

Abstract
Background
Recurrent vulvovaginal candidiasis (RVVC) affects up to 5% of women. No comprehensive systematic review of treatments for RVVC has been published.
Objectives
The primary objective was to assess the effectiveness and safety of pharmacological and non‐pharmacological treatments for RVVC. The secondary objective was to assess patient preference of treatment options.
Search methods
We conducted electronic searches of bibliographic databases, including CENTRAL, MEDLINE, Embase, and CINAHL (search date 6 October 2021). We also handsearched reference lists of identified trials and contacted authors of identified trials, experts in RVVC, and manufacturers of products for vulvovaginal candidiasis.
Selection criteria
We considered all published and unpublished randomised controlled trials evaluating RVVC treatments for at least six months, in women with four or more symptomatic episodes of vulvovaginal candidiasis in the past year. We excluded women with immunosuppressive disorders or taking immunosuppressant medication. We included women with diabetes mellitus and pregnant women.
Diagnosis of RVVC must have been confirmed by presence of symptoms and a positive culture and/or microscopy. We included all drug and non‐drug therapies and partner treatment, assessing the following primary outcomes:
• number of clinical recurrences per participant per year (recurrence defined as clinical signs and positive culture/microscopy); • proportion of participants with at least one clinical recurrence during the treatment and follow‐up period; and • adverse events.
Data collection and analysis
Two authors independently reviewed titles and abstracts to identify eligible trials. Duplicate data extraction was completed independently by two authors. We assessed risk of bias as described in the Cochrane Handbook for Systematic Reviews of Interventions. We used the fixed‐effects model for pooling and expressed the results as risk ratio (RR) with 95% confidence intervals (CI). Where important statistical heterogeneity was present we either did not pool data (I2 > 70%) or used a random‐effects model (I2 40‐70%). We used the GRADE tool to assess overall certainty of the evidence for the pooled primary outcomes.
Main results
Studies: Twenty‐three studies involving 2212 women aged 17 to 67 years met the inclusion criteria. Most studies excluded pregnant women and women with diabetes or immunosuppression. The predominant species found on culture at study entry was Candida albicans. Overall, the included studies were small (<100 participants). Six studies compared antifungal treatment with placebo (607 participants); four studies compared oral versus topical antifungals (543 participants); one study compared different oral antifungals (45 participants); two studies compared different dosing regimens for antifungals (100 participants); one study compared two different dosing regimens of the same topical agent (23 participants); one study compared short versus longer treatment duration (26 participants); two studies assessed the effect of partner treatment (98 participants); one study compared a complementary treatment (Lactobacillus vaginal tablets and probiotic oral tablets) with placebo (34 participants); three studies compared complementary medicine with antifungals (354 participants); two studies compared 'dermasilk' briefs with cotton briefs (130 participants); one study examined Lactobacillus vaccination versus heliotherapy versus ciclopyroxolamine (90 participants); one study compared CAM treatments to an antifungal treatment combined with CAM treatments (68 participants). We did not find any studies comparing different topical antifungals. Nine studies reported industry funding, three were funded by an independent source and eleven did not report their funding source.
Risk of bias: Overall, the risk of bias was high or unclear due to insufficient blinding of allocation and participants and poor reporting.
Primary outcomes: Meta‐analyses comparing drug treatments (oral and topical) with placebo or no treatment showed there may be a clinically relevant reduction in clinical recurrence at 6 months (RR 0.36, 95% CI 0.21 to 0.63; number needed to treat for an additional beneficial outcome (NNTB) = 2; participants = 607; studies = 6; I² = 82%; low‐certainty evidence) and 12 months (RR 0.80, 95% CI 0.72 to 0.89; NNTB = 6; participants = 585; studies = 6; I² = 21%; low‐certainty evidence). No study reported on the number of clinical recurrences per participant per year.
We are very uncertain whether oral drug treatment compared to topical treatment increases the risk of clinical recurrence at 6 months (RR 1.66, 95% CI 0.83 to 3.31; participants = 206; studies = 3; I² = 0%; very low‐certainty evidence) and reduces the risk of clinical recurrence at 12 months (RR 0.95, 95% CI 0.71 to 1.27; participants = 206; studies = 3; I² = 10%; very low‐certainty evidence). No study reported on the number of clinical recurrences per participant per year.
Adverse events were scarce across both treatment and control groups in both comparisons. The reporting of adverse events varied amongst studies, was generally of very low quality and could not be pooled. Overall the adverse event rate was low for both placebo and treatment arms and ranged from less than 5% to no side effects or complications.
Authors' conclusions
In women with RVVC, treatment with oral or topical antifungals may reduce symptomatic clinical recurrences when compared to placebo or no treatment. We were unable to find clear differences between different treatment options (e.g. oral versus topical treatment, different doses and durations). These findings are not applicable to pregnant or immunocompromised women and women with diabetes as the studies did not include or report on them. More research is needed to determine the optimal medication, dose and frequency.
Plain language summary
The effectiveness and safety of treatments for recurrent vulvovaginal candidiasis (thrush)
Review question
Cochrane authors set out to investigate the effectiveness and safety of drug treatments or non‐drug treatments (such as complementary and alternative medicines) for women with recurrent vulvovaginal candidiasis (thrush).
Background
Thrush of the vaginal/vulvar area is caused by Candida, a form of yeast that is commonly found in the vagina as part of normal flora without causing symptoms. For unknown reasons, Candida can start growing and cause symptoms of vulvovaginal candidiasis (commonly named thrush). Symptoms of vulvovaginal thrush include itching, swelling, and irritation of the vaginal and vulval areas. It is estimated that uncomplicated vulvovaginal thrush affects up to 75% of women at some time during their reproductive years. Recurrent vulvovaginal candidiasis (RVVC) occurs when a woman has four or more fungal infections during a 12‐month period. Up to 5% of women suffer from RVVC. Some doctors advise taking antifungals as a prevention, but there are no clear evidence‐based guidelines.
Study characteristics
We identified 23 studies involving 2212 participants between 17 and 67 years old with a diagnosis of RVVC confirmed by a positive test. The studies compared a range of antifungal medicines (taken by mouth or inserted into the vagina), and some complementary or alternative treatments (such as Lactobacillus vaccines or probiotics and special underwear). The studies reported the effects on recurrence of thrush after 6 and 12 months. Only one study reported the number of clinical recurrences at 12 months. Nine studies reported industry funding, three were funded by an independent source and nine studies did not report their funding source. The evidence is current to October 2021.
Key results
Six studies (607 participants) compared antifungal medication with placebo or no treatment. Based on low certainty evidence antifungal treatments may give a clinically relevant reduction in clinical recurrence at 6 and 12 months. We are uncertain if oral treatments are better than topical treatments (very low certainty evidence for no difference).
Adverse effects of taking antifungal medication to prevent recurrence of thrush were not common. Studies reported on adverse effects differently, making comparisons difficult. More research is needed to determine the optimal medication, dose and frequency. We were unable to determine the effects in women who are pregnant or have diabetes.
Certainty of the evidence
Our confidence in the evidence was low to very low due to serious concerns about risk of bias, unclear reporting and the limited number of studies that could be combined. This means that new studies might change our confidence in the effects of treatments and our conclusions.
Summary of findings
Background
Description of the condition
Candida is a yeast that is commonly found in the vagina as part of normal flora without causing symptoms. For largely unknown reasons, Candida changes from being a commensal organism (i.e. it can live in the environment without causing problems for the host) to a pathogenic one (Sobel 2007), which causes symptoms of vulvovaginal candidiasis (VVC, commonly named thrush) (Sobel 2007). VVC can be diagnosed clinically, with signs and symptoms including vaginal itching or burning with or without redness and swelling of the vulvae, and a white discharge, and stinging or burning when passing urine. Diagnosis can be confirmed with a wet mount preparation (saline with 10% KOH) or Gram stain of the discharge, which will show budding yeasts and hyphae under the microscope, and/or a culture of Candida (CDC 2015).
It is estimated that uncomplicated VVC affects up to 75% of women some time during their reproductive years (Sobel 2007), although these figures have been disputed (Rathod 2014). Predisposing factors have been identified for uncomplicated VVC (Patel 2004), which include the use of antibiotics, hormone replacement therapy, pregnancy, diabetes mellitus, genetic factors, and behavioural factors (Sobel 2006).
Up to 5% of women suffer from recurrent vulvovaginal candidiasis (RVVC), which is commonly defined as four or more episodes of VVC in a 12‐month period (Sobel 2007). On a global scale RVVC affects approximately 138 million women each year (range 103‐172 million). The global prevalence is estimated as 3871 per 100 000 women with 372 million women affected over their lifetime (Denning 2018), specifically women between 25 and 35 years old. Denning calculated that in high‐income countries the economic burden of lost productivity could be as high as US$14.39 billion per year (Denning 2018). The role of predisposing factors for uncomplicated vulvovaginal candidiasis is not certain in RVVC. In approximately half of women with RVVC, no risk factors can be identified (Nyirjesy 2008).
The aetiology of RVVC is unclear. Most cases (85% to 95%) of uncomplicated vulvovaginal candidiasis are caused by Candida albicans. However, less common candidal species such as Candida glabrata may be implicated in RVVC. Vaginitis caused by non‐albicans species tends to be more resistant to treatment (Sobel 2007). Many theories, such as maladaptive immune response and involvement of polymorphonuclear leucocytes, remain controversial (Fidel 1998; Peters 2014; Sobel 2007), and the role of individual and genetic susceptibility has not yet been defined (Sobel 2007).
The effects of RVVC on the intimate relationships and daily living of women can be significant. Ehrstrom 2007 found that women with RVVC were significantly more likely to report signs of burnout, emotional and physical stress, and poor work‐life balance than a control group of women without RVVC. The major impact of the physical symptoms, including discharge, itchiness, pain and psychological effects, often goes unrecognised (Chapple 2000). Additionally, in some countries long‐term treatment can be expensive (Sobel 2014), and approximately 50% of women experience recurrence of symptoms within months of finishing treatment (Sobel 2004b).
Description of the intervention
Management of uncomplicated vulvovaginal candidiasis usually consists of topical or oral antifungal treatments with frequency ranging from a single dose to treatment for up to 14 days (Pappas 2015; Therapeutic Guidelines 2015). Antifungal drugs fall broadly into five classes: polyenes, azoles, allylamines, echinocandins, and other agents, including griseofulvin and flucytosine (Chen 2007). The most commonly recommended antifungals for the treatment of vulvovaginal thrush are azoles (e.g. clotrimazole, fluconazole, itraconazole, miconazole, ketoconazole) and nystatin (a polyene). These treatments have been shown to be effective as topical treatment in pregnant women (Young 2001) and non‐pregnant women (Lopez 2013). Systematic reviews (Lopez 2013; Nurbhai 2007 and Watson 2002) found that oral and intravaginal (topical) treatments were equally effective in women with uncomplicated acute (i.e. less than four episodes in 12 months) vulvovaginal candidiasis, but Nurbhai 2007 found that women generally prefer oral treatment.
The recommended treatment regimen for complicated vulvovaginitis such as RVVC as outlined in clinical guidelines is not effective for all women (Pappas 2015; Therapeutic Guidelines 2015), whether oral or topical (Shahid 2009). Some women experience adverse effects including headache, abdominal pain, and nausea with oral treatment and dyspareunia or irritation with vaginal treatment (Sobel 1995; Stein 1993).
Topical antifungal agents are applied to the vaginal mucosa, and are delivered in the form of creams or pessaries. Oral antifungal treatment exists in the form of tablets or capsules. The currently recommended treatment for RVVC rarely cures this condition but rather aims to suppress symptoms (Pappas 2015). Initially high doses of oral or topical antifungal agents are used for up to two weeks to induce suppression of symptoms. In severe cases, the suppression of symptoms may take up to six months (Sobel 2004b). This suppression period is followed by long‐term regular (weekly or monthly) antifungal treatment to maintain clinical remission (Pappas 2015; Therapeutic Guidelines 2015).
Hormones, such as depo‐medroxyprogesterone (Falagas 2006; Miller 2000) have been suggested as treatment for VVC, but their efficacy has been questioned by some studies (Pirotta 2004), and the lack of supporting evidence has been highlighted by others (Van Kessel 2003).
Other treatment options include changing contraceptive, partner treatment, and use of topical gentian violet. These options have been poorly researched.
Conventional treatment of RVVC is not always successful and often involves long‐term or multiple treatments (Pappas 2015; Therapeutic Guidelines 2015). Significant variation in approach is seen between individual practitioners (Watson 2011). Due either to the limitations of current treatments or patient preference, many women seek treatment alternatives. Complementary and alternative medicine (CAM) is highly acceptable to women and is widely used in managing this condition (Nyirjesy 2001). One study found that up to 40% of women use CAM to treat or prevent vulvovaginal candidiasis despite the wide availability of conventional antifungal agents (Pirotta 2003). Examples of CAM used are herbal preparations such as tea tree oil, garlic, probiotics such as Lactobacillus, and vaginal acidifying agents. Evaluation of the effectiveness and safety of CAM for vulvovaginal candidiasis in the literature has been sparse. A review of the evidence concludes the effectiveness of oral or intravaginal garlic, intravaginal teat tree oil and yoghurt (containing Lactobacillus acidophilus) either oral or intravaginal, is unknown (Lopez 2013). Garlic taken orally can cause gastro‐intestinal symptoms such as heartburn, nausea, diarrhoea and bloating, and prolonged intravaginal use may result in allergic reactions or chemical burns (Lopez 2013). Topical tea tree oil can irritate the skin and cause a severe allergic rash (Lopez 2013). Yoghurt can cause gastrointestinal discomfort in people with lactose intolerance (Lopez 2013).
A fungal immunotherapeutic vaccine (NDV‐3A) has recently been the subject of phase 2 trials and shows potential in reducing recurrences of VVC (Edwards 2018). Given that resistance to conventional antifungal treatment for RVVC has been reported and that conventional therapy does not work for all women (Sobel 2016), it is vital to investigate novel treatments that may increase options for RVVC management.
How the intervention might work
The mode of action of antifungal agents is generally fungistatic, that is they Interfere with biosynthesis or integrity of ergosterol, the major sterol in the fungal cell membrane, and induce breakdown of the fungal cell wall (Chen 2007; Wildfeuer 1997). The most commonly used antifungal class is the azoles, which is made up of the imidazoles (e.g. ketoconazole, miconazole, clotrimazole and econazole) and the triazoles (e.g. fluconazole and itraconazole) (Chen 2007). Imidazole drugs are used in superficial fungal infections, while triazoles have a place in both superficial and invasive fungal infections (Chen 2007). The azoles act by inhibiting the fungal cytochrome P450–Erg11p or cytochrome P51p enzymes, inhibiting 14a‐demethylation of lanosterol in the ergosterol biosynthetic pathway (Odds 2003). This alters the fluidity and permeability of the fungal cell wall.
Alteration of the host environment so that it is less favourable for the proliferation of Candida is the underlying theory supporting the use of other therapies such as probiotics, gels used to restore vaginal acid balance, and treatments such as depo‐medroxyprogesterone (Falagas 2006; Miller 2000).
Some less commonly used treatments such as immunotherapy claim to promote the restoration of the immune system (Moraes 2000).
Why it is important to do this review
A number of systematic reviews address treatment options for uncomplicated acute VVC (Nurbhai 2007; Xie 2017; Young 2001). However, RVVC poses different challenges and there is currently no comprehensive systematic review of the treatment options for RVVC. Available guidelines are based on consensus only. RVVC is a common condition that can severely impact women and their partners both physically and psychologically. Many treatments are expensive, and the evidence for the efficacy of several treatments has not been systematically collated. There are also concerns about safety, especially for the non‐conventional complementary and alternative treatment. Evaluation of the many therapies used to manage this condition is essential to provide information so that women and their healthcare practitioners can make informed decisions about the management of RVVC.
Objectives
The primary objective of this systematic review was to assess the effectiveness and safety of pharmacological and non‐pharmacological treatments for recurrent vulvovaginal candidiasis. The secondary objective of the review was to assess patient preference of these treatment options.
Methods
Criteria for considering studies for this review
Types of studies
We considered all published and unpublished randomised controlled trials evaluating treatments for RVVC for at least six months for inclusion. Outcome measurement at six months was considered meaningful as the focus of this review is on managing a recurring condition rather than managing a single episode. We considered all types of randomised trials (including parallel and cluster randomised trials). We did not identify any cluster‐randomised trials.
Types of participants
We included all women with at least four symptomatic episodes in the past year of vulvovaginal candidiasis, confirmed by the presence of symptoms and a positive culture or symptoms and positive microscopy. We included women with diabetes and women who are pregnant. We excluded women with immunosuppressive disorders or taking immunosuppressant medication.
We included all settings (e.g. family medicine clinic, gynaecology outpatient clinic, sexually transmitted disease or family planning clinic).
Types of interventions
We considered the following interventions.
Antifungal treatments, administered intravaginally or orally
Other treatments for candida vulvovaginitis, such as probiotics, gentian violet, acidifying agents (including cider vinegar, boric acid, and vaginal gels), tea tree oil, douching, garlic and dietary modification
Partner treatment
We made the following comparisons.
Drug treatment (oral and topical) versus placebo/no treatment (excluding partner treatment)
Oral drug treatment versus topical drug treatment
Oral drug treatment versus oral drug treatment
Topical drug treatment versus topical drug treatment
Comparison of different doses of the same agent
Short duration of treatment versus longer duration of treatment
Partner treatment versus placebo/no treatment
Complementary and alternative medicine versus placebo/no treatment
Complementary and alternative medicine versus drug treatments
Complementary and alternative medicine versus non‐drug treatments
Vaccination versus other treatment
Types of outcome measures
We included the following primary and secondary outcome measures.
Primary outcomes
Number of clinical recurrences per participant per year (recurrence defined as clinical features and positive culture or microscopy)
Proportion of participants with at least one clinical recurrence during the treatment and follow‐up period
Adverse events
Secondary outcomes
Time to first recurrence
Number of symptomatic days per year
Number of mycological recurrences per participant per year
Proportion of participants with at least one mycological recurrence during the treatment and follow‐up period
Duration of symptoms after treatment initiation
Patient preference
Search methods for identification of studies
We attempted to identify as many relevant randomised controlled trials (RCTs) as possible of "treatment" for "recurrent vulvovaginal candidiasis", irrespective of language of publication, publication date, and publication status (published, unpublished, in press, and in progress). We used both electronic searching in bibliographic databases and handsearching, as described in the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2017).
Electronic searches
We contacted the Information Specialist of the Cochrane Sexually Transmitted Infections Group and our local Information Specialist to design a comprehensive search strategy to identify as many relevant RCTs as possible in the electronic databases. We used a combination of controlled vocabulary (MeSH, Emtree, DeCS, including exploded terms) and free‐text terms (considering spelling variants, synonyms, acronyms and truncation) for "vulvovaginal candidiasis" and "recurrence", with field labels, proximity operators, and Boolean operators. There were no date or language restrictions.
We searched the following electronic databases.
Cochrane Central Register of Studies Online (CENTRAL) (inception to 6 October 2021) (Appendix 1)
MEDLINE, Ovid platform (1946 to 6 October 2021) (Appendix 1)
Embase, Embase.com platform (inception to 6 October 2021) (Appendix 1)
CINAHL (Cumulative Index to Nursing and Allied Health Literature) (inception to 11 September 2020) (Appendix 2). Any later CINAHL output is contained in the CENTRAL 6 October 2021 search output.
The following appendices present earlier searches of CENTRAL (Appendix 3; Appendix 4), MEDLINE (Appendix 3; Appendix 5), Embase (Appendix 3; Appendix 6), Web of Science (Appendix 7), and ProQuest (Appendix 8).
For MEDLINE, we used the Cochrane Highly Sensitive Search Strategy for identifying RCTs: sensitivity‐ and precision‐maximising version Ovid format (Deeks 2017).
Searching other resources
We searched the following trial registers on 27 July 2019. Ongoing trials from both trial registries were included in the 2021 CENTRAL search.
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (clinicaltrials.gov/) (Appendix 9)
World Health Organization International Clinical Trials Registry Platform (apps.who.int/trialsearch/) (Appendix 10)
We handsearched reference lists of systematic reviews, other relevant publications on the same topic, and the reference lists of all included studies to identify further potentially eligible studies. We also contacted the authors of identified trials, experts in RVVC, and manufacturers producing products for vulvovaginal candidiasis to identify unpublished studies.
Data collection and analysis
Selection of studies
Two review authors (GC and CW) independently reviewed the titles and abstracts identified by the search for potentially relevant studies and then assessed the full texts of those studies deemed potentially relevant for inclusion in the review. We excluded double publications and reports of the same study at different points of time of follow up. Any disagreements were resolved by discussion or by consulting with a third review author (MVD). We contacted trial authors if we needed more information before deciding on inclusion.
Data extraction and management
Two review authors (GC and CW) independently extracted data using a paper data extraction form. Any discrepancies were resolved by discussion or by consulting with a third review author (MVD). The data extraction form included information on study citation; study characteristics (design, sample size, randomisation method, blinding, measurement of outcomes, method of analysis, (intention‐to‐treat, per protocol, etc.), duration of follow‐up; population (age of participants, inclusion and exclusion criteria, setting, number of excluded patients, number lost to follow up, number of analysed patients); interventions (drugs/treatments, dose, route of administration, duration of treatment, comparisons); outcomes (primary and secondary outcomes, including definition of objective and subjective outcomes, attrition); and other issues (including information on funding) (see Characteristics of included studies). We contacted authors for additional clarification or information if necessary. We performed data analysis using Review Manager 5 software (Review Manager 2014).
Assessment of risk of bias in included studies
Four review authors (JS, MP, LD, and MVD) independently evaluated risk of bias in the included trials as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), including assessment of sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and other sources of bias. Any discrepancies were resolved by discussion or by consulting with a third review author (MVD or GC). We contacted authors of trials for more information if necessary.
We assessed the risk as 'low' if sufficient information was reported and the method described was adequate. We assessed the risk as 'high' if the described method was inadequate or if there was insufficient information to permit an assessment and it was likely that a rigorous method was not used. We assessed the risk of bias as 'unclear' if insufficient information was reported to permit assessment of the methods used.
Random sequence generation (selection bias)
We assessed the method used to generate the allocation sequence as described in the study publication (and/or protocol if available) as:
'low risk' if a random process was used, e.g. random number table or computer random number generator;
'high risk' if a non‐random process was used, e.g. odd or even date of birth, alternating dates, hospital record number; or
'unclear risk' if the trial is described as randomised, but the method used for the allocation sequence generation is not or is insufficiently described.
Allocation concealment (selection bias)
We assessed the method used to conceal the allocation sequence as described in the study publication (and/or protocol if available) as: • 'low risk' if an appropriately concealed method was used (e.g. central randomisation; sealed, opaque envelopes); • 'high risk' if open random allocation was used or other unblinded methods (e.g. unsealed or non‐opaque envelopes, alternate dates); or • 'unclear risk' if the trial is described as randomised but the method used to conceal sequence allocation is not or is insufficiently described.
Blinding of participants and personnel (performance bias)
We assessed the method used to ensure blinding of participants and personnel as described in the study publication (and/or protocol if available) as:
• 'low risk' if an appropriate method of blinding was used (e.g. identical appearance of treatments and identical administration routines); • 'high risk' if the method used was transparent (e.g. oral versus topical administration); or • 'unclear risk' if the trial is described as blinded but the method used to ensure blinding is not or is insufficiently described.
Blinding of outcome assessment (detection bias)
We assessed the risk of bias related to blinding of outcome assessment as described in the study publication (and/or protocol if available) as:
• 'low risk' if outcome assessors were unable to determine the treatment allocated; • 'high risk' if outcome assessors had knowledge or could have had knowledge of the allocated treatment, and this could have influenced their assessment (e.g. in the case of instruments assessed through interview); or • 'unclear risk' if information about blinding of outcome assessors was insufficient to permit a judgement of low or high risk of bias.
Incomplete outcome data (attrition bias)
For each study, we reported the number of participants randomised and the number for whom outcomes were reported for the different outcomes and at different time points. We assessed the completeness of reporting and attrition as described in the study publication as: • 'low risk' if outcomes are reported for all or more than 80% of randomised participants across groups; • 'high risk' if missing data are not balanced between groups and/or outcome data are missing for > 20% of randomised participants and no explanation is provided; or • 'unclear risk' if this is insufficiently described.
Selective reporting bias
We assessed the risk of reporting bias by comparing the outcomes reported in the study protocol (if available) or the methods section of the published trial report with the outcomes reported in the results section of the published trial report as: • 'low risk' if it is clear that all of the study’s prespecified outcomes have been reported; • 'high risk' if not all of the study’s prespecified outcomes have been reported or one or more reported primary outcomes were not prespecified; or
•'unclear risk' if the information provided in the study report is insufficient.
Other bias
We assessed the risk of other types of bias such as conflicts of interest or funding sources that could have impacted the study results as: • 'low risk' of other bias; • 'high risk' of other bias; or • 'unclear risk' of other bias.
We took risk of bias into account when making a judgement about the overall certainty of the pooled evidence as per the GRADE tool.
Measures of treatment effect
For dichotomous data, we reported the results as risk ratios with 95% confidence intervals. For continuous data, we planned to report mean difference of pre‐ and post‐measurements or weighted mean difference if different scales were used. We also reported standard deviations.
Unit of analysis issues
The unit of analysis in meta‐analysis was the woman. If the woman is not the unit of randomisation, such as is the case in cluster‐randomised trials, we would make adjustments for clustering following the guidelines in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). In the case of multiple study arms, we combined the active interventions if this was clinically appropriate and compared them to placebo, in order to avoid double counting.
Dealing with missing data
We attempted to obtain information on missing data from study authors. If this was not successful, we performed intention‐to‐treat (ITT) analysis, which considers all missing data as treatment failures. We followed the guidance in the Cochrane Handbook for Systematic Reviews of Interventions to perform a sensitivity analysis that explored the impact of studies with high risk of bias due to large numbers of missing data (Higgins 2011).
Assessment of heterogeneity
We assessed heterogeneity between trials that investigate effects of the same interventions in two ways. Before pooling, we first explored clinical, face value heterogeneity (study populations, interventions, etc.). If we considered the trials to be too different (e.g. clinically different populations, different interventions, clinically non‐comparable outcomes), we did not pool the studies. We then assessed statistical heterogeneity by visual exploration of the results on the forest plot and by performing a Chi2 test and calculating the Higgins I2 statistic according to the guidelines in the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2017). We interpreted the I2 value as follows (Higgins 2011):
0% to 40%: may not be important; a fixed effects model is recommended;
40% to 70%: may represent moderate heterogeneity; a random effects model is recommended;
>70%: may represent substantial heterogeneity; pooling is not recommended.
Assessment of reporting biases
If outcome data for relevant outcomes that were mentioned in the study protocol or methods of the study publication were not reported (i.e. risk of reporting bias), we contacted the authors to request information about the missing outcome data. We planned to assess publication bias by generating funnel plots if 10 or more trials were available for the comparison (Higgins 2011).
Data synthesis
We used Review Manager 5 software to perform the statistical analysis (Review Manager 2014). Where we judged the trial populations, methods, and outcome measures to be similar (low clinical heterogeneity), and the I2 was less than 40% (low statistical heterogeneity), we pooled the data using a fixed‐effect model (Higgins 2011). We did not pool data when there was obvious clinical heterogeneity and pooling studies did not make clinical sense (see Assessment of heterogeneity). Where statistical heterogeneity was moderate (I2 40% to 70%) or substantial (I2 >70%), we pooled the data using a random‐effects model and performed a sensitivity analysis to assess the impact of heterogeneity on the robustness of the overall effect estimate (see Sensitivity analysis) (Higgins 2011).
We calculated a number needed to treat for an additional beneficial outcome (NNTB) and a number needed to treat for an additional harmful outcome (NNTH) where data were available and the results were statistically significant. We used the formulae provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Subgroup analysis and investigation of heterogeneity
We planned to carry out the following subgroup analyses based on relevant variables.
Sexually active women versus non‐sexually active women
Pregnant versus non‐pregnant women
Women with diabetes mellitus versus non‐diabetic women
RVVC caused by Candida albicans versus non‐albicans species
Heterogeneity was assessed as per the guidance in Assessment of heterogeneity.
Sensitivity analysis
We performed the following sensitivity analyses:
To assess the effect of risk of selection bias on the overall estimate of the meta‐analysis we first pooled all studies and then we excluded those studies with high risk of selection bias in order to evaluate the change in the pooled effect estimator.
Summary of findings and assessment of the certainty of the evidence
We generated the Summary of findings tables using GRADEpro and Cochrane methods (Higgins 2011; GRADEpro GDT). These tables evaluate the overall quality of the body of evidence for the main review outcomes (proportion of participants with at least one clinical recurrence during the treatment and follow‐up period, adverse events) for the main review comparisons (Drug treatment (oral and topical) versus placebo/no treatment (excluding partner treatment) and Oral drug treatment versus topical drug treatment). We assessed the certainty of the evidence using GRADE criteria (risk of bias, consistency of effect, imprecision, indirectness and publication bias). Judgements about evidence certainty (high, moderate, low or very low) were made by two review authors working independently (GC and LD), with disagreements resolved by discussion and an arbiter (MVD). We give a narrative description of the effects taking into account the level of certainty as per the handbook recommendations (Higgins 2011).
Results
Description of studies
The results of the searches and included and excluded studies are described below.
Results of the search
The searches up to 6 October 2021 identified 1782 references from electronic databases (trial registries excluded). We identified an additional four publications from contacting experts in the field (including the authors of this review) (Fan 2015; Fardyazar 2007 (2 publications); (Sobel 1985a), and one additional publication from contacting manufacturers (Merkus 1990). Our review of reference lists of included studies and publications selected from the electronic database searches identified one full‐text study for review (Guaschino 2001). We identified a further study from the trial registry searches (Rabiee 2013). After removal of duplicates, 1181 abstracts were available for review. Of these 1070 were excluded as they did not meet our inclusion criteria. We selected a total of 111 abstracts for full‐text review (Figure 1). Eighty‐two studies were excluded because participants did not have RVVC (n = 57), the study was not an RCT (n = 17), the duration of follow‐up was less than 6 months (n = 6), or the study was not a primary study (n = 2). Six full‐text publications contained inadequate information to permit a decision regarding inclusion in the review (Coric 2006; Diba 2010; Fan 2005; Houang 1989; Miller 1984; Shalev 1996); we contacted the authors of these studies, but none of these publications were found to be suitable for inclusion.
1.
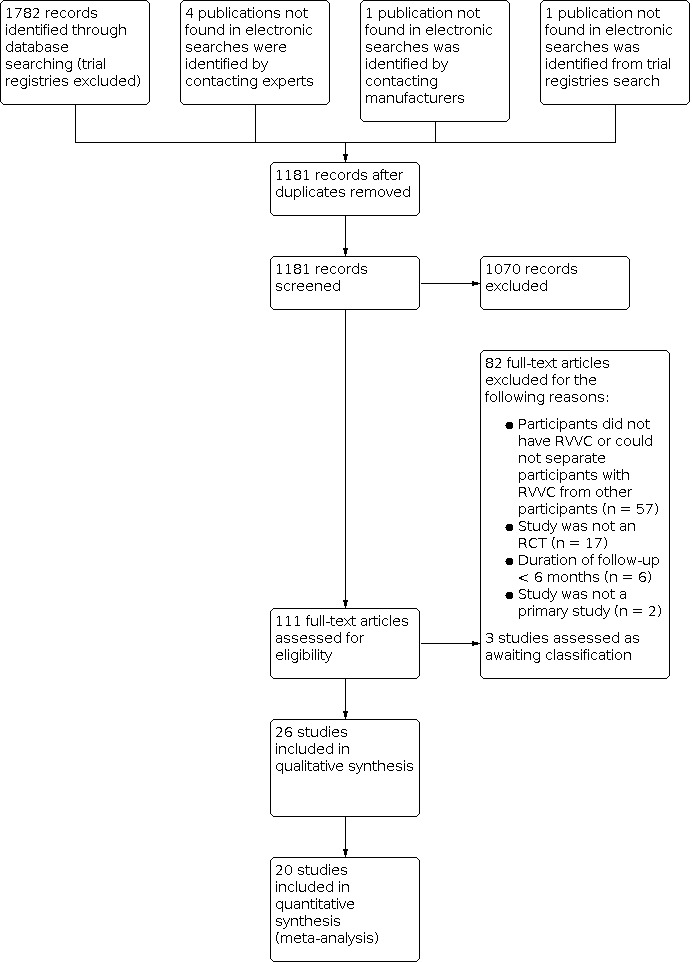
Study flow diagram.
Two studies were not published in English and we have placed them in Awaiting classification pending translation into English (Rabiee 2013 ‐ published in Persian; Zivaljevic 2012 ‐ published in Serbian). In one study it was not clear if women met the inclusion criteria for our review (Russo 2019).
Our search in 2020 identified three registered ongoing trials: NCT04029116 is recruiting, NCT04208555 is not yet recruiting. For EUCTR2019‐000925‐27‐SK it is unclear if recruitment has started, however, this trial has also been registered in clinicaltrials.gov which reports the trial is still recruiting (NCT04734405). We identified 10 additional trials from the trial registry searches in 2020, however, no publication was located for these trials. We contacted the primary contact identified in the database record, but received no additional information or trial results for seven trials (ACTRN12614001258640; ChiCTR‐IPR‐15006314; ChiCTR‐TRC‐10000833; EUCTR2013‐002480‐26‐PL; NCT00479947; NCT02251093; RBR‐892mp4). The contact listed in the database record could not be contacted for three trials (EUCTR2010‐021502‐38‐DE; EUCTR2011‐004718‐40‐IT; NCT00915629), either because there were insufficient details in the database or the details were not current. Thus this study has been assessed as awaiting classification.
The search in October 2021 identified three additional trials in clinicaltrials.gov: NCT04292704 is still recruiting; NCT04639544 and NCT04699240 have been assessed as awaiting classification as it is unclear from the information in the trials database whether microbiological confirmation of VVC was an inclusion criterion. NCT04734405 was identified as a duplicate registration of EUCTR2019‐000925‐27‐SK.
Included studies
We included 23 studies involving a total of 2212 participants in the review. We identified 20 studies from the electronic searches (Bolouri 2009; Chopra 2013; Corthay 1988; D'Antuono 2012; D'Antuono 2013; Fong 1992a; Fong 1992b; Fong 1994; Kumari 2011; Li 2018; Lopez‐Olmos 2000; Mendling 2011; Metts 2003; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spacek 2005; Spinillo 1997; Witt 2009). The remaining three studies were identified from the personal libraries of authors of this review (Fan 2015; Fardyazar 2007; Sobel 1985a). However, three studies did not report data for our primary outcomes in a way that could be extracted (Corthay 1988; D'Antuono 2013; Li 2018). We requested further information from D'Antuono 2013; Li 2018, but unfortunately the authors were not able to provide us with the required data. Corthay 1988 was a conference abstract from 1988 and the authors could not be traced.
Participants and setting
Overall, the included studies were small, with 16 of the 23 studies including fewer than 100 participants (Bolouri 2009; Corthay 1988; D'Antuono 2013; Fong 1992a; Fong 1992b; Fong 1994; Kumari 2011; Li 2018; Lopez‐Olmos 2000; Mendling 2011; Metts 2003; Roth 1990; Sobel 1985a; Sobel 1986; Sobel 1989; Spacek 2005). The largest study included 387 participants (Sobel 2004). Eleven studies excluded participants with diabetes (Bolouri 2009; Chopra 2013; D'Antuono 2012; D'Antuono 2013; Fong 1992a; Fong 1992b; Fong 1994; Kumari 2011; Mendling 2011; Spinillo 1997; Witt 2009). One study had no participants with diabetes (Sobel 1989). Five studies did not explicitly exclude women with diabetes but did not state if any participants had diabetes (Corthay 1988; Metts 2003; Roth 1990; Spacek 2005; Witt 2009). Six studies included some participants with diabetes. One study included a single participant with diabetes (Fan 2015). Almost 7% of participants had diabetes in Lopez‐Olmos 2000, and 11% of participants had diabetes in Fardyazar 2007, one had 3% (Sobel 1985a), one had 2% (Sobel 1986), and one had 2% in the fluconazole group and 5% in the placebo group (Sobel 2004).
We did not find any study including pregnant women. Eighteen studies excluded pregnant women (Bolouri 2009; Chopra 2013; D'Antuono 2012; D'Antuono 2013; Fan 2015; Fong 1992a; Kumari 2011; Li 2018; Mendling 2011; Metts 2003; Roth 1990; Sobel 1985a; Sobel 1986; Sobel 1989; Sobel 2004; Spacek 2005; Spinillo 1997; Witt 2009). One study did not exclude pregnant women, but none enrolled (Fardyazar 2007). Four further studies also did not explicitly exclude pregnant women, but did not state if any participants were pregnant (Corthay 1988; Fong 1992b; Fong 1994; Lopez‐Olmos 2000).
Five studies required participants to have a culture C albicans at enrolment (Roth 1990; Sobel 1985a; Sobel 1986; Spinillo 1997; Witt 2009). Nine studies did not report the prevalence of C albicans at enrolment (Corthay 1988; Chopra 2013; Fardyazar 2007; Fong 1992a; Fong 1992b; Fong 1994; Li 2018; Mendling 2011; Metts 2003). In the remaining studies, the predominant Candida species at enrolment was C albicans, with between 27% and 100%. Lopez‐Olmos 2000 did not require a positive culture at enrolment; however, if the culture was positive, it was most commonly C albicans.
Five studies required women to have a negative culture for Candida spp prior to commencing the treatment phase (Bolouri 2009; Fan 2015; Roth 1990; Sobel 1989; Sobel 2004). In one study participants were given additional treatment to achieve negative cultures for Candida spp (Spinillo 1997), and in four studies participants did not need to have a negative culture for Candida spp (Fardyazar 2007; Fong 1992a; Li 2018; Sobel 1986).
The most common setting was an outpatient clinic (Bolouri 2009; Chopra 2013; D'Antuono 2012; D'Antuono 2013; Fan 2015; Fardyazar 2007; Fong 1992a; Fong 1992b; Kumari 2011; Li 2018; Spacek 2005; Spinillo 1997; Witt 2009). One study was conducted exclusively in a primary care setting (a university student health centre) (Metts 2003). Two studies included participants from multiple sites (gynaecology/family planning clinics) (Lopez‐Olmos 2000; Mendling 2011). A third study was also multicentre, but the settings were not described (Sobel 2004). The setting was not stated in six studies (Corthay 1988; Fong 1994; Roth 1990; Sobel 1985a; Sobel 1986; Sobel 1989).
Ten studies were conducted in Europe (Austria, the Czech Republic, Germany, Italy, Spain, and Sweden) (Chopra 2013; D'Antuono 2012; D'Antuono 2013; Kumari 2011; Lopez‐Olmos 2000; Mendling 2011; Roth 1990; Spacek 2005; Spinillo 1997; Witt 2009), and eight in North America (Fong 1992a; Fong 1992b; Fong 1994; Metts 2003; Sobel 1985a; Sobel 1986; Sobel 1989; Sobel 2004). One study did not state the location (Corthay 1988). The remaining four studies were conducted in Asia, two in Iran ( Bolouri 2009; Fardyazar 2007) and two in China (Fan 2015; Li 2018).
Interventions and comparators
The included studies involved a variety of comparisons. Six studies compared drug treatments to placebo or no treatment (Bolouri 2009; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spinillo 1997). Four studies compared oral drug treatment with topical drug treatment (Fan 2015; Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000), and one compared two types of oral drugs (Lopez‐Olmos 2000), but none compared different topical agents. Two studies compared different oral doses of the same agent (Sobel 1986; Spacek 2005), and one compared different oral treatment durations (Spacek 2005). One study compared two different dosing regimens of the same topical agent (Fong 1994). Two studies compared partner treatments with placebo or no treatment (Fong 1992b; Sobel 1985a), and two studies compared non‐drug treatments (DermaSilk briefs) with other treatments (cotton briefs) (D'Antuono 2012; D'Antuono 2013). One study compared adenosine triphosphate (ATP)‐infrared bio‐effect treatment and a nursing intervention with usual care (Li 2018). CAM treatments were compared with placebo in one study (Metts 2003), and with drug treatments in three studies (Chopra 2013; Kumari 2011; Witt 2009). Another study compared CAM treatments (HPT with an aqueous Candida albicans extract to an antifungal treatment (local + digestive), then a low‐sugar diet with vitamins, biotin and lyophilized bacillus subfilis supplements (Corthay 1988). One study compared vaccination therapy with drug treatment and alternative medicine (Mendling 2011).
Fifteen studies had an intervention duration of six months (Bolouri 2009; D'Antuono 2012; D'Antuono 2013; Fardyazar 2007; Fong 1992a; Fong 1994; Kumari 2011; Li 2018; Lopez‐Olmos 2000; Metts 2003; Roth 1990; Sobel 1989; Sobel 2004; Spinillo 1997; Witt 2009). One study had an intervention duration of three months (Corthay 1988). The three arms in Sobel 1986 had variable but similar lengths (6 menstrual cycles, 5 months, 6 months). One study had a 24‐month intervention period (Chopra 2013). The two partner treatment studies had shorter durations: Fong 1992b only treated participants once (for a five‐day course), and Sobel 1985a treated partners for one week. The duration of the interventions varied in Mendling 2011. Spacek 2005 randomised participants to one or three days of treatment.
Outcome measurement
Fifteen studies continued outcome measurement beyond the intervention period as per their study protocols (additional ~6 months ‐ Bolouri 2009; Corthay 1988; Chopra 2013; Fan 2015; Fardyazar 2007; Fong 1992a; Kumari 2011; Lopez‐Olmos 2000; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spacek 2005; Spinillo 1997; Witt 2009; two studies additional ~12 months ‐ Fong 1992b; Sobel 1985a; one study was variable due to the variable length of the interventions ‐ Mendling 2011). Eleven studies stated that they assessed participants between planned visits if they developed symptoms in the intervening period (Chopra 2013; Fan 2015; Fong 1992b; Mendling 2011; Metts 2003; Roth 1990; Sobel 1985a; Sobel 1986; Sobel 1989; Spinillo 1997; Witt 2009).
Reporting of primary outcomes
All included studies, except three studies (Corthay 1988; D'Antuono 2013; Li 2018), provided information for one of our primary outcomes. Only one study presented data for number of clinical recurrences per participant per year (Mendling 2011). Eighteen studies reported the proportion of women with clinical recurrence (Bolouri 2009; Chopra 2013; D'Antuono 2012; D'Antuono 2013; Fardyazar 2007; Fong 1992a; Fong 1992b; Kumari 2011; Lopez‐Olmos 2000; Metts 2003; Roth 1990; Sobel 1985a; Sobel 1986; Sobel 1989; Sobel 2004; Spacek 2005; Spinillo 1997; Witt 2009), but in three studies the data for this outcome were not presented in a way that allowed for data extraction (D'Antuono 2013; Fong 1994; Metts 2003; Witt 2009). Sixteen studies reported adverse events (Bolouri 2009; Chopra 2013; D'Antuono 2012; Fan 2015; Fardyazar 2007; Fong 1992a; Fong 1992b; Kumari 2011; Mendling 2011; Metts 2003; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spacek 2005; Witt 2009).
Reporting of secondary outcomes
Two studies reported data for time to first recurrence (Sobel 1986; Sobel 2004). No studies reported on number of symptomatic days per year or number of mycological recurrences per participant per year. Eight studies reported data for proportion of participants with at least one mycological recurrence during the treatment and follow‐up period (Bolouri 2009; Fong 1992a; Kumari 2011; Roth 1990; Sobel 1985a; Sobel 1986; Sobel 2004; Spinillo 1997). No studies reported on duration of symptoms after treatment initiation. Four studies reported data for patient preference (Fardyazar 2007; Fong 1994; Mendling 2011; Sobel 1985a).
See the Characteristics of included studies tables for more information on setting, participants, interventions, and outcomes of specific studies.
Excluded studies
After review of full text we excluded 23 studies that on face value appeared to have been eligible for inclusion (Avijgan 2012; Azima 2018; Bartz 2000; Brand 2018; Bushell 1988a; Bushell 1998b; Coric 2006; Davidson 1978; Diba 2010; Donders 2008; Edwards 2018; Fan 2005; Golero 1993; Hilton 1992; Houang 1989; Miller 1984; Rashid 1991; Shalev 1996; Silverman 1971; Sobel 1994; Sobel 2001; Vladareanu 2018; Yang 2000). The reasons excluding these studies are outlined in the Characteristics of excluded studies tables. The most common reason for exclusion was that the case definition of RVVC as reported in our protocol was not met (e.g. a case definition of only three episodes, rather than four episodes, of candidiasis in the past 12 months was used) (Avijgan 2012; Bartz 2000; Brand 2018; Bushell 1988a; Davidson 1978; Edwards 2018; Golero 1993; Silverman 1971; Sobel 1994; Sobel 2001; Yang 2000).
Risk of bias in included studies
Summaries of the 'Risk of bias' assessments for each study are outlined in Figure 2 and Figure 3.
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Random sequence generation
We assessed seven studies that used computer‐generated or other adequate random number sequence processes as at low risk of bias (Chopra 2013; Fong 1992a; Fong 1994; Kumari 2011; Metts 2003; Spinillo 1997; Witt 2009). Two studies were judged to be of high risk of bias for this domain. Li 2018 did not describe the sequence generation and method of randomisation. Fan 2015 was also classified as at high risk of bias for random sequence generation as women with RVVC known to be caused by C glabrata at admission (before Candida culture and identification) were not randomised but were enrolled in the nystatin treatment group. We assessed the remaining studies as at unclear risk of bias as the randomisation method was unclear (often claimed to be a randomised study but no description was provided to enable assessment of risk of selection bias).
Allocation concealment
We assessed four studies that used sealed bags or opaque envelopes as low risk of bias for allocation concealment (D'Antuono 2012; D'Antuono 2013; Fong 1992a; Metts 2003). We assessed six studies to be at high risk of bias for this domain (Fan 2015; Fong 1992b; Li 2018Lopez‐Olmos 2000; Mendling 2011; Sobel 1985a). Lopez‐Olmos 2000 allocated treatment by day of the week, which implies lack of proper concealment and therefore a high risk of bias for this domain. There was no clear description of concealment in the remaining studies, which were therefore assessed as at unclear risk of selection bias (Bolouri 2009; Chopra 2013; Corthay 1988; Fardyazar 2007; Fong 1994; Kumari 2011; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spacek 2005; Spinillo 1997; Witt 2009).
Blinding
Performance bias
We assessed blinding against the primary outcomes, which all involved a component of patient reporting/symptoms. We initially considered only two studies as low risk of performance bias for the primary outcomes (Metts 2003; Roth 1990), as both were blinded to both participants and investigators. It was initially unclear if the studies by D'Antuono were adequately blinded (D'Antuono 2012; D'Antuono 2013), but author correspondence reassured us about the difficulty distinguishing between the different underwear fabrics, therefore we rated these studies as at low risk of bias for this domain. Five studies were assessed as having unclear risk of bias; two studies lacked clarity about whether the placebo was identical to the intervention (Bolouri 2009; Sobel 1986), one study did not refer to blinding (Corthay 1988) and the remaining two studies reported blinding but lacked clarity about whether it was participants, clinicians, or laboratory staff being blinded (Sobel 1989; Sobel 2004).
We assessed 14 studies as at high risk of bias for this domain (Chopra 2013; Fan 2015; Fardyazar 2007; Fong 1992a; Fong 1992b; Fong 1994; Kumari 2011; Li 2018; Lopez‐Olmos 2000; Mendling 2011; Sobel 1985a; Spacek 2005; Spinillo 1997; Witt 2009), due predominantly to lack of masking between the intervention and control groups. The three comparators used by Mendling 2011 were quite different, being ultraviolet A and B rays, vaginal pessaries, and intramuscular injections, and were therefore easy to distinguish.
Detection bias
We considered the risk of detection bias to be low in only one study (Roth 1990). Blinding of outcome assessment was unclear for sixteen of the studies (Bolouri 2009; Chopra 2013; Corthay 1988; D'Antuono 2012; D'Antuono 2013; Fan 2015; Fardyazar 2007; Fong 1992b; Fong 1994; Kumari 2011; Li 2018; Lopez‐Olmos 2000; Metts 2003; Sobel 1986; Sobel 1989; Sobel 2004; Spacek 2005). We assessed the risk of detection bias to be high for five studies, usually because outcomes were assessed by participants who were not blinded and the outcome was "soft" (Fong 1992b; Mendling 2011; Sobel 1985a; Spinillo 1997; Witt 2009).
Incomplete outcome data
We assessed eight studies with low attrition rates (15% or less) as well as good explanations for any loss to follow‐up as at low risk of attrition bias (Chopra 2013; D'Antuono 2012; D'Antuono 2013; Fardyazar 2007; Fong 1992a; Fong 1992b; Fong 1994; Roth 1990). Sobel 2004 reported only the per‐protocol analysis but claimed that the results were similar in a modified intention‐to‐treat‐analysis for which the data were not shown, therefore we assessed the risk of attrition bias for this study to be unclear. Other studies that were deemed to have unclear risk of bias for this domain were two studies that described per‐protocol analysis rather than intention‐to‐treat (Lopez‐Olmos 2000; Spinillo 1997), and two studies where withdrawal and loss to follow‐up were not clearly described (Spacek 2005; Sobel 1985a). We considered 10 studies as at high risk of attrition bias due to high attrition rates or incomplete explanations for this, or both (Bolouri 2009; Corthay 1988; Fan 2015; Kumari 2011; Li 2018; Mendling 2011; Metts 2003; Sobel 1986; Sobel 1989; Witt 2009).
Selective reporting
No published protocol was available for any of the studies. We considered all but two studies as at unclear risk of reporting bias as there was insufficient information in the available publications to assess whether all intended outcomes had been reported. We assessed Kumari 2011 as at high risk for selective reporting because outcome measures were not described in sufficient detail. Sobel 2004 was also considered high risk of bias for this domain, as one of the primary outcome (number of clinical recurrences per participant per year) was not reported.
Other potential sources of bias
We considered four studies to a lowrisk of other bias, as the studies and their authors appeared to be independent of pharmaceutical financial support (Bolouri 2009; Fan 2015; Metts 2003; Spacek 2005). Three studies were funded by companies with vested interests such as pharmaceutical manufacturers and were therefore assessed as at high risk of bias (Fardyazar 2007; Sobel 2004; Witt 2009). Furthermore, in Fardyazar 2007 non‐compliant participants were excluded from the analysis. In Sobel 2004, the authors report that "about halfway through the enrolment period (before the data were analysed), the sponsor decided to combine the parallel trials into a single trial". The third study judged to be at high risk of bias did not provide details about similarity between treatment groups at baseline (Witt 2009). One study was considered at high risk of bias as a conference paper abstract only was located, with no full publication identified Corthay 1988. We considered the remaining 14 studies as at unclear risk of bias as the role of the founder was not clear or the funding source was not reported (Chopra 2013; D'Antuono 2012; D'Antuono 2013; Fong 1992a; Fong 1992b; Fong 1994; Kumari 2011; Lopez‐Olmos 2000; Mendling 2011; Roth 1990; Sobel 1985a; Sobel 1986; Sobel 1989; Spinillo 1997).
Effects of interventions
Summary of findings 1. Drug treatment compared to placebo or no treatment for recurrent vulvovaginal candidiasis.
| Drug treatment compared to placebo/no treatment (excluding partner treatment) for recurrent vulvovaginal candidiasis (thrush) | ||||||
| Patient or population: non‐pregnant women with a diagnosis of recurrent vulvovaginal candidiasis Setting: outpatients Intervention: antifungals (fluconazole, clotrimazole, ketoconazole, itraconazole) Comparison: placebo or no treatment (excluding partner treatment) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo/no treatment (excluding partner treatment) | Risk with drug treatment | |||||
| Primary outcome 1: Number of clinical recurrences per participant per year | ‐ | ‐ | (0 studies) | ‐ | Not reported | |
| Primary outcome 2: Clinical recurrence at 6 months | Study population | RR 0.36 (0.21 to 0.63) | 607 (6 RCTs) | ⊕⊕⊝⊝ LOW 1 | ||
| 647 per 1000 | 233 per 1000 (136 to 408) | |||||
| Primary outcome 2: Clinical recurrence at 12 months | Study population | RR 0.80 (0.72 to 0.89) | 585 (6 RCTs) | ⊕⊕⊝⊝ LOW 1 | ||
| 781 per 1000 | 625 per 1000 (562 to 695) | |||||
| Primary outcome 3: Adverse events | ‐ | Not estimable | (5 RCTs) | ⊕⊝⊝⊝ VERY LOW 2 3 | Pooling of the incidence of adverse events was not possible as the outcome was reported differently across the included trials. Overall the adverse event rate was low for both placebo and treatment arms. Sobel 2004 reported that 2.9% of participants dropped out due to adverse events in the fluconazole group and 1.2% in the placebo group. 2 participants dropped out in Sobel 1986. No participants dropped out in Bolouri 2009. Less than 5% reported adverse effects in Sobel 1989, and no side effects or complications occurred in Roth 1990. | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded two levels due to very serious risk of bias for blinding or participants and assessors (Spinillo 1997), incomplete outcome data (Bolouri 2009; Sobel 1986; Sobel 1989), and pharmaceutical funding (Sobel 2004). 2Downgraded two levels due to very serious risk of bias for incomplete outcome data, Bolouri 2009; Sobel 1986; Sobel 1989, and pharmaceutical funding, Sobel 2004. 3Downgraded one level due to imprecision (we were not able to pool the data).
Summary of findings 2. Oral drug treatment compared to topical drug treatment for recurrent vulvovaginal candidiasis.
| Oral drug treatment compared to topical drug treatment for recurrent vulvovaginal candidiasis | ||||||
| Patient or population: non‐pregnant women with a diagnosis of recurrent vulvovaginal candidiasis Setting: outpatients Intervention: oral drug treatment (fluconazole, itraconazole) Comparison: topical drug treatment (nystatin, clotrimazole) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with topical drug treatment | Risk with oral drug treatment | |||||
| Primary outcome 1: Number of clinical recurrences per participant per year | ‐ | ‐ | (0 studies) | ‐ | Not reported | |
| Primary outcome 2: Clinical recurrence at 6 months | Study population | RR 1.66 (0.83 to 3.31) | 206 (3 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 | ||
| 118 per 1000 | 196 per 1000 (98 to 392) | |||||
| Primary outcome 2: Clinical recurrence at 12 months | Study population | RR 0.95 (0.71 to 1.27) | 206 (3 RCTs) | ⊕⊝⊝⊝ VERY LOW 1 2 3 | ||
| 495 per 1000 | 470 per 1000 (351 to 628) | |||||
| Primary outcome 3: Adverse events | ‐ | Not estimable | (3 RCTs) | ⊕⊝⊝⊝ VERY LOW 4 5 | Due to heterogeneity in reporting we were not able to pool the data. | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded two levels due to very serious risk of bias (allocation concealment (Lopez‐Olmos 2000), blinding of participants (Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000), blinding of assessment (Fong 1992a), and pharmaceutical funding (Fardyazar 2007)). 2Downgraded one level due to imprecision (wide confidence interval). 3Downgraded one level due to inconsistency (some studies showed superior effects for oral treatment, whereas others showed superior effects for topical treatment). 4Downgraded two levels due to very serious risk of bias (selection bias (Fan 2015), blinding of participants (Fan 2015; Fardyazar 2007; Fong 1992a), blinding of assessment (Fong 1992a), incomplete outcome data (Fan 2015), and pharmaceutical funding (Fardyazar 2007)). 5Downgraded one level due to imprecision (we were not able to pool data).
This section presents the available data from the included studies only. Two 'Summary of findings' tables collate the main results of this review (Table 1; Table 2).
Comparison 1: Drug treatment versus placebo/no treatment (excluding partner treatment)
See Table 1.
Six studies examined drug treatment versus placebo/no treatment (excluding partner treatment) (Bolouri 2009; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spinillo 1997). Spinillo 1997 used a no‐treatment comparator, whilst the remaining five studies used a placebo comparator. All studies presenting data for this comparison involved treatment with azoles, therefore a single analysis, grouped into two categories (oral and topical treatments), was performed for each relevant outcome. The characteristics of studies against this comparison are summarised in a supplementary table (Table 3).
1. Summary of characteristics of studies included in Comparison 1: Drug treatment versus placebo/no treatment (excluding partner treatment).
| Study ID | Bolouri 2009 | Roth 1990 | Sobel 1986 | Sobel 1989 | Sobel 2004 | Spinillo 1997 |
| Participants (n) | 97 | 64 | 74 | 42 | 387 | 114 |
| Candida albicansat enrolment (%) | 78 | 100a | 87 | 86 | 94 | 100a |
| Mean episodes in previous 12 months | NSb | 6.2 (clotrimazole), 6.5 (placebo) | NSb | 9.2 (clotrimazole), 8.3 (placebo) | NSb | NSb |
| Withdrawals/loss to follow‐up (%) | 34 | 3 | 15 | 36 | 4 | 7 |
| Setting | Hospital outpatient clinic | NSb | NSb | NSb | Multicentre | Outpatient clinic |
| Country | Iran | Sweden | USA | USA | USA | Italy |
| Intervention 1 | Fluconazole (weekly) | Clotrimazole (postmenstrual)* | Ketoconazole (with menses) | Clotrimazole (postmenstrual)* | Fluconazole (weekly) | Itraconazole (with menses) |
| Intervention 2 | Placebo (weekly) | Placebo (postmenstrual)* | Ketoconazole (daily) | Placebo (postmenstrual)* | Placebo (weekly) | No treatment (with menses) |
| Intervention 3 | ‐ | ‐ | Placebo (daily) | ‐ | ‐ | ‐ |
| Duration of intervention | 6 months | 6 months | 6 months | 6 months | 6 months | 6 months |
| Duration of observation after intervention | 6 months | 6 months | 6 months | 6 months | 6 months | 6 months |
| Planned assessments | Monthly for 6 months, then 9 months, 12 months | Monthly for 6 months, then 9 months, 12 months | Monthly for 12 months | Monthly for 6 months, then 9 months, 12 months | Monthly for 6 months, then 9 months, 12 months | 3, 6, and 12 months |
| Assessment between planned visits if symptoms developed | ‐ | Yes | Yes | Yes | ‐ | Yes |
aC albicans was a selection criterion. bNot reported or unclear.
*Topical treatment
Primary outcomes
1. Number of clinical recurrences per participant per year
None of the six studies in this comparison reported this outcome (Bolouri 2009; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spinillo 1997).
2. Proportion of participants with at least one clinical recurrence during the treatment and follow‐up period
Data were available for this outcome from all six studies at both six and 12 months for 607 and 585 participants, respectively. Each study had an active treatment phase of six months and a further period of six months of surveillance after the active treatment had been completed, therefore clinical recurrence at six months represented recurrence whilst on treatment and at 12 months included a six‐month period where participants were not on active treatment.
Clinical recurrence at 6 months
Oral treatments
When results were pooled for oral treatments (fluconazole, itraconazole, ketoconazole ‐ Bolouri 2009; Sobel 1986; Sobel 2004; Spinillo 1997), oral treatments may reduce clinical recurrence at six months (risk ratio (RR) 0.29, 95% confidence interval (CI) 0.14 to 0.62; participants = 518; studies = 4; I2= 84%; low certainty evidence; Analysis 1.1, Figure 4). The incidence of recurrence in the treatment group was 17% (46/270) compared to 63% (156/248) in the placebo/no treatment group. The number needed to treat to prevent one participant having one or more clinical recurrence at six months was two (number needed to treat for an additional beneficial outcome (NNTB) = 2). Given the I2 of 84%, we applied a random‐effects model. However, our confidence in these findings is low.
1.1. Analysis.

Comparison 1: Drug treatment versus placebo/no treatment (excluding partner treatment) (Comparison 1), Outcome 1: Clinical recurrence at 6 months
4.

Forest plot of comparison: 1 Drug treatment versus placebo/no treatment (excluding partner treatment) (Comparison 1), outcome: 1.1 Clinical recurrence at 6 months.
We downgraded the certainty of the evidence by two levels to low due to very serious risk of bias in several studies (high risk of bias for blinding of participants and assessors (Spinillo 1997), incomplete outcome data (Bolouri 2009; Sobel 1986), and pharmaceutical funding (Sobel 2004)).
Regarding the sensitivity of this finding to heterogeneity, removing Spinillo 1997 (the only study without a placebo) from the analysis reduced the I2 to 51%, with no impact on direction of effect and no meaningful change to the magnitude of effect (RR 0.22, 95% CI 0.12 to 0.39). When we regarded missing data as treatment failures, the findings remained similar but the magnitude of the potential reduction was reduced (RR 0.52, 95% CI 0.41 to 0.66; random‐effects; I2= 47%; NNTB = 3). When pooling the two studies involving fluconazole (Bolouri 2009; Sobel 2004), the incidence of clinical recurrence in the treatment groups was 11% (19/173) compared to 61% (107/174) for placebo (RR 0.22, 95% CI 0.09 to 0.57; participants = 347; random‐effects; I2 = 75%; Analysis 1.1). The number needed to treat to prevent one participant having one or more clinical recurrence at six months was two (NNTB = 2). When we regarded missing data as treatment failures, the findings were similar but the magnitude of the potential reduction was reduced (RR 0.54, 95% CI 0.37 to 0.80; random‐effects; I2 = 71%; NNTB = 3).
We downgraded the certainty of the evidence by two levels to low due to very serious risk of bias (incomplete outcome data in Bolouri 2009 and pharmaceutical funding in Sobel 2004).
Topical treatments
Of the two trials using a topical agent (clotrimazole), one reported a reduction in clinical recurrence at six months (Roth 1990), but the other did not (Sobel 1989). When pooling these two studies topical treatment with clotrimazole may have little to no effect on clinical recurrence at six months, but the evidence is very uncertain (RR 0.55, 95% CI 0.26 to 1.14; participants = 89; studies = 2; I2 = 68%; random‐effects; very low certainty evidence; Analysis 1.1). The clotrimazole group had a recurrence rate of 38% (18/48) compared to 76% (31/41) in the placebo group. However, our confidence in these findings is very low.
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias (incomplete outcome data in Sobel 1989) and imprecision (data came from only two studies).
Oral and topical treatments combined
When all drug treatments versus placebo/no treatment were considered, the pooled analysis showed that clinical recurrence at six months may be reduced with oral/topical treatments compared with placebo (RR 0.36, 95% CI 0.21 to 0.63; participants = 607; studies = 6; I2 = 82%; random‐effects; NNTB = 2; low certainty evidence; Analysis 1.1). The incidence in the treatment group was 20% (64/318) compared to 65% (187/289) in the placebo group. However, our confidence in these findings is low.
We performed a sensitivity analysis to assess the impact of heterogeneity on the pooled result by removing Sobel 2004 from the pooled analysis. This reduced the I2 to 51% with no impact on the direction of effect and no meaningful change to the magnitude of effect (RR 0.45, 95% CI 0.31 to 0.66). The number needed to treat to prevent one participant having one or more clinical recurrence at six months was two participants. When regarding the missing data as treatment failures, the findings remained similar (RR 0.54, 95% CI 0.43 to 0.69; I2 = 61%; random‐effects; NNTB = 3).
We downgraded the certainty of the evidence by two levels to low due to very serious risk of bias in several studies (blinding of participants and assessors (Spinillo 1997), incomplete outcome data (Bolouri 2009; Sobel 1986; Sobel 1989), and pharmaceutical funding (Sobel 2004)) and heterogeneity.
Clinical recurrence at 12 months
Oral treatments
Four trials assessed the recurrence at 12 months with oral active drugs (Bolouri 2009; Sobel 1986; Sobel 2004; Spinillo 1997). When results were pooled, the analysis showed that oral treatments may reduce clinical recurrence at 12 months (RR 0.77, 95% CI 0.68 to 0.88; participants = 496; studies = 4; I2 = 0%, fixed‐effect; low certainty evidence; Analysis 1.2, Figure 5). This suggests that there may be a persistence of an effect of the drug beyond the six‐month treatment period. The number needed to treat to prevent one participant having one or more clinical recurrence at 12 months was 5.6 (NNTB = 6). When regarding the missing data as treatment failures, the findings remained similar (RR 0.86, 95% CI 0.79 to 0.93; fixed‐effect; I2 = 0%; NNTB = 8). However, our confidence in these findings is low.
1.2. Analysis.

Comparison 1: Drug treatment versus placebo/no treatment (excluding partner treatment) (Comparison 1), Outcome 2: Clinical recurrence at 12 months (6 months active, 6 months observation)
5.

Forest plot of comparison: 1 Drug treatment versus placebo/no treatment (excluding partner treatment) (Comparison 1), outcome: 1.2 Clinical recurrence at 12 months (6 months active, 6 months observation).
We downgraded the certainty of the evidence by two levels to low due to very serious risk of bias (blinding of participants and assessors (Spinillo 1997), incomplete outcome data (Bolouri 2009; Sobel 1986), and pharmaceutical funding (Sobel 2004)).
For studies examining fluconazole (Bolouri 2009; Sobel 2004), when pooled, results show that fluconazole may reduce clinical recurrence at 12 months (RR 0.76, 95% CI 0.66 to 0.89; participants = 327; studies = 2; I2 = 26%; fixed‐effect; low certainty evidence). The number needed to treat to prevent one participant having one or more clinical recurrence at 12 months was 6. When regarding the missing data as treatment failures, the findings remained in the same (RR 0.87, 95% CI 0.79 to 0.95; fixed‐effect; I2 = 0%; NNTB = 9). However, our confidence in these findings is low.
We downgraded the certainty of the evidence by two levels to low due to very serious risk of bias (incomplete outcome data in Bolouri 2009 and pharmaceutical funding in Sobel 2004).
Topical treatments
Two studies assessed topical treatment (Sobel 1989 ; Roth 1990). When they were pooled the results show that topical treatment with clotrimazole may have effect to no effect on clinical recurrence at 12 months (RR 0.93, 95% CI 0.77 to 1.13; participants = 89; studies = 2; I2 = 0%; fixed‐effect; very low certainty evidence; Analysis 1.2). However, our confidence in these findings is very low.
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias (incomplete outcome data in Sobel 1989) and imprecision (data came from only two studies).
Oral and topical treatments combined
When topical and oral treatment studies are considered together results show oral/topical treatments may reduce clinical recurrence at 12 months (RR 0.80, 95% CI 0.72 to 0.89; participants = 585; studies = 6; I2 = 21%, fixed‐effect; NNTB = 6; low certainty evidence; Analysis 1.2). The incidence was 62% (188/302) in the treatment group compared to 78% (221/283) in the placebo/no treatment group. The number needed to treat to prevent one participant having one or more clinical recurrence at 12 months was 6 (NNTB = 6). When regarding the missing data as treatment failures the findings remained similar (RR 0.87, 95% CI 0.80 to 0.93; fixed‐effect; I2 = 0%; NNTB = 8.5). However, our confidence in these findings is low.
We downgraded the certainty of the evidence by two levels to low due to very serious risk of bias in several studies (blinding of participants and assessors (Spinillo 1997), incomplete outcome data (Bolouri 2009; Sobel 1986; Sobel 1989), and pharmaceutical funding (Sobel 2004)).
3. Adverse events
Of the six studies reporting this comparison (Bolouri 2009; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spinillo 1997), only Spinillo 1997 did not present any information regarding adverse events. Overall, the adverse event rate was low for both placebo and treatment arms in these trials. It was not possible to pool data for this outcome due to the variability in the way the outcome was reported. We downgraded the certainty of the evidence for this outcome (adverse events) by three levels to very low due to very serious risk of bias in multiple domains for the included studies, in particular relating to selective reporting and incomplete outcome data, and imprecision (we were not able to pool results).
Regarding clotrimazole, no cessation of therapy occurred due to adverse effects (Roth 1990; Sobel 1989). More specifically, in Roth 1990 no side effects or complications resulted from prophylactic treatment with either clotrimazole vaginal tablets or placebo vaginal tablets were reported. Regarding fluconazole, Sobel 2004 reported adverse reactions resulting in discontinuation as 2.9% in the fluconazole group and 1.2% in the placebo group, whilst no cessation of therapy occurred due to side effects in the other study of this drug (Bolouri 2009). In Sobel 2004 the main reported adverse events were: abdominal pain (22), nausea/vomiting (17), diarrhoea (15), flatulence (4), headache/migraine (56), central nervous system disorder (27), musculoskeletal disorder (29), rash (12), allergic reaction (9), menstrual disorder (3), alopecia (1). In the study of itraconazole (Sobel 1986), two women dropped out due to adverse events (1 due to a rash and 1 due to nausea); however, it was not stated if these dropouts occurred in the treatment or placebo group. Sobel 1986 reports the following adverse effects: mild to moderate nausea (7/63), headache (2/63), mild transient rise in serum aspartate aminotransferase level (3/63).
Secondary outcomes
1. Time to first recurrence
Two studies reported time to first recurrence for this comparison (Sobel 1986; Sobel 2004). In the Sobel 1986 study, which examined the effect of ketoconazole versus placebo, the mean time to first recurrence in the perimenstrual treatment group was 3.6 months compared to 1.8 months for the placebo group. No data were presented for the mean time to recurrence in the continuous treatment group. In Sobel 2004, fluconazole also increased the time to first recurrence (P < 0.001): the median time to first recurrence was 4.0 months in the placebo group compared to 10.2 months in the fluconazole group. Data for this outcome were limited and could not be pooled in a meta‐analysis. We downgraded the certainty of the evidence for this outcome by two levels to very low due to very serious risk of bias (incomplete outcome data in Sobel 1986 and pharmaceutical funding in Sobel 2004) and imprecision.
2. Number of symptomatic days per year
None of the six studies in this comparison reported this outcome (Bolouri 2009; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spinillo 1997).
3. Number of mycological recurrences per participant per year
None of the six studies in this comparison reported this outcome (Bolouri 2009; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spinillo 1997).
4. Proportion of participants with at least one mycological recurrence during the treatment and follow‐up period
Mycological recurrence at 6 months
Oral treatments
At six months, all four trials comparing oral treatments to placebo/no treatment drugs demonstrated a reduction in mycological recurrence (Bolouri 2009; Sobel 1986; Sobel 2004; Spinillo 1997). When pooled, the two studies of fluconazole showed fluconazole may reduce mycological recurrence at 6 months (Bolouri 2009; Sobel 2004) (RR 0.27, 95% CI 0.20 to 0.38; two studies, participants = 335; I2 = 35%; fixed‐effect; NNTB = 2; low certainty evidence). The incidence was 19% (33/172) in the treatment group compared to 70% (114/163) in the placebo group. However, our confidence in these findings is low.
When results were pooled for all oral treatments (fluconazole, itraconazole, ketoconazole), results show that oral treatments may reduce microbiological recurrence at 6 months (RR 0.37, 95% CI 0.22 to 0.63; participants = 506; studies = 4; I2 = 78%; random‐effects; low certainty evidence; Analysis 1.3 ). However, our confidence in these findings is low. There was an incidence of 38% (65/269) in the treatment group compared to 69% (164/237) in the placebo/no treatment group. We performed a sensitivity analysis to assess the impact of heterogeneity on the pooled result by removing Spinillo 1997, the only study with a no treatment control rather than a placebo. This reduced the I2 to 0% with no impact on the direction of effect and no meaningful change to the magnitude of effect (RR 0.40, 95% CI 0.18 to 0.88; heterogeneity: Tau2 = 0.00; Chi2 = 1.57, df = 2 (P = 0.46); I2 = 0%).
1.3. Analysis.

Comparison 1: Drug treatment versus placebo/no treatment (excluding partner treatment) (Comparison 1), Outcome 3: Mycological recurrence at 6 months
We downgraded the certainty of the evidence by two levels to low due to very serious risk of bias (blinding of participants and assessors (Spinillo 1997), incomplete outcome data (Bolouri 2009; Sobel 1986), and pharmaceutical funding (Sobel 2004)).
Topical treatments
Of the two studies examining clotrimazole versus placebo, only Roth 1990 presented information for this outcome. In this publication, the difference between the treatment and placebo arms for mycological recurrence was not significant at six months. We downgraded the certainty of the evidence by two levels to low due to serious risk of bias (unclear reporting of randomisation and allocation concealment) and imprecision (data came from only one study).
Oral and topical treatments combined
Five studies presented findings for this outcome at six months (Bolouri 2009; Roth 1990; Sobel 1986; Sobel 2004; Spinillo 1997). When all drug treatments versus placebo/no treatment were considered, the pooled analysis demonstrated that oral/topical treatments may reduce mycological recurrence at 6 months. There was an incidence of 29% (88/302) in the treatment group compared to 71% (189/266) in the placebo/no treatment group (RR 0.44, 95% CI 0.25 to 0.78; participants = 568; studies = 5; I2 = 89%; random‐effects; NNTB = 3; low certainty evidence; Analysis 1.3). However, our confidence in these findings is low.
We downgraded the certainty of the evidence by two levels to low due to very serious risk of bias (blinding of participants and assessors (Spinillo 1997), incomplete outcome data (Bolouri 2009; Sobel 1986), and pharmaceutical funding (Sobel 2004)).
Mycological recurrence at 12 months
Oral treatments
Two trials with oral active drugs presented findings for this outcome at 12 months (6 months active treatment, 6‐month surveillance period) (Bolouri 2009; Sobel 1986). When the results were pooled oral treatments may have no effect on mycological recurrence at 12 months (RR 0.86, 95% CI 0.71 to 1.04; participants = 127; studies = 2; I2 = 0%; fixed‐effect; very low certainty evidence; Analysis 1.4). The incidence of mycological recurrence was 69% (51/74) in the treatment group compared to 83% (44/53) in the placebo group. However, our confidence in these findings is very low.
1.4. Analysis.

Comparison 1: Drug treatment versus placebo/no treatment (excluding partner treatment) (Comparison 1), Outcome 4: Mycological recurrence at 12 months
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias (incomplete outcome data (Bolouri 2009; Sobel 1986)) and imprecision (based on only two studies).
Topical treatments
Of the two studies examining clotrimazole versus placebo, only Roth 1990 presented information for this outcome. In this publication, the difference between the treatment and placebo arms for mycological recurrence was not significant at 12 months. We downgraded the certainty of the evidence by two levels to low due to serious risk of bias (unclear reporting of randomisation and allocation concealment) and imprecision (data came from only one study).
Oral and topical treatments combined
Only three studies presented data for this outcome at 12 months (Bolouri 2009; Roth 1990; Sobel 1986). When pooled oral/topical treatments may not have an effect on mycological recurrence at 12 months (RR 0.90, 95% CI 0.79 to 1.03; participants = 189; studies = 3; I2 = 0%; fixed‐effect; low certainty evidence; Analysis 1.4). However, our confidence in these findings is low.
We downgraded the certainty of the evidence by two levels to low due to very serious risk of bias (incomplete outcome data (Bolouri 2009; Sobel 1986)).
5. Duration of symptoms after treatment initiation
None of the six studies in this comparison reported this outcome (Bolouri 2009; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spinillo 1997).
6. Patient preference
None of the six studies in this comparison reported this outcome (Bolouri 2009; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spinillo 1997).
Comparison 2: Oral drug treatment versus topical drug treatment
See Table 2.
Four studies examined oral drug treatment versus topical drug treatment (Fan 2015; Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000). Fan 2015 compared oral fluconazole to nystatin. Fardyazar 2007 compared oral fluconazole to clotrimazole. Fong 1992a compared oral itraconazole to topical clotrimazole, and Lopez‐Olmos 2000 compared oral fluconazole (19 participants) to both oral itraconazole (14 participants) and topical clotrimazole (12 participants). Each of these studies had a six‐month active‐treatment phase followed by a further six months of surveillance. The characteristics of studies against this comparison are summarised in a supplementary table (Table 4).
2. Summary of characteristics of studies included in Comparison 2: Oral drug treatment versus topical drug treatment.
| Study ID | Fan 2015 | Fardyazar 2007 | Fong 1992a | Lopez‐Olmos 2000 |
| Participants (n) | 330 | 124 | 44 | 45 |
| Candida albicansat enrolment (%) | 77.5 | ‐ | 98 | 27a |
| Mean episodes in previous 12 months | NSb | NSb | 8.8 (itraconazole), 9.7 (clotrimazole) | NSb |
| Withdrawals/loss to follow‐up (%) | 11 | 6 | 14 | 8 |
| Setting | Outpatient clinic | Outpatient clinic | Hospital outpatient clinic | Multicentre ‐ a gynaecology outpatient clinic and a family planning clinic |
| Country | China | Iran | Canada | Spain |
| Intervention 1 | Fluconazole (weekly) | Fluconazole (weekly) | Itraconazole (twice weekly) | Fluconazole (with menses) |
| Intervention 2 | Nystatin (with menses) | Clotrimazole (twice weekly) | Clotrimazole (twice weekly) | Itraconazole (with menses) |
| Intervention 3 | ‐ | ‐ | ‐ | Clotrimazole (with menses) |
| Duration of intervention | 6 months | 6 months | 6 months | 6 months |
| Duration of observation after intervention | 6 months | 6 months | 6 months | 6 months |
| Planned assessments | Monthly for 6 months and at 9 months and 12 months | Monthly for 12 months | Monthly for 12 months | At 6 months and 12 months |
| Assessment between planned visits if symptoms developed | Yes | ‐ | ‐ | ‐ |
aNot all participants had positive cultures at enrolment; 12 (27%) participants had C albicans and 5 (11%) had C glabrata. bNot reported or unclear.
Primary outcomes
1. Number of clinical recurrences per participant per year
None of the four studies in this comparison reported this outcome (Fan 2015; Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000).
Clinical recurrence at 6 months
At six months when all oral drug treatments versus topical treatment were considered, oral treatments may have little to no effect on clinical recurrence compared with topical treatments, but the evidence is very uncertain(RR 1.66, 95% CI 0.83 to 3.31; participants = 206; studies = 3; I2 = 0%; fixed‐effect; very low certainty evidence; Analysis 2.1, Figure 6). There was an incidence of 21% (24/113) in the oral treatments group compared to 12% (11/93) in the topical treatment group. However, our confidence in these findings is very low.
2.1. Analysis.

Comparison 2: Oral drug treatment versus topical drug treatment (Comparison 2), Outcome 1: Clinical recurrence at 6 months
6.

Forest plot of comparison: 2 Oral drug treatment versus topical drug treatment (Comparison 2), outcome: 2.1 Clinical recurrence at 6 months.
Lopez‐Olmos 2000 had a high risk of selection bias as it appeared to have not used a random allocation method, therefore we conducted a sensitivity analysis of this effect estimate by removing Lopez‐Olmos 2000 from the analysis. This did not alter the direction of effect or the conclusion (RR 1.31, 95% CI 0.63 to 2.75; participants = 161; studies 2; I2 = 0%; fixed‐effect).
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias (allocation concealment (Lopez‐Olmos 2000), blinding of participants (Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000), blinding of assessment (Fong 1992a), and pharmaceutical funding (Fardyazar 2007) and imprecision.
Clinical recurrence at 12 months
At 12 months, when all oral drug treatments versus topical treatment were considered, oral treatments may have little to no effect on clinical recurrence compared with topical treatments, but the evidence is very uncertain (RR 0.95, 95% CI 0.71 to 1.27; participants = 206; studies = 3; I2 = 10%; fixed‐effect; very low certainty evidence; Analysis 2.2, Figure 7). There was an incidence of 47% (53/113) in the oral treatment group compared to 49% (46/93) in the topical treatment group. However, our confidence in these findings is very low.
2.2. Analysis.

Comparison 2: Oral drug treatment versus topical drug treatment (Comparison 2), Outcome 2: Clinical recurrence at 12 months (6 months active, 6 months observation)
7.

Forest plot of comparison: 2 Oral drug treatment versus topical drug treatment (Comparison 2), outcome: 2.2 Clinical recurrence at 12 months (6 months active, 6 months observation).
Lopez‐Olmos 2000 had a high risk of selection bias as it appeared to have not used a random allocation method, therefore we conducted a sensitivity analysis of this effect estimate by removing Lopez‐Olmos 2000 from the analysis. This did not alter the direction of effect or the conclusion (RR 0.91, 95% CI 0.66 to 1.25; participants = 161; I2 = 44%; fixed‐effect).
Two studies compared fluconazole to clotrimazole (Fardyazar 2007; Lopez‐Olmos 2000). When pooled, oral fluconazole compared to topical clotrimazole may slightly reduce clinical recurrence, but the evidence is very uncertain at six months (clinical recurrence of 18% in fluconazole group and 8% in clotrimazole group; RR 1.94, 95% CI 0.75 to 5.03; participants = 148; I2 = 57%; fixed‐effect; very low certainty evidence) or at 12 months (clinical recurrence of 48% in fluconazole group and 42% in clotrimazole group; RR 1.12, 95% CI 0.78 to 1.62; participants = 148; I2 = 0%; fixed‐effect; very low certainty evidence).
We downgraded the certainty of the evidence for this outcome by three levels to very low due to very serious risk of bias (allocation concealment (Lopez‐Olmos 2000), blinding of participants (Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000), blinding of assessment (Fong 1992a), and pharmaceutical funding (Fardyazar 2007), inconsistent results, and imprecision.
3. Adverse events
Three studies reported findings for this outcome. In Fan 2015, one woman from the nystatin group switched to the fluconazole group due to aggravated vaginal burning pain, vulvar or edema, and vulvar itching. In the fluconazole group, three women (2%) experienced oligomenorrhoea, and one woman (0.7%) experienced gastrointestinal symptoms (including nausea).
Fardyazar 2007 had no withdrawals due to adverse effects in the fluconazole group (0/58), but 5% of participants (3/59) withdrew due to adverse effects in the clotrimazole group. Fluconazole users reported nausea (20 women) and vomiting (four women) and some mild gastrointestinal effects that were not specified or quantified. In the clotrimazole group, five women experienced local sensitivity (three of whom withdrew from the study). The authors also reported that systemic complications were significantly less in the cream users than in the capsule users, but did not provide any participant numbers to support this claim (Fardyazar 2007).
In Fong 1992a, no withdrawals occurred due to adverse effects in either arm, but adverse effects occurred in 33% (7/21) of the itraconazole group compared to no adverse effects (0/22) in the clotrimazole group at six months. Reported adverse events in the itraconazole group included mild nausea (four women), mild diarrhoea (one woman), headaches (one woman), and transient faintness with dizziness (one woman).
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias (selection bias (Fan 2015), blinding of participants (Fan 2015; Fardyazar 2007; Fong 1992a), blinding of assessment (Fong 1992a), incomplete outcome data (Fan 2015), and pharmaceutical funding (Fardyazar 2007)) and imprecision (we were not able to pool results).
Secondary outcomes
1. Time to first recurrence
None of the four studies in this comparison reported this outcome (Fan 2015; Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000).
2. Number of symptomatic days per year
None of the four studies in this comparison reported this outcome (Fan 2015; Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000).
3. Number of mycological recurrences per participant per year
None of the four studies in this comparison reported this outcome (Fan 2015; Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000).
4. Proportion of participants with at least one mycological recurrence during the treatment and follow‐up period
Only Fong 1992a reported findings for this outcome, with mycological recurrence 50% (11/22) in the itraconazole group compared to 41% (9/22) in the clotrimazole group at six months (RR 1.22, 95% CI 0.64 to 2.35; participants = 44; very low certainty evidence; Analysis 2.3).
2.3. Analysis.

Comparison 2: Oral drug treatment versus topical drug treatment (Comparison 2), Outcome 3: Mycological recurrence at 6 months
We downgraded the certainty of the evidence for this outcome by three levels to very low due to very serious risk of bias and imprecision (based on only one study).
5. Duration of symptoms after treatment initiation
None of the four studies in this comparison reported this outcome (Fan 2015; Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000).
6. Patient preference
Only Fardyazar 2007 reported data for this outcome, finding that participants in the clotrimazole group more commonly missed two or more consecutive doses of the drug (15% (9/59)) than participants in the fluconazole group (7 % (4/58)).
We downgraded the certainty of the evidence for this outcome by four levels to very low due to very serious risk of bias in Fardyazar 2007, indirectness (Fardyazar 2007 used a proxy to measure patient preference), and imprecision (based on only one study).
Comparison 3: Oral drug treatment versus oral drug treatment
One study presented findings relevant to the comparison of oral treatment versus a different oral treatment (Lopez‐Olmos 2000). In this study, fluconazole was administered as a single tablet of 150 mg (19 participants) compared to itraconazole (100 mg, 2 capsules a day; 14 participants). Each regimen was administered on the sixth day of the menstrual cycle over a period of six months.
Primary outcomes
1. Number of clinical recurrences per participant per year
The one study in this comparison did not report this outcome (Lopez‐Olmos 2000).
2. Proportion of participants with at least one clinical recurrence during the treatment and follow‐up period
Lopez‐Olmos 2000 found 47% recurrences in the fluconazole group compared with 14% in the itraconazole group at 6 months (RR 3.32, 95% CI 0.84 to 13.02; participants = 33; studies = 1; very low certainty evidence; Analysis 3.1) and 58% (11/19) in the fluconazole group versus 36% (5/14) in the itraconazole group at 12 months (6 months active treatment, 6 months observation) (RR 1.62, 95% CI 0.73 to 3.61; participants = 33; studies = 1; very low certainty evidence; Analysis 3.2). Our confidence in these findings is very low.
3.1. Analysis.

Comparison 3: Oral drug treatment versus oral drug treatment (Comparison 3), Outcome 1: Clinical recurrence at 6 months
3.2. Analysis.

Comparison 3: Oral drug treatment versus oral drug treatment (Comparison 3), Outcome 2: Clinical recurrence at 12 months
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias and imprecision.
3. Adverse events
The one study in this comparison did not report this outcome (Lopez‐Olmos 2000).
Secondary outcomes
None of the secondary outcomes could be extracted.
Comparison 4: Topical drug treatment versus topical drug treatment
None of the included studies compared an active topical treatment with another active tropical treatment.
Comparison 5: Comparison of different doses of the same agent
Three studies presented findings relevant to this comparison (Fong 1994; Sobel 1986; Spacek 2005). Fong 1994 compared empiric self‐treatment with cyclical monthly prophylactic use of 500 mg clotrimazole vaginal ovules. Sobel 1986 compared 400 mg of daily perimenstrual ketoconazole for six cycles with 100 mg of ketoconazole daily for five months. Spacek 2005 compared a one‐day regimen of 400 mg itraconazole with a three‐day regimen of 600 mg itraconazole. The characteristics of studies against this comparison are summarised in a supplementary table (Table 5).
3. Summary of characteristics of studies included in Comparison 5: Comparison of different doses of the same agent.
| Study ID | Fong 1994 | Sobel 1986 | Spacek 2005 |
| Participants (n) | 23 | 74 | 26 |
| Candida albicans at enrolment (%) | ‐ | 87 | 96 |
| Mean episodes in previous 12 months | 7.5 | NSa | NSa |
| Withdrawals/loss to follow‐up (%) | 0 | 15 | 4 |
| Setting | NS | NSa | Outpatient clinic |
| Country | Canada | USA | Czech Republic |
| Intervention 1 | Clotrimazole (perimenstrually) | Ketoconazole (with menses) | Itraconazole, 400 mg |
| Intervention 2 | Clotrimazole (empirically, with symptoms) | Ketoconazole (daily) | Itraconazole, 600 mg |
| Intervention 3 | ‐ | Placebo (daily) | ‐ |
| Duration of intervention | 6 months | 6 months | 1 to 3 days |
| Duration of observation after intervention | N/A Cross over trial | 6 months | 6 months |
| Planned assessments | Bimonthly for 12 months | Monthly for 12 months | 14 days, 1 month, 3 months, 6 months |
| Assessment between planned visits if symptoms developed | ‐ | Yes | ‐ |
aNot reported or unclear.
Primary outcomes
1. Number of clinical recurrences per participant per year
None of the three studies in this comparison reported this outcome (Fong 1994; Sobel 1986; Spacek 2005).
2. Proportion of participants with at least one clinical recurrence during the treatment and follow‐up period
Due to considerable clinical heterogeneity between the two studies, we decided not to pool the results. After six months 29% of participants in the perimenstrual ketoconazole group compared to 5% in the daily ketoconazole group developed at least one clinical recurrence in the Sobel 1986 study. In the Spacek 2005 study, 62% of participants in the one‐day group and 77% in the three‐day treatment group developed at least one clinical recurrence (see Analysis 4.1). Fong 1994 did not report this outcome.
4.1. Analysis.

Comparison 4: Comparison of different doses of the same agent (Comparison 4), Outcome 1: Clinical recurrence at 6 months
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias (high risk of bias for incomplete outcome data in Sobel 1986 and blinding of participants in Spacek 2005) and imprecision.
Only Sobel 1986 reported results at 12 months, finding low‐dose ketoconazole compared to high‐dose may not reduce clinical recurrence (RR 0.83, 95% CI 0.47 to 1.49; participants = 42; studies = 1; I2 = 0%; fixed‐effect; very low certainty evidence; Analysis 4.2). Our confidence in these findings is very low.
4.2. Analysis.

Comparison 4: Comparison of different doses of the same agent (Comparison 4), Outcome 2: Clinical recurrence at 12 months
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias and imprecision.
3. Adverse events
Only Spacek 2005 reported adverse events. In this study of 26 participants with RVVC and 34 participants with acute VVC, one participant developed reversible alopecia areata and one reported mild nausea with diarrhoea. However, it was not clear if these women had RVVC or acute VCC nor to which treatment group they had been allocated. Our confidence in these findings is very low.
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias and imprecision.
Secondary outcomes
1. Time to first recurrence
In Sobel 1986, the mean time to first recurrence after cessation of therapy was the same (2.6 months) in both the perimenstrual ketoconazole and the daily ketoconazole groups.
2. Number of symptomatic days per year
None of the three studies in this comparison reported this outcome (Fong 1994; Sobel 1986; Spacek 2005).
3. Number of mycological recurrences per participant per year
None of the three studies in this comparison reported this outcome (Fong 1994; Sobel 1986; Spacek 2005).
4. Proportion of participants with at least one mycological recurrence during the treatment and follow‐up period
Only Sobel 1986 reported this outcome, finding daily administration of ketoconazole may not reduce mycological recurrence compared to perimenstrual administration at six months (RR 0.50, 95% CI 0.14 to 1.74; participants = 42; very low certainty evidence; Analysis 4.3) and at 12 months (RR 0.86, 95% CI 0.53 to 1.38; participants = 42; very low certainty evidence; Analysis 4.4). The rate of mycological recurrence was 29% (6/21) in the perimenstrual ketoconazole group and 14% (3/21) in the daily ketoconazole group at six months and 67% (14/21) and 57% (12/21) respectively at 12 months. Our confidence in these findings is very low.
4.3. Analysis.

Comparison 4: Comparison of different doses of the same agent (Comparison 4), Outcome 3: Mycological recurrence at 6 months
4.4. Analysis.

Comparison 4: Comparison of different doses of the same agent (Comparison 4), Outcome 4: Mycological recurrence at 12 months
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias and imprecision.
5. Duration of symptoms after treatment initiation
None of the three studies in this comparison reported this outcome (Fong 1994; Sobel 1986; Spacek 2005).
6. Patient preference
In Fong 1994, participants preferred empiric self‐treatment with clotrimazole (73.9%) with perimenstrual clotrimazole (17.4%), with some participants not expressing a preference (8.7%) (P<0.05).
Comparison 6: Short duration of treatment versus longer duration of treatment
One study compared a one‐day regimen of itraconazole with a three‐day regimen of itraconazole (Spacek 2005).
Primary outcomes
1. Number of clinical recurrences per participant per year
The one study in this comparison did not report this outcome (Spacek 2005).
2. Proportion of participants with at least one clinical recurrence during the treatment and follow‐up period
Spacek 2005 only reported the proportion of participants with at least one clinical recurrence after six months. In this single study, short‐term treatment may reduce to no reduce clinical recurrence compared to and long‐term treatment (RR 0.80, 95% CI 0.47 to 1.35; participants = 26; studies = 1; I2 = 0%; fixed‐effect; very low certainty evidence; Analysis 5.1). Our confidence in these findings is very low.
5.1. Analysis.

Comparison 5: Short duration versus long duration of the same treatment (Comparison 5), Outcome 1: Clinical recurrence at 6 months
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias and imprecision.
3. Adverse events
In this study of 26 participants with RVVC and 34 participants with acute VVC, one participant developed reversible alopecia areata and one reported mild nausea with diarrhoea (Spacek 2005). However, it was not clear if these women had RVVC or acute VCC nor to which treatment group they had been allocated.
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias and imprecision.
Secondary outcomes
None of the secondary outcomes could be extracted.
Comparison 7: Partner treatment versus placebo/no treatment
Two studies examined this comparison: Fong 1992b, where male partners were treated with a short course of ketoconazole, and Sobel 1985a, where male partners were treated with a short course of miconazole cream. In both studies, the control group received no treatment. The characteristics of studies against this comparison are summarised in a supplementary table (Table 6).
4. Summary of characteristics of studies included in Comparison 7: Partner treatment versus placebo/no treatment.
| Study ID (*) | Fong 1992b | Sobel 1985a |
| Participants (n) | 58 | 40 |
| Candida albicansat enrolment (%) | ‐ | 100 |
| Mean episodes in previous 12 months | 8.4 (ketoconazole), 9.5 (no treatment) | 5.1 (miconazole), 5.3 (no treatment) |
| Withdrawals/loss to follow‐up (%) | 7 | 9 |
| Setting | Hospital outpatient clinic | NSa |
| Country | Canada | USA |
| Intervention 1 | Partner treatment with ketoconazole daily for 5 days | 1% miconazole cream daily for 1 week |
| Intervention 2 | No treatment | No treatment |
| Intervention 3 | ‐ | ‐ |
| Duration of intervention | Single treatment | 1 week |
| Duration of observation after intervention | 12 months | 12 months |
| Planned assessments | Monthly for 12 months | Monthly for 6 months, then 9 months, 12 months |
| Assessment between planned visits if symptoms developed | Yes | Yes |
aNot reported or unclear.
Primary outcomes
1. Number of clinical recurrences per participant per year
Neither of the two studies in this comparison reported this outcome (Fong 1992b; Sobel 1985a).
2. Proportion of participants with at least one clinical recurrence during the treatment and follow‐up period
Only Fong 1992b reported one of our primary outcomes, finding that may reduce to no reduce clinical recurrence at six or 12 months. The incidence of clinical recurrence at six months was 65% (17/26) in the ketoconazole group compared to 71% (20/28) in the no‐treatment group (RR 0.92, 95% CI 0.64 to 1.32; participants = 54; very low certainty evidence; Analysis 6.1). At 12 months, it was 85% (22/26) and 82% (23/28), respectively (RR 1.03, 95% CI 0.81 to 1.31; participants = 54; very low certainty evidence; Analysis 6.2). Our confidence in these findings is very low.
6.1. Analysis.

Comparison 6: Partner treatment versus placebo/no treatment (Comparison 6), Outcome 1: Clinical recurrence at 6 months
6.2. Analysis.

Comparison 6: Partner treatment versus placebo/no treatment (Comparison 6), Outcome 2: Clinical recurrence at 12 months (6 months active, 6 months observation)
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias and imprecision.
3. Adverse events
In Fong 1992b, the adverse event rate was minimal. One participant in the untreated group was removed from the study due to an adverse reaction. No removals occurred for this reason in the treated group.
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias and imprecision.
Secondary outcomes
1. Time to first recurrence
Neither of the two studies in this comparison reported this outcome (Fong 1992b; Sobel 1985a).
2. Number of symptomatic days per year
Neither of the two studies in this comparison reported this outcome (Fong 1992b; Sobel 1985a).
3. Number of mycological recurrences per participant per year
Neither of the two studies in this comparison reported this outcome (Fong 1992b; Sobel 1985a).
4. Proportion of participants with at least one mycological recurrence during the treatment and follow‐up period
Clinical recurrence at 6 months
Sobel 1985a reported this outcome, finding a mycological recurrence rate of 55% (11/20) in the treated‐partners group compared to 75% (15/20) in the untreated‐partners group at six months (RR 0.73, 95% CI 0.46 to 1.17; participants = 40; very low certainty evidence; Analysis 6.3). Our confidence in these findings is very low.
6.3. Analysis.

Comparison 6: Partner treatment versus placebo/no treatment (Comparison 6), Outcome 3: Mycological recurrence at 6 months
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias (high risk of bias for allocation concealment in Sobel 1985a and blinding of participants and assessment in Sobel 1985a) and imprecision.
Clinical recurrence at 12 months
At 12 months the mycological recurrence rates were 70% (14/20) in the treated group and 80% (16/20) in the untreated group (RR 0.88, 95% CI 0.61 to 1.26; participants = 40; very low certainty evidence; Analysis 6.4). Our confidence in these findings is very low.
6.4. Analysis.

Comparison 6: Partner treatment versus placebo/no treatment (Comparison 6), Outcome 4: Mycological recurrence at 12 months
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias (high risk of bias for allocation concealment in Sobel 1985a and blinding of participants and assessment in Sobel 1985a) and imprecision.
5. Duration of symptoms after treatment initiation
Neither of the two studies in this comparison reported this outcome (Fong 1992b; Sobel 1985a).
6. Patient preference
Sobel 1985a reported that an "overwhelming majority" felt like they had benefited from the treatment, but did not provide additional detail on patient preference.
Comparison 8: Complementary and alternative medicine versus placebo/no treatment
Metts 2003 evaluated Lactobacillus vaginal tablets and probiotic oral tablets in a three‐way comparison against placebo tablets over a six‐month period. This study enrolled 34 women, but only nine women completed the study. No data could be extracted.
Primary outcomes
1. Number of clinical recurrences per participant per year
The one study in this comparison did not report this outcome (Metts 2003).
2. Proportion of participants with at least one clinical recurrence during the treatment and follow‐up period
Data to calculate clinical recurrence rate were collected but were not presented in a format that permitted extraction from the article. We contacted the authors but received no additional information.
3. Adverse events
Metts 2003 reported that one participant in the group receiving vaginal Lactobacillus tablets and an oral probiotic tablet dropped out due to brown vaginal discharge. We downgraded the certainty of the evidence by two levels to low due to high risk of bias for incomplete outcome data and imprecision.
Secondary outcomes
Secondary outcomes were not reported for this comparison.
Comparison 9: Complementary and alternative medicine versus drug treatments
Three studies examined this comparison (Chopra 2013; Kumari 2011; Witt 2009). Chopra 2013 and Kumari 2011 evaluated the effect of a polygodyal/anethole phytocompound (K‐712) compared to oral itraconazole. Witt 2009 randomised participants into three groups to compare monthly 1) itraconazole to 2) vaginal lactobacilli and to 3) classical homeopathy. The characteristics of studies against this comparison are summarised in a supplementary table (Table 7).
5. Summary of characteristics of studies included in Comparison 9: Complementary and alternative medicine versus placebo/no treatment.
| Study ID | Chopra 2013 | Kumari 2011 | Witt 2009 |
| Participants (n) | 122 | 82 | 150 |
| Candida albicansat enrolment (%) | ‐ | 54 | 100a |
| Mean episodes in previous 12 months | ‐ | NSb | NSb |
| Withdrawals/loss to follow‐up (%) | 0 | 10 | 53 |
| Setting | Gynaecology outpatients clinic | Hospital outpatient clinic | NSb |
| Country | Italy | Italy | Austria |
| Intervention 1 | Itraconazole (weekly) | Itraconazole (weekly) | Itraconazole (weekly) |
| Intervention 2 | Polygodyal/anethole phytocompound (twice daily for 1 week a month) | Polygodyal/anethole phytocompound (twice weekly) | Itraconazole (monthly) and lactobacilli (monthly for 6 days) |
| Intervention 3 | ‐ | ‐ | Classic homeopathy |
| Duration of intervention | 24 months | 6 months | 6 months |
| Duration of observation after intervention | 6 months | 6 months | 6 months |
| Planned assessments | Monthly for 24 months, then 6 months | Monthly for 6 months, then 9 months, 12 months | Monthly for 12 months |
| Assessment between planned visits if symptoms developed | Yes | ‐ | Yes |
aC albicans was a selection criterion. bNot reported or unclear.
Primary outcomes
1. Number of clinical recurrences per participant per year
None of the three studies in this comparison reported this outcome (Chopra 2013; Kumari 2011; Witt 2009).
2. Proportion of participants with at least one clinical recurrence during the treatment and follow‐up period
Chopra 2013 and Kumari 2011 reported this outcome.
Clinical recurrence at 6 months
Only Kumari 2011 reported results for this outcome after six months. Recurrence rate was similar in the six‐month treatment phase, with 5% (2/41) recurrence in the K‐712 group and 10% (4/41) recurrence in itraconazole group (RR 0.50, 95% CI 0.10 to 2.58; participants = 82; studies = 1; very low certainty evidence; Analysis 7.1). Our confidence in these findings is very low.
7.1. Analysis.

Comparison 7: Complementary and alternative medicine versus drug treatments (Comparison 7), Outcome 1: Clinical recurrence at 6 months
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias (blinding of participants, incomplete outcome data, and selective reporting) and imprecision.
Clinical recurrence at 12 months
However, at 12 months, pooling of Chopra 2013 and Kumari 2011 showed that complementary medicine may reduce clinical recurrence (RR 0.54, 95% CI 0.36 to 0.80; participants = 189; studies = 2; I2 = 0%; fixed‐effect; NNTB = 5; very low certainty evidence; Analysis 7.2). We downgraded the certainty of the evidence by three levels to very low due to imprecision and very serious risk of bias in Kumari 2011.
7.2. Analysis.

Comparison 7: Complementary and alternative medicine versus drug treatments (Comparison 7), Outcome 2: Clinical recurrence at 12 months
Clinical recurrence at 24 months
Only Chopra 2013 reported results after 24 months, finding a lower recurrence rate in the group receiving complementary medicine: 36% (22/56) recurrence in the K‐712 group and 64% (39/51) recurrence in itraconazole group (RR 0.51, 95% CI 0.36 to 0.74; participants = 107; studies = 1; low certainty evidence; Analysis 7.3). Our confidence in these findings is low.
7.3. Analysis.

Comparison 7: Complementary and alternative medicine versus drug treatments (Comparison 7), Outcome 3: Clinical recurrence at 24 months
We downgraded the certainty of the evidence by two levels to low due to serious risk of bias for blinding of participants and imprecision.
3. Adverse events
All three studies reported adverse events. Chopra 2013 reported transient/mild symptoms in 5% of participants in the K‐712 group compared to 31% in the itraconazole group. Kumari 2011 reported no adverse events in the K‐712 group compared to a rate of 10% in (4/41) in the itraconazole group, where participants suffered from nausea, abdominal discomfort, and an unpleasant taste. In Witt 2009, an adverse event thought to be attributable to itraconazole occurred in two participants (local allergic reaction and diarrhoea), resulting in discontinuation of the treatment. However, no adverse events were recorded in the classical homeopathy group. Our confidence in these findings is very low.
We downgraded the certainty of the evidence by three levels to very low due to very serious risk of bias in the included studies and imprecision.
Secondary outcomes
1. Time to first recurrence
None of the three studies in this comparison reported this outcome (Chopra 2013; Kumari 2011; Witt 2009).
2. Number of symptomatic days per year
None of the three studies in this comparison reported this outcome (Chopra 2013; Kumari 2011; Witt 2009).
3. Number of mycological recurrences per participant per year
None of the three studies in this comparison reported this outcome (Chopra 2013; Kumari 2011; Witt 2009).
4. Proportion of participants with at least one mycological recurrence during the treatment and follow‐up period
One study examined this outcome. Kumari 2011 found a 22% (9/41) mycological recurrence rate in the K‐712 group compared to 17% (7/41) in itraconazole group at six months. This rose to 34% (14/41) and 66% respectively at 12 months. Our confidence in these findings is very low.
We downgraded the certainty of the evidence by three levels to very low due to imprecision and very serious risk of bias in Kumari 2011.
5. Duration of symptoms after treatment initiation
None of the three studies in this comparison reported this outcome (Chopra 2013; Kumari 2011; Witt 2009).
6. Patient preference
None of the three studies in this comparison reported this outcome (Chopra 2013; Kumari 2011; Witt 2009).
Comparison 10: Complementary and alternative medicine versus non‐drug treatments
Two studies examined this comparison (D'Antuono 2012; D'Antuono 2013). D'Antuono 2012 and D'Antuono 2013 both evaluated the effect of DermaSilk briefs compared to cotton underwear for a six‐month period. The only difference between the two studies was that in the 2012 study, participants were also treated with fluconazole (150 mg weekly) for six months, whereas in the 2013 study, the only intervention was wearing DermaSilk versus cotton briefs. The characteristics of studies against this comparison are summarised in a supplementary table (Table 8).
6. Summary of characteristics of studies included in Comparison 10: Non‐drug treatment versus other treatment.
| Study ID (*) | D'Antuono 2012 | D'Antuono 2013 |
| Participants (n) | 100 | 30 |
| Candida albicansat enrolment (%) | 85 | 100 |
| Mean episodes in previous 12 months | NSa | NSa |
| Withdrawals/loss to follow‐up (%) | 4 | 0 |
| Setting | Hospital outpatient clinic | Hospital outpatient clinic |
| Country | Italy | Italy |
| Intervention 1 | DermaSilk briefs | DermaSilk briefs |
| Intervention 2 | Cotton briefs | Cotton briefs |
| Intervention 3 | ‐ | ‐ |
| Duration of intervention | 6 months | 6 months |
| Duration of observation after intervention | ‐ | ‐ |
| Planned assessments | 1 months, 3 months, and 6 months | 3 months and 6 months |
| Assessment between planned visits if symptoms developed | ‐ | ‐ |
aNot reported or unclear.
Primary outcomes
1. Number of clinical recurrences per participant per year
Neither of the two studies in this comparison reported this outcome (D'Antuono 2012; D'Antuono 2013).
2. Proportion of participants with at least one clinical recurrence during the treatment and follow‐up period
Both studies reported on the proportion of participants with clinical recurrence (D'Antuono 2012; D'Antuono 2013). However, only the results of D'Antuono 2012 were presented in a way that permitted data extraction. At six months, clinical recurrence was lower in the DermaSilk brief group (77% (37/48)) than in the cotton brief group (92% (44/48)) (RR 0.84, 95% CI 0.71 to 1.00; participants = 96; studies = 1; low certainty evidence; Analysis 8.1). Our confidence in these findings is low.
8.1. Analysis.

Comparison 8: Non‐drug treatment versus other treatment (Comparison 8), Outcome 1: Clinical recurrence at 6 months
We downgraded the certainty of the evidence by two levels to low due to imprecision and serious risk of bias (unclear randomisation).
3. Adverse events
No side effects were reported in either arm of D'Antuono 2012 or D'Antuono 2013.
Secondary outcomes
Not reported.
Comparison 11: Vaccination versus other treatment
One study examined the impact of 1) Lactobacillus vaccination (three vaccinations over six weeks), 2) heliotherapy (six‐week course), and 3) ciclopyroxolamine (six‐day course) (Mendling 2011). Ninety participants were randomised over the three treatment groups.
Primary outcomes
1. Number of clinical recurrences per participant per year
Mendling 2011 reported results for this outcome. Participants randomised to Lactobacillus vaccination had a mean number of clinical recurrences per participant per year of 1.4 (standard deviation 1.6), compared to 2.0 (1.9) in the heliotherapy group and 1.8 (1.6) in the ciclopyroxolamine group (see Analysis 9.1). All three groups had significantly fewer recurrences compared to the year prior to study enrolment, but there was no difference in recurrence rate across the 12‐month study period between groups. Our confidence in these findings is very low.
9.1. Analysis.

Comparison 9: Vaccination versus other treatment (Comparison 9), Outcome 1: Mean number of clinical recurrences per participant per year
We downgraded the certainty of the evidence by two levels to very low due to imprecision and very serious risk of bias in the included study.
2. Proportion of participants with at least one clinical recurrence during the treatment and follow‐up period
The one study in this comparison did not report this outcome (Mendling 2011).
3. Adverse events
In Mendling 2011, two participants in the vaccine group reported flu‐like symptoms, one of whom withdrew from the study. Our confidence in these findings is very low.
We downgraded the certainty of the evidence by two levels to very low due to imprecision and very serious risk of bias in the included study.
Secondary outcomes
1. Time to first recurrence
The one study in this comparison did not report this outcome (Mendling 2011).
2. Number of symptomatic days per year
The one study in this comparison did not report this outcome (Mendling 2011).
3. Number of mycological recurrences per participant per year
The one study in this comparison did not report this outcome (Mendling 2011).
4. Proportion of participants with at least one mycological recurrence during the treatment and follow‐up period
The one study in this comparison did not report this outcome (Mendling 2011).
5. Duration of symptoms after treatment initiation
The one study in this comparison did not report this outcome (Mendling 2011).
6. Patient preference
Mendling 2011 assessed patient preference by measuring the percentage of participants satisfied with the treatment. Overall, this was low across the study, with 48%, 27%, and 20% being satisfied in the vaccine, heliotherapy, and ciclopyroxolamine groups, respectively. Our confidence in these findings is very low.
We downgraded the certainty of the evidence by three levels to very low due to imprecision and very serious risk of bias in the included study.
Subgroup analyses
We were unable to undertake the subgroup analyses planned in our protocol due to insufficient data.
Discussion
Summary of main results
Only one study reported results for our first primary outcome (number of clinical recurrences per participant per year) (Mendling 2011). Eighteen studies presented data for our second primary outcome (proportion of participants with at least one clinical recurrence during the treatment and follow‐up period) (Bolouri 2009; Chopra 2013; D'Antuono 2012; D'Antuono 2013; Fardyazar 2007; Fong 1992a; Fong 1992b; Kumari 2011; Lopez‐Olmos 2000; Roth 1990; Sobel 1985a; Sobel 1986; Sobel 1989; Sobel 2004; Spacek 2005; Spinillo 1997). Sixteen studies reported on adverse events (Bolouri 2009; Chopra 2013; D'Antuono 2012; Fan 2015; Fardyazar 2007; Fong 1992a; Fong 1992b; Kumari 2011; Mendling 2011; Metts 2003; Roth 1990; Sobel 1986; Sobel 1989; Sobel 2004; Spacek 2005; Witt 2009). However, we were unable to pool any of the adverse events due to heterogeneity in reporting.
At six months, the proportion of women with clinical and mycological recurrences of VVC may be lower in those receiving antifungal drug treatment compared with those receiving placebo or no treatment. At 12 months (following six months active treatment/placebo or no treatment followed by six months observation), the proportion of women with clinical recurrence may be lower in the treatment group compared with the placebo/no treatment group; however, no differences were found in mycological recurrences between the two groups. The evidence at six and twelve months is uncertain.
Four studies compared oral versus topical antifungal treatment (Fan 2015; Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000). The evidence is very uncertain if there is a difference in clinical recurrence between oral and topical treatments. This concurs with a previous Cochrane Review (Nurbhai 2007), which found no difference in efficacy between oral and topical antifungal treatments. It is possible that non‐compliance may have contributed to therapeutic failure in some participants. However, participant compliance was not adequately reported in most studies.
Overall completeness and applicability of evidence
This review has some key strengths. Whilst other authors have summarised part of this body of literature (Pontes 2014; Rosa 2013; Van Kessel 2003; Watson 2007), this is the first systematic review to comprehensively address treatments for recurrent vulvovaginal candidiasis. The search strategy for this review was comprehensive and included contacting manufacturers of antifungal medications and content experts, which resulted in one trial being included despite the abstract not referring to the study as a randomised controlled trial (Sobel 1985a).
We were unable to perform analysis for many of the intended outcomes due to heterogeneity between included studies and the lack of studies reporting similar outcomes. Many studies compared different intervention regimens, with timing of treatments weekly, twice weekly, monthly, or for several days at a particular phase of the menstrual cycle. There are limited data on the efficacy of non‐pharmaceutical management of RVVC.
The vast majority of women included in the studies were colonised with Candida albicans (when reported usually >80%) and only a small proportion with C. krusei or C. glabrata, the latter requiring culture for diagnosis and often more difficult to treat with standard first line treatments (CDC 2015). Assessing the significance of mycological Candida spp. as a stand‐alone outcome was uncertain due to the high prevalence of asymptomatic colonisation in the community (Beigi 2004). However, colonisation is necessary for subsequent symptomatic episodes. It is uncertain what causes a commensal organism like Candida spp. to become pathogenic.
Comparison of some studies was complicated by the induction regimen. Several studies required women to achieve culture‐negative status prior to commencing the treatment phase (Bolouri 2009; Roth 1990; Sobel 1989; Sobel 2004); one study gave additional induction treatment to achieve negative cultures (Spinillo 1997); and some studies did not require participants to achieve culture‐negative status for Candida spp. (Fardyazar 2007; Fong 1992a; Sobel 1986).
Although we did not exclude pregnant women from our eligibility criteria, all but three studies identified studies (Fardyazar 2007; Fong 1992b; Lopez‐Olmos 2000) explicitly excluded pregnant women. It is unlikely that these studies will have included pregnant women and therefore, the conclusions of our review cannot be considered generalisable to women who are pregnant. Diabetes mellitus was an exclusion criterion in ten of the included studies, limiting our ability to draw conclusions about treatment of RVVC in this group.
Adverse events were variably reported. Systemic adverse events were reported more frequently with oral antifungal agents (nausea, vomiting, and diarrhoea) in two studies, whilst local sensitivity was reported with topical antifungal agents in two studies. Some studies reported this outcome comprehensively; others mentioned adverse events that resulted in withdrawal from the study; and still others did not mention adverse events. Due in part to this and the small number of included trials, a significant limitation is that rare adverse events were unlikely to have been detected in this review. Patient preference and cost‐effectiveness of the interventions were poorly reported in the included studies.
We were unable to draw conclusions regarding partner treatment. Comparing studies for some outcomes was problematic due to methodological issues and the small sample sizes of studies. For example, it was unclear in Fong 1992b why a dose of 200 mg of ketoconazole was used for five days to treat male partners of women with RVVC, when a previous study demonstrated that 400 mg of ketoconazole for five days resulted in significantly fewer clinical recurrences (Sobel 1986).
Quality of the evidence
The majority of the 21 included studies were small, with most having fewer than 100 participants. Most studies did not report sample size calculations, resulting in studies that were not powered to detect stated outcomes. There was generally a lack of homogeneity amongst included studies, with different comparators, length of intervention, and follow‐up periods. This resulted in small numbers of studies that could be pooled for each outcome.
The assessment of risk of bias across the included studies was challenged by poor reporting of the methods used in the studies. In particular, older studies often reported insufficient information to assess the risk of selection, performance, or detection bias. Many of the 'Risk of bias' items were therefore ranked as unclear or high risk of bias.
Only one of the included studies reported adequate blinding of participants, personnel, and assessors (Roth 1990). Only five included studies had placebo controls. We regarded the lack of placebo blinding with the use of vaginal cream or pessaries as a major issue, especially where studies compared the effect of non‐vaginal medications such as oral tablets (Fardyazar 2007; Fong 1992a; Lopez‐Olmos 2000; Roth 1990; Sobel 1989) and intramuscular injections (Mendling 2011). This generally resulted in a high risk of bias due to lack of blinding of participants and assessors. We considered only five studies as at low risk of bias regarding documentation and explanation of attrition. Additionally, most studies were funded by companies with a vested interest.
We downgraded the certainty of the evidence for the majority of outcomes to low, mainly due to serious risk of bias in the included studies and imprecision (low number of studies and inability to pool data). This means that additional studies are likely to have an important impact on our confidence in the estimates of effect and are likely to change the estimate. However, they may not alter the conclusions of this review.
Potential biases in the review process
We conducted a comprehensive search in multiple databases for this review. Several review authors independently assessed the eligibility of the studies identified by the search. Nevertheless, we may have missed studies in our search. By monitoring clinical trials registers, we attempt to keep this review up‐to‐date. Due to insufficient studies per comparison, we were unable to construct a funnel plot to assess for publication bias in this way.
Data extraction and 'Risk of bias' assessment were also conducted by up to four review authors independently. Any discrepancies were discussed by the team to ensure consistency.
Agreements and disagreements with other studies or reviews
A systematic review has examined the effect of weekly fluconazole therapy for recurrent vulvovaginal candidiasis (Rosa 2013). This study identified the same two trials we found in our systematic search of the literature (Bolouri 2009; Sobel 2004), and also concluded that fluconazole reduced the frequency of clinical recurrence for the six months of active treatment as well as in the subsequent six months. However, unlike our review, Rosa 2013 rated the risk of bias of the included studies as satisfactory overall. Of note, Rosa 2013 did not assess selective outcome reporting or other sources of bias in their assessment.
A second systematic review examined the impact of panty liners on vulvovaginal candidiasis (Pontes 2014). As in our review, Pontes 2014 did not identify any RCTs in RVVC. Van Kessel 2003 examined the evidence for complementary and alternative therapies for yeast vaginitis and bacterial vaginosis and arrived at a similar conclusion to this review regarding the paucity and low certainty of evidence in this area.
Four Cochrane Reviews evaluate treatments for vulvovaginal candidiasis (Nurbhai 2007; Ray 2011; Xie 2017; Young 2001), although only in the acute setting. As in our review of RVVC, the authors of Nurbhai 2007 found no difference in cure rates between oral or topical antifungals in acute uncomplicated vulvovaginal candidiasis.
Authors' conclusions
Implications for practice.
In non‐pregnant women with recurrent vulvovaginal candidiasis (RVVC), suppressive therapy with oral or topical antifungal agents may reduce symptomatic, clinical recurrences when compared to placebo or no treatment. The therapy used should be according to patient preference and affordability. To date, good‐quality evidence for complementary and alternative therapies and the benefit of partner treatment for RVVC is limited.
Implications for research.
Further studies are required in this area. Researchers of new studies should focus on:
methodological quality and the reporting of such ‐ focusing in particular on rigour of blinding (participants, personnel, and outcome assessors);
collecting outcomes that are relevant to patients (e.g. mean number of recurrences in a 12‐month period, symptom‐free days, and patient preference) rather than simply the dichotomous outcome of any clinical recurrence;
describing the outcomes that are collected in sufficient detail (e.g. clinical recurrence clearly including both symptoms and mycological confirmation);
collecting outcome data at both defined time points as well as when symptoms develop (only nine of the 21 included studies stated that they assessed participants between planned visits if they developed symptoms in the intervening period, which is likely to result in underreporting of both primary and secondary outcomes);
reporting baseline characteristics more comprehensively, especially the severity of RVVC (e.g. average number of recurrences in the preceding 12 months);
using the commonly accepted case definition of RVVC (several studies were excluded from this review because they used a non‐standard definition of RVVC);
complementary and alternative medicine trials should focus in particular on quality as well as appropriate, commonly used comparison treatments;
only one study reported data on our first primary outcome (number of clinical recurrences per participant per year). Researchers of future studies should consider including this outcome in their study design;
more studies comparing oral versus topical treatments and studies investigating the optimal dose would be of clinical interest.
What's new
| Date | Event | Description |
|---|---|---|
| 25 January 2022 | Amended | Correction of wording in Results of the search |
History
Protocol first published: Issue 5, 2011 Review first published: Issue 1, 2022
Acknowledgements
The authors would like to acknowledge Sarah Thorning for designing the search strategies for this review and conducting the primary search. The authors would also like to acknowledge Lars Eriksson for his assistance with updating the searches.
Appendices
Appendix 1. Search update 2020‐2021
| Search electronic report #1 | |
| Search type | Update |
| Databases | MEDLINE |
| Platform | Ovid |
| Search date | 06/10/2021 |
| Update date | Undefined |
| Range of search date | 2019‐Current |
| Language restrictions | None |
| Other limits | None |
| Search strategy (results) | 1. exp Candidiasis, Vulvovaginal/ (3632)
2. exp Candida/ (48200)
3. exp Candidiasis/ (32981)
4. candid*.tw. (358579)
5 monilia*.tw. (1266)
6. thrush*.tw. (1206)
7. or/2‐6 (376084)
8. exp Vaginal Diseases/ (28738)
9. exp Vulvar Diseases/ (18167)
10. vulv*.tw. (19712)
11. vagin*.tw. (108669)
12. vulvovagin*.tw. (3355)
13. vulvo‐vagin*.tw. (352)
14. genit*.tw. (80077)
15. or/8‐14 (201525)
16. 7 and 15 17. 1 or 16 (8599) 18. exp Recurrence/ (191862) 19. exp Secondary Prevention/ (21647) 20. exp Chemoprevention/ (21467) 21. (recur* or relaps* or prevent* or chemoprev* or chemoprophyla* or prophylax* or prophylac* or refractory or repeat* or repetit* or chronic*).tw. (3634433) 22. exp Chronic Disease/ (271265) 23. treatment failure/ (36424) 24. (treatment$ adj2 fail$).tw. (39494) 25. or/18‐24 (3798342) 26. 17 and 25 (2592) 27. randomized controlled trial.pt. (544063) 28. controlled clinical trial.pt. (94402) 29. randomized.ab. (463771) 30. placebo.ab. (201328) 31. clinical trials as topic.sh. (197484) 32. randomly.ab. (310818) 33. trial.ti. (215023) 34. or/27‐33 (1256039) 35. exp animals/ not humans.sh. (4889865) 36. 34 not 35 (1144770) 37. 26 and 36 (350) 38. limit 37 to yr="2020‐Current" (18) |
| # of records identified | 18 |
| Search electronic report #2 | |
| Search type | Update |
| Databases | EMBASE |
| Platform | ELSEVIER |
| Search date | 06/10/2021 |
| Update date | Undefined |
| Range of search date | 2018‐Current |
| Language restrictions | None |
| Other limits | None |
| Search strategy (results) | 1. vagina candidiasis'/exp 5,796 2. candida'/exp 93,690 3. candidiasis'/exp 55,58 4. candid*:ab,ti OR monilia*:ab,ti OR thrush*:ab,ti 568,224 5. #2 OR #3 OR #4 612,797 6. vagina disease'/exp 70,593 7. vulva disease'/exp 20,455 8. vulv*:ab,ti OR vagin*:ab,ti OR vulvovagin*:ab,ti OR genit*:ab,ti OR ((vulvo NEAR/1 vagin*):ab,ti) 301,184 9. #6 OR #7 OR #8 329,889 10. #5 AND #9 15,697 11. #1 OR #10 15,697 12. recurrent disease'/de 194,304 13. secondary prevention'/de 31,012 14. prophylaxis'/de OR 'chemoprophylaxis'/de OR 'infection prevention'/de 212,635 15. recur*:ab,ti OR relaps*:ab,ti OR prevent*:ab,ti OR chemoprev*:ab,ti OR repeat*:ab,ti OR repetit*:ab,ti OR chronic*:ab,ti OR prophylax*:ab,ti OR prophylac*:ab,ti OR refractory:ab,ti 5,759,315 16. chronic disease'/de 206,400 17. treatment failure'/exp 182,363 18. (treatment* NEAR/2 fail*):ab,ti 71,300 19. #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 6,052,729 20. #11 AND #19 5,116 21. randomized controlled trial'/de 680,287 22. 'controlled clinical study'/de 435,176 23. random*:ti,ab 1,709,875 24. randomization'/de 91,949 25. intermethod comparison'/de 277,719 26. placebo:ti,ab 330,912 27. compare:ti OR compared:ti OR comparison:ti 570,466 28. (evaluated:ab OR evaluate:ab OR evaluating:ab OR assessed:ab OR assess:ab) AND (compare:ab OR compared:ab OR comparing:ab OR comparison:ab) 2,373,746 29. (open NEAR/1 label):ti,aB 91,224 30. ((double OR single OR doubly OR singly) NEAR/1 (blind OR blinded OR blindly)):ti,ab 251,275 31. double blind procedure'/de 188,893 32. (parallel NEXT/1 group*):ti,ab 28,194 33. crossover:ti,ab OR 'cross over':ti,ab 113,165 34. ((assign* OR match OR matched OR allocation) NEAR/5 (alternate OR group* OR intervention* OR patient* OR subject* OR participant*)):ti,ab 364,722 35. assigned:ti,ab OR allocated:ti,ab 428,789 36. (controlled NEAR/7 (study OR design OR trial)):ti,ab 391,000 37. volunteer:ti,ab OR volunteers:ti,ab 262,747 38. trial:ti 346,345 39. human experiment'/de 557,732 40. #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36 OR #37 OR #38 OR #39 5,560,462 41. #20 AND #40 1,116 42. #20 AND #40 AND [embase]/lim AND [2020‐2021]/py 98 |
| # of records identified | 98 |
| Search electronic report #3 | |
| Search type | Update |
| Databases | The Cochrane Central Register of Controlled Trials (CENTRAL) |
| Platform | Ovid |
| Search date | 06/10/2021 |
| Update date | Undefined |
| Range of search date | 2019‐Current |
| Language restrictions | None |
| Other limits | None |
| Search strategy (results) | 1. exp Candidiasis, Vulvovaginal/ (333) 2. exp Candida/ (444) 3. exp Candidiasis/ (958) 4. candid*.tw. (20077) 5. monilia*.tw. (31) 6. thrush*.tw. (124) 7. or/2‐6 (20406) 8. exp Vaginal Diseases/ (1321) 9. exp Vulvar Diseases/ (668) 10. vulv*.tw. (1853) 11. vagin*.tw. (19025) 12. vulvovagin*.tw. (786) 13. vulvo‐vagin*.tw. (77) 14 genit*.tw. (6036) 15. or/8‐14 (24627) 16. 7 and 15 (1355) 17. 1 or 16 (1355) 18. exp Recurrence/ (12295) 19. exp Secondary Prevention/ (3106) 20. exp Chemoprevention/ (1612) 21. (recur* or relaps* or prevent* or chemoprev* or chemoprophyla* or prophylax* or prophylac* or refractory or repeat* or repetit* or chronic*).tw. (476046) 22. exp Chronic Disease/ (13339) 23. treatment failure/ (3336) 24. (treatment$ adj2 fail$).tw. (13490) 25. or/18‐24 (489667) 26. 17 and 25 (540) 27. limit 26 to yr="2020‐Current" (51) |
| # of records identified | 51 |
Appendix 2. CINAHL search strategy
From inception to 30 May 2019 (later CINAHL output is included in the CENTRAL 6 October 2021 search output)
S1 (MH "Candidiasis, Vulvovaginal")
S2 (MH "Candida+")
S3 (MH "Candidiasis+") Search modes ‐ Boolean/Phrase Interface ‐ EBSCOhost
S4 TI ( candid* or monilia* or thrush* ) OR AB ( candid* or monilia* or thrush* )
S5 S2 or S3 or S4
S6 (MH "Vaginal Diseases+")
S7 (MH "Vulvar Diseases+")
S8 TI ( vulv* or vulvovagin* or vulvo‐vagin* or genit* ) OR AB ( vulv* or vulvovagin* or vulvo‐vagin* or genit* )
S9 S6 or S7 or S8
S10 S5 and S9
S11 S1 or S10
S12 (MH "Recurrence")
S13 (MH "Chemoprevention+")
S14 TI ( recur* or relaps* or prevent* or chemoprev* or chemoprophyla* or prophyla* or repeat* or repetit* or chronic* or refractory ) OR AB ( recur* or relaps* or prevent* or chemoprev* or chemoprophyla* or prophyla* or repeat* or repetit* or chronic* or refractory )
S15 (MH "Chronic Disease")
S16 (MH "Treatment Failure")
S17 TI treatment* N2 fail* OR AB treatment* N2 fail*
S18 S12 or S13 or S14 or S15 or S16 or S17
S19 S11 and S18
S20 (MH "Clinical Trials+")
S21 PT clinical trial
S22 TI clinic* trial* OR AB clinic* trial*
S23 TI ( singl* blind* or doubl* blind* or tripl* blind* or trebl* blind* ) OR AB ( singl* blind* or doubl* blind* or tripl* blind* or trebl* blind* )
S24 TI ( singl* mask* or doubl* mask* or tripl* mask* or trebl* mask* ) OR AB ( singl* mask* or doubl* mask* or tripl* mask* or trebl* mask* )
S25 TI random* OR AB random*
S26 TI placebo* OR AB placebo*
S27 (MH "Placebos")
S28 (MH "Quantitative Studies")
S29 S20 or S21 or S22 or S23 or S24 or S25 or S26 or S27 or¬ S28
S30 S19 and S29
Appendix 3. Search update 2019‐2020
| Search electronic report #1 | |
| Search type | Update |
| Databases |
|
| Platform | Ovid |
| Search date | 11/09/2020 |
| Update date | Undefined |
| Range of search date | 2019‐Current |
| Language restrictions | None |
| Other limits | None |
| Search strategy (results) | 1. exp Candidiasis, Vulvovaginal/ (3531) 2. exp Candida/ (46152) 3. exp Candidiasis/ (32038) 4. candid*.tw. (396019) 5. monilia*.tw. (1323) 6. thrush*.tw. (1376) 7. or/2‐6 (413427) 8. exp Vaginal Diseases/ (27998) 9. exp Vulvar Diseases/ (17635) 10. vulv*.tw. (21101) 11. vagin*.tw. (115328) 12. vulvovagin*.tw. (3540) 13. vulvo‐vagin*.tw. (385) 14. genit*.tw. (85644) 15. or/8‐14 (213986) 16. 7 and 15 (9110) 17. 1 or 16 (9110) 18. exp Recurrence/ (184235) 19. exp Secondary Prevention/ (20479) 20. exp Chemoprevention/ (20280) 21. (recur* or relaps* or prevent* or chemoprev* or chemoprophyla* or prophylax* or prophylac* or refractory or repeat* or repetit* or chronic*).tw. (3894076) 22. exp Chronic Disease/ (263842) 23. treatment failure/ (35169) 24. (treatment$ adj2 fail$).tw. (42517) 25. or/18‐24 (4056936) 26. 17 and 25 (2769) 27. randomized controlled trial.pt. (512768) 28. controlled clinical trial.pt. (93834) 29. randomized.ab. (491720) 30. placebo.ab. (210785) 31. clinical trials as topic.sh. (192845) 32. randomly.ab. (340563) 33. trial.ti. (224685) 34. or/27‐33 (1311991) 35. exp animals/ not humans.sh. (4732465) 36. 34 not 35 (1207857) 37. 26 and 36 (366) 38. limit 37 to yr="2019 ‐Current" (33) |
| # of records identified | 33 |
| Search electronic report #2 | |
| Search type | Update |
| Database | EMBASE |
| Platform | EMBASE.com |
| Search date | 11/09/2020 |
| Update date | Undefined |
| Range of search date | 2019‐Current |
| Language restrictions | None |
| Other limits | None |
| Search strategy (results) | 1. 'vagina candidiasis'/de 5482 2. 'candida'/exp 88356 3. 'candidiasis'/exp 52847 4. candid*:ab,ti OR monilia*:ab,ti OR thrush*:ab,ti 520092 5. #2 OR #3 OR #4 561823 6. 'vagina disease'/exp 66430 7. 'vulva disease'/exp 19434 8. vulv*:ab,ti OR vagin*:ab,ti OR vulvovagin*:ab,ti OR genit*:ab,ti OR ((vulvo NEAR/1 vagin*):ab,ti) 283527 9. #6 OR #7 OR #8 310638 10. #5 AND #9 14851 11. #1 OR #10 14851 12. 'recurrent disease'/de 182579 13. 'secondary prevention'/de 28684 14. 'prophylaxis'/de OR 'chemoprophylaxis'/de OR 'infection prevention'/de 195734 15. recur*:ab,ti OR relaps*:ab,ti OR prevent*:ab,ti OR chemoprev*:ab,ti OR repeat*:ab,ti OR repetit*:ab,ti OR chronic*:ab,ti OR prophylax*:ab,ti OR prophylac*:ab,ti OR refractory:ab,ti 5344766 16. 'chronic disease'/de 197683 17. 'treatment failure'/exp 165886 18. (treatment* NEAR/2 fail*):ab,ti 65657 19. #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 5618762 20. #11 AND #19 4782 21. 'randomized controlled trial'/de 618196 22. 'controlled clinical study'/de 430974 23. random*:ti,ab 1565124 24. 'randomization'/de 87421 25. 'intermethod comparison'/de 265038 26. placebo:ti,ab 310203 27. compare:ti OR compared:ti OR comparison:ti 538415 28. (evaluated:ab OR evaluate:ab OR evaluating:ab OR assessed:ab OR assess:ab) AND (compare:ab OR compared:ab OR comparing:ab OR comparison:ab) 2152786 29. (open NEAR/1 label):ti,ab 80601 30. ((double OR single OR doubly OR singly) NEAR/1 (blind OR blinded OR blindly)):ti,ab 236846 31. 'double blind procedure'/de 175674 32. (parallel NEXT/1 group*):ti,ab 25917 33. crossover:ti,ab OR 'cross over':ti,ab 106609 34. ((assign* OR match OR matched OR allocation) NEAR/5 (alternate OR group* OR intervention* OR patient* OR subject* OR participant*)):ti,ab 336166 35. assigned:ti,ab OR allocated:ti,ab 394454 36. (controlled NEAR/7 (study OR design OR trial)):ti,ab 356897 37. volunteer:ti,ab OR volunteers:ti,ab 250269 38. trial:ti 313056 39. 'human experiment'/de 512550 40. #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36 OR #37 OR #38 OR #39 5125028 41. #20 AND #40 1046 42. #20 AND #40 AND [embase]/lim AND [2018‐2020]/py 158 |
| # of records identified | 485 |
| Search electronic report #3 | |
| Search type | Update |
| Database | The Cochrane Central Register of Controlled Trials (CENTRAL) |
| Platform | Ovid |
| Search date | 11/09/2020 |
| Update date | Undefined |
| Range of search date | 2019‐Current |
| Language restrictions | None |
| Other limits | None |
| Search strategy (results) | 1. exp Candidiasis, Vulvovaginal/ (321) 2. exp Candida/ (434) 3. exp Candidiasis/ (937) 4. candid*.tw. (17916) 5. monilia*.tw. (31) 6. thrush*.tw. (117) 7. or/2‐6 (18241) 8. exp Vaginal Diseases/ (1261) 9. exp Vulvar Diseases/ (630) 10. vulv*.tw. (1698) 11. vagin*.tw. (17510) 12. vulvovagin*.tw. (713) 13. vulvo‐vagin*.tw. (69) 14. genit*.tw. (5513) 15. or/8‐14 (22664) 16. 7 and 15 (1264) 17. 1 or 16 (1264) 18. exp Recurrence/ (11873) 19. exp Secondary Prevention/ (2995) 20. exp Chemoprevention/ (1553) 21. (recur* or relaps* or prevent* or chemoprev* or chemoprophyla* or prophylax* or prophylac* or refractory or repeat* or repetit* or chronic*).tw. (439212) 22. exp Chronic Disease/ (13008) 23. treatment failure/ (3246) 24. (treatment$ adj2 fail$).tw. (12562) 25. or/18‐24 (452213) 26. 17 and 25 (498) 27. 27 limit 26 to yr="2019 ‐Current" (46) |
| # of records identified | 46 |
Appendix 4. CENTRAL (Cochrane Register of Studies Online) search strategy
Searched 30 May 2019
Web platform
1 exp Candidiasis, Vulvovaginal/ (258) 2 exp Candida/ (411) 3 exp Candidiasis/ (769) 4 candid*.tw. (8908) 5 monilia*.tw. (29) 6 thrush*.tw. (70) 7 or/2‐6 (9185) 8 exp Vaginal Diseases/ (936) 9 exp Vulvar Diseases/ (435) 10 vulv*.tw. (886) 11 vagin*.tw. (10054) 12 vulvovagin*.tw. (372) 13 vulvo‐vagin*.tw. (34) 14 genit*.tw. (2880) 15 or/8‐14 (12858) 16 7 and 15 (730) 17 1 or 16 (730) 18 exp Recurrence/ (10470) 19 exp Secondary Prevention/ (2658) 20 exp Chemoprevention/ (1388) 21 (recur* or relaps* or prevent* or chemoprev* or chemoprophyla* or prophylax* or prophylac* or refractory or repeat* or repetit* or chronic*).tw. (259095) 22 exp Chronic Disease/ (11240) 23 treatment failure/ (2947) 24 (treatment$ adj2 fail$).tw. (7248) 25 or/18‐24 (268760) 26 17 and 25 (265)
Appendix 5. MEDLINE search strategy
From 1946 to 30 May 2019
OVID platform
1 exp Candidiasis, Vulvovaginal/ (3284) 2 exp Candida/ (41702) 3 exp Candidiasis/ (29756) 4 candid*.tw. (322013) 5 monilia*.tw. (1289) 6 thrush*.tw. (1153) 7 or/2‐6 (338616) 8 exp Vaginal Diseases/ (26406) 9 exp Vulvar Diseases/ (16455) 10 vulv*.tw. (18763) 11 vagin*.tw. (102773) 12 vulvovagin*.tw. (2957) 13 vulvo‐vagin*.tw. (335) 14 genit*.tw. (76285) 15 or/8‐14 (191717) 16 7 and 15 (8238) 17 1 or 16 (8238) 18 exp Recurrence/ (168388) 19 exp Secondary Prevention/ (17732) 20 exp Chemoprevention/ (17558) 21 (recur* or relaps* or prevent* or chemoprev* or chemoprophyla* or prophylax* or prophylac* or refractory or repeat* or repetit* or chronic*).tw. (3353096) 22 exp Chronic Disease/ (246406) 23 treatment failure/ (31554) 24 (treatment$ adj2 fail$).tw. (35821) 25 or/18‐24 (3504658) 26 17 and 25 (2443) 27 randomized controlled trial.pt. (454273) 28 controlled clinical trial.pt. (92178) 29 randomized.ab. (403817) 30 placebo.ab. (186669) Cochrane Sexually Transmitted Infections School of Medicine Universidad Nacional de Colombia Ciudad Universitaria Bogotá D.C. Colombia VM 107 [Feb‐2018] 31 clinical trials as topic.sh. (182669) 32 randomly.ab. (285621) 33 trial.ti. (178408) 34 or/27‐33 (1135006) 35 exp animals/ not humans.sh. (4428797) 36 34 not 35 (1045278) 37 26 and 36 (324)
Appendix 6. Embase search strategy
From inception to 30 May 2019
EMBASE.com platform
1 'vagina candidiasis'/de (4796) 2 'candida'/exp (77193) 3 'candidiasis'/exp (46756) 4 candid*:ab,ti OR monilia*:ab,ti OR thrush*:ab,ti (414882) 5 #2 OR #3 OR #4 (451733) 6 'vagina disease'/exp (61474) 7 'vulva disease'/exp (17200) 8 vulv*:ab,ti OR vagin*:ab,ti OR vulvovagin*:ab,ti OR genit*:ab,ti OR ((vulvo NEAR/1 vagin*):ab,ti) (244258) 9 #6 OR #7 OR #8 (269706) 10 #5 AND #9 (13006) 11 #1 OR #10 (13006) 12 'recurrent disease'/de (158043) 13 'secondary prevention'/de (23700) 14 'prophylaxis'/de OR 'chemoprophylaxis'/de OR 'infection prevention'/de (164651) 15 recur*:ab,ti OR relaps*:ab,ti OR prevent*:ab,ti OR chemoprev*:ab,ti OR repeat*:ab,ti OR repetit*:ab,ti OR chronic*:ab,ti OR prophylax*:ab,ti OR prophylac*:ab,ti OR refractory:ab,ti (4470138) 16 'chronic disease'/de (176824) 17 'treatment failure'/exp (128921) 18 (treatment* NEAR/2 fail*):ab,ti (53300) 19 #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR 4703510 20 #11 AND #19 (4052) 21 'randomized controlled trial'/de (485581) 22 'controlled clinical study'/de (421456) 23 random*:ti,ab (1261628) 24 'randomization'/de (76749) 25 'intermethod comparison'/de (230724) 26 placebo:ti,ab (264790) 27 compare:ti OR compared:ti OR comparison:ti (464913) 28 (evaluated:ab OR evaluate:ab OR evaluating:ab OR assessed:ab OR assess:ab) AND (compare:ab OR compared:ab OR comparing:ab OR comparison:ab) (1680360) 29 (open NEAR/1 label):ti,ab (61758) 30 ((double OR single OR doubly OR singly) NEAR/1 (blind OR blinded OR blindly)):ti,ab (204170) 31 'double blind procedure'/de (146064) 32 (parallel NEXT/1 group*):ti,ab (21027) 33 crossover:ti,ab OR 'cross over':ti,ab (90348) 34 ((assign* OR match OR matched OR allocation) NEAR/5 (alternate OR group* OR intervention* OR patient* OR subject* OR participant*)):ti,ab (272980) 35 assigned:ti,ab OR allocated:ti,ab (320668) 36 (controlled NEAR/7 (study OR design OR trial)):ti,ab (284673) 37 volunteer:ti,ab OR volunteers:ti,ab (219833) 38 trial:ti (243380) 39 'human experiment'/de (396075) 40 #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 OR #34 OR #35 OR #36 OR #37 OR #38 OR #39 (4169943) 41 #20 AND #40 (863)
Appendix 7. Web of Science search strategy
From inception to 30 May 2019
#1Topic=((candid* or monilia or thrush) NEAR/5 (vagin* or vulv* or vulvovagin* or vulvo‐vagin* or genit*))
#2Topic=(recur* or relaps* or prevent* or chemoprev* or chemoprophyla* or prophylax* or prophylac* or repeat* or chronic* or refractory)
#3 #2 AND #1
#4Topic=(random* or placebo* or "clinic* trial*" or "singl* blind*" or "doubl* blind*")
#5 #4 AND #3
DocType=All document types; Language=All languages;
Appendix 8. ProQuest Dissertations search strategy
From 1/1/1980 to 30 May 2019
ab(candid* OR thrush OR mongolia) AND
ab(vulvovagin* OR vulvo‐vagin* OR vulv* OR vagin* OR genit*) AND
ab(recur* OR relaps* OR prevent* OR chemoprev* OR chemoprophyla* OR prophylax* OR prophylac* OR repeat* OR refractory)
Appendix 9. ClinicalTrials.gov search strategy
From inception to 27 July 2019
Search type: Advanced search
Condition or disease: vulvovaginal candidiasis OR vaginal candidiasis OR vaginal thrush OR vulvovaginal thrush
Study type: Interventional Studies
Appendix 10. WHO International Clinical Trials Registry Platform search strategy
From inception to 27 July 2019
Search type: Advanced
Condition: vulvovaginal candidiasis OR vaginal candidiasis OR vaginal thrush OR vulvovaginal thrush
Recruitment status: All
Data and analyses
Comparison 1. Drug treatment versus placebo/no treatment (excluding partner treatment) (Comparison 1).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Clinical recurrence at 6 months | 6 | 607 | Risk Ratio (M‐H, Random, 95% CI) | 0.36 [0.21, 0.63] |
| 1.1.1 Oral | 4 | 518 | Risk Ratio (M‐H, Random, 95% CI) | 0.29 [0.14, 0.62] |
| 1.1.2 Topical | 2 | 89 | Risk Ratio (M‐H, Random, 95% CI) | 0.55 [0.26, 1.14] |
| 1.2 Clinical recurrence at 12 months (6 months active, 6 months observation) | 6 | 585 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.72, 0.89] |
| 1.2.1 Oral | 4 | 496 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.68, 0.88] |
| 1.2.2 Topical | 2 | 89 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.77, 1.13] |
| 1.3 Mycological recurrence at 6 months | 5 | 568 | Risk Ratio (M‐H, Random, 95% CI) | 0.44 [0.25, 0.78] |
| 1.3.1 Oral | 4 | 506 | Risk Ratio (M‐H, Random, 95% CI) | 0.37 [0.22, 0.63] |
| 1.3.2 Topical | 1 | 62 | Risk Ratio (M‐H, Random, 95% CI) | 0.81 [0.62, 1.06] |
| 1.4 Mycological recurrence at 12 months | 3 | 189 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.79, 1.03] |
| 1.4.1 Oral | 2 | 127 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.71, 1.04] |
| 1.4.2 Topical | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.82, 1.17] |
Comparison 2. Oral drug treatment versus topical drug treatment (Comparison 2).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 Clinical recurrence at 6 months | 3 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.66 [0.83, 3.31] |
| 2.2 Clinical recurrence at 12 months (6 months active, 6 months observation) | 3 | 206 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.71, 1.27] |
| 2.3 Mycological recurrence at 6 months | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.64, 2.35] |
Comparison 3. Oral drug treatment versus oral drug treatment (Comparison 3).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 3.1 Clinical recurrence at 6 months | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.32 [0.84, 13.02] |
| 3.2 Clinical recurrence at 12 months | 1 | 33 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.62 [0.73, 3.61] |
Comparison 4. Comparison of different doses of the same agent (Comparison 4).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 4.1 Clinical recurrence at 6 months | 2 | 68 | Risk Ratio (M‐H, Random, 95% CI) | 0.45 [0.08, 2.69] |
| 4.2 Clinical recurrence at 12 months | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.47, 1.49] |
| 4.3 Mycological recurrence at 6 months | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.50 [0.14, 1.74] |
| 4.4 Mycological recurrence at 12 months | 1 | 42 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.53, 1.38] |
Comparison 5. Short duration versus long duration of the same treatment (Comparison 5).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 5.1 Clinical recurrence at 6 months | 1 | 26 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.47, 1.35] |
Comparison 6. Partner treatment versus placebo/no treatment (Comparison 6).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 6.1 Clinical recurrence at 6 months | 1 | 54 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.64, 1.32] |
| 6.2 Clinical recurrence at 12 months (6 months active, 6 months observation) | 1 | 54 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.81, 1.31] |
| 6.3 Mycological recurrence at 6 months | 1 | 40 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.73 [0.46, 1.17] |
| 6.4 Mycological recurrence at 12 months | 1 | 40 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.61, 1.26] |
Comparison 7. Complementary and alternative medicine versus drug treatments (Comparison 7).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 7.1 Clinical recurrence at 6 months | 1 | 82 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.50 [0.10, 2.58] |
| 7.2 Clinical recurrence at 12 months | 2 | 189 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.54 [0.36, 0.80] |
| 7.3 Clinical recurrence at 24 months | 1 | 107 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.51 [0.36, 0.74] |
Comparison 8. Non‐drug treatment versus other treatment (Comparison 8).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 8.1 Clinical recurrence at 6 months | 1 | 96 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.84 [0.71, 1.00] |
Comparison 9. Vaccination versus other treatment (Comparison 9).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 9.1 Mean number of clinical recurrences per participant per year | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.1.1 Vaccination versus heliotherapy | 1 | 47 | Mean Difference (IV, Fixed, 95% CI) | ‐0.60 [‐1.61, 0.41] |
| 9.1.2 Vaccination versus ciclopirox olamine | 1 | 46 | Mean Difference (IV, Fixed, 95% CI) | ‐0.40 [‐1.33, 0.53] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bolouri 2009.
| Study characteristics | ||
| Methods | Randomised controlled trial, placebo controlled Blinding ‐ not clearly stated Withdrawals/loss to follow‐up: 34% (33/97) Intention‐to‐treat analysis: No |
|
| Participants | N = 97 enrolled, 64 completed study Inclusion criteria: Female outpatients aged 18 to 45 years with an acute episode of vulvovaginal candidiasis (VVC) and a history of recurrent vulvovaginal candidiasis (RVVC) Definition of RVVC: At least 4 documented episodes of Candida vaginitis in the previous 12 months Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Fluconazole ‐ Oral, 150 mg, weekly, 6 months Placebo ‐ Oral, weekly, 6 months |
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 6 months, 9 months, 12 months (6 months active treatment, 6 months further follow‐up) Assessed if became symptomatic between planned visits: Not reported Primary outcomes
Secondary outcomes
|
|
| Funding | Pharmaceutical Sciences Resource Centre, Tehran University of Medical Sciences | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation and method of randomisation not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Placebo used. No comment as to whether similar between treatment and placebo in appearance |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is not clear if the assessors were blinded to the type of treatment (oral fluconazole vs placebo) received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Withdrawals/loss to follow‐up: 34%. Reasons for this not outlined. Per‐protocol analysis |
| Selective reporting (reporting bias) | Unclear risk | No protocol available for assessment. Side effects were monitored for during monthly visit but not reported. |
| Other bias | Low risk | Funding from Pharmaceutical Sciences Resource Centre, Tehran University of Medical Sciences |
Chopra 2013.
| Study characteristics | ||
| Methods | Randomised controlled trial, active control Blinding ‐ not stated Withdrawals/loss to follow‐up: 0% (1/122) Intention‐to‐treat analysis: No participants lost to follow‐up or non‐compliant with treatment regimen were excluded from analyses. Participants who relapsed during the 2‐year follow‐up and who were not mycologically cured after prespecified treatment protocol were excluded; 56 of 61 participants in the K‐712 group and 51 of 61 in the itraconazole group were included in the analysis. |
|
| Participants | N = 122 enrolled, 121 completed the study Inclusion criteria: Women with overall general good health, presenting to the gynaecology outpatient clinic with a history of RVVC Definition of RVVC: 4 proven cases of VVC in past 12 months Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Polygodyal phytocompound (K‐712) ‐ 1 tablet twice a day for 1 week to a month (the 100 mg composition is: 10 mg of oleoresin from Pseudowintera colorata at 30% concentration in polygodyal together with trace amounts of Olea europea) for 24 months. In case of relapse, participants received 1 tablet a day for 4 weeks. Itraconazole ‐ 200 mg once a week (administered as 100 mg tablets twice daily with meals) for 24 months. In case of relapse, participants received 200 mg every day for 7 days. |
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 2 years (active treatment), then 6‐month follow‐up post‐treatment Assessed if became symptomatic between planned visits: Yes Primary outcomes
Secondary outcomes
|
|
| Funding | Not reported | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Random numbers were computer generated" |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding is not referred to in trial publication. Given the different dosing regimens, it is unlikely that blinding occurred or was preserved. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is not clear if the assessors were blinded to the type of treatment received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Withdrawals/loss to follow‐up: 0% |
| Selective reporting (reporting bias) | Unclear risk | No protocol located to permit judgement of low risk or high risk. |
| Other bias | Unclear risk | Role of industry funding unclear |
Corthay 1988.
| Study characteristics | ||
| Methods | Randomised controlled trial, active control Blinding ‐ not stated Withdrawals/loss to follow‐up: unclear ‐ "Only 16 completed the 3 months ACFR." Intention‐to‐treat analysis: Not clear |
|
| Participants | N = 68 enrolled, number completing unclear ‐ "Only 16 completed the 3 months ACFR." Inclusion criteria: "Young women" with recurrent vaginal candidosis (RCV), otherwise healthy Definition of RVVC: 7 or more recurrences a year Exclusion criteria:
Setting
Baseline characteristics
|
|
| Interventions | ‐ Hyposensitization Treatment (HPT) with an aqueous Candida Albicans (CA) whole extract (n=33) An antifungal treatment (local + digestive) then a low‐sugar diet with vitamins, biotin and lyophilized bacillus subfilis supplements for 3 months (n=35) |
|
| Outcomes |
Timing of measurements Assessed at: 3, 6 and 9 months Assessed if became symptomatic between planned visits: Not reported Primary outcome
Secondary outcomes
|
|
| Funding | Not reported | |
| Notes | Abstract only, no full publication available | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation and method of randomisation not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not described |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Not described, but it is reported that only 16 women completed the 3 months Anti‐Candida Food Regimen in group 2 |
| Selective reporting (reporting bias) | Unclear risk | No protocol located to permit a judgement of low risk or high risk. |
| Other bias | High risk | Conference paper abstract only, no full publication identified |
D'Antuono 2012.
| Study characteristics | ||
| Methods | Randomised controlled trial, active control Blinding ‐ double‐blind Withdrawals/loss to follow‐up: 4% (4/100) Intention‐to‐treat analysis: No |
|
| Participants | N = 100 enrolled, 96 completed Inclusion criteria: Women aged 18+ years with a history of RVVC, presenting with a current episode of acute vulvovaginal candidiasis, confirmed with a positive culture for Candida spp. and a vaginitis severity score of greater than or equal to 3 Definition of RVVC: 4 or more episodes of Candida vaginitis in 1 year Exclusion criteria:
Setting
Baseline characteristics
|
|
| Interventions | DermaSilk briefs (3 pairs), worn daily for 6 months Cotton briefs (3 pairs), worn daily for 6 months Co‐intervention – All women were treated with fluconazole (150 mg weekly) for 6 months |
|
| Outcomes |
Timing of measurements Assessed at: 1, 3, 6 months Assessed if became symptomatic between planned visits: Not reported Primary outcome
Secondary outcomes
|
|
| Funding | Alpretec, producer of DermaSilk briefs, provided materials required to perform the study. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation and method of randomisation not described |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes used. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "The study was double‐blinded". Cotton and DermaSilk underwear are of similar appearance (author correspondence). |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Severity score assessed by participant ("double blinded" as per above) and lab result, but unclear if assessor of lab report was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Withdrawal/loss to follow‐up 4% |
| Selective reporting (reporting bias) | Unclear risk | No protocol located to permit a judgement of low risk or high risk. It is likely that information about mycological recurrence would have been collected by this study, but it was not reported. |
| Other bias | Unclear risk | Underpants supplied by the manufacturer. No information on how the study was funded. Age, mean duration of VVC, and incidence of symptoms and signs similar at baseline, but other factors not reported. |
D'Antuono 2013.
| Study characteristics | ||
| Methods | Randomised controlled trial, active control Blinding ‐ Double‐blind Withdrawals/loss to follow‐up: 0% Intention‐to‐treat analysis: Not mentioned, but no loss to follow‐up or withdrawals |
|
| Participants | N = 30 enrolled, 30 completed Inclusion criteria: Women aged 18+ years with a history of long‐term RVVC who had declined treatment with oral antimycotic drugs and who were presenting with an episode of vulvovaginal discomfort, confirmed by a vaginitis severity score of > 3 (severe) and a positive culture for Candida spp. Definition of RVVC: 4 or more episodes of Candida vaginitis in 1 year including at least 1 confirmed by microbiological culture Exclusion criteria:
Setting
Baseline characteristics
|
|
| Interventions | DermaSilk briefs (3 pairs), worn day and night for 6 months Cotton briefs (3 pairs), worn day and night for 6 months Note: Participants were given instructions on how to wash their briefs (by hand, with a mild shampoo, water 30 to 40 °C). They were also asked not to apply topical creams or vaginal pessaries, and to wash the area after defaecation (not more than twice a day) with a mild cleanser (perfume‐ and preservative‐free). |
|
| Outcomes |
Timing of measurements Assessed at: 3, 6 months Assessed if became symptomatic between planned visits: Not reported Primary outcomes
Secondary outcomes
|
|
| Funding | Alpretec, producer of DermaSilk briefs, provided equipment required to perform the study. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation and method of randomisation not described |
| Allocation concealment (selection bias) | Low risk | Sealed envelopes used. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "The study was double‐blinded". Cotton and DermaSilk underwear were of similar appearance (author correspondence). |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Severity score assessed by participant ("double blinded" as per above) and lab result, but unclear if assessor of lab report was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Withdrawal/loss to follow‐up 0% |
| Selective reporting (reporting bias) | Unclear risk | No protocol located to permit a judgement of low risk or high risk. It is likely that information about mycological recurrence would have been collected by this study, but it was not reported. |
| Other bias | Unclear risk | Underpants supplied by the manufacturer. No information on how the study was funded |
Fan 2015.
| Study characteristics | ||
| Methods | Randomised controlled trial, active control
Blinding ‐ No, open‐label Withdrawals/loss to follow‐up: 11% (37/330) Intention‐to‐treat analysis: Not mentioned |
|
| Participants | N = 330 enrolled, 293 completed Inclusion criteria: Women aged 18 to 50 years with RVVC Definition of RVVC: 4 or more episodes of proven infection in the previous 12‐month period (the presence of vulvar itching, vaginal discharge, demonstration of blastoconidia, and pseudohyphae on a wet 10% KOH (potassium hydroxide)‐treated vaginal slide and positive Candida culture) Exclusion criteria:
Setting
Baseline characteristics
|
|
| Interventions | Nystatin group ‐ Initial course consisted of 20000 units/day of nystatin vaginal suppositories (Zhonglian Pharmaceutical Co, Ltd, China) for 14 days. The maintenance course consisted of 20000 units/day of vaginal nystatin 7 days before and after menstruation. This treatment regimen was followed for 6 months. Fluconazole group – Initial course consisted of 150 mg oral fluconazole capsule (Pfizer Pharmaceuticals Ltd) on days 1, 4, and 7. The maintenance course consisted of a weekly 150 mg dose of oral fluconazole capsule for 6 months. Note: The maintenance course was initiated after the first follow‐up if microscopic examination and Candida cultures were negative. Participants agreed to either abstain from sexual intercourse or to use condoms during the treatment period and to abstain from using any other vaginal product. |
|
| Outcomes |
Timing of measurements Assessed at: 7 to 14 days post‐initial treatment, monthly for 6 months and at 9 and 12 months if clinically cured at 6 months (6 months active treatment, 6 months further follow‐up) Assessed if became symptomatic between planned visits: Yes Primary outcome
Secondary outcomes
|
|
| Funding | Shenzhen Science and Technology Grant 201201001 | |
| Notes | Participants with RVVC known to be caused by C glabrata at the admission (before Candida culture and identification) were enrolled in the nystatin group. We contacted the authors to request data that excluded these participants, but this information was not forthcoming. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Sequence generation and method of randomisation not described. Participants with RVVC known to be caused by C glabrata at the admission (before Candida culture and identification) were not randomised but were enrolled in the nystatin group. |
| Allocation concealment (selection bias) | High risk | The study was not blinded, and participants with RVVC known to be caused by C glabrata at the admission (before Candida culture and identification) were enrolled in the nystatin group. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | The study was not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is not clear if the assessors were blinded to the treatment regimen received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Withdrawals/loss to follow‐up: 11% (37/330), reasons for loss to follow‐up not specified, and no intention‐to‐treat analyses were performed |
| Selective reporting (reporting bias) | Unclear risk | No protocol located to permit a judgement of low risk or high risk. |
| Other bias | Low risk | This research was supported by a Shenzhen Science and Technology Grant 201201001. |
Fardyazar 2007.
| Study characteristics | ||
| Methods | Randomised controlled trial, active control Blinding ‐ unclear Withdrawals/loss to follow‐up: 5.6% (7/124) Intention‐to‐treat analysis: No |
|
| Participants | N = 124 enrolled, 117 completed Inclusion criteria: Women with a history of RVVC and current signs and symptoms of vulvovaginal candidiasis at the time of enrolment (pruritis, irritation, burning, discharge, erythema, oedema) Definition of RVVC: ≥ 4 episodes of symptomatic VVC each year, at least 1 diagnosed by a physician Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Fluconazole ‐ Oral, 150 mg, initial dose at enrolment, then weekly for 6 months Clotrimazole ‐ Vaginal cream 5 g daily for 7 days at enrolment, then 5 g twice weekly for 6 months |
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 12 months (6 months active treatment, 6 months further follow‐up) Assessed if became symptomatic between planned visits: Not reported Primary outcomes
Secondary outcomes
|
|
| Funding | Not reported | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “Patients were randomised systematically” |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not stated, but difference between vaginal cream and oral tablets would be obvious to participants. Without placebo tablets and cream, blinding is unlikely to be possible/maintained. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is not clear if the assessors were blinded to the type of treatment (oral fluconazole vs vaginal clotrimazole) received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Not an intention‐to‐treat analysis, but loss to follow‐up/withdrawals small (5.6%) and similar across groups. |
| Selective reporting (reporting bias) | Unclear risk | No protocol located to permit a judgement of low risk or high risk. |
| Other bias | High risk | Participants were excluded from the analysis for non‐compliance. (“Patients had to discontinue [if they] missed two or more consecutive doses of the drug or had irregular control visits”). Groups balanced at baseline for reported criteria, but no figure provided for number of episodes in the previous 12 months. |
Fong 1992a.
| Study characteristics | ||
| Methods | Randomised active controlled, open‐label trial Blinding ‐ No, open‐label Withdrawals/loss to follow‐up: 14% (6/44) Intention‐to‐treat analysis: Yes |
|
| Participants | N = 44 enrolled, 38 completed study Inclusion criteria: Recurrent, clinical symptomatic vaginal candidiasis, presenting with an acute episode Definition of RVVC: Clinical symptomatic vaginal candidiasis; defined as greater than 4 episodes (proven by culture) in the past year Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Itraconazole ‐ 200 mg orally daily (administered as 100 mg twice daily with meals) for 5 days, then 200 mg twice weekly for 6 months Clotrimazole ‐ 200 mg, intravaginally daily for 5 days, then 200 mg twice weekly for 6 months |
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 12 months (6 months active treatment, 6 months follow‐up) Assessed if became symptomatic between planned visits: Not reported Primary outcomes
Secondary outcomes
|
|
| Funding | Janssen Pharmaceutica Inc, Canada | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The random numbers were computer generated. |
| Allocation concealment (selection bias) | Low risk | Numbered, sealed envelopes containing the therapeutic regimen were kept in the Pharmacy Department, ensuring that the investigator remained blinded to the randomisation. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Study is open‐label. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome assessment uses culture and clinical symptoms; participants not blinded, lab assessment not described. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Withdrawals/loss to follow‐up: 14% (6/44). 5 participants dropped out in the clotrimazole group (2 non‐compliance, 3 lost to follow‐up), compared to 1 in the itraconazole group (desired to be pregnant). Both per‐protocol and intention‐to‐treat analysis conducted. |
| Selective reporting (reporting bias) | Unclear risk | No protocol located. |
| Other bias | Unclear risk | Funded by Janssen Pharmaceuticals |
Fong 1992b.
| Study characteristics | ||
| Methods | Randomised controlled trial, no treatment as control Single‐blind Withdrawal/loss to follow‐up: 7% (4/58) |
|
| Participants | N = 58 enrolled, 54 completed study Inclusion criteria: Women with RVVC and their male sexual partners, who were in stable, monogamous relationships Definition of RVVC: 4 or more episodes of candidiasis (proven by culture) in the year preceding the study Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Ketoconazole ‐ 200 mg daily for 5 days for male partners treated at enrolment No treatment |
|
| Outcomes |
Timing of measurements Assessed: Monthly for 12 months (5 days active treatment, then 12 months of follow‐up) Assessed if became symptomatic between planned visits: Yes Primary outcomes
Secondary outcomes
|
|
| Funding | Janssen Pharmaceuticals, Canada | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method unclear |
| Allocation concealment (selection bias) | High risk | "Numbered envelopes contained the specific regimens". As the envelopes contained the treatment or no tablets, it is likely that the allocation may not have been concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | "Single blind" study, assumed that the partners who received the treatment were blinded, but treating doctors were not. No treatment as comparator. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcome assessed by lab culture plus clinical symptoms; not specifically stated that assessors were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Withdrawal/loss to follow‐up: 7% (4/58). In the treated group, 2 participants dropped out of the study due to lack of interest. In the untreated group, 1 participant was removed from the study due to an adverse reaction and 1 dropped out due to disinterest. |
| Selective reporting (reporting bias) | Unclear risk | No protocol located to permit a judgement of low risk or high risk. |
| Other bias | Unclear risk | Funded by Janssen Pharmaceuticals |
Fong 1994.
| Study characteristics | ||
| Methods | Randomised controlled trial, active control ‐ cross‐over design Unblinded ‐ open trial Withdrawal/loss to follow‐up: 0% (0/23) |
|
| Participants | N = 23 enrolled, 23 completed study Inclusion criteria: Women with RVVC Definition of RVVC: Greater than four episodes of clinical symptomatic vaginal candidiasis (microbiologically proven) in the past year. Exclusion criteria: ‐ Diabetes mellitus‐ Chronic illnesses‐ History of chronic use of antibiotics or steroids Setting ‐ Country: Canada Baseline characteristics ‐ Age: 33.0 years (SD 7.4) ‐ Mean episodes of vulvovaginal candidiasis in previous 12 months: 7.5 (range 5‐12) |
|
| Interventions | Clotrimazole 500 mg vaginal ovules perimenstrually (once a month prophylactically), plus for symptomatic episodes in between. Patients with a history of recurrent symptoms before the menses were advised to insert the ovule 5‐7 days before the expected menses. For patients with symptoms usually occurring after the menses, the ovule was inserted the last day of the period. Empiric self‐treatment with single doses of clotrimazole 500 mg ovules at onset of vaginitis symptoms. Total duration of treatment was 6 months. |
|
| Outcomes |
Timing of measurements Assessed: initially, and then every 2 months for 12 months Assessed if became symptomatic between planned visits: No Primary outcomes Number of clinical recurrences per participant per year: only reports "number of symptomatic episodes of vaginitis over 6 month period": 50 symptomatic periods in the prophylactic group (mean 2.2 ± 1.8) versus 86 episodes in the empiric self‐treatment group (mean 3.1 ± 2.9) No data available to calculate recurrences per patient Proportion of women with clinical recurrence: Not reported Adverse events: Not reported Secondary outcomes Time to first recurrence: Not reported Number of symptomatic days per year: Not reported Number of mycological recurrences per participant per year: Not reported Proportion of participants with at least one mycological recurrence during the treatment and follow‐up period: Not reported Duration of symptoms after treatment initiation: Not reported Patient preference: 17 (73.9%) preferred the empiric self‐treatment approach, 4 (17.4%) preferred the prophylactic approach and 2 (8.7%) had no personal preference, p < 0.05 (note in table p‐value is reported as 0.001). |
|
| Funding | Not stated | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The random numbers were computer generated." |
| Allocation concealment (selection bias) | Unclear risk | "Numbered, sealed envelopes containing the therapeutic regimen, ensuring that the investigator remained blinded to the randomisation", but no comment as to whether envelopes were opaque |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open study |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is not clear if the assessors were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Outcome data for all 23 participants is reported |
| Selective reporting (reporting bias) | Unclear risk | No protocol located to permit judgement of low risk or high risk. |
| Other bias | Unclear risk | No information on how the study was funded. |
Kumari 2011.
| Study characteristics | ||
| Methods | Randomised controlled trial Blinding ‐ not stated Withdrawals/loss to follow‐up: 10% (8/82) Intention‐to‐treat analysis: Unclear ‐ “Only patients adhering to the protocol were analysed for efficacy; patients lost to follow‐up or non‐compliant with the treatment regimen were excluded from analysis". Later in text stated that "patients lost to follow‐up or who had recurrences due to non‐compliance were assessed as failures" (p547). |
|
| Participants | N = 109 eligible, 82 enrolled, 76 analysed (the text describes 4 dropouts/exclusions per group, but the analysis describes 38 participants per group, which would equate to 3 dropouts/exclusions per group) Inclusion criteria: Women with overall general good health, presenting to the gynaecology outpatient clinic with abnormal vaginal discharge (confirmed on speculum examination) and with a history of at least 4 proven episodes of VVC in the prior 12 months Definition of RVVC: 4 proven cases of VVC in past 12 months Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Polygodyal/anethole phytocompound (K‐712) ‐ the 100 mg composition is: 10 mg of oleoresin from Pseudowintera colorata at 30% concentration in polygodyal together with trace amounts of Olea europea. Assumed to be oral and self‐administered. 1 tablet twice a day for 4 weeks and then for the first 2 weeks each month for a total of 6 months. Itraconazole ‐ 100 mg twice daily with meals for 4 days, then 200 mg once weekly for 6 months |
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 6 months, then at 9 and 12 months (6 months active treatment, 6 months further follow‐up) Assessed if became symptomatic between planned visits: Not reported Primary outcomes
Secondary outcomes
|
|
| Funding | Not stated | |
| Notes | Author contacted, not able to provide data in format suitable for this review. Polygodyal/anethole phytocompound (K‐712) was supplied by Canova Foundation, Lesmo, Italy. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Random numbers were computer generated" |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding is not referred to in the trial publication. Given the different dosing regimens, it is unlikely that blinding occurred or was preserved. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is not clear if the assessors were blinded to the type of treatment received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | It is unclear why 82 participants were randomised from 109 eligible participants. Dropouts and exclusions are described, but these do not align with the figures provided (e.g. the text describes 4 per arm of the trial but figures reported show 3 per arm). |
| Selective reporting (reporting bias) | High risk | Outcome measures are not described in detail, such that it is unclear what was being measured and reported as a primary outcome measure and in the graphical representations of data. A protocol was not published prior to reporting of the outcomes. |
| Other bias | Unclear risk | Role of industry funding is not clear. |
Li 2018.
| Study characteristics | ||
| Methods | Randomised controlled trial Withdrawals/loss to follow‐up: not reported Intention‐to‐treat analysis: Not reported |
|
| Participants | N = 68 Inclusion criteria:
Definition of RVVC: Mycologically confirmed symptomatic vulvovaginal candidiasis (VVC) 4 times or more within 1 year Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions |
Intervention group
Control group
|
|
| Outcomes |
Timing of measurements: 1 month, 3 months, and 6 months after all courses of treatment Primary outcomes
Secondary outcomes: Not reported |
|
| Funding | Not reported | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Sequence generation and method of randomisation not described |
| Allocation concealment (selection bias) | High risk | Allocation concealment not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | The study was not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is not clear if the assessors were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Withdrawal was not reported but “patients who could adhere to the therapeutic regimen and follow‐up on time” was an inclusion criterion. |
| Selective reporting (reporting bias) | Unclear risk | No protocol located to permit judgement of low risk or high risk. |
| Other bias | Low risk | No grant was received for this study; authors declare no conflict of interest. |
Lopez‐Olmos 2000.
| Study characteristics | ||
| Methods | Randomised controlled trial, active controlled (3 treatment arms) Blinding unclear Withdrawals/loss to follow‐up: 8% (4/49) ‐ 4 women were excluded at some stage (but may have been before or after randomisation) Intention‐to‐treat analysis: No |
|
| Participants | N = 45 randomised, 4 women were excluded at some stage (but may have been before or after randomisation) Inclusion criteria: Women with RVVC presenting to gynaecology or family planning clinic Definition of RVVC: 4 or more episodes of infection per year Exclusion criteria: Not reported Setting
Baseline characteristics
|
|
| Interventions | Fluconazole ‐ 150 mg, orally on sixth day of the menstrual cycle for 6 months Clotrimazole ‐ 1 tablet of 500 mg vaginally on sixth day of the menstrual cycle for 6 months Itraconazole ‐ 2 tablets of 100 mg orally on sixth day of the menstrual cycle for 6 months |
|
| Outcomes |
Timing of measurements Assessed at: 6 and 12 months. Symptomatic women were treated as per usual practice between visits (6 months active treatment, 6 months further follow‐up). Assessed if became symptomatic between planned visits: Not reported Primary outcomes
Secondary outcomes
|
|
| Funding | Not reported | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly distributed", but specific evidence not provided |
| Allocation concealment (selection bias) | High risk | Allocated to groups according to which day of the week they were seen in a family planning clinic |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Allocated to groups according to which day of the week they were seen in a family planning clinic |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is not clear if the assessors were blinded to the type of treatment received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Withdrawals/loss to follow‐up: 8%. Not intention‐to‐treat analysis |
| Selective reporting (reporting bias) | Unclear risk | No protocol publication located. |
| Other bias | Unclear risk | Funding not reported |
Mendling 2011.
| Study characteristics | ||
| Methods | Randomised controlled trial, not placebo controlled Blinding ‐ No Withdrawals/loss to follow‐up: 24% (22/90) Intention‐to‐treat analysis: Yes |
|
| Participants | N = 90 randomised, divided into 3 groups Withdrawals: 5 participants in vaccine group, 8 in heliotherapy group, 9 in ciclopirox olamine group excluded due to withdrawal (total 22) Inclusion criteria: Women with RVVC presenting to a gynaecology or family planning clinic in Berlin, Germany Definition of RVVC: More than 4 episodes of infection per year; diagnosis confirmed by a positive culture at time of inclusion or (if not a current acute infection) a positive culture within previous 3 months Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions |
Lactobacillus vaccination ‐ 7 x 109 inactivated lactobacilli of 8 species, administered 3 times intramuscular (IM) every 2 weeks Heliotherapy ‐ according to skin type with sub‐erythematous doses of ultraviolet A and B rays, administered 3 times per week for 6 weeks Ciclopyroxilamine ‐ 100 mg vaginal tablets daily for 6 days |
|
| Outcomes |
Timing of measurements Assessed at baseline, 6 to 12 weeks later, and 1 year later Assessed if became symptomatic between planned visits: Yes (but not clearly mentioned in methods section; in case of recurrence during the study women received 150 mg fluconazole) Also questionnaire developed by researchers assessing sexuality, partner relationship, doctor‐patient relationship, and use of antimycotics Primary outcomes
Secondary outcomes
|
|
| Funding | Dr Kern GmbH provided the heliotherapy equipment and funding for laboratory tests and statistical analysis (the latter performed at the Institute of Natural Medicine). Strathmann GmbH provided the vaccine. Taurus Pharma provided the ciclopirox olamine vaginal capsules. Pfizer Pharma provided the fluconazole capsules. |
|
| Notes | Publication in German | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | The title suggests the study is randomised, but the method of sequence generation is not described anywhere in the paper. |
| Allocation concealment (selection bias) | High risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | The study is not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Primary outcome includes symptoms as well as lab tests; participants were not blinded and it is not clear if the assessors of lab tests were blinded to the type of treatment received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 22 of 90 randomised participants withdrew before completion of the study at 1‐year follow‐up. The authors performed intention‐to‐treat (ITT) analysis to take this into account. |
| Selective reporting (reporting bias) | Unclear risk | All outcomes in methods section are reported. However, a protocol was not published prior to reporting of the outcomes. |
| Other bias | Unclear risk | Industry funding, but the role of industry is not clear. The first author reports receiving honoraria for presentations from Strathmann and Taurus Pharma. The second author does not have any interests to declare. |
Metts 2003.
| Study characteristics | ||
| Methods | Randomised controlled trial, placebo controlled Blinding ‐ Double‐blind Withdrawals/loss to follow‐up: 74% (25/34) Intention‐to‐treat: Yes ‐ modified (only included women who returned for initial follow‐up visit) |
|
| Participants | N = 34 enrolled, 27 returned for initial follow‐up visit; 9 completed study Inclusion criteria: Undergraduate and graduate female students with RVVC who had been free of symptoms for 1 month Definition of RVVC: a total of 4 or more candidal vulvovaginal infections in the past 12 months, with at least 2 documented by a medical provider Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | (A) Lactobacillus acidophilus NAS strain vaginal tablet 3 times weekly and placebo oral tablet daily (B) Lactobacillus acidophilus NAS strain vaginal tablet 3 times weekly and probiotic oral tablet daily (C) Placebo vaginal 3 times weekly and oral tablet daily |
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 6 months and when symptoms of vaginitis occurred Assessed if became symptomatic between planned visits: Yes Primary outcomes
Secondary outcomes
|
|
| Funding | Grant from American Academy of Family Physicians Foundation Probiotic strains were provided by Natren Inc, Westlake Village, CA, USA. |
|
| Notes | Data to calculate clinical recurrence rate were collected, but not presented in a format that permitted data extraction. Authors contacted but additional information not forthcoming. Not included in meta‐analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomised using a random number generator" |
| Allocation concealment (selection bias) | Low risk | "Participants and health care providers (investigators/assessors) were blinded and unaware of allocation." |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Participants and health care providers (investigators/assessors) were blinded and unaware of allocation. At the participating pharmacy, women collected the probiotics/control in identical opaque paper bags identified by the randomised number. The paper bags contained capsules and brown bottles identical in appearance." |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | "Participants and health care providers (investigators/assessors) were blinded and unaware of allocation". No further methods to ensure blinding of outcome assessors were discussed. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Withdrawals/loss to follow‐up: 74% modified intention‐to‐treat analysis. "Thirty‐four of the 43 women who met the inclusion criteria were entered into the study.... Seven women did not return for any follow‐up visits. Thus, 27 women participated in total, for an average 3.3 months and nine women completed the 6‐month program" |
| Selective reporting (reporting bias) | Unclear risk | No protocol was available. |
| Other bias | Low risk | Grant from American Academy of Family Physicians Foundation Probiotic strains were provided by Natren Inc, Westlake Village, CA, USA. |
Roth 1990.
| Study characteristics | ||
| Methods | Randomised controlled trial, placebo control ‐ randomisation stratified according to frequency of VVC (4 to 5, 6+ episodes per year) Blinding ‐ Triple (participant, clinician, and mycologist) Withdrawals/loss to follow‐up: 3% (2/64) Intention‐to‐treat analysis: Per‐protocol analysis presented in paper. |
|
| Participants | N = 64 enrolled, 62 completed study Inclusion criteria
Definition of RVVC: At least 4 episodes of vulvovaginal candidiasis in the past 12 months Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Clotrimazole ‐ 500 mg vaginally, 1 week after menstruation given by doctor, for 6 months Placebo ‐ vaginally, 1 week after menstruation given by doctor, for 6 months |
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 6 months, then at 9 and 12 months (6 months active treatment, 6 months further follow‐up) Assessed if became symptomatic between planned visits: Yes Primary outcomes
Secondary outcomes
|
|
| Funding | Not reported | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described. Stratified according to frequency of recurrence (4 to 6, 6+ episodes in preceding 12 months) |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "The active and placebo vaginal tablets were indistinguishable. The containers were pre‐packed and randomised so that neither the clinician, mycologist, nor the patient knew which treatment was being given." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "The active and placebo vaginal tablets were indistinguishable. The containers were pre‐packed and randomised so that neither the clinician, mycologist, nor the patient knew which treatment was being given." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Withdrawals/loss to follow‐up: 3%. Dropouts ‐ 1 due to pregnancy, 1 due to recurrence of symptoms before treatment commenced |
| Selective reporting (reporting bias) | Unclear risk | No protocol was available for assessment. |
| Other bias | Unclear risk | Funding not reported |
Sobel 1985a.
| Study characteristics | ||
| Methods | Randomised controlled trial, no treatment control Blinding ‐ Open‐label Withdrawals/loss to follow‐up: 9%. Unclear ‐ 1 participant dropped out in first month, outcome data appear to be available for 37/40 participants Intention‐to‐treat analysis: Unclear |
|
| Participants | N = 40 enrolled, 37 completed study Inclusion criteria: Male partners of women with RVVC and an acute episode of candidal vaginitis Definition of RVVC: "Presence of at least four documented episodes of candidal vaginitis in the 12‐month period preceding entry into the study" Exclusion criteria: Related to women rather than to male partners
Setting
Baseline characteristics
|
|
| Interventions | Treated male partners ‐ 1% topical cream, applied to genitalia (shaft of penis, glans, under foreskin, and to the coronal sulcus) once daily for 1 week Untreated male partners ‐ no intervention Note: All women received oral ketoconazole 400 mg per day for 14 days and then ketoconazole 400 mg with onset of menses for 5 days, for 3 menstrual cycles. |
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 6 months, 9 months, and 12 months (1 week active treatment, 12 months further follow‐up) Assessed if became symptomatic between planned visits: Yes ‐ within 48 hours of any symptoms developing Primary outcomes
Secondary outcomes
|
|
| Funding | Not reported | |
| Notes | Data to calculate clinical recurrence rate were collected but were not presented in a numerical format in the publication. Numbers from Figure 2 assuming that number randomised to each group was 20. Authors contacted but additional information not forthcoming. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation not stated. "Patients were randomly divided into two additional groups" |
| Allocation concealment (selection bias) | High risk | Open‐label study |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open‐label study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome is based on symptoms only (participants not blinded). |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Withdrawals/loss to follow‐up: Unclear ‐ 1 participant dropped out in first month, outcome data appear to be available for 37/40 participants. |
| Selective reporting (reporting bias) | Unclear risk | No protocol was available for assessment. |
| Other bias | Unclear risk | Funding not reported |
Sobel 1986.
| Study characteristics | ||
| Methods | Randomised controlled trial, placebo controlled Blinding ‐ Unclear Withdrawals/loss to follow‐up: 15% (11/74); reasons for dropouts ‐ 1 pregnancy, 1 trying for pregnancy, 2 adverse effects, 7 logistical reasons Intention‐to‐treat analysis: No ‐ per‐protocol analysis presented in paper |
|
| Participants | N = 74 enrolled, 63 completed study Inclusion criteria
Definition of RVVC: At least 4 documented episodes of Candida vaginitis in 12‐month period Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Ketoconazole ‐ 400 mg daily for 5 days with onset of menses for 6 cycles Ketoconazole ‐ 100 mg daily for 5 months Placebo ‐ daily for 6 months or until clinical recurrence occurs |
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 12 months (~6 months active treatment, followed by ~6 months of follow‐up) Assessed if became symptomatic between planned visits: Yes, within 48 hours of symptoms developing Primary outcomes
Secondary outcomes
|
|
| Funding | "Supported by Janssen Pharmaceutica" | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described. "...were randomly assigned to receive..." |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Placebo used, but blinding not described. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcome includes symptoms and lab tests. It is not clear if the assessors of lab tests were blinded to the type of treatment received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Withdrawals/loss to follow‐up: 15%. Reasons for withdrawal ‐ 1 pregnancy, 1 trying for pregnancy, 2 adverse effects, 7 logistical reasons. All dropouts accounted for, but it is unclear in which groups they occurred. No intention‐to‐treat analysis presented in paper. |
| Selective reporting (reporting bias) | Unclear risk | No protocol was available for assessment. |
| Other bias | Unclear risk | Industry funding |
Sobel 1989.
| Study characteristics | ||
| Methods | Randomised controlled trial, placebo control Blinding ‐ Double‐blind Withdrawals/loss to follow‐up: 36% (15/42) Intention‐to‐treat analysis: No |
|
| Participants | N = 42 enrolled and randomised, 27 completed study Inclusion criteria: 4+ documented episodes of Candida vaginitis in the 12 months preceding the study, presenting with an acute episode of vaginitis Definition of RVVC: At least 4 documented episodes of candidal vaginitis in a 12‐month period Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Clotrimazole ‐ single dose, 500 mg immediately after menses for 6 months Placebo ‐ single dose, 500 mg immediately after menses for 6 months |
|
| Outcomes |
Timing of measurements Assessed at: Monthly intervals for 6 months, then at 9 and 12 months (6 months active treatment, 6 months further follow‐up) Assessed if became symptomatic between planned visits: Yes Primary outcomes
Secondary outcomes
|
|
| Funding | Miles Pharmaceuticals | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomised", but method not clearly described. |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not clearly described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Double blind manner". Used placebo |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is not clear if the assessors were blinded to the type of treatment received by the participants |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Withdrawals/loss to follow‐up: 36%. Per‐protocol analysis presented in paper. Description of outcome (symptomatic recurrence) unclear in text. Author contacted, but no reply received. |
| Selective reporting (reporting bias) | Unclear risk | Unable to locate a protocol for this study |
| Other bias | Unclear risk | Industry funding |
Sobel 2004.
| Study characteristics | ||
| Methods | Randomised controlled trial, placebo control Blinding ‐ Double‐blind Withdrawals/loss to follow‐up: 3.6% (14/387) ‐ 4 dropouts, 3 loss to follow‐up, 7 withdrawn due to protocol violations Intention‐to‐treat analysis: Modified – “modified intention‐to‐treat population included all patients who had been randomly assigned to receive at least one dose of the study medication” |
|
| Participants | N = 387 randomised, 373 included in the modified ITT analysis, 343 included in efficacy analysis (defined at each visit, included all women who met the criteria for inclusion, had not missed 2 or more consecutive doses of the study drug before the visit, had not taken any prohibited medication, and who underwent clinical and mycologic evaluations within the appropriate time frame) Inclusion criteria: 18 years old + with RVVC and an episode of active VVC (severity score ≥3) Definition of RVVC: at least 4 documented episodes of Candida vaginitis in the previous 12 months Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Fluconazole ‐ Oral, 150 mg, weekly, 6 months Placebo ‐ Oral, weekly, 6 months |
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 6 months, then at 9 and 12 months (6 months active treatment, 6 months follow‐up) Assessed if became symptomatic between planned visits: Not reported Primary outcomes
Secondary outcomes
|
|
| Funding | Pfizer | |
| Notes | Obtained from institutional review boards from all participating centres | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Participants were randomly assigned. No description of method of randomisation. "Patients were randomly assigned on the basis of a 1:1 ratio" |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment was not described. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Double‐blind. Unclear if this included clinicians and laboratory staff. "...the study medication (administered in a double‐blind manner)" |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcomes include symptoms and lab tests. It is not clear if the assessors of lab tests were blinded to the type of treatment received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Withdrawals/loss to follow‐up: 3.6% (14/387) ‐ 4 dropouts, 3 loss to follow‐up, 7 withdrawn due to protocol violations. Analysis presented as a "modified ITT design”, i.e. women who received at least 1 dose of medication and underwent at least 1 evaluation (n = 373) and a per‐protocol analysis (n = 343). |
| Selective reporting (reporting bias) | Unclear risk | Data not reported for the modified ITT analysis, only for the per‐protocol analysis. "The results were similar in a modified intention‐to‐treat analysis (data not shown)." |
| Other bias | High risk | Funded by pharmaceutical company. "About halfway through the enrolment period (before the data were analysed), the sponsor decided to combine the parallel trials into a single trial." |
Spacek 2005.
| Study characteristics | ||
| Methods | Randomised controlled trial, short duration versus long duration of the same treatment
Blinding – Not described Withdrawals/loss to follow‐up: Not clearly described, but likely that 1 participant was lost to follow‐up, 4% (1/26) Intention‐to‐treat analysis: Not described |
|
| Participants | N = 26 participants with RVVC enrolled, 26 completed. Trial also enrolled 34 participants with acute RVVC. Inclusion criteria: Diagnosis of RVVC confirmed by a positive culture at enrolment. All participants with RVVC had the primary idiopathic form with no known causes. Definition of RVVC: a history of 4 or more culture‐documented attacks within the last year (or at least 3 episodes unrelated to antibiotic therapy) Exclusion criteria
Setting
Baseline characteristics (participants with RVVC only)
|
|
| Interventions | 1‐day regimen ‐ itraconazole (oral), 400 mg total, divided into 2 doses of 200 mg on the same day 3‐day regimen ‐ itraconazole (oral), 600 mg total, divided into 3 doses of 200 mg on 3 consecutive days |
|
| Outcomes |
Timing of measurements Assessed at: 14 days, 1 month, 3 months, and 6 months (mentioned in results not in methods) (1‐ or 3‐day active treatment, followed by 6 months of follow‐up) Assessed if became symptomatic between planned visits: Not reported Primary outcome
Secondary outcomes
|
|
| Funding | The study was supported by the research project IGA No. 3694‐3 of the Czech Ministry of Health. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Sequence generation and method of randomisation not described |
| Allocation concealment (selection bias) | Unclear risk | Allocation concealment not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Given the nature of the treatment (1 vs 3 days) and absence of a double‐dummy design, blinding of participants was not possible. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | It is not clear if the assessors were blinded to the treatment regimen (1‐ vs 3‐day itraconazole course) received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Withdrawals/loss to follow‐up: not clearly described |
| Selective reporting (reporting bias) | Unclear risk | No protocol located to permit a judgement of low risk or high risk. |
| Other bias | Low risk | The study was supported by the research project IGA No. 3694‐3 of the Czech Ministry of Health. |
Spinillo 1997.
| Study characteristics | ||
| Methods | Randomised controlled trial, no‐treatment control Blinding ‐ Participants not blinded, both nurses and physicians were "unaware of the study", microbiology staff ‐ unclear Withdrawals/loss to follow‐up: 7% (8/114) Intention‐to‐treat analysis: Per‐protocol analysis presented in paper |
|
| Participants | N = 114 enrolled, 106 completed study Inclusion criteria: Patients with 4+ documented episodes of vulvovaginal candidiasis, presenting with an acute episode of vaginitis Definition of RVVC: At least 4 documented episodes (positive vaginal culture) of symptomatic vulvovaginal candidiasis in the 12 months preceding enrolment Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions | Itraconazole ‐ 400 mg monthly (200 mg, 12 hours apart), during fourth or fifth day of menstrual cycle for 6 months No‐treatment control |
|
| Outcomes |
Timing of measurements Assessed at: 3, 6, and 12 months (6 months active treatment, 6 months further follow‐up) Assessed if became symptomatic between planned visits: Yes ("If symptom developed between visits, patients were examined within 48 hours.") Primary outcomes
Secondary outcomes
|
|
| Funding | Not reported | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Random numbers generated by a personal computer" |
| Allocation concealment (selection bias) | Unclear risk | "Sealed envelope method", but no comment as to whether envelopes were opaque |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | "Both nurses and physicians who carried out the visits were unaware of the study being performed." However, women were not blinded as there was a 'no treatment' arm of the trial rather than a placebo. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome includes symptoms and lab tests. It is not clear if the assessors of lab tests were blinded to the type of treatment received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Withdrawals/loss to follow‐up: 7% (8/114) Intention‐to‐treat analysis: Per‐protocol analysis presented in paper |
| Selective reporting (reporting bias) | Unclear risk | No protocol was available for assessment. |
| Other bias | Unclear risk | Funding not reported |
Witt 2009.
| Study characteristics | ||
| Methods | Randomised controlled trial, placebo control Blinding ‐ No, open‐label Withdrawals/loss to follow‐up: 53% (79/150) Intention‐to‐treat analysis: No |
|
| Participants | N = 150 enrolled and randomised, 71 completed study Inclusion criteria: 4+ documented episodes of Candida vaginitis in the 12 months preceding the study, presenting with an acute episode of vaginitis Definition of RVVC: At least 4 documented episodes of candidal vaginitis in a 12‐month period Exclusion criteria
Setting
Baseline characteristics
|
|
| Interventions |
|
|
| Outcomes |
Timing of measurements Assessed at: Monthly for 12 months Assessed if became symptomatic between planned visits: Yes ("If symptom developed between visits, patients were examined within 48 hours.") Primary outcomes
Secondary outcomes
|
|
| Funding | Not reported | |
| Notes | Author contacted, not able to provide data in format suitable for this review. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Use of a computerised randomisation list |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcome includes symptoms and lab tests. Participants were not blinded, and it is not clear if the assessors of lab tests were blinded to the type of treatment received by the participants. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 79 women (53%) did not complete the study, Almost half of the participants (49%) were lost to follow‐up. Loss to follow‐up similar across groups (25 itraconazole group, 25 itraconazole + lactobacilli group, 23 classic homeopathy group). Per‐protocol analysis only presented. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol available for assessment. |
| Other bias | High risk | No details provided regarding similarity of groups at baseline. Itraconazole groups treated for 6 months, classical homeopathy group treated for 12 months. Funding not reported. |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Avijgan 2012 | Diagnostic criteria for recurrent vulvovaginal candidiasis (RVVC) did not meet inclusion criteria ‐ RVVC defined as 3 or more attacks of vulvovaginal candidiasis (VVC) in 12 months. |
| Azima 2018 | Diagnostic criteria for RVVC did not meet inclusion criteria (number of previous episodes not documented). |
| Bartz 2000 | Diagnostic criteria for RVVC did not meet inclusion criteria ("two or more episodes of clinician‐identified vaginitis in a 6 month timeframe"). |
| Brand 2018 | Diagnostic criteria for RVVC did not meet inclusion criteria ("Subject eligibility required a documented history of RVVC (defined as three episodes of acute VVC in the past 12 months, which included the episode at the screening visit"). |
| Bushell 1988a | Diagnostic criteria for RVVC did not meet inclusion criteria ("at least three documented episodes of vaginal candidosis"). |
| Bushell 1998b | Publication very brief. Diagnostic criteria for RVVC not provided. Unclear if this is a randomised study |
| Coric 2006 | Additional information requested from author but not received. |
| Davidson 1978 | Diagnostic criteria for RVVC did not meet inclusion criteria ("a history of recurrent 'thrush' for at least one year treated elsewhere each time with anti‐fungal therapy, and confirmed where possible, or had had at least three proved treated clinical attacks of candidosis in the previous six months in the clinic"). |
| Diba 2010 | Additional information requested from author but not received. |
| Donders 2008 | Not a randomised controlled trial |
| Edwards 2018 | Diagnostic criteria for RVVC did not meet inclusion criteria ("at least two episodes of vaginitis during the12 months prior to the current episode"). |
| Fan 2005 | Unable to separate findings for participants who had recurrent vulvovaginal candidiasis from those who just had acute candidiasis. Authors contacted but no additional information provided. |
| Fong 1993 | Not an original randomised controlled trial (RCT). This study uses data of previously published randomised trials to study in vitro resistance of Candida albicans to the imidazoles. |
| Golero 1993 | Diagnostic criteria for RVVC did not meet inclusion criteria ("patients with chronic vaginal candidosis, unresponsive to previous topical antimycotic treatments, were included in this study"). |
| Hilton 1992 | Not reported as an RCT ‐ after 8 months trial stopped randomising participants to different arms. The data reported in the publication include participants enrolled both before and after this change in protocol. Author contacted but no additional information provided. |
| Houang 1989 | Inadequate information in publication to extract data. Author contacted but no additional information provided. |
| Miller 1984 | Unable to separate findings for participants who had recurrent vulvovaginal candidiasis from those who just had acute candidiasis. Authors contacted but no additional information provided. |
| Rashid 1991 | Not a randomised controlled trial |
| Shalev 1996 | Unable to separate findings for participants who had recurrent vulvovaginal candidiasis from those who just had acute candidiasis. Authors contacted but no additional information provided. |
| Silverman 1971 | Diagnostic criteria for RVVC did not meet inclusion criteria ("recent (two years) history of two or more attacks of candidal vaginitis"). |
| Sobel 1994 | Diagnostic criteria for RVVC did not meet inclusion criteria ("three or more episodes of acute candidal vaginitis in the 12 months prior"). |
| Sobel 2001 | Diagnostic criteria for RVVC did not meet inclusion criteria ("three or more episodes of acute candidal vaginitis in the 12 months prior"). |
| Vladareanu 2018 | Follow‐up for less than 6 months (90 days) |
| Yang 2000 | Diagnostic criteria for RVVC did not meet inclusion criteria ("three or more episodes of acute candidal vaginitis in the 12 months prior"). |
Characteristics of studies awaiting classification [ordered by study ID]
ACTRN12614001258640.
| Methods | Interventional study |
| Participants | Inclusion criteria:
|
| Interventions | Fluconazole ‐ 50 mg orally daily for 12 weeks Fluconazole ‐ 150 mg orally weekly for 12 weeks |
| Outcomes | Presence of chronic vulvovaginal candidiasis symptoms at 6 weeks, 12 weeks, and 12 months |
| Notes | In trial database record, diagnostic criteria for this study do not clearly require pathological confirmation of diagnosis and may not meet the inclusion criteria for this review (4+ episodes of vulvovaginal candidiasis (VVC) within the past 12 months). Trial database record states that the trial was "stopped early" after having recruited 75 participants (target sample size 200 participants). We emailed the primary contact but have received no reply. |
ChiCTR‐IPR‐15006314.
| Methods | Interventional study ‐ randomised parallel controlled trial |
| Participants | Inclusion criteria:
|
| Interventions | "JUC Spray Dressing" Miconazole nitrate |
| Outcomes | Symptoms and signs Fungal microscopy |
| Notes | Unlikely to meet inclusion criteria for this review as may only be enrolling participants with acute VVC. Trial database record states that the trial is still recruiting, but the last update of the database record was on 27 April 2015. We emailed the primary contact but have received no reply. |
ChiCTR‐TRC‐10000833.
| Methods | Interventional study ‐ randomised parallel controlled trial |
| Participants | Inclusion criteria:
|
| Interventions | XiangLian suppositories Miconazole nitrate suppositories |
| Outcomes |
|
| Notes | Trial database record states that recruitment has been completed. We emailed the primary contact but have received no reply. |
EUCTR2010‐021502‐38‐DE.
| Methods | Interventional ‐ randomised controlled trial |
| Participants | Patients with histologically/cytologically confirmed cervical intraepithelial neoplasia grade 1 or higher Patients with chronic, recurrent vaginal candidiasis with at least 4 infection episodes in the last year and microbiologically confirmed candidal infection at inclusion in the study |
| Interventions | 4 phenyl‐butyrate prolonged release tablet |
| Outcomes | Measurement of vaginal interleukins Assessment of vaginal candidiasis |
| Notes | Database entry in German. Trial status in database is "prematurely ended". It is not clear why this occurred, nor is it clear if enrolment of participants had commenced when the study was ceased. No contact details for primary investigator included in record. |
EUCTR2011‐004718‐40‐IT.
| Methods | Interventional ‐ randomised trial. Record states that study was randomised, but not controlled. |
| Participants | Participants were women with vaginal infections by Candida albicans and non‐albicans Candida spp relapsing recurrent (≥ 4 events/year) in the acute phase of the disease. |
| Interventions | Clotrimazole and metronidazole |
| Outcomes | Reduction in recurrence |
| Notes | The trial database stated the recruitment status of this trial is ongoing. The record in the database was created on 8 March 2012. However, the email address of the primary contact was not current and no further details could be located. |
EUCTR2013‐002480‐26‐PL.
| Methods | Interventional ‐ randomised placebo‐controlled trial |
| Participants | Patients with recurrent vulvovaginal candidiasis, defined by the existence of at least 4 episodes of VVC during the previous year including the episode that was the subject of the screening visit (in addition to the current episode, at least 1 episode that occurred in the previous 2 years should also be documented by mycological examination) |
| Interventions | Lcr Regenerans Placebo |
| Outcomes |
|
| Notes | Trial database record states that the trial concluded on 22 February 2017. No publication has been located. We emailed the primary contact but have received no reply. |
NCT00479947.
| Methods | Interventional ‐ randomised, placebo‐controlled trial |
| Participants | Premenopausal women suffering from acute or chronic yeast vaginitis and a history of 3 or 4 episodes over the past 12 months were eligible to participate. |
| Interventions | 1 oral dose of fluconazole + capsules of Lactobacillus rhamnosus GR‐1 and L reuteri RC‐14 containing 5000 million live organisms for 3 months 1 oral dose of fluconazole + oral placebo capsules for 3 months |
| Outcomes | Vaginal symptoms and swabs It is not clear if the outcomes were collected for 3 months or 6 months (active treatment for 3 months, plus a further 3 months follow‐up). |
| Notes | The trial database states the recruitment status of this trial is unknown. The database record was created on 30 May 2007, and no update has been provided since then. We emailed the primary contact but have received no reply. |
NCT00915629.
| Methods | Interventional ‐ randomised trial |
| Participants | Participants were women (16 to 65 years) with RVVC (4 or more episodes of VVC during the year prior to the survey). Participants were all symptomatic at time of enrolment with microbiological evidence of Candida albicans infection. |
| Interventions | Lactibiane candisis 5M 2 gelatin capsules per day for 2 months then 1 gelatin capsule per day for 4 months |
| Outcomes | Outcomes not clear but measured to 9 months. |
| Notes | The database record for this trial was created on 8 June 2009 and last updated on 6 October 2011. No publication has been located for this trial. The contact details in the database were insufficient to locate a current contact for the primary investigator. The database states that the trial has been terminated. |
NCT02251093.
| Methods | Interventional ‐ randomised controlled trial |
| Participants | Participants had RVVC defined as "the existence of at least four VVC episodes during the past year, including the one concerned by the screening visit In addition to the current episode, at least one episode occurring during the two previous years must also have been documented by mycological examination". |
| Interventions | Lcr Regenerans Placebo |
| Outcomes | Not clear from database record |
| Notes | The trial database stated the recruitment status of this trial is completed. The database record was created on 26 September 2014 and last updated on 25 March 2016. The record states that 350 participants were enrolled in the trial. We emailed the primary contact but have received no reply. |
NCT04639544.
| Methods | RCT |
| Participants | Inclusion Criteria:
Exclusion Criteria:
|
| Interventions | 1. Placebo Comparator: Control group Volunteers will take 1 capsule per day with maltodextrin for 6 months Intervention: Dietary Supplement: Placebo 2. Experimental: Probiotic group Volunteers will take 1 capsule per day with the Lactobacillus strain for 6 months Intervention: Dietary Supplement: Lactobacillus strain |
| Outcomes | Primary Outcomes:
Secondary Outcomes:
|
| Notes | Setting: Spain Unclear if RVVC confirmed by microbiology https://clinicaltrials.gov/ct2/show/record/NCT04639544 |
NCT04699240.
| Methods | RCT |
| Participants | Inclusion Criteria:
Exclusion Criteria:
|
| Interventions | 1. Active Comparator: Clotrimazole vaginal tablets Intensive treatment: clotrimazole vaginal tablets 500mg, every 72 hours, three consecutive times Consolidation treatment: clotrimazole vaginal tablets 500mg, once a week, 6 months Intervention: Drug: clotrimazole vaginal tablets 2. Active Comparator: Clotrimazole vaginal tablets+ Lactobacillus Intensive treatment: clotrimazole vaginal tablets 500mg, every 72 hours, three consecutive times + Lactobacillus Consolidation treatment: clotrimazole vaginal tablets 500mg, once a week, 6 months Intervention: Drug: Clotrimazole vaginal tablets+ Lactobacillus |
| Outcomes | Primary Outcome: The cure rate of RVVC, [ Time Frame: 6 months ] Secondary Outcome: Recurrence of RVVC [ Time Frame: 6 months ] |
| Notes | Setting: China Unclear if RVVC confirmed by microbiology https://clinicaltrials.gov/ct2/show/record/NCT04699240 |
Rabiee 2013.
| Methods | Interventional |
| Participants | Participants had recurrent vulvovaginal candidiasis that had a positive culture without any predisposing factors. |
| Interventions | Zataria multiflora 1% vaginal cream for 6 months Boric acid 3% vaginal cream for 6 months |
| Outcomes | Cure rate measured to 6 months |
| Notes | Publication located for this trial, which is written in Persian. Awaiting review of full‐text publication by Persian speaker. |
RBR‐892mp4.
| Methods | Interventional ‐ randomised controlled trial |
| Participants | Participants will have recurrent vulvovaginal candidiasis. |
| Interventions | 3 perineal exercises daily for a year No‐intervention control group |
| Outcomes | Recurrence |
| Notes | The trial database stated the recruitment status of this trial is "terminated", with the last planned enrolment on 20 September 2015. The database record was created on 17 June 2015 and the last update was 18 January 2016. We emailed the primary contact but have received no reply. |
Russo 2019.
| Methods | Interventional ‐ randomised controlled trial |
| Participants | 48 women positive for Candida albicans, symptoms of VVC, and documented history of recurrences |
| Interventions | Respecta ‐ lactobacilli mixture (5 × 109 Colony Forming Units per capsule) including Lactobacillus acidophilus GLA‐14 (BCCM/LMG Bacteria Collection, LMG S‐29159) and Lactobacillus rhamnosus HN001 (American Tissue Culture Collection, ATCC Number: SD5675) in combination with bovine lactoferrin RCX (50 mg) Placebo ‐ inactive ingredient maltodextrin (100 mg) Induction phase ‐ 2 capsules per day for 5 days, then 1 capsule per day for 10 days Maintenance phase ‐ 1 capsule daily for 10 consecutive days per month in premenstrual phase |
| Outcomes | Clinical cure, overall cure, clinical recurrence rate |
| Notes | The publication is unclear regarding the number of recurrences. Awaiting reply from authors regarding definition of RVVC used in the trial. |
Zivaljevic 2012.
| Methods | Unclear |
| Participants | Unclear |
| Interventions | Fenticonazole vaginal capsule 600 mg |
| Outcomes | Unclear |
| Notes | Unlikely to meet inclusion criteria for this review as it was unclear from the English abstract if this was a randomised controlled trial, nor does the trial clearly enrol participants with RVVC. Awaiting review of full‐text publication by Serbian speaker |
Characteristics of ongoing studies [ordered by study ID]
EUCTR2019‐000925‐27‐SK.
| Study name | A phase IIb/III, parallel‐arm, randomized, active‐controlled, double‐blind, double‐dummy, multicenter, non‐inferiority study in patients with recurrent vulvovaginal candidosis to compare the clinical efficacy, safety and tolerability of topically administered ProF‐001 (Candiplus®) to oral fluconazole |
| Methods | DB‐RCT |
| Participants | Inclusion criteria: •Female patients = 18 years •Patients suffering from an acute episode in RVVC, characterized by: o Positive vaginal smear (native or KOH) for budding yeasts and/or (pseudo‐) hyphae, normal or intermediate flora o Two or more of the following signs and symptoms of VVC that are characterized as moderate or severe: itching, burning, irritation, edema, redness, or excoriation/fissure. o At least 3 previous episodes of VVC during the last 12 months (i.e. at least 4 episodes including the current episode) •Readiness for sexual abstinence from start of treatment until test of cure (TOC) ‐ visit •Ability to understand trial instructions and rating scales as well as ability to comply with treatment •Written informed consent |
| Interventions | Candiplus (Clotrimazole plus diclofenac) vaginal cream vs Fluconazole 150mg capsules |
| Outcomes | Primary end point(s): Percentage of patients with at least one episode of clinical relapse of VVC during the 12 months study period. |
| Starting date | 11 September 2019 |
| Contact information | Profem GmbH Email: office@profem.at |
| Notes | Country: Austria, Poland, Slovakia Sponsor: Profem GmbH Study identical to NCT04734405 |
NCT04029116.
| Study name | A Phase 3, Multicenter, Randomized, Double‐Blind, Placebo‐Controlled Study to Evaluate the Efficacy and Safety of Oral Ibrexafungerp (SCY‐078) Compared to Placebo in Subjects With Recurrent Vulvovaginal Candidiasis (VVC) |
| Methods | RCT |
| Participants | Key Inclusion Criteria:
Key exclusion Criteria:
|
| Interventions | Experimental: Ibrexafungerp Oral Fluconazole 150 mg every 72 hours for 3 doses followed by Oral Ibrexafungerp 300 mg BID (one day) every 4 weeks for a total of 6 dosing days Placebo Comparator: Placebo Oral Fluconazole 150 mg every 72 hours for 3 doses followed by Oral Placebo BID (one day) every 4 weeks for a total of 6 dosing days |
| Outcomes | Primary Outcome Measures: Clinical Success [ Time Frame: Week 24 ]Efficacy as measured by the percentage of subjects with documented Clinical Success. Secondary Outcome Measures: The percentage of subjects with no Mycologically Proven Recurrence [ Time Frame: Week 24 and Week 36 ] Efficacy as measured by the percentage of subjects with no Mycologically Proven Recurrence Safety and tolerability [ Time Frame: Week 24 ] Safety as measured by the number of subjects who discontinue due to treatment related adverse events. |
| Starting date | 23 September 2019 |
| Contact information | Contact: Philip Deane (philip.deane@scynexis.com), Nkechi Azie, MD (Nkechi.azie@scynexis.com) |
| Notes | Country: not reported Sponsor: Scynexis, Inc. |
NCT04208555.
| Study name | A Randomized Comparison of Boric Acid Versus Terconazole in Treatment of Recurrent Vulvovaginal Candidiasis |
| Methods | RCT |
| Participants | Women 18 Years to 50 Years (Adult) Inclusion Criteria:
Exclusion Criteria:
|
| Interventions | Experimental: Boric acid vaginal suppository (600 mg/day) for 14 days Control: Terconazole 80 mg vaginal suppository daily for 6 days |
| Outcomes | Primary Outcome Measures ‐ Mycological cure rate [ Time Frame: At day 15 of treatment ] ‐ Negative Candida by cultures of high vaginal swabs |
| Starting date | 15 January 2020 |
| Contact information | Study Chair: Hatem Abu Hashim, MD.FRCOG.PhD; T: +20502300002; Email: hatem_ah@hotmail.com; Faculty of Medicine, Mansoura University Principal Investigator:Asmaa Swidan, MBBCh; New Mansoura General Hospital |
| Notes | Country: Egypt https://clinicaltrials.gov/ct2/show/NCT04208555 |
NCT04292704.
| Study name | The Role of Fractional CO2 Laser in Consolidation Treatment of Recurrent Vulvovaginal Candidiasis (RVVC) :a Study Protocol for a Randomized Controlled Trial |
| Methods | RCT |
| Participants | 200 RVVC patients will be eligible for the trial if they fulfil the following criterion:
5 healthy volunteers as the normal control group will be eligible for the trial if they fulfil the following criterion:
Exclusion criteria:
|
| Interventions |
|
| Outcomes |
|
| Starting date | December 13, 2019 |
| Contact information | Contact: Ledan Wang, Doctor +8613858850907; ledanwang331@163.com Contact: Yiqin Hu, Master +8615158662656; huyiqin1996@163.com |
| Notes | Setting: China https://clinicaltrials.gov/ct2/show/record/NCT04292704 |
Differences between protocol and review
Criteria for considering studies for this review
Types of studies: We clarified that we would only consider studies that evaluated treatments for RVVC for at least six months.
Types of studies: Many identified studies did not specify if the assessor was blinded. Instead of excluding these studies as we stated in the protocol, we included them and performed 'Risk of bias' assessment and sensitivity analysis. Secondly, we clarified the duration of our studies. As this review aimed to assess the prevention of recurrence in RVVC, we only included studies that followed participants for at least six months.
Types of interventions: Our protocol prespecified several comparisons. However, these did not take into account that not all studies would include a placebo. We also decided to divide the comparisons into drug and non‐drug comparisons, as "any treatment versus placebo" was an unhelpful comparison clinically. We adjusted the comparisons according to the following table:
| Comparison in protocol | Comparison(s) in final review |
| Any treatment versus placebo | 1. Drug treatment versus placebo/no treatment (excluding partner treatment). Within this comparison, we analysed separately the studies using fluconazole versus placebo/no treatment as this is a relevant question for clinicians. 8. Complementary and alternative medicine versus placebo/no treatment |
| Short duration of treatment versus longer duration of treatment | 6. UNCHANGED |
| Systemic versus local treatment | 2. Oral drug treatment versus topical drug treatment |
| Partner treatment versus placebo | 7. Partner treatment versus placebo/no treatment |
| Comparison of two different classes of drugs | DELETED |
| Comparison of different doses of the same agent | 5. UNCHANGED |
| N/A | 3. Oral drug treatment versus oral drug treatment 4. Topical drug treatment versus topical drug treatment 9. Complementary and alternative medicine versus drug treatment 10. Non‐drug treatment versus other treatment 11. Vaccination versus other treatment |
| Adverse events listed as secondary outcome | Adverse events listed as primary outcome |
Search methods for identification of studies
Electronic searches: In the protocol we stated that we would specifically search for conference paper abstracts. We screened conference paper abstracts as part of the electronic searches in MEDLINE, Embase, etc., but did not screen conference proceedings of specific conferences.
Data collection and analysis
Assessment of risk of bias in included studies: We also assessed detection bias (blinding of outcome assessment) as a source of bias. We included the criteria for assessing risk of bias as low, high, or unclear in the Methods section.
Assessment of heterogeneity: We updated the section on assessment of heterogeneity in accordance with the updated Cochrane Handbook for Systematic Reviews of Interventions.
Data synthesis: We updated how we dealt with statistical and clinical heterogeneity and included a section on how the 'Summary of findings' tables were generated.
Subgroup analyses ‐ route of administration: topical versus systemic and intervention ‐ duration: short versus long treatment were removed from the subgroup analyses. This should have been included in the comparisons only, not in the subgroup analyses.
Sensitivity analysis: Clarification: planned sensitivity analysis was done for risk of selection bias.
Outcomes: Our protocol listed complications and adverse events as separate outcomes. We combined these into a single outcome measure in the review.
Contributions of authors
Cathy Watson (CW) and Georga Cooke (GC) wrote the protocol. Mieke van Driel (MVD), Marie Pirotta (MP), and Jane Smith (JS) provided comments and advice on the protocol. All authors approved the final version of the protocol.
GC screened the literature searches, reviewed the full texts for eligibility, extracted data from the included studies, conducted the analyses, and prepared the manuscript for publication.
CW screened the literature searches, reviewed the full texts for eligibility, extracted data from the included studies and prepared the manuscript for publication. CW also verified data entry for the review.
Laura Deckx (LD) ran updated searches, extracted data from the included studies, updated analyses with new included studies, and prepared the manuscript for publication.
MP and JS conducted the 'Risk of bias' assessment and assisted with preparing the manuscript for publication.
MVD advised on the methodology of the review, conducted the 'Risk of bias' assessment, supervised data extraction and analysis, and contributed to the preparation and drafting of the review for publication.
GC, LD, CW, and MVD revised the review following editorial review.
Sources of support
Internal sources
-
Centre for Research in Evidence‐Based Practice, Bond University, Australia
In‐kind support
-
Primary Care Clinical Unit, Faculty of Medicine, The University of Queensland, Australia
In‐kind support
-
Department of General Practice, University of Melbourne, Australia
In‐kind support
External sources
-
General Practice Education and Training, Australia
During part of this review process, GC's position at Bond University was funded by General Practice Education and Training
Declarations of interest
Georga Cooke: no conflicts of interest Cathy Watson: no conflicts of interest Laura Deckx: no conflicts of interest Marie Pirotta: no conflicts of interest Jane Smith: no conflicts of interest Mieke L van Driel: no conflicts of interest
Edited (no change to conclusions)
References
References to studies included in this review
Bolouri 2009 {published data only (unpublished sought but not used)}
- Bolouri F, Tabrizi NM, Tanha FD, Niroomand N, Azmoodeh A, Emami S, et al.Effectiveness of fluconazole for suppressive maintenance therapy in patients with RVVC: a randomized placebo-controlled study. Iranian Journal of Pharmaceutical Research 2009;8:307-13. [Google Scholar]
Chopra 2013 {published and unpublished data}
- Chopra V, Marotta F, Kumari A, Bishier MP, He F, Zerbinati N, et al.Prophylactic strategies in recurrent vulvovaginal candidiasis: a 2-year study testing a phytonutrient vs itraconazole. Journal of Biological Regulators and Homeostatic Agents 2013;27(3):875-82. [PMID: ] [PubMed] [Google Scholar]
Corthay 1988 {published data only (unpublished sought but not used)}
- Corthay P, Perrenoud C, Gumowski PI, Girard JP.Candida albicans specific immune responses in patients with recurrent chronic vaginitis treated with an anti-candida food regimen (ACFR) or an hyposensitization treatment (HPT). Allergy 1988;43:51. [Google Scholar]
D'Antuono 2012 {published and unpublished data}
- D'Antuono A, Baldi E, Bellavista S, Banzola N, Zauli S, Patrizi A.Use of Dermasilk briefs in recurrent vulvovaginal candidosis: safety and effectiveness. Mycoses 2012;55(3):e85-9. [DOI] [PubMed] [Google Scholar]
D'Antuono 2013 {published data only (unpublished sought but not used)}
- D'Antuono A, Bellavista S, Gaspari V, Filippini A, Patrizi A.Dermasilk® briefs in recurrent vulvovaginal candidosis. An alternative option in long-lasting disease. Minerva Ginecologica 2013;65(6):697-705. [PubMed] [Google Scholar]
Fan 2015 {published data only}
- Fan S, Liu X, Wu C, Xu L, Li J.Vaginal nystatin versus oral fluconazole for the treatment for recurrent vulvovaginal candidiasis. Mycopathologia 2015;179:95-101. [DOI: ] [DOI] [PubMed] [Google Scholar]
Fardyazar 2007 {published data only (unpublished sought but not used)}
- Fardyazar Z, Habibzadeh S, Abdollahi-Fard S, Tello M.Vaginal azoles versus oral fluconazole in treatment of recurrent vulvovaginal candidiasis. Iranian Journal of Clinical Infectious Diseases 2007;2:17-22. [Google Scholar]
- Fardyazar Z, Habibzadeh S.Long term vaginal azoles versus prophylactic oral fluconazole in treatment of recurrent vulvovaginal candidiasis. Research Journal of Biological Sciences 2007;2(6):663-6. [Google Scholar]
Fong 1992a {published data only (unpublished sought but not used)}
- Fong IW.The value of chronic suppressive therapy with itraconazole versus clotrimazole in women with recurrent vaginal candidiasis. Genitourinary Medicine 1992;68:374-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fong 1992b {published data only (unpublished sought but not used)}
- Fong IW.The value of treating the sexual partners of women with recurrent vaginal candidiasis with ketoconazole. Genitourinary Medicine 1992;68:174-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fong 1994 {published data only}
- Fong IW.The value of prophylactic (monthly) clotrimazole versus empiric self-treatment in recurrent vaginal candidiasis. Genitourinary Medicine 1994;70:124-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kumari 2011 {published data only}
- Kumari A, Bishier MP, Naito Y, Sharma A, Solimene U, Jain S, et al.Protective effect of an oral natural phytonutrient in recurrent vulvovaginal candidiasis: a 12-month study. Journal of Biological Regulators & Homeostatic Agents 2011;25(4):543-51. [PubMed] [Google Scholar]
Li 2018 {published data only}
- Li W.Influence of nursing intervention on recurrent vulvovaginal candidiasis patients treated with ATP-infrared bio-effect technique. Iranian Journal of Public Health 2018;47(10):1511-9. [PMC free article] [PubMed] [Google Scholar]
Lopez‐Olmos 2000 {published and unpublished data}
- Lopez-Olmos J, Lerma E.Treatment of recurring vulvo-vaginal candidiasis: a comparative prospective study during six months of three anti-mycotic preparations of a single dosis. Clinica e Investigacion en Ginecologia y Obstetricia 2000;27:366-75. [Google Scholar]
Mendling 2011 {published data only}
- Mendling W, Birkner V.Vaccination with inactivated lactobacilli or heliotherapy can improve the quality-of-life of women with chronic recurrent vulvovaginal candidosis a prospective randomized study [Die Vakzination mit inaktivierten Laktobazillen oder mit Heliotherapie kann die Lebensqualitat von Frauen mit rezidivierender vulvovaginaler Kandidose verbessern - Eine prospektive 3-armige randomisierte Studie]. Geburtshilfe und Frauenheilkunde 2011;71(9):767-72. [Google Scholar]
Metts 2003 {published data only (unpublished sought but not used)}
- Metts J, Famula TR, Trenev N, Clemens RA.Lactobacillus acidophilus, strain NAS (H2O2 positive), in reduction of recurrent candidal vulvovaginitis. Journal of Applied Research 2003;3:340-8. [Google Scholar]
Roth 1990 {published data only (unpublished sought but not used)}
- Roth AC, Milsom I, Forssman L, Wahlen P.Intermittent prophylactic treatment of recurrent vaginal candidiasis by postmenstrual application of a 500 mg clotrimazole vaginal tablet. Genitourinary Medicine 1990;66:357-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sobel 1985a {published data only (unpublished sought but not used)}
- Sobel JD.Management of recurrent vulvovaginal candidiasis (VVC) with ketoconazole (K) prophylaxis [abstract]. Archives of Gynecology 1985;237 Suppl:281. [Google Scholar]
- Sobel JD.Management of recurrent vulvovaginal candidiasis with intermittent ketoconazole prophylaxis. Obstetrics & Gynecology 1985;65:435-40. [PubMed] [Google Scholar]
Sobel 1986 {published data only (unpublished sought but not used)}
- Sobel JD.Recurrent vulvovaginal candidiasis. A prospective study of the efficacy of maintenance ketoconazole therapy. New England Journal of Medicine 1986;315:1455-8. [DOI] [PubMed] [Google Scholar]
Sobel 1989 {published data only (unpublished sought but not used)}
- Sobel JD, Schmitt C, Meriwether C.Clotrimazole treatment of recurrent and chronic candida vulvovaginitis. Obstetrics & Gynecology 1989;73:330-4. [PubMed] [Google Scholar]
Sobel 2004 {published data only (unpublished sought but not used)}
- Sobel JD, Wiesenfeld HC, Martens M, Danna P, Hooton TM, Rompalo A, et al.Maintenance fluconazole therapy for recurrent vulvovaginal candidiasis. New England Journal of Medicine 2004;351:876-83. [DOI] [PubMed] [Google Scholar]
Spacek 2005 {published data only}
- Spacek J, Buchta V.Itraconazole in the treatment of acute and recurrent vulvovaginal candidosis: comparison of a 1-day and a 3-day regimen. Mycoses 2005;48:165-71. [DOI] [PubMed] [Google Scholar]
Spinillo 1997 {published data only}
- Spinillo A, Colonna L, Piazzi G, Baltaro F, Monaco A, Ferrari A.Managing recurrent vulvovaginal candidiasis. Intermittent prevention with itraconazole. Journal of Reproductive Medicine 1997;42:83-7. [PubMed] [Google Scholar]
Witt 2009 {published data only (unpublished sought but not used)}
- Witt A, Kaufmann U, Bitschnau M, Tempfer C, Ozbal A, Haytouglu E, et al.Monthly itraconazole versus classic homeopathy for the treatment of recurrent vulvovaginal candidiasis: a randomized trial. Obstetrical and Gynecological Survey 2010;65(1):26-7. [DOI] [PubMed] [Google Scholar]
- Witt A, Kaufmann U, Bitschnau M, Tempfer C, Ozbal A, Haytouglu E, Gregor H, Kiss H.Monthly itraconazole versus classic homeopathy for the treatment of recurrent vulvovaginal candidiasis: a randomised trial. British Journal of Obstetrics & Gynaecology 2009;116(11):1499-505. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Avijgan 2012 {published data only}
- Avijgan M, Mirzadeh F, Nia EA.The comparative study of anti-fungal effect of pharmaceutical products containing hydroalcoholic extract of Echinophora platyloba DC and fluconazole in women with chronic recurrent vaginitis caused by candida albicans. Journal of Research in Medical Sciences 2012;17:S103-S107. [Google Scholar]
Azima 2018 {published data only}
- Azima S, Houshyar S, Motamedi Far M, Kaviani M, Zare N.The Effect of Vaginal Probiotic Capsule On Vaginal Colonization and Treatment Results inPatients with Vulvar and Vaginal Candidiasis. Journal of Zanjan University of Medical Sciences and Health Services 2018;26(114):40-50. [Google Scholar]
Bartz 2000 {published data only}
- Bartz BR.Efficacy of zinc supplementation in reducing the incidence of recurrent vaginitis. ProQuest Dissertations and Theses 2000:64.
Brand 2018 {published data only}
- Brand S, Degenhardt T, Nyirjesy P, Sobel J, Handelsman C, Person K, Schotzinger R, Tavakkol A.To evaluate the efficacy and safety of VT-1161, a potent, highly selective inhibitor of fungal CYP51, in treating women with a documented history of recurrent vulvovaginal candidiasis (RVVC). American Journal of Obstetrics and Gynecology 2016;215(6):S821. [DOI: 10.1016/j.ajog.2016.09.016] [DOI] [Google Scholar]
- Brand SR, Degenhardt TP, Person K, Sobel JD, Nyiriesy P, Schotzinger RJ, Tavakkol A.A phase 2, randomized, double-blind, placebo-controlled, dose-ranging study to evaluate the efficacy and safety of orally administered VT-1161 in the treatment of recurrent vulvovaginal candidiasis. American Journal of Obstetrics and Gynecology 2018;218(6):1e.1-1e.9. [DOI] [PubMed]
- Sobel JD, Brand SR, Degenhardt TP, Person K, Nyirjesy P, Schotzinger RJ, Tavakkol A.Results from a phase 2, randomized, double-blind, placebo-controlled, dose ranging study to evaluate the efficacy and safety of VT 1161 oral tablets in the treatment of patients with recurrent vulvovaginal candidiasis. American Journal of Obstetrics and Gynecology 2017;217(6):715. [Google Scholar]
Bushell 1988a {published data only}
- Bushell TE, Evans EG, Meaden JD, Milne JD, Warnock DW.Intermittent local prophylaxis against recurrent vaginal candidosis. Genitourinary Medicine 1988;64:335-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bushell 1998b {published data only}
- Bushell TE, Evans EG, Llewellyn PA, Meaden JD, Milne JD, Warnock DW.Prophylactic use of clotrimazole in recurrent vaginal candidosis. Annals of the New York Academy of Sciences 1988;544:558-60. [ISSN 0077-8923] [DOI] [PubMed] [Google Scholar]
Coric 2006 {published data only}
- Coric M, Barisic D, Lovric H.Fluconazole versus 3-day clotrimazole in the treatment of sporadic and recurrent vulvovaginal candidiasis. International Journal of Gynaecology & Obstetrics 2006;95:171-2. [DOI] [PubMed] [Google Scholar]
Davidson 1978 {published data only}
- Davidson F, Mould RF.Recurrent genital candidosis in women and the effect of intermittent prophylactic treatment. British Journal of Venereal Diseases 1978;54:176-83. [DOI] [PMC free article] [PubMed] [Google Scholar]
Diba 2010 {published data only}
- Diba K, Namaki A, Bahadori F.Comparative study of fluconazole and clotrimazole for the treatment of vulvovaginal candidiasis. Journal of Sexual Medicine 2010;7:431. [Google Scholar]
Donders 2008 {published data only}
- Donders G, Bellen G, Byttebier G, Verguts L, Hinoul P, Walckiers R, Stalpaert M, Vereecken A, Van Eldere J.Individualized decreasing-dose maintenance fluconazole regimen for recurrent vulvovaginal candidiasis (ReCiDiF trial). American Journal of Obstetrics & Gynecology 2008;199(6):613.e1-9. [ISSN 1097-6868] [DOI] [PubMed] [Google Scholar]
Edwards 2018 {published data only}
- Edwards JE Jr, Schwartz MM, Schmidt CS, Sobel JD, Nyirjesy P, Schodel F, et al.A Fungal Immunotherapeutic Vaccine (NDV-3A) for Treatment of Recurrent Vulvovaginal Candidiasis-A Phase 2 Randomized, Double-Blind, Placebo-Controlled Trial. Clin Infect Dis 2018;66(12):1928-1936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyirjesy P, Sobel JD, Edwards JE, Schwarz MW, Schmidt CS, Hennessey JP.NDV-3A vaccine reduces the frequency of vaginitis in patients with recurrent vulvovaginal candidiasis. American Journal of Obstetrics and Gynecology 2016;215(6):S822. [DOI: 10.1016/j.ajog.2016.09.019] [DOI] [Google Scholar]
Fan 2005 {published data only}
- Fan SR, Liu XP, Li JW, Xu AP, Liu M.Study on classification and treatment of vulvovaginal candidiasis. Chung-Hua Fu Chan Ko Tsa Chih [Chinese Journal of Obstetrics & Gynecology] 2005;40:532-5. [PubMed] [Google Scholar]
Fong 1993 {published data only (unpublished sought but not used)}
- Fong IW, Bannatyne RM, Wong P.Lack of in vitro resistance of Candida albicans to ketoconazole, itraconazole and clotrimazole in women treated for recurrent vaginal candidiasis. Genitourinary Medicine 1993;69(1):44-46. [DOI] [PMC free article] [PubMed] [Google Scholar]
Golero 1993 {published data only}
- Gorlero F, Larosa E, Cauwenbergh G, Woestenborghs R, Heykants J, Cilli P, Dececco L.Itraconazole plasma and vaginal mucosal levels in patients with chronic vaginal candidosis treated with itraconazole 200mg once-daily for 3 consecutive days. Drug Investigation 1993;6(1):22-24. [ISSN 0114-2402] [Google Scholar]
Hilton 1992 {published data only (unpublished sought but not used)}
- Hilton E, Isenberg HD, Alperstein P, France K, Borenstein MT.Ingestion of yogurt containing Lactobacillus acidophilus as prophylaxis for candidal vaginitis. Annals of Internal Medicine 1992;116:353-7. [DOI] [PubMed] [Google Scholar]
Houang 1989 {published data only}
- Houang E.Fluconazole in recurrent vaginal candidiasis - preliminary-results of a double-blind, randomized clinical-trial. In: Fluconazole and its role in vaginal candidiasis. In: Richardson RG, editors(s). International Congress and Symposium Series. Vol. 160. London: Royal Society of Medicine Services, 1989:22-31. [Google Scholar]
Miller 1984 {published data only}
- Miller PI, Humphries M, Grassick K.A single-blind comparison of oral and intravaginal treatments in acute and recurrent vaginal candidosis in general practice. Pharmatherapeutica 1984;3:582-7. [PubMed] [Google Scholar]
Rashid 1991 {published data only}
- Rashid S, Collins M, Kennedy RJ.A study of candidosis: the role of fomites. Genitourinary Medicine 1991;67(2):137-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
Shalev 1996 {published data only}
- Shalev E, Battino S, Weiner E, Colodner R, Keness Y.Ingestion of yogurt containing Lactobacillus acidophilus compared with pasteurized yogurt as prophylaxis for recurrent candidal vaginitis and bacterial vaginosis. Archives of Family Medicine 1996;5:593-6. [DOI] [PubMed] [Google Scholar]
Silverman 1971 {published data only}
- Silverman M, Okun R.Oxytetracycline-nystatin in the prevention of candidal vaginitis. American Journal of Obstetrics & Gynecology 1971;111:398-404. [DOI] [PubMed] [Google Scholar]
Sobel 1994 {published data only}
- Sobel JD, Schmitt C, Stein G, Mummaw N, Christensen S, Meriwether C.Initial management of recurrent vulvovaginal candidiasis with oral ketoconazole and topical clotrimazole. Journal of Reproductive Medicine 1994;39(7):517-20. [ISSN 0024-7758] [PubMed] [Google Scholar]
Sobel 2001 {published data only}
- Sobel JD, Kapernick PS, Zervos M, Reed BD, Hooton T, Soper D, et al.Treatment of complicated Candida vaginitis: comparison of single and sequential doses of fluconazole. American Journal of Obstetrics & Gynecology 2001;185:363-9. [DOI] [PubMed] [Google Scholar]
Vladareanu 2018 {published data only}
- Vladareanu R, Mihu D, Mitran M, Mehedintu C, Boiangiu A, Manolache M, Vladareanu S.New evidence on oral L. plantarum P17630 product in women with history of recurrent vulvovaginal candidiasis (RVVC): a randomized double-blind placebo-controlled study. European Review for Medical and Pharmacological Sciences 2018;22(1):262-267. [DOI: 10.26355/eurrev_201801_14128] [DOI] [PubMed] [Google Scholar]
Yang 2000 {published data only}
- Yang F, Zhou H, Mo XZ, Yan DD.Itraconazole maintaining therapy in prevention recurrent vulva-vaginal candidiasis (Chinese). Chinese Journal of Leprosy and Skin Disease 2000;16(4):235. [Google Scholar]
References to studies awaiting assessment
ACTRN12614001258640 {published data only (unpublished sought but not used)}
- ACTRN12614001258640.A randomized, double-blinded study investigating the safety and efficacy of daily low-dose oral fluconazole versus weekly fluconazole in patients with chronic vulvovaginal candidiasis. https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12614001258640 2 December 2012.
ChiCTR‐IPR‐15006314 {published data only (unpublished sought but not used)}
- ChiCTR-IPR-15006314.Multi-center clinical study on JUC Spray Dressing under the patent technology "Physical Antimicrobial Film" in preventing the recurrence of vulvovaginal candidiasis (VVC). http://www.chictr.org.cn/showproj.aspx?proj=10772 14 April 2015.
ChiCTR‐TRC‐10000833 {published data only (unpublished sought but not used)}
- ChiCTR-TRC-10000833.The clinical research of Chinese herb XiangLian Suppository in the treatment of recurrent vulvovaginal candidiasis. http://www.chictr.org.cn/showproj.aspx?proj=8703 28 March 2010.
EUCTR2010‐021502‐38‐DE {published data only}
- EUCTR2010-021502-38-DE.Study for measuring vaginal interleukins in patients with cervical neoplasia (CIN 1-3) or chronic vaginal candidiasis with phenyl-4-butyrate [STUDIE ZUR MESSUNG DER VAGINALEN INTERLEUKINE BEI PATIENTINNEN MIT ZERVIKALEN NEOPLASIEN (CIN 1-3) ODER CHRONISCHER CANDIDIASIS VAGINALIS UNTER BEHANDLUNG MIT 4PHENYL-BUTYRATE]. https://www.clinicaltrialsregister.eu/ctr-search/trial/2010-021502-38/DE 11 November 2010. [2010-021502-38]
EUCTR2011‐004718‐40‐IT {published data only}
- EUCTR2011-004718-40-IT.Activities of Metronidazole + Clotrimazole in the treatment and prophylaxis of recurrent vaginal infections recurrent Candida albicans and Candida albicans spp non albicans. https://www.clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2011-004718-40 8 March 2012. [2011-004718-40]
EUCTR2013‐002480‐26‐PL {published data only (unpublished sought but not used)}
- EUCTR2013-002480-26-PL.Study of the efficacy and safety of treatment with total freeze-dried culture of Lcr Regenerans® administered intravaginally in the prevention of recurrent vulvovaginal candidiasis.International, randomized, phase III, multi-centre, 2-arm, parallel group, double-blind, placebo-controlled superiority trial.. https://www.clinicaltrialsregister.eu/ctr-search/trial/2013-002480-26/PL 30 July 2014. [EUCTR2013-002480-26-PL]
NCT00479947 {published data only (unpublished sought but not used)}
- NCT00479947.Use of Oral Probiotics as an Adjunctive Therapy to Fluconazole in the Treatment of Yeast Vaginitis. http://clinicaltrials.gov/show/NCT00479947 30 May 2007. [NCT00479947]
NCT00915629 {published data only}
- NCT00915629.Prevention of Recurrent Vulvovaginal Candidiasis With Lactibiane Candisis 5M®. https://clinicaltrials.gov/ct2/show/NCT00915629 8 June 2009.
NCT02251093 {published data only (unpublished sought but not used)}
- NCT02251093.Study of the Efficacy and Tolerance of Intra-vaginal Treatment With a Total Freeze-dried Culture of Lcr Regenerans® in the Prevention of Relapses of Recurrent Vulvovaginal Candidiasis. https://clinicaltrials.gov/ct2/show/NCT02251093 26 September 2014.
NCT04639544 {published data only}
NCT04699240 {published data only}
Rabiee 2013 {published data only}
- IRCT2012102911302N1.Comparison of clinical response to vaginal cream zataria multiflora and boric acid in patients with recurrent vulvovaginal candidiasis. http://en.irct.ir/trial/11581 17 December 2012. [IRCT2012102911302N1]
- Rabiee M, Akbari H, Naseri M, Bekhradi R, Nikzad M, Torkestani F.Comparison of clinical response to Zatariamultiflora vaginal cream and boric acid inpatients with recurrent vulvovaginal candidiasis. Scientific-ResearchJournal of Shahed University 2013;102:1-8. [Google Scholar]
RBR‐892mp4 {published data only (unpublished sought but not used)}
- lRBR-892mp4.Effectiveness of therapeutic exercise applied to the pelvic floor muscles to prevent recurrence of Vulvovaginitis and improve female sexuality: randomized clinical trial. http://www.ensaiosclinicos.gov.br/rg/RBR-892mp4/ 17 June 2015. [RBR-892mp4]
Russo 2019 {published data only}
- Russo R, Superti F, Karadja E, De Seta F.Randomised clinical trial in women with Recurrent Vulvovaginal Candidiasis: Efficacy of probiotics and lactoferrin as maintenance treatment. Mycoses 2019;62:328–335. [DOI] [PubMed] [Google Scholar]
Zivaljevic 2012 {published data only}
- Zivaljevic B, Golubovic I, Seratlic J, Nikolic P, Simic D, Magdic I, et al.Efficiency of Fenticonazole for the Treatment of Vaginal Candidiasis. Srpski Arhiv Za Celokupno Lekarstvo 2012;140(7-8):469-474. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
EUCTR2019‐000925‐27‐SK {published data only}
- A phase IIb/III, parallel-arm, randomized, active-controlled, double-blind, double-dummy, multicenter, non-inferiority study in patients with recurrent vulvovaginal candidosis to compare the clinical efficacy, safety and tolerability of topically administered ProF-001 (Candiplus®) to oral fluconazole. ICTRP. [URL: https://trialsearch.who.int/?TrialID=EUCTR2019-000925-27-SK]
- A Phase IIb/III Study of Prof-001 for the Treatment of Patients With Recurrent Vulvovaginal Candidiasis (RVVC). clinicaltrials.gov. [URL: https://clinicaltrials.gov/ct2/show/NCT04734405]
NCT04029116 {published data only}
- A Phase 3, Multicenter, Randomized, Double-Blind, Placebo-Controlled Study to Evaluate the Efficacy and Safety of Oral Ibrexafungerp (SCY-078) Compared to Placebo in Subjects With Recurrent Vulvovaginal Candidiasis (VVC). ClinicalTrials.gov. [https://clinicaltrials.gov/ct2/show/NCT04029116]
NCT04208555 {published data only}
- A Randomized Comparison of Boric Acid Versus Terconazole in Treatment of Recurrent Vulvovaginal Candidiasis. ClinicalTrials.gov. [URL: https://clinicaltrials.gov/ct2/show/NCT04208555]
NCT04292704 {published data only}
- NCT04292704. clinicaltrials.gov. [URL: https://clinicaltrials.gov/ct2/show/record/NCT04292704]
Additional references
Beigi 2004
- Beigi RH, Meyn LA, Moore DM, Krohn MA, Hillier SL.Vaginal yeast colonization in nonpregnant women: a longitudinal study. Obstetrics & Gynecology 2004;104(5 Pt 1):926-930. [DOI] [PubMed] [Google Scholar]
CDC 2015
- Vulvovaginal candidiasis. Sexually Transmitted Diseases Treatment Guidelines 2015. [https://www.cdc.gov/std/tg2015/candidiasis.htm] [PMC free article] [PubMed]
Chapple 2000
- Chapple A, Hassell K, Nicholson M, Cantrill J."You don't really feel you can function normally": women's perceptions and personal management of vaginal thrush". Journal of Reproductive and Infant Psychology 2000;18(4):309-319. [Google Scholar]
Chen 2007
- Chen S, Sorrell T.Antifungal agents. Medical Journal of Australia 2007;187(7):404-409. [DOI] [PubMed] [Google Scholar]
Deeks 2017
- Deeks JJ, Higgins JPT, Altman DG, editor(s).Chapter 9: Analysing data and undertaking metaanalyses. In: Higgins JPT, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.2.0 (updated June 2017). Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Denning 2018
- Denning DW, Kneale M, Sobel JD, Rautemaa-Richardson R.Global burden of recurrent vulvovaginal candidiasis: a systematic review. Lancet Infect Dis 2018;August 2:e339-47. [DOI: 10.1016/S1473-3099(18)30103-8] [DOI] [PubMed] [Google Scholar]
Ehrstrom 2007
- Ehrstrom S, Kornfeld D, Rylander E.Perceived stress in women with recurrent vulvovaginal candidiasis. Journal of Psychosomatic Obstetrics and Gynecology 2007;28(3):169-176. [DOI] [PubMed] [Google Scholar]
Falagas 2006
- Falagas M, Betsi GI, Athanasiou S.Probiotics for prevention of recurrent vulvovaginal candidiasis: A review. Journal of Antimicrobial Chemotherapy 2006;58:266-72. [DOI] [PubMed] [Google Scholar]
Fidel 1998
- Fidel PL, Sobel JD.Protective immunity in experimental Candida vaginitis. Research in Immunology 1998;149(4-5):361-73. [DOI] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- McMaster University (developed by Evidence Prime) GRADEpro GDT.Hamilton (ON): McMaster University (developed by Evidence Prime), 2014. Available at gradepro.org.
Guaschino 2001
- Guaschino S, De Seta F, Sartore A, Ricci G, De Santo D, Piccoli M, Alberico S.Efficacy of maintenance therapy with topical boric acid in comparison with oral itraconazole in the treatment of recurrent vulvovaginal candidiasis. American Journal of Obstetrics and Gynecology 2001;184(4):598-602. [ISSN 002-9378] [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors).Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. In: The Cochrane Collaboration. The Cochrane Collaboration, 2011. [Available from www.cochrane-handbook.org.] [Google Scholar]
Lopez 2013
- Lopez JEM.Candidiasis (vulvovaginal). BMJ Clin Evid 2013;3:0815. [Google Scholar]
Merkus 1990
- Merkus JM, Van Heusden AM.Chronic vulvovaginal candidosis: the role of oral treatment. British Journal of Clinical Practice 1990;71:s81-84. [PubMed] [Google Scholar]
Miller 2000
- Miller L, Patton DL, Meier A, Thwin S, Hooton TM, Eschenbach DA.Depomedroxyprogesterone-induced hypoestrogenism and changes in vaginal flora and epithelium. Obstetrics & Gynecology 2000;96(3):431-9. [DOI] [PubMed] [Google Scholar]
Moraes 2000
- Moraes PS, Lima Goiaba S, Taketomi EA.Candida albicans allergen immunotherapy in recurrent vaginal candidiasis. Journal of Investigational Allergology & Clinical Immunology 2000;10(5):305-9. [PubMed] [Google Scholar]
Nurbhai 2007
- Nurbhai M, Grimshaw J, Watson M, Bond CM, Mollison JA, Ludbrook A.Oral versus intra-vaginal imidazole and triazole anti-fungal treatment of uncomplicated vulvovaginal candidiasis (thrush). Cochrane Database of Systematic Reviews 2007, Issue 4. Art. No: CD002845. [DOI: 10.1002/14651858.CD002845.pub2] [DOI] [PubMed] [Google Scholar]
Nyirjesy 2001
- Nyirjesy P.Chronic vulvovaginal candidiasis. American Family Physician 2001;63(4):697-702. [PubMed] [Google Scholar]
Nyirjesy 2008
- Nyirjesy P.Vulvovaginal candidiasis and bacterial vaginosis. Infectious Disease Clinics of North America 2008;22(4):637-52. [DOI] [PubMed] [Google Scholar]
Odds 2003
- Odds FC, Brown AJP, Gow NAR.Antifungal agents: mechanisms of action. Trends in Microbiology 2003;11(6):272-9. [DOI] [PubMed] [Google Scholar]
Pappas 2015
- Pappas PG, Kauffman CA, Andes DR, Clancy CJ, Marr KA, Ostrosky-Zeichner L, et al.Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clinical Infectious Diseases 2015;62(4):e1-e50. [DOI] [PMC free article] [PubMed] [Google Scholar]
Patel 2004
- Patel DA, Gillespie B, Sobel JD, Leaman D, Nyirjesy P, Weitz MV, Foxman B.Risk factors for recurrent vulvovaginal candidiasis in women receiving maintenance antifungal therapy: results of a prospective cohort study. American Journal of Obstetrics and Gynecology 2004;190(3):644-53. [DOI] [PubMed] [Google Scholar]
Peters 2014
- Peters BM, Yano J, Noverr MC, Fidel Jr PL.Candida Vaginitis: When opportunism knocks, the host responds. PLOS Pathogens 2014;10(4):e1003965. [DOI: 10.1371/journal.ppat.1003965] [DOI] [PMC free article] [PubMed] [Google Scholar]
Pirotta 2003
- Pirotta MV, Gunn JM, Chondros P."Not thrush again!" Women's experience of post-antibiotic vulvovaginitis. Medical Journal of Australia 2003;179(1):43-46. [DOI] [PubMed] [Google Scholar]
Pirotta 2004
- Pirotta M, Gunn J, Chondros P, Grover S, O'Malley P, Garland S.The effect of lactobacillus in preventing post-antibiotic vulvovaginal candidiasis: a randomised controlled trial. British Medical Journal. 2004;329:548-552. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pontes 2014
- Pontes AC, Amaral RLG, Giraldo PC, Beghini J, Giraldo HPD, Cordeiro ES.A systematic review of the effect of daily panty liner use on the vulvovaginal environment. International Journal of Gynecology and Obstetrics 2014;127:1-5. [DOI] [PubMed] [Google Scholar]
Rathod 2014
- Rathod SD, Buffler PA.Highly-cited estimates of the cumulative incidence and recurrence of vulvovaginal candidiasis are inadequately documented. BMC Women's Health 2014;14:43. [DOI: 10.1186/1472-6874-14-43] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ray 2011
- Ray A, Ray S, George AT, Swaminathan N.Interventions for prevention and treatment of vulvovaginal candidiasis in women with HIV infection. Cochrane Database of Systematic Reviews 2011, Issue 8. Art. No: CD008739. [DOI: 10.1002/14651858.CD008739.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration Review Manager 5 (RevMan 5).Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rosa 2013
- Rosa MI, Silva BR, Pires PS, Silva FR, Silva NC, Silva FR, et al.Weekly fluconazole therapy for recurrent vulvovaginal candidiasis: a systematic review and meta-analysis. European Journal of Obstetrics & Gynecology and Reproductive Biology 2013;167:132-136. [DOI] [PubMed] [Google Scholar]
Shahid 2009
- Shahid Z, Sobel JD.Reduced fluconazole susceptibility of Candida albicans isolates in women with recurrent vulvovaginal candidiasis: effects of long-term fluconazole therapy. Diagnostic Microbiology and Infectious Disease 2009;64(3):354-56. [DOI] [PubMed] [Google Scholar]
Sobel 1995
- Sobel JD, Brooker D, Stein GE, Thomason JL, Wermeling DP, Bradley B, Weinstein L.Single oral dose fluconazole compared with conventional clotrimazole topical therapy of candida-vaginitis. American Journal of Obstetrics and Gynecology 1995;172(4):1263-68. [DOI] [PubMed] [Google Scholar]
Sobel 2004b
- Sobel JD, Wiesenfeld HC, Martens M, Danna P, Hooton TM, Rompalo A, et al.Maintenance fluconazole therapy for recurrent vulvovaginal candidiasis. New England Journal of Medicine 2004;351(9):876-83.. [DOI] [PubMed] [Google Scholar]
Sobel 2006
- Sobel JD.Management of recurrent vulvovaginal candidiasis: unresolved issues. Current Infectious Disease Reports 2006;8(6):481-86. [DOI] [PubMed] [Google Scholar]
Sobel 2007
- Sobel JD.Vulvovaginal candidosis. Lancet 2007;369(9577):1961-71. [DOI] [PubMed] [Google Scholar]
Sobel 2014
- Sobel JD.Factors involved in patient choice of oral or vaginal treatment for vulvovaginal candidiasis. Patient Preference and Adherence 2013;8:31-34. [DOI: 10.2147/PPA.S8984] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sobel 2016
- Sobel JD.Recurrent vulvovaginal candidiasis. American Journal of Obstetrics & Gynecology 2016;214(1):15-21. [DOI] [PubMed] [Google Scholar]
Stein 1993
- Stein GE, Mummaw N.Placebo-controlled trial of itraconazole for the treatment of acute vaginal candidiasis. Antimicrobial Agents and Chemotherapy 1993;37(1):89-92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Therapeutic Guidelines 2015
- Therapeutic Guidelines.eTG: Antibiotic. updated June 2019 edition. Melbourne, Victoria: Therapeutic Guidelines Limited, 2015. [Google Scholar]
Van Kessel 2003
- Van Kessel K, Assefi N, Marrazzo J, Eckert L.Common complementary and alternative therapies for yeast vaginitis and bacterial vaginosis: A systematic review. Obstetrical & Gynecological Survey 2003;58(5):351-58. [DOI] [PubMed] [Google Scholar]
Watson 2002
- Watson MC, Grimshaw JM, Bond CM, Mollison J, Ludbrook A.Oral versus intra-vaginal imidazole and triazole anti-fungal agents for the treatment of uncomplicated vulvovaginal candidiasis (thrush): a systematic review. British Journal of Obstetrics and Gynaecology 2002;109:85-95. [DOI] [PubMed] [Google Scholar]
Watson 2007
- Watson C, Calabretto H.Comprehensive review of conventional and non-conventional methods of management of recurrent vulvovaginal candidiasis. Australian and New Zealand Journal of Obstetrics and Gynaecology 2007;47:262-272. [DOI] [PubMed] [Google Scholar]
Watson 2011
- Watson C, Pirotta M.Recurrent vulvovaginal candidiasis - current management. Australian Family Physician March 2011;40(3):149-151. [PubMed] [Google Scholar]
Wildfeuer 1997
- Wildfeuer A, Laufen H, Schmalreck AF, Yeates RA, Zimmermann T.Fluconazole: comparison of pharmacokinetics, therapy and in vitro susceptibility. Mycoses 1997;40(7-8):259-65. [DOI] [PubMed] [Google Scholar]
Xie 2017
- Xie HY, Feng D, Wei DM, Mei L, Chen H, Wang X, Fang F.Probiotics for vulvovaginal candidiasis in non-pregnant women. Cochrane Database of Systematic Reviews 2017, Issue 11. Art. No: CD010496. [DOI: 10.1002/14651858.CD010496.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Young 2001
- Young G, Jewell D.Topical treatment for vaginal candidiasis (thrush) in pregnancy. Cochrane Database of Systematic Reviews 2001, Issue 4. Art. No: CD000225. [DOI: 10.1002/14651858.CD000225] [DOI] [PubMed] [Google Scholar]