

Abstract
Background
Acupuncture has been used by rehabilitation specialists as an adjunct therapy for the symptomatic treatment of rheumatoid arthritis (RA). Acupuncture is a traditional Chinese medicine where thin needles are inserted in specific documented points believed to represent concentration of body energies. In some cases a small electrical impulse is added to the needles. Once the needles are inserted in some of the appropriate points, endorphins, morphine‐like substances, have been shown to be released in the patient's system, thus inducing local or generalised analgesia (pain relief). This review is an update of the original review published in July 2002.
Objectives
To evaluate the effects of acupuncture or electroacupuncture on the objective and subjective measures of disease activity in patients with RA.
Search methods
A comprehensive search of MEDLINE, EMBASE, PEDro, Current Contents , Sports Discus and CINAHL, initially done in September 2001, was updated in May 2005.The Cochrane Field of Rehabilitation and Related Therapies and the Cochrane Musculoskeletal Review Group were also contacted for a search of their specialized registries. Handsearching was conducted on all retrieved papers and content experts were contacted to identify additional studies.
Selection criteria
Comparative controlled studies, such as randomized controlled trials and controlled clinical trials in patients with RA were eligible. Trials published in languages other than French and English were not analyzed. Abstracts were excluded unless further data could be obtained from the authors.
Data collection and analysis
Two independent reviewers identified potential articles from the literature search and extracted data using pre‐defined extraction forms. Consensus was reached on all the extracted data. Quality was assessed by two reviewers using a five point validated tool that measured the quality of randomization, double‐blinding and description of withdrawals.
Main results
After the updated searches were conducted, five further potential articles were identified; however, these did not meet the inclusion criteria. Two studies involving a total of 84 people were included. One study used acupuncture while the other used electroacupuncture. In the acupuncture study, no statistically significant difference was found between groups for erythrocyte sedimentation rate (ESR), C‐reactive protein (CRP), visual analogue scale for patient's global assessment (VAS G), number of swollen joints and tender joints, general health questionnaire (GHQ), modified disease activity scale (DAS) or for the decrease in analgesic intake. Although not statistically significant, pain in the treatment group improved by 4 points on a 0‐100mm visual analogue scale versus no improvement in the placebo group. In the second study, using electroacupuncture, a significant decrease in knee pain was reported in the experimental group, 24 hours post treatment, when compared to the placebo group (WMD: ‐2.0 with 95% CI ‐3.6,‐4.0). A significant decrease was found also at four months post‐treatment (WMD ‐0.2, 95% CI: ‐0.36, ‐0.04)
Authors' conclusions
Although the results of the study on electroacupuncture show that electroacupuncture may be beneficial to reduce symptomatic knee pain in patients with RA 24 hours and 4 months post treatment, the reviewers concluded that the poor quality of the trial, including the small sample size preclude its recommendation. The reviewers further conclude that acupuncture has no effect on ESR, CRP, pain, patient's global assessment, number of swollen joints, number of tender joints, general health, disease activity and reduction of analgesics. These conclusions are limited by methodological considerations such as the type of acupuncture (acupuncture vs electroacupuncture), the site of intervention, the low number of clinical trials and the small sample size of the included studies.
Plain language summary
Acupunture and electroacupuncture for rheumatoid arthritis
Does acupuncture work for treating rheumatoid arthritis?
Two studies of low to medium quality were reviewed and provide the best evidence we have today. The studies tested 84 people who had rheumatoid arthritis. The studies compared acupuncture to a placebo (fake therapy) or a steroid injection. Improvement was measured after one treatment or after five treatments given once per week.
What causes shoulder pain and how can acupuncture help? Rheumatoid arthritis (RA) is a disease in which the body's immune system attacks its own healthy tissues. The attack happens mostly in the joints of the hands and feet and causes redness, pain, swelling and heat around the joints. Drug and non‐drug treatments are used to relieve pain and/or swelling.
Acupuncture is a non‐drug therapy being in which thin needles are inserted into the body at specific spots. It is thought that acupuncture works either by releasing chemical compounds in the body that relieve pain, by overriding pain signals in the nerves or by allowing energy (Qi) or blood to flow freely through the body. It is not known whether acupuncture works or is safe.
What do the studies show? In one study, people had acupuncture or fake therapy for five weeks, once per week. Pain, number of swollen and tender joints, disease activity, overall well‐being, lab results, or amount of pain medication needed was about the same whether they had acupuncture or fake therapy.
In the other study, people had acupuncture with an electric current going through the needles at specific or real acupuncture spots in the knee or at fake spots in the knee. Knee pain while at rest, while moving or while standing decreased more in the people who had the real acupuncture. The improvement lasted up to 4 months after acupuncture. Unfortunately, the authors of this review believe that this trial was of low quality and may overestimate how well acupuncture works.
How safe is it? Side effects were not measured in the studies.
What is the bottom line? The quality of the evidence is 'silver'.
From the little evidence that there is, acupuncture does not appear to improve the symptoms of rheumatoid arthritis.
Background
Acupuncture is a technique based on Chinese medical practice whereby needles are inserted into specific exterior body locations to relieve pain and for other therapeutic purposes (Dorland 1988). It affects electroatropines mainly mediated by endorphins or serotonin, morphine‐like compounds (Dumoulin 1978). The impact of acupuncture can be enhanced by electrical current, termed electroacupuncture (Wong 1987). These substances cause analgesia by decreasing pain and modulating stress. They also support homeostasis by releasing regulators responsible for other hormones (Wong 1987).
Based on these physiological effects, acupuncture could have potential benefits for the symptomatic treatment of RA. There is however, very little evidence to support the use or non use of acupuncture for symptomatic treatment of RA patients. Patient management recommendations have not supported the use of acupuncture due to the lack of scientific evidence to date (Walker 1996). In fact, to our knowledge, there are no existing evidence‐based clinical practice guidelines in the scientific literature.
This review is an update of the original review published in July 2002.
Objectives
To evaluate the effectiveness of acupuncture or electroacupuncture therapy for the relief of signs and symptoms of patients with RA, compared to placebo and other treatment interventions.
Methods
Criteria for considering studies for this review
Types of studies
According to an a priori protocol, all comparative controlled trials, including randomized controlled trials (RCT) and controlled clinical trials without randomization (CCT), were included. Trials which used same patients as their own control were not accepted. The results were graded according to the strength of the study design.
Trials published in languages other than French and English were not analyzed because of the time and cost involved in translation. Abstracts were excluded unless further data could be obtained from the authors.
Types of participants
Adult patients with classic or definite rheumatoid arthritis treated with acupuncture or electroacupuncture. Any joint except the spine was considered.
Types of interventions
Acceptable interventions included acupuncture applications using any combination of parameters. For example, use of electric current, stimulation of various points or types of needles employed were not discriminated with regards to the inclusion criteria.
Types of outcome measures
The primary outcome measure was pain. All secondary outcome measures were from the potential core set identified by the OMERACT conference on rheumatoid arthritis outcomes (OMERACT 1993), including: Number of tender joints per patient Number of swollen joints per patient Physician global assessment Patient global assessment Functional status.
Range of motion (ROM), strength, physiological outcomes such as skin and joint temperature were not included in the analysis.
Search methods for identification of studies
The initial literature search was conducted up to September 2001 and updated recently to include articles published up to May 2005. The search was done according to the sensitive search strategy for RCTs designed for the Cochrane Collaboration (Dickersin 1994), with modifications proposed by Haynes et al. (Haynes 1994). Additional terms for the study design were used to identify observational studies including: case‐control, cohort, comparative study, clinical trial. MEDLINE, EMBASE, HealthSTAR, Sports Discus, CINAHL, the Cochrane Field of Rehabilitation and Related Therapies and the Cochrane Musculoskeletal Review Group were searched using a keyword and textword search strategy (shown in Appendix 1). In addition, the reference lists of included trials were searched and content experts were contacted for additional studies.
Data collection and analysis
Two independent reviewers (VR, LB) examined the titles and abstracts of the trials identified by the search strategy to select trials that met the inclusion criteria. All trials classified as relevant by at least one of the reviewers were retrieved. The retrieved articles were re‐examined to ensure they met the inclusion criteria and were assessed for quality. The results of the individual trials were extracted from each of the included trials using pre‐determined extraction forms by two independent reviewers (LB, VR). The data was cross‐checked by a third reviewer (LC). The extraction forms were developed and pilot‐tested, based on other forms used by the Cochrane Musculoskeletal Review Group. The extraction form documented specific information about acupuncture therapy. The final data values were based on consensus of the two reviewers. Most outcomes were continuous in nature and the results are presented as weighted mean differences (WMD). Relative risks would have been calculated for dichotomous outcomes.
To rank the strength of scientific evidence we used the grading system adopted by the Cochrane Musculoskeletal Group (Tugwell 2004). This grading system is based on four levels: Platinum, Gold, Silver and Bronze.
Platinum: A published systematic review that has at least two individual controlled trials each satisfying the following : ·Sample sizes of at least 50 per group ‐ if these do not find a statistically significant difference, they are adequately powered for a 20% relative difference in the relevant outcome. ·Blinding of patients and assessors for outcomes. ·Handling of withdrawals >80% follow up (imputations based on methods such as Last Observation Carried Forward (LOCF) are acceptable). ·Concealment of treatment allocation.
Gold: At least one randomised clinical trial meeting all of the following criteria for the major outcome(s) as reported: ·Sample sizes of at least 50 per group ‐ if these do not find a statistically significant difference, they are adequately powered for a 20% relative difference in the relevant outcome. ·Blinding of patients and assessors for outcomes. ·Handling of withdrawals > 80% follow up (imputations based on methods such as LOCF are acceptable). ·Concealment of treatment allocation.
Silver: A systematic review or randomised trial that does not meet the above criteria. Silver ranking would also include evidence from at least one study of non‐randomised cohorts that did and did not receive the therapy, or evidence from at least one high quality case‐control study. A randomised trial with a 'head‐to‐head' comparison of agents would be considered silver level ranking unless a reference were provided to a comparison of one of the agents to placebo showing at least a 20% relative difference.
Bronze: The bronze ranking is given to evidence if at least one high quality case series without controls (including simple before/after studies in which patients act as their own control) or if the conclusion is derived from expert opinion based on clinical experience without reference to any of the foregoing (for example, argument from physiology, bench research or first principles).
Results
Description of studies
The initial literature search and hand‐searching identified eight potential articles. Of these, two RCT studies were included involving 84 RA patients (David 1999, Man 1974). The updated search in May of 2005 further identified five potential articles; however, these did not meet the inclusion criteria.
The reasons for the exclusion of the eleven trials from both the initial and updated search are as follows: 1) Tukmashi 2000: Not a clinical trial; 2) Depei 1992: No numerical data; 3) Devyani 1985: Literature review; 4) Camerlain 1981: Data not analysable; 5) Camerlain 1976: Population mixed (not confined to RA patients); 6) Shen 1973: Incomplete data with patients used as their own control; 7) Usichenko 2003: Less than 5 patients in the control group; 8)XI YJ 1986: No control group; 9) Sun 1992: No control group; 10) LI C 1999: No control group; 11) XI D 1992: animals used as comparison group.
In the first included study (David 1999), a cross‐over design was used. Sixty‐four patients between the ages of 46 and 66 were randomly assigned to an experimental or placebo group. Eight participants withdrew prior to the start of the study. In the experimental group, the treatment consisted of inserting one needle (0.25 x 30 mm) in the liver 3 (Li3) point found on each foot, for a total of two needles. The length of application was four minutes. The needles however, were manipulated for five seconds, two minutes after being inserted. In the placebo group, the guides for needle insertion were placed without pressure, on the surface of the skin at the Li3 points, but the needles were not inserted. In both groups the patients were treated supine with a screen blocking their vision from the waist down. The intervention took place for a total of five sessions at one week intervals. Once the five sessions were completed, a wash‐out period of six weeks was prescribed before the patients were crossed‐over into the other group (experimental or placebo) for an additional five weeks of intervention. The outcome measures were assessed for all patients prior to the start of the first five weeks, post‐intervention #1, prior to the start of the 2nd five weeks, post‐intervention #2 and upon follow‐up at six weeks post treatment.
In the second included study (Man 1974), a parallel design was used. Twenty patients of undetermined age with knee pain were randomly assigned to an experimental or a placebo group. In the experimental group, electroacupuncture at 6.26 5mA was applied once for 15 minutes using three 1.5 cm long needles. The needles were inserted in one of the knees at the GB 34, SP 9 and S43 acupuncture points. The other knee was injected with 50 mg of hydrocortisone, hence the parallel design. In the placebo group, electroacupuncture was applied to three incorrect points around the knee using the same instrumentation as the experimental group. The other knee was also injected with 50 mg of hydrocortisone. The outcome measure was a pain reduction scale ranging from 0 to 4 where grade zero indicated no reduction in pain, grade one indicated a marked decrease in pain, grade two indicated a moderate decrease in pain, grade three indicated a minimal decrease in pain and grade four indicated no decrease in pain. Pain was assessed on the basis of the degree of discomfort reported by the patient at rest, during knee flexion/extension and during weight bearing as well as walking activities. The outcome measure was assessed 24 hours after treatment, weekly for four weeks and monthly for three months.
Risk of bias in included studies
Methodological quality was assessed using a validated assessment tool (Jadad 1996). The components of quality focus on randomization, double‐blinding and description of withdrawals. Two independent reviewers (LB, VR) assessed quality and differences were resolved by consensus (LC). Quality was used in subgroup analyses to test the hypothesis that poorly conducted trials demonstrate greater efficacy of the intervention under evaluation. Each item (i.e. randomization, blinding and withdrawals) was examined separately for its effect.
To rank the strength of scientific evidence we used the grading system adopted by the Cochrane Musculoskeletal Group . This grading system is based on four levels: Platinum, Gold, Silver and Bronze. The ranking is given according to different criteria, including sample size, blinding, handling of withdrawals and concealment allocation. For all the outcomes included in this review, a silver level of evidence has been given, mostly because of the small samples size.
The median methodological quality of the two RCTs was 3 (David 1999 score was 4, Man 1974 score was 2). Both the David 1999 and Man 1974 studies were double‐blind.
Effects of interventions
The results of this systematic review of acupuncture or electroacupuncture for the symptomatic treatment of RA are as follows. Each following recommendation as been graded as silver level of evidence. From the two trials included in this study (David 1999; Man 1974), only one showed positive results for the use of acupuncture on symptomatic RA knees (Man 1974).
The first study (David 1999) compared two groups: a) experimental and b) placebo. The experimental group was treated with acupuncture at a specific documented point believed to affect overall health and the placebo control group received sham treatment to the exact same point.
David 1999 found no significant difference was found between the experimental and placebo groups for any of the study outcomes: erythrocyte sedimentation rate (ESR), values of C‐reactive protein (CRP), score on the visual analogue scale for pain (VAS P), score on the visual analogue scale for patient's global assessment (VAS G), number of swollen joints, number of tender joints, score on the general health questionnaire (GHQ), score on the modified disease activity scale (DAS) and decrease in analgesic intake. Pain score on the visual analogue scale (VASP) in the treatment group improved by 4 points on the 0‐100 mm scale versus no improvement in the control group, resulting in a relative improvement of 8%, but it was not statistically significant (WMD ‐7.00, 95%CI, ‐14.40, 0.40). The number of swollen joints (SJC) did not change in either group after treatment (end of study treatment group mean SJC=2.0, control group mean = 3.0, WMD ‐1.00, 95%CI: ‐3.11 to 1.11). The number of tender joints (TJC) in the treatment group improved by 0.5 compared to an improvement of 1 in the control group (WMD ‐1.50,95%CI: ‐5.70 to 2.70). The score on the general health questionnaire (GHQ) improved by 1 in the treatment group compared to no improvement in the placebo group (WMD 3.00, 95%CI: ‐0.25,6.25). The modified disease activity scale (DAS) score improved by 0.2 in the treatment group compared to 0.4 in the placebo group (WMD ‐0.10, 95%CI: ‐1.30 to 1.10) and neither group had a decrease in their analgesic intake after treatment.
In the second study (Man 1974), electroacupuncture to three specifically documented points around the knee was compared to a placebo group receiving electroacupuncture to three incorrect points around the knee. A significant decrease in knee pain was reported in the experimental group, 24 hours post treatment (WMD ‐2.00, 95%CI: ‐3.60 to ‐0.40), with a relative improvement of 66.6% when compared to the placebo group. A significant difference was found also at four months (WMD ‐0.2, 95% CI: ‐0.36, ‐0.04) with a relative improvement of 5.1% in favour of the treatment group. Due to the lack of baseline data, absolute improvements could not be calculated.
Discussion
In the study by Man 1974 the methodology used was clearly described. Nonetheless, this is a small study and the acupuncture technique was questionable. It is unclear why only one point was treated bilaterally and why Li3 was selected. Although the authors attempted to explain their choice, these decisions are not generally accepted (Tukmachi 2000). Similarly, the treatment time and the frequency chosen can also be questioned. The authors did however, strengthen their results by choosing four of the OMERACT 1993 primary outcome measures; number of swollen joints, number of tender joints, patient global assessment and functional status.
In the Man 1974 study, a significant decrease in knee pain was reported with electroacupuncture at 24 hours, and four months post treatment, when comparing the experimental to the placebo group. One can conclude that the effects of the electroacupuncture in the Man 1974 study were only short term. The research methodology was not as clearly outlined in this trial. The age of the participants was not included. The purpose of the hydrocortisone injection was not clearly described and may in fact have impacted on the results. The outcome measure used is not currently recognised and did not provide strong objective data. Furthermore, no means or standard deviations were reported and for the purpose of this review, they were calculated from the graphical representation of the data. The quality of the data was therefore strongly impacted by poor reporting and a weak outcome measure.
Generally, methodological considerations that may have impacted on the results of the included studies are the randomization method, quality of double‐blinding, sample size, study duration and selection of outcome measures. Clearly, the treatment application protocol differed between studies, one used acupuncture while the other used electroacupuncture. This fundamental difference exemplifies the lack of standardization in application methods and contributes to the difficulty of pooling data. Also, in this review, only two RCTs that met the inclusion criteria, were retrieved from the literature. Furthermore, the low quality observed in the Man 1974 study may have caused an overestimation of effect. In particular, patients were subjectively questioned on improvement and this constituted the only outcome measure. Standardized outcomes measures (OMERACT 1993) and measurement periods should be used to facilitate the pooling of data of several studies. Reporting data should also be standardized among the included RCTs. Mean and standard deviation of every outcome should be provided systematically.
From a practical point of view, acupuncture cannot usually be applied at home by patients and requires the consultation of a trained health care professional. Since, one of the major components of RA management is the education of self‐care and empowerment (Lineker 1999), acupuncture does not fit very well into the treatment approach. Nonetheless, there are several potentially beneficial physiological and clinical effects of acupuncture therapy for RA patients that are worth exploring.
Authors' conclusions
Implications for practice.
Although the results of the Man study (Man 1974) show that electroacupuncture may be beneficial to reduce symptomatic knee pain in patients with RA , the authors of this systematic review note that there is insufficient evidence to support this conclusion. The poor quality of the trial, including the small sample size preclude its recommendation. Acupuncture has not yet been shown in the literature to have an effect on ESR, CRP, pain, patient's global assessment, number of swollen joints, number of tender joints, general health, disease activity and reduction of analgesics. These conclusions are limited by methodological considerations such as the site of intervention, the low number of clinical trials and the small sample size of the included studies.
Finally, with a silver level of evidence, we conclude that there is little evidence that acupuncture relieves RA symptoms.
Implications for research.
This review has not clearly proven efficacy of acupuncture or electroacupuncture in the symptomatic treatment of RA. The conclusions are limited by the methodological considerations such as poor quality of the trials, the high methodological variability, the low number of clinical trials and the small sample size of the included studies. No harmful side effects were reported. More sensitive and valid clinical outcomes should be used in studies on the use of acupuncture to reflect the physiological effects found in the scientific literature. More focus should be made on the optimal characteristics of the therapeutic application of acupuncture on different human RA joints. If sufficient studies were ever available on this subject it is recommended that acupuncture and electroacupuncture be reviewed separately.
Feedback
Comments
Summary
Comment Acupuncture and electroacupuncture for the treatment of RA (Cochrane Review) Cite this comment as http://www.update‐software.com/ccng/ccng.exe?SourceID=CD003788#Content897 Sender Dr. A.P. Burford‐Mason Ph.D Sender Description Director of Scientific Affairs for the Acupuncture Foundation of Canada Sender Emailaburford‐mason@sympatico.ca Sender Address 80 Carlton Street, Toronto, ON. M5B 1L5 Date Received 13/09/02 22:28:29
Unlike drug trials, systematic reviews of Complementary and Alternative medicine (CAM) therapies like acupuncture need two components to be evaluated: 1) The clinical trial design AND 2) the clinical methodology employed. This requires that the reveiwers are sufficiently familair with the real world of acupuncture to be able to critically evaluate whether or not the acupuncture used in the various studies was also appropriate. Just as no one would take seriously a drug trial of baby aspirin for the treatment of cancer pain, when most oncologists would use morphine, well qualified acupuncture practitioners would never use such a simple protocol as that used by David et al (1999) to treat pain in RA. Both studies that met the inclusion criteria for this review used an approach to acupuncture which would be unacceptable to appropriately qualified acupuncture practitioners. Future systematic reviews of acupuncture as well as other CAM therapies such ensure that the review panel included members who were able to evaluate the clincal side of the studies as well as the trial design.
I certify that I have no affiliations with or involvement in any organisation or entity with a direct financial interest in the subject matter of my criticisms.Until This high‐lights a problems with systematic reviews of
Reply
You're comments are very interesting and I do share with you a certain level of discomfort with the David article. This topic was dicussed in great length with an expert panel. Since, we were not able, as a group to uncover published standards for acupuncture protocols, nor did we find consensus in the literature retrieved, we had no grounds to exclude the paper. It is interesting to note that not one included or excluded paper, had an identical procedure. This I believe, reflects the lack of evidence and concensus among professionals who use acupuncture and electroacupuncture. How could we then, judge the procedure used? I feel our personal discomfort with the results of the David study lies with our personal experience and beliefs, not with scientific evidence. The article was methodologically sound and who knows, the technique used could have proven beneficial. Although your analogy does conjure up a powerful image, the situation with acupuncture is not the same. We at least have some level of evidence on the clinical indications for baby aspirine, something that does not exist yet in the world of acupuncture. If anything, I believe this Cochrane review highlights the need for standardised procedures. Perhaps future investigators could inspire themselves for the David methodology to test other acupuncture test point combinations.
Contributors
Lynn Casimiro Pht, MA
What's new
| Date | Event | Description |
|---|---|---|
| 19 September 2008 | Amended | Converted to new review format. CMSG ID: C002‐R |
History
Review first published: Issue 3, 2002
| Date | Event | Description |
|---|---|---|
| 22 August 2005 | New citation required and conclusions have changed | Substantive amendment |
Acknowledgements
The authors wish to thank Jessie McGowan, Catherine Lamothe, Shannon Rees, Lucie Lavigne and Nathalie Jean for their indispensable contributions. The authors also wish to thank Maria Judd, CMSG coordinator for her help with final drafts.
Appendices
Appendix 1. Full search strategy
1 exp osteoarthritis/ 2 osteoarthritis.tw. 3 osteoarthrosis.tw. 4 degenerative arthritis.tw. 5 exp arthritis, rheumatoid/ 6 rheumatoid arthritis.tw. 7 rheumatism.tw. 8 arthritis, juvenile rheumatoid/ 9 caplan's syndrome.tw. 10 felty's syndrome.tw. 11 rheumatoid.tw. 12 ankylosing spondylitis.tw. 13 arthrosis.tw. 14 sjogren$.tw. 15 or/1‐14 16 exp acupuncture 17 acupuncture or electroacupuncture.tw. 18 or/16‐17 19 15 and 18 20 clinical trial.pt. 21 randomized controlled trial.pt. 22 tu.fs. 23 dt.fs. 24 random$.tw. 25 placebo$.tw. 26 ((sing$ or doubl$ or tripl$) adj (masked or blind$)).tw 27 sham.tw. 28 or/20‐27 29 18 and 28
Data and analyses
Comparison 1. Electroacupuncture vs Placebo (end of treatment ‐24hrs).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 *Pain (0‐4 scale, 0‐no pain) | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐2.0 [‐3.60, ‐0.40] |
1.1. Analysis.
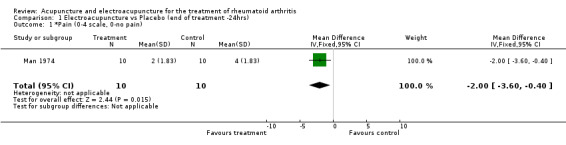
Comparison 1 Electroacupuncture vs Placebo (end of treatment ‐24hrs), Outcome 1 *Pain (0‐4 scale, 0‐no pain).
Comparison 2. Acupuncture vs Placebo, (end of treatment‐ 5 weeks).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain (VAS 0‐100mm) | 1 | 55 | Mean Difference (IV, Fixed, 95% CI) | ‐7.0 [‐14.40, 0.40] |
| 2 Swollen joints count | 1 | 55 | Mean Difference (IV, Fixed, 95% CI) | ‐1.0 [‐3.11, 1.11] |
| 3 Tender joints count | 1 | 55 | Mean Difference (IV, Fixed, 95% CI) | ‐1.5 [‐5.70, 2.70] |
| 4 Disease Activity (Scale 1‐10) | 1 | 55 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐1.30, 1.10] |
| 5 Global Health Questionnaire (Scale 1‐10) | 1 | 55 | Mean Difference (IV, Fixed, 95% CI) | 3.00 [‐0.25, 6.25] |
2.1. Analysis.
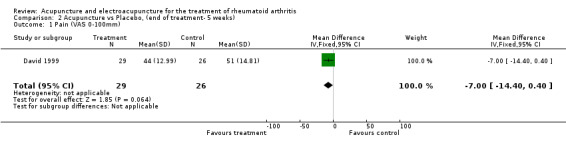
Comparison 2 Acupuncture vs Placebo, (end of treatment‐ 5 weeks), Outcome 1 Pain (VAS 0‐100mm).
2.2. Analysis.
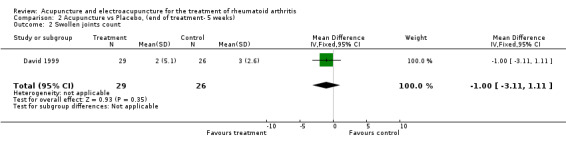
Comparison 2 Acupuncture vs Placebo, (end of treatment‐ 5 weeks), Outcome 2 Swollen joints count.
2.3. Analysis.
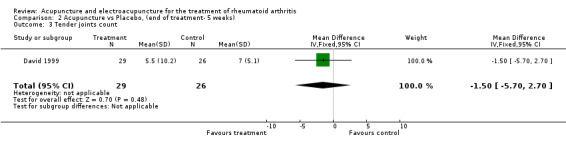
Comparison 2 Acupuncture vs Placebo, (end of treatment‐ 5 weeks), Outcome 3 Tender joints count.
2.4. Analysis.
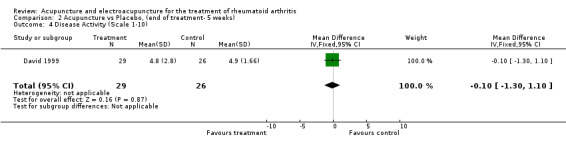
Comparison 2 Acupuncture vs Placebo, (end of treatment‐ 5 weeks), Outcome 4 Disease Activity (Scale 1‐10).
2.5. Analysis.
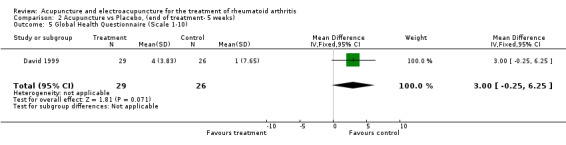
Comparison 2 Acupuncture vs Placebo, (end of treatment‐ 5 weeks), Outcome 5 Global Health Questionnaire (Scale 1‐10).
Comparison 3. Electroacupuncture vs Placebo (follow‐up 4 months).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 *Pain (0‐4 scale, 0‐no pain) | 1 | 20 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐0.36, ‐0.04] |
3.1. Analysis.
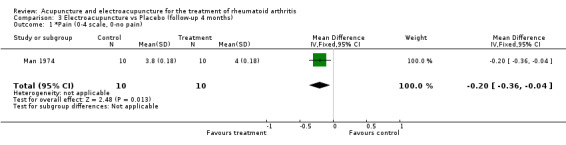
Comparison 3 Electroacupuncture vs Placebo (follow‐up 4 months), Outcome 1 *Pain (0‐4 scale, 0‐no pain).
Characteristics of studies
Characteristics of included studies [ordered by study ID]
David 1999.
| Methods | Randomized, cross‐over design. Sample size: 64(8 withdrawals) Group 1:29 acupuncture Group 2: 27 placebo Treatment duration: 5 weeks 6 weeks break cross‐overs in other groups for 5 weeks, follow up after 6 weeks post‐treatment | |
| Participants | Inclusion:definite or classic R.A., 18 to 75 years old. Mean age for group 1: 61 Group 2: 57 Disease duration group 1: 8 Disease duration group 2: 12 | |
| Interventions | Group 1: 5 treatments of acupuncture 4min. at weekly intervals
Group 2: 5 placebo only guide for needle is placed for 4 min Size of needles : 0.25 x 30mm Total number of sites: 2 (Li3), Duration of treatment: 4 min., Total number of treatment sessions: 5 |
|
| Outcomes | CRP, ESR, VAS pain, VAS global assessment, Swollen joint, Tender joint, GHQ, modified DAS, Analgesics | |
| Notes | R=2 B=1 W=1 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
Man 1974.
| Methods | Randomized, Parallel design, Sample size: 20, Electro‐ acupuncture duration: 15 min., Follow‐up: 1x 24 hours, 4x weekly and 3x monthly Experimental group: 10, Control group: 10 | |
| Participants | Inclusion: definite and classic R.A. present for 5 years or longer, Pain in both knees, Disease duration: 5 years or more. Group 1: 3 males and 7 females, Group 2: 3 males and 7 females. | |
| Interventions | Group 1: one knee treated with electroacupuncture and steroid injection in the other knee(50 mg), Group 2: One knee treated incorrectly and steroid injection in the other knee (50 mg). Electroacupuncture sites for experimental group: GB 34, SP 9, S 43, Electroacupuncture sites for control group: 3 points with no known effects. Size of needles: 1,5 cm long, Total number of needles: 3 + connected to electro‐stimulator 6.26 at 5mA. Duration of treatment : 15 min., Total number of treatment sessions: 1 | |
| Outcomes | Pain reduction scale 0‐4. Number of patients with significant decrease in pain. 10/10, 24 hrs: 9/10, 1m: 9/10, 2m: 7/10, 3m: 0/10, 4m | |
| Notes | R=1 B=1 W=0 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment? | Low risk | A ‐ Adequate |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Camerlain 1976 | Mixed population (not confined to RA patients) |
| Camerlain 1981 | Data not analysable |
| Depei 1992 | No numerical data |
| Devyani 1985 | Literature Review |
| LI C 1999 | No control group |
| Shen 1973 | Incomplete data, patients own control, no means or standard deviations |
| Sun 1992 | No control group |
| Tukmashi 2000 | Not a clinical trial |
| Usichenko 2003 | Les than 5 patients in the control group |
| XI D 1992 | Animals used as comparison group |
| XI YJ 1986 | No control group |
Contributions of authors
VR extracted and analyzed data and selected trials for the original review.
LB contributed to the data extraction, updated the selection of the reference list, updated the analyses and update of the interpretation of results.
SM was responsible for language revision, contributed to the data extraction and updated the analyses.
LC was responsible for writing the manuscript, contributed to data extraction and updated the analyses and interpretation of results.
GW and PT contributed their methodological expertise and commented on early drafts.
Declarations of interest
None known
Edited (no change to conclusions)
References
References to studies included in this review
David 1999 {published data only}
- David J, Townsend S, Sathananan R. The Effect of Acupuncture on Patients with RA: A Randomized, Placebo‐Controlled Cross‐Over Study. Rheumatology 1999;38:864‐869. [DOI] [PubMed] [Google Scholar]
Man 1974 {published data only}
- Man SC, Baragar FD. Preliminary Clinical Study of Acupuncture in RA. The Journal of Rheumatology 1974;1(1):126‐129. [PubMed] [Google Scholar]
References to studies excluded from this review
Camerlain 1976 {published data only}
- Camerlain M, Myhal D. [L'Acupuncture en Rhumatology]. L'Union Médicale du Canada 1976;105:552‐556. [6‐AC] [PubMed] [Google Scholar]
Camerlain 1981 {published data only}
- Camerlain M, Leung CY, Santerre A, Munan L, Myhal D. [Évaluation de l'acupuncture dans l'arthrite rhumatoide]. L'Union médicale du Canada 1981;110:1041‐1044. [1‐AC] [PubMed] [Google Scholar]
Depei 1992 {published data only}
- Depei X, Jianzhong H, Zhongyi A, Zuolu S. Acupuncture Treatment of Rheumatoid Arthritis and Exploration of Acupuncture Manipulations. Journal of Traditional Chinese Medicine 1992;12:35‐40. [4‐AC] [PubMed] [Google Scholar]
Devyani 1985 {published data only}
- Devyani BS. Acunpuncture for Rheumatoid Arthritis: An Analysis of Literature. Seminars in Arthritis and Rheumatism 1985;14(4):225‐231. [6‐AC] [DOI] [PubMed] [Google Scholar]
LI C 1999 {published data only}
- Li C, Jiang Z, Li Y. Therapeutic Effect of Needle Warming Through Moxibustion at Twelve SHU Points on Rheumatoid Arthritis. Journal of Traditional Chinese Medicine 1999;19(1):22‐26. [PubMed] [Google Scholar]
Shen 1973 {published data only}
- Shen AC, Whitehouse MJ, Powers TR, Rhodes CY, Engleman EP. A Pilot Study of the Effects of Acupuncture in Rheumatoid Arthritis. Arthritis and Rheumatism 1973;16(4):569‐570. [Google Scholar]
Sun 1992 {published data only}
- Sun, L, et al. Treatment of Rheumatoid Arthritis by Warming Needle. Journal of Traditional Chinese Medicine 1992;12(1):41‐44. [PubMed] [Google Scholar]
Tukmashi 2000 {published data only}
- Tukmashi ES. Acupuncture for Rheumatoid Arthritis. Acupuncture in medicine 2000;18(1):70‐73. [5‐AC] [Google Scholar]
Usichenko 2003 {published data only}
- Usichenko TI, Ivashkivsky OI, Gizhko VV. Treatment of Rheumatoid Arthritis with Electromagnetic Millimeter Waves Applied to Acupuncture Points‐a Randomized Double Blind Clinical Study. Acupuncture & Electro‐Therapeutics Research 2003;28(1‐2):11‐8. [DOI] [PubMed] [Google Scholar]
XI D 1992 {published data only}
- Xi D, Han JH, Zhang Z. Acupuncture Treatment of Rheumatoid Arthritis and Exploration of Acupuncture Manipulations. Journal of Traditional Chinese Medicine 1992;12(1):35‐40. [PubMed] [Google Scholar]
XI YJ 1986 {published data only}
- Xi YJ, Pu YX, Chen G, Xu XD, Lui LG, Hou G. Acupuncture Treatment of Early Rheumatoid Arthritis. Journal of Traditional Chinese Medicine 1986;6(3):162‐164. [PubMed] [Google Scholar]
Additional references
Dickersin 1994
- Dickersin K, Scherer R, Lefebvre C. Identifying relevant studies for systematic reviews. BMJ 1994;309:1286‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dorland 1988
- Dorland's illustrated medical dictionnary 27th ed. Toronto: Saunders, 1988. [Google Scholar]
Dumoulin 1978
- Dumoulin J, Bisschop G. Électrothérapie 3ième ed.. Paris: Maloine, 1978. [Google Scholar]
Haynes 1994
- Haynes R, Wilczynski N, McKibbon KA, Walker CJ, Sinclair JC. Developing optimal search strategies for detecting clinically sound studies in MEDLINE. Journal of the American Medical Informatics Association 1994;1:447‐58. [DOI] [PMC free article] [PubMed] [Google Scholar]
Jadad 1996
- Jadad A, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gravaghan DJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17:1‐17. [DOI] [PubMed] [Google Scholar]
Lineker 1999
- Lineker S, Wood H. Rheumatoid arthritis management protocol. The Arthritis Society: Consultation and Therapy Services. Toronto: The Arthritis Society, 1990. [Google Scholar]
OMERACT 1993
- OMERACT. [Conference on outcome measures in rheumatoid arthritis clinical trials]. Journal of Rheumatology. 1993; Vol. 20:526‐591. [PubMed]
Tugwell 2004
- Tugwell P, Shea B, Brooks P, Boers M, Simon L, Strand V, et al. Evidence Based Rheumatology. BMJ Books, 2004. [Google Scholar]
Tukmachi 2000
- Tukmachi E. Acupuncture and rheumatoid arthritis. Rheumatology 2000;39:1153‐1154. [DOI] [PubMed] [Google Scholar]
Walker 1996
- Walker JM, Helewa A. Physical therapy in arthritis. Montréal: W.B. Saunders company, 1996. [Google Scholar]
Wong 1987
- Wong T, Cheng R. The science of acupuncture 2nd ed.. Hong Kong: Kola Mayland co., 1987. [Google Scholar]