases), a type of Vatavyadhi (∼neuromusculo skeleton disorders). The patient was treated with Shalishashtika Pinda Swedana and Mustadi Yapana Basti for the duration of 16 days along with following Ayurvedic oral medicines: Yograj Guggulu 500 mg with 40 ml Dashamoola Kwatha, Ekangaveera Rasa 125 mg with honey, a combination of Ashwagandha Churna -2g, Satavari Churna - 2g, and Sankha Bhasma 500 mg with milk, Narsinha Churna- 3g and Ashwagandhavleha- 5g with milk. All medicines were given twice a day. Patient's condition was assessed for symptoms of pain, walking distance, power and reflexes of both upper and lower limb and psedohypertrophy of both calf muscles. Serum Creatine Phoshphokinase (S.CPK) level and electromyography (EMG) were also measured. There was symptomatic improvement in the patient's condition and reduction in S.CPK level. The study suggests that LGMD can be satisfactorily managed with Ayurvedic oral medicines and Panchakarma therapy.
Keywords: Ayurvedic management, Limb girdle muscular dystrophy, Mansagata vata
Graphical abstract
1. Introduction
Muscular dystrophies (MDs) are genetically heterogeneous cluster of muscle disorders with progressive weakness and muscle wasting. Duchene muscular dystrophy (DMD), Becker muscular dystrophy (BMD), congenital muscular dystrophy (CMD), Myotonicmuscular dystrophy (MMD), Fascioscapulohumeralmuscular dystrophy (FSMD) and Limb girdle muscular dystrophy (LGMD) are common MDs [1] Each of these disorders differs in terms of age of onset, severity, affecting muscle groups and pattern of inheritance [2]. LGMDs are autosomal, heterogeneous neuromuscular disorders of progressive weakness and wasting of the limb girdle muscles [3]. The combined prevalence rate of the MDs range between 19.8–25.1 per 100,000 people per year [4]. Worldwide prevalence rate of LGMDs are 1 in 14,500–45,000 [3]. MD patients are known to have mortality at younger age and there is lack of effective management [5]. There is need to explore alternative options for MDs managements. The present case is first attempted study in Pub Med indexed journals till date to explore Ayurvedic management in MDs with satisfactory outcome. The primary focus of the management was to ameliorate the symptoms of the disease. The Ayurvedic diagnosis was made as Mansagata Vata (∼neuromuscular diseases), a type of Nirupsthambhita (∼disease due to unobstructed Vata Dosha) Vatavyadhi (∼neuromuscular skeleton disorders) [6].
2. Case report
A 35 years old married female patient visited the Panchakarma outpatient department of National Institute of Ayurveda (N.I.A.) on December 4, 2018 with complaints of lower back ache, pain in bilateral knee joints and difficulty in walking and performing routine household activities since past 5 years. Patient was not able to walk more than 10–20 m on flat surface. There was gradual weakening and heaviness (like stones tied to body) in both upper and lower limbs. There was difficulty in getting up from squatting or sitting position, climbing up stairs, lifting heavy objects and doing overhead activities like combing or shampooing hair since last 9 years. The patient had consulted on 12/01/2016 in neurology department of Swai Man Singh medical college and hospital, Jaipur and was diagnosed as LGMD – sarcanoglycopathy. She was advised conservative treatment and genetic analysis. Patient was not satisfied with the treatment and hence approached N.I.A. hospital.
2.1. Clinical finding
Patient was conscious, well oriented, and spoke normally. There was absence of pallor, icterus, clubbing, cyanosis and edema. She had difficulty in walking (waddling gait) and positive Gower's sign. Neurological examination revealed normal Cranial nerve functions, the tone of upper and lower extremities was reduced and grade 4 power was observed in bilateral shoulder joint, knee joint and in both upper and lower limbs. Bilateral Achilles tendon reflexes were diminished. The sensory functions like pain, touch and temperature were normal. Pseudohypertrophy was observed in bilateral calf muscles. Erythrocyte sedimentation rate, Complete blood count and thyroid profile were within normal limits. Serum Creatine Phoshphokinase (S. CPK) was elevated. Electromyography dated 12/01/2016 (EMG) shows the myopathic pattern. Tenfold examination of patient suggested Vatakapha Prakriti (∼physical constitution) Madhyama Samhanana (∼medium body constitution), Avara Sara (∼lowermost purest body tissue), Avara Vyayam Shakti (∼lowermost capability to carry on physical activities), Madhyama Abhyavarana and Jaranashakti (∼middlemost food intake and digestive power). Mansavaha Srotodushti was observed (Vitiation in micro-channels related to muscular tissues) in this patient. Srotasa Pariksha (examinations of other microchannels) revealed normal status of other Srotasas.
3. Timeline (Table 1)
Table 1.
Timeline.
| Year | Incidence/Intervention |
|---|---|
| 2009 | Progressive weakness of both lower limb causing difficulty in getting up from squatting or sitting position and difficulty in climbing stairs. |
| 2012 | Progressive weakness in both upper limbs causing difficulty in lifting heavy objects, doing overhead activities such as combing and shampooing hair. Patient also noticed prominence of both calf muscles. |
| 2014 | Patient suffered from lower back ache, pain in bilateral knee joints and difficulty in walking and activities related to routine house work. |
| 12/01/2016 | Patient consulted in neurology department of Swai Man Singh medical college and hospital, Jaipur for the complaints. Serum CPK was value was 1450 IU/L and EMG suggested of myopathic pattern. Patient was diagnosed as LGMD (sarcanoglycopathy). She was advised conservative treatment and genetic analysis. Only multi-vitamins were prescribed to the patient. |
| 04/12/2018 | Patient was unsatisfied with the management hence approached Panchakarma outpatient department of National Institute of Ayurveda, Jaipur for the complaints of lower back ache, pain in bilateral knee joints and difficulty in walking and household activities since past 5 years. Lower back region and bilateral knee joints pain was grade 5 on visual analogue scale (VAS). She had difficulty in walking (waddling gait) and Positive Gower's sign. Measurements of calf muscles (pseudohypertrophy) were 54.6 cm in right leg and 52.8 cm in left leg. Walking distance on flat surface assessed by 6 min walk test (6MWT) was 10–20 m. The power was at grade 4 on medical research council scale (MRC) in bilateral shoulder joint, knee joint and in both upper and lower limb. Bilateral Achilles tendon reflex were diminished. The Ayurvedic diagnosis of the condition was considered as Mansagata Vata, a type of Vatavyadhi. The management was focused on providing symptomatic relief. The general management of Vatavyadhi was adopted. Shalishashtika Pinda Swedana and Basti Karma were planned with oral medications. |
| 04/12/2018 | Selected Ayurvedic oral medications were –Yograj Guggulu 500 mg with 40 ml Dashamoola Kwatha, a combination of Ashwagandha Churna (powder of Withaniasomnifera Dunal)-2g, Satavari Churna (powder of Asparagus racemosus WILD.)- 2g, and Sankha Bhasma (calx of conch shell)- 500 mg with milk, Narsinha Churna 3 g and Ashwagandhavleha - 5g with milk. All medicines were prescribed twice a day. |
| 10/12/2018–26/12/2019 | Shalishashtika Pinda Swedana and Mustadi Yapana Basti was carried out for 16 days |
| 04/01/2019 | Narsinha Churna was discontinued and rest of the medications were continued till date. |
| 29/03/2019 | Ekangaveera Rasa 125 mg with honey, twice a day was inorporated in daily regime and continued till date. |
| (2/4/19–17/04/2019) | Shalishashtika Pinda Swedana with Mustadi Yapana Basti were repeated for 16 days |
| 17/04/2019 | Patient was assessed for pain, walking distance, power and reflexes of both upper and lower limb with measurement of calf region. Lower back region and bilateral knee joints pain were at grade 3 on VAS. Walking ability was improved to 500 m on 6MWT. Calf muscles measurements were reduced to 51 cm in right leg and 49 cm in left leg. The power was at grade 4 on MRC in bilateral shoulder joint, knee joint and in both upper and lower limb. Bilateral Achilles tendon reflex were 2+. |
| 30/05/2019 | The S. CPK and EMG assessements were repeated after the treatment. S. CPK level was decreased from 1450 IU/L on 11/01/2016 to 909 IU/L on 30/05/2019. No change in EMG was observed. Other blood investigations were within normal limits. |
| 13/09/2019 | Lower back and bilateral knee joints pain was reduced to 0 on VAS. Walking ability was improved to 800 m on 6MWT. Mild improvement in waddling gate was reported by patient herself. Calf muscles pseudohypertrophy was further reduced to 42 cm in right leg and 41 cm in left leg. The power was at grade 4 on MRC in bilateral shoulder joint, knee joint and in both upper and lower limbs. Patient reported that there was no heaviness in the body and she could perform the routine house work with ease. Mild difficulty in climbing up stairs and lifting heavy objects was reported by patient. |
Disease course, management and outcomes.
4. Diagnostic focus and assessment
The patient was a known case of LGMD (sarcanoglycopathy type). The types of muscular dystrophy i.e. DMD, BMD, CMD and FSMD were the potential diagnosis for the case. The age of onset excluded DMD, BMD, and CMD, while normal functioning of cranial nerves excluded FSMD. Heaviness of the body, severe body ache similar to Dandamushthihata (body has been beaten with a cudgel or fist cuffs) and extreme exhaustion are the symptoms of Mansagata Vata [6] which were exhibited in patient. Mansakshaya or Shosh (depletion of muscular tissues) was the differential diagnosis of the disease. Specific part of body involved in pathology ruled out the condition of Mansakshaya. Other Vatavyadhis such as Snayugata Vata and Mansagata Vata which can lead to depletion of muscular tissues were also the potential diagnosis [6 verse 35–36]. But other symptoms of these Vatavyadhis were absent in the case. Systemic examination of other systems and Srotasas Pariksha were normal except Mansavaha Srotodusti hence these were ruled out. Swayathu (edema/inflammation), Mansa Shosh (depletion of muscular tissues, fibrosis of muscles fibers) are the common symptoms due to damages of Mansavaha Srotasas (micro-channels related to muscular tissues) [7]. Difficulties in climbing stairs, walking and rising from the floor also indicate Mansavaha Srotodusti as there is disruption of the function of Mansa Dhatu (∼nutrients related to muscular tissues) which is transferring through these channels. Thus Ayurvedic diagnosis was established as Mansagata Vata, a Nirupsthambhita Vatavyadhi. As the chronicity of disease is more than one year it was considered as Yapya Vyadhi (palliative disease).
5. Treatment plan
The management was focused on providing symptomatic relief. The general management of Vatavyadhi was adopted. Shalishashtika Pinda Swedana [which provided both Snehana (oleation) and Swedana (perspiration)] and Basti Karma (medicated enema) were planned with oral medications. Details of Ayurvedic medications and Panchakarma are summarized in Table 2, Table 3.
Table 2.
Oral Ayurveda medication used for the case of Limb girdle muscular dystrophy.
| Name of the drug | Anupana | Days of treatment | Dose |
|---|---|---|---|
| Yograj Guggulu | Twice a day with Dashamoola Kwatha | 4/12/18–7/10/2019 | 500 mg |
| Dashamoola Kwatha | Twice a day | 4/12/18–7/10/2019 | 40 ml |
| combination of Ashwagandha and Satavari Churna with Sankha Bhasma | Twice a day with luke warm milk | 4/12/18–7/10/2019 | 2g 2g 500 mg |
| Narsinha Churna | Twice a day with luke warm milk | 4/12/18 to 4/1/19 | 3g |
| Ashwagandhavleha | Twice a day with luke warm milk | 4/12/18–7/10/2019 | 5g |
| Ekangaveera Rasa | Twice a day with honey | 29/03/19–7/10/2019 | 125 mg |
Table 3.
Panchakarma procedures used for the case of Limb girdle muscular dystrophy.
| Panchakarma procedures with method of preparation | Method of application | Days of treatment |
|---|---|---|
| Shalishashtika Pinda Swedana - 250g Shashtika Shali is cooked in 1.5 L of decoction of Bala Moola and milk. Cooked mixture is made into bolus in cotton cloth. Bala Moola decoction and milk mixture is used as reheating medium for bolus | Whole body Massage with Dashamoola oil was done for 10 min followed by whole body massage for 45 min with bolus of Shashtika Shali.Then Abhyanga with Dashmoola taila was repeated for next 10 min. | 16 days (10/12/18–26/12/18) 16 days (2/4/19–17/4/19) |
| Mustadi Yapana Basti - Madhu (honey) 50g, Saindhava Lavana (rock salt) 5g, Panchatikta Ghrita 50 ml, Ashwagandha oil 50 ml, Satapushpa (Anethum sowa Kurz) Kalka 15g, milk processed with Mustadi Yapana Basti Kwatha drugs 300 ml and Mansarasa (soup of goat meat) 50 ml were mixed in standard sequence for Basti preparation to form a homogenous emulsion which was indirectly heated on a water bath. | Given before meal by Basti Yantra Route of administration – anal region |
16 days (10/12/18–26/12/18) (total 16 Bastis were given as Yapana formulation no separate Anuvasana Basti was needed for it), then again for 16 days (2/4/19–17/4/19) |
6. Outcome measures and follow up
Patient was assessed for Pain, walking ability, power and reflexes of both upper and lower limbs, pseudohypertrophy of calf muscles, S.CPK level and EMG at baseline and endline (completion of Panchakarma procedures). Lower back region and bilateral knee joints pain were at grade 5 on visual analogue scale on 4/12/18 it reduced to 3 on 17/4/19 and further reduced to 0 on 13/09/2019. Walking ability on flat surface assessed by 6 min walk test was improved from 10 to 20 m on 04/12/2018, 500 m on 17/04/2019 and 800 m on 13/09/2019. Additionally mild improvement was experienced by patient in waddling gait. Measurements of calf muscles pseudohypertrophy were 54.56 cm of right leg and 52.8 cm of left leg on 04/12/2018 which reduced to 51 cm of right leg and 49 cm of left leg on 17/04/2019 and further reduced to 42 cm in right leg and 41 cm in left leg on 13/09/2019. The power was at grade 4 on medical research council scale on 04/12/2018 which improved to grade 5 on 17/04/2019 and on 13/09/2019 in bilateral shoulder joint, knee joint and in both upper and lower limb. Bilateral Achilles tendon reflex were 2+ on 17/04/2019 and on 13/09/2019. Patient reported that there was no heaviness in the body and she could perform the routine house work with ease. Mild difficulty in climbing up stairs and lifting heavy objects was experienced by patient on 13/09/2019. The S. CPK and EMG were reassessed after the therapy. The value of S. CPK level was reduced from 1450 IU/L on 11/01/2016 to 909 IU/L on 30/05/2019. EMG didn't show any changes after the therapy. Other blood investigations were within normal limits[Supplementary Table 1].
7. Discussion
The main pathology in LGMD is gene mutations causing autosomal, heterogeneous hereditary disorder. In Ayurveda there is concept of Aadibala Pravrita Vyadhi (∼hereditary disorders) caused by Vata Dosha [7, Sutra Sthan chapter 24 verse 6]. Vata plays prime role in the organogenesis, tissue formation and systemic maturation during fetal development [8] and on vitiation through Swaprakopaka Karana (i.e. Beeja Dosha), Dhatukshaya (∼depletion of body tissue) and Margavarana (obstruction in the pathway of Vata) causes Kubja (hunch backed), Pangu (crippled), Muka (dumb) etc. Vatavyadhis. [7, chapter 2 verse 54]. In present case vitiated Vata Dosha must have focused on Mansa in fetal life and developed Mansagata Vata. Ekanga Swayathu (Pseudohypertrophy) in calf muscles was developed due to Prakupita (vitiated) Doshas and mainly Vata Dosha which affected the Twak (skin and subcutaneous tissues), Mansa (muscles), Shonita (blood), etc. and lead to Swayathu. [8, chapter 18 verse 6/1]. At the time of first encounter on 04/12/2018 Sthanika Shleshka Kapha depletion (localized depletion of Kapha Dosha) symptoms and vitiation of Vata Dosha at lumbar and knee region, which probably caused knee joint pain and lower back ache. In present case line of treatment for Dhatukshayaja Vatavyadhi of chronic nature was planned. As the patient was suffering with Mandagni (suboptimum digestive power), oral Ayurveda medicine was given before Panchakarma to digest the Ama (∼undigested food that vitiated the Doshas). The line of treatment of Vatavyadhi comprises of Snehana, Swedana, Mriduvirechana (∼mild purgation) and Basti [6 Verse 75–84]. Likewise Virechana, Niruha Basti (Medicated enema mainly comprises of decoction of medicinal plant for Vatavyadhi etc) and Shamana (palliative) therapies are indicated in the management of Mansagata Vata [6 Verse 93]. For Dhatukshaya, the main treatment includes Snehana, Swedana, Basti along with Ayurvedic oral medications. In chronic Vatavyadhis, Nanatamaj Vata and for Avrita Vata Yapana Basti, Guggulu, Rasayana and Shilajeeta are indicated [6 Verse 240–241]. Thus following the textual line of management, Shalishashtika Pinda Swedana and Mustadi Yapana Basti were planned along with oral medication. Shalishashtika Pinda Swedana has the property of Brunhana because it is a kind of Snigdha Swedana (∼provides nourishment to muscles and bones). Mustadi Yapana Basti is indicated for increasing strength, Jeevana Shakti (∼vigor or quality life) and Vrishya (∼fertility). It is useful in Sopha (∼inflammation or pseudohypertrophy), in Katishoola (low back ache), pain in calf and thigh region and Vatarakta (∼various disease of rheumatic spectrum). It also has Rasayana properties. It can break the pathogenesis of the disease by removing obstruction and purification of channels and depletion of Dhatus by its Brunhana nature. Mustadi Yapana Basti is able to control most muscle, bone and bone marrow diseases [6, Siddhi Sthan chapter 12 verse 15]. The oral medication -Yograj Guggulu is useful in Aamvata (rheumatic disorders), Vatarakta, various Sandhi – Majjagata Vatika disorders (∼neurological, rheumatic and musculoskeletal and bone marrow diseases), it increases Agni (metabolic fire) and Bala (physical strength) [9]. Dashamoola Kwatha have Tridoshaghana properties (alleviate the deranged humors) and treats the depletion of tissues [10]. Ashwagandha [11] and Satavari [11, verse 291] both have Rasayana and Balya (anabolic) properties. Sankha Bhasma correct the Agnimandhya (improves the digestive fire), Balya (anabolic) in nature Amlapitta Nashaka (anti-hyperacidity) and alleviates the deranged Vata Dosha [12]. It is also useful in hyperacidity which may be caused in some patients due to use of Narsinha Churna. Narsinha Churna is useful in low back pain, Kshaya (depletion of body) and all types of Vatika, Pattika and Kaphaja Vikara (∼diseases due to derangements of all humors) [9, Chapter 67 verse 15–24]. It is also effective in Mansakshaya condition [13]. Ekangaveera Rasa is effective in Vataja disorders, Vatakaphaja disorders and Pakshaghata (Hemiplegia) [13, Kharaliya Rasayana Prakarana, p 470]. Repeated uses of Snehana and Swedana and other Vatanashaka (alleviating the Vata Dosha) process may lead to accumulation of Malas (waste metabolites) in Srotasas and hinders the normal process of Vata Dosha [6, verse 85–86]. Here Anulomana (mild purgation) Deepana and Pachana (Drugs having the property to improve the digestion) and Vatakapha Nashaka (Vatakapha Dosha alleviating) drugs such as Ekangaveera Rasa are effective. Ekangaveera Rasa is a compound of Kuchala (Strychnos nux-vomica L.) which is useful in imparting the strength to muscles fibers [13, Kharaliya Rasayana Prakarana, p 408]. Ekangaveera Rasa is also having the property of Brunhana (Having the nourishing property to the tissues) and thus helpful in alleviating the degeneration of muscles. Hence the Ayurvedic line of management fulfills all the necessarily treatments used in the progressive diseases such as anti-inflammatory drugs, physical therapy and synthetic steroids which are often associated with side effects in long term use [14]. As this is a Aadibalapravritta Vyadhi (hereditary disease), this is Yapya (palliative) in nature. It can be managed by repairing the genes. Panchakarma procedures and Rasayana drugs may affect the epigenetic process and thus brings hopes of management in this disease by genetic alteration and expression in positive way [15,16]. It is indicated that basic nutrients and heavy metals can induce epigenetic process [17]. The present case findings are important because they indicate a better and safer treatment strategy with satisfactory outcome for a disease condition that requires lifelong supportive treatment.
8. Conclusion
This case study demonstrated the satisfactory management in LGMD with Panchakarma procedures and Ayurvedic medicinal interventions and provides foundation for future research studies.
9. Patient consent
Written informed consent for publication of this case study had been obtained from the patient.
10. Patient's perspective
Patient was satisfied with the provided treatment.
Source of funding
None.
Conflict of interest
No conflict of interest.
Author contributions
Kshipra Rajoria: Methodology, investigation, resources, writing- original draft, review draft.
Sarvesh Kumar Singh: conceptualization, investigation, resources, writing original draft, review draft, supervision.
Suman Dadhich: writing original draft, investigations.
Footnotes
Peer review under responsibility of Transdisciplinary University, Bangalore.
Supplementary data to this article can be found online at https://doi.org/10.1016/j.jaim.2021.07.002.
Appendix A. Supplementary data
The following are the supplementary data to this article:
Supplementary file 1.

Supplementary file 2.

Supplementary file 3.

Supplementary file 4.

Supplementary file 5.

Supplementary file 6.

Supplementary file 7.

Supplementary file 8.

2
3
4
5
6
References
- 1.Mercuri E., Muntoni F. Muscular dystrophies. Lancet. 2013;381:845–860. doi: 10.1016/S0140-6736(12)61897-2. PMID: 23465426. [DOI] [PubMed] [Google Scholar]
- 2.Mercuri E., Muntoni F. Muscular dystrophy: new challenges and review of the current clinical trials. Curr Opin Pediatr. 2013;25:701–707. doi: 10.1097/MOP.0b013e328365ace5. PMID: 24240289. [DOI] [PubMed] [Google Scholar]
- 3.Murphy A.P., Straub V. The classification, natural history and treatment of the limb girdle muscular dystrophies. J Neuromuscul Dis. 2015;2:S7–S19. doi: 10.3233/JND-150105. PMID: 27858764; PMCID: PMC5271430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Theadom A., Rodrigues M., Roxburgh R., Balalla S., Higgins C., Bhattacharjee R., et al. Prevalence of muscular dystrophies: a systematic literature review. Neuroepidemiology. 2014;43(3–4):259–268. doi: 10.1159/000369343. Epub 2014 Dec 16. PMID: 25532075. [DOI] [PubMed] [Google Scholar]
- 5.Gawlik K.I. At the crossroads of clinical and preclinical research for muscular dystrophy-are we closer to effective treatment for patients? Int J Mol Sci. 2018;19(5):1490. doi: 10.3390/ijms19051490. PMID: 29772730; PMCID: PMC5983724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pandey G., editor. Commentary vidhyotini of charaka samhita of agnivesa - 2nd volume, chikitsa sthan chapter 28 verse 32. Chaukhmbha Sanskrit Sansthan; Varanasi: 2012. p. 782. [Google Scholar]
- 7.Shastri A., editor. Commentary Ayurveda tattva sandipika of SushrutaSamhita of maharsi sushruta- 1st volume sharira sthan chapter 09 verse 12. Chaukhmbha Sanskrit Sansthan; Varanasi: 2012. p. 71. [Google Scholar]
- 8.Pandey G., editor. Commentary vidhyotini of charaka samhita of agnivesa - 1st volume, Sutra sthan chapter 12 verse 8. Chaukhmbha Sanskrit Sansthan; Varanasi: 2012. p. 174. [Google Scholar]
- 9.Diwedy R., editor. Commentary vaidyaprabha of chakaradatta of chakarpanidatta chapter 25 verse 30. Varanasi Chaukhmbha Sanskrit Bhawan; 2018. p. 168. Reprinted. [Google Scholar]
- 10.Mishra B., editor. Commentary vidhyotini of bhav prakash nighantu of bhavamishra, gudichayadivarg chapter 26, verse 41. 10th ed. Chaukhambha Sanskrit Sansthan; Varanasi: 2002. p. 294. [Google Scholar]
- 11.Aujha J., editor. Dhanvantari nighantu, GuduchyadiVarga chapter 1 verse 272. ChaukhmbhaSurbhartiPrakashan; Varanasi: 2004. p. 85. Reprinted. [Google Scholar]
- 12.Mishra S. Chaukhamba Surbharati Prakashan; Varanasi: 2007. Commentary sidhiprada of bhaisajyaratnavali of govindadas sena, chapter 3 verse 275-276; p. 68. [Google Scholar]
- 13.Rastantrasara, Sangrah Siddhayogasara. Churna Prakarana. 17th ed. Vol. 1. Krisna Gopal Ayurveda Bhavana; Ajmer: 2006. pp. 672–674. [Google Scholar]
- 14.Lovering R.M., Porter N.C., Bloch R.J. The muscular dystrophies: from genes to therapies. Phys Ther. 2005;85(12):1372–1388. [PMC free article] [PubMed] [Google Scholar]
- 15.Vishwanatha U., Guruprasad K.P., Gopinath P.M., Acharya R.V., Prasanna B.V., Nayak J., et al. Effect of Amalakirasayana on DNA damage and repair in randomized aged human individuals. J Ethnopharmacol. 2016;191:387–397. doi: 10.1016/j.jep.2016.06.062. PMID: 27364038. [DOI] [PubMed] [Google Scholar]
- 16.a Sharma H. Ayurveda: science of life, genetics, and epigenetics. Ayu. 2016;37(2):87–91. doi: 10.4103/ayu.AYU_220_16. [DOI] [PMC free article] [PubMed] [Google Scholar]; b Sharma H. Ayurveda: science of life, genetics, and epigenetics. Ayu. 2016 Apr-Jun;37(2):87–91. doi: 10.4103/ayu.AYU_220_16. PMID: 29200745; PMCID: PMC5688840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Weinhold B. Epigenetics: the science of change. Environ Health Perspect. 2006;114(3):A160–A167. doi: 10.1289/ehp.114-a160. PMID: 16507447; PMCID: PMC1392256. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
2
3
4
5
6