

Abstract
Background
Motor control exercise (MCE) is used by healthcare professionals worldwide as a common treatment for low back pain (LBP). However, the effectiveness of this intervention for acute LBP remains unclear.
Objectives
To evaluate the effectiveness of MCE for patients with acute non‐specific LBP.
Search methods
We searched MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL), four other databases and two trial registers from their inception to April 2015, tracked citations and searched reference lists. We placed no limitations on language nor on publication status.
Selection criteria
We included only randomised controlled trials (RCTs) examining the effectiveness of MCE for patients with acute non‐specific LBP. We considered trials comparing MCE versus no treatment, versus another type of treatment or added as a supplement to other interventions. Primary outcomes were pain intensity and disability. Secondary outcomes were function, quality of life and recurrence.
Data collection and analysis
Two review authors screened for potentially eligible studies, assessed risk of bias and extracted data. A third independent review author resolved disagreements. We examined MCE in the following comparisons: (1) MCE versus spinal manipulative therapy; (2) MCE versus other exercises; and (3) MCE as a supplement to medical management. We used the GRADE (Grades of Recommendation, Assessment, Development and Evaluation) approach to assess the quality of evidence. For missing or unclear information, we contacted study authors. We considered the following follow‐up intervals: short term (less than three months after randomisation); intermediate term (at least three months but within 12 months after randomisation); and long term (12 months or longer after randomisation).
Main results
We included three trials in this review (n = 197 participants). Study sample sizes ranged from 33 to 123 participants. Low‐quality evidence indicates no clinically important differences between MCE and spinal manipulative therapy for pain at short term and for disability at short term and long term. Low‐quality evidence also suggests no clinically important differences between MCE and other forms of exercise for pain at short or intermediate term and for disability at intermediate term or long term follow‐up. Moderate‐quality evidence shows no clinically important differences between MCE and other forms of exercise for disability at short term follow‐up. Finally, very low‐quality evidence indicates that addition of MCE to medical management does not provide clinically important improvement for pain or disability at short term follow‐up. For recurrence at one year, very low‐quality evidence suggests that MCE and medical management decrease the risk of recurrence by 64% compared with medical management alone.
Authors' conclusions
We identified only three small trials that also evaluated different comparisons; therefore, no firm conclusions can be drawn on the effectiveness of MCE for acute LBP. Evidence of very low to moderate quality indicates that MCE showed no benefit over spinal manipulative therapy, other forms of exercise or medical treatment in decreasing pain and disability among patients with acute and subacute low back pain. Whether MCE can prevent recurrences of LBP remains uncertain.
Plain language summary
Motor control exercise for acute non‐specific low back pain
Review question
To evaluate the effectiveness of motor control exercise (MCE) for patients with acute non‐specific low back pain (LBP).
Background
LBP is a common disorder that is often associated with pain and disability. One common intervention for patients with LBP is exercise therapy, and MCE is widely used for these patients. However, its effectiveness for patients with acute LBP remains unclear.
Search date
Evidence is current to April 2015.
Study characteristics
We included in this review three trials evaluating acute or subacute pain in patients with LBP (n = 197 participants). Most participants were middle‐aged and were recruited from primary or tertiary care centres. Duration of treatment programmes ranged from four weeks to six weeks.
Key results
MCE showed no benefit over spinal manipulative therapy, other forms of exercise or medical treatment for reducing pain or disability among patients with acute and subacute LBP. Whether MCE can prevent recurrences of LBP remains unclear.
Quality of the evidence
Results of this review include evidence of very low to moderate quality. We downgraded all comparisons for imprecision due to small study sample sizes.
Summary of findings
Background
Low back pain (LBP) continues to be the leading cause of disability and work loss in industrialised countries (Stephens 2007). According to the Global Burden of Disease study, LBP ranks first among the leading causes of disability globally (Murray 2012). Exercise therapy is endorsed in clinical guidelines (Koes 2010) as an effective treatment for chronic non‐specific LBP, and is also suggested by some systematic reviews (Hayden 2005; Hayden 2005b; Macedo 2010). However, current clinical guidelines suggest that supervised exercises programmes are not indicated for those with acute LBP (Koes 2010). Instead, the recommendation is to begin treatment of acute LBP with simple analgesics and to stay active (Hancock 2007; Machado 2010). Regardless of current recommendations, evidence on effects of exercise in acute and subacute populations is of moderate quality (Hayden 2005), and exercise is commonly prescribed for patients with acute pain in many countries (Williams 2010).
An intervention commonly used for patients with LBP is motor control exercise (MCE). MCE was developed to restore co‐ordination, control and capacity of trunk muscles (Hodges 2003). This intervention involves training isolated contraction of deep trunk muscles and further integrating the activation of these muscles into more complex static, dynamic and functional tasks (Ferreira 2007; O'Sullivan 1997). The treatment also provides co‐ordination and optimal control of global trunk muscles (Costa 2009; Macedo 2012). Two previous systematic reviews have evaluated the evidence on MCE for acute LBP (Ferreira 2006; Rackwitz 2006). However, each of these reviews included only one trial, and both were published in 2006. Therefore, a Cochrane systematic review on this topic was conducted to provide updated estimates of treatment effects of MCE for patients with acute LBP.
Description of the condition
Low back pain (LBP) is considered a major health and socioeconomic problem that is highly associated with work absenteeism, disability and high costs for patients and for society (Airaksinen 2006). LBP could be defined as pain and discomfort located below the ribs and above the gluteal crease, with or without referred leg pain (Airaksinen 2006; van Tulder 2006). The term 'non‐specific LBP' has often been used in research, as the source of pain could not be established in most cases (Hancock 2007; Niemisto 2004; Niemisto 2005). Thus, non‐specific LBP is defined as LBP that cannot be attributed to a recognisable or specific pathology such as nerve root compromise or serious spinal pathology (i.e. fracture, cancer and inflammatory disease) (Airaksinen 2006; van Tulder 2006). 'Acute LBP' describes episodes lasting less than six weeks, and 'subacute LBP' refers to episodes between six and 12 weeks in duration (Furlan 2009).
Description of the intervention
Motor control exercise (MCE) applies principles of motor learning to integrate control and co‐ordination of the spine muscles for functional activities. Exercise is individualised and tailored upon initial assessment of each patient’s individual posture, muscle activation and co‐ordination. MCE is designed to train muscles that are identified as having poor control (often deep trunk muscles such as multifidus and transversus abdominis) and to reduce the activity of muscles that are overactive (often large external trunk muscles such as rectus abdominis and erector spinae muscles) (Hodges 1996; O'Sullivan 1997). This intervention progresses from static isolated contraction of deep trunk muscles towards integration of these muscles into simple static activities, then to dynamic tasks and finally functional activities (Costa 2009; Macedo 2012).
Protocols implemented in randomised controlled trials do not always completely match the previous description because of the complexity of this intervention (Macedo 2009). Often after undergoing assessment, patients are instructed to contract the deep trunk muscles, then integrate them into other activities without considering the principles of motor learning and without focusing on the need to progress to more functional activities (Macedo 2012; Menezes Costa 2009). For this reason, the intervention is often described as specific stabilisation exercises, not necessarily as exercises for motor control.
How the intervention might work
Motor control exercise (MCE) was developed on the basis of results of cross‐sectional laboratory studies reporting that individuals with LBP have impaired control of the deep trunk muscles (e.g. transversus abdominis, transversus multifidus) responsible for maintaining stability of the spine (Hodges 1997; Hodges 1998; Moseley 2002). For instance, these cross‐sectional studies have shown that people with LBP have delayed activity of transversus abdominis (Hodges 1996) and multifidus muscles (Macdonald 2011). Furthermore, paraspinal muscles of people with LBP have been found to have decreased cross‐sectional area (Hides 1994), increased fatigability (Roy 1989) and increased intramuscular fat (Alaranta 1993).
Studies have found that individuals with LBP have impaired control of superficial trunk muscles (e.g. rectus abdominis, latissimus dorsi, external and internal obliques) (Cholewicki 2005; Radebold 2000; van Dieen 2003). These impairments have been identified during tasks of trunk perturbance whereby patients with LBP have demonstrated increased co‐contraction of flexors and extensors of the trunk, delayed offset of agonists and delayed onset of antagonists (Radebold 2000). Delayed muscle response during the same task was found to be associated with development of future LBP (Cholewicki 2005). Position sense of the extensors of the trunk has been found to be altered in patients with LBP (Newcomer 2000). Thus, MCE was developed to target these differences and potentially restore the individual’s muscle co‐ordination and control.
Why it is important to do this review
Over the past two decades, MCE has become one of the popular exercise therapies provided for back pain, and the number of studies evaluating the effectiveness of this intervention has increased significantly. Consequently, systematic reviews have been published to summarise this evidence (Brumit 2013; Bystrom 2013; Ferreira 2006; Macedo 2009); however, a great majority of these reviews have focused on effects of the intervention on individuals with chronic LBP (Bystrom 2013; Macedo 2009) without including studies evaluating acute back pain (Hauggaard 2007). Only two reviews included and analysed acute LBP trials separately, but these reviews were published in 2006 and included only one trial (Ferreira 2006; Rackwitz 2006).
Objectives
To evaluate the effectiveness of MCE for patients with acute non‐specific LBP.
Methods
Criteria for considering studies for this review
Types of studies
We included only randomised controlled trials (RCTs). We did not consider trials with a quasi‐random allocation procedure for inclusion in this review, to avoid biased estimates of treatment effects across included studies (Higgins 2011), and to comply with recommendations provided in current guidelines of the Cochrane Back and Neck Review Group (CBN) (Furlan 2015).
Types of participants
We included trials that explicitly reported that a criterion for entry was acute or subacute non‐specific LBP (with or without leg pain). We excluded trials including individuals with specific conditions such as disc herniation with nerve root compromise, spinal stenosis, cancer, etc., and we included trials evaluating adults of either gender. We included trials with a mixed population in relation to type and duration of back pain only if separate data were provided for each group, or if the acute/subacute population corresponded to the majority of included participants (> 75%). However, we did not identify any trials with mixed populations for consideration for inclusion. When manuscripts did not include enough information to classify participants as having non‐specific LBP or to specify the duration of pain, we contacted study authors for clarification. If we received no response within one month, following bi‐weekly emails, we excluded and adequately referenced the study.
Types of interventions
We included trials comparing MCE versus no treatment or another treatment and trials in which MCE was added as a supplement to other interventions. When MCE was used in addition to other treatments, it had to represent at least 50% of the total treatment programme for the study to be included.
We considered trials to have evaluated MCE if investigators described exercise treatment as motor control or specific stabilisation exercise, and/or if they described exercise aimed to activate, train or restore stabilisation function or co‐ordination of specific muscles of the spine, such as multifidus and transversus abdominis. We considered specific stabilisation exercises and exercises aiming to activate, train or restore stabilisation or co‐ordination of specific deep muscles because these principles characterise the MCE intervention. As reports of trials do not always consider the principles of motor learning, study authors often describe the intervention as specific stabilisation exercise rather than as MCE.
Because a Cochrane review on Pilates is being conducted (Costa 2012), we excluded from this review trials evaluating Pilates, although principles of Pilates may overlap with principles of a motor control intervention (Herrington 2005).
Types of outcome measures
Primary outcomes were pain intensity and disability. Secondary outcomes were function, quality of life, adverse events and recurrence.
Search methods for identification of studies
Electronic searches
We searched the following electronic databases from their inception to 2 April 2015.
MEDLINE (Ovid SP, 1946 to Week 5 March 2015).
MEDLINE In‐Process & Other Non‐Indexed Citations (Ovid SP, 1 April 2015).
EMBASE (Ovid SP, 1980 to Week 13 2015).
Cochrane Central Register of Controlled Trials (CENTRAL) (March 2015; Issue 3).
Cumulative Index to Nursing and Allied Health Literature (CINAHL) (EBSCO, 1981 to April 2015).
Allied and Complementary Medicine (AMED) (Ovid, 1985 to March 2015).
SportDiscus (EBSCO, 1800 to April 2015).
Physiotherapy Evidence Database (PEDro).
Latin American and Caribbean Health Sciences Literature (LILACS).
ClinicalTrials.gov.
World Health Organization International Clinical Trials Registry Platform (WHO ICTRP).
PubMed.
We conducted searches in 2012 and 2014. For the 2015 update, we added a search of MEDLINE In‐Process & Other Non‐Indexed Citations and PubMed, using the strategy applied by Duffy 2014, to capture studies not yet available in MEDLINE.
We used the search strategies developed by the Cochrane Back and Neck Review Group. We did not restrict searches or inclusion criteria to any specific language. See Appendix 1.
Searching other resources
We performed citation tracking by using Web of Science (Thomson Reuters) and by conducting a manual search of the reference lists of previous reviews and eligible trials.
Data collection and analysis
Selection of studies
Two review authors (LGM and LC or BTS and TPY) screened all search results for potentially eligible studies, assessed risk of bias and extracted study data. A third independent review author (RWJGO or CGM) resolved disagreements on inclusion of trials, quality assessment and data extraction. For non‐English language manuscripts, we identified a native speaker within local universities to assist with translation. Pilot testing of assessment of risk of bias and extraction of data were performed for two studies, as recommended by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Data extraction and management
We extracted data from each included study using a standardised data extraction form. Two review authors extracted the data (BTS and TPY) and resolved disagreements through discussion with or arbitration of a third review author (CGM). We extracted from the trial reports mean scores, standard deviations and sample sizes for continuous outcomes, and sample sizes and numbers of events for dichotomous outcomes. When this information was not provided in the trial report, we calculated or estimated the values using methods recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We also extracted from the studies information about characteristics of participants, treatments and co‐interventions provided, duration of treatment and outcome measures and risk of bias criteria.
Assessment of risk of bias in included studies
We assessed risk of bias using the Cochrane Back and Neck Review Group expanded criteria (12 items) (Furlan 2009; Higgins 2011) described in Appendix 2. We labelled the risk of bias for a trial as ‘low risk' (at least six of the 12 criteria met) or as 'high risk' (fewer than six criteria met).
Measures of treatment effect
We expressed treatment effects of continuous variables as mean differences and 95% confidence intervals (CIs). We used risk ratios and odds ratios with 95% CIs to calculate treatment effects of dichotomous variables. We converted ordinal variables if present to dichotomous variables for the purpose of the analysis. We expressed pooled effects of continuous variables as mean differences if the same outcomes were used. If continuous outcome measures were different between studies, we expressed pooled effects with mean differences but first converted the different outcome measures to a common 0 to 100 scale. Although use of standardised mean differences is recommended when studies with different outcomes measures are pooled, we chose to use mean differences in this study because they are easier to interpret, and because included outcomes can be used interchangeably (Roland 2000). Finally, we preferred to used intention‐to‐treat analysis over per‐protocol or per‐treated analysis (in the case that a trial presented both analyses).
Unit of analysis issues
If trials were sufficiently homogenous, we conducted a meta‐analysis for these follow‐up time points: short (within three months after randomisation), intermediate (at least three months but within 12 months after randomisation) and long term (12 months or longer after randomisation). When multiple time points fell within the same category, we used the one that was closer to the end of treatment ‐ 6 months or 12 months.
Dealing with missing data
When information provided by trial authors was insufficient to allow evaluation of treatment effects, we contacted these authors to request the required information. We estimated data from graphs when not reported in tables or text. If information regarding standard deviations (SDs) was missing, we calculated SDs from confidence intervals or standard errors (if available), or we estimated them from the range provided in the same study. Finally, if no measure of variability was presented anywhere in the report, we adopted the standard deviation from the most similar trial in the review.
Assessment of heterogeneity
We performed visual inspection of the forest plot and of the overlap of confidence intervals to evaluate heterogeneity. Furthermore, we calculated Chi2 and I2 statistics as recommended by the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We defined substantial heterogeneity as I2 > 50%, and we described results in the text qualitatively. When I2 values were slightly higher than 50% but no clear heterogeneity was identified by visual inspection, we combined results into a meta‐analysis using the random‐effects model and downgraded the quality of evidence assessment for inconsistency (Grading of Recommendations Assessment, Development and Evaluation ‐ GRADE).
Data synthesis
Regardless of whether sufficient data were available to perform quantitative analyses to summarise the data, we assessed the overall quality of the evidence for each outcome. To accomplish this, we used the GRADE approach, as recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) and adapted in the updated CBN method guidelines (Furlan 2015). We based the quality of the evidence upon five main domains, and for each domain that was not met, we reduced the quality by one level from high quality to moderate, low or very low quality. We used the following five domains: (1) study design and risk of bias (downgraded if > 25% of participants were included in studies with high risk of bias); (2) inconsistency of results (downgraded if significant heterogeneity was presented upon visual inspection or I² > 50%); (3) indirectness (generalisability of findings; downgraded if > 50% of participants were outside the target group) and indirectness of outcome measurements; (4) imprecision (downgraded if fewer than 400 participants were included in the comparison for continuous data and fewer than 300 events for dichotomous data (Mueller 2007)); and (5) other bias (e.g. publication bias). We considered single studies with fewer than 400 participants for continuous outcomes (or fewer than 300 participants for dichotomous outcomes) to be inconsistent and imprecise, providing 'low‐quality evidence', which could be downgraded to 'very low‐quality evidence' if we identified limitations on the quality of evidence (Rubinstein 2012). We described the quality of the evidence (Balshem 2011) as follows.
High‐quality evidence: consistent findings among at least 75% of RCTs with no limitations in study design; consistent, direct and precise data; and no known or suspected publication bias. We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate‐quality evidence: one of the domains not met. We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but it may be substantially different.
Low‐quality evidence: two domains not met. Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect.
Very low‐quality evidence: three domains not met. We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
No evidence: no RCTs identified that addressed this outcome.
Finally, we evaluated the quality of the evidence by considering the size of effects identified in the review. A clinically important effect was considered when the magnitude of the effect size was at least medium (>10% of the scale).
Sensitivity analysis
We did not plan to perform any sensitivity analysis, as we expected the number of included trials to be low.
Results
Description of studies
See Characteristics of included studies and Characteristics of excluded studies.
Results of the search
The search retrieved 2055 records of trials, of which we selected 181 for full text assessment; three trials fulfilled the inclusion criteria (total sample = 197). Figure 1 shows the flowchart of the inclusion process for studies in this review.
1.
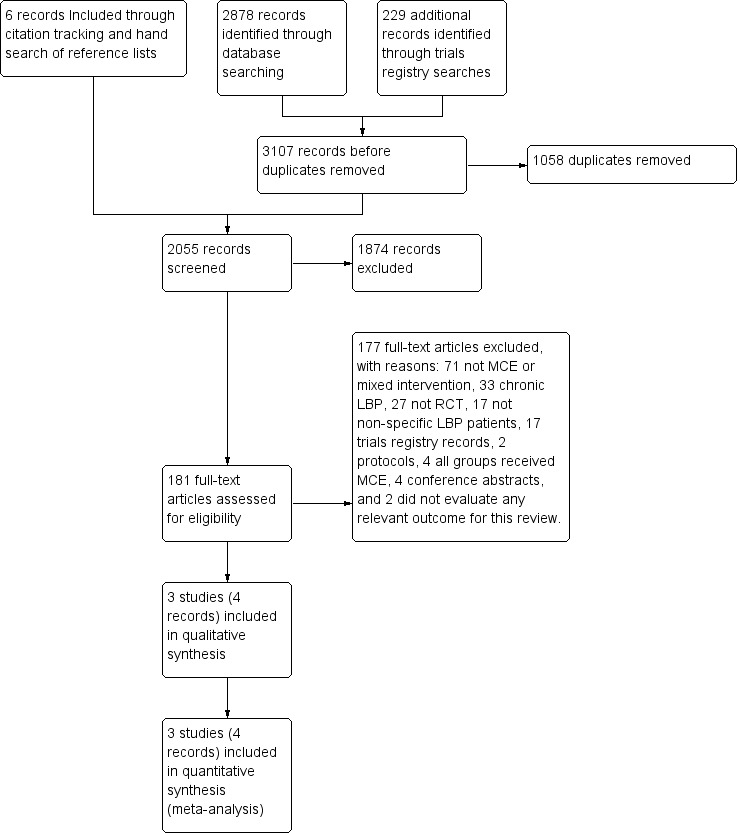
Study flow diagram.
Searches for ongoing and unpublished trials in registries yielded 17 registered trials and 2 published protocols. Two records described the same trial (ISRCTN80064281; Saner 2011). One registered trial was ineligible, as both groups received MCE (NCT01061632), three were not considered to provide MCE (ACTRN12609000293268; NCT00624533; ISRCTN80064281) and one included a mix of MCE and manual therapy in the intervention group (ACTRN12609000334202).The remaining registered trials did not enrol patients with acute LBP and were ineligible (ACTRN12609000343202; ACTRN12611000971932; Magalhaes 2013; NCT01362049; NCT02112760; NCT02170753; NCT02221609; NCT02374970; NCT02398760; NCT02200913; NCT00201513; NCT00555802; NCT01124201).
Included studies
We included three trials in this review (197 participants) (Aluko 2013; Brennan 2006; Hides 1996). Study sample sizes ranged from 33 to 123 participants (median (interquartile range (IQR)) = 41 (65.5)). We included in the review data from three trials with four publications, as two records reported data from the same participants (Hides 1996). Trials included in this review were conducted in Australia (Hides 1996), United Kingdom (Aluko 2013) and United States (Brennan 2006). Data in the Brennan 2006 publication were presented to test unmatched versus matched treatment, but when contacted, study authors provided data indexed by randomised treatment assignment.
Types of studies
Two trials compared MCE versus other types of exercise including general exercise (Aluko 2013) and specific exercise (i.e. the direction that reduced symptoms) (Brennan 2006). One trial compared MCE versus spinal manipulative therapy (Brennan 2006), and the other trial (Hides 1996) included MCE as a supplement to medical management. In this trial, medical management comprised advice on bed rest, absence from work, prescription of medication and advice to resume normal activity as tolerated. For one trial (Brennan 2006), we included two comparison groups used for different comparisons.
Study population
Most participants were middle‐aged (median (IQR) = 36 (4.75) years; range 31 to 38.4 years) patients recruited from primary or tertiary care centres. All included participants reported acute or subacute LBP. One trial (Aluko 2013) included patients referred for treatment of acute non‐specific LPB with a maximum duration of six weeks, and another trial (Hides 1996) included patients experiencing their first episode of mechanical LBP for less than three weeks. One trial (Brennan 2006) included patients with a primary complaint of LBP lasting less than 90 days, with or without leg pain.
Technique: number and duration of treatments
The duration of treatment programmes ranged from four to six weeks. Brennan 2006 and Hides 1996 included a twice‐weekly programme provided for four weeks for a maximum of eight sessions, and Aluko 2013 reported an exercise programme lasting six weeks.
Primary outcomes
Pain intensity: All included trials measured pain intensity by using a visual analogue scale (VAS).
Disability: Two trials (Aluko 2013; Hides 1996) measured disability using the Roland Morris Disability Questionnaire, and one trial (Brennan 2006) used the Oswestry Disability Index.
Secondary outcomes
Recurrence: One trial (Hides 1996) reported recurrence outcomes using a questionnaire developed by the authors of the trial.
Included trials provided no data on the other secondary outcomes (function, quality of life, adverse events).
Follow‐up
All trials measured short‐term follow‐up; two at four weeks (Brennan 2006; Hides 1996), and one at six weeks (Aluko 2013). Only one trial included intermediate‐term follow‐up of three months (Aluko 2013), and two trials (Brennan 2006; Hides 1996) measured long‐term follow‐up, disability at one year and recurrence at one year, respectively.
Excluded studies
We excluded a total of 177 studies during the full text analysis stage. We considered 71 studies as not providing MCE or as providing a mix of interventions (Aasa 2015; Ali 2006; Ammar 2011; Andrusaitis 2011; Bentsen 1997; Bi 2013; Bronfort 1996; Bronfort 2011; Brooks 2012; Brox 2003; Byuon 2012; Cairns 2003; Chan 2011; Cho 2014; Chung 2013; Descarreaux 2002; Donzelli 2006; Dufour 2010; Durante 2010; Dvorak 2011; Faas 1993; Faas 1995; Freitas 2008; Gagnon 2005; Gatti 2011; Hagen 2010; Hansen 1993; Harkapaa 1989; Harts 2008; Helewa 1999; Helmhout 2004; Henchoz 2010; Hunter 2012; Hwang 2013; Jang 2013; Johannsen 1995; Johnson 2007; Jones 2007; Kaapa 2006; Kline 2013; Kofotolis 2008; Koldas 2008; Kumar 2011; Lie 1999; Long 2004; Mannion 1999; Mannion 2009; Mannion 2012Marshall 2008; Mohseni‐Bandpei 2011; Moseley 2002; Nelson 1995; Niemisto 2003; Niemisto 2004; Niemisto 2005; Oguzhan 2011; Riipinen 2005; Rydeard 2006; Saner 2015; Shnayderman 2013; Smith 2011; Suni 2006; Torstensen 1998; Wang 2012; Willemink 2012; Williamson 2008; Xueqiang 2012; Yelland 2004; Yoo 2012; You 2014; Zhang 2015), 33 examined chronic LBP (Akbari 2008; Alp 2014; Areeudomwong 2012; Cairns 2006; Costa 2009; Critchley 2007; Ferreira 2007; Franca 2010; Franca 2012; Goldby 2006; Hemmati 2011; Hosseinifar 2013; Inani 2013; Javadian 2012; Kachanathu 2012; Koumantakis 2005; Kumar 2009; Kumar 2010; Lomond 2015; Macedo 2012; Miller 2005; Moon 2013; Puntumetakul 2013; Rabin 2014; Rasmussen‐Barr 2003; Rasmussen‐Barr 2009; Rhee 2012; Shaughnessy 2004; Stankovic 2012; Tsauo 2009; Unsgaard‐Tondel 2010; Vasseljen 2010; Vasseljen 2012), 27 were not RCTs (Allison 2012; Appling 2009; Barbosa 2013; Buchbinder 2002; Croft 1999; Dehner 2009; Gustafsson 2008; Harringe 2007; Hides 2008; Hurwitz 2005; Karimi 2009; Kumar 2012; Kuukkanen 1996; Magnusson 2008; Mannion 2009; Mannion 2012; Monteiro 2009; Moussouli 2014; Navalgund 2009; Nelson‐Wong 2009; Norris 2008; Ota 2011; Pereira 2010; Smeets 2009; Sokunbi 2008; Streicher 2014; Yang 2010), 17 did not include participants with non‐specific LBP (Aggarwal 2010; Belcher 1998; Bilgin 2013; Bordiak 2012; Childs 2009; Childs 2010; Ewert 2009; George 2011; Guven 2003; Kladny 2003; Lee 2015; Monticone 2004; O'Sullivan 1997; Shakeri 2013; Shnayderman 2013; Stuge 2004; Teyhen 2010), four described MCE provided to all groups (Ahmed 2014; Lewis 2005; Moseley 2003; Trampas 2014) and four were presented as conference abstracts but enrolled chronic LBP patients only (Alp 2011; Bayraktar 2013; Carmo 2013; Meira 2013). Finally, 17 were registered trials and 2 were protocols already discussed, and 2 did not include any relevant outcome for this review (Earde 2014; Javadian 2015).
Risk of bias in included studies
We considered two trials in this review as having low risk of bias (Aluko 2013; Brennan 2006) and one trial as having high risk of bias (Hides 1996). Figure 2 shows results of the risk of bias analysis for individual studies.
2.
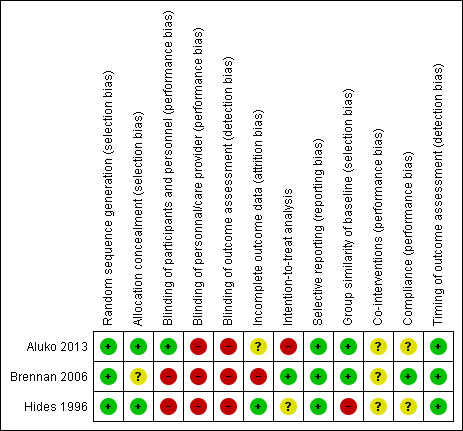
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
All included studies met the criteria for adequate randomisation and allocation concealment, except for one study that provided insufficient information about the allocation process (Brennan 2006).
Blinding
Two trials reported blinding of outcome assessors (Brennan 2006; Hides 1996); however, as outcomes were self reported in these trials, we did not consider the assessor to be blinded. One trial blinded participants (Aluko 2013), and we assumed that blinding of therapists was not possible because of the nature of the intervention.
Incomplete outcome data
One trial provided adequate information about missing data and reported acceptable rates (Hides 1996). In one trial, information about missing data was unclear (Aluko 2013), and investigators in another trial could not keep the dropout rate below 20% for short‐term and intermediate‐term, and 30% for long‐term, outcomes (Brennan 2006).
Selective reporting
It was not possible to find any registry or published protocol for the included trials. However, according to the study reports, we considered it likely that all expected outcomes were included. Therefore, all trials fulfilled this criterion and were considered at low risk of reporting bias.
Other potential sources of bias
Publication bias: It was not possible to assess publication bias by using funnel plots, as this review included only three trials with a maximum of two trials per comparison.
Effects of interventions
See: Table 1; Table 2; Table 3
for the main comparison.
| Motor control exercise vs spinal manipulative therapy for acute low back pain | ||||
|
Patient or population: patients with acute low back pain Settings: primary or tertiary care Intervention: motor control exercise Comparison: spinal manipulative therapy | ||||
| Outcomes | Illustrative comparative risks* (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | |
| Assumed risk | Corresponding risk | |||
| Spinal manipulative therapy | Motor control exercise | |||
|
Pain VAS (0 to 100) Follow‐up: short term (< 3 months from randomisation) |
Mean pain in the control group was 15 points |
Mean pain in the intervention group was 9 points higher (1.56 lower to 19.56 higher) |
58 participants (1 study) |
⊕⊕⊝⊝ Lowa,b |
|
Disability Oswestry Disability Index (0 to 100) Follow‐up: short term (< 3 months from randomisation) |
Mean disability in the control group was 17.9 points |
Mean disability in the intervention group was 4 points higher (3.38 lower to 11.38 higher) |
85 participants (1 study) | ⊕⊕⊝⊝ Lowa,b |
|
Disability Oswestry Disability Index (0 to 100) Follow‐up: intermediate term (> 3 months, < 12 months) |
Mean disability in the control group was 16.8 points |
Mean disability in the intervention group was 3.7 points higher (4.10 lower to 11.50 higher) |
85 participants (1 study) | ⊕⊕⊝⊝ Lowa,b |
|
Adverse events None of the included studies evaluated adverse events |
Not reported | Not reported | ||
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) CI: Confidence interval | ||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low quality: We are very uncertain about the estimate | ||||
aDowngraded for imprecision
bDowngraded for inconsistency
2.
| Motor control exercise vs other exercises for acute low back pain | ||||
|
Patient or population: patients with acute low back pain Settings: primary or tertiary care Intervention: motor control exercise Comparison: other exercises | ||||
| Outcomes | Illustrative comparative risks* (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | |
| Assumed risk | Corresponding risk | |||
| Other exercises | Motor control exercise | |||
|
Pain VAS (0 to 100) Follow‐up: short term (< 3 months from randomisation) |
Mean pain ranged across control groups from 18 to 26.7 points | Mean pain in the intervention groups was 5.74 points higher (3.34 lower to 14.82 higher) |
89 participants (2 studies) | ⊕⊕⊕⊝ Moderatea |
|
Pain VAS (0 to 100) Follow‐up: intermediate term (> 3 months, < 12 months) |
Mean pain in the control group was 27.1 points | Mean pain in the intervention groups was 1.2 points lower (18.24 lower to 15.84 higher) |
33 participants (1 study) | ⊕⊕⊝⊝ Lowa,b |
|
Disability Multiple scales (transformed 0 to 100) Follow‐up: short term (< 3 months from randomisation) |
Mean disability ranged across control groups from 20.6 to 39.2 points | Mean disability in the intervention groups was 0.84 points lower (8.72 lower to 7.04 higher) |
116 participants (2 studies) | ⊕⊕⊕⊝ Moderatea |
|
Disability Roland Morris Disability Questionnaire (transformed 0 to 100) Follow‐up: intermediate term (> 3 months, < 12 months) |
Mean disability in the control group was 28.3 points | Mean disability in the intervention groups was 6.70 points lower (22.80 lower to 9.40 higher) |
33 participants (1 study) | ⊕⊕⊝⊝ Lowa,b |
|
Disability Oswestry Disability Index (0 to 100) Follow‐up: long term (< 3 months after randomisation) |
Mean disability in the control group was 20.5 |
Mean disability in the intervention groups was
5.70 points higher (1.38 lower to 12.78 higher] |
83 participants (1 study) | ⊕⊕⊝⊝ Lowa,b |
|
Adverse events None of the included studies evaluated adverse events |
Not reported | not reported | ||
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) CI: Confidence interval | ||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low quality: We are very uncertain about the estimate | ||||
aDowngraded for imprecision
bDowngraded for inconsistency
3.
| Motor control exercise as a supplement to medical management for patients with acute low back pain | |||||
|
Patient or population: patients with acute LBP Settings: primary or tertiary care Intervention: motor control exercise Comparison: medical management | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | |
| Assumed risk | Corresponding risk | ||||
| Medical management | Motor control exercise | ||||
|
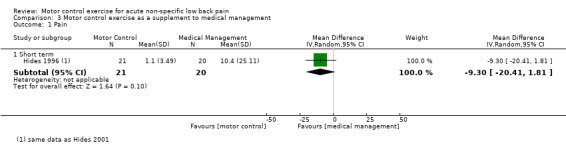
Pain VAS (0 to 100) Follow‐up: short term (< 3 months from randomisation) |
Mean pain in the control group was 10.4 | Mean pain in the intervention group was 9.30 points lower (20.41 lower to 1.81 higher) |
41 participants (1 study) | ⊕⊕⊝⊝ Very lowa,b,c | |
|
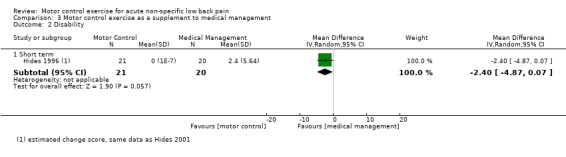
Disability Roland Morris Disability Questionnaire (transformed 0 to 100) Follow‐up: short term (< 3 months from randomisation) |
Mean disability in the control group was 2.4 |
Mean disability in the intervention group was
2.40 points lower (4.87 lower to 0.07 higher) |
41 participants (1 study) | ⊕⊕⊝⊝ Very lowa,b,c | |
|
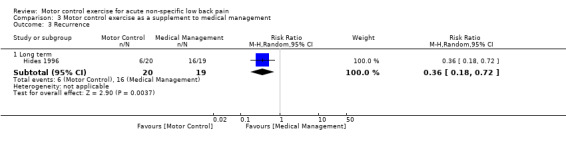
Recurrence Follow‐up: long term (1 year) |
16 of 19 | 6 of 20 |
RR 0.36 (0.18 to 0.72) |
39 participants (1 study) |
⊕⊕⊝⊝ Very lowa,b,c |
|
Adverse events None of the included studies evaluated adverse events |
Not reported | Not reported | |||
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI) CI: Confidence interval | |||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low quality: We are very uncertain about the estimate | |||||
aDowngraded for imprecision
bDowngraded for inconsistency
cDowngraded for high risk of bias
See Table 1; Table 2; and Table 3.
Effect of motor control exercise versus spinal manipulative therapy
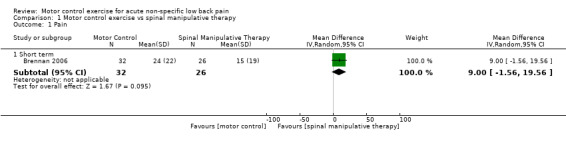
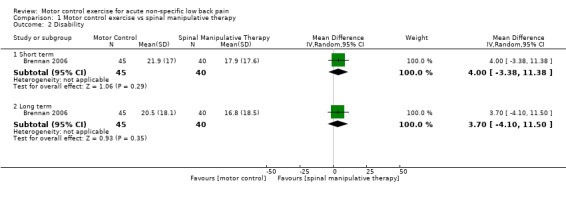
One trial included in this comparison (Brennan 2006) provided low‐quality evidence (downgraded for imprecision and inconsistency) that there is no clinically important difference between MCE and spinal manipulative therapy for pain relief at short‐term follow‐up (mean difference (MD) 9.00, 95% confidence interval (CI) –1.56 to 19.56; one trial; n = 58) nor for improved disability at short‐term (MD 4.00, 95% CI –3.38 to 11.38; one trial; n = 95) and long‐term follow‐up (MD 3.70, 95% CI –4.10 to 11.50; one trial; n = 95). We cannot discard an important effect for pain and disability as the confidence interval includes a clinically important effect.
Effect of motor control exercise versus other exercise
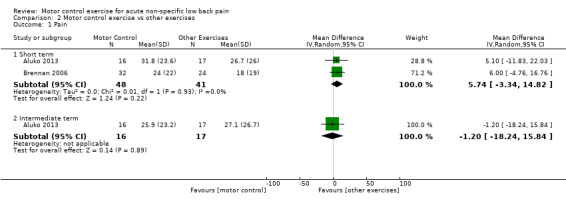
We included two trials for this comparison (Aluko 2013; Brennan 2006), both with low risk of bias. For pain, we noted no clinically important differences between MCE and other exercise at short‐term follow‐up, with moderate‐quality evidence (downgraded for imprecision) (MD 5.74, 95% CI ‐3.34 to 14.82; two trials; n = 89), and at intermediate‐term follow‐up, with low‐quality evidence (downgraded for imprecision and inconsistency) (MD ‐1.20, 95% CI ‐18.24 to 15.84; one trial; n = 33) (Figure 3). However, we cannot discard an important effect for pain as the confidence interval includes a clinically important effect.
3.
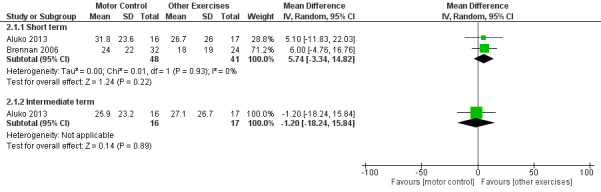
Forest plot of comparison: 2 Motor control exercise vs other exercises, outcome: 2.1 Pain.
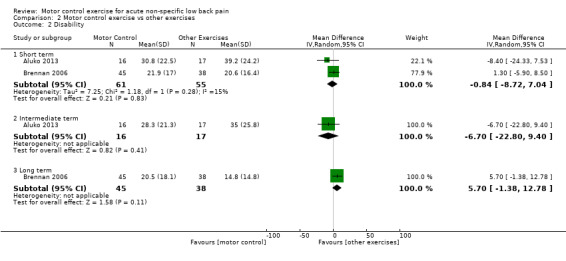
For disability, moderate‐quality evidence (downgraded for imprecision) indicated no clinically important differences in outcomes with MCE compared to other exercise at short‐term follow‐up (MD ‐0.84, 95% CI ‐8.72 to 7.04; two trials; n = 116). Low‐quality evidence (downgraded for imprecision and inconsistency) showed no clinically important differences between MCE and other exercise at intermediate‐term (MD ‐6.70, 95% CI ‐22.80 to 9.40; one trial; n = 33) and long‐term follow‐up (MD 5.70, 95% CI ‐1.38 to 12.78; one trial; n = 83) (Figure 4). We cannot discard an important effect for disability at long term as the confidence interval includes a clinically important effect.
4.
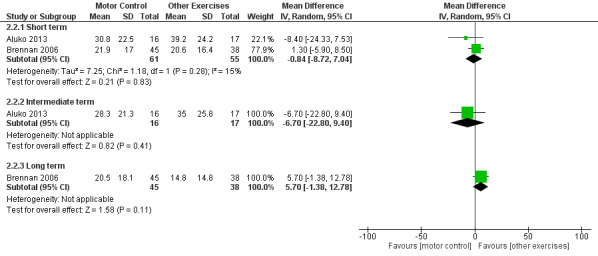
Forest plot of comparison: 2 Motor control exercise vs other exercises, outcome: 2.2 Disability.
Effect of motor control exercise as a supplement to medical management
We included in this comparison data from one trial (Hides 1996), which provided very low‐quality evidence (downgraded for risk of bias, imprecision and inconsistency) showing that MCE added to medical management does not provide any clinically important difference for pain (MD ‐9.30; 95% CI ‐20.41 to 1.81; one trial; n = 42) nor for disability (MD ‐0.90, 95% CI ‐4.77 to 2.97; one trial; n = 41) at short‐term follow‐up. However, we cannot discard an important effect for pain as the confidence interval includes a clinically important effect. For recurrence at one year, very low‐quality evidence (downgraded for risk of bias, imprecision and inconsistency) suggests that MCE and medical management decrease the risk of recurrence by 64% compared with medical management alone (risk ratio (RR) 0.36, 95% confidence interval (CI) 0.18 to 0.72; P value = 0.004; one trial; n = 39).
Discussion
Summary of main results
This review provides evidence of very low to moderate quality indicating no clinically important differences in outcome with motor control exercise (MCE) compared to other forms of treatment for patients with acute low back pain (LBP). Specifically, low‐quality evidence when MCE is compared to spinal manipulative therapy for pain at short‐term follow‐up and for disability at short‐term and long‐term follow‐up. Low‐quality evidence also indicates that MCE is not better than other forms of exercise for pain at short‐term and intermediate‐term follow‐up, and for disability at intermediate‐term and long‐term follow‐up. Moderate‐quality evidence reveals no clinically important differences between MCE and other forms of exercise for disability at short‐term follow‐up. Evidence of very low quality suggests that addition of MCE does not improve outcomes of medical management in terms of pain and disability at short term. Finally, evidence of very low quality indicates that MCE and medical management decrease risk of recurrence by 64% compared with medical management alone.
Overall completeness and applicability of evidence
This review is based on data from three small randomised controlled trials (RCTs) that enrolled a total of 197 participants from three different countries: Australia, United Kingdom and United States. Two trials included primarily patients with acute LBP (< six weeks) (Aluko 2013; Hides 1996), and one study included patients with acute and subacute LBP (< 90 days) (Brennan 2006). Hides 1996 included patients recruited from accident and emergency care, who can be different from those recruited from outpatient rehabilitation centres; this needs to be considered when results of this trial are evaluated. Hides 1996 reported a lower recurrence rate in the MCE group at one year. Given that most patients with acute LBP recover (Henschke 2008), and that motor control has been linked to the prognosis of LBP (Cholewicki 2005), evaluation of recurrence by future trials is needed.
Quality of the evidence
We considered two trials in this review to have low risk of bias (Aluko 2013; Brennan 2006), and one trial to have high risk of bias (Hides 1996). Two studies (Aluko 2013; Brennan 2006) provided inadequate information about incomplete data, and none of the included studies blinded outcome assessors. Additionally, given the small sample sizes among the included studies, we downgraded all conclusions about the strength of evidence according to the GRADE (Grades of Recommendation, Assessment, Development and Evaluation) method on the basis of imprecision and inconsistency. Thus, the small sample sizes and the small number of included studies limited the strength of our review conclusions.
Potential biases in the review process
We did not assess publication bias in this review because we included only three trials. Further, we followed a strict review process in accordance with Cochrane guidelines and a pre‐established protocol to avoid potential sources of bias. We minimised the potential for language bias by including trials reported in any language. A limitation of this review is that we included trials for which study authors described the intervention as MCE, and we acknowledge that this term may be interpreted differently by different researchers. The distinction between MCE, specific spinal stabilisation exercise and stabilisation exercise is subtle, and development and adoption of consensus terms and operational definitions for these forms of therapeutic exercise could facilitate improved understanding among care providers in this field.
Agreements and disagreements with other studies or reviews
Results of this review are consistent with current clinical guidelines that do not recommend structured exercises for acute LBP (van Tulder 2006). Moreover, other trials evaluating different exercise modalities for patients with acute LBP have not found clinically important differences (Machado 2010), and researchers have not provided a review of conservative treatment for acute LBP (van Tulder 1997). Also, the Cochrane review on exercise therapy for non‐specific LBP (Hayden 2005) showed no evidence for the effectiveness of exercise therapy in acute LBP, including MCE, as review authors included only one trial (Hides 1996).
For recurrence at one year, we found that MCE added to medical management decreases the risk of recurrence by 64% compared with medical management alone. Although we found evidence of very low quality, this finding is consistent with those of a previous review, which concluded that post‐treatment exercise programmes can prevent recurrence of LBP (Choi 2010).
Authors' conclusions
Implications for practice.
Evidence of very low to moderate quality shows that motor control exercise provides no benefit over spinal manipulative therapy, other forms of exercise or medical treatment in decreasing pain and disability among patients with acute and subacute low back pain. It remains uncertain whether motor control exercise can prevent recurrences of low back pain. These results are consistent with current clinical practice guidelines and the findings of previous systematic reviews.
Implications for research.
Results of this review are based on evidence of very low to moderate quality but are consistent with the findings of other reviews and with clinical practice guidelines in concluding that exercise is not recommended for those with acute or subacute low back pain. It is unclear whether motor control exercise can prevent recurrences of low back pain because available evidence is of very low quality. Future studies should use adequate sample sizes and methods to focus on the role of exercise in preventing recurrence of acute back pain, and should discern ideal timing for these preventive interventions.
Acknowledgements
The authors would like to thank institutions providing funding to the authors of this review. Dr Luciana G Macedo is supported by the Canadian Institutes of Health Research and the Alberta Innovates Health Solutions. Professor Chris Maher is supported by a National Health and Medical Research Council Fellowship. Bruno T Saragiotto is supported by CNPQ (Conselho Nacional de Desenvolvimento Científico e Tecnológico), in Brazil, and Tiê P Yamato is supported by CAPES (Coordenacção de Aperfeiçoamento de Pessoal de Nível Superior), also in Brazil.
Appendices
Appendix 1. Database Search Strategies
MEDLINE
Last searched 2 April 2015
randomized controlled trial.pt.
controlled clinical trial.pt.
clinical trial.pt.
exp clinical trial/
Random Allocation/
Double‐Blind Method/
Single‐Blind Method/
Comparative Study/
evaluation studies/
Follow‐Up Studies/
cross‐over studies/
Research Design/
Placebos/
(clinic$ adj25 trial$).tw.
((single$ or double$ or treble$ or triple$) adj (mask$ or blind$)).tw.
(control$ or prospective$ or volunteer$).tw.
(latin adj square).tw.
placebo$.tw.
random$.tw.
or/1‐19
(animals not (humans and animals)).sh.
20 not 21
dorsalgia.ti,ab.
exp Back Pain/
backache.ti,ab.
(lumbar adj pain).ti,ab.
coccyx.ti,ab.
coccydynia.ti,ab.
sciatica.ti,ab.
exp sciatic neuropathy/
spondylosis.ti,ab.
lumbago.ti,ab.
low back pain.mp.
or/23‐33
22 and 34
exp Exercise/
exercise$.mp.
train$.mp.
36 or 37 or 38
specific.mp.
stabili$.mp.
segment$.mp.
multifidus.mp.
transversus.mp.
motor control.mp.
or/40‐45
39 and 46
35 and 47
limit 48 to yr=2014‐2015
limit 48 to ed=20140516‐20150402
49 or 50
MEDLINE In‐Process & Other Non‐Indexed Citations
Searched 2 April 2015
randomized controlled trial.pt.
controlled clinical trial.pt.
clinical trial.pt.
exp clinical trial/
Random Allocation/
Double‐Blind Method/
Single‐Blind Method/
Comparative Study/
evaluation studies/
Follow‐Up Studies/
cross‐over studies/
Research Design/
Placebos/
(clinic$ adj25 trial$).tw.
((single$ or double$ or treble$ or triple$) adj (mask$ or blind$)).tw.
(control$ or prospective$ or volunteer$).tw.
(latin adj square).tw.
placebo$.tw.
random$.tw.
or/1‐19
(animals not (humans and animals)).sh.
20 not 21
dorsalgia.ti,ab.
exp Back Pain/
backache.ti,ab.
(lumbar adj pain).ti,ab.
coccyx.ti,ab.
coccydynia.ti,ab.
sciatica.ti,ab.
exp sciatic neuropathy/
spondylosis.ti,ab.
lumbago.ti,ab.
low back pain.mp.
or/23‐33
22 and 34
exp Exercise/
exercise$.mp.
train$.mp.
36 or 37 or 38
specific.mp.
stabili$.mp.
segment$.mp.
multifidus.mp.
transversus.mp.
motor control.mp.
or/40‐45
39 and 46
35 and 47
EMBASE
Last searched 2 April 2015
randomi#ed controlled trial.mp.
clinical trial/
double blind.mp.
single blind.mp.
placebo/
Controlled Study/
Randomized Controlled Trial/
Double Blind Procedure/
Single Blind Procedure/
crossover procedure/
random$.mp.
((singl$ or doubl$ or trebl$ or tripl$) adj25 (blind$ or mask$)).mp.
(versus or vs).mp.
(clinic$ adj2 trial$).tw.
or/1‐14
limit 15 to human
dorsalgia.mp.
back pain.mp.
exp BACKACHE/
(lumbar adj pain).mp.
coccyx.mp.
coccydynia.mp.
sciatica.mp.
exp ISCHIALGIA/
spondylosis.mp.
lumbago.mp.
low back pain.mp.
or/17‐27
16 and 28
exp exercise/
exercise$.mp.
train$.mp.
30 or 31 or 32
motor control.mp.
stabili$.mp.
segment$.mp.
multifidus.mp.
transversus.mp.
or/34‐38
33 and 39
29 and 40
limit 41 to yr=2014‐2015
limit 41 to em=201419‐201513
42 or 43
CENTRAL
Last searched 2 April 2015
#1 MeSH descriptor: [Back Pain] explode all trees
#2 dorsalgia
#3 backache
#4 MeSH descriptor: [Low Back Pain] explode all trees
#5 lumbar next pain OR coccyx OR coccydynia OR sciatica OR spondylosis
#6 MeSH descriptor: [Sciatica] explode all trees
#7 MeSH descriptor: [Spine] explode all trees
#8 MeSH descriptor: [Spinal Diseases] explode all trees
#9 lumbago OR discitis OR disc near degeneration OR disc near prolapse OR disc near herniation
#10 spinal fusion
#11 spinal neoplasms
#12 facet near joints
#13 MeSH descriptor: [Intervertebral Disk] explode all trees
#14 postlaminectomy
#15 arachnoiditis
#16 failed near back
#17 MeSH descriptor: [Cauda Equina] explode all trees
#18 lumbar near vertebra*
#19 spinal near stenosis
#20 slipped near (disc* or disk*)
#21 degenerat* near (disc* or disk*)
#22 stenosis near (spine or root or spinal)
#23 displace* near (disc* or disk*)
#24 prolap* near (disc* or disk*)
#25 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12 or #13 or #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24
#26 MeSH descriptor: [Exercise] explode all trees
#27 exercis*
#28 train*
#29 #26 or #27 or #28
#30 motor control
#31 transversus
#32 multifidus
#33 segment*
#34 stabili*
#35 #31 or #32 or #33 or #34
#36 #25 and #29 and #35 Publication Year from 2014 to 2015, in Trials
CINAHL
Last searched 2 April 2015
S62 S61 Limiters ‐ Published Date: 20130501‐20150431
S61 S49 AND S56 AND S60
S60 S57 OR S58 OR S59
S59 "train*"
S58 "exercise*"
S57 (MH "Exercise+")
S56 S50 OR S51 OR S52 OR S53 OR S54 OR S55
S55 specific W2 stabili?ation
S54 "stabili?ation"
S53 "multifidus"
S52 (MH "Multifidus Muscles")
S51 "transversus"
S50 "motor control"
S49 S28 and S48
S48 S35 or S43 or S47
S47 S44 or S45 or S46
S46 "lumbago" 33
S45 (MH "Spondylolisthesis") OR (MH "Spondylolysis")
S44 (MH "Thoracic Vertebrae")
S43 S36 or S37 or S38 or S39 or S40 or S41 or S42
S42 lumbar N2 vertebra
S41 (MH "Lumbar Vertebrae")
S40 "coccydynia"
S39 "coccyx"
S38 "sciatica"
S37 (MH "Sciatica")
S36 (MH "Coccyx")
S35 S29 or S30 or S31 or S32 or S33 or S34
S34 lumbar N5 pain
S33 lumbar W1 pain 282
S32 "backache"
S31 (MH "Low Back Pain")
S30 (MH "Back Pain+")
S29 "dorsalgia"
S28 S26 NOT S27
S27 (MH "Animals")
S26 S7 or S12 or S19 or S25
S25 S20 or S21 or S22 or S23 or S24
S24 volunteer*
S23 prospectiv*
S22 control*
S21 followup stud*
S20 follow‐up stud*
S19 S13 or S14 or S15 or S16 or S17 or S18
S18 (MH "Prospective Studies+")
S17 (MH "Evaluation Research+")
S16 (MH "Comparative Studies")
S15 latin square
S14 (MH "Study Design+")
S13 (MH "Random Sample")
S12 S8 or S9 or S10 or S11
S11 random*
S10 placebo*
S9 (MH "Placebos")
S8 (MH "Placebo Effect")
S7 S1 or S2 or S3 or S4 or S5 or S6
S6 triple‐blind 94
S5 single‐blind 6,829
S4 double‐blind 24,437
S3 clinical W3 trial 14,324
S2 "randomi?ed controlled trial*"
S1 (MH "Clinical Trials+")
AMED
Last searched 2 April 2015
randomized controlled trial.pt.
controlled clinical trial.pt.
clinical trial.pt.
exp clinical trials/
random allocation/
double blind method/
single blind method/
comparative study/
follow up studies/
research design/
placebos/
(clinic$ adj25 trial$).tw.
((single$ or double$ or treble$ or triple$) adj (mask$ or blind$)).tw.
(control$ or prospective$ or volunteer$).tw.
(latin adj square).tw.
placebo$.tw.
random$.tw.
or/1‐17
(animals not (humans and animals)).sh.
18 not 19
dorsalgia.mp.
exp backache/
sciatica/
(lumbar adj pain).ti,ab.
sciatica.mp.
spondylosis.mp.
coccyx.mp.
lumbago.mp.
low back pain.mp.
or/21‐29
20 and 30
exercise/
exercise$.mp.
train$.mp.
or/32‐34
specific.mp.
stabili$.mp. [mp=abstract, heading words, title]
segment$.mp.
multifidus.mp.
transversus.mp.
motor control.mp.
or/36‐41
35 and 42
31 and 43
limit 44 to yr=2014‐2015
SportDiscus
Last searched 2 April 2015
S28 S27 Limiters ‐ Published Date: 20140501‐20150431
S27 S16 AND S20 AND S26
S26 S21 OR S22 OR S23 OR S24 OR S25
S25 specific W2 stabili?ation
S24 stabili?ation
S23 multifidus
S22 transversus
S21 motor control
S20 S17 OR S18 OR S19
S19 train*
S18 exercise*
S17 DE "EXERCISE" or DE "BACK exercises" or DE "EXERCISE therapy" or DE "PHYSICAL education & training" or DE "PHYSICAL fitness"
S16 S10 AND S15
S15 S11 OR S12 OR S13 OR S14
S14 DE "LUMBAR vertebrae" or DE "LUMBOSACRAL region"
S13 DE "SCIATICA"
S12 low back pain
S11 DE "BACKACHE"
S10 S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 OR S9
S9 single blind
S8 random allocation
S7 SU randomized controlled trial
S6 SU clinical trials
S5 clinical trials
S4 placebo
S3 controlled clinical trial
S2 double blind
S1 randomi?ed controlled trial
PEDro
Last searched 2 April 2015
Abstract & Title: Exercise
AND
Problem: pain
AND
Body Part: lumbar spine, sacro‐iliac joint or pelvis
AND
Method: clinical trial
New records added since: 15/05/2014
LILACS
Last searched 2 April 2015
back pain AND exercise, all indexes on the homepage
Filter: Type of study: clinical Trial OR guidelines
dor lombar AND exercicio, all indexes on the homepage
Filter: Type of study: clinical trial OR guidelines
ClinicalTrials.gov
Last searched 2 April 2015
Condition: back pain
Intervention: exercise
received on or after 05/15/2014
WHO ICTRP
Last searched 2 April 2015
Condition: back pain
Intervention: exercise
Date of registration is between 15/05/2014‐02/04/2015
PubMed
Searched 2 April 2015
((dorsalgia OR back pain OR backache OR lumbar pain OR coccydynia OR sciatica OR lumbago OR spondylosis) AND ((exercise* OR train*) AND (specific* OR stabili* OR segment* OR multifidus OR transverses OR motor control)) AND (pubstatusaheadofprint OR publisher[sb] or pubmednotmedline[sb]))
From 2014/05/01 to 2015/12/31
Appendix 2. Risk of bias criteria
Random sequence generation (selection bias)
Selection bias (biased allocation to interventions) due to inadequate generation of a randomized sequence
Risk of selection bias is low if investigators describe a random component in the sequence generation process such as referring to a random number table, using a computer random number generator, tossing a coin, shuffling cards or envelopes, throwing dice, drawing lots and minimisation (minimisation may be implemented without a random element; this is considered equivalent to being random).
Risk of selection bias is high if investigators describe a non‐random component in the sequence generation process such as sequence generation by odd or even date of birth, date (or day) of admission or hospital or clinic record number; or allocation by judgement of the clinician, preference of the participant, results of a laboratory test or a series of tests or availability of the intervention.
Allocation concealment (selection bias)
Selection bias (biased allocation to interventions) due to inadequate concealment of allocations before assignment
Risk of selection bias is low if participants and investigators enrolling participants could not foresee assignment because one of the following, or an equivalent method, was used to conceal allocation: central allocation (including telephone, Web‐based and pharmacy‐controlled randomisation); sequentially numbered drug containers of identical appearance; or sequentially numbered, opaque, sealed envelopes.
Risk of bias is high if participants or investigators enrolling participants could possibly foresee assignments and thus introduce selection bias such as allocation based on using an open random allocation schedule (e.g. a list of random numbers); using assignment envelopes without appropriate safeguards (e.g. envelopes were unsealed or non‐opaque or were not sequentially numbered), alternation or rotation, date of birth, case record number or other explicitly unconcealed procedures.
Blinding of participants
Performance bias due to knowledge of allocated interventions by participants during the study
Risk of performance bias is low if blinding of participants was ensured and it was unlikely that blinding could have been broken; or if no blinding or incomplete blinding was provided but review authors judged that the outcome is not likely to be influenced by lack of blinding.
Blinding of personnel/care providers (performance bias)
Performance bias due to knowledge of allocated interventions by personnel/care providers during the study
Risk of performance bias is low if blinding of personnel was ensured and it was unlikely that blinding could have been broken; or if no blinding or incomplete blinding was provided but review authors judged that the outcome is not likely to be influenced by lack of blinding.
Blinding of outcome assessors (detection bias)
Detection bias due to knowledge of allocated interventions by outcome assessors
Risk of detection bias is low if blinding of the outcome assessment was ensured and it was unlikely that blinding could have been broken; or if no blinding or incomplete blinding was provided but review authors judged that the outcome is not likely to be influenced by lack of blinding, or:
for patient‐reported outcomes in which the patient was the outcome assessor (e.g. pain, disability): low risk of bias for outcome assessors if low risk of bias for participant blinding (Boutron 2005);
for outcome criteria that are clinical or therapeutic events that will be determined by the interaction between patients and care providers (e.g. co‐interventions, length of hospitalisation, treatment failure), in which the care provider is the outcome assessor: low risk of bias for outcome assessors if low risk of bias for care providers (Boutron 2005); and
for outcome criteria that are assessed from data from medical forms: low risk of bias if treatment or adverse effects of treatment could not be noticed in the extracted data (Boutron 2005).
Incomplete outcome data (attrition bias)
Attrition bias due to amount, nature or handling of incomplete outcome data
Risk of attrition bias is low if no outcome data were missing; reasons for missing outcome data were unlikely to be related to the true outcome (for survival data, censoring unlikely to be introducing bias); missing outcome data were balanced in numbers, with similar reasons for missing data across groups; for dichotomous outcome data, the proportion of missing outcomes compared with the observed event risk was not enough to have a clinically relevant impact on the intervention effect estimate; for continuous outcome data, the plausible effect size (difference in means or standardised difference in means) among missing outcomes was not enough to have a clinically relevant impact on observed effect size or missing data were imputed using appropriate methods (if dropouts were very large, imputation using even 'acceptable' methods may still suggest high risk of bias) (van Tulder 2003). Percentages of withdrawals and dropouts should not exceed 20% for short‐term follow‐up and 30% for long‐term follow‐up, and should not lead to substantial bias (these percentages are commonly used but arbitrary and are not supported by the literature) (van Tulder 2003).
Selective reporting (reporting bias)
Reporting bias due to selective outcome reporting
Risk of reporting bias is low if the study protocol is available and all of the study's prespecified (primary and secondary) outcomes that are of interest in the review have been reported in the prespecified way, or if the study protocol is not available but published reports clearly include all expected outcomes, including those that were prespecified (convincing text of this nature may be uncommon).
Risk of reporting bias is high if not all of the study's prespecified primary outcomes have been reported; one or more primary outcomes was reported using measurements, analysis methods or subsets of the data (e.g. subscales) that were not prespecified; one or more reported primary outcomes were not prespecified (unless clear justification for their reporting is provided, such as an unexpected adverse effect); one or more outcomes of interest in the review are reported incompletely so that they cannot be entered in a meta‐analysis; or the study report fails to include results for a key outcome that would be expected to have been reported for such a study.
Group similarity at baseline (selection bias)
Bias due to dissimilarity at baseline for the most important prognostic indicators
Risk of bias is low if groups are similar at baseline for demographic factors, values of main outcome measure(s) and important prognostic factors (examples in the field of back and neck pain include duration and severity of complaints, vocational status, percentage of patients with neurological symptoms) (van Tulder 2003).
Co‐interventions (performance bias)
Bias due to differences in co‐interventions across groups
Risk of bias is low if no co‐interventions were provided, or if interventions were similar between index and control groups (van Tulder 2003).
Compliance (performance bias)
Bias due to inappropriate compliance with interventions across groups
Risk of bias is low if compliance with the interventions was acceptable on the basis of reported intensity/dosage, duration, number and frequency for both index and control intervention(s). For single‐session interventions (e.g. surgery), this item is irrelevant (van Tulder 2003).
Intention‐to‐treat analysis
Risk of bias is low if all randomly assigned participants were reported/analysed in the groups to which they were allocated by randomisation.
Timing of outcome assessments (detection bias)
Bias due to different timing of important outcomes measurements across groups
Risk of bias is low if all important outcome assessments for all intervention groups were measured at the same time (van Tulder 2003).
Other bias
Bias due to problems not covered elsewhere in the table
Risk of bias is low if the study appears to be free of other sources of bias not addressed elsewhere (e.g. study funding).
Data and analyses
Comparison 1. Motor control exercise vs spinal manipulative therapy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Short term | 1 | 58 | Mean Difference (IV, Random, 95% CI) | 9.0 [‐1.56, 19.56] |
| 2 Disability | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Short term | 1 | 85 | Mean Difference (IV, Random, 95% CI) | 4.0 [‐3.38, 11.38] |
| 2.2 Long term | 1 | 85 | Mean Difference (IV, Random, 95% CI) | 3.70 [‐4.10, 11.50] |
1.1. Analysis.
Comparison 1 Motor control exercise vs spinal manipulative therapy, Outcome 1 Pain.
1.2. Analysis.
Comparison 1 Motor control exercise vs spinal manipulative therapy, Outcome 2 Disability.
Comparison 2. Motor control exercise vs other exercises.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Short term | 2 | 89 | Mean Difference (IV, Random, 95% CI) | 5.74 [‐3.34, 14.82] |
| 1.2 Intermediate term | 1 | 33 | Mean Difference (IV, Random, 95% CI) | ‐1.20 [‐18.24, 15.84] |
| 2 Disability | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Short term | 2 | 116 | Mean Difference (IV, Random, 95% CI) | ‐0.84 [‐8.72, 7.04] |
| 2.2 Intermediate term | 1 | 33 | Mean Difference (IV, Random, 95% CI) | ‐6.70 [‐22.80, 9.40] |
| 2.3 Long term | 1 | 83 | Mean Difference (IV, Random, 95% CI) | 5.70 [‐1.38, 12.78] |
2.1. Analysis.
Comparison 2 Motor control exercise vs other exercises, Outcome 1 Pain.
2.2. Analysis.
Comparison 2 Motor control exercise vs other exercises, Outcome 2 Disability.
Comparison 3. Motor control exercise as a supplement to medical management.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pain | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Short term | 1 | 41 | Mean Difference (IV, Random, 95% CI) | ‐9.3 [‐20.41, 1.81] |
| 2 Disability | 1 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Short term | 1 | 41 | Mean Difference (IV, Random, 95% CI) | ‐2.4 [‐4.87, 0.07] |
| 3 Recurrence | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 3.1 Long term | 1 | 39 | Risk Ratio (M‐H, Random, 95% CI) | 0.36 [0.18, 0.72] |
3.1. Analysis.
Comparison 3 Motor control exercise as a supplement to medical management, Outcome 1 Pain.
3.2. Analysis.
Comparison 3 Motor control exercise as a supplement to medical management, Outcome 2 Disability.
3.3. Analysis.
Comparison 3 Motor control exercise as a supplement to medical management, Outcome 3 Recurrence.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Aluko 2013.
| Methods | Randomised controlled trial | |
| Participants | 33 participants were recruited between July 2008 and June 2010 from within a primary care musculoskeletal physiotherapy service in the London borough of Hillingdon Participants were excluded if they demonstrated evidence of any of the following: degenerative conditions affecting the spine, diabetes, pregnancy, underlying neurological conditions, active treatment of an ongoing spinal condition, active legal/compensation procedures, a history of depression, a history of multiple recurrent episodes of LBP and involvement in other research studies. Participants for whom English was not their primary language were also excluded |
|
| Interventions | All patients referred for treatment of non‐specific low back pain within physiotherapy service providers were assessed and subsequently offered a place in a “core stability” class consisting of both specific and global trunk exercises. Participants in both groups received this protocol as minimum intervention. The intervention group received further instruction on 8 specific exercises for stabilisation of muscles involving the transversus abdominis (TrA) and the lumbar multifidus (LM) Core stability exercises (CSEs): Selection of exercises used in this study therefore relied on current belief systems, suggesting that isolation of TrA and LM is important for trunk stability. These exercises included the following: abdominal hollowing in prone lying, alternate straight‐leg raise in supine, abdominal hollowing in sitting, Crook lying–alternate heel slide, 4‐point kneeling pelvic shift (side to side), trunk curl in crook lying, pelvic tilt in sitting and alternate knee raise in sitting. Exercises met suggested criteria for safety, including avoidance of active hip flexion with fixed positioning of feet and pulling with the hands behind the head, while ensuring knee and hip flexion during all upper body exercises. Intervention group participants were required to perform 10 repetitions of each of the above exercises 3 times a day. To facilitate compliance, participants were required to complete a compliance diary. The diary method was chosen to avoid adding to participants' perceived barriers to exercise by impinging on available time to do the exercise routine |
|
| Outcomes | Pain: assessed by a VAS comprising a 100‐mm line with no numbers Disability: assessed by the Roland Morris Disability Questionnaire Both outcomes were measured at the start of the study and at 3, 6 and 12 weeks subsequently |
|
| Notes | No funding sources or conflicts of interest were reported for this study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The randomization was done by a colleague independent and blind to the study using concealed envelopes within which the group description was randomly placed within them. The envelopes were numbered sequentially and chosen by the participants in the order in which they were recruited" |
| Allocation concealment (selection bias) | Low risk | "The randomization was done by a colleague independent and blind to the study using concealed envelopes within which the group description was randomly placed within them. The envelopes were numbered sequentially and chosen by the participants in the order in which they were recruited" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Although the participants were randomly allocated as they were recruited and blinded to the study, it was not possible to blind the assessment process" |
| Blinding of personnal/care provider (performance bias) All outcomes | High risk | Care provider was not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | "Data were collected by the researcher who was therefore not blinded to the grouping of any of the participants" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not described |
| Intention‐to‐treat analysis | High risk | Not considered. "An intention‐to‐treat analysis was used with missing data replaced with the Last Observation Carried Forward for incomplete data sets". |
| Selective reporting (reporting bias) | Low risk | Published report clearly included all expected outcomes |
| Group similarity of baseline (selection bias) | Low risk | Participants did not differ in baseline characteristics, as shown in Table 2 |
| Co‐interventions (performance bias) | Unclear risk | Not described |
| Compliance (performance bias) | Unclear risk | Not described |
| Timing of outcome assessment (detection bias) | Low risk | All important outcomes assessments for both groups were measured at the same time |
Brennan 2006.
| Methods | Randomised controlled trial | |
| Participants | 123 participants. Primary recruitment occurred at a single clinic between January 1, 2000, and July 1, 2003. Additional recruitment occurred at 2 other clinics between January 1, 2002, and September 1, 2002. Each clinic was located in Utah and was affiliated with Intermountain Health Care System Inclusion criteria: Patients between 18 and 65 years of age with a primary complaint of LBP of less than 90 days' duration, with or without referral into the lower extremity, and an Oswestry Disability score of 25% were eligible Exclusion criteria: visible lateral shift or acute kyphotic deformity, signs of nerve root compression (positive straight‐leg raise test and reflex or strength deficits), any red flags indicating serious pathology such as spinal neoplasm, infection or fracture, inability to reproduce any symptoms with lumbar spine active range of motion (AROM) or palpation, current pregnancy, prior surgery to the lumbar and/or sacral region |
|
| Interventions | All participants were scheduled for treatment twice weekly for 4 weeks for a maximum of 8 sessions Manipulation treatment group: Participants randomly assigned to the manipulation group were treated via manual therapy techniques, which could include thrust manipulation, or by low‐amplitude mobilisation procedures directed to the lumbosacral region, and were given instruction on a lumbar active range of motion exercise. The therapist providing treatment was permitted to reexamine the participant and could choose 1 of 2 manual therapy techniques. The decision on which technique to use was left to the therapist's discretion, but 1 of the 2 techniques had to be used. With the first technique, the participant was supine, with the lumbar spine placed into side‐bending and rotation to the opposite direction. The therapist delivered a force through the participant's pelvis in a posterior and inferior direction. For the second technique, the participant was side‐lying. The lumbar spine was positioned in flexion or extension followed by rotation in an attempt to isolate forces to a particular spinal level. The therapist delivered the force through the participant's pelvis and trunk. Selection of technique was left to the discretion of the therapist. AROM exercise was performed by instructing the participant to alternately flex and extend the lumbar spine while in a quadruped position. Specific exercise treatment group: Participants in the specific exercise group received instruction on repeated range of motion (ROM) exercises into lumbar flexion or extension. All participants in this group had to be treated using directional exercises; however, the direction of the exercise was determined by the treating therapist on the basis of reassessment of the participant's response to movement testing and symptom response to the position of sitting, standing or walking. Flexion exercises were used for participants who centralised with or had a preference for flexion movements or positions (i.e. sitting), whereas extension exercises were used for participants who centralised or had a preference for extension (i.e. standing or walking). Flexion or extension exercises were used, but not both. Flexion exercises were performed with the participant sitting, supine or quadruped. Extension exercises were performed in prone, while using prone on elbows or prone press‐up activities Stabilisation treatment group: Participants in the stabilisation group were treated with a programme of trunk strengthening and stabilisation exercises. Participants were instructed to perform abdominal bracing exercises in supine and quadruped positions, progressing to more functional positions and activities as described by Richardson and Jull. Participants were also instructed on alternating arm and leg extension exercises in quadruped to strengthen the lumbar extensor muscles. Strengthening for the oblique abdominals included curl‐up and side support exercises |
|
| Outcomes | Pain: 11‐point rating scale (0 no pain to 10 worst imaginable pain) to assess current pain intensity Disability: Modified Oswestry Questionnaire (OSW) to assess disability related to LBP |
|
| Notes | Supported by a research grant from the Deseret Foundation. Foundation funds were received in support of this work. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the topic of this study | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "A random number generator was used to generate a randomization list before initiation of the study. The list was maintained by the secretarial staff of the participating clinics" |
| Allocation concealment (selection bias) | Unclear risk | Sequence generation procedure or method of allocation was not mentioned |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No mention of any attempts to blind participants |
| Blinding of personnal/care provider (performance bias) All outcomes | High risk | No mention of any attempts to blind care provider |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | "Baseline and follow‐up examinations were conducted by a physical therapist who remained blind to the treatment group assignment"; outcome measures were self reported, thus, assessor was not considered blinded |
| Incomplete outcome data (attrition bias) All outcomes | High risk | "Eighty one patients (66%) completed the long‐term follow‐up, with no differences in the median number of days between baseline and follow‐up or the proportions of patients with completed follow‐up between patients receiving matched or unmatched treatments" |
| Intention‐to‐treat analysis | Low risk | "Analysis was performed using intention‐to‐treat principles, with the last available OSW score carried forward for any missing data" |
| Selective reporting (reporting bias) | Low risk | Published report clearly included all expected outcomes |
| Group similarity of baseline (selection bias) | Low risk | Participants did not differ in baseline characteristics, as presented in Table 1, and no differences were found in additional data provided by study authors |
| Co‐interventions (performance bias) | Unclear risk | Not described |
| Compliance (performance bias) | Low risk | Compliance was acceptable on the basis of reported intensity/dosage, duration, number and frequency for all 3 groups |
| Timing of outcome assessment (detection bias) | Low risk | All important outcomes assessments for both groups were measured at the same time |
Hides 1996.
| Methods | Randomised controlled trial | |
| Participants | 41 patients recruited from an accident and emergency department at a hospital over a 6‐month period Inclusion criteria: Men and women were eligible for the study in the first instance if they were 18 to 45 years of age and were experiencing their first episode of unilateral, mechanical LBP for less than 3 weeks Exclusion criteria: previous history of LBP or injury, previous lumbar surgery, spinal abnormalities indicated on radiographs, neuromuscular or joint disease, reflex and/or motor signs of nerve root compression or cauda equina compression, evidence of systemic disease, carcinoma or organ disease, pregnancy, any sports or fitness training involving the low back muscles done in the past 3 months |
|
| Interventions | Medical management group: advice on bed rest and absence from work and prescription of medication. Minimal bed rest (1 to 3 days) and only minor analgesics were prescribed. These analgesics included aspirin, paracetamol, combinations of low doses of codeine and aspirin, non‐steroidal anti‐inflammatory agents, Digestics and Capadex. Prescription of Valium was also allowable Exercise therapy: Therapeutic exercises were designed to re‐educate the multifidus muscle in its stabilising role. They involved facilitating an active, isometric multifidus contraction in co‐contraction with deep abdominal muscles. Participants performed the contraction in the standing position with the lumbar spine in a neutral position. Contraction of the multifidus was confirmed by real‐time ultrasound imaging |
|
| Outcomes | Pain: McGill Pain Questionnaire and visual analogue scales Disability: Roland Morris Disability Index |
|
| Notes | Financial support from The Menzies Foundation, The JP Kelly Mater Research Foundation, The Wenkart Foundation, The Physiotherapy Research Foundation and the Manual Therapy Special Group (Australia) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Random assignment to the control or treatment group was achieved by selecting the group number from sealed, shuffled envelopes" |
| Allocation concealment (selection bias) | Low risk | "Random assignment to the control or treatment group was achieved by selecting the group number from sealed, shuffled envelopes" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No mention of any attempts to blind participants |
| Blinding of personnal/care provider (performance bias) All outcomes | High risk | No mention of any attempts to blind care provider |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | "Assessments were performed by two independent examiners, who were blinded to group allocation and patient presentation"; outcome measures were self reported, thus, assessor was not considered blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Percentages of withdrawals and dropouts were within the acceptable rate |
| Intention‐to‐treat analysis | Unclear risk | Not described |
| Selective reporting (reporting bias) | Low risk | Published report clearly included all expected outcomes |
| Group similarity of baseline (selection bias) | High risk | Groups were not similar at baseline regarding outcome disability |
| Co‐interventions (performance bias) | Unclear risk | Not described |
| Compliance (performance bias) | Unclear risk | Not described |
| Timing of outcome assessment (detection bias) | Low risk | All important outcomes assessments for both groups were measured at the same time |
AROM: active range of motion.
CSE: core stability exercise.
LBP: low back pain.
LM: lumbar multifidus.
OSW: Modified Oswestry Questionnaire.
ROM: range of motion.
TrA: transversus abdominis
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Aasa 2015 | No MCE and no mixed intervention |
| ACTRN12609000293268 | No MCE and no mixed intervention |
| ACTRN12609000334202 | No MCE and no mixed intervention |
| ACTRN12609000343202 | Chronic LBP |
| ACTRN12611000971932 | Chronic LBP |
| Aggarwal 2010 | No patients with non‐specific LBP |
| Ahmed 2014 | All groups given MCE |
| Akbari 2008 | Chronic LBP |
| Ali 2006 | No MCE and no mixed intervention |
| Allison 2012 | Not an RCT |
| Alp 2011 | Chronic LBP |
| Alp 2014 | Chronic LBP |
| Ammar 2011 | No MCE and no mixed intervention |
| Andrusaitis 2011 | No MCE and no mixed intervention |
| Appling 2009 | Not an RCT |
| Areeudomwong 2012 | Chronic LBP |
| Barbosa 2013 | Not an RCT |
| Bayraktar 2013 | Chronic LBP |
| Belcher 1998 | No patients with non‐specific LBP |
| Bentsen 1997 | No MCE and no mixed intervention |
| Bi 2013 | No MCE and no mixed intervention |
| Bilgin 2013 | No patients with non‐specific LBP |
| Bordiak 2012 | No patients with non‐specific LBP |
| Bronfort 1996 | No MCE and no mixed intervention |
| Bronfort 2011 | No MCE and no mixed intervention |
| Brooks 2012 | No MCE and no mixed intervention |
| Brox 2003 | No MCE and no mixed intervention |
| Buchbinder 2002 | Not an RCT |
| Byuon 2012 | No MCE and no mixed intervention |
| Cairns 2003 | No MCE and no mixed intervention |
| Cairns 2006 | Chronic LBP |
| Carmo 2013 | Chronic LBP |
| Chan 2011 | No MCE and no mixed intervention |
| Childs 2009 | No patients with non‐specific LBP |
| Childs 2010 | No patients with non‐specific LBP |
| Cho 2014 | No MCE and no mixed intervention |
| Chung 2013 | No MCE and no mixed intervention |
| Costa 2009 | Chronic LBP |
| Critchley 2007 | Chronic LBP |
| Croft 1999 | Not an RCT |
| Dehner 2009 | Not an RCT |
| Descarreaux 2002 | No MCE and no mixed intervention |
| Donzelli 2006 | No MCE and no mixed intervention |
| Dufour 2010 | No MCE and no mixed intervention |
| Durante 2010 | No MCE and no mixed intervention |
| Dvorak 2011 | No MCE and no mixed intervention |
| Earde 2014 | No evaluation of relevant outcomes for this review |
| Ewert 2009 | No patients with non‐specific LBP |
| Faas 1993 | No MCE and no mixed intervention |
| Faas 1995 | No MCE and no mixed intervention |
| Ferreira 2007 | Chronic LBP |
| Franca 2010 | Chronic LBP |
| Franca 2012 | Chronic LBP |
| Freitas 2008 | No MCE and no mixed intervention |
| Gagnon 2005 | No MCE and no mixed intervention |
| Gatti 2011 | No MCE and no mixed intervention |
| George 2011 | No patients with non‐specific LBP |
| Goldby 2006 | Chronic LBP |
| Gustafsson 2008 | Not an RCT |
| Guven 2003 | No patients with non‐specific LBP |
| Hagen 2010 | No MCE and no mixed intervention |
| Hansen 1993 | No MCE and no mixed intervention |
| Harkapaa 1989 | No MCE and no mixed intervention |
| Harringe 2007 | Not an RCT |
| Harts 2008 | No MCE and no mixed intervention |
| Helewa 1999 | No MCE and no mixed intervention |
| Helmhout 2004 | No MCE and no mixed intervention |
| Hemmati 2011 | Chronic LBP |
| Henchoz 2010 | No MCE and no mixed intervention |
| Hides 2008 | Not an RCT |
| Hosseinifar 2013 | Chronic LBP |
| Hunter 2012 | No MCE and no mixed intervention |
| Hurwitz 2005 | Not an RCT |
| Hwang 2013 | No MCE and no mixed intervention |
| Inani 2013 | Chronic LBP |
| ISRCTN80064281 | No MCE and no mixed intervention |
| Jang 2013 | No MCE and no mixed intervention |
| Javadian 2012 | Chronic LBP |
| Javadian 2015 | No evaluation of relevant outcomes for this review |
| Johannsen 1995 | No MCE and no mixed intervention |
| Johnson 2007 | No MCE and no mixed intervention |
| Jones 2007 | No MCE and no mixed intervention |
| Kaapa 2006 | No MCE and no mixed intervention |
| Kachanathu 2012 | Chronic LBP |
| Karimi 2009 | Not an RCT |
| Kladny 2003 | No patients with non‐specific LBP |
| Kline 2013 | No MCE and no mixed intervention |
| Kofotolis 2008 | No MCE and no mixed intervention |
| Koldas 2008 | No MCE and no mixed intervention |
| Koumantakis 2005 | Chronic LBP |
| Kumar 2009 | Chronic LBP |
| Kumar 2010 | Chronic LBP |
| Kumar 2011 | No MCE and no mixed intervention |
| Kumar 2012 | Not an RCT |
| Kuukkanen 1996 | Not an RCT |
| Lee 2015 | No patients with non‐specific LBP |
| Lewis 2005 | All groups given MCE |
| Lie 1999 | No MCE and no mixed intervention |
| Lomond 2015 | Chronic LBP |
| Long 2004 | No MCE and no mixed intervention |
| Macedo 2008 | Chronic LBP |
| Macedo 2012 | Chronic LBP |
| Magalhaes 2013 | Protocol |
| Magnusson 2008 | Not an RCT |
| Maher 2005 | Chronic LBP |
| Mannion 1999 | No MCE and no mixed intervention |
| Mannion 2009 | Not an RCT |
| Mannion 2012 | Not an RCT |
| Marshall 2008 | No MCE and no mixed intervention |
| Meira 2013 | Chronic LBP |
| Miller 2005 | Chronic LBP |
| Mohseni‐Bandpei 2011 | No MCE and no mixed intervention |
| Monteiro 2009 | Not an RCT |
| Monticone 2004 | No patients with non‐specific LBP |
| Moon 2013 | Chronic LBP |
| Moseley 2002 | No MCE and no mixed intervention |
| Moseley 2003 | All groups given MCE |
| Moussouli 2014 | Not an RCT |
| Navalgund 2009 | Not an RCT |
| NCT00201513 | Chronic LBP |
| NCT00555802 | Chronic LBP |
| NCT00624533 | No MCE and no mixed intervention |
| NCT01061632 | All groups given MCE |
| NCT01124201 | Chronic LBP |
| NCT01362049 | Chronic LBP |
| NCT02112760 | Chronic LBP |
| NCT02170753 | Chronic LBP |
| NCT02200913 | Chronic LBP |
| NCT02221609 | Chronic LBP |
| NCT02374970 | Chronic LBP |
| NCT02398760 | Chronic LBP |
| Nelson 1995 | No MCE and no mixed intervention |
| Nelson‐Wong 2009 | Not an RCT |
| Niemisto 2003 | No MCE and no mixed intervention |
| Niemisto 2004 | No MCE and no mixed intervention |
| Niemisto 2005 | No MCE and no mixed intervention |
| Norris 2008 | Not an RCT |
| O'Sullivan 1997 | No patients with non‐specific LBP |
| Oguzhan 2011 | No MCE and no mixed intervention |
| Ota 2011 | Not an RCT |
| Pereira 2010 | Not an RCT |
| Puntumetakul 2013 | Chronic LBP |
| Rabin 2014 | Chronic LBP |
| Rasmussen‐Barr 2003 | Chronic LBP |
| Rasmussen‐Barr 2009 | Chronic LBP |
| Rhee 2012 | Chronic LBP |
| Riipinen 2005 | No MCE and no mixed intervention |
| Rydeard 2006 | No MCE and no mixed intervention |
| Saner 2011 | No MCE and no mixed intervention |
| Saner 2015 | No MCE and no mixed intervention |
| Shakeri 2013 | No patients with non‐specific LBP |
| Shaughnessy 2004 | Chronic LBP |
| Shnayderman 2013 | No MCE and no mixed intervention |
| Smeets 2009 | Not an RCT |
| Smith 2011 | No MCE and no mixed intervention |
| Sokunbi 2008 | Not an RCT |
| Stankovic 2012 | Chronic LBP |
| Streicher 2014 | Not an RCT |
| Stuge 2004 | No patients with non‐specific LBP |
| Suni 2006 | No MCE and no mixed intervention |
| Teyhen 2010 | No patients with non‐specific LBP |
| Torstensen 1998 | No MCE and no mixed intervention |
| Trampas 2014 | All groups given MCE |
| Tsauo 2009 | Chronic LBP |
| Unsgaard‐Tondel 2010 | Chronic LBP |
| Vasseljen 2010 | Chronic LBP |
| Vasseljen 2012 | Chronic LBP |
| Wang 2012 | No MCE and no mixed intervention |
| Willemink 2012 | No MCE and no mixed intervention |
| Williamson 2008 | No MCE and no mixed intervention |
| Xueqiang 2012 | No MCE and no mixed intervention |
| Yang 2010 | Not an RCT |
| Yelland 2004 | No MCE and no mixed intervention |
| Yoo 2012 | No MCE and no mixed intervention |
| You 2014 | No MCE and no mixed intervention |
| Zhang 2015 | No MCE and no mixed intervention |
LBP: low back pain.
MCE: motor control exercise.
RCT: randomised controlled trial.
Differences between protocol and review
No previous protocol published.
Contributions of authors
Luciana Gazzi Macedo, Bruno Tirotti Saragiotto, Leonardo Costa, Luciola Menezes Costa and Chris Maher selected all studies for inclusion. Bruno Tirotti Saragiotto and Tiê Parma Yamato assessed risk of bias of the articles and extracted and analysed study data. All other review authors contributed to writing of the protocol and writing and editing of the review.
Sources of support
Internal sources
None, Other.
External sources
None, Other.
Declarations of interest
None known.
New
References
References to studies included in this review
Aluko 2013 {published data only}
- Aluko A, DeSouza L, Peacock J. The effect of core stability exercises on variations in acceleration of trunk movement, pain, and disability during an episode of acute non specific low back pain: a pilot clinical trial. Journal of Manipulative and Physiological Therapeutics 2013;36:497. [DOI] [PubMed] [Google Scholar]
Brennan 2006 {published data only}
- Brennan GP, Fritz JM, Hunter SJ, Thackeray A, Delitto A, Erhard RE. Identifying subgroups of patients with acute/subacute nonspecific low back pain: results of a randomized clinical trial. Spine 2006;31:623‐31. [DOI] [PubMed] [Google Scholar]
Hides 1996 {published data only}
- Hides JA, Jull GA, Richardson CA. Long‐term effects of specific stabilizing exercises for first‐episode low back pain. Spine 2001;26:E243‐8. [DOI] [PubMed] [Google Scholar]
- Hides JA, Richardson CA, Jull GA. Multifidus muscle recovery is not automatic after resolution of acute, first‐episode low back pain. Spine 1996;21:2763‐9. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Aasa 2015 {published data only}
- Aasa B, Berglund L, Michaelson P, Aasa U. Individualized low‐load motor control exercises and education versus a high‐load lifting exercise and education to improve activity, pain intensity, and physical performance in patients with low back pain: a randomized controlled trial. Journal of Orthopaedic & Sports Physical Therapy 2015;45:77‐85. [DOI] [PubMed] [Google Scholar]
ACTRN12609000293268 {published data only}
- ACTRN12609000293268. Effects of advice versus physiotherapy functional restoration on pain and function for people with multi‐factorial persistent low back pain: a randomised controlled trial. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=83875 (accessed 25 June 2015).
ACTRN12609000334202 {published data only}
- ACTRN12609000334202. Effects of physiotherapy manual therapy on pain and function for people with subacute low back pain with or without leg pain: a randomised controlled trial. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12609000334202 (accessed 26 June 2015).
ACTRN12609000343202 {published data only}
- ACTRN12609000343202. Effects of specific physiotherapy treatment and advice versus advice alone on pain and function for people with sub‐acute reducible discogenic low back pain: a randomised controlled trial. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12609000343202 (accessed 25 June 2015).
ACTRN12611000971932 {published data only}
- ACTRN12611000971932. A comparison of mechanical diagnosis & therapy and motor control exercises on the thickness of the trunk muscle in patients with chronic low back pain. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12611000971932 (accessed 25 June 2015).
Aggarwal 2010 {published data only}
- Aggarwal A, Kumar S, Kumar D. Effect of core stabilization training on the lower back endurance in recreational active individuals. Journal of Musculoskeletal Research 2010;13:167‐76. [Google Scholar]
Ahmed 2014 {published data only}
- Ahmed R, Shakil‐ur‐Rehman S, Sibtain F. Comparison between specific lumber mobilization and core‐stability exercises with core‐stability exercises alone in mechanical low back pain. Pakistan Journal of Medical Sciences 2014;30:157‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Akbari 2008 {published data only}
- Akbari A, Khorashadizadeha S, Abdi G. The effect of motor control exercise versus general exercise on lumbar local stabilizing muscles thickness: randomized controlled trial of patients with chronic low back pain. Journal of Back and Musculoskeletal Rehabilitation 2008;21:105‐12. [Google Scholar]
Ali 2006 {published data only}
- Ali TA. Stabilization exercises for patients with low back pain. Dissertation.. Texas Woman's University, Denton, Texas; Texas Woman's University; 2006.
Allison 2012 {published data only}
- Allison GT. Abdominal muscle feedforward activation in patients with chronic low back pain is largely unaffected by 8 weeks of core stability training. Journal of Physiotherapy 2012;58:200. [DOI] [PubMed] [Google Scholar]
Alp 2011 {published data only}
- Alp A, Mengi G, Atik T, Mert M, Avsarotlu H. The evaluation of the efficacy of core stabilization exercises on female patients with chronic low back pain [Kronik bel atrili kadin hastalarda core‐stabilizasyon egzersizi etkinlitinin deterlendirilmesi]. Turkiye Fiziksel Tip ve Rehabilitasyon Dergisi 2011;57:249. [Google Scholar]
Alp 2014 {published data only}
- Alp A, Mengi G, Avsaroglu AH, Mert M, Sigirli D. Efficacy of core‐stabilization exercise and its comparison with home‐based conventional exercise in low back pain patients. Turkiye Fiziksel Tip ve Rehabilitasyon Dergisi 2014;60:S36‐42. [Google Scholar]
Ammar 2011 {published data only}
- Ammar TA, Mitchell K, Saleh A. Stabilization exercises in postnatal low back pain. Indian Journal of Physiotherapy and Occupational Therapy 2011;5:122‐4. [Google Scholar]
Andrusaitis 2011 {published data only}
- Andrusaitis SF, Brech GC, Vitale GF, Greve JM. Trunk stabilization among women with chronic lower back pain: a randomized, controlled, and blinded pilot study. Clinics 2011;66:1645‐50. [DOI] [PMC free article] [PubMed] [Google Scholar]
Appling 2009 {published data only}
- Appling SA, Chalona A, Edwards P, Green T, Jones C, LaVigne W. Effect of a progressive core stabilization exercise program on lumbar stability and abdominal strength. Journal of Orthopaedic & Sports Physical Therapy 2009;39:A83‐4. [Google Scholar]
Areeudomwong 2012 {published data only}
- Areeudomwong P, Puntumetakul R, Jirarattanaphochai K, Wanpen S, Kanpittaya J, Chatchawan U, et al. Core stabilization exercise improves pain intensity, functional disability and trunk muscle activity of patients with clinical lumbar instability: a pilot randomized controlled study. Journal of Physical Therapy Science 2012;24:1007‐12. [Google Scholar]
Barbosa 2013 {published data only}
- Barbosa AC, Martins FL, Barbosa MC, Dos Santos RT. Manipulation and selective exercises decrease pelvic anteversion and low‐back pain: a pilot study. Journal of Back & Musculoskeletal Rehabilitation 2013;26:33‐6. [DOI] [PubMed] [Google Scholar]
Bayraktar 2013 {published data only}
- Bayraktar D, Guclu‐Gunduz A, Lambeck J, Yazici G, Aykol S, Demirci H, et al. Core stability exercises: In water or on land? Comparison of the effects of two different core stabilization training. Annals of the Rheumatic Diseases 2013;72:1. [Google Scholar]
Belcher 1998 {published data only}
- Belcher MA. Pelvic stabilization exercise versus conventional weight training exercise during resistance training: its effect on the development of lumbar extension strength. Dissertation.. University of Southern Mississippi, Hattiesburg, Mississippi: University of Southern Mississippi; 1998.
Bentsen 1997 {published data only}
- Bentsen H, Lindgarde F, Manthorpe R. The effect of dynamic strength back exercise and/or a home training program in 57‐year‐old women with chronic low back pain. Results of a prospective randomized study with a 3‐year follow‐up period. Spine 1997;22:1494‐5000. [DOI] [PubMed] [Google Scholar]
Bi 2013 {published data only}
- Bi X, Zhao J, Zhao L, Liu Z, Zhang J, Sun D, et al. Pelvic floor muscle exercise for chronic low back pain. Journal of International Medical Research 2013;41:146‐52. [DOI] [PubMed] [Google Scholar]
Bilgin 2013 {published data only}
- Bilgin S, Temucin CM, Nurlu G, Kaya DO, Kose N, Gunduz AG. Effects of exercise and electrical stimulation on lumbar stabilization in asymptomatic subjects: a comparative study. Journal of Back and Musculoskeletal Rehabilitation 2013;26:261‐6. [DOI] [PubMed] [Google Scholar]
Bordiak 2012 {published data only}
- Bordiak FC, Silva EB. Electrical stimulation and core training on pain and range of motion in low back pain [Eletroestimulação e core training sobre dor e arco de movimento na lombalgia]. Fisioterapia em Movimento 2012;25:759‐66. [Google Scholar]
Bronfort 1996 {published data only}
- Bronfort G, Goldsmith CH, Nelson CF, Boline PD, Anderson AV. Trunk exercise combined with spinal manipulative or NSAID therapy for chronic low back pain: a randomized, observer‐blinded clinical trial. Journal of Manipulative and Physiological Therapeutics 1996;19:570‐82. [PubMed] [Google Scholar]
Bronfort 2011 {published data only}
- Bronfort G, Maiers MJ, Evans RL, Schulz CA, Bracha Y, Svendsen KH, et al. Supervised exercise, spinal manipulation, and home exercise for chronic low back pain: a randomized clinical trial. The Spine Journal 2011;11:585‐98. [DOI] [PubMed] [Google Scholar]
Brooks 2012 {published data only}
- Brooks C, Kennedy S, Marshall PWM. Specific trunk and general exercise elicit similar changes in anticipatory postural adjustments in patients with chronic low back pain: a randomized controlled trial [with consumer summary]. Spine 2012;37:E1543‐50. [DOI] [PubMed] [Google Scholar]
Brox 2003 {published data only}
- Brox JI, Sørensen R, Friis A, Nygaard Ø, Indahl A, Keller A, et al. Randomized clinical trial of lumbar instrumented fusion and cognitive intervention and exercises in patients with chronic low back pain and disc degeneration. Spine 2003;28:1913‐21. [DOI] [PubMed] [Google Scholar]
Buchbinder 2002 {published data only}
- Buchbinder R, Hoving J. Specific spinal exercise substantially reduces the risk of low back pain recurrence. Australian Journal of Physiotherapy 2002;48:55. [DOI] [PubMed] [Google Scholar]
Byuon 2012 {published data only}
- Byuon S, Son H. The effects of proprioceptive neuromuscular facilitation and stabilizing exercise on trunk repositioning errors. Journal of Physical Therapy Science 2012;24:1017‐20. [Google Scholar]
Cairns 2003 {published data only}
- Cairns M. Manipulation Association of Chartered Physiotherapists (UK) Research Presentation Award: a pragmatic randomized controlled trial of stabilization exercises in the management of recurrent low back pain. Manual Therapy 2003;8:185. [Google Scholar]
Cairns 2006 {published data only}
- Cairns MC, Foster NE, Wright C. Randomized controlled trial of specific spinal stabilization exercises and conventional physiotherapy for recurrent low back pain. Spine 2006;31:E670‐81. [DOI] [PubMed] [Google Scholar]
Carmo 2013 {published data only}
- Carmo CM, Jacob MFA, Takara KS, Santos FG, Caromano FA, Tanaka C. Trunk stabilizing exercise and strengthening exercises in patients with non‐specific chronic low back pain: a pilot blinded randomized trial. Annals of the Rheumatic Diseases 2012;71(Suppl 3):745. [Google Scholar]
Chan 2011 {published data only}
- Chan CW, Mok NW, Yeung EW. Aerobic exercise training in addition to conventional physiotherapy for chronic low back pain: a randomized controlled trial. Archives of Physical Medicine and Rehabilitation 2011;92:1681‐5. [DOI] [PubMed] [Google Scholar]
Childs 2009 {published data only}
- Childs JD, Teyhen DS, Benedict TM, Morris JB, Fortenberry AD, McQueen RM, et al. Effects of sit‐up training versus core stabilization exercises on sit‐up performance. Medicine & Science in Sports & Exercise 2009;41:2072‐83. [DOI] [PubMed] [Google Scholar]
Childs 2010 {published data only}
- Childs JD, Teyhen DS, Casey PR, McCoy‐Singh KA, Feldtmann AW, Wright AC, et al. Effects of traditional sit‐up training versus core stabilization exercises on short‐term musculoskeletal injuries in US army soldiers: a cluster randomized trial. Physical Therapy 2010;90:1404‐12. [DOI] [PubMed] [Google Scholar]
Cho 2014 {published data only}
- Cho HY, Kim EH, Kim J. Effects of the CORE exercise program on pain and active range of motion in patients with chronic low back pain. Journal of Physical Therapy Science 2014;26:1237‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chung 2013 {published data only}
- Chung S, Lee J, Yoon J. Effects of stabilization exercise using a ball on multifidus cross‐sectional area in patients with chronic low back pain. Journal of Sports Science & Medicine 2013;12:533‐41. [PMC free article] [PubMed] [Google Scholar]
Costa 2009 {published data only}
- Costa LO, Maher CG, Latimer J, Hodges PW, Herbert RD, Refshauge KM, et al. Motor control exercise for chronic low back pain: a randomized placebo‐controlled trial. Physical Therapy 2009;89:1275‐86. [DOI] [PubMed] [Google Scholar]
- Costa LO, Maher CG, McAuley JH, Hancock MJ, Herbert RD, Refshauge KM, et al. Prognosis for patients with chronic low back pain: inception cohort study. BMJ 2009;339:b3829. [DOI] [PMC free article] [PubMed] [Google Scholar]
Critchley 2007 {published data only}
- Critchley DJ, Ratcliffe J, Noonan S, Jones RH, Hurley MV. Effectiveness and cost‐effectiveness of three types of physiotherapy used to reduce chronic low back pain disability: a pragmatic randomized trial with economic evaluation. Spine 2007;32:1474‐81. [DOI] [PubMed] [Google Scholar]
Croft 1999 {published data only}
- Croft PR, Papageorgiou AC, Thomas E, Macfarlane GJ, Silman AJ. Short‐term physical risk factors for new episodes of low back pain. Prospective evidence from the South Manchester Back Pain Study. Spine 1999;24:1556‐61. [DOI] [PubMed] [Google Scholar]
Dehner 2009 {published data only}
- Dehner C, Schmelz A, Valker H, Krischak G, Kramer M. Low back pain intensity, microcirculation and muscle performance of the multifidus following back muscle strengthening in young elite oarsmen (Editor's Selection). International Sports Medicine Journal 2009;10:163‐75. [Google Scholar]
Descarreaux 2002 {published data only}
- Descarreaux M, Normand MC, Laurencelle L, Dugas C. Evaluation of a specific home exercise program for low back pain. Journal of Manipulative & Physiological Therapeutics 2002;25:497‐503. [DOI] [PubMed] [Google Scholar]
Donzelli 2006 {published data only}
- Donzelli S, Domenica E, Cova AM, Galletti R, Giunta N. Two different techniques in the rehabilitation treatment of low back pain: a randomized controlled trial. Europa Medicophysica 2006;42:205‐10. [PubMed] [Google Scholar]
Dufour 2010 {published data only}
- Dufour N, Thamsborg G, Oefeldt A, Lundsgaard C, Stender S. Treatment of chronic low back pain: a randomized, clinical trial comparing group‐based multidisciplinary biopsychosocial rehabilitation and intensive individual therapist‐assisted back muscle strengthening exercises. Spine 2010;35:469‐76. [DOI] [PubMed] [Google Scholar]
Durante 2010 {published data only}
- Durante H, Vasconcelos ECLM. Comparison between Isostretching method and conventional kinesiotherapy in low back pain treatment [Comparação do método Isostretching e cinesioterapia convencional no tratamento da lombalgia]. Semina: Ciências Biológicas e da Saúde 2010;30:83‐90. [Google Scholar]
Dvorak 2011 {published data only}
- Dvorak H, Kujat C, Brumitt J. Effect of therapeutic exercise versus manual therapy on athletes with chronic low back pain. Journal of Sport Rehabilitation 2011;20:494‐504. [DOI] [PubMed] [Google Scholar]
Earde 2014 {published data only}
- Earde P, Vongsirinavarat M, Sakulsriprasert P, Vachalathiti R. Immediate effects of trunk stabilizer muscles training on muscle response time in individuals with non‐specific chronic low back pain. Journal of the Medical Association of Thailand 2014;97(Suppl 7):S89‐94. [PubMed] [Google Scholar]
Ewert 2009 {published data only}
- Ewert T, Limm H, Wessels T, Rackwitz B, Garnier K, Freumuth R, et al. The comparative effectiveness of a multimodal program versus exercise alone for the secondary prevention of chronic low back pain and disability. PM & R: The Journal of Injury, Function, and Rehabilitation 2009;1:798‐808. [DOI] [PubMed] [Google Scholar]
Faas 1993 {published data only}
- Faas A, Chavannes AW, Eijk JT, Gubbels JW. A randomized, placebo‐controlled trial of exercise therapy in patients with acute low back pain. Spine 1993;18:1388‐95. [PubMed] [Google Scholar]
Faas 1995 {published data only}
- Faas A, Eijk JT, Chavannes AW, Gubbels JW. A randomized trial of exercise therapy in patients with acute low back pain. Efficacy on sickness absence. Spine 1995;20:941‐7. [DOI] [PubMed] [Google Scholar]
Ferreira 2007 {published data only}
- Ferreira ML, Ferreira PH, Latimer J, Herbert RD, Hodges PW, Jennings MD, et al. Comparison of general exercise, motor control exercise and spinal manipulative therapy for chronic low back pain: a randomized trial. Pain 2007;131:31‐7. [DOI] [PubMed] [Google Scholar]
Franca 2010 {published data only}
- Franca FR, Burke TN, Hanada ES, Marques AP. Segmental stabilization and muscular strengthening in chronic low back pain: a comparative study. Clinics 2010;65:1013‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Franca 2012 {published data only}
- Franca FR, Burke TN, Caffaro RR, Ramos LA, Marques AP. Effects of muscular stretching and segmental stabilization on functional disability and pain in patients with chronic low back pain: a randomized controlled trial. Journal of Manipulative and Physiological Therapeutics 2012;35:279‐85. [DOI] [PubMed] [Google Scholar]
Freitas 2008 {published data only}
- Freitas CD, D'Andrea JM. Comparison between isokinetic dynamometer and therapeutic ball exercise in chronic low back pain of mechanical origin [Estudo comparativo entre exercícios com dinamômetro isocinético e bola terapêutica na lombalgia crônica de origem mecânica]. Revista Fisioterapia & Pesquisa 2008;15:380‐6. [Google Scholar]
Gagnon 2005 {published data only}
- Gagnon LH. Efficacy of Pilates exercises as therapeutic intervention in treating patients with low back pain. Dissertation.. University of Tennessee, Knoxville, Tennessee; University of Tennessee; 2005.
Gatti 2011 {published data only}
- Gatti R, Faccendini S, Tettamanti A, Barbero M, Balestri A, Calori G. Efficacy of trunk balance exercises for individuals with chronic low back pain: a randomized clinical trial. Journal of Orthopaedic & Sports Physical Therapy 2011;41:542‐52. [DOI] [PubMed] [Google Scholar]
George 2011 {published data only}
- George SZ, Childs JD, Teyhen DS, Wu SS, Wright AC, Dugan JL, et al. Brief psychosocial education, not core stabilization, reduced incidence of low back pain: results from the Prevention of Low Back Pain in the Military (POLM) cluster randomized trial. BMC Medicine 2011;9:128. [DOI] [PMC free article] [PubMed] [Google Scholar]
Goldby 2006 {published data only}
- Goldby LJ, Moore AP, Doust J, Trew ME. A randomized controlled trial investigating the efficiency of musculoskeletal physiotherapy on chronic low back disorder. Spine 2006;31:1083‐93. [DOI] [PubMed] [Google Scholar]
Gustafsson 2008 {published data only}
- Gustafsson J, Nilsson‐Wikmar L. Influence of specific muscle training on pain, activity limitation and kinesiophobia in women with back pain post‐partum: a single‐subject research design. Physiotherapy Research International 2008;13:18‐30. [DOI] [PubMed] [Google Scholar]
Guven 2003 {published data only}
- Guven Z, Marangozoglu I, Gunduz OH. Effectiveness of lumbopelvic stabilization exercise education in patients with chronic mechanical low back pain [Kronik mekanik bel agrili hastalarda lumbopelvik stabilizasyon egzersiz egitiminin etkinligi]. Turkiye Fiziksel Tip ve Rehabilitasyon Dergisi 2003;49:17. [Google Scholar]
Hagen 2010 {published data only}
- Hagen EM, Odelien KH, Lie SA, Eriksen HR. Adding a physical exercise programme to brief intervention for low back pain patients did not increase return to work. Scandinavian Journal of Public Health 2010;38:731‐8. [DOI] [PubMed] [Google Scholar]
Hansen 1993 {published data only}
- Hansen FR, Bendix T, Skov P, Jensen CV, Kristensen JH, Krohn L, et al. Intensive, dynamic back‐muscle exercises, conventional physiotherapy, or placebo‐control treatment of low‐back pain. A randomized, observer‐blind trial. Spine 1993;18:98‐108. [DOI] [PubMed] [Google Scholar]
Harkapaa 1989 {published data only}
- Harkapaa K, Jarvikoski A, Mellin G, Hurri H. A controlled study on the outcome of inpatient and outpatient treatment of low back pain. Part I. Pain, disability, compliance, and reported treatment benefits three months after treatment. Scandinavian Journal of Rehabilitation Medicine 1989;21:81‐9. [PubMed] [Google Scholar]
Harringe 2007 {published data only}
- Harringe ML, Nordgren JS, Arvidsson I, Werner S. Low back pain in young female gymnasts and the effect of specific segmental muscle control exercises of the lumbar spine: a prospective controlled intervention study. Knee Surgery, Sports Traumatology, Arthroscopy 2007;15:1264‐71. [DOI] [PubMed] [Google Scholar]
Harts 2008 {published data only}
- Harts CC, Helmhout PH, Bie RA, StaaI JB. A high‐intensity lumbar extensor strengthening program is little better than a low‐intensity program or a waiting list control group for chronic low back pain: a randomised clinical trial. Australian Journal of Physiotherapy 2008;54:23‐31. [DOI] [PubMed] [Google Scholar]
Helewa 1999 {published data only}
- Helewa A, Goldsmith CH, Lee P, Smythe HA, Forwell L. Does strengthening the abdominal muscles prevent low back pain: a randomized controlled trial. The Journal of Rheumatology 1999;26:1808‐15. [PubMed] [Google Scholar]
Helmhout 2004 {published data only}
- Helmhout PH, Harts CC, Staal JB, Candel MJ, Bie RA. Comparison of a high‐intensity and a low‐intensity lumbar extensor training program as minimal intervention treatment in low back pain: a randomized trial. European Spine Journal 2004;13:537‐47. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hemmati 2011 {published data only}
- Hemmati S, Rajabi R, Karimi N, Jahandideh AA. Effects of consecutive supervised core stability training on pain and disability in women with nonspecific chronic low back pain [Persian]. Koomesh 2011;12:244‐52. [Google Scholar]
Henchoz 2010 {published data only}
- Henchoz Y, Pinget C, Wasserfallen JB, Paillex R, Goumoens P, Norberg M, et al. Cost‐utility analysis of a three‐month exercise programme versus usual care following multidisciplinary rehabilitation for chronic low back pain. Journal of Rehabilitation Medicine 2010;42:846‐52. [DOI] [PubMed] [Google Scholar]
Hides 2008 {published data only}
- Hides JA, Stanton WR, McMahon S, Sims K, Richardson CA. Effect of stabilization training on multifidus muscle cross‐sectional area among young elite cricketers with low back pain. Journal of Orthopaedic & Sports Physical Therapy 2008;38:101‐8. [DOI] [PubMed] [Google Scholar]
Hosseinifar 2013 {published data only}
- Hosseinifar M, Akbari M, Behtash H, Amiri M, Sarrafzadeh J. The effects of stabilization and Mckenzie exercises on transverse abdominis and multifidus muscle thickness, pain, and disability: a randomized controlled trial in nonspecific chronic low back pain. Journal of Physical Therapy Science 2013;25:1541‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hunter 2012 {published data only}
- Hunter RF, McDonough SM, Bradbury I, Liddle SD, Walsh DM, Dhamija S, et al. Exercise and auricular acupuncture for chronic low‐back pain: a feasibility randomized‐controlled trial. The Clinical Journal of Pain 2012;28:259‐67. [DOI] [PubMed] [Google Scholar]
Hurwitz 2005 {published data only}
- Hurwitz EL, Morgenstern H, Chiao C. Effects of recreational physical activity and back exercises on low back pain and psychological distress: findings from the UCLA Low Back Pain Study. American Journal of Public Health 2005;95:1817‐24. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hwang 2013 {published data only}
- Hwang JA, Bae SH, Do Kim G, Kim KY. The effects of sensorimotor training on anticipatory postural adjustment of the trunk in chronic low back pain patients. Journal of Physical Therapy Science 2013;25:1189‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Inani 2013 {published data only}
- Inani SB, Selkar SP. Effect of core stabilization exercises versus conventional exercises on pain and functional status in patients with non‐specific low back pain: a randomized clinical trial. Journal of Back and Musculoskeletal Rehabilitation 2013;26:37‐43. [DOI] [PubMed] [Google Scholar]
ISRCTN80064281 {published data only}
- ISRCTN80064281. Movement control exercise for low back pain. http://www.isrctn.com/ISRCTN80064281 (accessed 25 June 2015).
Jang 2013 {published data only}
- Jang S, Lee J, Bang H. The effect of trunk control exercises performed on unstable surfaces on the spinal stability of low back pain patients. Journal of Physical Therapy Science 2013;25:459‐62. [Google Scholar]
Javadian 2012 {published data only}
- Javadian Y, Behtash H, Akbari M, Taghipour‐Darzi M, Zekavat H. The effects of stabilizing exercises on pain and disability of patients with lumbar segmental instability. Journal of Back and Musculoskeletal Rehabilitation 2012;25:149‐55. [DOI] [PubMed] [Google Scholar]
Javadian 2015 {published data only}
- Javadian Y, Akbari M, Talebi G, Taghipour‐Darzi M, Janmohammadi N. Influence of core stability exercise on lumbar vertebral instability in patients presented with chronic low back pain: a randomized clinical trial. Caspian Journal of Internal Medicine 2015;6(2):98–102. [PMC free article] [PubMed] [Google Scholar]
Johannsen 1995 {published data only}
- Johannsen F, Remvig L, Kryger P, Beck P, Warming S, Lybeck K, et al. Exercises for chronic low back pain: a clinical trial. The Journal of Orthopaedic and Sports Physical Therapy 1995;22:52‐9. [DOI] [PubMed] [Google Scholar]
Johnson 2007 {published data only}
- Johnson RE, Jones GT, Wiles NJ, Chaddock C, Potter RG, Roberts C, et al. Active exercise, education, and cognitive behavioral therapy for persistent disabling low back pain: a randomized controlled trial. Spine 2007;32:1578‐85. [DOI] [PubMed] [Google Scholar]
Jones 2007 {published data only}
- Jones M, Stratton G, Reilly T, Unnithan V. The efficacy of exercise as an intervention to treat recurrent nonspecific low back pain in adolescents. Pediatric Exercise Science 2007;19:349‐59. [DOI] [PubMed] [Google Scholar]
Kaapa 2006 {published data only}
- Kaapa EH, Frantsi K, Sarna S, Malmivaara A. Multidisciplinary group rehabilitation versus individual physiotherapy for chronic nonspecific low back pain: a randomized trial. Spine 2006;31:371‐6. [DOI] [PubMed] [Google Scholar]
Kachanathu 2012 {published data only}
- Kachanathu SJ, Zakaria AR, Sahni A, Jaiswal P. Chronic low back pain in fast bowlers: a comparative study of core spinal stabilization and conventional exercises. Journal of Physical Therapy Science 2012;24:821‐5. [Google Scholar]
Karimi 2009 {published data only}
- Karimi N, Ebrahimi I, Ezzati K, Kahrizi S, Torkaman G, Arab AM. The effects of consecutive supervised stability training on postural balance in patients with chronic low back pain. Pakistan Journal of Medical Sciences 2009;25:181. [Google Scholar]
Kladny 2003 {published data only}
- Kladny B, Fischer F C, Haase I. [Evaluation of specific stabilizing exercise in the treatment of low back pain and lumbar disk disease in outpatient rehabilitation]. [German]. Zeitschrift fur Orthopadie und Ihre Grenzgebiete 2003;141:401‐5. [DOI] [PubMed] [Google Scholar]
Kline 2013 {published data only}
- Kline JB, Krauss JR, Maher SF, Qu X. Core strength training using a combination of home exercises and a dynamic sling system for the management of low back pain in pre‐professional ballet dancers: a case series. Journal of Dance Medicine & Science 2013;17:24‐33. [DOI] [PubMed] [Google Scholar]
Kofotolis 2008 {published data only}
- Kofotolis ND, Vlachopoulos SP, Kellis E. Sequentially allocated clinical trial of rhythmic stabilization exercises and TENS in women with chronic low back pain. Clinical Rehabilitation 2008;22:99‐111. [DOI] [PubMed] [Google Scholar]
Koldas 2008 {published data only}
- Koldas Dogan S, Sonel Tur B, Kurtais Y, Atay MB. Comparison of three different approaches in the treatment of chronic low back pain. Clinical Rheumatology 2008;27:873‐81. [DOI] [PubMed] [Google Scholar]
Koumantakis 2005 {published data only}
- Koumantakis GA, Watson PJ, Oldham JA. Trunk muscle stabilization training plus general exercise versus general exercise only: randomized controlled trial of patients with recurrent low back pain. Physical Therapy 2005;85:209‐25. [PubMed] [Google Scholar]
Kumar 2009 {published data only}
- Kumar S, Sharma VP, Negi MPS. Efficacy of dynamic muscular stabilization techniques (DMST) over conventional techniques in rehabilitation of chronic low back pain. Journal of Strength and Conditioning Research 2009;23:2651‐9. [DOI] [PubMed] [Google Scholar]
Kumar 2010 {published data only}
- Kumar S, Sharma VP, Shukla R, Dev R. Comparative efficacy of two multimodal treatments on male and female sub‐groups with low back pain (part II). Journal of Back and Musculoskeletal Rehabilitation 2010;23:1‐9. [DOI] [PubMed] [Google Scholar]
Kumar 2011 {published data only}
- Kumar SP. Efficacy of segmental stabilization exercise for lumbar segmental instability in patients with mechanical low back pain: a randomized placebo controlled crossover study. North American Journal of Medical Sciences 2011;3:461. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kumar 2012 {published data only}
- Kumar S, Sharma VP, Aggarwal A, Shukla R, Dev R. Effect of dynamic muscular stabilization technique on low back pain of different durations. Journal of Back & Musculoskeletal Rehabilitation 2012;25:73‐9. [DOI] [PubMed] [Google Scholar]
Kuukkanen 1996 {published data only}
- Kuukkanen T, Malkia E. Muscular performance after a 3 month progressive physical exercise program and 9 month follow‐up in subjects with low back pain. A controlled study. Spine 1996;6:112‐21. [DOI] [PubMed] [Google Scholar]
Lee 2015 {published data only}
- Lee JS, Kim TH, Kim DY, Shim JH, Lim JY. Effects of selective exercise for the deep abdominal muscles and lumbar stabilization exercise on the thickness of the transversus abdominis and postural maintenance. Journal of Physical Therapy Science 2015;27:367‐70. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lewis 2005 {published data only}
- Lewis JS, Hewitt JS, Billington L, Cole S, Byng J, Karayiannis S. A randomized clinical trial comparing two physiotherapy interventions for chronic low back pain. Scandinavian Journal of Medicine & Science in Sports 2005;30:711‐21. [DOI] [PubMed] [Google Scholar]
Lie 1999 {published data only}
- Lie H, Frey S. [Mobilizing or stabilizing exercise in degenerative disk disease in the lumbar region?]. [Norwegian]. Tidsskrift for Den Norske Laegeforening 1999;119:2051‐3. [PubMed] [Google Scholar]
Lomond 2015 {published data only}
- Lomond KV, Jacobs JV, Hitt JR, DeSarno MJ, Bunn JY, Henry SM. Effects of low back pain stabilization or movement system impairment treatments on voluntary postural adjustments: a randomized controlled trial. Spine Journal 2015;15:596‐606. [DOI] [PMC free article] [PubMed] [Google Scholar]
Long 2004 {published data only}
- Long A, Donelson R, Fung T. Does it matter which exercise? A randomized control trial of exercise for low back pain. Spine 2004;29:2593‐602. [DOI] [PubMed] [Google Scholar]
Macedo 2008 {published data only}
- Macedo LG, Latimer J, Maher CG, Hodges PW, Nicholas M, Tonkin L, et al. Motor control or graded activity exercises for chronic low back pain? A randomised controlled trial. BMC Musculoskeletal Disorders 2008;5:65. [DOI] [PMC free article] [PubMed] [Google Scholar]
Macedo 2012 {published data only}
- Macedo LG, Latimer J, Maher CG, Hodges PW, McAuley JH, Nicholas MK, et al. Effect of motor control exercises versus graded activity in patients with chronic nonspecific low back pain: a randomized controlled trial. Physical Therapy 2012;93:1‐15. [DOI] [PubMed] [Google Scholar]
Magalhaes 2013 {published data only}
- Magalhaes MO, França FJR, Burke TN, Ramos LAV, Carvalho e Silva APMC, Almeida GPL, et al. Efficacy of graded activity versus supervised exercises in patients with chronic non‐specific low back pain: protocol of a randomised controlled trial. BMC Musculoskeletal Disorders 2013;14:36. [DOI: 10.1186/1471-2474-14-36] [DOI] [PMC free article] [PubMed] [Google Scholar]
Magnusson 2008 {published data only}
- Magnusson ML, Chow DH, Diamandopoulos Z, Pope MH. Motor control learning in chronic low back pain. Spine 2008;33:E532‐8. [DOI] [PubMed] [Google Scholar]
Maher 2005 {published data only}
- Maher CG, Latimer J, Hodges PW, Refshauge KM, Moseley L, Herbert RD, et al. The effect of motor control exercise versus placebo in patients with chronic low back pain. BMC Musculoskeletal Disorders 2005;6:54. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mannion 1999 {published data only}
- Mannion AF, Muntener M, Taimela S, Dvorak J. A randomized clinical trial of three active therapies for chronic low back pain. Spine 1999;24:2435‐48. [DOI] [PubMed] [Google Scholar]
Mannion 2009 {published data only}
- Mannion AF, Helbling D, Pulkovski N, Sprott H. Spinal segmental stabilisation exercises for chronic low back pain: programme adherence and its influence on clinical outcome. European Spine Journal 2009;18:1881‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mannion 2012 {published data only}
- Mannion AF, Caporaso F, Pulkovski N, Sprott H. Spine stabilisation exercises in the treatment of chronic low back pain: a good clinical outcome is not associated with improved abdominal muscle function. European Spine Journal 2012;21:1301‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Marshall 2008 {published data only}
- Marshall PW, Murphy BA. Muscle activation changes after exercise rehabilitation for chronic low back pain. Archives of Physical Medicine & Rehabilitation 2008;89:1305‐13. [DOI] [PubMed] [Google Scholar]
Meira 2013 {published data only}
- Meira DM. Functional reeducation program associated with back school improves functional disability and pain in workers with chronic low back pain: a pilot study. Annals of the Rheumatic Diseases 2013;72:A1095. [Google Scholar]
Miller 2005 {published data only}
- Miller ER, Schenk RJ, Karnes JL, Rousselle JG. A comparison of the McKenzie approach to a specific spine stabilization program for chronic low back pain. The Journal of Manual & Manipulative Therapy 2005;13:103‐12. [Google Scholar]
Mohseni‐Bandpei 2011 {published data only}
- Mohseni‐Bandpei MA, Rahmani N, Behtash H, Karimloo M. The effect of pelvic floor muscle exercise on women with chronic non‐specific low back pain. Journal of Bodywork & Movement Therapies 2011;15:75‐81. [DOI] [PubMed] [Google Scholar]
Monteiro 2009 {published data only}
- Monteiro FC, Kirkwood RN, Magalhaes CMB. Lumbar stabilization exercises and manual therapy for treatment of non‐specific and chronic low back pain [Exercícios de estabilizaçao lombar e terapia manual no tratamento da dor lombar crônica inespecífica]. Revista Fisioterapia Brasil 2009;10:442‐7. [Google Scholar]
Monticone 2004 {published data only}
- Monticone M, Barbarino A, Testi C, Arzano S, Moschi A, Negrini S. Symptomatic efficacy of stabilizing treatment versus laser therapy for sub‐acute low back pain with positive tests for sacroiliac dysfunction: a randomised clinical controlled trial with 1 year follow‐up. Europa Medicophysica 2004;40:263‐8. [PubMed] [Google Scholar]
Moon 2013 {published data only}
- Moon HJ, Choi KH, Kim DH, Kim HJ, Cho YK, Lee KH, et al. Effect of lumbar stabilization and dynamic lumbar strengthening exercises in patients with chronic low back pain. Annals of Rehabilitation Medicine 2013;37:110‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moseley 2002 {published data only}
- Moseley L. Combined physiotherapy and education is efficacious for chronic low back pain. Australian Journal of Physiotherapy 2002;48:297‐302. [DOI] [PubMed] [Google Scholar]
Moseley 2003 {published data only}
- Moseley GL. Joining forces ‐ combining cognition ‐ targeted motor control training with group or individual pain physiology education: a successful treatment for chronic low back pain. Journal of Manual & Manipulative Therapy 2003;11:88‐94. [Google Scholar]
Moussouli 2014 {published data only}
- Moussouli M, Vlachopoulos SP, Kofotolis ND, Theodorakis Y, Malliou P, Kellis E. Effects of stabilization exercises on health‐related quality of life in women with chronic low back pain. Journal of Physical Activity & Health 2014;11:1295‐303. [DOI] [PubMed] [Google Scholar]
Navalgund 2009 {published data only}
- Navalgund A. Evaluating the effect of a 10‐week stabilization exercise program on the postural stability and the neuromuscular control of the spine in subjects with subacute recurrent low back pain. Dissertation.. Ohio State University, Columbus, Ohio: Ohio State University; 2009.
NCT00201513 {published data only}
- NCT00201513. Anticipatory muscle control and effect of stabilizing exercises in patients with subacute and chronic low back pain. https://clinicaltrials.gov/ct2/show/NCT00201513 (accessed 25 June 2015).
NCT00555802 {published data only}
- NCT00555802. The effect of motor control exercise versus general exercise on lumbar local stabilizing muscles thickness. https://clinicaltrials.gov/ct2/show/NCT00555802 (accessed 25 June 2015).
NCT00624533 {published data only}
- NCT00624533. Efficiency of GDS method for lumbar stabilization for non‐specific low back pain in primary care. https://clinicaltrials.gov/ct2/show/NCT00624533 (accessed 25 June 2015).
NCT01061632 {published data only}
- NCT01061632. High (deadlift) versus low intensity motor control exercises on low back pain. https://clinicaltrials.gov/ct2/show/NCT01061632 (accessed 25 June 2015).
NCT01124201 {published data only}
- NCT01124201. Lumbar stabilization, strengthening and stretching in chronic low back pain. https://clinicaltrials.gov/ct2/show/NCT01124201 (accessed 25 June 2015).
NCT01362049 {published data only}
- NCT01362049. Mechanisms of specific trunk exercises in low back pain. https://clinicaltrials.gov/ct2/show/NCT01362049 (accessed 25 June 2015).
NCT02112760 {published data only}
- NCT02112760. Specific stabilization exercise with ultrasound feedback for patients with recurrent low back pain. https://clinicaltrials.gov/ct2/show/NCT02112760 (accessed 25 June 2015).
NCT02170753 {published data only}
- NCT02170753. Regional manual therapy and motor control exercise for chronic low back pain. https://clinicaltrials.gov/ct2/show/NCT02170753 (accessed 25 June 2015).
NCT02200913 {published data only}
- NCT02200913. Effects of core stabilization exercise on balance. https://clinicaltrials.gov/ct2/show/NCT02200913 (accessed 25 June 2015).
NCT02221609 {published data only}
- NCT02221609. Movement system impairment based classification versus general exercise for chronic non‐specific low back pain: a randomised controlled trial. https://clinicaltrials.gov/ct2/show/NCT02221609 (accessed 25 June 2015). [DOI] [PubMed]
NCT02374970 {published data only}
- NCT02374970. Transversus abdominis muscular training and chronic low back pain. https://clinicaltrials.gov/ct2/show/NCT02374970 (accessed 25 June 2015).
NCT02398760 {published data only}
- NCT02398760. Relationship between clinical tests and clinical outcomes after motor control exercises intervention. https://clinicaltrials.gov/ct2/show/NCT02398760 (accessed 25 June 2015).
Nelson 1995 {published data only}
- Nelson BW, O'Reilly E, Miller M, Hogan M, Wegner JA, Kelly C. The clinical effects of intensive, specific exercise on chronic low back pain: a controlled study of 895 consecutive patients with 1‐year follow up. Orthopedics 1995;18:971‐81. [DOI] [PubMed] [Google Scholar]
Nelson‐Wong 2009 {published data only}
- Nelson‐Wong E. Biomechanical predictors of functionally induced low back pain, acute response to prolonged standing exposure, and impact of a stabilization‐based clinical exercise intervention. Dissertation.. University of Waterloo (Canada), Waterloo, Ontario, Canada: University of Waterloo; 2009.
Niemisto 2003 {published data only}
- Niemisto L, Lahtinen‐Suopanki T, Rissanen P, Lindgren KA, Sarna S, Hurri H. A randomized trial of combined manipulation, stabilizing exercises, and physician consultation compared to physician consultation alone for chronic low back pain. Spine 2003;28:2185‐91. [DOI] [PubMed] [Google Scholar]
Niemisto 2004 {published data only}
- Niemisto L, Sarna S, Lahtinen‐Suopanki T, Lindgren KA, Hurri H. Predictive factors for 1‐year outcome of chronic low back pain following manipulation, stabilizing exercises, and physician consultation or physician consultation alone. Journal of Rehabilitation Medicine 2004;36:104‐9. [DOI] [PubMed] [Google Scholar]
Niemisto 2005 {published data only}
- Niemisto L, Rissanen P, Sarna S, Lahtinen‐Suopanki T, Lindgren KA, Hurri H. Cost‐effectiveness of combined manipulation, stabilizing exercises, and physician consultation compared to physician consultation alone for chronic low back pain: a prospective randomized trial with 2‐year follow‐up. Spine 2005;30:1109‐15. [DOI] [PubMed] [Google Scholar]
Norris 2008 {published data only}
- Norris C, Matthews M. The role of an integrated back stability program in patients with chronic low back pain. Complementary Therapies in Clinical Practice 2008;14:255‐63. [DOI] [PubMed] [Google Scholar]
O'Sullivan 1997 {published data only}
- O'Sullivan PB, Phyty GD, Twomey LT, Allison GT. Evaluation of specific stabilizing exercise in the treatment of chronic low back pain with radiologic diagnosis of spondylolysis or spondylolisthesis. Spine 1997;22:2959‐67. [DOI] [PubMed] [Google Scholar]
Oguzhan 2011 {published data only}
- Oguzhan H, Ozyurek S, Kaya E. Effectiveness of back school program to quality of life and disability in patients with chronic low back pain. European Journal of Pain Supplements. Conference: 7 Congress of the European Federation of Pain Chapters: Pain in Europe VII, EFIC. Hamburg, Germany, 2011.
Ota 2011 {published data only}
- Ota M, Kaneoka K, Hangai M, Koizumi K, Muramatsu T. Effectiveness of lumbar stabilization exercises for reducing chronic low back pain and improving quality of life. Journal of Physical Therapy Science 2011;23:679‐81. [Google Scholar]
Pereira 2010 {published data only}
- Pereira NT, Ferreira LAB, Pereira WM. Effectiveness of segmental stabilization exercises on mechanical‐postural chronic low back pain [Efetividade de exercícios de estabilização segmental sobre a dor lombar crônica mecânico‐postural]. Fisioterapia em Movimento 2010;23:605‐14. [Google Scholar]
Puntumetakul 2013 {published data only}
- Puntumetakul R, Areeudomwong P, Emasithi A, Yamauchi J. Effect of 10‐week core stabilization exercise training and detraining on pain‐related outcomes in patients with clinical lumbar instability. Patient Preference and Adherence 2013;7:1189‐99. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rabin 2014 {published data only}
- Rabin A, Shashua A, Pizem K, Dickstein R, Dar G. A clinical prediction rule to identify patients with low back pain who are likely to experience short‐term success following lumbar stabilization exercises: a randomized controlled validation study. Journal of Orthopaedic & Sports Physical Therapy 2014;44:6‐B13. [DOI] [PubMed] [Google Scholar]
Rasmussen‐Barr 2003 {published data only}
- Rasmussen‐Barr E, Nilsson‐Wikmarn L, Arvidsson I. Stabilizing training compared with manual treatment in sub‐acute and chronic low‐back pain. Manual Therapy 2003;8:233‐41. [DOI] [PubMed] [Google Scholar]
Rasmussen‐Barr 2009 {published data only}
- Rasmussen‐Barr E, Ang B, Arvidsson I, Nilsson‐Wikmar L. Graded exercise for recurrent low‐back pain: a randomized, controlled trial with 6‐, 12‐, and 36‐month follow‐ups. Spine 2009;34:221‐8. [DOI] [PubMed] [Google Scholar]
Rhee 2012 {published data only}
- Rhee HS, Kim YH, Sung PS. A randomized controlled trial to determine the effect of spinal stabilization exercise intervention based on pain level and standing balance differences in patients with low back pain. Medical Science Monitor 2012;18:CR174‐81. [DOI] [PMC free article] [PubMed] [Google Scholar]
Riipinen 2005 {published data only}
- Riipinen M, Niemisto L, Lindgren KA, Hurri H. Psychosocial differences as predictors for recovery from chronic low back pain following manipulation, stabilizing exercises and physician consultation or physician consultation alone. Journal of Rehabilitation Medicine 2005;37:152‐8. [DOI] [PubMed] [Google Scholar]
Rydeard 2006 {published data only}
- Rydeard R, Leger A, Smith D. Pilates‐based therapeutic exercise: effect on subjects with nonspecific chronic low back pain and functional disability: a randomized controlled trial. Journal of Orthopaedic & Sports Physical Therapy 2006;36:472‐84. [DOI] [PubMed] [Google Scholar]
Saner 2011 {published data only}
- Saner J, Kool J, Bie RA, Sieben JM, Luomajoki H. Movement control exercise versus general exercise to reduce disability in patients with low back pain and movement control impairment. A randomised controlled trial. BMC Musculoskeletal Disorders 2011;12:207. [DOI: 10.1186/1471-2474-12-207] [DOI] [PMC free article] [PubMed] [Google Scholar]
Saner 2015 {published data only}
- Saner J, Kool J, Sieben JM, Luomajoki H, Bastiaenen CH, Bie RA. A tailored exercise program versus general exercise for a subgroup of patients with low back pain and movement control impairment: a randomised controlled trial with one‐year follow‐up. Manual Therapy 2015 Feb 26 [Epub ahead of print]. [DOI] [PubMed]
Shakeri 2013 {published data only}
- Shakeri H, Fathollahi Z, Karimi N, Arab AM. Effect of functional lumbar stabilization exercises on pain, disability, and kinesiophobia in women with menstrual low back pain: a preliminary trial. Journal of Chiropractic Medicine 2013;12:160‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Shaughnessy 2004 {published data only}
- Shaughnessy M, Caulfield B. A pilot study to investigate the effect of lumbar stabilisation exercise training on functional ability and quality of life in patients with chronic low back pain. International Journal of Rehabilitation Research 2004;27:297‐301. [DOI] [PubMed] [Google Scholar]
Shnayderman 2013 {published data only}
- Shnayderman I, Katz‐Leurer M. An aerobic walking programme versus muscle strengthening programme for chronic low back pain: a randomized controlled trial. Clinical Rehabilitation 2013;27:207‐14. [DOI] [PubMed] [Google Scholar]
Smeets 2009 {published data only}
- Smeets RJEM. Do lumbar stabilising exercises reduce pain and disability in patients with recurrent low back pain?. Australian Journal of Physiotherapy 2009;55:138. [DOI] [PubMed] [Google Scholar]
Smith 2011 {published data only}
- Smith D, Bissell G, Bruce‐Low S, Wakefield C. The effect of lumbar extension training with and without pelvic stabilization on lumbar strength and low back pain. Journal of Back and Musculoskeletal Rehabilitation 2011;24:241‐9. [DOI] [PubMed] [Google Scholar]
Sokunbi 2008 {published data only}
- Sokunbi O, Watt P, Moore A. A randomised controlled trial (RCT) on the effects of frequency of application of spinal stabilisation exercises on multifidus cross sectional area (MFCSA) in participants with chronic low back pain. Physiotherapy Singapore 2008;11:9‐16. [Google Scholar]
Stankovic 2012 {published data only}
- Stankovic A, Lazovic M, Kocic M, Dimitrijevic L, Stankovic I, Zlatanovic D, et al. Lumbar stabilization exercises in addition to strengthening and stretching exercises reduce pain and increase function In patients with chronic low back pain: randomized clinical open‐label study. Turkish Journal of Physical Medicine and Rehabilitation 2012;58:177‐83. [Google Scholar]
Streicher 2014 {published data only}
- Streicher H, Matzold F, Hamilton C, Wagner P. Comparison of group motor control training versus individual training for people suffering from back pain. Journal of Bodywork and Movement Therapies 2014;18:489‐96. [DOI] [PubMed] [Google Scholar]
Stuge 2004 {published data only}
- Stuge B, Laerum E, Kirkesola G, Vollestad N. The efficacy of a treatment program focusing on specific stabilizing exercises for pelvic girdle pain after pregnancy: a randomized controlled trial. Spine 2004;29:359. [DOI] [PubMed] [Google Scholar]
Suni 2006 {published data only}
- Suni J, Rinne M, Natri A, Statistisian MP, Parkkari J, Alaranta H. Control of the lumbar neutral zone decreases low back pain and improves self‐evaluated work ability: a 12‐month randomized controlled study. Spine 2006;31:E611‐20. [DOI] [PubMed] [Google Scholar]
Teyhen 2010 {published data only}
- Teyhen DS, Usalis J, Szymanek EB, Paschall JC, Meagher MS, Harvey AD, et al. Rehabilitative ultrasound imaging assessment of the lumbar multifidus during stabilization exercises in healthy adults. Journal of Orthopaedic & Sports Physical Therapy 2010;40:A39. [Google Scholar]
Torstensen 1998 {published data only}
- Torstensen TA, Ljunggren AE, Meen HD, Odland E, Mowinckel P, Geijerstam S. Efficiency and costs of medical exercise therapy, conventional physiotherapy, and self‐exercise in patients with chronic low back pain. A pragmatic, randomized, single‐blinded, controlled trial with 1‐year follow‐up. Spine 1998;23:2616‐24. [DOI] [PubMed] [Google Scholar]
Trampas 2014 {published data only}
Tsauo 2009 {published data only}
- Tsauo JY, Chen WH, Liang HW, Jang Y. The effectiveness of a functional training programme for patients with chronic low back pain – a pilot study. Disability and Rehabilitation 2009;31:1100‐6. [DOI] [PubMed] [Google Scholar]
Unsgaard‐Tondel 2010 {published data only}
- Unsgaard‐Tondel M, Fladmark AM, Salvesen O, Vasseljen O. Motor control exercises, sling exercises, and general exercises for patients with chronic low back pain: a randomized controlled trial with 1‐year follow‐up. Physical Therapy 2010;90:1426‐40. [DOI] [PubMed] [Google Scholar]
Vasseljen 2010 {published data only}
- Vasseljen O, Fladmark AM. Abdominal muscle contraction thickness and function after specific and general exercises: a randomized controlled trial in chronic low back pain patients. Manual Therapy 2010;15:482‐9. [DOI] [PubMed] [Google Scholar]
Vasseljen 2012 {published data only}
- Vasseljen O, Unsgaard‐Tondel M, Westad C, Mork PJ. Effect of core stability exercises on feed‐forward activation of deep abdominal muscles in chronic low back pain. Spine 2012;37:1101‐8. [DOI] [PubMed] [Google Scholar]
Wang 2012 {published data only}
- Wang X, Zheng J, Bi X, Liu J. Effect of core stability training on patients with chronic low back pain. HealthMED 2012;6:754‐9. [Google Scholar]
Willemink 2012 {published data only}
- Willemink MJ, Es HW, Helmhout PH, Diederik AL, Kelder JC, Heesewijk JP. The effects of dynamic isolated lumbar extensor training on lumbar multifidus functional cross‐sectional area and functional status of patients with chronic nonspecific low back pain. Spine 2012;37:E1651‐8. [DOI] [PubMed] [Google Scholar]
Williamson 2008 {published data only}
- Williamson W. Effect of supervised and directed exercise on low back pain and functional activity. Dissertation.. Oklahoma State University, Stillwater, Oklahoma: Oklahoma State University; 2008:118.
Xueqiang 2012 {published data only}
- Xueqiang W, Jiejiao Z, Xia B, Jing L. Effect of core stability training on patients with chronic low back pain. HealthMED 2012;6:759. [Google Scholar]
Yang 2010 {published data only}
- Yang EJ, Park WB, Shin HI, Lim JY. The effect of back school integrated with core strengthening in patients with chronic low‐back pain. American Journal of Physical Medicine & Rehabilitation 2010;89:744‐54. [DOI] [PubMed] [Google Scholar]
Yelland 2004 {published data only}
- Yelland MJ, Glasziou PP, Bogduk N, Schluter PJ, McKernon M. Prolotherapy injections, saline injections, and exercises for chronic low‐back pain: a randomized trial. Spine 2004;29:9‐16. [DOI] [PubMed] [Google Scholar]
Yoo 2012 {published data only}
- Yoo YD, Lee YS. The effect of core stabilization exercises using a sling on pain and muscle strength of patients with chronic low back pain. Journal of Physical Therapy Science 2012;24:671‐4. [Google Scholar]
You 2014 {published data only}
- You JH, Kim SY, Oh DW, Chon SC. The effect of a novel core stabilization technique on managing patients with chronic low back pain: a randomized, controlled, experimenter‐blinded study. Clinical Rehabilitation 2014;28:460‐9. [DOI] [PubMed] [Google Scholar]
Zhang 2015 {published data only}
- Zhang Y, Tang S, Chen G, Liu Y. Chinese massage combined with core stability exercises for nonspecific low back pain: a randomized controlled trial. Complementary Therapies in Medicine 2015;23:1‐6. [DOI] [PubMed] [Google Scholar]
Additional references
Airaksinen 2006
- Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber‐Moffett J, Kovacs F, et al. European guidelines for the management of chronic nonspecific low back pain. European Spine Journal 2006;15(Suppl 2):192‐300. [DOI] [PMC free article] [PubMed] [Google Scholar]
Alaranta 1993
- Alaranta H, Tallroth K, Soukka A, Heliovaara M. Fat content of lumbar extensor muscles and low back disability: a radiographic and clinical comparison. Journal of Spinal Disorders 1993;6:137‐40. [PubMed] [Google Scholar]
Balshem 2011
- Balshem H, Helfand M, Schünemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines. 3. Rating the quality of evidence. Journal of Clinical Epidemiology 2011;64:401‐6. [DOI] [PubMed] [Google Scholar]
Boutron 2005
- Boutron I, Estellat C, Ravaud P. A review of blinding in randomized controlled trials found results inconsistent and questionable. Journal of Clinical Epidemiology 2005;58:1220‐6. [DOI] [PubMed] [Google Scholar]
Brumit 2013
- Brumit J, Matheson JW, Meira EP. Core stabilization exercises prescription, part 2: a systematic review of motor control and general (global) exercise rehabilitation approaches for patients with low back pain. Sports Health 2013;5:510‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bystrom 2013
- Bystrom MG, Rasmussen‐Barr E, Grooten WJA. Motor control exercise reduces pain and disability in chronic and recurrent low back pain. Spine 2013;38:E350‐8. [DOI] [PubMed] [Google Scholar]
Choi 2010
- Choi BK, Verbeek JH, Tam WW, Jiang JY. Exercises for prevention of recurrences of low‐back pain. Cochrane Database of Systematic Reviews 2010, Issue 1. [DOI: 10.1002/14651858.CD006555.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cholewicki 2005
- Cholewicki J, Silfies SP, Shah RA, Greene HS, Reeves NP, Alvi K, et al. Delayed trunk muscle reflex responses increase the risk of low back injuries. Spine 2005;30:2614‐20. [DOI] [PubMed] [Google Scholar]
Costa 2012
- Costa LOP, Hancock M, Maher CG, Ostelo RWJG, Cabral CMN, Menezes Costa LD. Pilates for low‐back pain. Cochrane Database of Systematic Reviews 2012, Issue 12. [DOI: 10.1002/14651858.CD010265] [DOI] [Google Scholar]
Duffy 2014
- Duffy S, Misso K, Noake C, Ross J, Stirk L. Supplementary searches of PubMed to improve currency of MEDLINE and MEDLINE In‐Process searches via OvidSP. Poster presented at the UK InterTASC Information Specialists' Sub‐Group (ISSG) Workshop; accessed 6.8.14. Available from: https://medicine.exeter.ac.uk/media/universityofexeter/medicalschool/research/pentag/documents/Steven_Duffy_ISSG_Exeter_2014_poster_1.pdf. York: Kleijnen Systematic Reviews Ltd, 2014.
Ferreira 2006
- Ferreira PH, Ferreira ML, Maher CG, Herbert RD, Refshauge K. Specific stabilisation exercise for spinal and pelvic pain: a systematic review. Australian Journal of Physiotherapy 2006;52:79‐88. [DOI] [PubMed] [Google Scholar]
Furlan 2009
- Furlan AD, Pennick V, Bombardier C, Tulder M, Editorial Board, Cochrane Back Review Group. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine 2009;34:1829‐41. [DOI: 10.1097/BRS.0b013e3181b1c99f] [DOI] [PubMed] [Google Scholar]
Furlan 2015
Hancock 2007
- Hancock MJ, Maher CG, Latimer J, Spindler MF, McAuley JH, Laslett M, et al. Systematic review of tests to identify the disc, SIJ or facet joint as the source of low back pain. European Spine Journal 2007;16:1539‐50. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hauggaard 2007
- Hauggaard A, Persson A. Specific spinal stabilisation exercises in patients with low back pain ‐ a systematic review. Physical Therapy Reviews 2007;12:233‐48. [Google Scholar]
Hayden 2005
- Hayden JA, Tulder MW, Malmivaara A, Koes BW. Exercise therapy for treatment of non‐specific low back pain. Cochrane Database of Systematic Reviews 2005, Issue 3. [DOI: 10.1002/14651858.CD000335.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hayden 2005b
- Hayden JA, Tulder MW, Tomlinson G. Systematic review: strategies for using exercise therapy to improve outcomes in chronic low back pain. Annals of Internal Medicine 2005;142:776‐85. [DOI] [PubMed] [Google Scholar]
Henschke 2008
- Henschke N, Maher CG, Refshauge KM, Herbert RD, Cumming RG, Bleasel J, et al. Prognosis in patients with recent onset low back pain in Australian primary care: inception cohort study. BMJ 2008;337:a171. [DOI] [PMC free article] [PubMed] [Google Scholar]
Herrington 2005
- Herrington L, Davies R. The influence of Pilates training on the ability to contract the transversus abdominis muscle in asymptomatic individuals. Journal of Bodywork and Movement Therapies 2005;9:52‐7. [Google Scholar]
Hides 1994
- Hides JA, Stokes MJ, Saide M, Jull GA, Cooper DH. Evidence of lumbar multifidus muscle wasting ipsilateral to symptoms in patients with acute/subacute low back pain. Spine 1994;19:165‐72. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [updated March 2011]. The Cochrane Collaboration, 2011. www.cochrane‐handbook.org.
Hodges 1996
- Hodges PW, Richardson CA. Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine 1996;21:2640‐50. [DOI] [PubMed] [Google Scholar]
Hodges 1997
- Hodges PW, Richardson CA. Relationship between limb movement speed and associated contraction of the trunk muscles. Ergonomics 1997;40:1220‐30. [DOI] [PubMed] [Google Scholar]
Hodges 1998
- Hodges PW, Richardson CA. Delayed postural contraction of transversus abdominis in low back pain associated with movement of the lower limb. Journal of Spinal Disorders 1998;11:46‐56. [PubMed] [Google Scholar]
Hodges 2003
- Hodges PW. Core stability exercise in chronic low back pain. Orthopedic Clinics of North America 2003;34:245‐54. [DOI] [PubMed] [Google Scholar]
Koes 2010
- Koes BW, Tulder M, Lin CW, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non‐specific low back pain in primary care. European Spine Journal 2010;19:2075‐94. [DOI] [PMC free article] [PubMed] [Google Scholar]
Macdonald 2011
- Macdonald DA, Dawson AP, Hodges PW. Behavior of the lumbar multifidus during lower extremity movements in people with recurrent low back pain during symptom remission. Journal of Orthopaedic & Sports Physical Therapy 2011;41:155‐64. [DOI] [PubMed] [Google Scholar]
Macedo 2009
- Macedo LG, Maher CG, Latimer J, McAuley JH. Motor control exercise for persistent, nonspecific low back pain: a systematic review. Physical Therapy 2009;89:9‐25. [DOI] [PubMed] [Google Scholar]
Macedo 2010
- Macedo LG, Smeets RJ, Maher CG, Latimer J, McAuley JH. Graded activity and graded exposure for persistent nonspecific low back pain: a systematic review. Physical Therapy 2010;90:860‐79. [DOI] [PubMed] [Google Scholar]
Machado 2010
- Machado LA, Maher CG, Herbert RD, Clare H, McAuley JH. The effectiveness of the McKenzie method in addition to first‐line care for acute low back pain: a randomized controlled trial. BMC Medicine 2010;8:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Menezes Costa 2009
- Menezes Costa LC, Maher CG, McAuley JH, Hancock MJ, Herbert RD, Refshauge KM, et al. Prognosis for patients with chronic low back pain: inception cohort study. BMJ 2009;339:b3829. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mueller 2007
- Mueller PS, Montori VM, Bassler D, Koenig BA, Guyatt GH. Ethical issues in stopping randomized trials early because of apparent benefit. Annals of Internal Medicine 2007;146:878‐81. [DOI] [PubMed] [Google Scholar]
Murray 2012
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability‐adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990‐2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet 2012;380:2197‐223. [DOI] [PubMed] [Google Scholar]
Newcomer 2000
- Newcomer KL, Laskowski ER, Yu B, Johnson JC, An KN. Differences in repositioning error among patients with low back pain compared with control subjects. Spine 2000;25:2488‐93. [DOI] [PubMed] [Google Scholar]
Rackwitz 2006
- Rackwitz B, Bie R, Limm H, Garnier K, Ewert T, Stucki G. Segmental stabilizing exercises and low back pain. What is the evidence? A systematic review of randomized controlled trials. Clinical Rehabilitation 2006;20:553‐67. [DOI] [PubMed] [Google Scholar]
Radebold 2000
- Radebold A, Cholewicki J, Panjabi MM, Patel TC. Muscle response pattern to sudden trunk loading in healthy individuals and in patients with chronic low back pain. Spine 2000;25:947‐54. [DOI] [PubMed] [Google Scholar]
Roland 2000
- Roland M, Fairbank J. The Roland‐Morris Disability Questionnaire and the Oswestry Disability Questionnaire. Spine 2000;25:3115‐24. [DOI] [PubMed] [Google Scholar]
Roy 1989
- Roy SH, Luca CJ, Casavant DA. Lumbar muscle fatigue and chronic lower back pain. Spine 1989;14:992‐1001. [DOI] [PubMed] [Google Scholar]
Rubinstein 2012
- Rubinstein SM, Terwee CB, Assendelft WJJ, Boer MR, Tulder MW. Spinal manipulative therapy for acute low‐back pain. Cochrane Database of Systematic Reviews 2012, Issue 9. [DOI: 10.1002/14651858.CD008880.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Stephens 2007
- Stephens B, Gross DP. The influence of a continuum of care model on the rehabilitation of compensation claimants with soft tissue disorders. Spine 2007;32:2898‐904. [DOI] [PubMed] [Google Scholar]
van Dieen 2003
- Dieen JH, Selen LP, Cholewicki J. Trunk muscle activation in low‐back pain patients, an analysis of the literature. Journal of Electromyography & Kinesiology 2003;13:333‐51. [DOI] [PubMed] [Google Scholar]
van Tulder 1997
- Tulder MW, Koes BW, Bouter LM. Conservative treatment of acute and chronic nonspecific low back pain. A systematic review of randomized controlled trials of the most common interventions. Spine 1997;22:2128‐56. [DOI] [PubMed] [Google Scholar]
van Tulder 2003
- Tulder M, Furlan A, Bombardier C, Bouter L, Editorial Board of the Cochrane Collaboration Back Review Group. Updated method guidelines for systematic reviews in the Cochrane Collaboration Back Review Group. Spine 2003;28(12):1290‐9. [DOI] [PubMed] [Google Scholar]
van Tulder 2006
- Tulder M, Becker A, Bekkering T, Breen A, Real MT, Hutchinson A, et al. Chapter 3. European guidelines for the management of acute nonspecific low back pain in primary care. European Spine Journal 2006;15(Suppl 2):S169‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Williams 2010
- Williams CM, Maher CG, Hancock MJ, McAuley JH, McLachlan AJ, Britt H, et al. Low back pain and best practice care: a survey of general practice physicians. Archives of Internal Medicine 2010;170:271‐7. [DOI] [PubMed] [Google Scholar]