

Abstract
Background
This study aimed to compare the clinical outcomes of implantation of various multifocal intraocular lenses (mIOLs) and the prediction accuracy of two intraocular lens (IOL) power calculation formulas for eyes that underwent previous corneal refractive surgery.
Methods
Four types of mIOLs [TECNIS Symfony (Group I), AcrySof IQ PanOptix (Group II), LENTIS Mplus (Group III), and TECNIS ZLB00 (Group IV)] were used and the IOL power was calculated with the two no-history methods, Shammas-PL and Barrett True-K. Visual acuity and refractive outcomes including manifest refraction, prediction error (PE), absolute error (AE), and median absolute error (MedAE) were evaluated at three months after the cataract surgery.
Results
For all groups the Barrett True-K formula produced a narrower range of PEs and lower MedAE than Shammas-PL. Eyes of lower predictive accuracy (group B, AE >0.5D) showed weak uncorrected distance visual acuity resulting from myopic refractive error and target refraction when compared to that of higher predictive accuracy (group A, AE ≤0.5 D).
Conclusions
Targeting emmetropia using the Barrett True-K, which considers both anterior and posterior corneal curvature is recommended in patients undergoing mIOL implantation with prior corneal refractive surgery. Additionally, history of prior large amount of laser ablation seems to be an important factor related to low predictive accuracy.
Keywords: Multifocal intraocular lens, laser corneal surgery, intraocular lens implantation, cataract
Introduction
With the popularization of refractive surgery, many patients have undergone refractive surgeries, and as the age of patients has increased, the number of cataract surgeries after refractive surgery has increased. There are many reports that intraocular lens (IOL) power calculation for eyes that have previously undergone refractive surgery is less accurate than that for virgin eyes (1-3). IOL power calculations for patients who have had corneal refractive surgery are clinically challenging because it is difficult to accurately predict corneal power and effective lens position (1,2). Many formulas are used to accurately calculate IOL power for eyes that have previously undergone corneal refractive surgery. When the refractive surgery parameters (pre-refractive surgery K-readings, amount of myopia corrected, or both) are known, many methods are available to correct the K-values and more accurately estimate the lens position (4,5). However, when the refractive surgery data is not available, the no-history method is a viable alternative for IOL power calculation after myopic refractive surgery (4).
In the absence of refractive surgery data, several formulas have been proposed to accurately calculate IOL power, including the Shammas post-LASIK (Shammas-PL) and Barrett True-K formulas (1,6). The Shammas-PL formula calculates IOL power based upon estimated postoperative anterior chamber depth (pACD), axial length (AL) and post-refractive surgery keratometry (1). The Barrett True-K formula (version 2.0) is based on the Barrett Universal II formula and is accessed online (7,8). Many studies have been published on monofocal IOL power calculation after refractive surgery, but to the best of our knowledge there have been few reports on multifocal IOL (mIOL) power calculation after refractive surgery. Although several studies have shown good refractive outcomes and visual acuity results, the use of mIOLs for eyes that have undergone corneal refractive laser surgery is controversial because of the assumption that the laser alteration of the cornea could cause vision to deteriorate after mIOL implantation (9,10).
To our knowledge, there are few studies that have evaluated refractive and visual outcomes and analyzed factors affecting prediction error (PE) for various mIOLs for patients who have had myopic refractive laser surgery. This retrospective study aimed to compare the clinical outcomes of four mIOLs and to evaluate predictive accuracy of two IOL power calculation formulas for patients that have previously undergone corneal refractive surgery. Additionally, preoperative characteristics that could lead to low predictive accuracy of IOL power calculation were evaluated.
We present the following article in accordance with the STROBE reporting checklist (available at https://dx.doi.org/10.21037/atm-21-3057).
Methods
Subjects
This retrospective study included 131 eyes of 131 patients who underwent cataract surgery with mIOLs from January 2018 to July 2019 and had previously undergone myopic refractive surgery. Exclusion criteria were previous ocular surgeries except corneal refractive procedures such as LASIK or LASEK, corneal diseases, pseudoexfoliation, zonular weakness, corneal astigmatism greater than 1.00 diopter (D), glaucoma, macular disease, and amblyopia. Eyes with best-corrected distant vision less than 20/40 in the postoperative state were also excluded. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The Institutional Review Board (IRB #2020-09-079) for Human Studies at Samsung Medical Center approved this study and informed consent was exempted by IRB of Samsung Medical Center.
Surgical technique
All procedures were performed by one experienced surgeon (TYC) under topical anesthesia. Phacoemulsification was performed through a 2.75 mm temporal clear corneal incision. After performing continuous curvilinear capsulorhexis with intended diameter 5.0 mm and hydrodissection, phacoemulsification of the nucleus and bimanual aspiration of the residual cortex were performed using a cataract surgery phacoemulsification device (Centurion Vision System, Alcon, Fort Worth, TX, USA). The mIOL was implanted into the capsular bag using an injector and disposable cartridge system before removing the ophthalmic viscosurgical device (OVD). Four types of mIOLs were used: extended range of vision (Group I; TECNIS Symfony, ZXR00, Johnson & Johnson Vision Care, Inc. Santa Ana, CA, USA), quadrifocal (Group II; AcrySof IQ PanOptix, TNFT00, Alcon, Fort Worth, TX, USA), asymmetric zonal refractive bifocal (Group III; LENTIS Mplus, LS-313 MF30, LS-313 MF30, Oculentis GmbH, Berlin, Germany), and traditional diffractive bifocal (Group IV; TECNIS multifocal IOL, ZLB00, Johnson & Johnson Vision Care, Inc., Santa Ana, CA, USA). Finally, a balanced salt solution was injected into the incision site to close the corneal incision, causing edema. After the surgery, postoperative antibiotic and corticosteroid eye drops were used four times daily and tapered over a month.
Patient examinations
Before cataract surgery, visual acuity was measured, including uncorrected distance visual acuity (UDVA) and uncorrected near visual acuity (UNVA). Manifest refraction (MR) testing was also conducted. To calculate mIOL power during cataract surgery, preoperative biometry of the eye was measured, namely the keratometry of the anterior surface, central corneal thickness, anterior chamber depth, and axial length, using a swept-source optical coherence tomography (SS-OCT) biometer (ARGOS, Suntec, Inc., Aichi, Japan). Keratometry of the posterior surface was measured with a Scheimpflug camera (Pentacam, Oculus, Wetzlar, Germany). Three months after the cataract surgery, visual acuity (UDVA and UNVA) and ocular refraction [MR and autorefraction (AR) with autorefractor] were measured. UDVA and UCVA were measured at 4 m and 40 cm respectively.
Main measurement outcomes
Differences were compared between the predicted refractive value for each mIOL calculated by using different formulas and the refractive value measured three months after cataract surgery. The IOL power was calculated using two methods, the Shammas-PL formula, which is built into the biometer used, and the Barrett True-K formula (version 2.0, http://calc.apacrs.org/Barrett_True_K_Universal_2105/), which can be computed using a website. To calculate IOL power, the Shammas-PL uses only the anterior corneal curvature measured by the biometer, whereas the Barrett true-K formula uses both this curvature and the posterior corneal curvature. To calculate IOL power with both formula, preoperative biometry was used measured values from SS-OCT biometer except keratometry of the posterior surface. Posterior corneal curvature from Scheimpflug camera was used in the Barrett true-K formula. The IOL constants of each formula were as follows; In Shammas-PL [TECNIS Symfony (Group I); 118.8, PanOptix (Group II); 119.1, LENTIS Mplus (Group III); 118.5, TECNIS ZLB00 (Group IV); 118.8], in Barrett True-K formula [TECNIS Symfony (Group I); 119.39, PanOptix (Group II); 119.1, LENTIS Mplus (Group III); 118.5, TECNIS ZLB00 (Group IV); 119.39].
Prediction error (PE) in refraction was defined as the predicted spherical equivalent (SE) from an IOL formula minus the actual postoperative SE, whereas the mean error (ME) was the mean of the PEs. Positive and negative signs of PE respectively represent myopic and hyperopic errors of postoperative refraction. The mean absolute error (MAE) and median absolute error (MedAE) were the mean and median of the absolute values of the MEs. We also calculated the percentage of eyes having MEs of ±0.25, ±0.50, and ±1.00 D or less. Additionally, PE for each mIOLs were analyzed based on postoperative MR. After these refractive outcomes were calculated, the predictive accuracies of the two formulas were evaluated.
Statistical analysis
Visual acuity and refractive outcomes including MR, AR, and PE were compared between four mIOLs using the Kruskal-Wallis H test. The refractive outcome measures MAE and MedAE of the Shammas-PL and Barrett True-K formulas were compared for each of the four mIOL groups. Box plots were used to compare the PEs of the Shammas-PL and Barrett True-K formulas. Statistical analyses were performed using SPSS statistical software (version 23.0, SPSS, Inc., Chicago, IL, USA) and statistical significance was defined as P<0.05.
Results
There was no difference in patient sex between the four groups (Table 1). Although the optical power of the implanted mIOLs was not different between the groups, group I showed younger age, flatter corneal curvature, and longer axial length than the other three groups (all P<0.05). From the preoperative biometry of group I, it can be inferred that the extended depth of focus (EDOF) IOL was used in cataract patients with prior higher degrees of myopic laser correction.
Table 1. Subject demographics.
| Characteristics | Group I | Group II | Group III | Group IV | P value |
|---|---|---|---|---|---|
| Number | 59 | 25 | 26 | 21 | |
| Age | 48.7±6.2§ | 50.4±4.8 | 52.5±4.6 | 50.5±6.1 | 0.031† |
| Female (%) | 40 (67.8) | 15 (60.0) | 18 (69.2) | 17 (81.0) | 0.50‡ |
| Visual acuity (LogMAR) | |||||
| UDVA | 0.56±0.37 | 0.29±0.20 | 0.25±0.33 | 0.37±0.30 | 0.23‡ |
| UNVA | 0.40±0.26 | 0.34±0.28 | 0.41±0.21 | 0.32±0.24 | 0.45‡ |
| Manifest refraction (D) | |||||
| Spherical equivalent | −0.73±1.97 | −0.49±0.92 | −0.84±1.17 | −0.75±1.36 | 0.56‡ |
| Refractive sphere | −0.43±2.02 | −0.22±0.91 | −0.35±0.49 | −0.44±1.37 | 0.22‡ |
| Refractive astigmatism | −0.60±0.61 | −0.53±0.71 | −0.36±0.35 | −0.61±0.59 | 0.48‡ |
| Keratometry (D) | 39.92±2.47§ | 41.30±1.65 | 41.66±2.16 | 40.61±2.52 | 0.010‡ |
| Central corneal thickness (μm) | 483.0±41.4§ | 514.5±33.2 | 482.4±42.4 | 479.8±34.0 | 0.007‡ |
| Anterior chamber depth (mm) | 3.42±0.31 | 3.52±0.25 | 3.32±0.32 | 3.38±0.32 | 0.051‡ |
| Axial length (mm) | 26.23±1.99§ | 25.21±1.07 | 24.92±1.33 | 25.48±1.79 | 0.003‡ |
| IOL power (D) | 20.11±4.64 | 20.28±3.52 | 19.98±2.07 | 21.12±2.78 | 0.46† |
†, P value by Kruskal-Wallis H test; ‡, P value by chi-squared test; §, Group I showed statistically different values compared to each of groups II, III, and IV. UDVA, uncorrected distance visual acuity; UNVA, uncorrected near visual acuity; IOL, intraocular lens.
Both postoperative UDVA and UNVA were improved in all groups compared with those before cataract surgery (all P<0.001). Both postoperative mean UDVA and UNVA were logMAR 0.1 or less in groups II, III, and IV (Table 2). UDVA was better for groups II, III, and IV than for group I, and UNVA was better for groups II and III than for groups I and IV. Postoperative mean MR for four groups were −0.37±0.64, −0.14±0.24, −0.16±0.26, and −0.050±0.44 D in groups I, II, III, and IV, respectively. There was no difference in SE based on MR between the four groups (P=0.106). Groups I and III showed myopic refractive error in mean AR compared to their mean MR. More than 60% of eyes in each group showed MR between −0.25 and +0.25 D (67.8%, 84.0%, 73.1%, and 66.7% in group I, II, III and IV, respectively; Figure 1). More than 80% of eyes showed MR within 1 D in all groups (84.7%, 100.0%, 92.3%, and 95.2% in group I, II, III and IV, respectively).
Table 2. Postoperative visual and refractive outcomes after cataract surgery in patients with prior refractive laser surgery.
| Outcome measures | Group I | Group II | Group III | Group IV | P value† |
|---|---|---|---|---|---|
| Number | 59 | 25 | 26 | 21 | |
| Visual acuity (LogMAR) | |||||
| UDVA | 0.11±0.16‡ | 0.076±0.14 | 0.043±0.10 | 0.072±0.10 | 0.047 |
| UNVA | 0.13±0.12§ | 0.051±0.077 | 0.030±0.061 | 0.10±0.11§ | <0.001 |
| Spherical equivalent (D) | |||||
| Manifest refraction | −0.37±0.64 | −0.14±0.24 | −0.16±0.26 | −0.050±0.44 | 0.11 |
| Auto refraction | −1.41±0.63¶ | −0.27±0.48 | −1.50±0.45¶ | −0.51±0.49 | <0.001 |
†, P value by Kruskal-Wallis H test; ‡, Group I showed statistically different values compared to each of groups II, III, and IV; §, Groups I and IV showed statistically different values compared to each of groups II and III; ¶, Groups I and III showed statistically different values compared to each of groups II and IV. UDVA, uncorrected distance visual acuity; UNVA, uncorrected near visual acuity.
Figure 1.
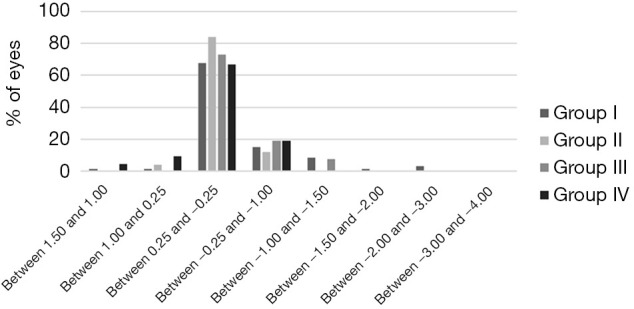
Postoperative manifest refractions of subjects implanted with various multifocal intraocular lenses.
Target refractions calculated from Barrett True-K showed no difference between all groups (P=0.355, Table 3). PEs based on Barrett True-K were closer to zero than those based on Shammas-PL in groups I and II (P=0.017 and 0.007, respectively; Figure 2). Although groups III and IV showed no difference in PE between Barrett True-K and Shammas-PL, mean PE values of Shammas-PL (0.050±0.40 and −0.29±0.65 D in groups III and IV, respectively) and Barrett True-K formulas (0.19±0.22 and −0.012±0.60 D in groups III and IV, respectively) were within 0.50 D of each other. For all groups, the Barrett True-K formula yielded lower MAE and MedAE than Shammas-PL. More eyes had MAE within 0.25 and 0.50 D when using the Barrett True-K formula (45.8%, 68.0%, 65.4%, 42.9% and 76.3%, 84.0%, 88.5%, 66.7% in group I, II, III, and IV, respectively) compared to Shammas-PL (23.8%, 44.0%, 50.0%, 38.1% and 72.9%, 84.0%, 76.9%, 66.7% in group I, II, III, and IV, respectively; Figure 3).
Table 3. Prediction accuracy of IOL power calculated using Shammas-PL and Barrett True-K formulas for four multifocal intraocular lenses.
| Prediction accuracy measures | Group I | Group II | Group III | Group IV | P value† |
|---|---|---|---|---|---|
| Number | 59 | 25 | 26 | 21 | |
| Target Refraction (D) | |||||
| Shammas-PL | −0.39±0.34 | 0.067±0.29 | −0.13±0.31 | −0.34±0.35 | <0.001 |
| Barrett True-K | −0.20±0.65 | −0.16±0.37 | 0.027±0.22 | −0.062±0.33 | 0.36 |
| Absolute Error (D) | |||||
| Shammas-PL | 0.44±0.30 | 0.47±0.33 | 0.32±0.24 | 0.49±0.50 | 0.28 |
| Barrett True-K | 0.41±0.50 | 0.29±0.19 | 0.24±0.17 | 0.45±0.39 | 0.16 |
| MedAE (D) | |||||
| Shammas-PL | 0.37 | 0.35 | 0.27 | 0.34 | |
| Barrett True-K | 0.28 | 0.28 | 0.22 | 0.29 |
†, P value by Kruskal-Wallis H test. MedAE, median absolute error.
Figure 2.
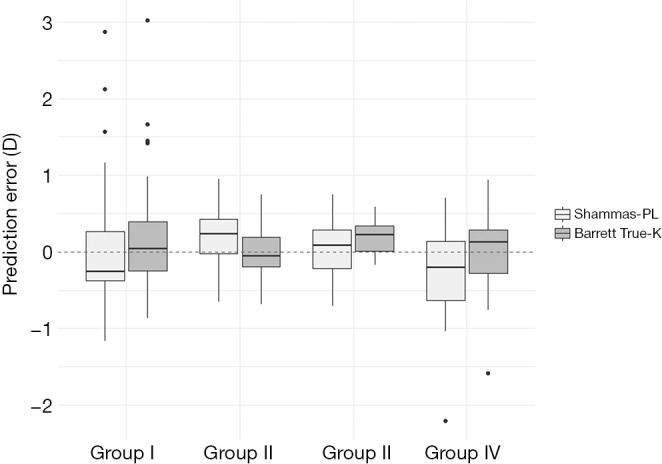
Prediction errors of Shammas-PL and Barrett True-K formulas [Prediction error = predicted spherical equivalent (SE) − postoperative SE].
Figure 3.
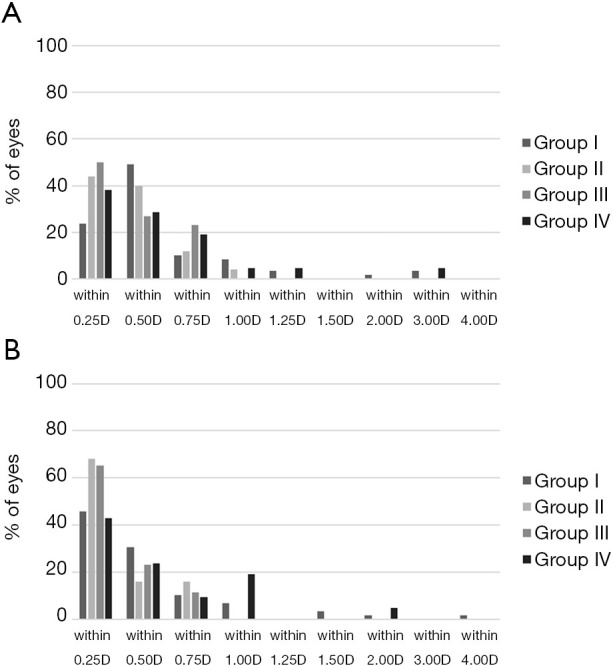
Mean absolute errors of (A) Shammas-PL and (B) Barrett True-K formulas.
Postoperative mean UDVA in eyes with postoperative MR between 0.25 and −0.25 D were 0.053±0.082, 0.044±0.11, 0.0072±0.017, and 0.058±0.094 in group I, II, III, and IV, respectively (Figure 4). Although there was no difference in UDVA between four groups in case with postoperative MR between +0.25 and −0.25 D (P=0.056), UNVA at 40 cm was better in groups II and III than groups I and IV (all P<0.001). Group I achieved UNVA better than 0.1 logMAR in wider range of postoperative MRs than other groups, showing the EDOF properties. In subgroup analysis based on postoperative MR, Group II, III, and IV showed the best UDVA and UNVA in postoperative MR between +0.25 and −0.25 D.
Figure 4.
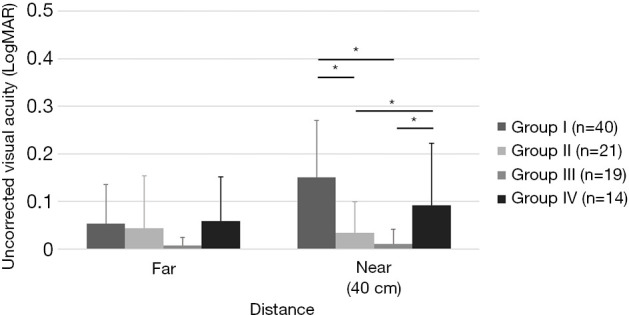
Postoperative LogMAR visual acuity of eyes having between 0.25 and −0.25 D of postoperative manifest refraction. Asterisks (*) indicate statistically significant differences (P<0.05, Kruskal-Wallis H test).
Twenty-three of the 131 subjects (17.56%) showed an absolute value of PE (AE) of 0.5 D or more based on the calculation with Barrett True-K formula (Table 4); these subjects were grouped as Group B. Their UDVA was lower (P<0.001) and their postoperative refraction error was more myopic (P=0.001) than subjects having AE less than 0.5 D (Group A). Both SE and refractive sphere based on MR were closer to emmetropia for group A (−0.16±0.36 and −0.0049±0.38 D, respectively) than for group B [−0.58±0.85 (P=0.016) and −0.40±0.87 D (P=0.028), respectively]. Lower K-values (P=0.002) and longer axial length (P=0.010) were found in group B compared to group A. It is supposed that subjects who experienced more ablation during laser refractive surgery before cataract surgery fell into the higher-PE group B. Target refraction preoperatively calculated with Barrett-True-K was more myopic for group B than group A (P<0.001). However, target refraction calculated with Shammas-PL did not show any difference between group A (−0.22±0.36 D) and group B (−0.36±0.41 D, P=0.090). Regardless of which IOL formula was used, group B showed myopic refractive error compared to group A. For the high-AE group B, IOL power selection targeting myopic seems to have resulted in postoperative myopic PE after cataract surgery.
Table 4. Factors related to absolute value of prediction error after cataract surgery in patients with prior refractive laser surgery. All subjects were divided into two groups: those having prediction error of 0.5 D or less (Group A) or prediction error more than 0.5 D (group B). Prediction error was calculated by using the Barrett True-K formula.
| Variables | Group A (AE ≤0.5 D) | Group B (AE >0.5 D) | P value |
|---|---|---|---|
| Number | 108 | 23 | |
| Postoperative values | |||
| Visual acuity (LogMAR) | |||
| UDVA | 0.061±0.10 | 0.19±0.22 | 0.001† |
| UNVA | 0.090±0.11 | 0.10±0.12 | 0.65† |
| Manifest refraction (D) | |||
| Spherical equivalent | −0.16±0.36 | −0.58±0.85 | 0.016† |
| Refractive sphere | −0.005±0.38 | −0.40±0.87 | 0.028† |
| Refractive astigmatism | −0.31±0.38 | −0.35±0.32 | 0.37† |
| Target refraction (D) | |||
| Barrett true-K | −0.069±0.25 | −0.36±1.05 | <0.001† |
| Preoperative values | |||
| Age | 50.1±5.8 | 50.0±5.8 | 0.70† |
| Female (%) | 40 (67.8) | 15 (60.0) | 0.92‡ |
| Keratometry (D) | 40.96±2.27 | 39.13±2.30 | 0.002† |
| Central corneal thickness (μm) | 489.6±37.1 | 481.4±54.8 | 0.84† |
| Anterior chamber depth (mm) | 3.43±0.32 | 3.34±0.23 | 0.36† |
| Axial length (mm) | 25.46±1.66 | 26.59±1.97 | 0.010† |
| IOL power (D) | 20.3±3.4 | 20.3±5.1 | 0.23‡ |
†, P value by Man-Whitney test; ‡, P value by chi-squared test. AE, absolute value of prediction error; UDVA, uncorrected distance visual acuity; UNVA, uncorrected near visual acuity; IOL, intraocular lens.
Discussion
MIOL implantation yielded good distant and near visual acuity in post-refractive surgery eyes, and the emmetropia target is also recommended for good near and distance visual acuity. In calculating mIOL power after refractive surgery, the Barrett True-K formula, which considers posterior corneal curvature as well as anterior corneal curvature, was more accurate than the Shammas-PL formula. However, eyes with history of larger amount of laser ablation in corneal refractive surgery seems to show weaker predictive accuracy of IOL power calculation when using the Barrett True-K formula.
The predictive accuracy of the Barrett True-K formula was higher than that of the Shammas-PL formula, which is thought to be due to the fact that the Barrett True-K formula showed more hyperopic PE than Shammas-PL formula (6). Although conventional formulas such as Shammas-PL and Haigis-L calculate IOL power based upon preoperative keratometry measuring only the anterior curvature, supplemental factors have been added to these formulas to reduce PE for eyes with prior corneal refractive surgery (4,11). Specific methods for corneal power correction have been used with both Shammas-PL and Haigis-L to compensate for overestimated keratometry in eyes with prior corneal refractive surgery. However, the keratometry used in both formulas were not measured values, but expected values developed by using regression analysis (a no-history method). As a result, IOL power calculations with Shammas-PL and Haigis-L have shown more myopic PE in eyes with prior corneal refractive surgery than those preoperatively expected (7). Recently published meta-analysis concluded that the ASCRS average based on ASCRS calculator (available at: http://www.ascrs.org) (6,12), Barrett True-K (7), or OCT formula (13) was recommended to calculate IOL power in eyes with prior laser refractive surgery for correcting myopia (14). Furthermore, the Barrett True-K (7), OCT (13), and optiwave refractive analysis formula (15) showed more accurate in prediction error than other formula including Haigis-L and Shammas formulas in eyes with previous myopic laser refractive surgery from Bayesian network meta-analysis (16).
The Barrett True-K formula more accurately calculates IOL power, representing the curvature of the entire cornea by including the posterior corneal curvature measurement (6,11,17,18). In previous studies reporting the results of cataract surgery after corneal refractive laser surgery, IOL power calculation using total keratometry which considers both anterior and posterior corneal curvature showed better results than conventional calculation using only the anterior corneal curvature (19-24). Additionally, Shammas-PL based on total keratometry measured with an IOLMaster 700 biometer showed improved accuracy compared to that based on anterior keratometry in clinical studies by Lawless et al. and Yeo et al. (25,26). Recently, formulas using a ray-tracing method developed directly by the research institute were presented for more accurate IOL power calculation considering the anterior and posterior corneal curvature as well as the corneal thickness (20,27-29). Keratometry calculated from directly measured corneal curvatures of both the anterior and posterior surfaces would improve refractive outcomes due to the correction of myopic refractive error along with conventional IOL power calculations in eyes with prior corneal refractive surgery.
In the present study, eyes with extreme biometry (mean K value of 39.13 D and mean AL of 26.59 mm) showed greater PE as calculated using Barrett True-K. IOL power calculation formulas for eyes with prior corneal refractive surgery are divided into history methods, which consider pre-refractive surgery data, and no-history methods, which are used when data from the refractive surgery are not available. Although there was no significant difference between the two methods (4,11,30), there has been no single formula showing high accuracy in various biometry conditions including eyes after corneal refractive surgery (31,32). Recently, Whang et al. reported in a retrospective study that the predictive accuracy of no-history IOL formulas depends on AL (33). Barrett True-K was most accurate for AL less than 28 mm, Triple-S was most accurate for AL between 28 and 30 mm, and Shammas-PL was most accurate for AL 30 mm or more. In the present study, mean preoperative AL was 25.84±1.81 mm and only two eyes had a preoperative AL of more than 30 mm; thus, further evaluation of prediction accuracy in the case of extremely long eyes requires further study.
Eyes with high PE as calculated by Barrett True-K (group B in Table 4) showed preoperative characteristics of lower K-values and longer axial length. These biometry results correspond to eyes that experienced larger amount of ablation during refractive laser surgery. Additionally, both IOL power selection targeting myopic refraction and postoperative myopic refractive outcome resulted in PE being myopic. Previous studies with earlier formulas recommended targeting myopic due to hyperopic refractive surprise when calculating IOL power in eyes with previous corneal refractive surgery (32-36). Recent studies have reported that it is good to make the postoperative MR close to emmetropia in eyes having general corneal curvature, and the same results were reported for eyes which have undergone corneal refractive surgery (37,38). However, targeting slightly myopia may improve near vision without compromising distant vision, especially in high myopic patients, which is the case in the real world practice. Based on our result, we recommend aiming emmetropia when using Barrett True-K formula for implanting mIOL in eyes that have undergone corneal refractive surgery. Moreover, this study shows that predictive accuracy is more important than mIOL type for postoperative visual outcomes of patients with prior corneal refractive surgery.
To measure postoperative refractive power of the eye, MR is recommended after mIOL implatation (39). Pseudophakia with a diffractive multifocal IOL (Tecnis ZM900 or ReSTOR) showed similar refraction between autorefraction and MR measurements, including both spherical and astigmatic values (39,40). However, for eyes with a refractive multifocal IOL (ReZoom and Lentis LS-312 MF30), spherical values were found to be underestimated by autorefraction compared to MR (39,41,42). Interestingly, in the present study both EDOF IOL (Tecnis Symfony) and rotationally asymmetric multifocal IOL (Lentis LS-312 MF30) also led to underestimation of spherical power by means of autorefraction compared to MR. Postoperative refraction in patients with refractive or EDOF mIOL should be measured by MR and AR cannot be a replacement for MR.
However, there were some limitations in this study. IOL power calculation formulas with no-history methods were not compared to history methods in this retrospective study. Type of corneal refractive surgery was not identified due to a lack of information in some medical records. SS-OCT biometer used in the present study (ARGOS) could not be the same one with other biometer which other clinician uses (IOL Master 700; Carl Zeiss Meditec AG, Jena, Germany). As there is a difference in axial length measurement between two biometer, the results from this study cannot be applied to the cases with IOL Master 700. The adequate values for keratometry and axial length to estimate the lower predictive accuracy for postoperative refraction error could not be concluded as only two eyes had an axial length of >30 were included into the present study. Therefore, further prospective study based on a larger number with same type of mIOL is needed in order to improve the predictive accuracy of each IOL power calculation, especially in eyes that have undergone a large amount of corneal ablation.
In conclusion, MIOL implantation after corneal refractive laser surgery showed good refractive and visual outcomes. The Barrett True-K formula, which considers both anterior and posterior corneal curvature, was more accurate than the Shammas-PL formula, which considers only anterior corneal curvature. Targeting emmetropia is recommended when implanting mIOL in eyes that have undergone corneal refractive surgery. Especially in eyes that have undergone extensive corneal ablation, the previously large amount of laser ablation for cornea seems to be an important factor causing low predictive accuracy of IOL power calculation in cataract surgery.
Supplementary
The article’s supplementary files as
Acknowledgments
Funding: This work was supported by a grant from a National Research Foundation of Korea grant funded by the Ministry of Education, Republic of Korea (NRF-2020R1A2C2014139; Seoul, Korea) and the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI) funded by the Ministry of Health &Welfare, Republic of Korea (HC19C0142).
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy of integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The Institutional Review Board (IRB #2020-09-079) for Human Studies at Samsung Medical Center approved this study and informed consent was exempted by IRB of Samsung Medical Center.
Footnotes
Reporting Checklist: The authors have completed the STROBE reporting checklist. Available at https://dx.doi.org/10.21037/atm-21-3057
Data Sharing Statement: Available at https://dx.doi.org/10.21037/atm-21-3057
Peer Review File: Available at https://dx.doi.org/10.21037/atm-21-3057
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://dx.doi.org/10.21037/atm-21-3057). DHL was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI) funded by the Ministry of Health &Welfare, Republic of Korea (HC19C0142). TYC was supported by a grant from a National Research Foundation of Korea grant funded by the Ministry of Education, Republic of Korea (NRF-2020R1A2C2014139; Seoul, Korea). The other authors have no conflicts of interest to declare.
References
- 1.Savini G, Hoffer KJ. Intraocular lens power calculation in eyes with previous corneal refractive surgery. Eye Vis (Lond) 2018;5:18. 10.1186/s40662-018-0110-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hoffer KJ. Intraocular lens power calculation after previous laser refractive surgery. J Cataract Refract Surg 2009;35:759-65. 10.1016/j.jcrs.2009.01.005 [DOI] [PubMed] [Google Scholar]
- 3.Koch DD, Liu JF, Hyde LL, et al. Refractive complications of cataract surgery after radial keratotomy. Am J Ophthalmol 1989;108:676-82. 10.1016/0002-9394(89)90860-X [DOI] [PubMed] [Google Scholar]
- 4.Shammas HJ, Shammas MC. No-history method of intraocular lens power calculation for cataract surgery after myopic laser in situ keratomileusis. J Cataract Refract Surg 2007;33:31-6. 10.1016/j.jcrs.2006.08.045 [DOI] [PubMed] [Google Scholar]
- 5.Shammas HJ, Shammas MC, Garabet A, et al. Correcting the corneal power measurements for intraocular lens power calculations after myopic laser in situ keratomileusis. Am J Ophthalmol 2003;136:426-32. 10.1016/S0002-9394(03)00275-7 [DOI] [PubMed] [Google Scholar]
- 6.Wang L, Tang M, Huang D, et al. Comparison of Newer Intraocular Lens Power Calculation Methods for Eyes after Corneal Refractive Surgery. Ophthalmology 2015;122:2443-9. 10.1016/j.ophtha.2015.08.037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Abulafia A, Hill WE, Koch DD, et al. Accuracy of the Barrett True-K formula for intraocular lens power prediction after laser in situ keratomileusis or photorefractive keratectomy for myopia. J Cataract Refract Surg 2016;42:363-9. 10.1016/j.jcrs.2015.11.039 [DOI] [PubMed] [Google Scholar]
- 8.Barrett GD. An improved universal theoretical formula for intraocular lens power prediction. J Cataract Refract Surg 1993;19:713-20. 10.1016/S0886-3350(13)80339-2 [DOI] [PubMed] [Google Scholar]
- 9.Vrijman V, van der Linden JW, van der Meulen IJE, et al. Multifocal intraocular lens implantation after previous corneal refractive laser surgery for myopia. J Cataract Refract Surg 2017;43:909-14. 10.1016/j.jcrs.2017.06.028 [DOI] [PubMed] [Google Scholar]
- 10.Muftuoglu O, Dao L, Mootha VV, et al. Apodized diffractive intraocular lens implantation after laser in situ keratomileusis with or without subsequent excimer laser enhancement. J Cataract Refract Surg 2010;36:1815-21. 10.1016/j.jcrs.2010.05.021 [DOI] [PubMed] [Google Scholar]
- 11.Vrijman V, Abulafia A, van der Linden JW, et al. Evaluation of Different IOL Calculation Formulas of the ASCRS Calculator in Eyes After Corneal Refractive Laser Surgery for Myopia With Multifocal IOL Implantation. J Refract Surg 2019;35:54-9. 10.3928/1081597X-20181119-01 [DOI] [PubMed] [Google Scholar]
- 12.Yang R, Yeh A, George MR, et al. Comparison of intraocular lens power calculation methods after myopic laser refractive surgery without previous refractive surgery data. J Cataract Refract Surg 2013;39:1327-35. 10.1016/j.jcrs.2013.03.032 [DOI] [PubMed] [Google Scholar]
- 13.Tang M, Wang L, Koch DD, et al. Intraocular lens power calculation after previous myopic laser vision correction based on corneal power measured by Fourier-domain optical coherence tomography. J Cataract Refract Surg 2012;38:589-94. 10.1016/j.jcrs.2011.11.025 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Li H, Nan L, Li J, et al. Accuracy of intraocular lens power calculation formulae after laser refractive surgery in myopic eyes: a meta-analysis. Eye Vis (Lond) 2020;7:37. 10.1186/s40662-020-00188-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ianchulev T, Hoffer KJ, Yoo SH, et al. Intraoperative refractive biometry for predicting intraocular lens power calculation after prior myopic refractive surgery. Ophthalmology 2014;121:56-60. 10.1016/j.ophtha.2013.08.041 [DOI] [PubMed] [Google Scholar]
- 16.Wei L, Meng J, Qi J, et al. Comparisons of intraocular lens power calculation methods for eyes with previous myopic laser refractive surgery: Bayesian network meta-analysis. J Cataract Refract Surg 2021;47:1011-8. 10.1097/j.jcrs.0000000000000562 [DOI] [PubMed] [Google Scholar]
- 17.Savini G, Hoffer KJ, Barrett GD. Results of the Barrett True-K formula for IOL power calculation based on Scheimpflug camera measurements in eyes with previous myopic excimer laser surgery. J Cataract Refract Surg 2020;46:1016-9. 10.1097/j.jcrs.0000000000000205 [DOI] [PubMed] [Google Scholar]
- 18.Jung S, Jung J. Comparison of Intraocular Lens Power Calculation Methods after Refractive Surgery Provided by the ASCRS. Journal of the Korean Ophthalmological Society 2018;59:827. 10.3341/jkos.2018.59.9.827 [DOI] [Google Scholar]
- 19.Wang L, Spektor T, de Souza RG, et al. Evaluation of total keratometry and its accuracy for intraocular lens power calculation in eyes after corneal refractive surgery. J Cataract Refract Surg 2019;45:1416-21. 10.1016/j.jcrs.2019.05.020 [DOI] [PubMed] [Google Scholar]
- 20.Wang L, Mahmoud AM, Anderson BL, et al. Total corneal power estimation: ray tracing method versus gaussian optics formula. Invest Ophthalmol Vis Sci 2011;52:1716-22. 10.1167/iovs.09-4982 [DOI] [PubMed] [Google Scholar]
- 21.Srivannaboon S, Chirapapaisan C. Comparison of refractive outcomes using conventional keratometry or total keratometry for IOL power calculation in cataract surgery. Graefes Arch Clin Exp Ophthalmol 2019;257:2677-82. 10.1007/s00417-019-04443-7 [DOI] [PubMed] [Google Scholar]
- 22.Fabian E, Wehner W. Prediction Accuracy of Total Keratometry Compared to Standard Keratometry Using Different Intraocular Lens Power Formulas. J Refract Surg 2019;35:362-8. 10.3928/1081597X-20190422-02 [DOI] [PubMed] [Google Scholar]
- 23.Koch DD, Ali SF, Weikert MP, et al. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg 2012;38:2080-7. 10.1016/j.jcrs.2012.08.036 [DOI] [PubMed] [Google Scholar]
- 24.Cho K, Lim DH, Yoo YS, et al. New method for intraocular lens power calculation using a rotating Scheimpflug camera in eyes with corneal refractive surgery. Sci Rep 2020;10:8992. 10.1038/s41598-020-65827-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Lawless M, Jiang JY, Hodge C, et al. Total keratometry in intraocular lens power calculations in eyes with previous laser refractive surgery. Clin Exp Ophthalmol 2020;48:749-56. 10.1111/ceo.13760 [DOI] [PubMed] [Google Scholar]
- 26.Yeo TK, Heng WJ, Pek D, et al. Accuracy of intraocular lens formulas using total keratometry in eyes with previous myopic laser refractive surgery. Eye (Lond) 2021;35:1705-11. 10.1038/s41433-020-01159-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Yagi-Yaguchi Y, Negishi K, Saiki M, et al. Comparison of the Accuracy of Newer Intraocular Lens Power Calculation Methods in Eyes That Underwent Previous Phototherapeutic Keratectomy. J Refract Surg 2019;35:310-6. 10.3928/1081597X-20190410-01 [DOI] [PubMed] [Google Scholar]
- 28.Hirnschall N, Buehren T, Trost M, et al. Pilot evaluation of refractive prediction errors associated with a new method for ray-tracing-based intraocular lens power calculation. J Cataract Refract Surg 2019;45:738-44. 10.1016/j.jcrs.2019.01.023 [DOI] [PubMed] [Google Scholar]
- 29.Yoo YS, Whang WJ, Hwang KY, et al. Use of the Crystalline Lens Equatorial Plane as a New Parameter for Predicting Postoperative Intraocular Lens Position. Am J Ophthalmol 2019;198:17-24. 10.1016/j.ajo.2018.09.005 [DOI] [PubMed] [Google Scholar]
- 30.Wang L, Koch DD. Intraocular Lens Power Calculations in Eyes with Previous Corneal Refractive Surgery: Review and Expert Opinion. Ophthalmology 2021;128:e121-31. 10.1016/j.ophtha.2020.06.054 [DOI] [PubMed] [Google Scholar]
- 31.Melles RB, Holladay JT, Chang WJ. Accuracy of Intraocular Lens Calculation Formulas. Ophthalmology 2018;125:169-78. 10.1016/j.ophtha.2017.08.027 [DOI] [PubMed] [Google Scholar]
- 32.Chen H, Chen X, Wang H, et al. Intraocular Lens power calculation after laser refractive surgery: A Meta-Analysis. Sci Rep 2020;10:2645. 10.1038/s41598-020-59487-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Whang WJ, Hoffer KJ, Kim SJ, et al. Comparison of intraocular lens power formulas according to axial length after myopic corneal laser refractive surgery. J Cataract Refract Surg 2021;47:297-303. 10.1097/j.jcrs.0000000000000445 [DOI] [PubMed] [Google Scholar]
- 34.Aramberri J. Intraocular lens power calculation after corneal refractive surgery: double-K method. J Cataract Refract Surg 2003;29:2063-8. 10.1016/S0886-3350(03)00957-X [DOI] [PubMed] [Google Scholar]
- 35.Seitz B, Langenbucher A, Nguyen NX, et al. Underestimation of intraocular lens power for cataract surgery after myopic photorefractive keratectomy. Ophthalmology 1999;106:693-702. 10.1016/S0161-6420(99)90153-7 [DOI] [PubMed] [Google Scholar]
- 36.Helaly HA, El-Hifnawy MA, Shaheen MS, et al. Accuracy of Corneal Power Measurements for Intraocular Lens Power Calculation after Myopic Laser In situ Keratomileusis. Middle East Afr J Ophthalmol 2016;23:122-8. 10.4103/0974-9233.171755 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Schuster AK, Schlichtenbrede FC, Harder BC, et al. Target refraction for best uncorrected distance and near vision in cataract surgery. Eur J Ophthalmol 2014;24:509-15. 10.5301/ejo.5000414 [DOI] [PubMed] [Google Scholar]
- 38.Hayashi K, Sato T, Igarashi C, et al. Effect of Spherical Equivalent Error on Visual Acuity at Various Distances in Eyes With a Trifocal Intraocular Lens. J Refract Surg 2019;35:274-9. 10.3928/1081597X-20190404-01 [DOI] [PubMed] [Google Scholar]
- 39.Muñoz G, Albarrán-Diego C, Sakla HF. Autorefraction after multifocal IOLs. Ophthalmology 2007;114:2100. 10.1016/j.ophtha.2007.05.049 [DOI] [PubMed] [Google Scholar]
- 40.Bissen-Miyajima H, Minami K, Yoshino M, et al. Autorefraction after implantation of diffractive multifocal intraocular lenses. J Cataract Refract Surg 2010;36:553-6. 10.1016/j.jcrs.2009.10.047 [DOI] [PubMed] [Google Scholar]
- 41.Muñoz G, Albarrán-Diego C, Sakla HF. Validity of autorefraction after cataract surgery with multifocal ReZoom intraocular lens implantation. J Cataract Refract Surg 2007;33:1573-8. 10.1016/j.jcrs.2007.05.024 [DOI] [PubMed] [Google Scholar]
- 42.van der Linden JW, Vrijman V, Al-Saady R, et al. Autorefraction versus subjective refraction in a radially asymmetric multifocal intraocular lens. Acta Ophthalmol 2014;92:764-8. 10.1111/aos.12410 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as