

Abstract
Neurodegenerative disorders such as Alzheimer's disease (AD) represent a mounting public health challenge. As these diseases are difficult to diagnose clinically, biomarkers of underlying pathophysiology are playing an ever‐increasing role in research, clinical trials, and in the clinical work‐up of patients. Though cerebrospinal fluid (CSF) and positron emission tomography (PET)‐based measures are available, their use is not widespread due to limitations, including high costs and perceived invasiveness. As a result of rapid advances in the development of ultra‐sensitive assays, the levels of pathological brain‐ and AD‐related proteins can now be measured in blood, with recent work showing promising results. Plasma P‐tau appears to be the best candidate marker during symptomatic AD (i.e., prodromal AD and AD dementia) and preclinical AD when combined with Aβ42/Aβ40. Though not AD‐specific, blood NfL appears promising for the detection of neurodegeneration and could potentially be used to detect the effects of disease‐modifying therapies. This review provides an overview of the progress achieved thus far using AD blood‐based biomarkers, highlighting key areas of application and unmet challenges.
Keywords: Alzheimer, Aβ, biomarkers, blood, P‐tau
Subject Categories: Biomarkers, Neuroscience
This Review discusses recent advances in blood‐based biomarkers for Alzheimer's disease, highlighting the key areas of application and unmet challenges.

Glossary
- Amyloid PET
Aβ‐specific ligands for use with positron emission tomography
- Antibodies
immune proteins produced in response to an antigen
- Area under the receiver operating curve
a measure of the ability of a classifier to distinguish between positive and negative classes (i.e., normal and abnormal)
- Aβ plaques
abnormal extracellular deposits of the Aβ peptide
- Biomarkers
a biomarker is an objectively measurable parameter that can be treated as an indicator of biological processes or responses to a treatment
- Enzyme‐linked immunosorbent assays
though various ELISA variants all are characterized by the following elements: an antigen, one or several antibodies specific to that antigen, and a system to quantify the amount of antigen present
- Head‐to‐head study
a study design in which two methods are directly compared using data from the same individuals
- Immunomagnetic reduction platforms
a technique in which the concentration is measured by comparing changes in magnetic responses between free and conjugated magnetic nanoparticles
- Immunoprecipitation mass spectrometry assay
an assay combining immunoprecipitation and mass spectrometry. Using this approach, desired analytes are first selectively captured from solution prior to analysis with mass spectrometry
- Mild cognitive impairment
a state of cognitive impairment intermediate between those due to normal aging and dementia (i.e., objective cognitive deficits beyond that expected given their age and education yet of insufficient severity to meet criteria for dementia)
- Neurofibrillary tangles
abnormal intracellular accumulations of the tau protein
- Neuroinflammation
astrocytic and microglial activation
- Preanalytical variables
these include tube type and time from blood collection to centrifugation and pipetting of the plasma
- Sensitivity
the ability of a test to correctly identify patients with a disease
- Single‐molecule array
a digital assay technique allowing for the measurement of single‐molecule immunocomplexes
- Specificity
the ability of a test to correctly identify people without the disease
- Tau PET
tau‐specific ligands for use with positron emission tomography
Introduction
Neurodegenerative disorders such as Alzheimer's disease (AD) are the leading causes of dementia and carry immense social and economic costs. Worldwide, an estimated 50 million people currently live with dementia, with this figure projected to exceed 80 million by 2030 (Prince et al, 2016). With increasing age as the greatest risk factor for dementia, a driving factor behind these rising prevalence figures is increased longevity (Winblad et al, 2016); as such, these disorders represent a major and increasing global health challenge.
On clinical grounds alone, the differential diagnosis of AD can prove challenging, even for dementia experts (Beach et al, 2012; Salloway et al, 2014). Accurate prognosis and disease monitoring are also difficult when relying on clinical information only. As a result, biomarkers have come to play an increasingly important role in the field. Providing an objective measure of relevant pathophysiology in vivo, biomarkers are now included in modern research diagnostic criteria for AD (Dubois et al, 2007, 2014; Albert et al, 2011; Jack et al, 2011, 2018; McKhann et al, 2011; Sperling et al, 2011a) and are recommended for use in clinical trials by regulatory agencies (Hampel et al, 2010). Further, the use of biomarkers is important in the context of treatment, both in terms of ensuring that AD patients access available symptomatic treatments and in terms of providing an accurate prognosis early on in the disease course should disease‐modifying therapies become available for AD (Abbasi, 2018). The AD biomarker research field is now moving from studies of group‐level associations to subject‐level diagnosis and prognosis in real‐world scenarios. Examples of this include recent work aiming to assess the risk for cognitive decline using biomarkers in patients with mild cognitive impairment (MCI) (van Maurik et al, 2017, 2019a, 2019b; Cullen et al, 2021a). However, a substantial irreversible neuronal loss can already be seen by this stage—which may reduce the likelihood of disease‐modifying therapies to prevent dementia onset (Sperling et al, 2011b). There is therefore now an increasing focus also on cognitively unimpaired (CU) older individuals at risk for progression to AD dementia on the basis of biomarker evidence of brain AD pathology (Sperling et al, 2014; Cullen et al, 2021b).
Due to it being in direct contact with the central nervous system, cerebrospinal fluid (CSF) has proven an ideal source of information for the detection and measurement of biochemical abnormalities within the brain (Hampel et al, 2012); examples include CSF amyloid‐β (Aβ) 42—alone, and in ratio with Aβ40 (Aβ42/Aβ40)—reflecting Aβ deposition; phosphorylated tau (P‐tau), reflecting tau pathology; and neurofilament light (NfL) (Khalil et al, 2018), reflecting neurodegeneration. These abnormalities can also be measured using positron emission tomography (PET) with compounds (tracers) specific for Aβ, tau, and synaptic impairment. The global use of CSF and imaging‐based biomarkers remains limited owing to the perceived invasiveness of lumbar punctures and the high cost and low availability of PET imaging (Duits et al, 2016). This has led to a growing interest in the use of blood‐based biomarkers, with recent work showing promising results (Nakamura et al, 2018; Palmqvist et al, 2019b; Schindler et al, 2019; Janelidze et al, 2020a; Karikari et al, 2020b, 2021). In the present review, we aim to provide an overview of the progress achieved thus far using AD blood‐based biomarkers and to highlight key areas of application and remaining challenges.
Markers of Aβ pathology (Aβ42/Aβ40)
Following the discovery of multiple C‐terminal forms of Aβ, the 42‐amino acid isoform of Aβ (Aβ42) was found to be highly aggregation‐prone and predominant in diffuse and cored plaques in AD (Iwatsubo et al, 1994; Tamaoka et al, 1994). Using enzyme‐linked immunosorbent assays (ELISAs) specific to Aβ42, a marked reduction in CSF Aβ42 was seen in AD (Motter et al, 1995; Blennow & Hampel, 2003), with levels shown to correlate inversely with cortical plaque load at post‐mortem (Strozyk et al, 2003; Tapiola et al, 2009) and in biopsy studies (Seppala et al, 2012). Combining Aβ42 with Aβ40 (using a ratio) corrects inter‐individual differences in Aβ processing and possible preanalytical confounders and increases concordance with amyloid PET (Hansson et al, 2019).
Assays
Plasma Aβ assays include ELISA‐based immunoassays on the Luminex xMAP (Hansson et al, 2010), single‐molecule array (Simoa) (Janelidze et al, 2016), Elecsys (Palmqvist et al, 2019b), and immunomagnetic reduction (IMR) platforms as well as immunoprecipitation mass spectrometry (IP/MS) assays (Pannee et al, 2014; Ovod et al, 2017; Schindler et al, 2019). For the IP/MS assays, plasma Aβ is enriched via immunoprecipitation with Aβ antibodies coated onto paramagnetic beads. These antibodies are either directed to the mid‐region (Ovod et al, 2017; Nakamura et al, 2018) or N‐terminal (Pannee et al, 2014) part of Aβ. Stable isotope‐labeled synthetic Aβ peptides (e.g., Aβ42 and Aβ40) are then used as mass spectrometry quantification standards. In the study by Nakamura et al, however (Nakamura et al, 2018), Aβ38 was used as a single stable isotope‐labeled standard for all Aβ isoforms.
Early work using Luminex xMAP technology in plasma failed to replicate the observed decrease of Aβ42 seen in CSF (Song et al, 2011; Toledo et al, 2013; Rembach et al, 2014; Swaminathan et al, 2014; Olsson et al, 2016), likely due to the use of clinical diagnosis as the standard of truth, analytical limitations inherent to these methods (e.g., epitope masking by hydrophobic Aβ peptides (Kuo et al, 1999)) and, possibly, to peripheral tissues contributing to the global pool of plasma Aβ (Li et al, 1998; Kuo et al, 2000; Roher et al, 2009; Hansson et al, 2010). In 2016, however, using a Simoa assay for Aβ—a technique allowing for the reduction of matrix effects via predilution of samples due to its very high analytical sensitivity (Rissin et al, 2010, 2011; Zetterberg et al, 2011)—plasma Aβ was found to be reduced in AD compared to controls and patients with MCI and vascular dementia and to separate abnormal from normal amyloid PET scans with moderate accuracy (AUC between 0.62 and 0.68) (Janelidze et al, 2016; Verberk et al, 2018). Higher AUCs have since been reported using a modified version of the Simoa assay with different antibodies (Verberk et al, 2020b). Simoa studies were followed by several studies using IP/MS (Ovod et al, 2017; Nakamura et al, 2018; Schindler et al, 2019). Using amyloid PET status as outcome, plasma Aβ42/Aβ40 showed high accuracy in CU individuals (Schindler et al, 2019) and across CU individuals and patients with mild‐to‐moderate AD (AUCs of between 0.84 and 0.97) (Ovod et al, 2017; Nakamura et al, 2018).
In a recent study that compared several IP/MS assays and immunoassays using a head‐to‐head design (Janelidze et al, 2021), certain IP/MS methods were shown to have superior performance to other IP/MS methods and all immunoassays using CSF Aβ42/40 and Aβ‐PET status as outcome. Though promising and highlighting the potential of plasma Aβ as an AD biomarker, IP/MS‐ and Simoa‐based studies are comparatively costly and require extensive development before they can be used in primary care or in screening large numbers of participants for AD clinical trials. Although this recent progress with high precision plasma Aβ measures has resulted in commercially available lab‐developed blood tests for the detection of AD pathology, fully automated, high‐throughput, and highly reliable analysis methods would facilitate implementation more broadly in clinical practice. Indeed, in the study by Janelidze et al (2021) comparing IP/MS and immunoassays, the Elecsys immunoassays (Roche Diagnostics) (Hansson et al, 2018) showed the numerically highest AUC (0.740). This is likely due to the immunoassays being fully automated and having very high analytical reliability and precision. Additional work using the Elecsys immunoassays for plasma Aβ42/Aβ40 showed that subjects could be differentiated based on their Aβ status with an AUC of 0.80 (Palmqvist et al, 2019b). The addition of APOE ε4 status—and, to a lesser extent, T‐tau and NfL—increased the AUC significantly to around 0.85–0.87, though accuracy was lower compared to those reported in the IP/MS studies (Ovod et al, 2017; Nakamura et al, 2018; Schindler et al, 2019).
In a recent study, however, a head‐to‐head comparison of plasma Aβ42/Aβ40 quantified with commercially available ELISA kits (EUROIMMUN) and prototype SIMOA assays (Amyblood; ADx NeuroSciences) (De Meyer et al, 2020) that used the same sets of monoclonal detector and capture antibodies showed that both provided identical accuracy for detecting amyloid PET status in a cohort of nondemented elderly individuals. The superior performance of these novel ELISAs can be attributed to technological advancements, including the use of C‐ and N‐terminal antibodies (Pesini et al, 2012), improved conjugation method (Cirrito et al, 2003; Lopez et al, 2008), and an improved understanding of the effects of preanalystical variables (Lachno et al, 2009). While head‐to‐head comparisons are required between the different ELISAs, their improved performance carries potentially important implications due to their being much more widely available than Simoa. Recently, novel ready‐to‐use Simoa‐based immunoassays (“Amyblood”) were developed to detect full‐length Aβ1–42 and Aβ1–40 (Thijssen et al, 2021b), with the Amyblood Aβ42/Aβ40 ratio showing technical and clinical performance comparable to the Quanterix triplex and Euroimmun ELISAs but superior specificity and selectivity than the Quanterix triplex kit.
A major limitation of plasma Aβ42/40, however, is that its levels are only decreased by 10–20% in individuals with cerebral Aβ pathology, compared to 40–60% for CSF Aβ42/40 (Nakamura et al, 2018; Verberk et al, 2018; Palmqvist et al, 2019a, 2019b; Schindler et al, 2019). This is likely due to plasma Aβ levels being affected by Aβ metabolism outside the brain (Li et al, 1998; Kuo et al, 2000; Roher et al, 2009; Hansson et al, 2010). As a result, plasma Aβ42/40 levels can be affected by small measurement variations caused by preanalytical handling (such as tube type and time from blood collection to centrifugation and pipetting of the plasma) and analytical performance (Rozga et al, 2019). This, in turn, can affect subject‐level classification (i.e., negative or positive for Aβ pathology). Given the more robust changes seen for Aβ42/40 in CSF—as well as the robustness of this measure to the interfering effects of preanalytical factors (Hansson et al, 2019)—CSF Aβ42/40 has overall shown a higher diagnostic accuracy than plasma Aβ42/40 and is less susceptible to variations in its optimal cut‐point (Schindler et al, 2019). Possibly, combining plasma Aβ42/40 with P‐tau or GFAP using an algorithm may make plasma Aβ42/40 more robust to preanalytical factors; however, this has not yet been studied.
Differential diagnosis of AD dementia
Thus far, only one study has examined the ability of plasma Aβ42/Aβ40 to differentiate AD dementia from non‐AD dementia disorders (Palmqvist et al, 2020). Using immunoassays, however (Euroimmun ELISAs)—as opposed to mass spectrometry methods—the study reported poor diagnostic accuracy (AUC of 0.62) when using clinically diagnosed participants (AD dementia [n = 121] vs a non‐AD group [n = 99] including 45 patients with Parkinson's disease (without or with dementia) or multiple system atrophy, 21 with progressive supranuclear palsy or corticobasal syndrome, 12 with vascular dementia, and 21 with behavioral variant frontotemporal dementia or primary progressive aphasia). The AUC of plasma Aβ42/Aβ40 was higher, however, when using neuropathologically confirmed cases (AUC of 0.72 for intermediate to high likelihood of AD [n = 34] vs non‐AD [n = 47], where primary neuropathological diagnoses included PART (seven possible, 11 definite), 13 PD, three PSP, two VaD, three with white matter changes due to infarcts, one ALS, one multiple sclerosis, one showing diffuse astrocytoma, two CBD, one FTLD with TDP‐43 pathology, and two with NFT predominant dementia) (Palmqvist et al, 2020).
Prediction of AD dementia and cognitive decline in MCI
Varying discriminative performance has been seen when differentiating MCI patients who converted to AD dementia from those that did not using plasma Aβ42/Aβ40 adjusted for age (AUC of 0.67) (Simren et al, 2021) and age, sex, education, and baseline MMSE (AUC ranging from 0.66 to 0.86 depending on cohort and assay) (Cullen et al, 2021a) (Table EV1). In a prospective study examining plasma Aβ42/Aβ40 and the risk of conversion from amnestic MCI to AD dementia, however, plasma Aβ42/Aβ40 at baseline adjusted for age, APOE ε4 status, and education carried an increased risk of progression (~70%) to AD dementia over 2 years (Perez‐Grijalba et al, 2019), with an AUC of 0.86 by comparison to stable MCI.
Prediction of AD dementia and cognitive decline in CU
In longitudinal studies that have examined the association between plasma Aβ42/Aβ40 and the risk of progression to MCI or AD dementia in CU individuals using up to 6 years follow‐up, time‐dependent receiver operating characteristic curves—a method which takes into account interindividual differences in follow‐up and conversion times—showed that Simoa‐based plasma Aβ42/Aβ40 had AUC values ≥ 0.85 across all yearly time points (range 0.85–0.92) (Stockmann et al, 2020). Plasma Aβ42/Aβ40 has also been shown to be associated with progression to both MCI and AD dementia (Verberk et al, 2018, 2021), independent of potential confounders (education; APOE carriership; or medication use for hypertension, hypercholesterolemia, and diabetes) and measures of neuroinflammation and neurodegeneration (plasma GFAP and NfL). Lower (more abnormal) plasma Aβ42/Aβ40 has also been shown to relate to a more pronounced decline in composite cognitive scores over time (adjusted for sex, age, education, treatment group, BMI, CDR, GDS score) (Giudici et al, 2020). This finding also held when using longitudinal MMSE scores. Similar results have been reported using domain‐specific findings, including attention, memory, language, and executive functioning (Verberk et al, 2020a).
Markers of tau pathology (P‐tau181, P‐tau217, and P‐tau231)
The identification of hyperphosphorylated tau as a major constituent of neurofibrillary tangles (Grundke‐Iqbal et al, 1986a, 1986b) led to the development of CSF assays for P‐tau (Iqbal & Grundke‐Iqbal, 1997) targeting specific serine and threonine amino acid residues. Though multiple phosphorylation sites exist on the tau protein (Portelius et al, 2008), the most commonly used assays for P‐tau detect phosphorylation at threonine 181 (P‐tau181). Using this measure, increased CSF P‐tau181 has been consistently shown in AD (Blennow et al, 2015). Using several different outcomes, however—including the separation of AD dementia from non‐AD neurodegenerative disorders and correlations with amyloid and tau PET—P‐tau217 has shown somewhat better performance than P‐tau181 (Janelidze et al, 2020b). Recently, P‐tau231 has also been detected in CSF (Buerger et al, 2003; Suarez‐Calvet et al, 2020) and plasma (Ashton et al, 2021c).
Although previous studies assumed that soluble P‐tau measures reflected tau pathology in AD (Jack et al, 2018), direct correlations between soluble P‐tau and neuropathology or PET measures of tau typically only found moderate correlations (Buerger et al, 2006, 2007; Mattsson et al, 2017b; La Joie et al, 2018).
More recent studies have instead linked changes in soluble P‐tau (for both CSF and plasma) to the accumulation of Aβ (Sato et al, 2018; Mattsson‐Carlgren et al, 2020a) and shown that changes in soluble P‐tau precede tau aggregation in AD as measured by PET or with neuropathology (Mattsson‐Carlgren et al, 2021).
Assays
In contrast to CSF where commercial P‐tau181 assays target mid‐region forms of tau phosphorylated at threonine 181 (Vanderstichele et al, 2006; Leitao et al, 2019; Lifke et al, 2019), the development of assays for P‐tau in blood have focused on N‐terminal to mid‐region tau fragments following the discovery that this is the predominant tau species in blood (Sato et al, 2018). For instance, Tatebe and colleagues (Tatebe et al, 2017) developed a Simoa‐based plasma P‐tau181 assay by replacing the detection antibody in an existing T‐tau assay with a monoclonal antibody specific for P‐tau181. This study was the first to report elevated levels of plasma P‐tau181 in AD dementia, yet the assay suffered from insufficient analytical sensitivity. Using electrochemiluminescence (ECL)‐based methods developed by Eli Lilly, significant increases in plasma P‐tau181 and P‐tau217 have been reported in AD (Mielke et al, 2018; Janelidze et al, 2020a). Novel P‐tau181 and P‐tau217 assays targeting P‐tau isoforms containing the N‐terminal amino acid 6–18 epitope were then later developed (Karikari et al, 2020b, 2021). Though designed for use with blood, these assays also work for the quantification of P‐tau in CSF (Janelidze et al, 2020a; Karikari et al, 2020a; Suarez‐Calvet et al, 2020). Two additional Simoa‐based assays from Janssen targeting P‐tau217 and phosphorylation at amino acid 212 have also been recently described (Triana‐Baltzer et al, 2020, 2021) as well as a study providing a direct comparison of modified versions of the ECL‐based Eli Lilly assays for P‐tau217 and P‐tau181 (Thijssen et al, 2021a) that differed only in their epitope‐specific capture antibodies.
Quantification of P‐tau231 in plasma has also recently been described using a phospho‐specific cis‐conformational monoclonal antibody ADx253 as a capture antibody and a biotin‐conjugated N‐terminal anti‐tau mouse monoclonal antibody for detection (Ashton et al, 2021c). A schematic overview of P‐tau assays is provided in Fig 1.
Figure 1. A schematic overview of the included P‐tau assays.
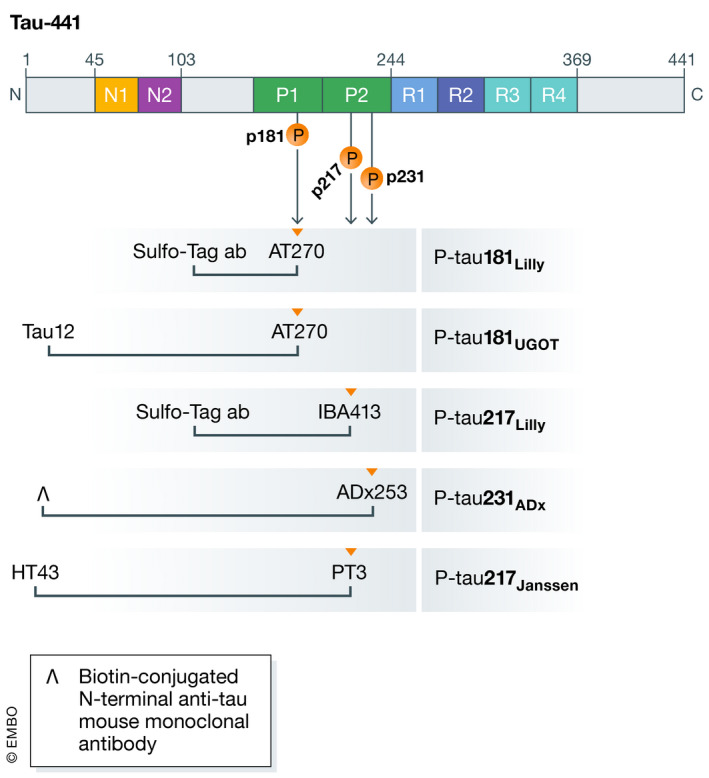
Schematic illustration of full‐length tau‐441, including N‐terminal, proline‐rich region, microtubuli binding domain, and C‐terminal. Anti‐tau antibodies are indicated for each of the five included P‐tau assays under the respective epitope region. P‐tau181UGOT is the P‐tau181 assay from the University of Gothenburg, as detailed in Karikari et al (2021).
For P‐tau231ADx, the inverted V symbol represents a biotin‐conjugated N‐terminal anti‐tau mouse monoclonal antibody, as detailed in Ashton et al (2021c).
Differential diagnosis of AD dementia
Increasingly, biomarkers are being incorporated into the clinical work‐up of patients presenting with cognitive impairment, in part due to the difficulty in differentiating AD from related non‐AD neurodegenerative disorders early on in the disease course (Beach et al, 2012; Salloway et al, 2014). In recent studies that have examined AD plasma biomarkers (Janelidze et al, 2020a; Karikari et al, 2020b; Palmqvist et al, 2020; Thijssen et al, 2020), diagnostic accuracies (AUC) for the separation of AD from non‐AD dementia disorders using clinical diagnosis as the standard of truth have ranged from 0.81 (Palmqvist et al, 2020) to 0.89 (Thijssen et al, 2020). In a larger cohort, plasma P‐tau181 was shown to differentiate AD dementia from non‐AD dementia disorders with a somewhat higher AUC (0.94), similar to those achieved using CSF P‐tau181 or tau PET (Janelidze et al, 2020a). More importantly, plasma P‐tau181 has been shown to be able to differentiate AD dementia from other neurodegenerative disorders using neuropathologically confirmed cases, with AUCs ranging from 0.85 (Janelidze et al, 2020a) to 0.95 (Thijssen et al, 2020). High accuracy for plasma P‐tau181 for discriminating AD from non‐pathologies when using neuropathological diagnoses as standard of truth was also reported (AUC of 0.97) using measures taken 8 years prior to autopsy (Lantero Rodriguez et al, 2020).
Using plasma P‐tau217, AD dementia cases were separated from non‐AD disorders with an AUC of 0.96 (Palmqvist et al, 2020) (Table EV1). Using neuropathologically confirmed cases, AUCs ranged from 0.89 to 0.98 (Palmqvist et al, 2020) for intermediate to high likelihood of AD, respectively (Mirra et al, 1991; 1997). In a recent head‐to‐head study comparing plasma P‐tau181 and P‐tau217 (Thijssen et al, 2021a)—measured using electrochemiluminescence‐based assays differing only in the biotinylated antibody epitope—though both measures showed high AUC values for differentiating pathology‐confirmed AD from pathologically confirmed FTLD, P‐tau217 slightly outperformed P‐tau181 (AUC 0.93 vs 0.91) when separating clinically diagnosed AD from FTLD syndromes. Plasma P‐tau231 has also been recently shown to have high accuracy for AD using clinical (AUC of 0.93) and neuropathological diagnoses (AUC of 0.99) using samples drawn 4.2 years on average prior to post‐mortem (Ashton et al, 2021c).
Prediction of AD dementia and cognitive decline in MCI
In patients with MCI, baseline plasma P‐tau181 levels have been shown to be increased in those who progressed to AD dementia compared to those that did not develop dementia or that developed dementia due to other causes (Janelidze et al, 2020a; Therriault et al, 2021) (Table EV2). Plasma P‐tau181 levels were also elevated in Aβ‐positive MCI who progressed to AD dementia by comparison to both Aβ‐positive and Aβ‐negative CU and MCI who did not convert to AD dementia. After adjusting for age, sex, and education, higher baseline plasma P‐tau181 levels were associated with a greater risk of progression to AD dementia, with a hazard ratio nearly identical to that for CSF P‐tau181. Similar findings were obtained when adjusting plasma P‐tau181 for plasma T‐tau, Aβ42/Aβ40, and NfL (Janelidze et al, 2020a). In a related study, survival analysis showed that high baseline plasma P‐tau181 was associated with an increased risk of progression to AD dementia in MCI over 84 months, as compared with Aβ‐negative CU, with similar findings observed using a shorter follow‐up interval of 48 months (Karikari et al, 2021). Using both follow‐up intervals, the performance of plasma P‐tau181 was similar to that for CSF P‐tau181. Plasma P‐tau181 has also been shown to outperform other plasma biomarkers for separating MCI patients who converted to AD dementia from those that did not, though the AUC reported in this study was modest (0.77) (Simren et al, 2021).
Using plasma P‐tau217, higher baseline levels were observed in MCI patients who progressed to AD dementia (Mattsson‐Carlgren et al, 2020b). Further, plasma P‐tau217 levels were found to increase over time, as compared to stable P‐tau217 levels in MCI patients who did not develop AD dementia. In work addressing the association between longitudinal plasma P‐tau217 and longitudinal cognition in MCI (Mattsson‐Carlgren et al, 2020b), increases in plasma P‐tau217 were associated with worsening cognition. Similar findings have been reported for plasma P‐tau181 (Chen et al, 2021; Therriault et al, 2021).
Prediction of AD dementia and cognitive decline in CU
In CU individuals, elevated baseline plasma P‐tau181 levels (adjusted for age, sex, and education) were found to carry an increased risk of progression to AD dementia (mean follow up of 4.9 years), with a hazard ratio nearly equivalent to that for CSF P‐tau181 (Janelidze et al, 2020a) (Table EV3). This finding held even after adjusting plasma P‐tau181 levels for plasma T‐tau, Aβ42/Aβ40, and NfL. High plasma P‐tau181 has also been shown to carry an increased risk of AD dementia in Aβ‐positive CU as compared with Aβ‐negative CU over 84 months and over a shorter interval of 48 months (Karikari et al, 2021). Here, however, the hazard ratio of CSF P‐tau181 was superior to that of plasma P‐tau181 (5.4 vs 3.25, respectively). Over a longer interval of 100 months, CU individuals who were plasma P‐tau181‐positive at baseline showed a faster cognitive decline compared to CU individuals who were P‐tau181‐negative (Karikari et al, 2021). Similar findings were shown over 60 months. Longitudinal increases in plasma P‐tau181 have also been found to be associated with future cognitive decline in CU individuals (Moscoso et al, 2021; Therriault et al, 2021). In a study examining the associations between longitudinal plasma P‐tau217 and longitudinal cognition (Mattsson‐Carlgren et al, 2020b), higher plasma P‐tau217 was associated with worsening cognition in CU individuals using both MMSE and mPACC as outcomes. In an analysis combining CU and MCI individuals (Pereira et al, 2021b), plasma P‐tau181 and P‐tau217 levels were associated with longitudinal decline in MMSE scores; however, P‐tau217 provided the best fit to the data and a larger effect size compared to P‐tau181. When combining plasma P‐tau181, P‐tau217, Aβ42/40, and NfL in a multivariate model, only P‐tau217 was a significant independent predictor of cognitive decline.
Markers of neurodegeneration
Among fluid biomarkers of neurodegeneration, NfL is one of the most promising. A marker of subcortical large‐caliber axonal degeneration (Hoffman et al, 1987; Norgren et al, 2003), CSF levels of NfL are elevated in AD and ever more so in ALS, FTD, and atypical parkinsonian disorders (i.e., PSP, MSA, and CBD) (Khalil et al, 2018) and after acute brain injury (e.g., stroke, traumatic brain injury or cardiac arrest). Due it being increased in multiple neurological disorders, NfL is considered to be a nonspecific marker of neuronal injury (preferentially axonal injury). Importantly, higher levels of NfL are associated with faster disease progression and higher rates of brain atrophy in most neurodegenerative disorders (Khalil et al, 2018; Preische et al, 2019); as such, NfL can be regarded as a measure of the intensity of ongoing neurodegeneration. NfL can also be measured in blood, where levels are elevated in the prodromal (Mattsson et al, 2017a) and dementia stages (Mattsson et al, 2019) of sporadic AD as well as in autosomal dominant AD (Preische et al, 2019; Quiroz et al, 2020). Similar to CSF, however, plasma NfL is not specific for AD and is elevated in all neurodegenerative disorders, in particular FTD (Rohrer et al, 2016), ALS (Verde et al, 2019) and atypical parkinsonian disorders (Donker Kaat et al, 2018). Other blood‐based markers of neurodegeneration, including SB100 and T‐tau, have also been described in AD (Olsson et al, 2016; Michetti et al, 2019); the clinical relevance of these measures has been shown to be comparatively low, however, and as such will not be covered here.
Assays
Plasma NfL has historically been measured using ELISA and ECL assay technology. However, the sensitivity of ELISA for quantifying plasma NfL has been found to be insufficient, and ECL is not sufficiently sensitive to detect the lowest concentrations of plasma NfL (Li & Mielke, 2019). Therefore, studies now utilize the ultra‐sensitive Simoa platform due to its greater sensitivity (Disanto et al, 2017; Gaetani et al, 2019). Plasma NfL concentrations in studies on AD (Mattsson et al, 2017a, 2019; Weston et al, 2017; Lewczuk et al, 2018; Mielke et al, 2019; Preische et al, 2019; Benedet et al, 2020) have since been measured on the Simoa platform (HD‐1 Analyser, Quanterix) (Gisslen et al, 2016; Rohrer et al, 2016; Disanto et al, 2017; Thijssen et al, 2021a).
Differential diagnosis of AD dementia
Using plasma NfL, poor diagnostic performance has been reported for the separation of bvFTD patients from those with AD dementia (AUC of 0.68) (Steinacker et al, 2018) (Table EV1). Similar findings have been reported when separating AD dementia from a broader group of non‐AD disorders (AUC of 0.75), including bvFTD, non‐fluent/agrammatic variant of primary progressive aphasia (nfPPA), semantic variant of progressive aphasia (svPPA), progressive supranuclear palsy (PSP), corticobasal syndrome (CBS), and ALS‐FTD (Illan‐Gala et al, 2021). In another study (Palmqvist et al, 2020), plasma NfL had an AUC of 0.51 for separating participants with a high likelihood of AD (tangles in neocortex and moderate‐to‐frequent Aβ plaques) from non‐AD participants (those with none‐to‐sparse Aβ plaques) based on neuropathological assessment (Mirra et al, 1991) and 0.50 for clinical AD dementia vs other neurodegenerative disorders. In a recent study, plasma NfL showed an AUC of 0.82 for separating clinically diagnosed AD dementia from patients with FTLD syndromes (Thijssen et al, 2021a), and AUCs of 0.97 and 0.96 for distinguishing neuropathologically confirmed AD from neuropathologically confirmed FTLD‐tau and FTLD‐TDP cases, respectively. When examining plasma NfL's ability to differentiate AD dementia from various non‐AD neurodegenerative disorders in two multicenter cohorts (Ashton et al, 2021a), AUCs ranged from 0.53 (PD/PDD) to 0.88 (ALS).
Prediction of AD dementia and cognitive decline in MCI
While those MCI patients with a positive Aβ‐biomarker have been shown to have higher plasma NfL levels than Aβ‐negative MCI, no differences in plasma NfL levels have been observed between Aβ‐positive patients who progressed to AD dementia after at least 2 years follow‐up and Aβ‐positive patients who did not (Mattsson et al, 2017a) (Table EV2). Elevated plasma NfL levels have also been associated with progression from MCI to all‐cause dementia over intervals of 2 and 4 years (Cullen et al, 2021a). Higher plasma NfL has also been associated with worse performance on several cognitive tests, including MMSE, ADAS‐COG 11, delayed recall of the WMS logical memory II, TMT‐B score, and WAIS‐R digit symbol substitution test score (Mattsson et al, 2017a), as well as a cognitive composite score across the cognitive domains of memory (free and total recall of the Free and Cued Selective Reminding Test [FCSRT]), language (the Category Naming Test), executive function (the DSST‐WAISR), and orientation (10 MMSE orientation items) (He et al, 2021).
Associations between increases in NfL and cognitive decline in MCI have also been reported using longitudinal data (Mattsson et al, 2019; He et al, 2021). In multivariable analyses combining MCI and CU individuals—adjusting for age, sex, and education—baseline plasma NfL was not found to be significantly associated with cross‐sectional cognitive measures (Mielke et al, 2019). Higher levels of baseline plasma NfL were significantly associated with declines in global cognition, however (Mielke et al, 2019). Higher baseline plasma NfL and longitudinal increases were both shown to associate with global cognition (Moscoso et al, 2021); this was reported in a clinically impaired group, however, though nearly three quarters had a diagnosis of MCI.
Prediction of AD dementia and cognitive decline in CU
Elevated plasma NfL has also been shown to carry an increased risk of all‐cause dementia (de Wolf et al, 2020; Verberk et al, 2021) and dementia due to AD (Verberk et al, 2021) in large‐scale prospective population‐based and memory clinic‐based cohorts. Among CU individuals, cross‐sectional and longitudinal measures of plasma NfL have been shown not to be significantly associated with cognition (Mattsson et al, 2017a, 2019) (Table EV3). In multivariate analyses (adjusted for age, sex, and education) combining CU and MCI individuals, no significant associations were found between plasma NfL levels at baseline and cross‐sectional cognitive measures (Mielke et al, 2019). Significant associations were found, however, between higher baseline plasma NfL and longitudinal cognition (Mielke et al, 2019). Other work showed no significant associations between plasma NfL and cognitive decline (Moscoso et al, 2021) when accounting for plasma P‐tau181.
Markers of neuroinflammation
Increasing evidence indicates that neuroinflammation plays an important role in AD and related dementia disorders (Calsolaro & Edison, 2016; Ardura‐Fabregat et al, 2017). Relevant biomarkers here include glial (astrocytic) proteins such as YKL‐40 (also known as chitinase‐3‐like‐1 protein), S100 calcium‐binding protein B (S100B), and glial fibrillary acidic protein (GFAP) (Carter et al, 2019). GFAP forms a major part of the cytoskeleton of astrocytes and is a marker of astroglia activation (Hol & Pekny, 2015). CSF levels of GFAP have been found to be significantly increased in AD and related neurodegenerative diseases compared to CU individuals (Ishiki et al, 2016; Abu‐Rumeileh et al, 2019). Plasma GFAP levels are elevated in CU older adults at risk of AD due to amyloid PET positivity (Chatterjee et al, 2021). As GFAP levels appear to increase in response to Aβ and tau aggregation (Garwood et al, 2017), GFAP will probably not be used as a marker of neuroinflammation but instead more often as a marker of Aβ.
Assays
Studies examining the role of blood GFAP in AD have so far all used Simoa technology using the Human GFAP Discovery Kit from Quanterix (Lexington, MA, USA) (Oeckl et al, 2019; Cicognola et al, 2021; Pereira et al, 2021a; Verberk et al, 2021).
Differential diagnosis of AD dementia
Using Simoa technology, significantly increased serum GFAP levels were observed in AD as compared to patients with bvFTD (Oeckl et al, 2019). Further, serum GFAP discriminated AD from bvFTD patients with 89% sensitivity and a specificity of 79% (Oeckl et al, 2019) (Table EV1).
Prediction of AD dementia and cognitive decline in MCI and CU
When using progression from MCI to AD dementia as outcome, plasma GFAP had an AUC of 0.84 (Cicognola et al, 2021) (Table EV2). The addition of age and APOE ε4 did not improve diagnostic accuracy. MCI patients who converted to AD dementia also showed steeper slopes when looking at longitudinal GFAP, as compared to stable MCI (Cicognola et al, 2021). Serum GFAP levels have also been shown to predict future cognitive decline and progression to dementia in CU individuals (Verberk et al, 2021) (Table EV3). Plasma GFAP levels have also been shown to be associated with cognitive decline in a cohort combining individuals with and without cognitive impairment (Pereira et al, 2021a). No significant results were found when the analyses were conducted in the CU and CI groups separately, however.
Diagnostic algorithms
Though disclosing a diagnosis of MCI is challenging for clinicians, patients, and their families (Whitehouse et al, 2004), findings suggest that the majority of people wish to be informed, particularly if AD is the underlying cause (Marzanski, 2000). In addition, having this information has been shown to change patient management (Rabinovici et al, 2019). Applying a multivariate approach to plasma biomarkers (Aβ42/Aβ40, P‐tau181, T‐tau, and NfL), Janelidze et al showed that P‐tau181 best predicted longitudinal conversion to AD dementia (Janelidze et al, 2020a) (Table EV4). Building on this work by applying the recent Aβ (A), tau (T), and neurodegeneration (N) classification system (Jack et al, 2016, 2018) to plasma AD biomarkers (Cullen et al, 2021a), a model combining P‐tau181 and NfL—but not Aβ42/Aβ40—was found to best predict cognitive decline (MMSE) and progression to AD dementia over a period of 4 years. Moreover, plasma‐based models showed either non‐inferiority or superior performance compared to corresponding CSF‐based models and outperformed a basic model consisting of age, sex, education, and baseline MMSE (Cullen et al, 2021a) (Table EV4). As a result of extensive internal and external validation analyses, the study by Cullen et al (2021a) provided an individualized online risk prediction tool for cognitive decline (MMSE, CDR‐SB, and conversion to AD dementia at 2 and 4 years after baseline) in patients with MCI (http://predictprogression.com). After entering age, sex, and baseline cognition (MMSE, CDR‐SB) into the tool, the user indicates biomarker status (positive or negative) for plasma (or CSF) Aβ42/Aβ40, P‐tau181, and NfL. The tool also allows for the testing of sparser models including the absence of biomarkers altogether or the availability of a subset only (http://predictprogression.com). The tool then returns linear and logistic regression model‐based prediction intervals and probabilities of conversion to AD dementia at 2 and 4 years after baseline.
When combining plasma biomarkers to predict cognitive decline in CU individuals (Cullen et al, 2021b), P‐tau217, Aβ42/Aβ40, and NfL together provided the most robust results. When examining progression to AD dementia, the combination of P‐tau217 and Aβ42/Aβ40 proved best, while P‐tau217, Aβ42/Aβ40, and NfL together proved best when examining conversion to all‐cause dementia (Cullen et al, 2021b) (Table EV4). Additional work has also shown that while high baseline GFAP and NfL were associated with an increased risk of all‐cause dementia, only GFAP remained significantly associated with an increased risk of dementia when both markers were entered together in the same model (Verberk et al, 2021). When adding plasma Aβ42/Aβ40 to this model, both GFAP and Aβ42/Aβ40 were independently associated with incident dementia, whereas NfL was not (Table EV4). When added to a model consisting of demographics, genetic, and clinical information (age, sex, education and APOE ε4 genotype and a composite cardiovascular and metabolic conditions score), plasma P‐tau181 significantly improved prediction of memory decline (using both binary and continuous data) in CU and MCI individuals (Therriault et al, 2021).
Though diagnostic algorithms—and machine learning‐based approaches, more broadly—are ultimately intended to support personalized medicine, allowing for individualization at the levels of diagnosis, prognosis and treatment, proper oversight, and validation of such tools are crucial. This includes ensuring the absence of technical errors that can result in erroneous risk scores and inappropriate generalization from the training sample without robust validation (Handelman et al, 2018). Additional studies must also address how well these and other algorithms perform in predicting AD in primary care settings and require validation in large, unselected populations, including ethnically diverse groups due to the risk of the algorithm accuracy varying across certain subpopulations, such as racial and ethnic minority groups (Grote & Berens, 2020). In such studies, it is important that the biomarkers are analyzed prospectively in a consecutive manner using pre‐defined cut offs when appropriate.
Clinical trials
For trial enrichment, blood‐based biomarkers can first help identify individuals with a high probability of having AD pathology—for instance, using plasma Aβ42/Aβ40 or P‐tau (Palmqvist et al, 2019b; Janelidze et al, 2020a). This approach is most likely needed in preclinical AD trials and may substantially reduce the number of negative CSF and PET examinations commonly seen during the screening phase for disease‐modifying trials (Cummings, 2019; Palmqvist et al, 2019b; Jack, 2020; Sperling et al, 2020). One possibility is that blood‐based biomarkers can be used as pre‐screening tools to select individuals for further, more definitive testing with CSF or PET examinations. This is likely to be the case when CSF or PET is being used to monitor pharmacodynamic treatment effects. In another possible scenario, if blood‐based biomarkers can achieve sufficiently high performance, they may be used without additional CSF or PET testing (but perhaps in combination with other modalities that are likely to be available anyway, such as magnetic resonance imaging (MRI) or cognitive tests, to boost their performance). This is suitable in trials where CSF or PET is not needed to subsequently show drug target engagement or pharmacodynamic response in every participant.
Blood‐based AD biomarkers could also be used as pharmacodynamic markers to detect direct target engagement and disease‐modifying effects. Both of these effects are critical to establish an appropriate dose and increase confidence that treatment results in disease‐relevant outcomes. If pharmacodynamic effects have less variability and changes that predict standard cognitive or functional outcomes, these blood‐based biomarkers could have utility as surrogate endpoints resulting in shorter clinical trials or smaller sample sizes. In the early stages of drug development, this may support go/no‐go decisions for subsequent larger trials of drug candidates, before effects are demonstrated on measures of cognition or function. To our knowledge, however, there are no published reports of results of putative AD disease‐modifying treatments (DMTs) on blood‐based biomarkers for Aβ or P‐tau. However, we note that there are reports of reduced CSF P‐tau levels after treatment with certain anti‐Aβ agents (Salloway et al, 2014; Ostrowitzki et al, 2017). Future studies will likely show whether similar effects are seen on blood‐based P‐tau measures.
Natural history studies have shown that plasma P‐tau has properties that may make it suitable as a pharmacodynamic marker, including longitudinal increases over a few years in both the preclinical and prodromal stages of AD, and longitudinal correlations with measures of cognition and brain structure (Mattsson‐Carlgren et al, 2020b). Changes in soluble P‐tau represent downstream effects from drug engagement of Aβ. However, we note that alterations in soluble P‐tau are closely linked to aggregated Aβ in the early stages of AD before there are increases in tau PET (Mattsson‐Carlgren et al, 2020a). It therefore seems unclear whether drug‐related reductions in aggregated Aβ will be followed quickly by changes in soluble P‐tau (in either CSF or plasma) and if soluble P‐tau will precede potential changes in tau PET by months or years. The strongest evidence that a drug affects the biological mechanisms of disease in a meaningful way may come from a general marker of neurodegeneration, such as NfL. Though there are as yet—to our knowledge—no published data on plasma NfL in trials of AD DMTs, decreases in plasma NfL levels have been shown to parallel clinical improvement in other neurological diseases, including in spinal muscular atrophy and multiple sclerosis (Kuhle et al, 2019; Olsson et al, 2019), where effective DMTs exist. This increases the likelihood that results for changes in plasma NfL may be robustly translated and interpreted between trials, independent of the primary drug target.
Future directions and conclusions
Rapid progress has been made in the field of blood‐based biomarkers for AD due to advances in sensitive and precise assays. Recent work (Ashton et al, 2021b; Boccardi et al, 2021) addressing the validation of AD blood biomarkers highlighted the need for studies addressing clinical validity and utility. Figure 2 provides a summary of the most promising plasma‐based biomarkers across the clinical continuum of AD. Much work remains, however, to develop and validate blood‐based biomarkers for non‐AD neurodegenerative disorders in order to be able to reliably measure key pathologies such as α‐synuclein or TDP‐43. From a clinical practice perspective, plasma biomarkers could be incorporated into primary care to determine which patients with cognitive symptoms have a high probability of having AD and should be referred to secondary settings for treatment and, when deemed necessary, also more advanced biomarker‐based investigations such as CSF or PET. However, in many countries, most elderly patients with cognitive symptoms are managed in primary care alone (i.e., not referred to secondary or tertiary centers). In a primary care setting, blood‐based diagnostic algorithms might already be sufficient to improve the accuracy of a clinical AD dementia diagnosis and positively influence patient management and care. Additional studies are required, however, to assess how to optimally combine plasma biomarkers, or other accessible and cost‐effective measures such as MRI and cognitive tests, and to further develop predictive algorithms, which will be especially important in non‐demented patients with cognitive complaints where additional non‐AD biomarkers could be incorporated. As described above, however, further validation is required in large ethnically diverse populations that are unselected and that have a lower pre‐test probability of underlying AD. In clinical trials, plasma biomarkers may be used to screen for individuals suitable for inclusion as well as disease‐relevant pharmacodynamic endpoint markers. Key requirements for the implementation of plasma biomarkers in these areas, however, are the development of high precision fully automated methods that can be used in clinical laboratory practice, the development of standard operating procedures for collecting and handling of blood samples prior to analyses, guidelines to ensure study reproducibility (Mattsson‐Carlgren et al, 2020c), and appropriate use criteria to guide clinical use, as has been done for CSF AD biomarkers (Shaw et al, 2018) and amyloid PET (Johnson et al, 2013).
Figure 2. Most promising plasma‐based biomarkers across the clinical continuum of AD.
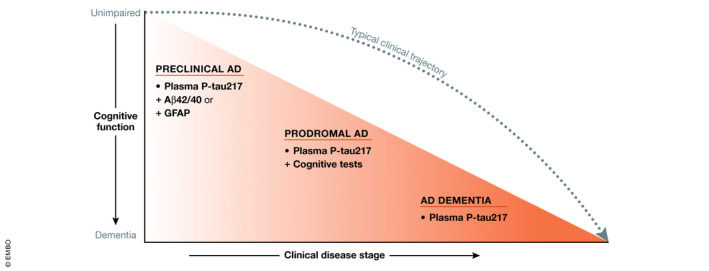
In this figure, cognitive function is represented on the y‐axis (top to bottom, unimpaired to dementia), with clinical disease stage shown on the x‐axis (preclinical AD, MCI due to AD [prodromal AD], and AD dementia). The dashed line represents the typical clinical trajectory from preclinical AD through prodromal and dementia stages. In each stage, the most promising plasma biomarker or plasma biomarker combination is indicated. For example, in preclinical AD, plasma P‐tau217 in combination with either plasma Aβ42/Aβ40 or GFAP is likely to prove best, while in prodromal AD plasma P‐tau217 in combination with simple to administer cognitive tests is likely best. In the AD dementia stage, plasma P‐tau217 alone is sufficient.
Author contributions
Drafting of the manuscript: AL, NM‐C, and OH. Critical revision of the manuscript for important intellectual content: AL, NM‐C, SJ, JLD, SP, and OH. Obtained funding and supervision.
For more information
Pending issues
Much work remains to develop and validate blood‐based biomarkers that can reliably measure non‐AD pathologies such as α‐synuclein or TDP‐43.
Studies are required in primary care settings to assess how best to combine plasma biomarkers with cognitive tests and other biomarkers and how to further develop algorithms capable of predicting cognitive decline and clinical progression.
Validation studies on plasma biomarkers are required in large ethnically diverse populations that are unselected and have a lower pre‐test probability of underlying AD pathology.
Overall, key requirements for the widespread use of plasma AD biomarkers include the development of high precision fully automated methods that can be used in clinical laboratory practice, standard operating procedures for the collection and handling of blood samples prior to analyses, reproducibility guidelines, and appropriate use criteria.
Supporting information
Table EV1
Table EV2
Table EV3
Table EV4
Acknowledgements
Work at the authors’ research center was supported by the Swedish Research Council (2016‐00906), the Knut and Alice Wallenberg foundation (2017‐0383), the Marianne and Marcus Wallenberg foundation (2015.0125), the Strategic Research Area MultiPark (Multidisciplinary Research in Parkinson’s disease) at Lund University, the Swedish Alzheimer Foundation (AF‐939932), the Swedish Brain Foundation (FO2021‐0293), The Parkinson foundation of Sweden (1280/20), the Konung Gustaf V:s och Drottning Victorias Frimurarestiftelse, the Skåne University Hospital Foundation (2020‐O000028), Regionalt Forskningsstöd (2020‐0314) and the Swedish federal government under the ALF agreement (2018‐Projekt0279).
Conflict of interest
AL, NMC, SJ, and SP report no disclosures. JLD is a former employee of Eli Lilly and Company. OH has acquired research support (for the institution) from Roche, GE Healthcare, Biogen, AVID Radiopharmaceuticals, and Euroimmun. In the past 2 years, he has received consultancy/speaker fees (paid to the institution) from Biogen and Roche.
EMBO Mol Med (2022) 14: e14408.
See the Glossary for abbreviations used in this article.
Contributor Information
Antoine Leuzy, Email: antoine.leuzy@med.lu.se.
Oskar Hansson, Email: oskar.hansson@med.lu.se.
References
- (1997 ) Consensus recommendations for the postmortem diagnosis of Alzheimer's disease. The National Institute on Aging, and Reagan Institute Working Group on Diagnostic Criteria for the Neuropathological Assessment of Alzheimer's disease. Neurobiol Aging 18: S1–S2 [PubMed] [Google Scholar]
- Abbasi J (2018) Promising results in 18‐month analysis of Alzheimer drug candidate. JAMA 320: 965 [DOI] [PubMed] [Google Scholar]
- Abu‐Rumeileh S, Steinacker P, Polischi B, Mammana A, Bartoletti‐Stella A, Oeckl P, Baiardi S, Zenesini C, Huss A, Cortelli P et al (2019) CSF biomarkers of neuroinflammation in distinct forms and subtypes of neurodegenerative dementia. Alzheimers Res Ther 12: 2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, Gamst A, Holtzman DM, Jagust WJ, Petersen RC et al (2011) The diagnosis of mild cognitive impairment due to Alzheimer's disease: recommendations from the National Institute on Aging‐Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 7: 270–279 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ardura‐Fabregat A, Boddeke EWGM, Boza‐Serrano A, Brioschi S, Castro‐Gomez S, Ceyzériat K, Dansokho C, Dierkes T, Gelders G, Heneka MT et al (2017) Targeting neuroinflammation to treat Alzheimer's disease. CNS Drugs 31: 1057–1082 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ashton NJ, Janelidze S, Al Khleifat A, Leuzy A, van der Ende EL, Karikari TK, Benedet AL, Pascoal TA, Lleó A, Parnetti L et al (2021a) A multicentre validation study of the diagnostic value of plasma neurofilament light. Nat Commun 12: 3400 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ashton NJ, Leuzy A, Karikari TK, Mattsson‐Carlgren N, Dodich A, Boccardi M, Corre J, Drzezga A, Nordberg A, Ossenkoppele R et al (2021b) The validation status of blood biomarkers of amyloid and phospho‐tau assessed with the 5‐phase development framework for AD biomarkers. Eur J Nucl Med Mol Imaging 48: 2140–2156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ashton NJ, Pascoal TA, Karikari TK, Benedet AL, Lantero‐Rodriguez J, Brinkmalm G, Snellman A, Schöll M, Troakes C, Hye A et al (2021c) Plasma p‐tau231: a new biomarker for incipient Alzheimer's disease pathology. Acta Neuropathol 141: 709–724 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beach TG, Monsell SE, Phillips LE, Kukull W (2012) Accuracy of the clinical diagnosis of Alzheimer disease at National Institute on Aging Alzheimer Disease Centers, 2005–2010. J Neuropathol Exp Neurol 71: 266–273 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benedet AL, Leuzy A, Pascoal TA, Ashton NJ, Mathotaarachchi S, Savard M, Therriault J, Kang MS, Chamoun M, Schöll M et al (2020) Stage‐specific links between plasma neurofilament light and imaging biomarkers of Alzheimer's disease. Brain 143: 3793–3804 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blennow K, Hampel H (2003) CSF markers for incipient Alzheimer's disease. Lancet Neurol 2: 605–613 [DOI] [PubMed] [Google Scholar]
- Blennow K, Dubois B, Fagan AM, Lewczuk P, de Leon MJ, Hampel H (2015) Clinical utility of cerebrospinal fluid biomarkers in the diagnosis of early Alzheimer's disease. Alzheimers Dement 11: 58–69 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Boccardi M, Dodich A, Albanese E, Gayet‐Ageron A, Festari C, Ashton NJ, Bischof GN, Chiotis K, Leuzy A, Wolters EE et al (2021) The strategic biomarker roadmap for the validation of Alzheimer's diagnostic biomarkers: methodological update. Eur J Nucl Med Mol Imaging 48: 2070–2085 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buerger K, Zinkowski R, Teipel SJ, Arai H, DeBernardis J, Kerkman D, McCulloch C, Padberg F, Faltraco F, Goernitz A et al (2003) Differentiation of geriatric major depression from Alzheimer's disease with CSF tau protein phosphorylated at threonine 231. Am J Psychiatry 160: 376–379 [DOI] [PubMed] [Google Scholar]
- Buerger K, Ewers M, Pirttila T, Zinkowski R, Alafuzoff I, Teipel SJ, DeBernardis J, Kerkman D, McCulloch C, Soininen H et al (2006) CSF phosphorylated tau protein correlates with neocortical neurofibrillary pathology in Alzheimer's disease. Brain 129: 3035–3041 [DOI] [PubMed] [Google Scholar]
- Buerger K, Alafuzoff I, Ewers M, Pirttila T, Zinkowski R, Hampel H (2007) No correlation between CSF tau protein phosphorylated at threonine 181 with neocortical neurofibrillary pathology in Alzheimer's disease. Brain 130: e82 [DOI] [PubMed] [Google Scholar]
- Calsolaro V, Edison P (2016) Neuroinflammation in Alzheimer's disease: Current evidence and future directions. Alzheimers Dement 12: 719–732 [DOI] [PubMed] [Google Scholar]
- Carter SF, Herholz K, Rosa‐Neto P, Pellerin L, Nordberg A, Zimmer ER (2019) Astrocyte biomarkers in Alzheimer's disease. Trends Mol Med 25: 77–95 [DOI] [PubMed] [Google Scholar]
- Chatterjee P, Pedrini S, Stoops E, Goozee K, Villemagne VL, Asih PR, Verberk IMW, Dave P, Taddei K, Sohrabi HR et al (2021) Plasma glial fibrillary acidic protein is elevated in cognitively normal older adults at risk of Alzheimer's disease. Transl Psychiatry 11: 27 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen SD, Huang YY, Shen XN, Guo Y, Tan L, Dong Q, Yu JT, Alzheimer's Disease Neuroimaging Initiative (2021) Longitudinal plasma phosphorylated tau 181 tracks disease progression in Alzheimer's disease. Transl Psychiatry 11: 356 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cicognola C, Janelidze S, Hertze J, Zetterberg H, Blennow K, Mattsson‐Carlgren N, Hansson O (2021) Plasma glial fibrillary acidic protein detects Alzheimer pathology and predicts future conversion to Alzheimer dementia in patients with mild cognitive impairment. Alzheimers Res Ther 13: 68 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cirrito JR, May PC, O'Dell MA, Taylor JW, Parsadanian M, Cramer JW, Audia JE, Nissen JS, Bales KR, Paul SM et al (2003) In vivo assessment of brain interstitial fluid with microdialysis reveals plaque‐associated changes in amyloid‐beta metabolism and half‐life. J Neurosci 23: 8844–8853 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cullen NC, Leuzy A, Palmqvist S, Janelidze S, Stomrud E, Pesini P, Sarasa L, Allué JA, Proctor NK, Zetterberg H et al (2021a) Individualized prognosis of cognitive decline and dementia in mild cognitive impairment based on plasma biomarker combinations. Nat Aging 1: 114–123 [DOI] [PubMed] [Google Scholar]
- Cullen NC, Leuzy A, Janelidze S, Palmqvist S, Svenningsson AL, Stomrud E, Dage JL, Mattsson‐Carlgren N, Hansson O (2021b) Plasma biomarkers of Alzheimer's disease improve prediction of cognitive decline in cognitively unimpaired elderly populations. Nat Commun 12: 3555 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cummings J (2019) The role of biomarkers in Alzheimer's disease drug development. Adv Exp Med Biol 1118: 29–61 [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Meyer S, Schaeverbeke JM, Verberk IMW, Gille B, De Schaepdryver M, Luckett ES, Gabel S, Bruffaerts R, Mauroo K, Thijssen EH et al (2020) Comparison of ELISA‐ and SIMOA‐based quantification of plasma Abeta ratios for early detection of cerebral amyloidosis. Alzheimers Res Ther 12: 162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Wolf F, Ghanbari M, Licher S, McRae‐McKee K, Gras L, Weverling GJ, Wermeling P, Sedaghat S, Ikram MK, Waziry R et al (2020) Plasma tau, neurofilament light chain and amyloid‐beta levels and risk of dementia; a population‐based cohort study. Brain 143: 1220–1232 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Disanto G, Barro C, Benkert P, Naegelin Y, Schädelin S, Giardiello A, Zecca C, Blennow K, Zetterberg H, Leppert D et al (2017) Serum neurofilament light: a biomarker of neuronal damage in multiple sclerosis. Ann Neurol 81: 857–870 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donker Kaat L, Meeter LH, Chiu WZ, Melhem S, Boon AJW, Blennow K, Zetterberg H, van Swieten JC (2018) Serum neurofilament light chain in progressive supranuclear palsy. Parkinsonism Relat Disord 56: 98–101 [DOI] [PubMed] [Google Scholar]
- Dubois B, Feldman HH, Jacova C, DeKosky ST, Barberger‐Gateau P, Cummings J, Delacourte A, Galasko D, Gauthier S, Jicha G et al (2007) Research criteria for the diagnosis of Alzheimer's disease: revising the NINCDS‐ADRDA criteria. Lancet Neurol 6: 734–746 [DOI] [PubMed] [Google Scholar]
- Dubois B, Feldman HH, Jacova C, Hampel H, Molinuevo JL, Blennow K, DeKosky ST, Gauthier S, Selkoe D, Bateman R et al (2014) Advancing research diagnostic criteria for Alzheimer's disease: the IWG‐2 criteria. Lancet Neurol 13: 614–629 [DOI] [PubMed] [Google Scholar]
- Duits FH, Martinez‐Lage P, Paquet C, Engelborghs S, Lleó A, Hausner L, Molinuevo JL, Stomrud E, Farotti L, Ramakers IHGB et al (2016) Performance and complications of lumbar puncture in memory clinics: results of the multicenter lumbar puncture feasibility study. Alzheimers Dement 12: 154–163 [DOI] [PubMed] [Google Scholar]
- Gaetani L, Blennow K, Calabresi P, Di Filippo M, Parnetti L, Zetterberg H (2019) Neurofilament light chain as a biomarker in neurological disorders. J Neurol Neurosurg Psychiatry 90: 870–881 [DOI] [PubMed] [Google Scholar]
- Garwood CJ, Ratcliffe LE, Simpson JE, Heath PR, Ince PG, Wharton SB (2017) Review: astrocytes in Alzheimer's disease and other age‐associated dementias: a supporting player with a central role. Neuropathol Appl Neurobiol 43: 281–298 [DOI] [PubMed] [Google Scholar]
- Gisslen M, Price RW, Andreasson U, Norgren N, Nilsson S, Hagberg L, Fuchs D, Spudich S, Blennow K, Zetterberg H (2016) Plasma concentration of the neurofilament light protein (NFL) is a biomarker of CNS injury in HIV infection: a cross‐sectional study. EBioMedicine 3: 135–140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giudici KV, de Souto Barreto P, Guyonnet S, Li Y, Bateman RJ, Vellas B, MAPT/DSA Group (2020) Assessment of plasma amyloid‐beta42/40 and cognitive decline among community‐dwelling older adults. JAMA Netw Open 3: e2028634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grote T, Berens P (2020) On the ethics of algorithmic decision‐making in healthcare. J Med Ethics 46: 205–211 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grundke‐Iqbal I, Iqbal K, Quinlan M, Tung YC, Zaidi MS, Wisniewski HM (1986a) Microtubule‐associated protein tau. A component of Alzheimer paired helical filaments. J Biol Chem 261: 6084–6089 [PubMed] [Google Scholar]
- Grundke‐Iqbal I, Iqbal K, Tung YC, Quinlan M, Wisniewski HM, Binder LI (1986b) Abnormal phosphorylation of the microtubule‐associated protein tau (tau) in Alzheimer cytoskeletal pathology. Proc Natl Acad Sci USA 83: 4913–4917 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hampel H, Frank R, Broich K, Teipel SJ, Katz RG, Hardy J, Herholz K, Bokde ALW, Jessen F, Hoessler YC et al (2010) Biomarkers for Alzheimer's disease: academic, industry and regulatory perspectives. Nat Rev Drug Discov 9: 560–574 [DOI] [PubMed] [Google Scholar]
- Hampel H, Lista S, Khachaturian ZS (2012) Development of biomarkers to chart all Alzheimer's disease stages: the royal road to cutting the therapeutic Gordian Knot. Alzheimers Dement 8: 312–336 [DOI] [PubMed] [Google Scholar]
- Handelman GS, Kok HK, Chandra RV, Razavi AH, Lee MJ, Asadi H (2018) eDoctor: machine learning and the future of medicine. J Intern Med 284: 603–619 [DOI] [PubMed] [Google Scholar]
- Hansson O, Zetterberg H, Vanmechelen E, Vanderstichele H, Andreasson U, Londos E, Wallin A, Minthon L, Blennow K (2010) Evaluation of plasma Abeta(40) and Abeta(42) as predictors of conversion to Alzheimer's disease in patients with mild cognitive impairment. Neurobiol Aging 31: 357–367 [DOI] [PubMed] [Google Scholar]
- Hansson O, Seibyl J, Stomrud E, Zetterberg H, Trojanowski JQ, Bittner T, Lifke V, Corradini V, Eichenlaub U, Batrla R et al (2018) CSF biomarkers of Alzheimer's disease concord with amyloid‐beta PET and predict clinical progression: a study of fully automated immunoassays in BioFINDER and ADNI cohorts. Alzheimers Dement 14: 1470–1481 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hansson O, Lehmann S, Otto M, Zetterberg H, Lewczuk P (2019) Advantages and disadvantages of the use of the CSF amyloid beta (Abeta) 42/40 ratio in the diagnosis of Alzheimer's disease. Alzheimers Res Ther 11: 34 [DOI] [PMC free article] [PubMed] [Google Scholar]
- He L, Morley JE, Aggarwal G, Nguyen AD, Vellas B, de Souto Barreto P, MAPT/DSA Group (2021) Plasma neurofilament light chain is associated with cognitive decline in non‐dementia older adults. Sci Rep 11: 128 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoffman PN, Cleveland DW, Griffin JW, Landes PW, Cowan NJ, Price DL (1987) Neurofilament gene expression: a major determinant of axonal caliber. Proc Natl Acad Sci USA 84: 3472–3476 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hol EM, Pekny M (2015) Glial fibrillary acidic protein (GFAP) and the astrocyte intermediate filament system in diseases of the central nervous system. Curr Opin Cell Biol 32: 121–130 [DOI] [PubMed] [Google Scholar]
- Illan‐Gala I, Lleo A, Karydas A, Staffaroni AM, Zetterberg H, Sivasankaran R, Grinberg LT, Spina S, Kramer JH, Ramos EM et al (2021) Plasma tau and neurofilament light in frontotemporal lobar degeneration and Alzheimer disease. Neurology 96: e671–e683 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iqbal K, Grundke‐Iqbal I (1997) Elevated levels of tau and ubiquitin in brain and cerebrospinal fluid in Alzheimer's disease. Int Psychogeriatr 9(Suppl 1): 289–296; discussion 317–221 [DOI] [PubMed] [Google Scholar]
- Ishiki A, Kamada M, Kawamura Y, Terao C, Shimoda F, Tomita N, Arai H, Furukawa K (2016) Glial fibrillar acidic protein in the cerebrospinal fluid of Alzheimer's disease, dementia with Lewy bodies, and frontotemporal lobar degeneration. J Neurochem 136: 258–261 [DOI] [PubMed] [Google Scholar]
- Iwatsubo T, Odaka A, Suzuki N, Mizusawa H, Nukina N, Ihara Y (1994) Visualization of A beta 42(43) and A beta 40 in senile plaques with end‐specific A beta monoclonals: evidence that an initially deposited species is A beta 42(43). Neuron 13: 45–53 [DOI] [PubMed] [Google Scholar]
- Jack CR Jr, Albert MS, Knopman DS, McKhann GM, Sperling RA, Carrillo MC, Thies B, Phelps CH (2011) Introduction to the recommendations from the National Institute on Aging‐Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 7: 257–262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jack CR, Bennett DA, Blennow K, Carrillo MC, Feldman HH, Frisoni GB, Hampel H, Jagust WJ, Johnson KA, Knopman DS et al (2016) A/T/N: An unbiased descriptive classification scheme for Alzheimer disease biomarkers. Neurology 87: 539–547 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jack CR, Bennett DA, Blennow K, Carrillo MC, Dunn B, Haeberlein SB, Holtzman DM, Jagust W, Jessen F, Karlawish J et al (2018) NIA‐AA research framework: toward a biological definition of Alzheimer's disease. Alzheimers Dement 14: 535–562 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jack CR Jr (2020) The transformative potential of plasma phosphorylated tau. Lancet Neurol 19: 373–374 [DOI] [PubMed] [Google Scholar]
- Janelidze S, Stomrud E, Palmqvist S, Zetterberg H, van Westen D, Jeromin A, Song L, Hanlon D, Tan Hehir CA, Baker D et al (2016) Plasma beta‐amyloid in Alzheimer's disease and vascular disease. Sci Rep 6: 26801 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Janelidze S, Mattsson N, Palmqvist S, Smith R, Beach TG, Serrano GE, Chai X, Proctor NK, Eichenlaub U, Zetterberg H et al (2020a) Plasma P‐tau181 in Alzheimer's disease: relationship to other biomarkers, differential diagnosis, neuropathology and longitudinal progression to Alzheimer's dementia. Nat Med 26: 379–386 [DOI] [PubMed] [Google Scholar]
- Janelidze S, Stomrud E, Smith R, Palmqvist S, Mattsson N, Airey DC, Proctor NK, Chai X, Shcherbinin S, Sims JR et al (2020b) Cerebrospinal fluid p‐tau217 performs better than p‐tau181 as a biomarker of Alzheimer's disease. Nat Commun 11: 1683 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Janelidze S, Teunissen CE, Zetterberg H, Allue JA, Sarasa L, Eichenlaub U, Bittner T, Ovod V, Verberk IMW, Toba K et al (2021) Head‐to‐head comparison of 8 plasma amyloid‐beta 42/40 assays in Alzheimer disease. JAMA Neurol 78: 1375–1382 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson KA, Minoshima S, Bohnen NI, Donohoe KJ, Foster NL, Herscovitch P, Karlawish JH, Rowe CC, Carrillo MC, Hartley DM et al (2013) Appropriate use criteria for amyloid PET: a report of the Amyloid Imaging Task Force, the Society of Nuclear Medicine and Molecular Imaging, and the Alzheimer's Association. Alzheimers Dement 9: e‐1‐16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karikari TK, Benedet AL, Ashton NJ, Lantero Rodriguez J, Snellman A, Suarez‐Calvet M, Saha‐Chaudhuri P, Lussier F, Kvartsberg H, Rial AM et al (2021) Diagnostic performance and prediction of clinical progression of plasma phospho‐tau181 in the Alzheimer's disease neuroimaging initiative. Mol Psychiatry 26: 429–442 [DOI] [PubMed] [Google Scholar]
- Karikari TK, Emeršič A, Vrillon A, Lantero‐Rodriguez J, Ashton NJ, Kramberger MG, Dumurgier J, Hourregue C, Čučnik S, Brinkmalm G et al (2020a) Head‐to‐head comparison of clinical performance of CSF phospho‐tau T181 and T217 biomarkers for Alzheimer's disease diagnosis. Alzheimers Dement 17: 755–767 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karikari TK, Pascoal TA, Ashton NJ, Janelidze S, Benedet AL, Rodriguez JL, Chamoun M, Savard M, Kang MS, Therriault J et al (2020b) Blood phosphorylated tau 181 as a biomarker for Alzheimer's disease: a diagnostic performance and prediction modelling study using data from four prospective cohorts. Lancet Neurol 19: 422–433 [DOI] [PubMed] [Google Scholar]
- Khalil M, Teunissen CE, Otto M, Piehl F, Sormani MP, Gattringer T, Barro C, Kappos L, Comabella M, Fazekas F et al (2018) Neurofilaments as biomarkers in neurological disorders. Nat Rev Neurol 14: 577–589 [DOI] [PubMed] [Google Scholar]
- Kuhle J, Kropshofer H, Haering DA, Kundu U, Meinert R, Barro C, Dahlke F, Tomic D, Leppert D, Kappos L (2019) Blood neurofilament light chain as a biomarker of MS disease activity and treatment response. Neurology 92: e1007–e1015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuo YM, Emmerling MR, Lampert HC, Hempelman SR, Kokjohn TA, Woods AS, Cotter RJ, Roher AE (1999) High levels of circulating Abeta42 are sequestered by plasma proteins in Alzheimer's disease. Biochem Biophys Res Commun 257: 787–791 [DOI] [PubMed] [Google Scholar]
- Kuo YM, Kokjohn TA, Watson MD, Woods AS, Cotter RJ, Sue LI, Kalback WM, Emmerling MR, Beach TG, Roher AE (2000) Elevated abeta42 in skeletal muscle of Alzheimer disease patients suggests peripheral alterations of AbetaPP metabolism. Am J Pathol 156: 797–805 [DOI] [PMC free article] [PubMed] [Google Scholar]
- La Joie R, Bejanin A, Fagan AM, Ayakta N, Baker SL, Bourakova V, Boxer AL, Cha J, Karydas A, Jerome G et al (2018) Associations between [(18)F]AV1451 tau PET and CSF measures of tau pathology in a clinical sample. Neurology 90: e282–e290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lachno DR, Vanderstichele H, De Groote G, Kostanjevecki V, De Meyer G, Siemers ER, Willey MB, Bourdage JS, Konrad RJ, Dean RA (2009) The influence of matrix type, diurnal rhythm and sample collection and processing on the measurement of plasma beta‐amyloid isoforms using the INNO‐BIA plasma Abeta forms multiplex assay. J Nutr Health Aging 13: 220–225 [DOI] [PubMed] [Google Scholar]
- Lantero Rodriguez J, Karikari TK, Suarez‐Calvet M, Troakes C, King A, Emersic A, Aarsland D, Hye A, Zetterberg H, Blennow K et al (2020) Plasma p‐tau181 accurately predicts Alzheimer's disease pathology at least 8 years prior to post‐mortem and improves the clinical characterisation of cognitive decline. Acta Neuropathol 140: 267–278 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leitao MJ, Silva‐Spinola A, Santana I, Olmedo V, Nadal A, Le Bastard N, Baldeiras I (2019) Clinical validation of the Lumipulse G cerebrospinal fluid assays for routine diagnosis of Alzheimer's disease. Alzheimers Res Ther 11: 91 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewczuk P, Ermann N, Andreasson U, Schultheis C, Podhorna J, Spitzer P, Maler JM, Kornhuber J, Blennow K, Zetterberg H (2018) Plasma neurofilament light as a potential biomarker of neurodegeneration in Alzheimer's disease. Alzheimers Res Ther 10: 71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li QX, Whyte S, Tanner JE, Evin G, Beyreuther K, Masters CL (1998) Secretion of Alzheimer's disease Abeta amyloid peptide by activated human platelets. Lab Invest 78: 461–469 [PubMed] [Google Scholar]
- Li D, Mielke MM (2019) An update on blood‐based markers of alzheimer's disease using the SiMoA platform. Neurol Ther 8: 73–82 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lifke V, Kollmorgen G, Manuilova E, Oelschlaegel T, Hillringhaus L, Widmann M, von Arnim CAF, Otto M, Christenson RH, Powers JL et al (2019) Elecsys((R)) Total‐Tau and Phospho‐Tau (181P) CSF assays: analytical performance of the novel, fully automated immunoassays for quantification of tau proteins in human cerebrospinal fluid. Clin Biochem 72: 30–38 [DOI] [PubMed] [Google Scholar]
- Lopez OL, Kuller LH, Mehta PD, Becker JT, Gach HM, Sweet RA, Chang YF, Tracy R, DeKosky ST (2008) Plasma amyloid levels and the risk of AD in normal subjects in the Cardiovascular Health Study. Neurology 70: 1664–1671 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marzanski M (2000) Would you like to know what is wrong with you? On telling the truth to patients with dementia. J Med Ethics 26: 108–113 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattsson N, Andreasson U, Zetterberg H, Blennow K, Alzheimer's Disease Neuroimaging Initiative (2017a) Association of plasma neurofilament light with neurodegeneration in patients with Alzheimer disease. JAMA Neurol 74: 557–566 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattsson N, Scholl M, Strandberg O, Smith R, Palmqvist S, Insel PS, Hagerstrom D, Ohlsson T, Zetterberg H, Jogi J et al (2017b) (18)F‐AV‐1451 and CSF T‐tau and P‐tau as biomarkers in Alzheimer's disease. EMBO Mol Med 9: 1212–1223 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattsson N, Cullen NC, Andreasson U, Zetterberg H, Blennow K (2019) Association between longitudinal plasma neurofilament light and neurodegeneration in patients with Alzheimer disease. JAMA Neurol 76: 791–799 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattsson‐Carlgren N, Andersson E, Janelidze S, Ossenkoppele R, Insel P, Strandberg O, Zetterberg H, Rosen HJ, Rabinovici G, Chai X et al (2020a) Abeta deposition is associated with increases in soluble and phosphorylated tau that precede a positive Tau PET in Alzheimer's disease. Sci Adv 6: eaaz2387 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattsson‐Carlgren N, Janelidze S, Palmqvist S, Cullen N, Svenningsson AL, Strandberg O, Mengel D, Walsh DM, Stomrud E, Dage JL et al (2020b) Longitudinal plasma p‐tau217 is increased in early stages of Alzheimer's disease. Brain 143: 3234–3241 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattsson‐Carlgren N, Palmqvist S, Blennow K, Hansson O (2020c) Increasing the reproducibility of fluid biomarker studies in neurodegenerative studies. Nat Commun 11: 6252 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mattsson‐Carlgren N, Janelidze S, Bateman RJ, Smith R, Stomrud E, Serrano GE, Reiman EM, Palmqvist S, Dage JL, Beach TG et al (2021) Soluble P‐tau217 reflects amyloid and tau pathology and mediates the association of amyloid with tau. EMBO Mol Med 13: e14022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Maurik IS, Zwan MD, Tijms BM, Bouwman FH, Teunissen CE, Scheltens P, Wattjes MP, Barkhof F, Berkhof J, van der Flier WM et al (2017) Interpreting biomarker results in individual patients with mild cognitive impairment in the Alzheimer's biomarkers in daily practice (ABIDE) project. JAMA Neurol 74: 1481–1491 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Maurik IS, Visser LNC, Pel‐Littel RE, van Buchem MM, Zwan MD, Kunneman M, Pelkmans W, Bouwman FH, Minkman M, Schoonenboom N et al (2019a) Development and usability of ADappt: web‐based tool to support clinicians, patients, and caregivers in the diagnosis of mild cognitive impairment and alzheimer disease. JMIR Form Res 3: e13417 [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Maurik IS, Vos SJ, Bos I, Bouwman FH, Teunissen CE, Scheltens P, Barkhof F, Frolich L, Kornhuber J, Wiltfang J et al (2019b) Biomarker‐based prognosis for people with mild cognitive impairment (ABIDE): a modelling study. Lancet Neurol 18: 1034–1044 [DOI] [PubMed] [Google Scholar]
- McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, Kawas CH, Klunk WE, Koroshetz WJ, Manly JJ, Mayeux R et al (2011) The diagnosis of dementia due to Alzheimer's disease: recommendations from the National Institute on Aging‐Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 7: 263–269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michetti F, D'Ambrosi N, Toesca A, Puglisi MA, Serrano A, Marchese E, Corvino V, Geloso MC (2019) The S100B story: from biomarker to active factor in neural injury. J Neurochem 148: 168–187 [DOI] [PubMed] [Google Scholar]
- Mielke MM, Hagen CE, Xu J, Chai X, Vemuri P, Lowe VJ, Airey DC, Knopman DS, Roberts RO, Machulda MM et al (2018) Plasma phospho‐tau181 increases with Alzheimer's disease clinical severity and is associated with tau‐ and amyloid‐positron emission tomography. Alzheimers Dement 14: 989–997 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mielke MM, Syrjanen JA, Blennow K, Zetterberg H, Vemuri P, Skoog I, Machulda MM, Kremers WK, Knopman DS, Jack C et al (2019) Plasma and CSF neurofilament light: relation to longitudinal neuroimaging and cognitive measures. Neurology 93: e252–e260 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mirra SS, Heyman A, McKeel D, Sumi SM, Crain BJ, Brownlee LM, Vogel FS, Hughes JP, van Belle G, Berg L (1991) The Consortium to Establish a Registry for Alzheimer's Disease (CERAD). Part II. Standardization of the neuropathologic assessment of Alzheimer's disease. Neurology 41: 479–486 [DOI] [PubMed] [Google Scholar]
- Moscoso A, Grothe MJ, Ashton NJ, Karikari TK, Lantero Rodriguez J, Snellman A, Suarez‐Calvet M, Blennow K, Zetterberg H, Scholl M et al (2021) Longitudinal associations of blood phosphorylated Tau181 and neurofilament light chain with neurodegeneration in Alzheimer disease. JAMA Neurol 78: 396–406 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Motter R, Vigo‐Pelfrey C, Kholodenko D, Barbour R, Johnson‐Wood K, Galasko D, Chang L, Miller B, Clark C, Green R et al (1995) Reduction of beta‐amyloid peptide42 in the cerebrospinal fluid of patients with Alzheimer's disease. Ann Neurol 38: 643–648 [DOI] [PubMed] [Google Scholar]
- Nakamura A, Kaneko N, Villemagne VL, Kato T, Doecke J, Dore V, Fowler C, Li QX, Martins R, Rowe C et al (2018) High performance plasma amyloid‐beta biomarkers for Alzheimer's disease. Nature 554: 249–254 [DOI] [PubMed] [Google Scholar]
- Norgren N, Rosengren L, Stigbrand T (2003) Elevated neurofilament levels in neurological diseases. Brain Res 987: 25–31 [DOI] [PubMed] [Google Scholar]
- Oeckl P, Halbgebauer S, Anderl‐Straub S, Steinacker P, Huss AM, Neugebauer H, von Arnim CAF, Diehl‐Schmid J, Grimmer T, Kornhuber J et al (2019) Glial fibrillary acidic protein in serum is increased in Alzheimer's disease and correlates with cognitive impairment. J Alzheimers Dis 67: 481–488 [DOI] [PubMed] [Google Scholar]
- Olsson B, Lautner R, Andreasson U, Öhrfelt A, Portelius E, Bjerke M, Hölttä M, Rosén C, Olsson C, Strobel G et al (2016) CSF and blood biomarkers for the diagnosis of Alzheimer's disease: a systematic review and meta‐analysis. Lancet Neurol 15: 673–684 [DOI] [PubMed] [Google Scholar]
- Olsson B, Alberg L, Cullen NC, Michael E, Wahlgren L, Kroksmark AK, Rostasy K, Blennow K, Zetterberg H, Tulinius M (2019) NFL is a marker of treatment response in children with SMA treated with nusinersen. J Neurol 266: 2129–2136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ostrowitzki S, Lasser RA, Dorflinger E, Scheltens P, Barkhof F, Nikolcheva T, Ashford E, Retout S, Hofmann C, Delmar P et al (2017) A phase III randomized trial of gantenerumab in prodromal Alzheimer's disease. Alzheimers Res Ther 9: 95 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ovod V, Ramsey KN, Mawuenyega KG, Bollinger JG, Hicks T, Schneider T, Sullivan M, Paumier K, Holtzman DM, Morris JC et al (2017) Amyloid beta concentrations and stable isotope labeling kinetics of human plasma specific to central nervous system amyloidosis. Alzheimers Dement 13: 841–849 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palmqvist S, Insel PS, Zetterberg H, Blennow K, Brix B, Stomrud E, Alzheimer's Disease Neuroimaging Initiative , Fs SB, Mattsson N, Hansson O (2019a) Accurate risk estimation of beta‐amyloid positivity to identify prodromal Alzheimer's disease: Cross‐validation study of practical algorithms. Alzheimers Dement 15: 194–204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palmqvist S, Janelidze S, Stomrud E, Zetterberg H, Karl J, Zink K, Bittner T, Mattsson N, Eichenlaub U, Blennow K et al (2019b) Performance of fully automated plasma assays as screening tests for Alzheimer disease‐related beta‐amyloid status. JAMA Neurol 76: 1060–1069 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palmqvist S, Janelidze S, Quiroz YT, Zetterberg H, Lopera F, Stomrud E, Su YI, Chen Y, Serrano GE, Leuzy A et al (2020) Discriminative accuracy of plasma phospho‐tau217 for Alzheimer disease vs other neurodegenerative disorders. JAMA 324: 772 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pannee J, Tornqvist U, Westerlund A, Ingelsson M, Lannfelt L, Brinkmalm G, Persson R, Gobom J, Svensson J, Johansson P et al (2014) The amyloid‐beta degradation pattern in plasma–a possible tool for clinical trials in Alzheimer's disease. Neurosci Lett 573: 7–12 [DOI] [PubMed] [Google Scholar]
- Pereira JB, Janelidze S, Smith R, Mattsson‐Carlgren N, Palmqvist S, Teunissen CE, Zetterberg H, Stomrud E, Ashton NJ, Blennow K et al (2021a) Plasma GFAP is an early marker of amyloid‐beta but not tau pathology in Alzheimer's disease. Brain 10.1093/brain/awab223 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pereira JB, Janelidze S, Stomrud E, Palmqvist S, van Westen D, Dage JL, Mattsson‐Carlgren N, Hansson O (2021b) Plasma markers predict changes in amyloid, tau, atrophy and cognition in non‐demented subjects. Brain 144: 2826–2836 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perez‐Grijalba V, Romero J, Pesini P, Sarasa L, Monleon I, San‐Jose I, Arbizu J, Martinez‐Lage P, Munuera J, Ruiz A et al (2019) Plasma Abeta42/40 ratio detects early stages of Alzheimer's disease and correlates with CSF and neuroimaging biomarkers in the AB255 study. J Prev Alzheimers Dis 6: 34–41 [DOI] [PubMed] [Google Scholar]
- Pesini P, Perez‐Grijalba V, Monleon I, Boada M, Tarraga L, Martinez‐Lage P, San‐Jose I, Sarasa M (2012) Reliable measurements of the beta‐amyloid pool in blood could help in the early diagnosis of AD. Int J Alzheimers Dis 2012: 604141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Portelius E, Hansson SF, Tran AJ, Zetterberg H, Grognet P, Vanmechelen E, Höglund K, Brinkmalm G, Westman‐Brinkmalm A, Nordhoff E et al (2008) Characterization of tau in cerebrospinal fluid using mass spectrometry. J Proteome Res 7: 2114–2120 [DOI] [PubMed] [Google Scholar]
- Preische O, Schultz SA, Apel A, Kuhle J, Kaeser SA, Barro C, Gräber S, Kuder‐Buletta E, LaFougere C, Laske C et al (2019) Serum neurofilament dynamics predicts neurodegeneration and clinical progression in presymptomatic Alzheimer's disease. Nat Med 25: 277–283 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prince M, Comas‐Herrera A, Knapp M, Guerchet M & Karagiannidou M (2016) World Alzheimer Report 2016: Improving healthcare for people with dementia. https://www.alz.co.uk/research/
- Quiroz YT, Zetterberg H, Reiman EM, Chen Y, Su YI, Fox‐Fuller JT, Garcia G, Villegas A, Sepulveda‐Falla D, Villada M et al (2020) Plasma neurofilament light chain in the presenilin 1 E280A autosomal dominant Alzheimer's disease kindred: a cross‐sectional and longitudinal cohort study. Lancet Neurol 19: 513–521 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rabinovici GD, Gatsonis C, Apgar C, Chaudhary K, Gareen I, Hanna L, Hendrix J, Hillner BE, Olson C, Lesman‐Segev OH et al (2019) Association of amyloid positron emission tomography with subsequent change in clinical management among medicare beneficiaries with mild cognitive impairment or dementia. JAMA 321: 1286–1294 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rembach A, Faux NG, Watt AD, Pertile KK, Rumble RL, Trounson BO, Fowler CJ, Roberts BR, Perez KA, Li Q‐X et al (2014) Changes in plasma amyloid beta in a longitudinal study of aging and Alzheimer's disease. Alzheimers Dement 10: 53–61 [DOI] [PubMed] [Google Scholar]
- Rissin DM, Kan CW, Campbell TG, Howes SC, Fournier DR, Song L, Piech T, Patel PP, Chang L, Rivnak AJ et al (2010) Single‐molecule enzyme‐linked immunosorbent assay detects serum proteins at subfemtomolar concentrations. Nat Biotechnol 28: 595–599 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rissin DM, Fournier DR, Piech T, Kan CW, Campbell TG, Song L, Chang L, Rivnak AJ, Patel PP, Provuncher GK et al (2011) Simultaneous detection of single molecules and singulated ensembles of molecules enables immunoassays with broad dynamic range. Anal Chem 83: 2279–2285 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roher AE, Esh CL, Kokjohn TA, Castaño EM, Van Vickle GD, Kalback WM, Patton RL, Luehrs DC, Daugs ID, Kuo Y‐M et al (2009) Amyloid beta peptides in human plasma and tissues and their significance for Alzheimer's disease. Alzheimers Dement 5: 18–29 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rohrer JD, Woollacott IOC, Dick KM, Brotherhood E, Gordon E, Fellows A, Toombs J, Druyeh R, Cardoso MJ, Ourselin S et al (2016) Serum neurofilament light chain protein is a measure of disease intensity in frontotemporal dementia. Neurology 87: 1329–1336 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rozga M, Bittner T, Batrla R, Karl J (2019) Preanalytical sample handling recommendations for Alzheimer's disease plasma biomarkers. Alzheimers Dement (Amst) 11: 291–300 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salloway S, Sperling R, Fox NC, Blennow K, Klunk W, Raskind M, Sabbagh M, Honig LS, Porsteinsson AP, Ferris S et al (2014) Two phase 3 trials of bapineuzumab in mild‐to‐moderate Alzheimer's disease. N Engl J Med 370: 322–333 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sato C, Barthélemy NR, Mawuenyega KG, Patterson BW, Gordon BA, Jockel‐Balsarotti J, Sullivan M, Crisp MJ, Kasten T, Kirmess KM et al (2018) Tau kinetics in neurons and the human central nervous system. Neuron 98: 861–864 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schindler SE, Bollinger JG, Ovod V, Mawuenyega KG, Li Y, Gordon BA, Holtzman DM, Morris JC, Benzinger TLS, Xiong C et al (2019) High‐precision plasma beta‐amyloid 42/40 predicts current and future brain amyloidosis. Neurology 93: e1647–e1659 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seppala TT, Nerg O, Koivisto AM, Rummukainen J, Puli L, Zetterberg H, Pyykko OT, Helisalmi S, Alafuzoff I, Hiltunen M et al (2012) CSF biomarkers for Alzheimer disease correlate with cortical brain biopsy findings. Neurology 78: 1568–1575 [DOI] [PubMed] [Google Scholar]
- Shaw LM, Arias J, Blennow K, Galasko D, Molinuevo JL, Salloway S, Schindler S, Carrillo MC, Hendrix JA, Ross A et al (2018) Appropriate use criteria for lumbar puncture and cerebrospinal fluid testing in the diagnosis of Alzheimer's disease. Alzheimers Dement 14: 1505–1521 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simrén J, Leuzy A, Karikari TK, Hye A, Benedet AL, Lantero‐Rodriguez J, Mattsson‐Carlgren N, Schöll M, Mecocci P, Vellas B et al (2021) The diagnostic and prognostic capabilities of plasma biomarkers in Alzheimer's disease. Alzheimers Dement 17: 1145–1156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Song F, Poljak A, Valenzuela M, Mayeux R, Smythe GA, Sachdev PS (2011) Meta‐analysis of plasma amyloid‐beta levels in Alzheimer's disease. J Alzheimers Dis 26: 365–375 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sperling RA, Aisen PS, Beckett LA, Bennett DA, Craft S, Fagan AM, Iwatsubo T, Jack CR, Kaye J, Montine TJ et al (2011a) Toward defining the preclinical stages of Alzheimer's disease: recommendations from the National Institute on Aging‐Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 7: 280–292 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sperling RA, Jack CR Jr, Aisen PS (2011b) Testing the right target and right drug at the right stage. Sci Transl Med 3: 111cm133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sperling RA, Rentz DM, Johnson KA, Karlawish J, Donohue M, Salmon DP, Aisen P (2014) The A4 study: stopping AD before symptoms begin? Sci Transl Med 6: 228fs213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sperling RA, Donohue MC, Raman R, Sun CK, Yaari R, Holdridge K, Siemers E, Johnson KA, Aisen PS, A4 Study Team (2020) Association of factors with elevated amyloid burden in clinically normal older individuals. JAMA Neurol 77: 735–745 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinacker P, Anderl‐Straub S, Diehl‐Schmid J, Semler E, Uttner I, von Arnim CAF, Barthel H, Danek A, Fassbender K, Fliessbach K et al (2018) Serum neurofilament light chain in behavioral variant frontotemporal dementia. Neurology 91: e1390–e1401 [DOI] [PubMed] [Google Scholar]
- Stockmann J, Verberk IMW, Timmesfeld N, Denz R, Budde B, Lange‐Leifhelm J, Scheltens P, van der Flier WM, Nabers A, Teunissen CE et al (2020) Amyloid‐beta misfolding as a plasma biomarker indicates risk for future clinical Alzheimer's disease in individuals with subjective cognitive decline. Alzheimers Res Ther 12: 169 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strozyk D, Blennow K, White LR, Launer LJ (2003) CSF Abeta 42 levels correlate with amyloid‐neuropathology in a population‐based autopsy study. Neurology 60: 652–656 [DOI] [PubMed] [Google Scholar]
- Suarez‐Calvet M, Karikari TK, Ashton NJ, Lantero Rodriguez J, Mila‐Aloma M, Gispert JD, Salvado G, Minguillon C, Fauria K, Shekari M et al (2020) Novel tau biomarkers phosphorylated at T181, T217 or T231 rise in the initial stages of the preclinical Alzheimer's continuum when only subtle changes in Abeta pathology are detected. EMBO Mol Med 12: e12921 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swaminathan S, Risacher SL, Yoder KK, West JD, Shen L, Kim S, Inlow M, Foroud T, Jagust WJ, Koeppe RA et al (2014) Association of plasma and cortical amyloid beta is modulated by APOE epsilon4 status. Alzheimers Dement 10: e9–e18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tamaoka A, Kondo T, Odaka A, Sahara N, Sawamura N, Ozawa K, Suzuki N, Shoji S, Mori H (1994) Biochemical evidence for the long‐tail form (A beta 1–42/43) of amyloid beta protein as a seed molecule in cerebral deposits of Alzheimer's disease. Biochem Biophys Res Commun 205: 834–842 [DOI] [PubMed] [Google Scholar]
- Tapiola T, Alafuzoff I, Herukka SK, Parkkinen L, Hartikainen P, Soininen H, Pirttila T (2009) Cerebrospinal fluid {beta}‐amyloid 42 and tau proteins as biomarkers of Alzheimer‐type pathologic changes in the brain. Arch Neurol 66: 382–389 [DOI] [PubMed] [Google Scholar]
- Tatebe H, Kasai T, Ohmichi T, Kishi Y, Kakeya T, Waragai M, Kondo M, Allsop D, Tokuda T (2017) Quantification of plasma phosphorylated tau to use as a biomarker for brain Alzheimer pathology: pilot case‐control studies including patients with Alzheimer's disease and down syndrome. Mol Neurodegener 12: 63 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Therriault J, Benedet AL, Pascoal TA, Lussier FZ, Tissot C, Karikari TK, Ashton NJ, Chamoun M, Bezgin G, Mathotaarachchi S et al (2021) Association of plasma P‐tau181 with memory decline in non‐demented adults. Brain Commun 3: fcab136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thijssen EH, La Joie R, Wolf A, Strom A, Wang P, Iaccarino L, Bourakova V, Cobigo Y, Heuer H, Spina S et al (2020) Diagnostic value of plasma phosphorylated tau181 in Alzheimer's disease and frontotemporal lobar degeneration. Nat Med 26: 387–397 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thijssen EH, La Joie R, Strom A, Fonseca C, Iaccarino L, Wolf A, Spina S, Allen IE, Cobigo Y, Heuer H et al (2021a) Plasma phosphorylated tau 217 and phosphorylated tau 181 as biomarkers in Alzheimer's disease and frontotemporal lobar degeneration: a retrospective diagnostic performance study. Lancet Neurol 20: 739–752 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thijssen EH, Verberk IMW, Vanbrabant J, Koelewijn A, Heijst H, Scheltens P, van der Flier W, Vanderstichele H, Stoops E, Teunissen CE (2021b) Highly specific and ultrasensitive plasma test detects Abeta(1–42) and Abeta(1–40) in Alzheimer's disease. Sci Rep 11: 9736 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Toledo JB, Shaw LM, Trojanowski JQ (2013) Plasma amyloid beta measurements ‐ a desired but elusive Alzheimer's disease biomarker. Alzheimers Res Ther 5: 8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Triana‐Baltzer G, Van Kolen K, Theunis C, Moughadam S, Slemmon R, Mercken M, Galpern W, Sun H, Kolb H (2020) Development and validation of a high sensitivity assay for measuring p217 + tau in cerebrospinal fluid. J Alzheimers Dis 77: 1417–1430 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Triana‐Baltzer G, Moughadam S, Slemmon R, Van Kolen K, Theunis C, Mercken M, Kolb HC (2021) Development and validation of a high‐sensitivity assay for measuring p217+tau in plasma. Alzheimers Dement (Amst) 13: e12204 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vanderstichele H, De Vreese K, Blennow K, Andreasen N, Sindic C, Ivanoiu A, Hampel H, Bürger K, Parnetti L, Lanari A et al (2006) Analytical performance and clinical utility of the INNOTEST PHOSPHO‐TAU181P assay for discrimination between Alzheimer's disease and dementia with Lewy bodies. Clin Chem Lab Med 44: 1472–1480 [DOI] [PubMed] [Google Scholar]
- Verberk IMW, Slot RE, Verfaillie SCJ, Heijst H, Prins ND, van Berckel BNM, Scheltens P, Teunissen CE, van der Flier WM (2018) Plasma amyloid as prescreener for the earliest Alzheimer pathological changes. Ann Neurol 84: 648–658 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verberk IMW, Hendriksen HMA, van Harten AC, Wesselman LMP, Verfaillie SCJ, van den Bosch KA, Slot RER, Prins ND, Scheltens P, Teunissen CE et al (2020a) Plasma amyloid is associated with the rate of cognitive decline in cognitively normal elderly: the SCIENCe project. Neurobiol Aging 89: 99–107 [DOI] [PubMed] [Google Scholar]
- Verberk IMW, Thijssen E, Koelewijn J, Mauroo K, Vanbrabant J, de Wilde A, Zwan MD, Verfaillie SCJ, Ossenkoppele R, Barkhof F et al (2020b) Combination of plasma amyloid beta(1–42/1‐40) and glial fibrillary acidic protein strongly associates with cerebral amyloid pathology. Alzheimers Res Ther 12: 118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verberk IMW, Laarhuis MB, van den Bosch KA, Ebenau JL, van Leeuwenstijn M, Prins ND, Scheltens P, Teunissen C, van der Flier W (2021) Serum markers glial fibrillary acidic protein and neurofilament light for prognosis and monitoring in cognitively normal older people: a prospective memory clinic‐based cohort study. Lancet Healthy Longev 2: e87–e95 [DOI] [PubMed] [Google Scholar]
- Verde F, Steinacker P, Weishaupt JH, Kassubek J, Oeckl P, Halbgebauer S, Tumani H, von Arnim CAF, Dorst J, Feneberg E et al (2019) Neurofilament light chain in serum for the diagnosis of amyotrophic lateral sclerosis. J Neurol Neurosurg Psychiatry 90: 157–164 [DOI] [PubMed] [Google Scholar]
- Weston PSJ, Poole T, Ryan NS, Nair A, Liang Y, Macpherson K, Druyeh R, Malone IB, Ahsan RL, Pemberton H et al (2017) Serum neurofilament light in familial Alzheimer disease: a marker of early neurodegeneration. Neurology 89: 2167–2175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Whitehouse P, Frisoni GB, Post S (2004) Breaking the diagnosis of dementia. Lancet Neurol 3: 124–128 [DOI] [PubMed] [Google Scholar]
- Winblad B, Amouyel P, Andrieu S, Ballard C, Brayne C, Brodaty H, Cedazo‐Minguez A, Dubois B, Edvardsson D, Feldman H et al (2016) Defeating Alzheimer's disease and other dementias: a priority for European science and society. Lancet Neurol 15: 455–532 [DOI] [PubMed] [Google Scholar]
- Zetterberg H, Mortberg E, Song L, Chang L, Provuncher GK, Patel PP, Ferrell E, Fournier DR, Kan CW, Campbell TG et al (2011) Hypoxia due to cardiac arrest induces a time‐dependent increase in serum amyloid beta levels in humans. PLoS One 6: e28263 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table EV1
Table EV2
Table EV3
Table EV4