

Sir,
A summit organized by the UN on noncommunicable diseases prevention called for interventions to decrease the salts, sugars, and fats in foods.[1] The inappropriate introduction of sugary foods increases a child's risk of later obesity and dental caries.[2] Due to a busy lifestyle in urban areas, parents choose packed baby foods for their growing children. Knowledge of baby foods sold in the market is an important step toward public health. However, the Indian market is lacking knowledge.
A study was undertaken to assess the sugar and salt content of baby foods sold in the Indian market and to identify foods with high content. 114 different complementary baby foods and infant formulas which included dry baby foods, prepared baby foods, and others including snacks, instant foods, dessert, pureed fruits, beverages, and perishables for infants aged 0–24 months were studied. Researchers recorded the nutrition facts label for each product and checked the sodium and sugar levels by content analysis. Complementary foods for preschoolers and pureed vegetables and fruits were excluded as these are categorized as pure foods with no added sugar and contain naturally occurring sugars, so therefore by excluding these products from the study enabled us to target essentially on added sugars even though some products may have naturally occurring sugars.
The nutrition facts label was checked and the amount of sugar and salt was identified by assessing the concentration per 100 g, per serving, and in relation to the calories. Researchers checked the nutrition facts label for the following: Type of sugar (e.g., fructose/sucrose/glucose/lactose and maltose), Package size (g)/(ml), Serving size of sugar per 100 (g), Sugar per serving (g), Energy per 100 ml/g (kcal), Energy per serving (kcal), Salt per serving (mg), Salt per 100 g (mg), Added sugar (any type of sugar listed as one of the ingredients), Added salt (salt listed as one of the ingredients).
The sodium levels of products per serving were assessed considering the reference intake of the “US Institute of medicine and dietary reference,” while the sugar levels of the products per serving were estimated according to the “recommendations by the American Heart Association.” The products showing sodium less than <130 mg per serving were classified as acceptable, whereas the products showing sodium more than >260 mg per serving were classified as high in sodium. The Institute of Medicine has set a feeding guideline, also known as the adequate daily intake level (AI), which is 370 mg for babies and 1000 mg for toddlers.[3] According to the American Heart Association Recommendations, the foods which derive over 20% of their calories from sugar are categorized under poor nutritional quality.[4] The results of this study are presented in the form of quantitative data using summary statistics and bar charts.
In our study, the mean sodium content of the 114 infant formulas and complementary baby foods was low in general. Nearly all infant and complementary foods contained <130 mg/serving sodium, classifying it under “acceptable.” Only two products reported >260 mg/serving sodium. Hence, according to the Institute of Medicine's dietary reference, it will be considered as “high.”[3] According to the American Heart Association Recommendations and other published literature, if the food products derived over 20% of their calories from sugar, they were categorized as of poor nutritional quality.[4] This study showed that a total of 32 products out of 114 infant formulas and complementary baby foods derived number <20% of their calories from sugars per serving. Almost 28% of the products assessed had a “high sugar profile.” Examples included dry baby foods/prepared baby foods including cereal, beverages, pureed desserts, pureed fruits, and snacks. Approximately 51% of the baby food products listed sugar or its analog such as natural, sucrose, lactose, and nucleotides in the first four ingredients on the label. Majority of the assessed foods did not list added sugars, while on the other hand, toddler's foods, drinks; snacks contained added sugars in the ingredient list (four toddler cereals and one infant milk have added sugar specified). Comparing the commercially available foods that were meant only for infants, and baby foods that were meant for toddlers and infants, the toddler foods showed >1 source of added sugars. As shown in Figure 1, about 41% of the baby food brands sold in the Indian marketplace contained high sugar in various dry baby foods, beverages, and snacks including cereal bars and snack bars.
Figure 1.
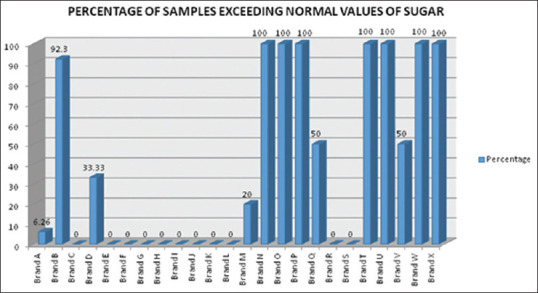
Summary of the sugar profile among various brands
Food choice is a complex process that involves many different factors, particularly in case of babies and toddlers can affect taste preferences that are in the developmental stage of early life. This flavor consequence learning includes sweet and salted taste which can lead to long-term health effects. Further, the higher sodium intake has been related to higher systolic pressure, especially the children who are overweight. In recent times, sugar intake and childhood obesity are interlinked, highlighting that this generation is engaged to a considerable amount of sweetened foodscape. This environment may impede the growth and development of young children resulting in various noncommunicable diseases in later life.
Parents are influential primary role models for healthy eating and reducing the child's risk of developing caries. Complementary feeding is a major aspect in the shift from breastfeeding to home-cooked foods, making it a very critical period for growth and development of a child. Therefore, complementary foods must meet the nutritional requirements to avoid any nutritional deficiencies which may have negative effects on health of the child. Excessive quantity of SSB's consumed by toddlers was related to obesity and rampant caries in later life.[3] Over the last several decades, with busy lifestyles in urban areas, families have substantially increased the purchases of less nutritious take-out readymade foods. Despite being aware of the constituents of a healthy diet, parents routinely purchase and feed their children with such unhealthy foods.[5] Infant and toddler foods contain decent amounts of sodium, emphasizing the need for standardized regulation of sodium levels in baby food products. Considering the findings of our study, in relation to sugar and salt consumption, we must call for public health group efforts, which will make it easier for parents to choose healthier food options for their children. While choosing the commercially available foods for their infants and toddlers, parents should inspect: (i) the amount of added sugars in the infant formulas, cereals, snack bars, teething biscuits, pancakes, pureed baby foods, etc., and (ii) the sodium levels in commercially available food products, especially for toddlers.
Reducing the child's risk to developing caries and childhood obesity are important components to address the public health problems. There is a need for a broad and combined approach that will look into individual behaviors and environmental factors. Pediatricians can play a significant role in counseling the parents regarding the selection of suitable healthy foods to feed their young children, hence preventing an overall unhealthy oral cavity, dental caries, hypertension, childhood obesity, and other noncommunicable diseases.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Assembly UG. Political Declaration of the High-Level Meeting of The General Assembly on the Prevention and Control of Non-Communicable Diseases. New York: General Assembly. United Nations. New York; 2011. [Last accessed on 2021 Apr 28]. Available from: https://www.un.org/en/ga/ncdmeeting2011/ [Google Scholar]
- 2.Murray RD. Savoring Sweet: Sugars in Infant and Toddler Feeding. Ann Nutr Metab. 2017;70(Suppl 3):38–46. doi: 10.1159/000479246. [DOI] [PubMed] [Google Scholar]
- 3.Elliott CD, Conlon MJ. Packaged baby and toddler foods: Questions of sugar and sodium. Pediatr Obes. 2015;10:149–55. doi: 10.1111/j.2047-6310.2014.223.x. [DOI] [PubMed] [Google Scholar]
- 4.Elliott C. Assessing 'fun foods': Nutritional content and analysis of supermarket foods targeted at children. Obes Rev. 2008;9:368–77. doi: 10.1111/j.1467-789X.2007.00418.x. [DOI] [PubMed] [Google Scholar]
- 5.Anjum MS, Reddy PP, Monica M, Rao KY, Abbas I, Poornima K. Association of maternal food choices with caries status and sugar consumption among preschool children in Vikarabad town. J Indian Assoc Public Health Dent. 2015;13:285–91. [Google Scholar]