

Abstract
Oro-facial-digital syndrome (OFD) is a disorder with varied inheritance patterns. They deal mainly with abnormalities of the face, digits, i.e., fingers and toes, and oral cavity. Hypoplasia of nasal alar cartilage, broad nasal bridge, frontal bossing, and micrognathia are the common facial abnormalities observed in its multiple potential forms. Among the oral features, lobulated tongue, multiple frenulae, and cleft lip/palate are the common findings. The subject presented in our case manifested cleft of the hard palate at the time of presentation, along with other diverse features, which could not match any of the defined OFD types in literature. Furthermore, follow-up of the infant observed closure of the palate spontaneously, without any intervention. Hence, the purpose is to add to the knowledge the typical features of this unspecified type of OFD, along with this unique unprompted cleft palate closure, which aroused the need of close watch in such cases.
Keywords: Broad toes, cleft palate, hypertelorism, oro-facial-digital syndrome, spontaneous cleft palate fusion
Introduction
Oro-facial-digital syndrome (OFD) represents distinctive genetic anomalies affecting the development of the oral cavity, facial region and digits. There are multiple reported variants with characteristic features occasionally overlapping with other syndromes.[1] Diagnosis of a particular subtype is difficult considering the varied presentation of the syndrome. When it comes to the clinical presentation of the oral cavity, cleft palate is the most commonly observed feature, wherein bone regeneration post its surgical closure has been documented in the literature.[2] However, spontaneous closure of cleft palate without any intervention has not been reported in the English literature. PubMed, Scopus, Cochrane CENTRAL database literature search for “spontaneous closure of cleft palate,” “cleft palate closure in OFD syndrome” and “palate and OFD syndrome,” followed by the reading of the pertinent articles could not yield any results describing spontaneous cleft palate closure. Furthermore, the clinical feature seen in our reported case does not fit into any of the defined types. Hence, we report this rare case as an “unspecified type” of OFD syndrome which will help in further delineating its growing variants.
Case Report
A 7-month-old child reported to the oral and maxillofacial surgery department with a complaint of difficulty in swallowing along with recurrent aspiration pneumonia with mildly delayed milestones. The child was born preterm (34 weeks) out of nonconsanguineous marriage. There was no reported family history of genetic disorders. Parents gave the history of exclusive breastfeeding until 1.5 months followed by oro-gastric tube feed. Facial features depicted no facial asymmetry but increased inter-orbital distance (hypertelorism), telecanthus but normal slanting palpebral fissures, frontal bossing, sparse medial two-third of eyebrows, broad nose with the flattened nasal bridge, thin upper lip with normal margins, smooth and long philtrum, low set and small ears with no hearing loss and micro-retrognathia [Figure 1a]. Intra-orally high arched U-shaped palate associated with a cleft up the posterior hard palate was observed in the midline [Figure 2a], with no cleft lip. A lobate tongue was found along with multiple nontender soft nodules over its dorsal surface [Figure 1b], with no oral adhesions and normal oral frenulae. Alveolar ridges were thickened. Evaluation of the digits revealed bilateral broad great toes without bifid nails or syndactyly with respect to feet, while hands had tapering fingers [Figures 1c, d and 2b]. Ultrasound abdomen, echocardiogram , and computed tomography of the brain revealed no significant abnormalities.
Figure 1.

(a) Frontal facial picture depicting increased inter-orbital distance (hypertelorism), broad nose, flattened nasal bridge, thin upper lip, smooth philtrum and low set ears. (b) Lobate tongue was found along with multiple nontender soft nodules over its dorsal surface. (c and d) No abnormality was detected with respect to hands except for tapering fingers
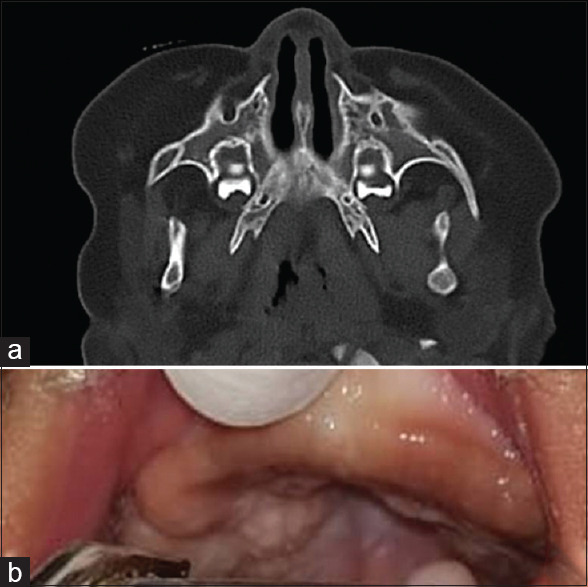
Figure 2.
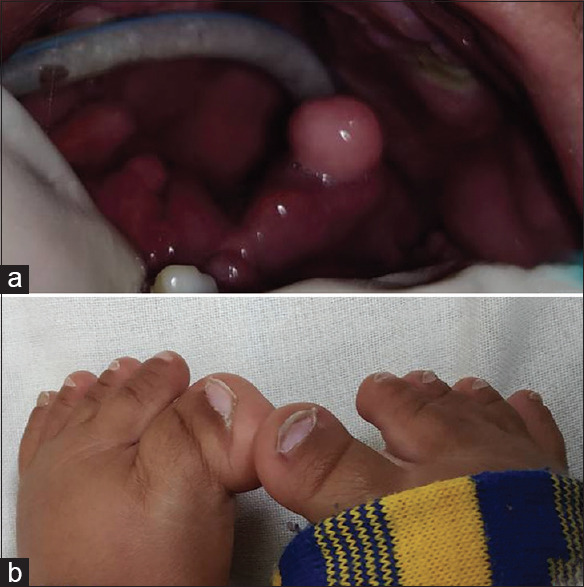
(a) Cleft hard palate can be observed along with oro-gastric tube in situ. (b) Bilateral broad great toes with respect to feet
The patient was kept on follow-up for consideration of palatal closure at 9–18 months of age. However, the spontaneous fusion of cleft palate was observed at the age of 1 year, which was confirmed with radiological investigations [Figure 3a and b].
Figure 3.
(a) Axial section of noncontrast computed tomography of face showing fusion of cleft palate. (b) Fusion of the cleft palate can be observed clinically
Discussion
OFD syndrome is a distinct disease comprising a heterogeneous group of genetic disorders affecting the oral cavity development along with associated facial and digital anomalies.[3] It was first described in 1954 by Papillon-League and Psaume as “orofacial dysostosis” but with time the term “OFD syndrome” was preferred due to the involvement of various tissues other than bone.[4] The estimated incidence of OFD's is 1 in 50,000–2,50,000 newborns.[5] Literature has reported various forms of this syndrome, but its full spectrum is still not understood. Type I has shown maximum occurrence rate and autosomal recessive being the most common mode of inheritance amongst its variants.[6] Table 1 enumerates the types of OFD's along with their characteristic features and associated systemic abnormalities based on OMIM search.
Table 1.
Enumerates the types of oro-facial-digital syndrome along with their characteristic features and associated systemic abnormalities based on OMIM search
| Clinical features | Our case | OFD I | OFD II | OFD III | OFD IV | OFD V | OFD VI | OFD VII | OFD VIII | OFD IX | OFD X | OFD XI | OFD XII | OFD XIII | OFD XIV | OFD XV | OFD XVI | OFD XVII |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Thickened alveolar ridges | + | + | ||||||||||||||||
| Abnormal dentition | + | + | + | + | + | + | ||||||||||||
| Lobate tongue | + | + | + | + | + | + | + | + | + | + | + | + | + | |||||
| Hypertelorism | + | + | + | + | + | + | + | |||||||||||
| Cleft palate | + | + | + | + | + | + | + | + | + | |||||||||
| Broadnose/flatnasalbridge | + | + | + | + | + | |||||||||||||
| Retrognathia | + | + | + | + | + | |||||||||||||
| Broad nose | + | + | + | |||||||||||||||
| Conductive hearing loss | + | + | + | + | + | |||||||||||||
| Recurrent aspiration pneumonia | + | + | ||||||||||||||||
| Hypoplasia/aplasia of epiglottis | + | + | + | + | ||||||||||||||
| Syndactyly | + | + | ||||||||||||||||
| Clinodactyly | + | + | ||||||||||||||||
| Brachydactly | + | + | + | |||||||||||||||
| Oligodactyly | + | |||||||||||||||||
| Preaxial polydactyly hands | + | + | + | + | + | |||||||||||||
| Postaxial polydactyly hands | + | + | + | + | + | + | + | + | + | + | ||||||||
| Preaxial polydactyly feets | + | + | + | + | + | |||||||||||||
| Postaxial polydactyly feet | + | + | + | + | + | + | + | |||||||||||
| Bilateral duplication of halluces | + | + | + | + | ||||||||||||||
| CNS involvement | + | + | + | + | + | + | + | + | + | + | + | + | + | + | + | |||
| Mental retardation | + | + | + | + | + | + | + | + | + | |||||||||
| Neuromuscular disturbance | + | + | + | + | + | |||||||||||||
| Kidney disorders | + | + | + | + | + | + | + | |||||||||||
| Cardiac defects | + | + | + | + | + | + | + | + | + | |||||||||
| Hypoplastic genitalia | + | + | + | + | ||||||||||||||
| Short limbs | + | + | + | |||||||||||||||
| Ophthalmic abnormalities | + | + | + | + | + | |||||||||||||
| Rib and skeletal deformities | + | + | + | + | + | + | ||||||||||||
| Tibial dysplasia | + | + | ||||||||||||||||
| OMIM number | #311200 | %252100 | %258850 | #258860 | #615464 | #277170 | 608518 | %300484 | %258865 | 165590 | %612913 | #615948 | #617127 | #617563 | #617926 |
OFD: Oro-facial-digital; CNS: Central Nervous System ; OMIM: Online Mendelian Inheritance in Man; OFDXII: Moran- Barroso syndrome; OFD XIII: Degner Syndrome
Features like abnormal oral frenula and cleft lip are common in almost every type of OFD. However, certain features are found characteristic to a particular type like alveolar and lingual clefting, granular facial appearance, hypoplasia of alar cartilages, diffuse alopecia, dry hair, liver and pancreatic disorder in type I; angular alveolar process, talon cusp and bifid uvula in type II; talipes (club foot) in type IV; frontal bossing in type V (also in type XIV and type XVII rarely); hexadactyly in type VI; bifid tongue (also in type XIV and type XVII) and pre-auricular skin tags in type VII; bifid nasal tip in type VIII; radial shortening and fibular agenesis in type X; nasopharyngeal hairy poly, psychiatric symptoms and vertebral anomalies in type XI; frontal narrowing, skull deformity, rotated ears, epispadias, skeletal ciliopathy, trident acetabula and short webbed neck in type XIV; respiratory difficulty in type XV and type XVI; short palpebral fissures and low set ears in type XVI; bifid thumbs and toes and low weight in type XVII.
The clinical feature seen in our reported case does not fit into any of the defined types of OFD. It can be differentiated from Binder syndrome as nasal bones are not abnormally positioned nor the nasal spine is absent, there is no atrophy of nasal mucosa, absence of maxillary hypoplasia and frontal sinus is present.[7] Although the molecular basis of all types of OFD's are not known till date, molecular study, in this case, was not done due to personal reasons. Considering the varied presentation of this syndrome, diagnosing a particular subtype is difficult. However, Bruel et al. did 15 years of research on these syndromes and suggested that they are a subgroup of ciliopathies.[8] They proposed a new classification into three main subtypes rendering the previous classification obsolete for wide molecular and clinical heterogeneity leading to various overlapping features.
Cleft palate or cleft lip is a common intra-oral finding observed in OFD's. However, to our knowledge, this is the only case report documenting spontaneous fusion of cleft palate with time without any surgical intervention. It could be speculated that palatal shelves retained the innate force which came into action at a later developmental stage leading to spontaneous fusion. No genetic or molecular basis could be ascertained for the above.
It is also important that a frequent follow-up and multidisciplinary approach is required for monitoring such cases and its complications.[9] Family counseling should be provided to the parents regarding such syndromes. Parents, in this case, were counseled about 25% recurrence risk associated with each pregnancy. They were also educated about the possible antenatal diagnosis of cleft palate and digital anomalies to rule out syndromic malformations. Furthermore, dental care of such cases should only cater to urgent needs, as its management is challenging.[10]
The above case does not fall into any defined types of OFD syndrome. Hence, this report further delineates its growing variants along with presenting a rare spontaneous cleft palate fusion which has never been reported before. Thus, if not urgent, we recommend a close watch on such cases so that such speculation can be proved in the coming future. Furthermore, it can help reduce the number of surgical interventions required in these syndromes.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the legal guardian has given his consent for images and other clinical information to be reported in the journal. The guardian understands that names and initials will not be published and due efforts will be made to conceal patient identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Horlenko O, Lenchenko A, Kossey G, Tomey A, Debretseni O. Oral-facial-digital syndrome Type I (clinical case) Georgian Med News. 2018;285:47–51. [PubMed] [Google Scholar]
- 2.Scheuermann M, Vanreusel I, Van de Casteele E, Nadjmi N. Spontaneous bone regeneration after closure of the hard palate cleft: A literature review. J Oral Maxillofac Surg. 2019;77:1074.e1. doi: 10.1016/j.joms.2018.12.018. [DOI] [PubMed] [Google Scholar]
- 3.Belengeanu V, Marian D, Hosszu T, Ogodescu AS, Belengeanu AD, Samoilă C, et al. A comprehensive evaluation of an OFDI syndrome from child to teenager. Rom J Morphol Embryol. 2019;60:697–706. [PubMed] [Google Scholar]
- 4.Dave KV, Patel SC, Dudhia BB, Panja P. Orofacial digital syndrome. Indian J Dent Res. 2013;24:132–5. doi: 10.4103/0970-9290.114920. [DOI] [PubMed] [Google Scholar]
- 5.Dhull KS, Acharya S, Mohanty M, Dhull RS, Panda S. Oro-facial-digital syndrome type 1: A case report. J Indian Soc Pedod Prev Dent. 2014;32:152–5. doi: 10.4103/0970-4388.130980. [DOI] [PubMed] [Google Scholar]
- 6.Kilinc D, Ozsarp E. Papillon-Leáge and psaume syndrome patient with multiple dental and orofacial anomalies. Niger J Clin Pract. 2019;22:872–6. doi: 10.4103/njcp.njcp_451_18. [DOI] [PubMed] [Google Scholar]
- 7.Bhatt Y, Vyas K, Tandale M, Panse N, Bakshi H, Srivastava R. Maxillonasal dysplasia (Binder's syndrome) and its treatment with costal cartilage graft: A follow-up study. Indian J Plast Surg. 2008;41:151–9. doi: 10.4103/0970-0358.44925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bruel AL, Franco B, Duffourd Y, Thevenon J, Jego L, Lopez E, et al. Fifteen years of research on oral-facial-digital syndromes: From 1 to 16 causal genes. J Med Genet. 2017;54:371–80. doi: 10.1136/jmedgenet-2016-104436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Minervini G, Romano A, Petruzzi M, Maio C, Serpico R, Di Stasio D, et al. Oral-facial-digital syndrome (OFD): 31-year follow-up management and monitoring. J Biol Regul Homeost Agents. 2018;32:127–30. [PubMed] [Google Scholar]
- 10.Chhabra N, Chhabra A, Tandon S. Orofacial manifestations and dental considerations in association with Varadi-Papp syndrome: Report of a rare case. Eur Arch Paediatr Dent. 2016;17:65–70. doi: 10.1007/s40368-015-0193-9. [DOI] [PubMed] [Google Scholar]