

Abstract
Real‐world evidence (RWE) is an emerging scientific discipline which is being increasingly utilized for decision making on prescription‐only medicines. However, there has been little focus to date on the application of RWE within the nonprescription sector. This paper reviews the existing and potential applications of RWE for nonprescription medicines, using the nonprescription medicine life cycle as a framework for discussion. Relevant sources of real‐world data (RWD) are reviewed and compared with those available for prescribed medicines. Existing life‐cycle data gaps are identified where RWE is required or where use of RWE can complement data from randomized controlled trials. Published RWE examples relating to nonprescription medicines are summarized, and potential relevant future sources of RWD discussed. Challenges and limitations to the use of RWE on nonprescription medicines are discussed, and recommendations made to promote optimal and appropriate use of RWE in this sector. Overall, RWE currently plays a key role in specific phases of the nonprescription medicine life cycle, including reclassification and postmarketing safety surveillance. The increasing availability of patient‐generated health data is likely to further increase the utilization of RWE to aid decision making on nonprescription medicines.
INTRODUCTION
Nonprescription medicines (also referred to as “over‐the‐counter” or “OTC” medicines) may legally be purchased without a doctor’s prescription and are used without medical supervision. As a consequence of their wide availability and rapid accessibility without the need for medical consultation, nonprescription medicines are a fundamentally important aspect of self‐care. Responsible self‐medication frees primary care resources to address more complex issues, empowers consumers, and is associated with important societal, public health and economic benefits. 1 , 2 , 3
Real‐world evidence (RWE) is an emerging scientific discipline in health care, increasingly used to aid licensing and access decisions for prescription medicines. 4 , 5 This review considers the role of RWE in aiding decision making for nonprescription medicines, with a focus on the European Union and the United States. The review highlights how the inherent utilization of nonprescription medicine influences the available sources of real‐world data (RWD), and discusses the unique challenges and opportunities relating to the use of RWE on nonprescription medicines. The life cycle of nonprescription medicines is discussed and contrasted with that of prescription‐only medicines, and examples are presented where RWE has been utilized at various stages of the nonprescription medicine life cycle. Potential future relevant sources of RWD and future uses of RWE are considered, and recommendations are proposed to ensure optimal and appropriate use of RWE for nonprescription medicines in the future.
BACKGROUND
RWD is a broad term which lacks a single internationally agreed definition. 6 For the purposes of this review, RWD is defined simply as “data used for decision making that are not collected in conventional randomized controlled trials.” 7 This definition encompasses both routinely collected data as well as data derived from real‐world trials (RWTs) conducted in settings which resemble everyday practice. 6 , 8 RWE is defined here as “evidence regarding the usage and potential benefits or risk of a medical product derived from analysis of RWD.” 9
Conventional randomized controlled trials (RCTs) have high internal validity, and remain necessary for demonstrating efficacy in controlled conditions. However, RWE has higher external validity, and can therefore complement evidence derived from RCTs. 8 Routinely collected data are readily available from large and inclusive samples, enabling analysis of subpopulations and less common effects. 10 Data gathered from “real‐world” scenarios also enables understanding of outcomes when drugs are used outside the context of a controlled setting. 11 , 12 RWE can also help to fill important data gaps when traditional RCTs are not feasible or appropriate 13 , 14 and in specific settings may present a more efficient and clinically relevant alternative to traditional RCTs. 12 However, RWD is also associated with a number of important limitations compared with data derived from conventional RCTs. Real‐world datasets are often incomplete and nonstandardized, and comparisons are frequently complicated by confounding factors. 12 , 14
The use of RWE to support decision making on medicinal products is not new—RWE has been the basis of safety signal evaluation, risk management, and ongoing benefit‐risk evaluation for decades. 5 More recently, RWE on prescription medicines has been utilized in other settings at various stages of product development, including as part of new drug applications, line extensions, comparative efficacy assessments, and market access and reimbursement decisions. 5 , 13 , 15 , 16 A recent review found 27 examples of the application of RWD in regulatory approval of new drug applications or line extensions for prescription‐only medicines, dating from 1998. 4
The potential utilization of RWE in healthcare decisions for prescribed medicines has gained significant attention among industry, regulators, and professional societies. 11 , 16 , 17 , 18 However, so far, there has been comparatively little focus on the potential role of RWE for nonprescription medicines. A rapid literature search was conducted to provide an initial indication of the volume of publications relating to RWD/RWE, and to determine how many of these related to nonprescription medicines. The full search methodology is described in the Supplementary Material. Overall, 55,404 RWE publications were identified, of which only 124 (0.22%) included keywords relevant to nonprescription medicines. Inconsistency of keywords used in both RWE publications and those related to nonprescription medicines is likely to have overestimated the total number of RWE publications, and possibly underestimated the proportion of these which related to nonprescription medicines. Therefore, despite the nonprescription sector arguably being a particularly well‐placed benefit from the use of RWE (see further discussion and examples in the following paragraphs), the lack of relevant publications suggests insufficient progress has been made so far.
THE NONPRESCRIPTION MEDICINE LIFE CYCLE
It is useful to consider the potential applications of RWE through the framework of the nonprescription medicine product life cycle. This facilitates discussion of potential evidence gaps at various stages of the product life cycle and helps identify areas where RWE may fill existing evidence gaps. Figure 1 presents a simplified nonprescription medicine life cycle, and includes a prescription medicine life cycle for comparison.
FIGURE 1.
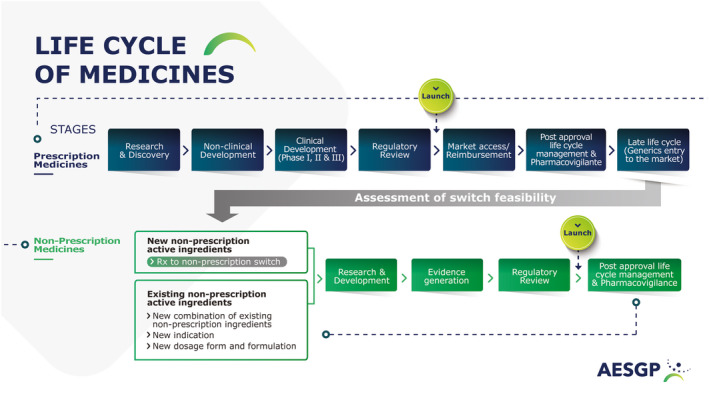
Life cycle of prescription and nonprescription medicines
In common with all medicinal products, a nonprescription product can broadly be defined by its active pharmaceutical ingredient(s) (API), unit dose, posology, dosage form, and indication. New nonprescription products reach the market through several different routes. Products containing APIs, which have only previously been available on prescription in a given territory, may become nonprescription products through a change of legal status from prescription‐only to nonprescription—commonly referred to as “prescription to OTC switch” or “Rx to OTC switch.” 19 , 20 New products containing existing nonprescription APIs are developed through combining existing active ingredients, extending or modifying indications for existing APIs, or through modifications to dose or dosage form.
It is important to note that nonprescription product authorization automatically grants direct access to the market by making products available for purchase. Therefore, in contrast to prescribed medicines, there is no additional market access barrier, and no requirement to provide data to decision makers to inform reimbursement. In common with prescribed medicines, postmarketing safety surveillance continues throughout the life of a nonprescription medicine, with the aim of ensuring a favorable ongoing benefit‐risk profile.
Specific mention should be made of the importance of consumer communication for nonprescription medicines. In contrast to prescribed medicines, where the choice of treatment primarily rests with the prescriber, the consumer is responsible for making the purchase decision. Information provided to consumers by manufacturers provides the primary source of information to enable consumers to choose the right treatment for themselves, and guide subsequent usage. It is therefore essential that the consumer receives balanced information on indications, warnings, precautions and contraindications, and risks and benefits. Regulatory‐approved product information, including the package label and leaflet, provides the main source of factual information on nonprescription medicines. Unlike prescribed medicines, for which direct‐to‐consumer (DTC) advertising is prohibited in most countries, additional communication may be provided to consumers of nonprescription medicines. This information, which must be consistent with the approved product information, may be informational, educational, and/or promotional. The ability to inform the consumer beyond the confines of regulatory‐approved factual information enables richer and more varied communication between the manufacturer and consumer. Product claims may inform the consumer of specific benefits in terms of (for example) speed of action or efficacy, whereas educational campaigns may help to dispel common myths about treatment 21 or highlight the impact of conditions and / or treatment on quality of life. Information derived from RWE is often useful to inform factual, educational, and promotional consumer communication.
REAL‐WORLD EVIDENCE IN THE CONTEXT OF NONPRESCRIPTION MEDICINES
Nonprescription medicines have an established efficacy and safety profile and are used without medical supervision by a broad population to manage a wide variety of health conditions. Therefore, in theory, these medicines would appear well suited for real‐world research. However, a number of important differences exist between prescription and nonprescription medicines in terms of the sources of RWD and the unmet evidence needs where RWE could potentially be utilized. These differences bring unique challenges in utilizing RWE for nonprescription medicines, but also opens up additional opportunities where RWE may be particularly relevant and help to address data gaps. Although different to those which exist for prescribed medicines, some of the unmet data needs within the nonprescription sector can arguably be best addressed through RWE.
Conventional sources of RWD include electronic health records (EHRs), patient registries, and claims databases 5 , 12 , 14 , 16 , 22 , 23 (Table 1). A number of these RWD sources are not available for nonprescription medicines due to the nature of how these medicines are obtained and used, and the conditions they are used to treat. The vast majority of nonprescription medicines are indicated for short‐term use for the treatment of nonserious, self‐limiting conditions. 24 By definition, consumers obtain non‐prescription medicines without a prescription or doctor consultation, and, in many cases, purchases occur within general stores. Even when nonprescription medicines are obtained through a pharmacy, details relating to the consumer, condition, product, and outcome are not routinely recorded. 24 , 25 As a result, EHRs are unlikely to capture most data relating to exposure to nonprescription medicines, or information on outcomes associated with their use. Similarly, most administrative claims databases would not capture information on nonprescription medicines as these would not be subject to reimbursement through health insurance. Overall, in contrast to prescription‐only medicines, the wealth of information on the real‐world use of nonprescription medicines is largely uncaptured.
TABLE 1.
Comparison of principal RWD sources
| Prescription‐only medicines | Nonprescription medicines | |
|---|---|---|
| Spontaneous adverse event reporting | ☑ | ☑ |
| Real‐world studies | ☑ | ☑ |
| Population health surveys | ☑ | ☑ |
| Social media | ☑ | ☑ |
| Patient/consumer surveys | ☑ | ☑ |
| Health apps | ☑ | ☑ |
| Electronic health records | ☑ | |
| Claims databases | ☑ | |
| Prescribing data | ☑ | |
| Patient and drug registries | ☑ | |
| Consumer grade medical devices | ☑ | |
| Consumer wearables | ☑ |
Abbreviation: RWD, real‐world data.
Despite the relative lack of specific data on nonprescription medicines in conventional RWD sources, these sources capture data which can be used for the generation of RWE relevant to the nonprescription setting. First, for products or APIs which have concurrent prescription and nonprescription availability, exposure data from prescribed products can be used to investigate a potential association with recorded adverse events. 26 Second, given that essentially all active ingredients contained in nonprescription products were previously only available through prescription, RWD from EHRs, registries, or administrative claims databases may be useful in deriving RWE which may help inform decisions on prescription to OTC switch. 27
Generating evidence from prospective real‐world studies is a particularly important area for nonprescription medicines. Given the relative paucity of routinely collected data, real‐world studies arguably represent the most important application of RWE to influence decision making on nonprescription medicines. Unlike conventional phase I–III studies, where strict supervision is required, nonprescription medicines have an established safety profile and can safely be investigated in pragmatic studies with minimal health care professional supervision. Where data are required to demonstrate appropriate self‐selection and safety when used without medical supervision as part of prescription to OTC switches, this can only be generated through studies conducted in real‐world settings. The section “Examples of RWE aiding decision‐making for non‐prescription medicines” discusses a number of published examples of real‐world studies which were conducted at various stages of the nonprescription medicine life cycle.
Patient‐generated health data (PGHD) is an emerging source of RWD which has significant potential to be utilized for RWE. PGHD has been defined as “wellness and / or health‐related data created, recorded, or gathered by individuals for themselves” 28 and includes patient health or experience data, medical and treatment history, symptoms, biometric data, lifestyle data, and patient‐reported outcomes (PROs). 29 The potential utilization of PGHD is particularly relevant for nonprescription medicines, given that consumers assume the primary role in managing their condition without healthcare professional supervision, and are also at the center of the generation and distribution of PGHD.
The demonstrated value and application of PGHD has so far been largely limited to therapy areas outside the remit of self‐care. 30 However, mobile phone sensors, electronic apps, and consumer wearables already exist which are capable of generating RWD relevant to nonprescription medicines. Such sources of data have the capability to be utilized in the future to generate data related to effectiveness, quality of life, or adherence, as part of prospective or retrospective studies.
Smartphones are now owned by up to 70% adults in some countries, and the technological capabilities of these devices has grown in line with their popularity. 28 Smartphones are capable of providing objective and automated measurements of physiological parameters and healthcare data, including data related to movement, sleep, and weight. 28 The capability for continuous audio recording means that smartphones may also be used to capture and track specific symptoms, such as a cough. 31 If end points are appropriately validated, the potential exists to conduct “virtual real‐world research” using mobile phones to generate ongoing end point data during treatment. Mobile phone apps are already widely used by consumers in areas such as smoking cessation, irritable bowel syndrome, allergy, sleep management, and weight management. 32 , 33 , 34 , 35 Many currently available apps include the ability for consumers to track symptoms, medication use, and lifestyle‐related data, potentially enabling collection of RWD and generation of RWE on effectiveness and related quality of life outcomes. 36 At least one marketed nonprescription medicine uses near field communication technology, which enables semi‐automated recording of product use data via a connected behavioral support app. 33 Specifically developed apps have already been used for study subjects to collect data within clinical studies and the wider potential to harness RWD from health apps has been recognized by a European regulatory agencies task force. 28 Consumer wearables act passively or actively to collect health data, such as activity, hydration status, energy expenditure, sleep, heart rate and rhythm, blood glucose, blood pressure, and respiratory rate. Wearables are increasingly being used, and wearable device research and development is continuously improving. 37 , 38 , 39 Wearables are capable of collecting continuous data in natural settings over long periods of time, and automated data collection can be complemented by use of digital diaries. 39 Wearable sleep monitors are an obvious example of a well‐researched technology relevant to nonprescription medicines. 40
Despite the potential value offered by PGHD, challenges exist with scaled implementation and integration into healthcare delivery for which appropriate solutions still need to be developed. Capturing and utilizing PGHD requires effort, time, and resources from consumers. Although diverse modes of tracking data allow consumers to test and select methods that work best for their needs, the diversity of data types and modes presents a challenge when managing data across multiple platforms. Interoperability between devices and platforms, or single platforms that support tracking across multiple dimensions of health, would reduce this complexity and facilitate sustained use. 41 Further challenges arise due to the lack of sensor validation, standardization of data collection, transparency of data processing assumptions, and accessibility to relevant data from consumer‐grade sensors. 42
Despite the challenges associated with utilization of PGHD, virtual studies which capture PGHD are likely to play an increasingly important role in healthcare decision making in the future. 29 , 43 , 44 Outside the formal study setting, PGHD has the potential to transform understanding of treatment usage, and impact on symptoms and daily performance. 37 , 38
AREAS WHERE RWE MAY AID DECISION MAKING FOR NONPRESCRIPTION MEDICINES
In determining the value and potential application of RWE in relation to nonprescription medicines, it is important to consider those areas where either conventional RCTs cannot address data requirements, or where RWE may present a more intuitive or efficient way of generating data to inform decision making.
Three general areas are highlighted here where RWE may play an important role—prescription to OTC switch, addressing postmarketing safety concerns, and investigating real‐world effectiveness/updating the benefit profile.
Prescription to OTC switch
Prescription to OTC switch is arguably the most important area where RWE can aid decision making for nonprescription medicines, and indeed where conventional RCTs are unable to meet some of the key data requirements. The European Union and United States criteria and data requirements for prescription to OTC switch differ, in part due to the existence of a pharmacy (“behind‐the‐counter”) category of medicines in many EU countries. In general, the condition being treated should be easily recognized by the consumer, the medicine should be safe for use without the supervision of a healthcare professional, the risk of misuse should be low, and the benefits of nonprescription availability should outweigh any associated risks. 19 , 20 , 45 In the United States, specific consumer studies are usually required to evaluate label comprehension, the ability of consumers to appropriately self‐select the product, and safety when used without health care professional supervision. 20 There is no general requirement in the European Union or the United States to (re)demonstrate efficacy as part of a switch application, unless the proposed dose, indication, or population differs from the prescribed product. 19 , 20
Defining the benefits of widened access is an important component of the decision making process for prescription to OTC switches. 1 Benefits of widened access may include improved access to effective drugs, improved clinical outcomes, improved public health, enhanced involvement of consumers in their own health care, and economic benefits. 1 Although data from conventional RCTs may inform some of these questions, existing RWD on exposure, improved public health outcomes, enhanced consumer involvement, and economic benefits are more relevant. Formal studies may not be necessary to define benefits associated with reclassification, although real‐world studies have proved useful in practice. For example, in the United States, RWD has demonstrated that nonprescription access to nicotine replacement therapy (NRT) was associated with a twofold increase of quit attempts using NRT. 46 , 47 A further study of nonprescription orlistat for weight management in a real‐world pharmacy setting demonstrated significant improvements in diet and exercise habits. 48
A number of key questions must be addressed as part of a reclassification application. These include whether consumers can accurately and easily identify the condition for which the product is indicated, whether they can make an appropriate decision on the personal suitability of the product, and whether the safety profile of the product when used unsupervised differs from when the product is used on prescription. 19 , 20 In the United States, “actual use” trials are commonly used to address some or all of these questions. Actual use trials are conducted in a simulated “real‐world” setting, with product selection occurring in a pharmacy or temporary storefront environment, following which subjects purchase and use the product at home. 49 Actual use trials are typically conducted as part of a switch program in the United States when a new therapeutic category or pharmacological class is involved.
Actual use trials are not routinely required to support reclassifications in the European Union, and the process of obtaining ethical approval for these studies has proved to be complex. 50 Perhaps as a result, there are few examples of “actual use” trials conducted outside the United States. However, there is at least one notable example of a large pharmacy‐based study which used an “actual use” design, and which illustrates the potential value of such studies in reclassification applications 51 (see section “Examples of RWE aiding decision‐making for non‐prescription medicines”).
Addressing postmarketing safety concerns
The primary use of RWD in the nonprescription sector to date has been in the area of drug safety, with respect to the collection and reporting of adverse event data. Although nonprescription medicines have usually been marketed for many years and achieved extremely wide exposure, new safety signals may rarely emerge during the “nonprescription phase” of an active ingredient. Notable examples include terfenadine (pro‐arrhythmic effects), aspirin (Reye’s syndrome), and phenylpropanolamine (hemorrhagic stroke). 52 , 53 , 54 Despite the importance of spontaneously reported safety data in identifying potential safety signals, determining the nature and strength of the potential association between nonprescription medicines and specific reported adverse events is often challenging. Furthermore, the lack of data on exposure to nonprescription medicines included in conventional RWD sources usually prevents a conventional pharmacoepidemiologic approach to investigate the potential association. 26
One approach, which has been used to investigate emergent safety signals on nonprescription medicines, relies on the co‐existence of many nonprescription ingredients in prescription and nonprescription medicines. The dose, duration of use, indication, and population for the prescribed iterations of a particular API may sometimes differ from nonprescription products containing the same API. However, the presence within EHRs, registries, and administrative claims databases of exposure data on prescribed products which contain the API in question enables a conventional pharmacoepidemiologic approach. 26 There are several inherent limitations to this approach—notably that conventional RWD sources are unlikely to reliably capture nonprescription use of the API, with the result that some “non‐exposed” individuals may actually have been exposed through nonprescription use. 26 , 55 However, in many circumstances, using RWD sources, such as prescription claims data, can provide valid estimates of association for active ingredients available as both prescription and nonprescription products. 26
Investigating real‐world effectiveness
Generating data on the real‐world effectiveness of nonprescription medicines has a number of potential applications. Evidence of real‐world effectiveness provides a way of complementing existing efficacy data which formed the basis of the original product authorization. Some established nonprescription APIs may have established efficacy through studies which would not meet modern standards, and the requirement to continually monitor the safety of marketed medicines in the absence of updated data on efficacy/effectiveness can therefore lead to a perceived imbalance in the risk‐benefit profile. This scenario presents an important challenge for decision making on nonprescription medicines, particularly when faced with new evidence of a potential safety signal. Demonstration of real‐world effectiveness of nonprescription medicines may also be valuable in situations where efficacy is established beyond doubt, but is derived from studies in which healthcare professional supervision or intervention is likely to have significantly influenced outcomes. 56
Conducting studies in real‐world settings is the only way to investigate whether efficacy demonstrated in RCTs translates into effectiveness in practice. The real‐world effectiveness of nonprescription medicines has been investigated in randomized and nonrandomized controlled studies as well as prospective uncontrolled studies. 48 , 56 , 57 , 58 In this context, controlled studies usually include comparisons with one or more active comparators, 57 , 58 whereas some uncontrolled studies have compared outcomes with those derived from uncontrolled studies in a real‐world prescription setting. 56 A further advantage of these real‐world studies is the ability to capture relevant real‐world patient‐reported outcomes, such as general health status, impact on sleep and daily activities, and quality of life, which may influence the overall benefit‐risk profile. 57
EXAMPLES OF RWE AIDING DECISION MAKING FOR NONPRESCRIPTION MEDICINES
The value of RWE in aiding decision making on nonprescription medicines can best be demonstrated through reference to specific examples. Four examples are briefly discussed here which illustrate the application of RWE throughout the nonprescription medicine life cycle.
An actual use trial involving the use of orlistat for weight management demonstrated the value of RWE within prescription to OTC switch applications in the United States and the European Union. 48 Conducted as part of a US switch program, this 3‐month, open label study investigated how orlistat was used without health care professional supervision. Adults with obesity were recruited through local newspaper advertisements and posters placed in US community pharmacies. Potential consumers responding to the advertisements were provided with an orlistat pack and invited to read the outer label. The decision to purchase the product at the intended market price was based on the consumers’ own assessment of their eligibility based on reviewing information on the outer pack, and minimal exclusion criteria were applied to ensure maximal external validity. Information on product use, weight, and adverse events was subsequently gathered through telephone interviews.
Forty percent of screened subjects purchased study medication, of which 83% used orlistat and completed at least one interview. Product usage was broadly consistent with the label directions, and subjects reported orlistat intake on a median of 90% days since enrollment, The proportion of subjects who reported following a diet plan increased from 26% at enrollment to 80% at the 14‐day interview, with 90% subjects indicating they were successful in maintaining their diet. Fifty‐one percent of the subjects reported longer or more frequent exercise during the study compared with a median increase of 30–40‐min exercise per week compared with enrollment. Ninety‐three percent of the subjects reported weight loss during the study period, with ~ 50% achieving a reduction in body weight of more than 5%. Reported adverse events were consistent with those observed in randomized placebo‐controlled studies.
Overall, the study demonstrated that orlistat can be appropriately and effectively used without medical supervision in a population of subjects, which closely reflects that who may purchase the medicine without prescription. Unsupervised use was demonstrated to result in a similar safety profile to that observed during healthcare professional supervised use in the context of RCTs. Perhaps most notable was the sustained behavioral change in diet and exercise observed in the study, demonstrating that longer‐term therapy, which demands concurrent lifestyle changes, is feasible in a nonprescription setting. Orlistat was subsequently approved by the US Food and Drug Administration (FDA) as a nonprescription drug. 59 Data from this actual use trial were also included as part of the application for a “centralized switch” in the European Union, which was approved by the Committee for Medicinal Products for Human Use (CHMP) and then endorsed by the Commission in 2009. 60
Although such studies are not routinely required for prescription to OTC switch applications in the European Union, a further example of an actual use trial illustrates their potential value outside the United States, particularly where prior exposure from prescription use has been low, and therefore significant postmarketing safety data is lacking. A study including more than 7000 subjects was conducted in the United Kingdom to provide data to accelerate the reclassification of flurbiprofen lozenges, indicated for the symptomatic relief of sore throat. 50 , 51 Subjects with sore throat were recruited via a network of 45 UK pharmacies, and randomized to receive either flurbiprofen lozenges or soluble aspirin in a 4:1 ratio. Subjects self‐determined eligibility by reading the proposed nonprescription label for flurbiprofen lozenges, and the actual label for aspirin. Pharmacists also made an independent assessment of suitability to receive the products. Given the existing prescription‐only status of flurbiprofen lozenges at the time of the study, relevant subject details were sent via fax to a remote physician, who was required to corroborate the pharmacist’s decision on suitability before the product was provided. Following provision of study medication, trained nurses conducted structured computer‐assisted telephone interviews with the subjects.
Overall, the study validated the feasibility of actual‐use studies in the United Kingdom, and demonstrated that high quality data can be generated in a real‐world pharmacy setting. Although measures of effectiveness were not reported, the study also demonstrates the potential to collect data on real‐world effectiveness using an active control as a comparator. Flurbiprofen lozenges were subsequently approved as nonprescription medicines in a number of EU countries. 61
Studies using actual use designs have also evaluated the real‐world effectiveness of NRT for smoking cessation. Although the efficacy of NRT has been established beyond doubt in multiple RCTs, most studies used significant levels of behavioral intervention not routinely available to consumers who purchase NRT without prescription. 56 The effectiveness of nonprescription NRT when used without behavioral support has therefore been questioned. 56 A number of independent studies were conducted to assess and compare smoking cessation outcomes associated with use of NRT patch and gum in “simulated over‐the‐counter” and prescription settings. 56 As the studies were conducted prior to the nonprescription availability of NRT in the United States, smokers were screened and enrolled as trial subjects, and invited to obtain NRT patch or gum via simulated purchase in pharmacies or general stores. Potential participants were provided with product labels and were allowed to choose the nicotine patch or a selection of different nicotine gum strengths. Products were subsequently used with no additional healthcare professional intervention. Smoking status was assessed according to FDA criteria through follow‐up visits after 6 weeks and 6 months. Abstinence rates in the simulated nonprescription groups were compared with smoking status assessments in smokers who had filled prescriptions for the NRT patch or gum 6 weeks or months earlier.
Among smokers using nicotine gum or patch in the simulated nonprescription setting, abstinence rates at both 6 weeks and 6 months were numerically higher compared with those using the equivalent format obtained via prescription. Compared with smokers who obtained NRT via prescription, abstinence rates were statistically significantly higher for nonprescription nicotine patch users at 6 months, and for nonprescription gum users at 6 weeks. Statistically significant differences between the groups remained after adjusting for individual differences. Adherence was notably higher for nonprescription users of both the nicotine patch and gum compared with those who used prescribed products, although abstinence rates remained numerically higher in nonprescription NRT users who reported using the product.
Although the lack of randomization was a significant limitation of these studies, the analysis provides strong evidence that NRT purchased and used without healthcare professional supervision is at least as effective as prescribed NRT. Given that widening access to NRT through nonprescription availability results in significantly increased utilization, the finding that outcomes are at least as good compared with prescribed NRT has very positive public health implications.
RWE also has valuable applications in the postmarketing phase of the nonprescription medicine life cycle. Although exposure data on nonprescription medicines is not routinely captured within EHRs, these data sources are valuable to investigate safety concerns on APIs, which are available within both prescribed and nonprescription products. One important example investigated the association between ibuprofen and severe coronavirus disease 2019 (COVID‐19) infection, following initial theoretical concerns that nonsteroidal anti‐inflammatory drugs (NSAIDS) could facilitate and / or aggravate COVID‐19. 55 Using data from the Danish National Patient Registry (DNPR), patients with a recorded diagnosis of COVID‐19 over a 3‐month period in 2020 were identified. The same source was used to identify ibuprofen prescription claims within 14 days prior to COVID‐19 diagnosis. The study outcome was a composite of severe COVID‐19 diagnosis, intensive care unit (ICU) admission, or death. Of 4002 relevant patients identified with COVID‐19 infection during the study period, 264 patients filled an ibuprofen prescription claim prior to diagnosis. As assessed by the standardized average risk ratio (SAVR), patients who filled an ibuprofen prescription claim were no more likely to meet the criteria for severe COVID‐19 than patients who did not (SAVR = 0.96).
Subsequent to the initial advice of some authorities that patients with COVID‐19 should avoid ibuprofen use, 62 the results of this and other similar studies provided further clarity on a possible causal association of ibuprofen with worsened COVID‐19 outcomes, resulting in a broad consensus that ibuprofen may be used for symptomatic relief of COVID‐19 symptoms. 63 As acknowledged by the authors, a key limitation of the study is that exposure from nonprescription ibuprofen use was not captured in the national registry, and patients who filed no ibuprofen prescription claim may still have been exposed. However, ibuprofen is likely to have been used for longer, and often in higher doses compared to nonprescription use, which is likely to mitigate any potential exposure misclassifications. A sensitivity analysis of other pharmacoepidemiologic studies on NSAIDs concluded that, in many circumstances, missing nonprescription drug exposure does not constitute a significant source of bias. 26
CONCLUSIONS
There is growing attention on the potential for RWE to fill data gaps and complement existing knowledge of the risks and benefits of drugs derived from conventional studies. However, to date, there has been very little focus on applications of RWE relating to nonprescription medicines, and relatively few relevant published examples exist of how RWE has influenced regulatory decision making.
Given that both the available sources of RWD and the evidence requirements differ from prescribed medicines, there is a need for a different approach to RWE within the nonprescription sector. In this context, RWD should be defined widely by regulators to include data generated from real‐world studies, as very few data are routinely collected on nonprescription medicines. Data from real‐world studies play a vital role in filling current data gaps and complementing existing knowledge on safety, efficacy, and benefit‐risk (including clinical trial data) during key parts of the life cycle of nonprescription medicines. Two areas in particular are highlighted where data requirements can only be met through use of RWE—reclassification and postmarketing safety surveillance. The role of RWE in these areas has been demonstrated by a number of high‐quality studies, which have provided data to inform decision making.
Given the specific data requirements for reclassification, which cannot be met through conventional RCTs, RWE from actual use trials will continue to play a key role in reclassification applications. Outside the United States, the opportunity exists to use actual use designs to accelerate switches by generating real‐world safety data, and confirming real‐world effectiveness. Although European Union reclassifications would not routinely require such data, such studies may be particularly valuable where prior exposure to the prescription‐only medicine is low.
In common with prescription medicines, postmarketing surveillance will remain the primary source of pharmacovigilance data for marketed nonprescription medicines. Where safety concerns arise on nonprescription medicines, the value of RWE approaches has been demonstrated. Safety signals relating to APIs, which are available within both prescribed and nonprescription products, can be investigated using conventional retrospective studies using data from EHRs, registries, or claims databases. A number of studies have also demonstrated the feasibility of generating high quality real‐world safety data on nonprescription products through community pharmacies in the United States and the European Union. 64 , 65 , 66
The importance of RWE in the nonprescription sector is likely to increase as new sources of RWD emerge. PGHD is a key emerging source of RWD, which may be used to generate RWE across a spectrum of settings ranging from prospective clinical trials to retrospective observational studies. 29 To date, the use of PGHD to generate RWE is largely unexplored, and has not been subject to rigorous scrutiny. 38 Therefore, the challenges of generating relevant, high quality data to support decision making should not be underestimated. However, RWD derived from PGHD has the potential to demonstrate additional benefits on real‐world impacts that are more relevant to the end‐user, and which go beyond treatment benefits captured in clinical trials.
In order to ensure the most appropriate use of RWE in the nonprescription sector, further dialogue between industry and regulatory bodies is recommended, particularly as the opportunities for utilizing RWE in the nonprescription sector increase as new RWD sources emerge. Including patient‐reported outcomes, such as quality of life, as part of the overall benefit‐risk profile for nonprescription medicines would enable a more balanced and patient‐centered assessment of the positive effects of self‐medication. Working toward a common understanding of where and how RWE could be of value in aiding decision making is critical to ensuring RWD can be leveraged appropriately.
CONFLICT OF INTEREST
E.C. is an employee of Bayer Consumer Healthcare. C.A.‐T. is an employee of AESGP, the Association of the European Self‐Care Industry, which represents the manufacturers of nonprescription medicinal products, self‐care medical devices, and food supplements in Europe. The association is funded by member companies and national member associations’ fees. M.J.F. is an employee of The Procter & Gamble Company. L.M. is an employee of Johnson & Johnson. D.T.P. is an employee of GSK Consumer Healthcare. S.L. is an employee of Sanofi‐Aventis Germany. Medical writing support was provided by Dr. James Walmsley (Snakestick).
Supporting information
Supplementary Material
ACKNOWLEDGEMENTS
The authors greatly appreciate the support from, Karen Crabbe, Health Data Policy Expert at the National Pharma Association of Belgium; Genevieve Ening, Clinical Development Schwabe Group; Andrew Steward, RWE Engagement Lead Senior Director Consumer Healthcare, Sanofi‐Aventis; Volker Spitzer Senior Director at IQVIA; Luis Rhodes Baiao, AESGP Governmental and Public Affairs Manager; Edwin Hemwall, Principal, Edwin Hemwall LLC Consulting Services and contributions from Duncan Ibbs and Kantar Health colleagues.
Csoke E, Landes S, Francis MJ, Ma L, Teotico Pohlhaus D, Anquez‐Traxler C. How can real‐world evidence aid decision making during the life cycle of nonprescription medicines? Clin Transl Sci. 2022;15:43–54. 10.1111/cts.13129
Funding information
The costs related to the completion of this review were funded by AESGP, the Association of the European Self‐Care Industry, which represents the self‐care industry sector in Europe. The association is funded by member companies and national member associations’ fees.
REFERENCES
- 1. Brass EP, Lofstedt R, Renn O. Improving the decision‐making process for nonprescription drugs: a framework for benefit‐risk assessment. Clin Pharmacol Ther. 2011;90(6):791‐803. [DOI] [PubMed] [Google Scholar]
- 2. The Association of the European Self‐Care Industry (AESGP) . The Economic and Public Health Value of Self‐Medication. 2004. https://aesgp.eu/content/uploads/2019/10/THE‐ECONOMIC‐AND‐PUBLIC‐HEALTH‐VALUE‐OF‐SELF‐MEDICATION.pdf. Accessed April 21, 2020.
- 3. Hughes CM, McElnay JC, Fleming GF. Benefits and risks of self medication. Drug Saf. 2001;24(14):1027‐1037. [DOI] [PubMed] [Google Scholar]
- 4. Bolislis WR, Fay M, Kühler TC. Use of real‐world data for new drug applications and line extensions. Clin Ther. 2020;42(5):926‐938. [DOI] [PubMed] [Google Scholar]
- 5. Cave A, Kurz X, Arlett P. Real‐world data for regulatory decision making: challenges and possible solutions for Europe. Clin Pharmacol Ther. 2019;106(1):36‐39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Makady A, de Boer A, Hillege H, et al. What is real‐world data? a review of definitions based on literature and stakeholder interviews. Value Health. 2017;20(7):858‐865. [DOI] [PubMed] [Google Scholar]
- 7. Garrison LP, Neumann PJ, Erickson DM, et al. Using real‐world data for coverage and payment decisions: the ISPOR real‐world data task force report. Value Health. 2007;10(5):326‐335. [DOI] [PubMed] [Google Scholar]
- 8. Freemantle N, Strack T. Real‐world effectiveness of new medicines should be evaluated by appropriately designed clinical trials. J Clin Epidemiol. 2010;63(10):1053‐1089. [DOI] [PubMed] [Google Scholar]
- 9. U.S. Food and Drug Administration website. https://www.fda.gov/science‐research/science‐and‐research‐special‐topics/real‐world‐evidence. Accessed April 21, 2020.
- 10. Hemkens LG, Contopoulos‐Ioannidis DG, Ioannidis JP. Routinely collected data and comparative effectiveness evidence: promises and limitations. CMAJ. 2016;188(8):E158‐E164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Joint ISPE‐ISPOR Special Task Force . https://www.ispor.org/member‐groups/task‐forces/joint‐ispe‐ispor‐special‐task‐force. Accessed April 21, 2020.
- 12. Katkade VB, Sanders KN, Zou KH. Real world data: an opportunity to supplement existing evidence for the use of long‐established medicines in health care decision making. J Multidiscip Healthc. 2018;11:295‐304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Eichler H‐G, Pignatti F, Schwarzer‐Daum B, et al. Randomized controlled trials versus real world evidence: neither magic nor myth. Clin Pharmacol Ther. 2021;109(5):1212‐1218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Sherman RE, Anderson SA, Dal Pan GJ, et al. Real‐world evidence ‐ What is it and what can it tell us? N Engl J Med. 2016;375(23):2293‐2297. [DOI] [PubMed] [Google Scholar]
- 15. Brown JS, Maro JC, Nguyen M, et al. Using and improving distributed data networks to generate actionable evidence: the case of real‐world outcomes in the Food and Drug Administration’s Sentinel system. J Am Med Inform Assoc. 2020;27(5):793‐797. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. U.S. Food and Drug Administration (FDA) . Framework for FDA’s Real‐World Evidence Program. https://www.fda.gov/media/120060/download. Accessed April 21, 2021.
- 17. EMA Regulatory Science Strategy to 2025. https://www.ema.europa.eu/en/about‐us/how‐we‐work/regulatory‐science‐strategy. Accessed April 21, 2021.
- 18. Association of the British Pharmaceutical Industry (ABPI) . Guidance: Demonstrating Value with Real World Data: a practical guide. https://www.abpi.org.uk/media/1591/2011‐06‐13‐abpi‐guidance‐demonstrating‐value‐with‐real‐world‐data.pdf. Accessed April 21, 2021.
- 19. European Commission . A guideline on changing the classification for the supply of a medicinal product for human use. Revision January 2006. https://ec.europa.eu/health/sites/health/files/files/eudralex/vol‐2/c/switchguide_160106_en.pdf. Accessed April 21, 2021.
- 20. Regulatory approaches for prescription to OTC switch. July 2 2015 https://www.fda.gov/files/drugs/published/Presentation‐‐Regulatory‐Approaches‐for‐Prescription‐to‐OTC‐Switch.pdf. Accessed April 21, 2021.
- 21. Hungin AP, Paxman L, Koenig K, et al. Prevalence, symptom patterns and management of episodic diarrhoea in the community: a population‐based survey in 11 countries. Aliment Pharmacol Ther. 2016;43:586‐595. [DOI] [PubMed] [Google Scholar]
- 22. Duke‐Margolis Center for Health Policy . White Paper: characterizing RWD quality and relevancy for regulatory purposes. https://healthpolicy.duke.edu/sites/default/files/2020‐08/Characterizing%20RWD%20for%20Regulatory%20Use.pdf. Accessed April 21, 2021.
- 23. Swift B, Jain L, White C, et al. Innovation at the intersection of clinical trials and real‐world data science to advance patient care. Clin Transl Sci. 2018;11(5):450‐460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Report of the working group on promoting good governance of non‐prescription drugs in Europe. June 2013. https://ec.europa.eu/docsroom/documents/7623?locale=en. Accessed April 21, 2021.
- 25. Kebodeaux CD. Prescription and over‐the‐counter medication record integration: a holistic patient‐centred approach. J Am Pharm Assoc. 2019;59:S13‐S17. [DOI] [PubMed] [Google Scholar]
- 26. Yood MU, Campbell UB, Rothman KJ, et al. Using prescription claims data for drugs available over‐the‐counter (OTC). Pharmacoepidemiol Drug Saf. 2007;16(9):961‐968. [DOI] [PubMed] [Google Scholar]
- 27. Pray WS, Pray GE. New statin risks and the battle for OTC status. US Pharm. 2015;40(2):12‐15. [Google Scholar]
- 28. Donegan K, Ovelgonne H, Flores G, Fuglerud P, Georgescu A. Heads of Medicines Agencies. European Medicines Agency. Social media and M‐Health data. Subgroup report. https://www.ema.europa.eu/en/documents/report/social‐media‐m‐health‐data‐subgroup‐report_en.pdf
- 29. Duke Margolis Center for Health Policy . Determining real‐world data’s fitness for use and the role of reliability. September 2019. https://healthpolicy.duke.edu/publications/determining‐real‐world‐datas‐fitness‐use‐and‐role‐reliability. Accessed April 21, 2021.
- 30. Bakker JP, Goldsack JC, Clarke M. A systematic review of feasibility studies promoting the use of mobile technologies in clinical research. NPJ Digit Med. 2019;2:47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Kvapilova L, Boza V, Dubec P, et al. Continuous sound collection using smartphones and machine learning to measure cough. Digit Biomark. 2019;3:166‐175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Cara Care website. https://cara.care. Accessed June 26, 2021
- 33. Nicorette website. https://www.nicorette.co.uk/nicorette‐quickmist‐smarttrack/12052962.html. Accessed June 26, 2021
- 34. MedApp website. https://www.f6s.com/medapplimited. Accessed June 26, 2021.
- 35. Grigsby‐Touusaint DS, Shin JC, Reeves DM, Beattie A, Auguste E, Jean‐Louis G. Sleep apps and behavioral constructs; a content analysis. Prev Med Rep. 2017;6:126‐129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Milne‐Ives M, van Velthoven MH, Meinert E. Mobile apps for real‐world evidence in health care. J Am Med Inform Assoc. 2020;27(6):976‐980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Spitzer V, Haumann E, Conus N, Kondapuram S, Ehret A. Virtual real‐world research: The new normal for consumer health claims generation. 2020. https://www.iqvia.com/‐/media/iqvia/pdfs/library/white‐papers/virtual‐real‐world‐research‐‐‐the‐new‐normal‐for‐consumer‐health‐claims‐generation.pdf
- 38. Popovic JP. Real‐world data as real‐world evidence: establishing the meaning of data as a prerequisite to determining secondary‐use value. PharmaSUG 2019 ‐ Paper RW‐310. https://www.pharmasug.org/proceedings/2019/RW/PharmaSUG‐2019‐RW‐310.pdf. Accessed April 21, 2021.
- 39. Izmailova ES, Wagner JA, Perakslis ED. Wearable devices in clinical trials: hype and hypothesis. Clin Pharmacol Ther. 2018;104(1):42‐52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. De Zambotti M, Cellini N, Goldstone A, Colrain IM, Baker FC. Wearable sleep technology in clinical and research settings. Med Sci Sports Exerc. 2019;51(7):1538‐1557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Lavallee DC, Lee JR, Austin E, et al. mHealth and patient generated health data: stakeholders perspectives on opportunities and barriers for transforming healthcare. mHealth. 2020;6:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Codella J, Partovian C, Chang H‐Y, Chen C‐H. Data quality challenge for person‐generated health and wellness data. IBM J Res Dev. 2018;62(1):3:1–3:8. [Google Scholar]
- 43. Dhruva SS, Ross JS, Akar JG, et al. Aggregating multiple real‐world data sources using a patient‐centered health‐data‐sharing platform. NPJ Digit Med. 2020;3:60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Steinhubl SR, Waalen J, Edwards AM, et al. Effect of a home‐Based wearable continuous ECG monitoring patch on detection of undiagnosed atrial fibrillation the mSToPS randomized clinical trial. JAMA. 2018;320(2):146‐155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Directive 2001/83/EC of the European Parliament and of the council . https://ec.europa.eu/health/sites/health/files/files/eudralex/vol‐1/dir_2001_83_consol_2012/dir_2001_83_cons_2012_en.pdf. Accessed April 21, 2021.
- 46. Shiffman S, Gitchell J, Pinney JM, et al. Public health benefit of over‐the‐counter nicotine medications. Tob Control. 1997;6:306‐310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Shiffman S, Sweeney CT. Ten years after the Rx to OTC switch of nicotine replacement therapy: what have we learned about the benefits and risks of non‐prescription availability? Health Policy. 2008;86:17‐26. [DOI] [PubMed] [Google Scholar]
- 48. Schwartz SM, Bansal VP, Hale C, et al. Compliance, behavior change, and weight loss with Orlistat in an over‐the‐counter setting. Obesity. 2008;16(3):623‐629. [DOI] [PubMed] [Google Scholar]
- 49. Bradford DC, McCammon DL, Page BC, et al. The actual use trial: a description of design principles and methods. SelfCare. 2010;1(4):117‐123. [Google Scholar]
- 50. Wingfield J, Gibb I. Ethical issues surrounding clinical trials in community pharmacies. Pharm J. 2001;267:693‐695. [Google Scholar]
- 51. Gibb IA, Miller K, Veltri JC, et al. Using community pharmacists to evaluate the safety of a prescription only medicine in an OTC environment: a unique method in Europe. Int J Pharm Pract. 2001;9:R10. [Google Scholar]
- 52. Lu HR, Hermans AN, Gallacher DJ. Does terfenadine‐induced ventricular tachycardia / fibrillation directly relate to its QT prolongation and Torsade do Pointes? Br J Pharmacol. 2012;166:1490‐1502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. McGovern MC, Glasgow JF, Stewart MC. Reye’s syndrome and aspirin: lest we forget. BMJ. 2001;322:1591‐1592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Kernan WN, Viscoli CM, Brass LM, et al. Phenylpropanolamine and the risk of haemorrhagic stroke. N Engl J Med. 2000;343:1826‐1832. [DOI] [PubMed] [Google Scholar]
- 55. Kragholm K, Gerds TA, Fosbøl E, et al. Association between prescribed ibuprofen and severe COVID‐19 infection: a nationwide register‐based cohort study. Clin Transl Sci. 2020;13:1103‐1107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Shiffman S, Rolf CN, Hellebusch SJ, et al. Real‐world efficacy of prescription and over‐the‐counter nicotine replacement therapy. Addiction. 2002;97:505‐516. [DOI] [PubMed] [Google Scholar]
- 57. Birring SS, Brew J, Kilbourn A, et al. Rococo study; a real‐world evaluation of an over‐the‐counter medicines in acute cough (a multicentre, randomised, controlled study). BMJ Open. 2017;7:e014112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Kardos P, Beeh KM, Sent U, et al. Characterization of differential patient profiles and therapeutic responses of pharmacy customers for four ambroxol formulations. BMC Pharmacol Toxicol. 2018;19:40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. FDA . Orlistat information. https://www.FDA.gov/drugs/postmarket‐drug‐safety‐information‐patients‐and‐providers/orlistat‐marketed‐alli‐and‐xenical‐information. Accessed April 21, 2021.
- 60. European Medicines Agency , January 2009. Assessment report for Alli. https://www.ema.europa.eu/en/documents/variation‐report/alli‐h‐c‐854‐x‐0001‐epar‐assessment‐report‐extension_en.pdf. Accessed April 21, 2021.
- 61. Reclassification of a medicine for consideration by the Medicine Classification Committee. Application for the reclassification of flurbiprofen lozenges (8.75mg flurbiprofen per lozenge) from Pharmacy Only Medicine to General Sale (Unscheduled) Medicine. https://medsafe.govt.nz/profs/class/Agendas/Agen65/Flubiprofen.pdf. Accessed April 21, 2021.
- 62. Moore N, Carleton B, Blin P, Bosco‐Levy P, Droz C. Does ibuprofen worsen COVID‐19? Drug Saf. 2020;43:611‐614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Quaglietta L, Martinelli M, Staiano A. Serious infectious events and ibuprofen administration in pediatrics : a narrative review in the era of COVID‐19 pandemic. Ital J Pediatr. 2021;47:20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64. Schulz M, Hämmerlein A, Hinkel U, Weis G, Gillissen A. Safety and usage pattern of an over‐the‐counter ambroxol cough syrup: a community pharmacy‐based cohort study. Int J Clin Pharmacol Ther. 2006;44(9):409‐421. [DOI] [PubMed] [Google Scholar]
- 65. Gauld NJ, Shaw JP. Surveillance of a recently‐switched on‐prescription medicine (Diclofenac) using a pharmacy‐based approach. Pharmacoepidemiol Drug Saf. 2000;9(3):207‐214. [DOI] [PubMed] [Google Scholar]
- 66. Sinclair HK, Bond CM, Hannaford PC. Pharmacovigilance of over‐the‐counter products based in community pharmacy: a feasible option? Pharmacoepidemiol Drug Saf. 1999;8(7):479‐491. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary Material