

Abstract
Tinnitus is associated with sensorineural hearing loss irrespective of its severity and configuration. Frequency discrimination training is a contemporary method used for the treatment of tinnitus. However, its efficacy in treating tinnitus associated with flat sensorineural hearing loss is not studied yet. The objectives were to assess (a) treatment effect across sessions on tinnitus percept using subjective questionnaires (b) association in the severity and handicap of tinnitus before and after FDT treatment. A total of 16 participants with mean age of 56 years, who had subjective tinnitus and flat sensorineural hearing loss ranging from mild to moderate were included in the study. However, only 11 participants completed the treatment regime. Each participant was provided FDT in a game format for 15 days. The Quantitative (tinnitus pitch and loudness in each session) and qualitative measurements (THI and TFI) were assessed in each participant. Friedman test revealed a significant reduction in handicap from tinnitus as reflected in THI and reduced functionality impairment from tinnitus as reflected in TFI across sessions. Besides, a significant association was observed in the Chi-square test in severity and handicap of tinnitus before and after therapy. A change in pitch and reduced loudness was noted in eight of 11 participants. Three of them had no tinnitus perception at the end of the treatment regime. The current study findings demonstrate the efficacy of FDT using a game module in treating tinnitus associated with flat sensorineural hearing loss. The perceived severity and handicap of tinnitus reduces as a function of treatment.
Keywords: Tinnitus treatment, Frequency discrimination training, Senorineural hearing loss, Subjective tinnitus
Introduction
Tinnitus is a ringing sound in the ear or head despite the absence of an acoustic event. Tinnitus is a health care burden [1], with a prevalence of 25.7% in elderly individuals above 60 years of age in the Indian population [2]. It is also reported that some of the causes of tinnitus are exposure to noise, age, and stress [3]. The primary cause of tinnitus is hearing loss [4]. The hearing loss in the frequency region of corresponding neurons is no longer excitable by the frequencies they were originally tuned to but become sensitive to neighboring frequencies because of the rewiring. This results in an over-representation of neuronal activity at the cortical level correspond to the neurons of frequencies at the edge of the sloping configuration of hearing loss [4].
A widely used clinical approach to manage tinnitus is the masking approach. Passive stimulation by a noise masks the tinnitus. But the patient hears the tinnitus sound in the absence of masking noise. Moreover, stimulation through masking noise eventually lacks interest due to monotonous stimulation and becomes boresome. Whereas, in active sound stimulation, patient participation is required to remap the maladaptive cortical map associated with tinnitus. One such active sound stimulation strategy to manage tinnitus is the frequency discrimination task (FDT) [5–8]. In FDT, attempts have been made to capture patients' motivation and attention using a gaming environment to lessen tinnitus.
The FDT in a game format was introduced with the premise to tap attention and use their working memory to encourage intrinsic motivation for sustained use [5]. The game in FDT produced measurable enjoyment in the participants and engagement with the software while carrying out the task. Previous researchers have studied the efficacy of FDT treatment using pure tones and high pass harmonic complex tone [9]. The results revealed a significant reduction in severity and handicap pertained to tinnitus in the Tinnitus Functional Index (TFI) and Tinnitus Handicap Inventory (THI) subjective measurements. The FDT is beneficial to alter tinnitus's psychoacoustic characteristics and subsequently remap the altered cortical map [9].
In FDT, the active discrimination of target frequency (1/3 octave below tinnitus pitch) from tinnitus pitch promotes change in the frequency representation of edge frequency in the sloping configuration of hearing loss. The synchronous firing of tinnitus-related neural impulses is blocked at the subconscious level, making the signal fail to reach conscious awareness at the auditory cortex. Over a period with focused attention and discriminating the target tone from the tinnitus pitch, the neurons are realized to respond to their characteristic frequency. To be specific, extending the support of undamaged neurons for the damaged neurons is stopped and subsequently reduces the tinnitus-related spontaneous neuronal activity.
The efficacy of FDT treatment is studied extensively on sloping hearing loss comorbid with tinnitus found beneficial. However, the efficacy of FDT in individuals with flat sensorineural hearing loss is yet to be comprehensively studied. It is hypothesized that even in the flat hearing loss configuration, realizing the neurons about their characteristic frequency through focused attention and discrimination can lessen the tinnitus percept. Thus, in the present study, FDT is used for fifteen days to treat the tinnitus in individuals with the flat configuration of sensorineural hearing loss. The handicap from tinnitus and the severity of tinnitus is assessed using THI and TFI subjective questionnaires. Also, the tinnitus pitch and loudness are described during the treatment program. The study investigates the effect of frequency discrimination on tinnitus percept using subjective and objective methods. The objectives are formulated as follows (a) treatment effect is compared between sessions on tinnitus percept using subjective questionnaires (b) association in the severity of tinnitus before and after FDT treatment is assessed. Similarly, the association is documented on handicap from tinnitus.
Methods
Participants
A time series research design was utilized to investigate the effect of frequency discrimantion effect on tinnitus relief. A total of 16 participants with flat mild to moderate degree of sensorineural hearing loss comorbid with unilateral tinnitus in the age range of 50–60 years (mean age years 56; SD = 3.1 years; range 9.5 years) were selected. They had normal middle ear status indicated by type ‘A’ tympanogram, and the acoustic reflex was elevated or absent depending on the degree of hearing loss. All the participants had moderate tinnitus severity and moderate handicap from tinnitus revealed in THI and TFI. The selected participants had no other neurological, psychological, and cognitive issues. Informed consent was obtained from each participant by explaining the treatment procedure and the time allocated for treatment. All procedures performed in studies involving human participants were in accordance with the institutional research committee of ethical standards. Five participants left in between the training regime due to the distance to reach the therapy center. A detailed characteristic of tinnitus and probable cause are tabulated in Table 1.
Table 1.
Details of tinnitus characteristics of each participant
| SI | Age | PTA | Tinnitus ear | Tinnitus pitch (Hz) | Loudness (SL) | THI | TFI | Probable cause |
|---|---|---|---|---|---|---|---|---|
| 1 | 55 | 53.5 | Left | 250 | 50 | Moderate | Moderate problem | Presbycusis |
| 2 | 60 | 48.3 | Left | 120 | 85 | Moderate | Moderate problem | Presbycusis |
| 3 | 50 | 55 | Right | 3000 | 55 | Moderate | Moderate problem | Presbycusis |
| 4 | 52 | 43.8 | Right | 950 | 55 | Moderate | Moderate problem | Presbycusis |
| 5 | 55 | 48.5 | Right | 400 | 60 | Moderate | Moderate problem | Presbycusis |
| 6 | 57 | 40.1 | Left | 250 | 50 | Moderate | Moderate problem | Presbycusis |
| 7 | 60 | 50.1 | Left | 2000 | 45 | Moderate | Moderate problem | Noise exposure |
| 8 | 55 | 45 | Right | 200 | 40 | Moderate | Moderate problem | Presbycusis |
| 9 | 57 | 40 | Left | 7000 | 55 | Moderate | Moderate problem | Presbycusis |
| 10 | 56 | 45.3 | Right | 1000 | 50 | Moderate | Moderate problem | Presbycusis |
| 11 | 59 | 48.3 | Left | 5000 | 40 | Moderate | Moderate problem | Noise exposure |
Quantitative Measures
Tinnitus pitch and loudness matching were performed on each of the participants. The adaptive method was adopted to assess tinnitus pitch and loudness [10]. The ear contralateral to the tinnitus was used for matching of tinnitus pitch and loudness. Loudness matching was carried out before the pitch matching. Loudness matching was performed at octave frequencies from 125 to 8000 Hz (above 8 kHz if required). For loudness matching, the initial presentation level was presented at 5 dB SL, and it was varied in the step of 1 dB until the patient was able to match the loudness. To match the pitch, a pair of loudness matched tones (in octave) were presented sequentially and instructed to report the tone closer to his/her tinnitus. This procedure continued for consecutive octave frequencies till the participant was able to match the pitch. It was ensured that the tones presented did not exceed the loudness discomfort level of the participant. Tinnitus pitch and loudness matching were assessed before the treatment (baseline) and during the treatment regime, prior to the each of the treatment sessions (treatment effect).
Qualitative Measures
The qualitative measures comprised of Tinnitus Handicap Inventory (THI) and Tinnitus Functional Index (TFI). These tests were administered before the treatment regime as a basline and every week during the treatment regime to determine the effectiveness of treatment.
Tinnitus Handicap Inventory
THI in the Kannada version, a south Indian Language was utilized in the current study [10–12]. It comprises a 25-items inventory that evaluates the functional and emotional implications of tinnitus and probes the severity of tinnitus in the study. The participant must answer each question with “yes” (4 points), sometimes (2 points), or “no” (0 points). Responses are summed to determine the patient's score, which ranges from 0 to 100 points. The patient’s total score is then compared to the THI scoring pattern to interpret tinnitus severity level. The scoring patterns are as follows 2–16 slight, 18–36 mild, 38–56 moderate, 58–76 severe, and 78–100 catastrophic.
Tinnitus Functional Index (TFI)
TFI developed by Henry et al. (2014) was utilized in the study. It comprises a 25-items inventory tool that includes eight subscales. Each item is rated using a 10-point rating scale ‘0’ represented as less affected and ‘10’ represented as extremely affected. The eight subscales are (i) the intrusiveness of tinnitus, (ii) sense of control the patient has, (iii) cognitive interference, (iv) sleep disturbance, (v) auditory issues, (vi) relaxation issues, (vii) quality of life and (viii) emotional distress. Each of the eight subscales consists of 3 items except for the Quality of life subscale, consisting of 4 items. For valid sub-scale scores, no more than 1 item should be omitted. Scores are summed from all subscales divided by the number of questions answered multiplied by 10. This procedure generates a score in the range of 0–100. A total score on TFI received from each patient was classified as—not a problem (range 0–17); small problem (range 18–31); moderate problem (range 32–53); big problem (range 54–72); and very big problem (range 73–100).
Frequency Discrimination Task (FDT): The Training Module
The frequency discrimination task was used in a game format to treat tinnitus for fifteen days. The FDT was provided for 45 min in each session. Frequency discrimination training alters the central frequency map of tinnitus by training sound discrimination near tinnitus pitch regions. It’s an activity to shift the tinnitus frequency to its neighboring frequency (in the multiples of 1/3rd octave of the tinnitus frequency) by conditioning the individual to memorize the neighboring frequency corresponding to the tinnitus pitch. Tinnitus pitch may change naturally and would lead to tonotopic reorganization at the auditory cortical level.
Stimuli Generation
The software automatically generates target and distracter stimuli based on the participant’s tinnitus pitch. The tinnitus pitch and loudness of the test ear were estimated using adaptive methods [10] in each treatment session. Pitch of the participant’s tinnitus was considered as target (T), tones with frequency 1/3rd, and 2/3rd octave below the pitch of the tinnitus was considered as distracter 1 (D1) and distracter 2, (D2), respectively. Furthermore, tones with frequency 1/3rd and 2/3rd octave above tinnitus frequency were considered distracter 3 (D3) and distracter 4 (D4). The participant's pitch was assessed before treatment to generate the target and distractor stimuli.
Target Familiarization
Each participant was made to identify the target tone (1/3rd octave below the tinnitus pitch) in the familiarization task. Familiarization of the target tone was carried out using the direction pattern mode. In the direction pattern mode, the participants are asked to locate the sound coming to either right or left, which was presented in sequence at the most comfortable level (MCL) (Fig. 1). The participants were instructed to write/tell the pattern of presentation of the stimulus. There are six combinations of patterns in which the target tone was presented to either right or left ear. Six patterns were repeated five times randomly (6 × 5 = 30 trails). In total, there were 30 sets of stimuli, where each set consisted of a pattern of presentation as follows RLR, RLL, LRR, LRL, RRL, LLR (R—Right ear and L—Left ear).
Fig. 1.

Target familiarization in frequency discrimination training page
To complete the target familiarization task, the participant has to correctly identify the pattern 70% i.e., among 30 trials the participant has to identify the target tone 21 times and or above correctly.
Discrimination Task
The discrimination task was performed after the target familiarization. The target tone intensity was played at MCL + 7 dB, and the other distracters were played at MCL. This was added as a cue to identify the target over other distracters. These stimuli were presented through iball headphone Rk25, which has a frequency response within 0.125 kHz to 10 kHz. The entire training regime was carried out in a Puzzle game format. Nine or sixteen pieces of puzzles were displayed on the personal computer to participants. Each participant was asked to identify the target sound correctly in the presence of a distractor to complete the puzzle (Fig. 2). In level 1, the target stimulus was presented with distractor D1. Pieces in the puzzle were associated with an audio file of target and distracter (D1) sounds, annotated by numbers. They were played sequentially in random order. If the target was correctly identified, the concealed grid unfurls, and the image appears. If not, the message “wrong” appears on the screen. The images used were not repeated to avoid monotonicity in the game. The game was sufficiently challenging to maintain interest and attention while being manageable to minimize fatigue. The game provided the patient with feedback regarding progress. Once the puzzle was completed, the patient was moved to the next level with a fresh puzzle. As the game level advances, the complexity increases with the number of distractors. At each level, the participant has to identify the target in the presence of distractors. A training session of three weeks was provided in a game format to lessen tinnitus percept in the study participants. Each day of the training session lasted for 30 min. End of each week of training, the qualitative measure was assessed to see the effect of training on severity ad handicap.
Fig. 2.

Puzzle game of frequency discrimination training page
Statistical Analyses
The THI data from participants across four sessions (day-1, day-5, day-10, and day-15 of post-treatment) were subjected to Friedman's test. Further, the Wilcoxon signed-rank test was conducted to see if any significance across sessions exists. Further Chi-Square test was performed on THI data to assess the association between day 1 and day15. A similar analysis was performed on the TFI data.
Results
The mean rankings of the THI between sessions were found significant [X2 (3, N = 11) = 26.39, p = 0.000] on Friedman's chi-square test. Further, a Wilcoxon signed-rank test was administered on mean rank data of THI across sessions. Except between day-1 and day-5, the mean rank of THI reduced significantly as a function of the sessions. The Z and p-value of the Wilcoxon signed-rank test for THI data are given in Table 2. The mean rank of THI across sessions is given in Fig. 3.
Table 2.
The Z and p values of Wilcoxon signed-rank test for the data of THI
| Sessions | Z value | p-value |
|---|---|---|
| Day 1–Day 5 | − 2.000 | 0.046 |
| Day 1–Day 10 | − 3.051 | 0.002 |
| Day 1–Day 15 | − 3.127 | 0.002 |
| Day 5–Day 10 | − 2.646 | 0.008 |
| Day 5–Day 15 | − 3.000 | 0.003 |
| Day 10–Day 15 | − 1.414 | 0.157 |
Fig. 3.
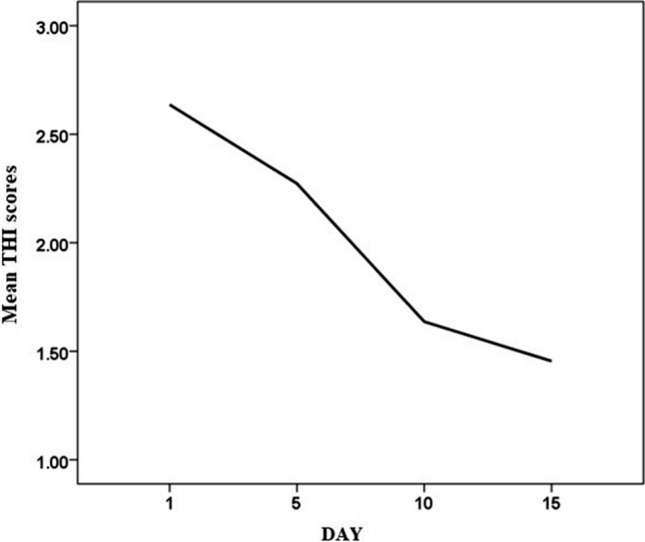
Line graph showing the mean rank of THI across sessions
A Friedman test was carried out to compare the mean rank of TFI across sections. There was a significant reduction in tinnitus functional index as a function of treatment [X2 (3, N = 11) = 26.39, p = 0.000]. Further, a Wilcoxon signed-rank test was administered on mean rank data of TFI across sessions. It was observed that the mean rank of TFI reduced as a function of the session, although there was no difference between day 1 and day 5. The Z and p-value of the Wilcoxon signed-rank test for the data of TFI are given in Table 3. The mean rank of TFI across sessions is given in Fig. 4.
Table 3.
The Z and p values of the Wilcoxon signed-rank test for the data of TFI
| Sessions | Z value | p-value |
|---|---|---|
| Day 1–Day 5 | − 2.000 | 0.046 |
| Day 1–Day 10 | − 3.051 | 0.002 |
| Day 1–Day 15 | − 3.127 | 0.002 |
| Day 5–Day 10 | − 2.646 | 0.008 |
| Day 5–Day 15 | − 3.000 | 0.003 |
| Day 10–Day 15 | − 1.414 | 0.157 |
Fig. 4.
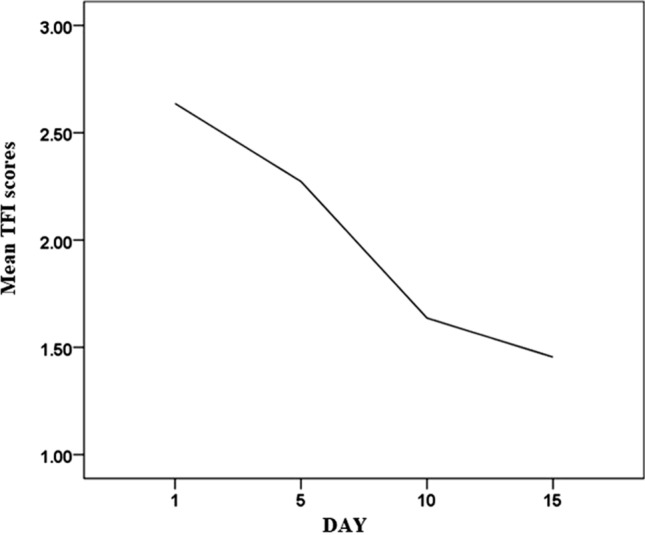
Line graph showing the mean rank of TFI across sessions
from tinnitus.
The severity of tinnitus reflected in THI on day-1 and day15 was analyzed. THI suggested that five participants experienced a change in severity from ‘moderate’ to ‘mild’ by the end of the therapy session. Two of them with a ‘moderate’ degree of tinnitus at the beginning of the session have stopped perceiving the tinnitus completely after the treatment. One of the participants who perceived ‘mild’ tinnitus at the beginning of the treatment stopped experiencing the tinnitus. Three of them experienced a reduction in severity from ‘mild’ to slight by the end of the treatment sessions.
The handicap from tinnitus reflected from TFI on day-1 and day-15 was analyzed. It was observed that the severity of the tinnitus reduced from ‘moderate’ to ‘small problem’ in five of the participants at the end of the treatment, while two of them who had a 'moderate’ degree of tinnitus stopped perceiving it completely. Three participants who had a 'small problem’ perceived a change in severity to ‘not a problem’ and one with ‘small problem’ stopped perceiving tinnitus at the end of the training.
A Chi-square test was used to assess whether an association exists between tinnitus severity and handicap before and after therapy. This was performed by comparing the observed THI and TFI index between day-1 and day-15. The results revealed that there is a significant association in severity and handicap of tinnitus before and after therapy in THI [X2 (1, N = 11) = 5.238, p = 0.045] and in TFI [X2 (1, N = 11) = 5.238, p = 0.045].
Psychoacoustic parameters of the tinnitus (pitch and loudness) were monitored to assess the treatment efficacy. A change in pitch and reduced loudness (Fig. 5) was noted as a function of treatment sessions in eight of 11 participants. Three of them had no tinnitus perception at the end of the treatment.
Fig. 5.

Each of the participants demonstrated the change in tinnitus pitch (a) and reduced loudness (b) across treatment sessions
Discussion
Tinnitus perception is a consequence of misinterpretation of abnormal neuronal activity at the auditory cortex. Auditory cortex neurons are deprived of normal thalamocortical input due to hearing loss. But do not become inactive, but “rewire” with excitatory inputs from neighboring neurons. As a result of bottom-up input deprivation, the neurons are no longer excitable by the frequencies they were originally tuned to but become sensitive to neighboring frequencies because of the rewiring. In the FDT training module, the focused attention towards identifying the target tone (1/3rd octave below tinnitus pitch) from tinnitus pitch makes the neurons realize to what frequency they are tuned to rather than excited for the neighboring frequency. In doing so, the tinnitus pitch was shifted towards the lower frequency and the loudness was reduced (Fig. 5) in 8 of 11 participants. In such a scenario, the limbic system redefines the emotion and eventually reduces the self-reinforcement of negative emotions. Thus, the study participants have reported the reduced severity of handicap as a function of treatment sessions. Consequently, the para-sympathetic neuron of the autonomic nervous system reacted and reduced the functional impairment reflected in TFI as a function of the treatment session. Besides, a significant association in severity and handicap of tinnitus before and after therapy in THI was observed in the study participants. Those participants who had a lesser degree of severity and handicap experienced greater relief from tinnitus percept, resultant in habituation of perception and or reaction after 15 days of treatment from FDT. Conversely, those who had severe handicap and severity of tinnitus experience a lesser degree of relief from tinnitus.
Perhaps in each treatment session, constantly redefining the tinnitus pitch to discriminate target sound from distractors led to the breakdown of the then conditioned reflex or strongest vicious neuronal pathway (auditory, limbic and autonomous nervous system). Thus, three participants had experienced habituation to the perception as they were no longer aware of tinnitus, except when focused attention on it, which was revealed when THI was administered. To perpetuate, over a period with active focused attention and discriminating the target tone from distractors breaks down the conditioned reflex and subsequently stops spreading tinnitus-related neuronal activity to the limbic and autonomic nervous systems. The decreased activation of these systems (auditory, limbic, and autonomic nervous system), facilitates habituation.
Conclusion
Realizing the neurons about their characteristic frequency through focused attention and discrimination by the frequency discrimination training can lessen the tinnitus percept in those with a flat sensorineural hearing loss having unilateral tinnitus.
Funding
No funding was received to assist with the preparation of this manuscript.
Data Availability
All data and materials as well as software application support the published claims and comply with field standards.
Code Availability
Software application.
Compliance with Ethical Standards
Conflicts of interest
The authors have no conflicts of interest to declare that are relevant to the content of this article.
Ethical Approval
The methodology for this study was approved by the Human Research Ethics committee of the Institution.
Consent for publication
Patients signed informed consent regarding publishing their data.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
N. Hemanth, Email: hemanthn.shetty@gmail.com
P. G. Vipin Ghosh, Email: vipinghosh78@gmaill.com
References
- 1.El-Shunnar SK, Hoare DJ, Smith S, Gander PE, Kang S, Fackrell K, Hall DA. Primary care for tinnitus: practice and opinion among GPs in England: GP management of tinnitus. J Eval Clin Pract. 2011;17:684–692. doi: 10.1111/j.1365-2753.2011.01696.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Thirunavukkarasu K, Geetha C. One-year prevalence and risk factors of tinnitus in children with otological problems. Int Tinnitus J. 2015;19:33–38. doi: 10.5935/0946-5448.20150006. [DOI] [PubMed] [Google Scholar]
- 3.Chung DY, Gannon RP, Mason K. Factors affecting the prevalence of tinnitus. Audiology. 1984;23:441–452. doi: 10.3109/00206098409070084. [DOI] [PubMed] [Google Scholar]
- 4.Noreña AJ, Moffat G, Blanc JL, Pezard L, Cazals Y. Neural changes in the auditory cortex of awake guinea pigs after two tinnitus inducers: salicylate and acoustic trauma. Neuroscience. 2010;166:1194–1209. doi: 10.1016/j.neuroscience.2009.12.063. [DOI] [PubMed] [Google Scholar]
- 5.Hoare DJ, Van Labeke N, McCormack A, Sereda M, Smith S, Al Taher H, Kowalkowski VL, Sharples M, Hall DA. Gameplay as a source of intrinsic motivation in a randomized controlled trial of auditory training for tinnitus. PLoS ONE. 2014;9:e107430. doi: 10.1371/journal.pone.0107430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.McNeill C, Távora-Vieira D, Alnafjan F, Searchfield GD, Welch D. Tinnitus pitch, masking, and the effectiveness of hearing aids for tinnitus therapy. Int J Audiol. 2012;51:914–919. doi: 10.3109/14992027.2012.721934. [DOI] [PubMed] [Google Scholar]
- 7.Tyler R, Stocking C, Secor C, Slattery WH., III Amplitude modulated S-tones can be superior to noise for tinnitus reduction. Am J Audiol. 2014;23:303–308. doi: 10.1044/2014_AJA-14-0009. [DOI] [PubMed] [Google Scholar]
- 8.Wise K, Kobayashi K, Searchfield GD. Feasibility study of a game integrating assessment and therapy of tinnitus. J Neurosci Methods. 2015;249:1–7. doi: 10.1016/j.jneumeth.2015.04.002. [DOI] [PubMed] [Google Scholar]
- 9.Hoare DJ, Gander PE, Collins L, Smith S, Hall DA. Management of tinnitus in English NHS audiology departments: an evaluation of current practice: tinnitus management in England. J Eval Clin Pract. 2012;18:326–334. doi: 10.1111/j.1365-2753.2010.01566.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jastreboff PJ (2000) Tinnitus habituation therapy (THI) and tinnitus retraining therapy (THI). Tinnitus Handb 357–376
- 11.Newman CW, Jacobson GP, Spitzer JB. Development of the tinnitus handicap inventory. Arch Otolaryngol Neck Surg. 1996;122:143–148. doi: 10.1001/archotol.1996.01890140029007. [DOI] [PubMed] [Google Scholar]
- 12.Zacharia T, Naik PV, Sada S, Kuniyil JG, Dwarakanath VM. Development and standardization of tinnitus handicap inventory in Kannada. Int Tinnitus J. 2012;17(2):117–123. doi: 10.5935/0946-5448.20120022. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data and materials as well as software application support the published claims and comply with field standards.
Software application.