

Abstract
The use of digital tools to measure physiological and behavioural variables of potential relevance to mental health is a growing field sitting at the intersection between computer science, engineering, and clinical science. We summarised the literature on remote measuring technologies, mapping methodological challenges and threats to reproducibility, and identified leading digital signals for depression. Medical and computer science databases were searched between January 2007 and November 2019. Published studies linking depression and objective behavioural data obtained from smartphone and wearable device sensors in adults with unipolar depression and healthy subjects were included. A descriptive approach was taken to synthesise study methodologies. We included 51 studies and found threats to reproducibility and transparency arising from failure to provide comprehensive descriptions of recruitment strategies, sample information, feature construction and the determination and handling of missing data. The literature is characterised by small sample sizes, short follow-up duration and great variability in the quality of reporting, limiting the interpretability of pooled results. Bivariate analyses show consistency in statistically significant associations between depression and digital features from sleep, physical activity, location, and phone use data. Machine learning models found the predictive value of aggregated features. Given the pitfalls in the combined literature, these results should be taken purely as a starting point for hypothesis generation. Since this research is ultimately aimed at informing clinical practice, we recommend improvements in reporting standards including consideration of generalisability and reproducibility, such as wider diversity of samples, thorough reporting methodology and the reporting of potential bias in studies with numerous features.
Subject terms: Human behaviour, Diagnostic markers, Machine learning
Introduction
Depression remains the leading cause of disability worldwide1, with a largely chronic course and poor prognosis2. Early recognition and access to treatment, as well as a better trial methodology, have been linked to improved treatment outcomes and prognosis3.
The use of digital technology to track mood and behaviour brings enormous potential for clinical management and the improvement of research in depression. By passively sensing motion, heart rate and other physiological variables, smartphone and wearable sensors provide continuous data on behaviours that are central to psychiatric assessment, such as sociability4, sleep/wake cycles5, cognition, activity6 and movement7.
With the global trend toward increased smartphone ownership (44.9% worldwide, 83.3% in the UK) and wearable device usage forecast to reach one billion by 20228, this new science of “remote sensing”, sometimes referred to as digital phenotyping or personal sensing9 presents a realistic avenue for the management and treatment of depression. When combined with the completion of questionnaires, remote sensing may generate more objective and frequent measures of mood and other core dimensions of mental disorders, instead of relying on retrospective accounts of patients or participants.
The first step in generating meaningful clinical information from data derived from digital sensors is to generate features, which are the smallest constructed building blocks, designed to explain the behaviours of interest (see Mohr et al. 10 for a detailed analytical framework). These low-level features are often aggregated to define high-level behavioural markers, which can be understood as symptoms. For example, GPS data (sensor), can be translated into ‘location type’ (low-level feature), ‘increased time at home location’ (high-level behaviour) derived from location data may indicate social withdrawal or lack of energy (symptom), and may therefore be associated with depression severity.
One of the main challenges that arise from this emerging field is that it sits at the intersection between computer science, engineering, and clinical science. The advantages of a multidisciplinary approach are evident, but these domains are yet to be brought together efficiently11,12, giving rise to large differences in reporting standards with the risk that reproducibility may be threatened13.
Previous reviews in affective disorders cite the level of heterogeneity across studies as a barrier to carrying out meta-analytic syntheses of the results. Additionally, these reviews have included non-validated measures of depression, and a mix of bipolar and unipolar samples, characteristics which not only show divergent results11,12,14, but add study diversity. There is therefore a need for a comprehensive review of methodologies, with more specific inclusion criteria, to highlight the sources of heterogeneity and methodological shortcomings in the field.
Given the difficulty in extracting a clear message from the available literature, the current work aims to review studies linking passive data from smartphone and wearable devices with depression and summarise key methodological aspects, to: (a) identify sources of heterogeneity and threats to reproducibility, and (b) identify leading digital signals for depression. We will also assess the quality of the included studies and evaluate their reporting of the feasibility of passive data collection methods, participant retention and missing data.
Results
Fifty-one studies were included in the review (see Fig. 1). The majority of articles (n = 45) were published in medical journals, and 33 (65%) were from North America. A summary of included studies is presented in Table 1.
Fig. 1. Study selection flowchart.

Medical and computer science databases were searched to ensure relevant fields were covered. The current flowchart lists reasons for excluding the study from the data extraction and quality assessment.
Table 1.
Summary characteristics of included studies.
| First author | Year | Country | Field | N (RMT)a | % female | Mean age (range/SD) | RMTa follow up (days) | Sample type | Depression measure | Passive feature type | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sleep | Physical activity | Circadian rhythm | Sociability | Location | Phone use | Physiological | Environmental | Total feature types | ||||||||||
| Avila-Moraes36 | 2013 | Brazil | M | 30 | 100.0 | 44 (18–60) | 7 | Clinical | BDI, HAMD, MADRS | x | x | x | 3 | |||||
| Ben-Zeev46 | 2015 | USA | M | 37 | 21.0 | 22.5 (19–0) | 70 | Student | PHQ-9 | x | x | x | x | 4 | ||||
| Boukhechba34 | 2018 | USA | M | 72 | 51.4 | 19.8 (2.4) | 14 | Student | DASS-21 | x | x | x | 3 | |||||
| Burns19 | 2011 | USA | M | 7 | 87.5 | 37.4 (19–51) | 56 | Community | PHQ-9 | x | x | x | x | x | 5 | |||
| Byrne25 | 2019 | Australia | M | 42 | 0.0 | (18–29) | 7 | Community | SCRAM - dep | x | x | x | 3 | |||||
| Caldwell76 | 2019 | USA | M | 115 | 100.0 | 27.5 (6.1) | 3 | Community | BDI-II | x | 1 | |||||||
| Cho4 | 2016 | South Korea | M | 532 | 56.0 | 57 | 720 | Community | BDI-II | x | 1 | |||||||
| David47 | 2018 | USA | M | 132 | 60.0 | 20.68 (18–21) | 7 | Student | PHQ-4 | x | x | 2 | ||||||
| Difrancesco20 | 2019 | Netherlands | M | 359 | 62.4 | 50.1 (11.1) | 7 | Community | BDI-II | x | x | x | 3 | |||||
| Dillon21 | 2018 | Ireland | M | 396 | 50.8 | nr | 7 | Clinical | CES-D | x | 1 | |||||||
| Doane77 | 2015 | USA | M | 76 | 76.0 | 18.1 (0.4) | 3 | Student | CES-D | x | 1 | |||||||
| Doryab44 | 2014 | USA | M | 6 | 33.3 | nr | 120 | Student | CES-D | x | x | x | 3 | |||||
| Ghandeharioun6 | 2017 | USA | CS | 12 | 75.0 | 37 (20–73) | 56 | Clinical | HAM-D | x | x | x | x | x | x | 6 | ||
| Haeffel78 | 2017 | USA | M | 47 | 55.3 | 20.9 | 7 | Student | BDI-II | x | 1 | |||||||
| Hori79 | 2016 | Japan | M | 40 | 52.5 | 39.8 | 7 | Clinical | HAM-D | x | 1 | |||||||
| Jacobson80 | 2019 | Brazil | M | 15 | 87.0 | 47.6 (10.5) | 7 | Clinical | BDI, HAMD | x | x | 2 | ||||||
| Kawada32 | 2007 | Japan | M | 105 | 29.5 | 24.1 (1.8) | 4 | Student | CES-D | x | x | x | 3 | |||||
| Knight81 | 2018 | Australia | M | 23 | 77.0 | 20.7 (3.2) | 3 | Community | DASS-21 | x | 1 | |||||||
| Li82 | 2018 | Australia | M | 375 | 53.9 | 59.5 (5.5) | 7 | Community | CES-D | x | 1 | |||||||
| Lu5 | 2018 | USA | CS | 103 | 76.7 | (18–25) | nr | Student | QIDS | x | x | x | 3 | |||||
| Luik83 | 2013 | Netherlands | M | 1734 | 53.4 | 62.3 (9.4) | 7 | Community | CES-D | x | 1 | |||||||
| Luik30 | 2015 | Netherlands | M | 1714 | 53.6 | 62.2 (9.4) | 7 | Community | CES-D | x | 1 | |||||||
| McCall84 | 2015 | USA | M | 58 | 67.0 | 42.1 (12.4) | 56 | Clinical | HAM-D | x | 1 | |||||||
| Mendoza-Vasconez85 | 2019 | USA | M | 266 | nr | 40.6 (9.9) | 7 | Community | HAM-D | x | 1 | |||||||
| Moukaddam27 | 2019 | USA | M | 22 | 76.0 | 50.3 (10.1) | 56 | Clinical | PHQ-9 | x | x | 2 | ||||||
| Naismith86 | 2011 | Australia | M | 44 | 43 | 62.3 | 14 | Clinical | HAM-D | x | 1 | |||||||
| Park87 | 2007 | USA | M | 54 | 57.4 | 43 (21–76) | 14 | Community | CES-D | x | x | 2 | ||||||
| Pillai88 | 2014 | USA | M | 39 | 73.8 | 55 (3.2) | 7 | Student | BDI-II | x | 1 | |||||||
| Pratap89 | 2019 | USA | M | 271 | 77.8 | 33.4 (10.7) | 90 | Community | PHQ-2 | x | x | 2 | ||||||
| Robillard33 | 2013 | Australia | M | 66 | 62.7 | 21.5 | 7 | Clinical | clinician assessment | x | 1 | |||||||
| Robillard41 | 2014 | Australia | M | 238 | 64.3 | 40.4 | 10 | Clinical | HAM-D | x | x | 2 | ||||||
| Robillard38 | 2015 | Australia | M | 342 | 55.1 | 22.3 | 14 | Clinical | clinician assessment | x | x | 2 | ||||||
| Robillard90 | 2016 | Australia | M | 25 | 48.0 | 20.9 (4.6) | 14 | Clinical | clinician assessment | x | x | 2 | ||||||
| Robillard91 | 2018 | USA | M | 12 | 58.0 | 20.1 (18–31) | 13 | Clinical | clinician assessment | x | 1 | |||||||
| Saeb7 | 2015 | USA | M | 21 | 71.4 | 28.9 (19– 58) | 14 | Student | PHQ-9 | x | x | x | 3 | |||||
| Saeb42 | 2016 | USA | M | 38 | 20.8 | nr | 70 | Community | PHQ-9 | x | x | 2 | ||||||
| Sano22 | 2018 | USA | M | 47 | 72.0 | (18– 25) | 30 | Student | MCSF-12 | x | x | x | x | x | x | x | 7 | |
| Slyepchenko37 | 2019 | Canada | M | 70 | 57.9 | (18– 65) | 15 | Clinical | MINI | x | x | x | 3 | |||||
| Smagula (a)39 | 2018a | USA | M | 145 | 67.0 | 60 (36-82) | 9 | Community | HAM-D | x | 1 | |||||||
| Smagula (b)92 | 2018 | USA | M | 45 | 38.8 | 38.08 | 10 | Community | HAM-D | x | 1 | |||||||
| Stremler93 | 2017 | Canada | M | 101 | 62.7 | 34.1 | 5 | Community | CES-D | x | 1 | |||||||
| Tao35 | 2019 | China | M | 220 | 52.3 | 20.3 (2.4) | 7 | Student | PROMIS - dep | x | 1 | |||||||
| Vallance94 | 2013 | Canada | M | 385 | 0.0 | 65.3 (7.5) | 3 | Community | CES-D | x | 1 | |||||||
| Vanderlind95 | 2014 | USA | M | 35 | 42.3 | 19.8 (18–23) | 21 | Student | CES-D | x | x | 2 | ||||||
| Wahle23 | 2016 | Switzerland | M | 36 | 64.3 | (20–57) | 14 | Community | PHQ-9 | x | x | x | x | 4 | ||||
| Wang26 | 2014 | USA | CS | 48 | 20.8 | nr | 7 | Student | PHQ-9 | x | x | x | 3 | |||||
| Wang96 | 2018 | USA | CS | 83 | 51.8 | 20.1 (2.3) | 126 | Student | PHQ-8 | x | x | x | x | x | x | 6 | ||
| White40 | 2017 | USA | M | 418 | 60.3 | 57 (35–85) | 7 | Community | CES-D | x | x | 2 | ||||||
| Yang45 | 2017 | China | CS | 48 | nr | nr | 70 | Student | PHQ-9 | x | 1 | |||||||
| Yaugher97 | 2015 | USA | M | 100 | 58.3 | 18.6 (18– 27) | 7 | Student | PAI-dep | x | 1 | |||||||
| Yue18 | 2018 | USA | CS | 54 | nr | (18–25) | nr | Student | PHQ-9 | x | x | 2 | ||||||
| N = 52 | Median | Median | Median | Median | Total N | Total | ||||||||||||
| 58.0 | 57.9 | 37.2 | 9 | 16 | 31 | 24 | 14 | 14 | 14 | 7 | 4 | 1 | ||||||
RMT remote measurement technologies, SD standard deviation, M medical field, CS computer science field, BDI Beck’s Depression Inventory, HAM-D Hamilton Depression Rating Scale, MADRS Montgomery–Åsberg Depression Rating Scale, PHQ Patient Health Questionnaire, PAI-dep Personality Assessment Inventory-depression subscale, CES-D Center for Epidemiologic Studies Depression Scale, MINI Mini International Neuropsychiatric Interview, PROMIS Patient-Reported Outcomes Measurement Information System, MCSF-12 Mental Component of the Short Form Health Survey, QIDS Quick Inventory of Depressive Symptomatology, DASS Depression Anxiety Stress Scales, SCRAM sleep, circadian rhythms, and mood questionnaire.
aNumber of participants/length of follow-up included in passive data collection samples; these may be lower than overall study sample sizes.
Studies were evenly divided between community samples (n = 19), student samples (n = 18) and clinical populations (n = 14). The median sample size was 58, the median age of participants was 38 years, and the median percentage of females was 58%. However, there was a striking lack of information on some key data—with 12% and 8% of studies failing to give data on age or gender, respectively, and 63% failing to include information on ethnicity. Computer science journals were less likely to report age and gender but more likely to report ethnicity (33% studies failing to report each demographic). Fifteen different measures of depression were used, the most commonly used scales being the Center for Epidemiological Studies Depression Scale (CES-D15; n = 12 studies), Hamilton Rating Scale for Depression (HAM-D16; n = 12 studies), and Patient Health Questionnaire-9 (PHQ-917; n = 9). There were 14 types of devices used across all studies: 12 of them actigraphy-based wrist-worn devices including one Fitbit and a Microsoft band, as well as one pedometer and smartphones (both android and iPhone). For a breakdown of devices, models and sensors used to measure behaviour see Supplementary Table 1.
Most studies had a cohort design, meaning that depression was measured at least at two different time points (see Table 2). However, these time points tended to be shorter than 2 weeks (Fig. 2). Two studies provided no information on the length of follow-up, instead only mentioning that data was obtained from participants providing at least 72 h of consecutive data5,18.
Table 2.
The breakdown of study designs within each sample type.
| Study design | Total | Student | Community | Clinical |
|---|---|---|---|---|
| Cross-sectional | 19 | 4 | 10 | 5 |
| Case-control | 6 | 0 | 1 | 5 |
| Cohort | 25 | 14 | 6 | 3 |
| RCT | 3 | 0 | 2 | 1 |
| Total | 51 | 18 | 19 | 14 |
Fig. 2. Sample sizes and follow-up times for all included studies.
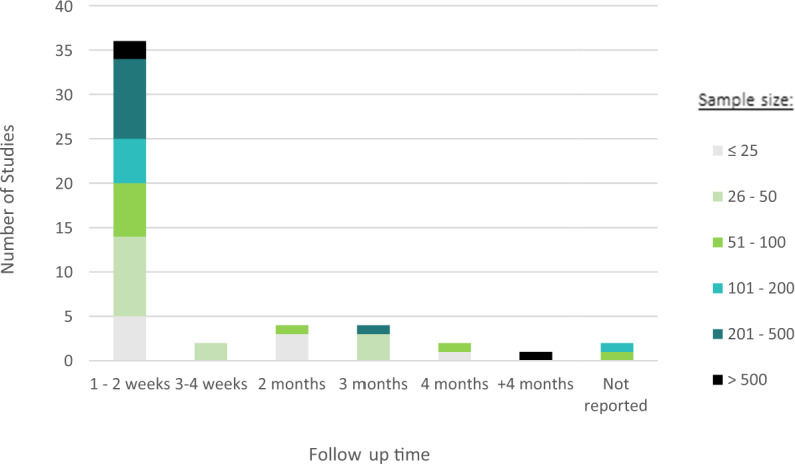
The number of studies by the length of time participants were followed up for in each study, differentiated by sample size.
To understand the relationships between depression and objective features, studies either looked at group differences (including classification analyses) or correlation and regression. Most studies presented direct bivariate relationships (n = 45), allowing for a closer evaluation of which features are promising markers of depressive symptomatology. Ten studies presented the result of a combination of features and their association with the depressive state (n = 7), or depression severity (n = 8), using machine learning methods. Bivariate Pearson correlation coefficients were the most used analytical method (n = 32).
Quality assessment and feasibility
Figure 3 shows a breakdown of quality scores for each item (see Supplementary Fig. 1 and Supplementary Table 2 for quality assessment scores per study). Justification of sample size was rarely given, and sample representativeness was poor, possibly reflecting that many reports were pilot or feasibility studies. Recruitment strategies and non-participation rates were not reported in the majority of cases. Missing data and strategies for handling missing data were infrequently described. Only four studies referred to a previously published protocol19–22.
Fig. 3. Quality of the literature by each domain.

The figure shows the number of studies scoring on each study quality item. 2 points are given for fully addressing quality criteria, 1 point for partially addressing quality criteria, and 0 points for failing to address quality criteria.
Only five studies reported engagement rates at follow-up, and they all measured engagement at different time points, making comparisons difficult. Additionally, sensor data was sometimes obtained for a subsample, whereas acceptability measures were reported for the wider sample. Eighteen studies (35%) reported, or provided enough information to calculate, how many participants completed the study—results ranging from 22% adherence to the study23 at 4 weeks, to 100%24, with a median of 86.6% completers.
Reasons for dropouts were provided in four studies and were due to equipment malfunction and technical problems using devices19,25–27 . Six additional studies reported issues including; lack of data for consecutive days, software error, participants forgetting to charge phones or devices, server and network connectivity problems, sensors breaking, missing clinical data which impeded comparisons with sensor data, and mobile software updates, which can interfere with data integrity7,22,28–31.
Associations between objective features and depression
The association between groups of features and depression is given in Fig. 4, broken down by feature type. We give the number of studies that have reported the feature and the number of feature–depression associations that reached statistical significance as a proportion of the total such associations reported. See Supplementary Tables 3–10 for a list of tables with terms and feature definitions.
Fig. 4. Feature associations with depression by behaviour type.

The number of times each feature (a sleep, b physical activity, c circadian rhythm, d sociability, e location and f phone use) has been reported in all included studies and their association with depression, where these associations are defined as having a below-threshold p-value (“Significant Association”), above-threshold p-value (“Non-Significant Association”), and where statistical methods have been used that do not yield p-values (“Non-p-value”). The graphs also show the number of studies assessing each feature.
Twenty-nine studies collected data on sleep, typically ascertained using accelerometer, light and heart rate sensors. Nine different features of sleep are reported in Fig. 4A. Sleep quality, encompassing features relating to sleep fragmentation (number of awakenings and wake after sleep onset [WASO]), was the most commonly reported feature. Sleep efficiency is presented as a separate feature given its prevalence in studies. For all significant results, lower sleep efficiency or quality was associated with higher depression scores. Features with higher proportions of significant findings are features of sleep stability, sleep offset, time in bed; longer time in bed and later sleep offset were associated with higher depression scores.
Across studies finding significant results, sleep variability was higher for those with depression compared to controls (27), and those with more severe symptoms (28). The average length of follow-up for studies showing significant associations between sleep stability and depression was 24.7 days (range = 4–63), whereas that for studies showing no significant associations was 8.6 (range = 3–21).
Total sleep time showed mixed directionality of significance, with some studies finding negative correlations between total sleep time and higher depression26,32, others finding the depressed group having longer sleep time than controls33.
Measures of physical activity were collected in 19 studies using a mixture of smartphone (n = 8) and wearable devices (n = 11). Activity levels were predominantly measured as a gross motor activity within a day, and showed that depression was negatively correlated with physical activity20,34. Out of the seven studies extracting ‘activity levels’ as a feature within physical activity, both studies using smartphones found a significant difference in depression severity, compared to one out of the five that used wrist actigraphy. Higher depressive symptoms were associated with less time spent engaging in physical activity5, movement speed18 and step count27. Two out of the three studies looking at intensity found lower depression in those with more instances of intense activity and fewer sedentary behaviours5,20, with the third study35 finding no significant associations. The authors reported very little variability in activity intensity, which could account for such findings.
A total of 13 studies assessed movement patterns within a 24-h period. All used accelerometery data, except for Saeb7 who used GPS data for circadian movement. All significant associations indicated that disturbed rest-activity patterns were associated with depressive symptoms, however, in the majority of instances where circadian rhythm was reported, no significant association with mood was detected. Depression has been associated with lower daytime activity and higher night-time activity (hour-based activity levels36,37), low intra-daily stability, more fragmented intra-daily movement, e.g., leaving for work and coming back at less regular times7, later acrophase, or later activity peaks38–40; lower amplitude, less difference between the average levels of activity during the peaks vs. the troughs of activity20,39. Four studies calculated circadian rhythmicity as a measure of the extent to which a participant’s pattern follows an expected Cosinor model, finding lower circadian rhythmicity more likely to be associated with being depressed37,41–43.
Eleven studies assessed sociability. The average number of ingoing and outgoing calls was found to be negatively correlated with depressive symptoms in one small study (n = 6), and only in men44. Yang et al.45, with a combination of microphone, GPS and Bluetooth sensing as a proxy for social proximity, found that an interaction between environmental noise and proximity to others was informative of depressive state, e.g. being in a quiet place with few people around, compared to either spending time outside alone or in a noisy environment with more than 3 people. Other studies found that a higher frequency of conversations in the day and at night correlated with lower depression26, as well as being around human speech for longer46.
Location was assessed in 11 studies, measured via GPS. In addition to traditional statistical analyses, Saeb et al.7 estimated accuracy and mean normalised residual mean square difference (NRMSD) to assess the performance of prediction models. We, therefore, do not have levels of significance as expressed via p-values for all features. Entropy was reported in 26 cases in four different studies. High entropy, or spending more time in fewer, more consistent locations, was associated with depression, as compared to lower entropy, where people spend more time in a greater number of more varied locations. Features of location variance—how varied a participant’s locations are—show a negative correlation with depression, where the more varied the locations, the lower the likelihood of being depressed. Homestay—the amount of time spent at home—shows one of the most consistent patterns across the field, with all included studies reporting a significant association with depression.
Three studies associated individual phone use features with depression. All studies found that increased unlock duration and unlock frequency were associated with depression, non-p-value tests reported a mean NRMSD of 0.268 and 0.249, and 74.2% and 68.6% accuracy in classifying depressed vs. non-depressed participants, respectively. Increased use of specific apps, such as Instagram, iOS maps, and the use of photo and video apps was associated with greater depression, whereas book apps were associated with milder symptoms47.
The temperature was measured by Ávila-Moraes et al.36, who extracted more than 5 skin temperature features from a wrist-worn device, and found depressed people to have a longer time of elevated temperature compared to controls. One study48 reported no association between heart rate and depression scores.
Ávila-Moraes et al.36 also used a wrist-worn actigraphy device to measure light exposure and extracted four features. She found depressed groups to have a lower variance of light intensity than controls. Another study found humidity to have a significant positive correlation with depressed symptoms (r = 0.4) in women, but a negative correlation in men, suggesting females, but not males might feel worsening in their condition during rainy weeks44.
Sensitivity analysis
We carried out a sensitivity analysis to evaluate whether including only high-quality studies had any effect on our overall findings, the results of which can be found in Supplementary Fig. 3. After excluding studies with a score of eight out of 15 or lower, 20 papers remained. Overall, we found that excluding poor-quality studies did not change the patterns of association or significance ratios for sleep, physical activity, sociability, and location, beyond reducing the number of studies and therefore features that were analysed. Many of the studies on circadian rhythms are excluded, making existing associations even more tenuous; all studies showing a significant association between mood and intradaily stability or acrophase are lost, as are those finding no association between hour-based activity levels and depression. No studies looking at bivariate associations between phone use and depression remained.
Combined features
Tables 3 and 4 show the ten studies combining digital features to predict symptom severity (regression models) or depressive state (classification models). Twenty-four models in total were presented by all studies, the majority of which (n = 18) included features of physical activity, followed by location (n = 14), phone use (n = 11) and sleep (n = 9). Both classification and regression models showed predictive value, however, many of them lacked information regarding the handling of missing sensor data and calibration. Those that do, report simple imputation methods such as mean imputation, with two studies using multiple imputation methods6,18.
Table 3.
Details for studies analysing combined features using classification models.
| Study ID | Quality rating | First Author, Year | Device | Groups | N | No. of features | Feature type | Algorithm/model | Performance measure | Discrimination value | Missing data handling | Validation method | Comparison models |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 12 | Sano, 2018 | Q sensor, smartphone | MCS SF-12 Low vs. High | 47 | 204 | PA, SC, Li | SVM RBF | Accuracy | 85.1 | Interpolation | 10-fold cross-validation | LASSO, SVM Linear |
| 441 | PA, L, PU, SC, ST | SVM RBF | Accuracy | 86.1 | |||||||||
| 700 | S, PA, PU, SC, ST, HR, Cl | SVM RBF | Accuracy | 77.2 | |||||||||
| 296 | S, PA, PU | SVM RBF | Accuracy | 78.7 | |||||||||
| 25 | PU | SVM RBF | Accuracy | 71.1 | |||||||||
| 25 | S | SVM RBF | Accuracy | 65 | |||||||||
| 2 | 8 | Yue, 2018 | Android | Clinician MDD vs. HC | 25 | 8 | PA, L | SVM RBF | F1 | 0.66 | Multiple Imputation | LOOCV | l2-regularised (ridge) regression |
| iPhone | 54 | 8 | PA, L | SVM RBF | F1 | 0.76 | |||||||
| 3 | 8 | Wahle, 2016 | Smartphone | PHQ-9 Dep vs. HC | 36 | 120 | PA, So, L, PU | Random Forest | Accuracy | 60.1 | Unclear | LOOCV | SVM |
| 4 | 10 | Pratap, 2019 | Smartphone | PHQ-2 Dep vs. HC | 93 | 10 | So, L | Random Forest | Median AUC | >0.50 (for 80.6% sample) | Mean imputation | None | |
| 5 | 7 | Saeb, 2015 | Android | PHQ-9 Dep vs. HC | 18 | 8 | CR, L | Elastic Net Logistic Regression | Accuracy | 78.8 | Unclear | LOOCV | |
| 6 | 7 | Wang, 2018 | Smartphone | PHQ 4 Dep vs. HC | 83 | 9 | S, PA, L, PU, HR | Lasso Logistic Regression | AUC | 0.809 | Unclear | 10-fold cross validation | |
| 7 | 9 | Lu, 2018 | smartphone and Fitbit | QIDS | 69 | 36 | S, PA, So | Multi-Task Deep Learning | F1 | 0.77 | Exclusion | LO(W)OCV | STL (Lasso) STL (Ridge), MTL Lasso and Ridge |
MCS SF mental component survey short form, PHQ Patient Health Questionnaire, MDD major depressive disorder, HC healthy control, S sleep, PA physical activity, CR circadian rhythm, So Sociability, L Location, PU phone use, SC skin conductance, ST skin temperature, HR heart rate, Li light, Cl clinical data, SVM RBF Support Vector Machine - Radial Basis Function, AUC Area Under the Curve, LOOCV Leave One Out Cross Validation, STL Single Task Learning, MTL = Multi-Task Learning
Table 4.
Details for studies analysing combined features using regression models.
| Study ID | Quality rating | First Author, Year | Device | Outcome | N | No. of features | Feature type | Algorithm | Performance measure | Exact statistic | Missing data handling | Validation method | Comparison |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2 | 8 | Yue, 2018 | Android | PHQ9 | 25 | 8 | PA, L | SVM RBF | r | 0.46 | Multiple Imputation | LOOCV | Support Vector Multivariate Linear Regression |
| iPhone | PHQ9 | 54 | 8 | PA, L | SVM RBF | r | 0.41 | Support Vector Multivariate Linear Regression | |||||
| 4 | 10 | Pratap, 2019 | Smartphone | PHQ2 | 93 | 10 | PA, So, L | Random Forests | R2 | ≈ 0 | Mean Imputation | None Reported | |
| 5 | 7 | Saeb, 2015 | Smartphone | PHQ9 | 18 | 8 | CR, L | Elastic net Linear Regression | Mean NRMSD | 0.251 | Unclear | LOOCV | |
| 21 | 2 | PU | Elastic net linear regression | Mean NRMSD | 0.273 | ||||||||
| 6 | 7 | Wang, 2018 | Smartphone | pre PHQ 8 | 83 | 10 | S, PA, L, PU, HR | Lasso Linear Regression | MAE | 2.4 | Unclear | 10-fold cross validation | |
| post PHQ 8 | 83 | 5 | S, PA, So, L, PU | Lasso Linear Regression | MAE | 3.6 | |||||||
| 7 | 9 | Lu, 2018 | Smartphone, Fitbit | QIDS | 69 | 36 | S, PA, So | Multi-Task deep Learning | R2 | 0.44 | Exclusion | LO(W)OCV | STL (Lasso) STL (Ridge), MTL Lasso and Ridge |
| 8 | 7 | Burns, 2011 | Smartphone | PHQ9 | 7 | 38 | PA, So, L, PU, Li | Regression Trees | Accuracy | nr | Unclear | 10-fold cross validation | |
| 9 | 8 | Jacobson, 2019 | Actiwatch | BDI-II | 15 | nr | PA, Li | Xgboost | r | 0.86 | Unclear | LOOCV | |
| 10 | 7 | Ghandeharioun, 2017 | Empatica, Smartphone | HRDS | 12 | 700 | S, PA, PU | Combination of regularised regression, robust-to-outlier, boosting, Random Forest and Gaussian Process | RMSE | 4.5 | Multiple Imputation | 10-fold cross validation |
PHQ Patient Health Questionnaire, QIDS Quick Inventory of Depressive Symptomatology, nr not reported, S sleep, PA physical activity, CR circadian rhythm, So sociability, L location, PU phone use, SC skin conductance, ST skin temperature, HR heart rate, Li light, Cl clinical data, SVM RBF support vector machine-radial basis function, NRMSD normalised root-mean-square deviation, RMSE root-mean-square error, MAE mean absolute error, STL single-task learning, MTL multi-task learning.
Discussion
We sought to summarise the literature on passive sensing for depression, in order to map the methodological challenges and threats to reproducibility, in an effort to generate standards in the literature that allow for quantitative synthesis of results. We also assessed the available evidence for a relationship between sensor data and mood to identify leading digital signals for depression.
The first methodological shortcoming stems from the recency of this field. Studies have mostly employed opportunistic study designs, with small sample sizes, short follow-up windows and many being conducted on students, which limits generalisability. Different features may reach peak predictability of mood with different sampling timeframes, so shorter follow-ups may harm the prediction abilities for some behaviours22. This is presumably more likely in feature types such as sleep and circadian rhythm which benefit from having more aggregated baseline data49. There is no consensus on the timeframe window for optimal phenotyping, different windows, therefore, need to be evaluated.
A critical source of heterogeneity comes from the multitude of methods to create any individual feature, often without providing reasonable details of the process. A feature of sleep quality, for instance, defined in different studies as “Nocturnal Awakenings”, may have been constructed by measuring counts of awakenings, total number of minutes awake, or a proportion of awake vs. asleep in a sleep session. Additionally, there may be differences in how raw sensor data is used to classify an event as sleep or awake. This heterogeneity challenges the ability of investigators to reproduce findings and hampered our ability to summarise results in a meta-analysis.
The exploratory nature of many of these studies means that many different versions of the same feature may have been generated but studies do not transparently describe and justify feature selection and its association with depression. Researchers should provide a description of the feature, in the paper or supplement materials, that is sufficiently clear to allow for appropriate reproducibility.
Additionally, due to the large number of variables obtained in sensing studies, it is likely that published papers are selective in their reporting, and typically emphasise “positive” findings over “negative” ones. Preregistering studies and analyses would be one way of handling this. As the field matures and more studies are published, issues of rigour and reproducibility become more salient, and preregistration becomes more important to reduce reporting bias and cherry-picking in the field.
The sources of heterogeneity arise from varying data collection timespans, depression assessment measures, feature construction, and analytical methods. Whilst differences in these areas represent a healthy heterogeneity in an evolving field, it means that nuance is required in interpreting the presence or absence of a relationship between any specific signal and depressed mood. For example, many studies recruited students, who have different socialisation patterns and smartphone usage to older adults12,50. Prediction models based on younger populations have been found not to transfer to older age groups51. Further, a signal detected in a clinical sample consisting of people with relatively severe depression may not be reproduced in a population sample where the majority of the sample have few or no depressive symptoms and there may be less variability in key sensor data (e.g. sleep or activity data).
For any broad concept (e.g. sleep or circadian rhythm) different sensor types or operating systems were used, and component features were derived using different approaches. For example, both iPhone and Android smartphone operating systems were included, and sometimes showed differences in significance levels for the same variables5,18. This could be due to differences in sampling and data collections for both operating systems, or differences in the user profiles of these products52.
We found significant shortcomings in the literature in terms of fundamentals of reporting, including the most basic descriptors of sample characteristics, recruitment, attrition, and missing data. Whilst many of these shortcomings would be resolved by authors and journals following established reporting conventions (e.g. STROBE guidelines), there are a number of issues that are specific to this field.
One of those issues is missing data. Our quality assessments reflect poor reporting of missing data at both the sample level (e.g. attrition and study non-completion) and individual level (e.g. missing sensor data from participants). Missing data can arise from issues with technology, such as device and system failures, or from user-related issues which may be associated with depressed mood. For missing data to be used informatively, these two types need to be identified and dealt with in different ways in terms of their exclusion or analysis. Additionally, researchers set different thresholds as to what counts as missing data. This varies between studies and generates an important threat to reproducibility, making it crucial that these thresholds are reported. Our recommendation is that papers should clearly state how much data were missing and how it was managed in the analysis.
Remote sensing is a relatively new technology that potentially places a considerable burden on study participants—it was therefore surprising that few studies reported on the acceptability of the study protocol to participants. Where this did happen the emphasis was more on evaluating active questionnaire data rather than passive data and device use, where arguably greater issues over privacy and acceptability arise6,41.
Finally, there is a general lack of discussion around the extent to which the devices used in these research studies are valid or reliable tools to detect the behaviours of interest. While some behaviours may appear relatively simple to infer from single sensors, such as GPS sensors to infer location and accelerometry as a measure of movement and physical activity, there are validity and reliability concerns surrounding them. For example, although GPS receivers are generally good at detecting location and movement53, smartphone-based GPS receivers may differ in their measures of distance travelled54. Accelerometers are also generally accepted as reliable but can vary in their output and validity in measuring physical activity across devices55.
More complex behaviours such as sociability and sleep require multisensory data and a larger inferential leap. The evidence for actigraphy for the detection of sleep is uncertain, as several studies have found strong correlations between actigraphy and the gold standard of polysomnography (PSG)56,57, but a scoping review of 43 studies finding only moderate to poor agreement58. A more recent systematic review, however, found that while actigraphy tended to overestimate sleep and underestimate wake, this inaccuracy was consistent, thereby maintaining its usefulness as a potential marker of sleep–wake patterns59.
There is a clear gap in the definition of validity and reliability of these devices, however, whether or not these sensors measure the exact ground truth may be less concerning than whether the features we do extract are consistent against each other and serve the purpose of detecting changes in health status. So even though we would expect less reliable technologies to increase the noise to signal ratio, the extent to which any inaccuracies in the devices reduce the strength of association in depression is unknown.
Association between mood and digital features
Given the heterogeneity in research quality and reporting standards across studies, making inferences from aggregated associations between digital features and mood may be misleading. It would, however, be a missed opportunity to ignore growing consensus between studies in detecting associations between mood and digital features. We, therefore, report a synthesis of the findings but urge the reader to interpret this summary with caution.
Features that consistently appear to be associated with depression are location-based features, with homestay and entropy both associated with the mood in 4 and 5 studies, respectively. However, these studies do not determine the direction of causality, i.e. whether changes in sensed features such as homestay are merely a reflection of behaviours that appear in depression, such as reduced physical activity and social withdrawal60,61 or whether they are, in themselves, predictors of deterioration in mood.
Several sleep features appear also to be consistently associated with depressed mood, with sleep stability showing the highest proportion of significant associations. When measuring socialisation, proximity-related features using Bluetooth and microphone sensors seem more sensitive to mood than call and message frequency counts. However, many of these studies have small sample sizes (median = 58), student samples with a low mean age34 or report a high degree of intra- and interindividual variance in daily phone usage62. Recent studies with larger and more diverse samples using classification machine learning techniques have found that a low average number and duration of calls made daily predicted depression state63.
Even though disruptions in circadian rhythms have been thought to affect depression64, the majority of studied features did not have a significant association with mood. As previously mentioned, this may be due to short follow-up since median follow-up times for circadian features = 9 days.
The findings of this review highlight the array of potential predictors that sensor data generates. As such, machine learning methods have been the choice analytic approach to the digital phenotyping of depression from multiple features. In addition to helping account for important interactions between the objective features, for example how the effect of being alone is mediated by location (being indoors vs outdoors)45, analysing multimodal data in this way may help cover missing data from one source to another. However, machine learning methods have been criticised for lacking transparency in how the model is built and how individual variables contribute to the overall prediction65. Some studies in the current review do report their top predictors and bivariate associations with depression, but the question of how well these models can be replicated remains, highlighting the importance of thorough reporting.
Strengths and limitations
Our attempt to summarise the literature is necessarily crude because the reporting of feature–depression associations was too opaque and diverse to allow any credible attempt at meta-analysis. We have therefore had to rely on simple counts of associations reported, and this comes with caveats that reports are not weighted by sample size, follow-up duration or study quality. It is possible that the associations we have reported are due to reporting bias, as mentioned in the previous section, where investigators emphasise “significant” findings over “non-significant” ones.
To present low-level features in a clear and meaningful way in this review, we combined them into broader low-level features and therefore some of the nuances between them were lost. For example, if one study extracted two features such as a total number of minutes spent in phone calls and the average length of a phone call, they would both load into Call Duration, within the “Sociability” Feature Type (Supplementary Tables 3–10).
Several studies included in this review have overlapping samples as they come from existing datasets. For example, four papers26,42,45,48 use the StudentLife open dataset, where there is some similarity in the analysis, meaning that some of the feature associations may be duplicated.
Recommendations and conclusions
Whilst there have been attempts at standardising reporting standards for actively collected questionnaire data on mood66, and guidelines exist for the reporting of observational data (STROBE67) and multivariable prediction models (TRIPOD statement68), there is a need to develop consensus over the manner in which such mobile health studies are conducted and reported. This should not come at the expense of stifling innovation and should acknowledge that a new field of study takes time to develop.
The literature we identified derives from both clinical and computer science disciplines and some of the heterogeneity we report results from these disciplines having distinct conventions, with medical outputs putting more weight on sample and clinical outcome characteristics but often overlooking feature extraction and analysis description. The importance of recruiting and reporting the diversity of study samples, however, is highlighted by the difference in validity of these devices in detecting the behaviours of interest. For example, some wearable devices may be more accurate on lighter skin tones69, and on men70.
There is a need for experts across the disciplines to build upon and generate a consensus on a set of established guidelines, but based on this work, the following recommendations emerge as a first step at attempting to improve the generalisability of research and generate a more standardised approach to passive sensing in depression.
Sample recommendations:
Report recruitment strategies, sampling frames and participation rates.
Increase the diversity of study populations by recruiting participants of different ages and ethnicities.
Report basic demographic and clinical data such as age, gender, ethnicity and comorbidities.
Measure and report participant engagement and acceptability in the form of attrition rates, missing data, and/or qualitative data.
Data collection and analysis:
Use established and validated scales for depression assessment.
Present the available evidence, if any, on the validity and reliability of the sensor or device used.
Register study protocol including pre-specification of analytical plans and hypotheses.
Describe in sufficient detail to allow replication, data processing and feature construction.
Provide a definition and description of missing data management.
In machine learning models, describe the model selection strategy, performance metrics and parameter estimates in the model with confidence intervals, or nonparametric equivalents (for a full guideline on reporting machine learning models see Luo71).
Data sharing considerations:
Make the code used for feature extraction available within an open science framework.
Share anonymised datasets on data repositories.
The above points cover aspects of transparency, validity and generalisability. Data sharing considerations become critical in this respect, especially with the use of big data and machine learning models, where validation of the model and data is an integral part of the process. It is therefore important to work towards the creation of open datasets or the widespread sharing of data and to work with community groups to standardise the description, exchange and use of mobile health data.
Our most pressing recommendation, however, is that there is a need for consistency in reporting in this field. The failure to report basic demographic information found in many studies, particularly from the computer science field, and the limited description in feature extraction and analysis in medical papers, have important implications for the interpretation of findings. A common framework, with standardised assessment and analytical tools, robust feature extraction and missing data descriptions, tested in more representative populations would be an important step towards improving the ability of researchers to evaluate the strength of the evidence.
Methods
Search strategy and selection criteria
We searched Pubmed, IEEE Xplore, ACM Digital library, Web of Science, and Embase and PsychInfo via OVID, for studies published between January 2007 until November 2019, and used a combination of terms related to the key concepts of (1) depression and (2) digital sensors and remote measurement technologies (RMTs) (full search in the Supplementary Note 1). We also conducted searches based on bibliographies of reviews and meta-analyses on the topic. The protocol was registered on PROSPERO 2019 CRD42019159929.
Studies had to have measured depressive symptoms in either clinical or epidemiological samples and to consist of samples with mean ages between 18 and 65 years, due to the differences in behavioural patterns for older adults and children. We limited studies to those which had extracted data for at least 3 consecutive days (to allow for intraday mood fluctuations) from smartphones and wrist-worn devices. Data from devices not worn on the wrist, e.g. on the chest, upper arm or hip, were excluded due to measurement discrepancies between devices worn in different body parts72. Studies had to link data between validated scales of depression severity or status (case/non-case) and digital sensor-based variables including measures of behaviour, e.g. activity, sleep, etc., gathered passively. Studies had to be written in English, German or Spanish because these are the languages spoken by the reviewers, be published, peer-reviewed and with accessible full text.
Studies were excluded if their primary focus related to a condition other than depression as well as those from inpatient settings. Studies focusing specifically on bipolar depression were excluded, however, mixed studies consisting of unipolar and bipolar were included provided unipolar cases comprised a substantial majority (at least 80%) of the sample. We excluded studies published before 2007 as this was when the first smartphones became available.
Procedure
Studies were checked for eligibility by two researchers independently screening titles and abstracts. Potentially eligible studies’ full texts were reviewed by one researcher, with a second researcher evaluating a random sample of 10% of all texts for validating purposes. Disagreements at any stage of eligibility and data extraction were resolved by discussing with an additional reviewer. Agreement of >90% was reached for all reviewer pairs. The eligibility process was documented according to PRISMA guidelines73.
Data extraction
Data extraction included the following variables: sample characteristics (N, mean age, gender, ethnicity), comorbidities, study design, study setting (clinical, community, student), depression outcome measures, length of follow-up, device type, features measured, sensors used, statistical analyses and significance levels.
Study quality assessment
No single quality assessment tool was suitable because of the ditabversity of study types. We, therefore, combined the Appraisal Tool for Cross-Sectional Studies (AXIS tool74 and the Newcastle–Ottawa Scale (NOS) for longitudinal studies75. Items were scored with two points for fully fulfilled items, one point for partially fulfilled items, and zero for a non-fulfilled item (see Supplementary Table 11 for a description of each criterion). We added an item regarding having a published protocol prior to publishing results (1 point for a published protocol). Data extraction was carried out on all studies, regardless of their quality assessment score.
Feasibility
We collected information on five measures of the feasibility of using digital health tools, with the aim of identifying potential obstacles to their implementation: engagement with study devices, reasons for study drop out, reported problems with technology, percentage of study tasks completed, attrition and missing data.
Data synthesis
Eight categories of behavioural features were identified: sleep, physical activity, circadian rhythm (rest-activity patterns through a 24-h period), sociability, location, physiological parameters, phone use and environmental features. Supplementary Tables 3–10 provide descriptions for each feature. Within each behavioural category, there are lower-level features, which group together several individual features as reported by each study. It was therefore possible for a single study to present multiple associations for the same feature. Significant associations according to 0.05 p-value thresholds are presented. Due to the heterogeneity of feature types, study designs and data reporting we did not conduct a meta-analysis.
Supplementary information
Acknowledgements
This study represents independent research funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
Author contributions
V.d.A. and M.H. conceived and designed the review. V.d.A. and F.M. generated the search strategy and V.d.A. searched the databases. Studies were screened for eligibility by V.d.A., S.L., K.W., C.O., A.P., E.O., who, along with D.L. and G.L., carried out data extraction. V.d.A. wrote the first draft and all authors contributed to subsequent drafts and edits to the manuscript. All authors approved the manuscript.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Competing interests
M.H. is principal investigator of the RADAR-CNS programme, a precompetitive public–private partnership funded by the Innovative Medicines Initiative and European Federation of Pharmaceutical Industries and Associations. The programme receives support from Janssen, Biogen, MSD, UCB and Lundbeck. D.C.M. has accepted honoraria and consulting fees from Apple, Inc., Otsuka Pharmaceuticals, Pear Therapeutics, and the One Mind Foundation, royalties from Oxford Press, and has an ownership interest in Adaptive Health, Inc. All other authors declare that they have no competing interests.
Footnotes
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
The online version contains supplementary material available at 10.1038/s41746-021-00548-8.
References
- 1.World Health Organisation. Depression. https://www.who.int/news-room/fact-sheets/detail/depression (2020).
- 2.Verhoeven JE, et al. Complete recovery from depression is the exception rather than the rule: prognosis of depression beyond diagnostic boundaries. Ned. Tijdschr. Geneeskd. 2018;162:D2920. [PubMed] [Google Scholar]
- 3.Kraus C, Kadriu B, Lanzenberger R, Zarate CA, Jr, Kasper S. Prognosis and improved outcomes in major depression: a review. Transl. Psychiatry. 2019;9:1–17. doi: 10.1038/s41398-019-0460-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cho YM, et al. A cross-sectional study of the association between mobile phone use and symptoms of ill health. Environ. Health Toxicol. 2016;31:e2016022. doi: 10.5620/eht.e2016022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lu, J. et al. Joint modeling of heterogeneous sensing data for depression assessment via multi-task learning. In Proc. ACM Interactive Mobile, Wearable and Ubiquitous Technology. Vol. 2, 21:1–21:21 (ACM, 2018).
- 6.Ghandeharioun, A. et al. Objective assessment of depressive symptoms with machine learning and wearable sensors data. In Proc.2017 7th International Conference on Affective Computing and Intelligent Interaction (ACII). 325–332 (IEEE, 2017).
- 7.Saeb S, et al. Mobile phone sensor correlates of depressive symptom severity in daily-life behavior: an exploratory study. J. Med. Internet Res. 2015;17:e175. doi: 10.2196/jmir.4273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Vailshery, L. S. Ownership of smartphones in the UK 2020. Statistahttps://www.statista.com/statistics/956297/ownership-of-smartphones-uk/ (2021).
- 9.Mohr DC, Shilton K, Hotopf M. Digital phenotyping, behavioral sensing, or personal sensing: names and transparency in the digital age. Npj Digit. Med. 2020;3:1–2. doi: 10.1038/s41746-020-0251-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mohr, et al Personal sensing: understanding mental health using ubiquitous sensors and machine learning. In Annual Review ofClinical Psychology, Vol. 13 (eds Widiger, T. & Cannon, T. D.) 23–47 (2017). [DOI] [PMC free article] [PubMed]
- 11.Rohani DA, Faurholt-Jepsen M, Kessing LV, Bardram JE. Correlations between objective behavioral features collected from mobile and wearable devices and depressive mood symptoms in patients with affective disorders: systematic review. JMIR MHealth UHealth. 2018;6:e165. doi: 10.2196/mhealth.9691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Melcher, J., Hays, R. & Torous, J. Digital phenotyping for mental health of college students: a clinical review. Evid. Based Ment. Health ebmental-2020-300180. 10.1136/ebmental-2020-300180 (2020). [DOI] [PMC free article] [PubMed]
- 13.Faurholt-Jepsen M, et al. Differences in psychomotor activity in patients suffering from unipolar and bipolar affective disorder in the remitted or mild/moderate depressive state. J. Affect. Disord. 2012;141:457–463. doi: 10.1016/j.jad.2012.02.020. [DOI] [PubMed] [Google Scholar]
- 14.Dogan E, Sander C, Wagner X, Hegerl U, Kohls E. Smartphone-based monitoring of objective and subjective data in affective disorders: where are we and where are we going? Systematic review. J. Med. Internet Res. 2017;19:e262. doi: 10.2196/jmir.7006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Radloff LS. The CES-D Scale: a self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977;1:385–401. [Google Scholar]
- 16.Hamilton M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry. 1960;23:56–62. doi: 10.1136/jnnp.23.1.56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J. Gen. Intern. Med. 2001;16:606–613. doi: 10.1046/j.1525-1497.2001.016009606.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Yue, C. et al. Fusing location data for depression prediction. IEEE Trans. Big Data 1–1 10.1109/TBDATA.2018.2872569 (2018). [DOI] [PMC free article] [PubMed]
- 19.Burns MN, et al. Harnessing context sensing to develop a mobile intervention for depression. J. Med. Internet Res. 2011;13:e55. doi: 10.2196/jmir.1838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Difrancesco S, et al. Sleep, circadian rhythm, and physical activity patterns in depressive and anxiety disorders: a 2-week ambulatory assessment study. Depress. Anxiety. 2019;36:975–986. doi: 10.1002/da.22949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dillon CB, McMahon E, O’Regan G, Perry IJ. Associations between physical behaviour patterns and levels of depressive symptoms, anxiety and well-being in middle-aged adults: a cross-sectional study using isotemporal substitution models. BMJ Open. 2018;8:e018978. doi: 10.1136/bmjopen-2017-018978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sano A, et al. Identifying objective physiological markers and modifiable behaviors for self-reported stress and mental health status using wearable sensors and mobile phones: observational study. J. Med. Internet Res. 2018;20:e210. doi: 10.2196/jmir.9410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wahle F, Kowatsch T, Fleisch E, Rufer M, Weidt S. Mobile sensing and support for people with depression: a Pilot Trial in the Wild. JMIR MHealth UHealth. 2016;4:e111. doi: 10.2196/mhealth.5960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Naismith SL, et al. Sleep disturbance relates to neuropsychological functioning in late-life depression. J. Affect. Disord. 2011;132:139–145. doi: 10.1016/j.jad.2011.02.027. [DOI] [PubMed] [Google Scholar]
- 25.Byrne JEM, Bullock B, Brydon A, Murray G. A psychometric investigation of the sleep, circadian rhythms, and mood (SCRAM) questionnaire. Chronobiol. Int. 2019;36:265–275. doi: 10.1080/07420528.2018.1533850. [DOI] [PubMed] [Google Scholar]
- 26.Wang, R. et al. StudentLife: assessing mental health, academic performance and behavioral trends of college students using smartphones. In Proc. 2014 ACM International Joint Conference on Pervasive and Ubiquitous Computing—UbiComp’14 Adjunct 3–14 (ACM Press, 2014).
- 27.Moukaddam N, Truong A, Cao J, Shah A, Sabharwal A. Findings from a trial of the Smartphone and OnLine Usage-based eValuation for Depression (SOLVD) application: what do apps really tell us about patients with depression? Concordance between app-generated data and standard psychiatric questionnaires for depression and anxiety. J. Psychiatr. Pract. 2019;25:365–373. doi: 10.1097/PRA.0000000000000420. [DOI] [PubMed] [Google Scholar]
- 28.Pillai V, Steenburg LA, Ciesla JA, Roth T, Drake CL. A seven day actigraphy-based study of rumination and sleep disturbance among young adults with depressive symptoms. J. Psychosom. Res. 2014;77:70–75. doi: 10.1016/j.jpsychores.2014.05.004. [DOI] [PubMed] [Google Scholar]
- 29.Vanderlind WM, et al. Sleep and sadness: exploring the relation among sleep, cognitive control, and depressive symptoms in young adults. Sleep. Med. 2014;15:144–149. doi: 10.1016/j.sleep.2013.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Luik AI, et al. 24-Hour activity rhythm and sleep disturbances in depression and anxiety: a population-based study of middle-aged and older persons. Depress. Anxiety. 2015;32:684–692. doi: 10.1002/da.22355. [DOI] [PubMed] [Google Scholar]
- 31.Takano K, Sakamoto S, Tanno Y. Repetitive thought impairs sleep quality: an Experience Sampling Study. Behav. Ther. 2014;45:67–82. doi: 10.1016/j.beth.2013.09.004. [DOI] [PubMed] [Google Scholar]
- 32.Kawada T, Katsumata M, Suzuki H, Shimizu T. Actigraphic predictors of the depressive state in students with no psychiatric disorders. J. Affect. Disord. 2007;98:117–120. doi: 10.1016/j.jad.2006.07.004. [DOI] [PubMed] [Google Scholar]
- 33.Robillard R, et al. Sleep–wake cycle and melatonin rhythms in adolescents and young adults with mood disorders: comparison of unipolar and bipolar phenotypes. Eur. Psychiatry J. Assoc. Eur. Psychiatry. 2013;28:412–416. doi: 10.1016/j.eurpsy.2013.04.001. [DOI] [PubMed] [Google Scholar]
- 34.Boukhechba, M. et al. Contextual analysis to understand compliance with smartphone-based ecological momentary assessment. In Proc. 12th EAI International Conference on Pervasive Computing Technologies for Healthcare 232–238 (ACM, 2018).
- 35.Tao K, et al. Associations between self-determined motivation, accelerometer-determined physical activity, and quality of life in Chinese College Students. Int. J. Environ. Res. Public Health. 2019;16:2941. doi: 10.3390/ijerph16162941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ávila Moraes C, et al. A new chronobiological approach to discriminate between acute and chronic depression using peripheral temperature, rest-activity, and light exposure parameters. BMC Psychiatry. 2013;13:77. doi: 10.1186/1471-244X-13-77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Slyepchenko A, et al. Association of functioning and quality of life with objective and subjective measures of sleep and biological rhythms in major depressive and bipolar disorder. Aust. N. Z. J. Psychiatry. 2019;53:683–696. doi: 10.1177/0004867419829228. [DOI] [PubMed] [Google Scholar]
- 38.Robillard R, et al. Ambulatory sleep-wake patterns and variability in young people with emerging mental disorders. J. Psychiatry Neurosci. JPN. 2015;40:28–37. doi: 10.1503/jpn.130247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Smagula SF, Krafty RT, Thayer JF, Buysse DJ, Hall MH. Rest–activity rhythm profiles associated with manic-hypomanic and depressive symptoms. J. Psychiatr. Res. 2018;102:238–244. doi: 10.1016/j.jpsychires.2018.04.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.White KH, Rumble ME, Benca RM. Sex differences in the relationship between depressive symptoms and actigraphic assessments of sleep and rest–activity rhythms in a population-based sample. Psychosom. Med. 2017;79:479–484. doi: 10.1097/PSY.0000000000000434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Robillard R, et al. Sleep–wake cycle in young and older persons with a lifetime history of mood disorders. PLoS ONE. 2014;9:e87763. doi: 10.1371/journal.pone.0087763. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Saeb S, Lattie EG, Schueller SM, Kording KP, Mohr DC. The relationship between mobile phone location sensor data and depressive symptom severity. PeerJ. 2016;4:e2537. doi: 10.7717/peerj.2537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Robillard R, et al. Sleep–wake profiles predict longitudinal changes in manic symptoms and memory in young people with mood disorders. J. Sleep Res. 2016;25:549–555. doi: 10.1111/jsr.12413. [DOI] [PubMed] [Google Scholar]
- 44.Doryab, A., Min, J. K., Wiese, J., Zimmerman, J. & Hong, J. Detection of behavior change in people with depression. In Proc. of the 28th AAAI Conference on Artificial Intelligence, Vol. 5 (Québec City, QC, Canada, 2014).
- 45.Yang, Z., Mo, X., Shi, D. & Wang, R. Mining relationships between mental health, academic performance and human behaviour. In 2017 IEEE SmartWorld, Ubiquitous Intelligence Computing, Advanced Trusted Computed, Scalable Computing Communications, Cloud Big Data Computing, Internet of People and Smart City Innovation (SmartWorld/SCALCOM/UIC/ATC/CBDCom/IOP/SCI). 1–8 (IEEE, 2017).
- 46.Ben-Zeev D, Scherer EA, Wang R, Xie H, Campbell AT. Next-generation psychiatric assessment: using smartphone sensors to monitor behavior and mental health. Psychiatr. Rehabil. J. 2015;38:218–226. doi: 10.1037/prj0000130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.David ME, Roberts JA, Christenson B. Too much of a good thing: investigating the association between actual smartphone use and individual well-being. Int. J. Hum.–Comput. Interact. 2018;34:265–275. [Google Scholar]
- 48.Wang, R. et al. Tracking depression dynamics in college students using mobile phone and wearable sensing. In Proc. ACM on Interactive, Mobile, Wearable and Ubiquitous Technology. Vol. 2, 43:1–43:26 (ACM, 2018).
- 49.Littner M, et al. Practice parameters for the role of actigraphy in the study of sleep and circadian rhythms: an update for 2002. Sleep. 2003;26:337–341. doi: 10.1093/sleep/26.3.337. [DOI] [PubMed] [Google Scholar]
- 50.Xu, X. et al. Leveraging routine behavior and contextually-filtered features for depression detection among college students. In Proc. ACM on Interactive, Mobile, Wearable and Ubiquitous Technology. Vol. 3, 1–33 (ACM, 2019).
- 51.Liu, T. et al. Machine learning for phone-based relationship estimation: the need to consider population heterogeneity. In Proc. ACM on Interactive, Mobile, Wearable and Ubiquitous Technology. Vol. 3, 145:1–145:23 (ACM, 2019). [DOI] [PMC free article] [PubMed]
- 52.Gerpott TJ, Thomas S, Weichert M. Characteristics and mobile Internet use intensity of consumers with different types of advanced handsets: an exploratory empirical study of iPhone, Android and other web-enabled mobile users in Germany. Telecommun. Policy. 2013;37:357–371. [Google Scholar]
- 53.Pirotti, F., Guarnieri, A., Piragnolo, M., Boscaro, M. & Cavalli, R. Analysis of geospatial behaviour of visitors of urban gardens: is positioning via smartphones a valid solution? Preprint at ArXiv: 2107:03925 Cs (2021).
- 54.Adamakis M. Comparing the validity of a GPS monitor and a smartphone application to measure physical activity. J. Mob. Technol. Med. 2017;6:28–38. [Google Scholar]
- 55.Plasqui G, Bonomi AG, Westerterp KR. Daily physical activity assessment with accelerometers: new insights and validation studies. Obes. Rev. 2013;14:451–462. doi: 10.1111/obr.12021. [DOI] [PubMed] [Google Scholar]
- 56.Elbaz M, Roue GM, Lofaso F, Quera Salva MA. Utility of actigraphy in the diagnosis of obstructive sleep apnea. Sleep. 2002;25:527–531. [PubMed] [Google Scholar]
- 57.Lichstein KL, et al. Actigraphy validation with insomnia. Sleep. 2006;29:232–239. [PubMed] [Google Scholar]
- 58.Baron KG, et al. Feeling validated yet? A scoping review of the use of consumer-targeted wearable and mobile technology to measure and improve sleep. Sleep Med. Rev. 2018;40:151–159. doi: 10.1016/j.smrv.2017.12.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Conley S, et al. Agreement between actigraphic and polysomnographic measures of sleep in adults with and without chronic conditions: a systematic review and meta-analysis. Sleep Med. Rev. 2019;46:151–160. doi: 10.1016/j.smrv.2019.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Cacioppo JT, Hughes ME, Waite LJ, Hawkley LC, Thisted RA. Loneliness as a specific risk factor for depressive symptoms: cross-sectional and longitudinal analyses. Psychol. Aging. 2006;21:140–151. doi: 10.1037/0882-7974.21.1.140. [DOI] [PubMed] [Google Scholar]
- 61.Segel-Karpas D, Ayalon L, Lachman ME. Loneliness and depressive symptoms: the moderating role of the transition into retirement. Aging Ment. Health. 2018;22:135–140. doi: 10.1080/13607863.2016.1226770. [DOI] [PubMed] [Google Scholar]
- 62.Pratap A, et al. The accuracy of passive phone sensors in predicting daily mood. Depress. Anxiety. 2019;36:72–81. doi: 10.1002/da.22822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Razavi R, Gharipour A, Gharipour M. Depression screening using mobile phone usage metadata: a machine learning approach. J. Am. Med. Inform. Assoc. 2020;27:522–530. doi: 10.1093/jamia/ocz221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Germain A, Kupfer DJ. Circadian rhythm disturbances in depression. Hum. Psychopharmacol. Clin. Exp. 2008;23:571–585. doi: 10.1002/hup.964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Wall R, Cunningham P, Walsh P, Byrne S. Explaining the output of ensembles in medical decision support on a case by case basis. Artif. Intell. Med. 2003;28:191–206. doi: 10.1016/s0933-3657(03)00056-3. [DOI] [PubMed] [Google Scholar]
- 66.Faurholt-Jepsen M, et al. Reporting guidelines on remotely collected electronic mood data in mood disorder (eMOOD)—recommendations. Transl. Psychiatry. 2019;9:1–10. doi: 10.1038/s41398-019-0484-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Elm Evon, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370:1453–1457. doi: 10.1016/S0140-6736(07)61602-X. [DOI] [PubMed] [Google Scholar]
- 68.Collins GS, Reitsma JB, Altman DG, Moons KGM. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): the TRIPOD statement. BMJ. 2015;350:g7594. doi: 10.1136/bmj.g7594. [DOI] [PubMed] [Google Scholar]
- 69.Colvonen PJ, DeYoung PN, Bosompra N-OA, Owens RL. Limiting racial disparities and bias for wearable devices in health science research. Sleep. 2020;43:zsaal159. doi: 10.1093/sleep/zsaa159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Nuss KJ, et al. Assessment of accuracy of overall energy expenditure measurements for the Fitbit Charge HR 2 and Apple Watch. Am. J. Health Behav. 2019;43:498–505. doi: 10.5993/AJHB.43.3.5. [DOI] [PubMed] [Google Scholar]
- 71.Luo W, et al. Guidelines for developing and reporting machine learning predictive models in biomedical research: a multidisciplinary view. J. Med. Internet Res. 2016;18:e5870. doi: 10.2196/jmir.5870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Cellini N, McDevitt EA, Mednick SC, Buman MP. Free-living cross-comparison of two wearable monitors for sleep and physical activity in healthy young adults. Physiol. Behav. 2016;157:79–86. doi: 10.1016/j.physbeh.2016.01.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Moher D, Liberati A, Tetzlaff J, Altman DG, Group TP. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Downes MJ, Brennan ML, Williams HC, Dean RS. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS) BMJ Open. 2016;6:e011458. doi: 10.1136/bmjopen-2016-011458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Wells, G. et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analysis. 21, (2000).
- 76.Caldwell BA, Redeker NS. Sleep patterns and psychological distress in women living in an inner city. Res. Nurs. Health. 2009;32:177–190. doi: 10.1002/nur.20308. [DOI] [PubMed] [Google Scholar]
- 77.Doane LD, Gress-Smith JL, Breitenstein RS. Multi-method assessments of sleep over the transition to college and the associations with depression and anxiety symptoms. J. Youth Adolesc. 2015;44:389–404. doi: 10.1007/s10964-014-0150-7. [DOI] [PubMed] [Google Scholar]
- 78.Haeffel GJ. Don’t sleep on it: less sleep reduces risk for depressive symptoms in cognitively vulnerable undergraduates. J. Pers. Soc. Psychol. 2017;113:925–938. doi: 10.1037/pspp0000119. [DOI] [PubMed] [Google Scholar]
- 79.Hori H, et al. 24-h activity rhythm and sleep in depressed outpatients. J. Psychiatr. Res. 2016;77:27–34. doi: 10.1016/j.jpsychires.2016.02.022. [DOI] [PubMed] [Google Scholar]
- 80.Jacobson NC, Weingarden H, Wilhelm S. Using digital phenotyping to accurately detect depression severity. J. Nerv. Ment. Disord. 2019;207:893–896. doi: 10.1097/NMD.0000000000001042. [DOI] [PubMed] [Google Scholar]
- 81.Knight A, Bidargaddi N. Commonly available activity tracker apps and wearables as a mental health outcome indicator: a prospective observational cohort study among young adults with psychological distress. J. Affect. Disord. 2018;236:31–36. doi: 10.1016/j.jad.2018.04.099. [DOI] [PubMed] [Google Scholar]
- 82.Li, X., Kearney, P. M. & Fitzgerald, A. P. Accelerometer-based physical activity patterns and correlates of depressive symptoms. In Health Information Science (HIS 2018), Vol. 11148 (eds Siuly, S., Lee, I., Huang, Z., Zhou, R., Wang, H. & Xiang, W.) 37–47 (Springer International, 2018).
- 83.Luik AI, Zuurbier LA, Hofman A, Van Someren EJW, Tiemeier H. Stability and fragmentation of the activity rhythm across the sleep–wake cycle: the importance of age, lifestyle, and mental health. Chronobiol. Int. 2013;30:1223–1230. doi: 10.3109/07420528.2013.813528. [DOI] [PubMed] [Google Scholar]
- 84.McCall WV. A rest–activity biomarker to predict response to SSRIs in major depressive disorder. J. Psychiatr. Res. 2015;64:19–22. doi: 10.1016/j.jpsychires.2015.02.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Mendoza-Vasconez AS, Marquez B, Linke S, Arredondo EM, Marcus BH. Effect of physical activity on depression symptoms and perceived stress in Latinas: a mediation analysis. Ment. Health Phys. Act. 2019;16:31–37. doi: 10.1016/j.mhpa.2019.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Naismith SL, et al. Sleep disturbance relates to neuropsychological functioning in late-life depression. J. Affect. Disord. 2011;132:139–145. doi: 10.1016/j.jad.2011.02.027. [DOI] [PubMed] [Google Scholar]
- 87.Park D-H, Kripke DF, Cole RJ. More prominent reactivity in mood than activity and sleep induced by differential light exposure due to seasonal and local differences. Chronobiol. Int. 2007;24:905–920. doi: 10.1080/07420520701669677. [DOI] [PubMed] [Google Scholar]
- 88.Pillai V, Steenburg LA, Ciesla JA, Roth T, Drake CL. A seven day actigraphy-based study of rumination and sleep disturbance among young adults with depressive symptoms. J. Psychosom. Res. 2014;77:70–75. doi: 10.1016/j.jpsychores.2014.05.004. [DOI] [PubMed] [Google Scholar]
- 89.Pratap A, et al. The accuracy of passive phone sensors in predicting daily mood. Depress. Anxiety. 2019;36:72–81. doi: 10.1002/da.22822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Robillard R, et al. Sleep-wake profiles predict longitudinal changes in manic symptoms and memory in young people with mood disorders. J. Sleep Res. 2016;25:549–555. doi: 10.1111/jsr.12413. [DOI] [PubMed] [Google Scholar]
- 91.Robillard R, et al. Circadian rhythms and psychiatric profiles in young adults with unipolar depressive disorders. Transl. Psychiatry. 2018;8:213. doi: 10.1038/s41398-018-0255-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Smagula SF, et al. Rest–activity rhythms characteristics and seasonal changes in seasonal affective disorder. Chronobiol. Int. 2018;35:1553–1559. doi: 10.1080/07420528.2018.1496094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Stremler R, Haddad S, Pullenayegum E, Parshuram C. Psychological outcomes in parents of critically ill hospitalized children. J. Pediatr. Nurs. 2017;34:36–43. doi: 10.1016/j.pedn.2017.01.012. [DOI] [PubMed] [Google Scholar]
- 94.Vallance JK, Eurich D, Lavallee C, Johnson ST. Daily pedometer steps among older men: associations with health-related quality of life and psychosocial health. Am. J. Health Promot. 2013;27:294–298. doi: 10.4278/ajhp.120316-QUAN-145. [DOI] [PubMed] [Google Scholar]
- 95.Vanderlind WM, et al. Sleep and sadness: exploring the relation among sleep, cognitive control, and depressive symptoms in young adults. Sleep Med. 2014;15:144–149. doi: 10.1016/j.sleep.2013.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Wang, R. et al. Tracking depression dynamics in college students using mobile phone and wearable sensing. In Proc. ACM Interactive Mobile, Wearable and Ubiquitous Technology, Vol. 2, 1–26 (2018).
- 97.Yaugher AC, Alexander GM. Internalizing and externalizing traits predict changes in sleep efficiency in emerging adulthood: an actigraphy study. Front. Psychol. 2015;6:1495. doi: 10.3389/fpsyg.2015.01495. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.