

Abstract
Aims
College students who drink are at an increased risk of driving after drinking and alcohol-involved traffic accidents and deaths. Furthermore, the persistence of driving after drinking over time underscores a need for effective interventions to prevent future drunk driving in adulthood. The present study examined whether brief alcohol interventions (BAIs) for college students reduce driving after drinking.
Methods
A two-step meta-analysis of individual participant data (IPD) was conducted using a combined sample of 6801 college students from 15 randomized controlled trials (38% male, 72% White and 58% first-year students). BAIs included individually delivered Motivational Interviewing with Personalized Feedback (MI + PF), Group Motivational Interviewing (GMI), and stand-alone Personalized Feedback (PF) interventions. Two outcome variables, driving after two+/three+ drinks and driving after four+/five+ drinks, were checked, harmonized and analyzed separately for each study and then combined for meta-analysis and meta-regression analysis.
Results
BAIs lowered the risk of driving after four+/five+ drinks (19% difference in the odds of driving after drinking favoring BAIs vs. control), but not the risk of driving after two+/three+ drinks (9% difference). Subsequent subgroup analysis indicated that the MI + PF intervention was comparatively better than PF or GMI.
Conclusions
BAIs provide a harm reduction approach to college drinking. Hence, it is encouraging that BAIs reduce the risk of driving after heavy drinking among college students. However, there may be opportunities to enhance the intervention content and timing to be more relevant for driving after drinking and improve the outcome assessment and reporting to demonstrate its effect.
Short Summary: BAIs have been a prevailing intervention strategy to prevent harm from drinking among college students. We found that BAIs statistically significantly lowered the risk of driving after four+/five+ drinks in a two-step meta-analysis of IPD. We provide clinical and methodological suggestions to enhance the effect.
INTRODUCTION
Driving after drinking is a serious public health concern in the USA. Although the prevalence of overall alcohol-involved traffic fatalities (National Center for Statistics and Analysis, 2019), young adult alcohol-involved traffic fatalities and binge drinking have decreased (Hingson et al., 2017; Schulenberg et al., 2019) in the last three decades, the rates of driving after drinking, especially among young adults remain concerning and in need of further improvement. The consequences of driving after drinking are profound, with high individual and societal costs. Among young adults, alcohol plays a disproportionate role in alcohol-related fatalities. In 2014, 53% of traffic deaths among 18- to 24-year-olds involved alcohol compared with 33% in all other age groups (Hingson et al., 2017).
In 2014, an estimated 12% of the college students ages 18–20 and 22% of students ages 21–24 in the USA had driven under the influence of alcohol compared with 9% and 18%, respectively, of their non-college, same-age peers (Hingson et al., 2017). A recent 7-year longitudinal study of incoming college students suggests that driving after drinking may be even more prevalent (Caldeira et al., 2017). After excluding students without access to a car, Caldeira and colleagues found that the prevalence of driving after drinking peaked at age 22 (66.9%) without any clear declines through age 24. Furthermore, driving after drinking persisted from year to year (83.9–89.1%) for 7 years, indicating that 8 or 9 out of 10 young adults who drive after drinking in a given year do so again in the subsequent years (Caldeira et al., 2017). Not surprisingly, a prior incident of alcohol-impaired driving is a strong predictor of future alcohol-impaired driving (see also LaBrie et al., 2012; Teeters et al., 2015). Similarly, drivers involved in fatal traffic accidents with a blood alcohol concentration (BAC) of 0.08% or higher were 4.5 times more likely to have prior convictions for driving while impaired (National Center for Statistics and Analysis, 2018).
Despite steady progress since the 1980s in reducing alcohol-related harm among young adults, work remains to prevent alcohol-involved driving among young adults and to sever its link to future drunk driving. Compared to alcohol-related problems that represent an actual consequence of drinking (e.g. a missed day of school), driving after drinking is a high-risk behavior that is connected with the potential for harm (e.g. traffic accidents that may or may not happen). Interestingly, Nguyen et al. (2013) reported that college students who reported recent driving after drinking were less likely to plan to limit their drinking in the future compared with students who did not report any recent driving after drinking. This suggests that it is important to prevent driving after drinking, not only because of the immediate safety risks but also because it can ‘embolden’ students to future risky behavior.
In the context of preventive interventions, it is critical to evaluate the effectiveness of existing alcohol interventions in lowering the risk of alcohol-involved driving among young adults. This knowledge would be the first step toward improving existing intervention strategies and developing alternative approaches to reducing driving after drinking. Unfortunately, although driving after drinking is an important and preventable alcohol-related problem and a frequent target of alcohol interventions, few studies have reported driving after drinking as a specific and separate outcome.
Large-scale evidence on the effectiveness of brief alcohol interventions for driving after drinking
There are two meta-analysis studies of driving after drinking using aggregate data (AD; i.e. study-level summary data, such as means, standard deviations, odds ratios [ORs], which are aggregated at the treatment arm level or at the study level) and one using individual participant data (IPD; i.e. original participant-level response), which analyzed driving after drinking as a separate clinical outcome of brief alcohol interventions (BAIs) for young adults (Steinka-Fry et al., 2015; Teeters et al., 2015; Foxcroft et al., 2016). Steinka-Fry et al. (2015) identified 12 BAI studies for a combined sample of 5664 young adults (mean age = 17, with an age range from 13.5 to 20.5 years). They found a statistically significant, though modest standardized effect size,  = 0.15 (95% confidence interval [CI] = 0.08, 0.21), favoring the BAIs compared to controls. However, they also discussed the evidence of potential publication bias from selective underreporting of null or negative findings from the existing trials. Therefore, the overall effect size from this meta-analysis may be an overestimate. Furthermore, the average age in this combined sample was 17, an age that triggers graduated driver licensing programs (e.g. supervised driving or nighttime driving restriction) for novice and beginning drivers in many states in the USA (Williams et al., 2016). Therefore, the reported intervention effect should be interpreted cautiously with these points in mind.
= 0.15 (95% confidence interval [CI] = 0.08, 0.21), favoring the BAIs compared to controls. However, they also discussed the evidence of potential publication bias from selective underreporting of null or negative findings from the existing trials. Therefore, the overall effect size from this meta-analysis may be an overestimate. Furthermore, the average age in this combined sample was 17, an age that triggers graduated driver licensing programs (e.g. supervised driving or nighttime driving restriction) for novice and beginning drivers in many states in the USA (Williams et al., 2016). Therefore, the reported intervention effect should be interpreted cautiously with these points in mind.
Foxcroft et al. (2016) identified six interventions that utilized Motivational Interviewing (MI) for young adults up to age 25 and analyzed outcomes at less than 4 months follow-up (four comparisons from three studies) and at 4 or more months follow-up (four comparisons from four studies). The standardized mean difference estimates on driving after drinking were −0.22 (P < 0.05), favoring the interventions compared to controls, at follow-up that occurred less than 4 months from intervention and −0.13 (P > 0.05; no evidence of any group difference) at 4 or more months follow-up. Due to the small sample of studies (i.e. six) and the small number of comparisons (i.e. four each) in this meta-analysis, combined with the limited evidence previously noted in general, it is difficult to determine whether MI interventions are effective for lowering the risk of driving after drinking.
Teeters et al. (2015) examined IPD from three separate trials (Murphy et al., 2010; Borsari et al., 2012; Martens et al., 2013), where driving after drinking was not previously reported but was measured as a clinical outcome in all three trials. Four brief motivational intervention (BMI) groups in three samples of college student drinkers were separately analyzed. The study found that BMIs focusing on clarifying misconceptions around drinking norms using an MI style (Miller and Rollnick, 2013) were effective in reducing driving after drinking at 6 or 9 months post-intervention. However, a single-component BMI focusing on the use of protective behavioral strategies, which was facilitated by an MI therapist, was not effective in reducing driving after drinking, suggesting effect heterogeneity within BMIs. Despite providing a wealth of information on the association between BMIs and driving after drinking using the most granular data (i.e. IPD), this study was limited by small sample size at the study level (i.e. three); the use of a single-item outcome question from the Brief Young Adult Alcohol Consequences Questionnaire (Kahler et al., 2005), which can be subjectively interpreted (‘I have driven a car when I knew I had too much to drink to drive safely’); and a separate analysis of three data sets without quantitatively combining data.
In sum, the available evidence cautiously suggests an intervention effect on driving after drinking for young adults. However, due to the noted limitations, it remains an open question as to the extent BAIs are effective and whether there are variables that moderate the intervention effect.
BAIs and IPD meta-analysis
Given that driving after drinking is an important clinical endpoint of alcohol interventions for college students, the current study examined whether BAIs lower the risk of driving after drinking using IPD in a two-step IPD meta-analysis. In the current study, we used the term BAI to include BMIs (e.g. the Brief Alcohol Screening and Intervention for College Students [BASICS; Dimeff, 1999]), which are based on a harm reduction approach (Marlatt and Witkiewitz, 2002) and typically facilitated by using MI principles to elicit motivation and commitment to change (Miller and Rollnick, 2013). In addition, stand-alone Personalized Feedback (PF) interventions without any in-person facilitation or group-based motivational interviewing interventions are inclusively referred to as BAIs in the current study. BAIs are generally efficacious for reducing alcohol consumption and alcohol-related problems for college students (for reviews, see Carey et al., 2007, 2016; Cronce and Larimer, 2011). A more fine-grained investigation using IPD revealed that the overall effect of BAI on alcohol consumption and alcohol-related problems might be small (Huh et al., 2015, 2019), with evidence that the combination of in-person MI and PF (MI + PF) effectively reduces alcohol-related problems (Huh et al., 2015; Jiao et al., 2020). However, whether BAIs have beneficial effects on reducing driving after drinking has not been studied.
The current study aims to overcome the limitations of existing evidence (e.g. small samples at the study level, limitations in measurement and sample characteristics and potential underreporting of null or negative effects) using IPD from Project INTEGRATE (Mun et al., 2015b) in a two-step IPD meta-analysis, where AD from individual studies are obtained by analyzing the corresponding IPD in the first step and then combined in the second step. Two-step IPD meta-analysis is currently the prevailing approach to IPD meta-analysis (Simmonds et al., 2015).
Meta-analysis has traditionally involved the analysis of summary data (i.e. AD) extracted from available published and unpublished reports. However, the analysis of IPD obtained from the original studies has emerged as the gold standard approach to meta-analysis (Sutton and Higgins, 2008). When the goal is to characterize average treatment effects, AD meta-analysis and IPD meta-analysis often produce comparable results (see Sutton and Higgins, 2008, for review and discussion). However, key advantages of IPD over AD in meta-analysis include the ability to check the data more carefully, ensure that the same analysis is conducted across all studies, evaluate subgroup differences in the magnitude of treatment effect, distinguish between-study vs. within-study effect modifiers (i.e. moderators) for ecologically valid inference and test moderators with greater power, compared to AD meta-analysis (Cooper and Patall, 2009; Riley et al., 2010). More importantly, with IPD, it is possible to conduct a meta-analysis of previously unreported outcomes. In the current study, we checked data and ensured the same analysis for the same interpretation across all studies in a novel meta-analysis of unreported alcohol-impaired driving outcomes in a two-step IPD meta-analysis. Given that driving after drinking is one of the potential consequences of heavy drinking, we hypothesized that BAIs would have a protective treatment effect and that MI + PF would be comparatively better than PF.
METHODS
Participants
The data come from Project INTEGRATE (Mun et al., 2015b), an ongoing large-scale synthesis study aimed at examining the comparative effectiveness of BAIs for reducing alcohol misuse among college students by utilizing IPD. All BAIs were delivered individually in person, in group, via mail or computer/online. All BAIs were considered brief but differed in the content topics covered and levels of personalization (Ray et al., 2014). Of the 24 studies with available IPD (N = 12,630 participants) that we obtained from the original investigators, 15 studies met the following inclusion criteria: (a) at least two-arm randomized trials with a control or comparison group and (b) available outcome (i.e. driving after drinking) measures at baseline and a follow-up within 12 months post-intervention (see Fig. 1 and Table 1). At baseline, IPD from 9485 participants from 15 studies were available. Of those, 2684 participants did not have outcomes at a first follow-up within 12 months post-intervention, resulting in a sample of 6801 participants (38% male, 72% White and 58% first-year student) across the 15 studies.
Fig. 1.
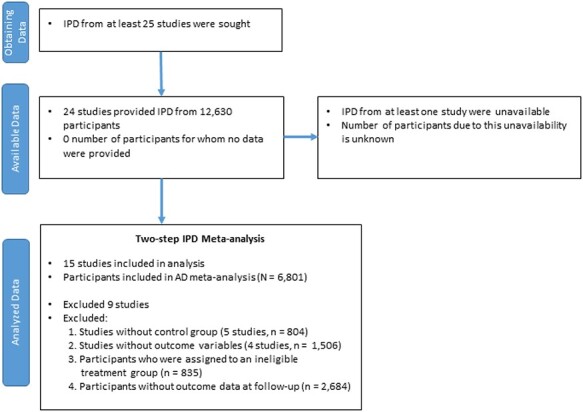
PRISMA IPD flow diagram. IPD come from Project INTEGRATE (Mun et al., 2015b), and data flow at the stages of identification, screening and eligibility is not applicable (unknown).
Table 1.
Description of the IPD at Baseline (N = 9485; 35 randomized groups and 15 studies)
| Study | Reference | BAI | n | Follow-up (months) | % White | % Male | % First year |
|---|---|---|---|---|---|---|---|
| 2 | White et al. (2008) | PF Control |
111 119 |
2 | 68.8 | 71.3 | 62.6 |
| 3 | Barnett et al. (2007) | MI + PF Control |
113 112 |
3 | 65.5 | 48.9 | 66.7 |
| 4 | Cimini et al. (2009) | GMI Control |
228 224 |
6 | 79.8 | 65.0 | 50.0 |
| 7.1 | Fromme et al. (2004) | GMI Control |
100 24 |
1 | 74.6 | 75.8 | 57.3 |
| 7.2 | Fromme et al. (2004) | GMI Control |
317 135 |
1 | 58.6 | 58.6 | 37.4 |
| 8a | Larimer et al. (2007) | PF Control |
736 750 |
12 | 86.6 | 33.5 | 49.6 |
| 8b | Larimer et al. (2007) | PF Control |
1094 1061 |
12 | 61.8 | 41.2 | 46.8 |
| 8c | Larimer et al. (2007) | PF Control |
303 297 |
12 | 83.5 | 37.8 | 36.0 |
| 9 | Lee et al. (2009) | GMI MI + PF PF Control |
97 101 100 101 |
3 | 72.2 | 37.8 | 100.0 |
| 10.1 | Baer et al. (2001) | MI + PF Control |
174 174 |
12 | 84.4 | 46.0 | 100.0 |
| 11 | Walters et al. (2007) | PF Control |
185 198 |
2 | 64.4 | 58.8 | 100.0 |
| 15 | LaBrie et al. (2008a) | GMI Control |
155 108 |
1 | 55.6 | 0.0 | 100.0 |
| 16 | LaBrie et al. (2009) | GMI Control |
161 126 |
1 | 57.0 | 0.0 | 99.7 |
| 19 | LaBrie et al. (2008b) | PF Control |
537 641 |
1 | 67.2 | 30.7 | 19.0 |
| 20 | Larimer et al. (2001) | MI + PF Control |
318 369 |
12 | 83.3 | 53.6 | 74.2 |
| 21 | Walters et al. (2009) | MI + PF PF Control |
76 68 72 |
3 | 84.7 | 35.7 | 41.7 |
Note. Study 7 is a single study but has two subsamples. 7.1 = Mandated student sample and 7.2 = Voluntary student sample. Control groups were waitlisted (Study 2), assessment-only controls (Studies 7, 8a, 8b, 8c, 9, 10.1, 11, 15, 16 and 19–21) or comparison groups that received general alcohol education (Studies 3 and 4). Control students in Studies 15, 16 and 20 received a packet or single-page information sheet containing information about alcohol use. PF, stand-alone personalized feedback intervention; MI + PF, in-person motivational interviewing intervention with personalized normative feedback profile; GMI, group motivational interviewing intervention.
Interventions and controls
Of the 15 studies that met the inclusion criteria, 13 studies were two-arm trials, two studies were multi-arm trials and one study had two subsamples, resulting in a total of 35 treatment arm groups: Five individually delivered Motivational Interviewing with Personalized Feedback (MI + PF) interventions, six Group Motivational Interviewing (GMI) interventions, eight stand-alone PF interventions and 16 Control groups (see Table 1).
Control groups were waitlist controls (Study 2), assessment-only controls (Studies 7, 8a–8c, 9, 10, 11, 15, 16 and 19–21) or comparison groups that received general alcohol education (Studies 3 and 4). Control group students in studies 15, 16 and 20 received a packet or single-page information sheet containing information about alcohol use. Therefore, the control/comparison groups were mostly assessment-only controls or were exposed to minimal intervention content. More details on these intervention groups can be found in previous articles (Ray et al., 2014; Mun et al., 2015b; Mun and Ray, 2018).
All but one study (Study 19) provided general information on BAC and intoxication as well as content on driving while intoxicated (DWI). Except for Study 2, which tailored DWI content to participants, all other studies provided general DWI content to participants. Studies 3, 4, 15, 16 and 20 also provided general information on BAC for control students, and Studies 3, 4, 15 and 16 provided general information on DWI to control students.
Measures
Driving after drinking outcomes
Most of the driving after drinking outcome variables included in the current study (see Table 2) come from two items added to the Rutgers Alcohol Problems Index (White and Labouvie, 1989). Studies 11 and 21 used a modified question, Study 7 had open-ended frequency questions about driving after drinking and Study 3 included an item from the Young Adult Driving Questionnaire (Donovan, 1993). These items varied slightly in terms of their wording (e.g. driving after two+, three+, four+, five+ drinks), referent time frame, response options and follow-up assessment timing. We harmonized them into two drinking and driving (DD) outcomes for a dichotomous response (1 = yes; 0 = no): Driving after more than two (two+) or three (three+) drinks (15 studies, 19 comparisons), and driving after more than four (four+) or five (five+) drinks (12 studies; 15 comparisons). Across all studies with the two outcomes, there was a correlation of 0.92.
Table 2.
The measure of driving after drinking by study
| Study | Original question | Original response | Harmonized response |
|---|---|---|---|
| 2, 4, 8a, 8b, 8c, 9, 10.1, 15, 16, 19, 20 | How many times did the following things happen to you while you were during alcohol or because of your alcohol use during the following time period? Drove shortly after having more than two drinks? (DD1) Drove shortly after having more than four drinks? (DD2) |
0 = 0 times 1 = 1–2 times 2 = 3–5 times 3 = 6–10 times 4 = More than 10 times/11 or more times (Study 2) |
0 = 0. Did not drive after more than two (four) drinks 1–4 = 1. Drove after more than two (four) drinks at least once |
| 3 | During the past 3 months, how many times did you drive within an hour or so after drinking 3 or more beers or other alcoholic drinks? (DD1) | Open-ended (0–10 times) | 0 = 0. Did not drive after three+ drinks in the past 3 months 1+ = 1. Drove after three+ drinks at least once in the past 3 months |
| 7.1 and 7.2 | Indicate how many times you participated in the following activities during the past month Drove after drinking 3–4 alcoholic drinks? (DD1) Drove after drinking 5 or more alcoholic drinks? (DD2) |
Open-ended (0–99 times) | 0 = 0. Did not drive after three+ (five+) drinks in the past month 1+ = Drove after three+ (five+) drinks at least once in the past month |
| 11 | Number of times in the past month user reported driving shortly after having 3+ drinks. (DD1) | Open-ended (0–8 times) | 0 = 0. Did not drive after 3+ drinks in the past months 1+ = Drove after 3+ drinks at least once in the past month |
| 21 | How many times did the following things happen to you while you were drinking or because of your alcohol use during the last 3 months? Drove a vehicle shortly after having three or more drinks? (DD1) | 0 = Never 1 = 1–2 times 2 = 3–5 times 3 = 6–10 times 4 = More than 10 times |
0 = 0. Did not drive after 3+ drinks in the past 3 month 1–4 = 1. Drove after 3+ drinks at least once in the past 3 month |
Notes. The referent time period for DD outcome was 1 month for Studies 7, 11, 15, 16, 19 and 20; 2 months for Study 2; 3 months for Studies 3, 8a, 8b, 8c, 9, 21; and 6 months for Studies 4 and 10.1. BL, baseline; FU, follow-up; DD1, driving after two+/three+ drinks; DD2 = driving after four+/five+ drinks.
Analysis plan
The current study used a two-step IPD meta-analysis. We utilized a random-effects meta-analysis model to obtain pooled effect sizes for both outcomes, which were analyzed separately. A random-effect meta-analysis model is based on more reasonable assumptions compared to a fixed-effect meta-analysis model, such as allowing heterogeneity in effect sizes across individual studies. For study  , in addition to within-study variability
, in addition to within-study variability  , a random-effects model assumes between-study effect size variation surrounding the underlying true common effect size
, a random-effects model assumes between-study effect size variation surrounding the underlying true common effect size  , which can be expressed as the variance
, which can be expressed as the variance  . Therefore, the observed effect size
. Therefore, the observed effect size  is assumed to be normally distributed with the corresponding study-specific true effects
is assumed to be normally distributed with the corresponding study-specific true effects  and sampling variance
and sampling variance  for study
for study  . The true effects
. The true effects  are, in turn, normally distributed with the average, underlying true effect
are, in turn, normally distributed with the average, underlying true effect  and variance
and variance  . These relationships can be expressed more formally as follows:
. These relationships can be expressed more formally as follows:

and

We used the OR as an effect size, one of the standard effect size measures for binary outcome variables, and displayed the overall effect size on the log OR (LOR) scale. The OR is the ratio of the odds for the intervention group to the odds for the control group having the outcome of interest. In the present study, an OR less than 1 indicates a favorable outcome for the intervention (i.e. less likely to drive after drinking for BAI vs. control), whereas an OR greater than 1 indicates a favorable outcome for the control group. All data preparations were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC) and meta-analyses were conducted using the package ‘metafor’ version 2.4 (Viechtbauer, 2010) for R version 4.0.1 (R Core Development Team, 2020). All statistical tests used a two-sided significance level of 0.05. We also conducted subgroup meta-analysis as well as meta-regression to identify potential moderators. All data and computing code in R can be accessed in the online repository (Mun et al., 2021).
RESULTS
Descriptive analysis
Figure 2 shows the percentage of driving after drinking for intervention and control groups for each study at baseline and follow-up. Figure 2 graphically illustrates the between-study heterogeneity in the outcomes. The percentage of driving after two+/three+ drinks and driving after four+/five+ drinks ranged from 1.9 to 45.8% and from 0 to 30.9%, respectively, at follow-up. In addition, there appear to be different degrees of effectiveness in reducing driving after drinking across BAI groups and studies.
Fig. 2.
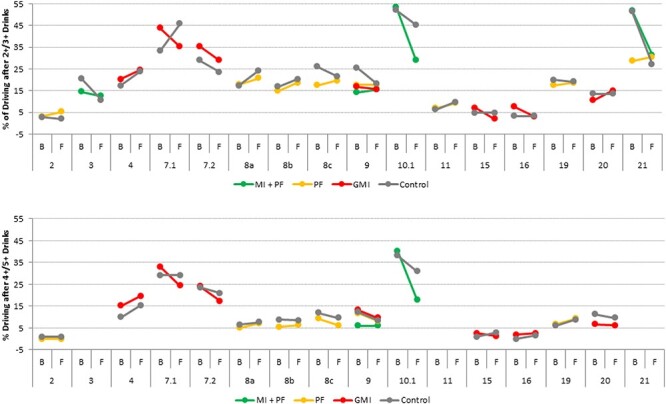
Percentage of driving after two+/three+ drinks (top) and driving after four+/five+ drinks (bottom) at baseline (B) and follow-up (F) per group by study.
Figure 3 displays contour-enhanced funnel plots for both outcomes. Funnel plots are used to detect any sign of publication bias. Figure 3 shows that effect sizes are symmetrically distributed without clear signs of ‘missing’ studies in specific regions of statistical significance or precision.
Fig. 3.
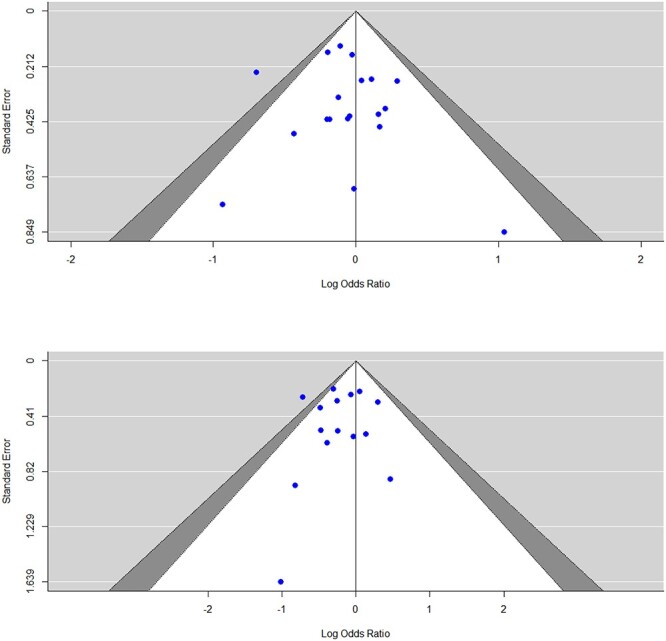
Contour-enhanced funnel plots of LORs: Driving after two+/three+ drinks (top) and after four+/five+ drinks (bottom). Filled circles indicate study-specific effect size estimates. When they are outside the triangle, they are statistically significant at P ≤ 0.05. The outer triangle layer in gray shows the area where 0.05 < P ≤ 0.10, and the inner triangle in white indicates the region where 0.10 < P ≤ 1.00.
Overall effectiveness of BAI on driving after drinking
The top panel of Fig. 4 shows that the effectiveness of BAIs in lowering the risk of driving after two+/three+ drinks was not statistically significant, LOR = −0.10 across k = 19 comparisons, z = −1.54 (OR = 0.91; 95% CI = 0.80, 1.03), P = 0.12. Most of the individual trial effect sizes (12 out of 19) were in the direction of favoring the BAIs. On average, the odds of driving after drinking was reduced by 9% for individuals after receiving BAI (vs. control), although the difference was not statistically significant.
Fig. 4.
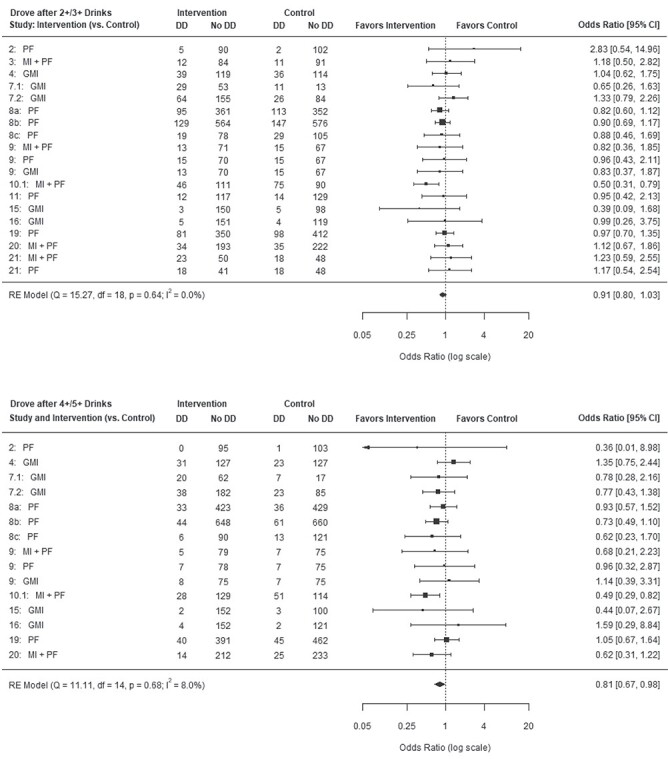
Forest plots of driving after two+/three+ drinks (top) and driving after four+/five+ drinks (bottom). DD, reported driving after drinking; no DD, did not report any driving after drinking.
The bottom panel of Fig. 4 shows the outcome of driving after four+/five+ drinks, where BAIs had a statistically significant intervention effect compared to controls, LOR = −0.21 across k = 15 comparisons, z = −2.15 (OR = 0.81; 95% CI = 0.67, 0.98), P = 0.03. Most of the individual effect sizes (11 out of 15) were in the direction of favoring the BAIs, on average, reducing the odds of driving after drinking by 19%, compared to their counterpart controls.
Study-level moderators of the BAI effect
Subsequent subgroup analysis indicated that MI + PF was statistically significant in lowering the risk of driving after four+/five+ drinks, LOR = −0.61 (OR = 0.54), k = 3, z = −3.03, P < 0.01. The college students allocated to the MI + PF group reduced their risk by 46%, compared with their counterpart controls. Neither GMI nor PF statistically significantly lowered the risk of driving after four+/five+ drinks, LOR = −0.02 (OR = 0.98), k = 6, z = −0.09, P = 0.92 and LOR = −0.15 (OR = 0.86), k = 6, z = −1.21, P = 0.23, respectively. For the outcome of driving after two+/three+ drinks, none of the BAI subgroups showed a statistically significant effect, MI + PF: LOR = −0.13 (OR = 0.87), k = 5, z = −0.65, P = 0.51; GMI: LOR = −0.01 (OR = 0.99), k = 6, z = −0.04, P = 0.97; and PF: LOR = −0.09 (OR = 0.91), k = 8, z = −1.13, P = 0.26.
We further probed whether the referent time window or whether the follow-up duration helped to explain the null finding for driving after two+/three+ drinks. Having a longer referent time frame may mean that students have more opportunities to drive after drinking and, consequently, more opportunities for the BAIs to have a positive impact. Meta-regression analysis results showed a trend toward a larger effect with a longer referent time frame (i.e. in the past 3 months vs. the past month) for driving after two+/three+ drinks, LOR = −0.08 (OR = 0.92), k = 19, z = −1.85, P = 0.06 (see Fig. 5). With each month, the odds of driving after drinking for BAIs, compared to controls, decreased an average of 8% points. Similarly, with the follow-up period, there was a nonsignificant effect, LOR = −0.02 (OR = 0.98), k = 19, z = −1.55, P = 0.12.
Fig. 5.
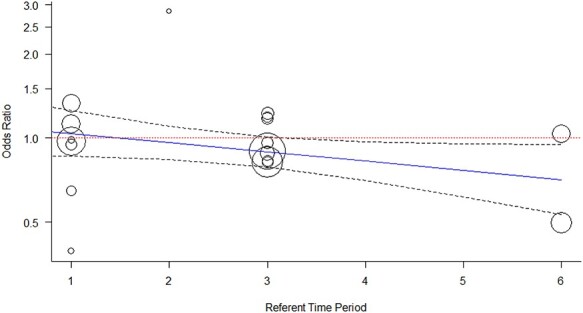
A trend toward better intervention effects (shown in a solid line) on driving after two+/three+ drinks for studies with a longer the referent time period. A dotted line shows a reference line where OR = 1 (i.e. null effect). The size of the circles corresponds to the weighted study sample size. Dashed curved lines indicate the 95% CI.
DISCUSSION
BAIs are effective for reducing the risk of driving after four+/five+ drinks
We found that BAIs statistically significantly lowered the risk of driving after drinking four+/five+ drinks for college students, but not the risk of driving after two+/three+ drinks. In addition, subsequent subgroup analysis indicated that MI + PF mostly carried that significant effect. Given that BAIs are motivated by a harm reduction approach, it is encouraging that BAIs reduce the likelihood of driving after drinking heavily.
The 9% reduction in odds for driving after two+/three+ drinks, though not statistically significant, and 19% reduction for four+/five+ drinks, which would approximately correspond to −0.06 and −0.12, respectively, in the standardized mean difference, should be interpreted in the context that many studies included in this meta-analysis provided BAC and DWI information to both intervention and control students. If control students did not get information on BAC or DWI, the observed effect might have been greater. In addition, most interventions did not specifically tailor their BAC or DWI information to individual students. Although the effect of personalization on clinical endpoints may be complex (Ray et al., 2014), the findings from the current study suggest a need to revisit how intervention can be improved for driving after drinking.
Note that the reported effect in the current study appears modest compared with the standardized mean difference effect size of 0.15 in Steinka-Fry et al. (2015). Given that Steinka-Fry et al. reported evidence of potential publication bias, the current finding, mostly from unreported outcomes, may be closer to the true population-level estimate. We translated the estimated ORs to standardized mean difference effect sizes to provide a comparative context because existing meta-analysis studies have reported effect sizes in the unit of a standard normal variable. However, ORs have a meaningful interpretation for a binary outcome (von Eye and Mun, 2003) and are intuitively easier to understand for policy makers and the public (Mun et al., 2010).
How to improve the effect of BAIs?
One of the difficulties in delivering interventions to college students for driving after drinking is that first-year students often live on-campus without access to a car and opportunities to drive. This situational factor may make interventions for driving after drinking less relevant for younger students. More than half of the sample in the current study was first-year students (58%), and we nonetheless found a significant effect for driving after four+/five+ drinks. A targeted intervention for driving after drinking, if delivered to students ages 21 or older, may yield greater benefits than what was reported in the current study because the prevalence of driving after drinking may plateau later (e.g. age 22; Caldeira et al., 2017).
A recent study from the Monitoring the Future also suggests that the mean age of peak binge drinking has steadily increased from ages 19.7 and 20.7 among women and men, respectively, to ages 21.6 and 23.0 in a more recent cohort of high school graduates (in 1996–2004), compared with older cohorts (Patrick et al., 2019). Given that binge drinking accounts for 85% of all alcohol-impaired driving episodes by those who report binge drinking (Jewett et al., 2015), there is a need to develop alcohol interventions for this slightly older college student population to reduce high-risk behaviors such as driving and drinking. Instead of maturing out, young adults in their early- to mid-20s sometimes experience a developmental transition period marked by more frequent risky behaviors, including DD. Social norm information about peer acceptance of driving after drinking as well as information about alcohol-related impairment in executive functions may be helpful.
We found that MI + PF had the strongest intervention effect on driving after drinking four+/five+ drinks. This result is consistent with earlier reports that identified MI + PF as effective for reducing alcohol-related problems through 12 months post-intervention (Huh et al., 2015; Jiao et al., 2020). In contrast, the beneficial effects of BAIs on alcohol consumption may be comparatively short-lived. Reductions in alcohol consumption (such as frequency or quantity) are important goals by themselves but may not be necessary conditions for reducing alcohol-related harm. For example, Teeters et al. (2015) found that reductions in alcohol consumption did not predict driving after drinking at follow-up. Further investigations can provide an insight into these causal mechanisms.
Methodologically, we note a few observations. First, it may be desirable to establish targeted clinical endpoints and outcome measures for future BAIs. In the absence of consensus outcomes, many different measures are assessed in individual trials, and many important outcomes may not be fully reported in practice. For example, of the possible outcomes from the studies included in Project INTEGRATE, only half of the outcomes assessed were actually reported (Li et al., 2019). From a meta-analysis perspective, it is imperative that trials report all outcomes regardless of whether they have null or negative findings. The fact that all studies but one (Study 7) included in this meta-analysis have not been previously reported in other published meta-analysis reports emphasizes the need to report all outcomes in the original trials for better discoverability. Second, when designing an intervention targeting driving after drinking, it may be advantageous to use a longer referent time frame (e.g. in the past 3 months rather than in the past month) and a longer follow-up period (e.g. 6–12 months rather than 3 months) to appropriately capture the effect of this low-base rate behavior.
Limitations and implications
The current study addressed some of the limitations of the existing studies—potential publication bias, limitations in the sample and measure, small N at the study level and lack of quantitative synthesis. Nonetheless, the current study is not without limitations. First, this study included an IPD sample that was not systematically searched and obtained. Although the combined sample is a reasonably good representation of the existing BAIs between 1990 and 2010 (Mun et al., 2015b), how representative this IPD sample is, relative to a sample that was systematically searched and obtained, remains a question. Relatedly, the current study reports data from trials of comparable recency with respect to existing meta-analysis studies. However, there have been promising BAIs that utilize smartphone technology, supplemental components or stakeholder buy-in for greater effects in the past decade. Clarifying the comparative effectiveness of these divergent intervention approaches, compared with the earlier generation of BMIs, remains an important research question.
Second, we had several comparisons that were nested within studies. Although it may not be ideal to analyze more than one effect size from the same study as if effect sizes were independent, this practice is fairly common. Also, given that most of the trials were two-arm trials, its effect on the inference may be limited. Third, we analyzed two outcomes separately, which may be seen as a limitation. The two outcomes within studies were highly correlated (r = 0.92). Although within-study correlations typically improve estimation in a multivariate meta-analysis (Jackson et al., 2011), this created an estimation challenge due to non-convergence in our study. We deemed it more important to provide results at two different tiers of drinking for substantive interpretation. Finally, we note that between-study heterogeneity in effect sizes was not substantial, at least based on the relevant statistics (see Fig. 4). Nonetheless, study-level variations existed, which can be examined in future IPD meta-analysis studies.
The current study, to our best knowledge, is the largest-scale meta-analysis on driving after drinking among young adults (15 studies, 34 comparisons, N = 6801). In addition, this is the first IPD meta-analysis on this critical outcome. Using IPD, we checked and ensured data accuracy, ensured that AD from different studies would have the same interpretation and appropriately synthesized them across studies in a meta-analysis. Since the 1980s, meta-analysis applications have proliferated (Cheung, 2015; Ioannidis, 2016). With the proliferation, the concern about low-quality or redundant meta-analysis reviews has also surfaced (Ioannidis, 2016). The field of BAIs has not been an exception as we have previously discussed (Mun et al., 2015a). The use of IPD, which offers the most fine-grained information, may improve the body of evidence in the field, which is increasingly feasible with greater data sharing and advances in computing methods.
ACKNOWLEDGEMENTS
We thank Nickeisha Clarke, Yang Jiao, Su-Young Kim and Anne E. Ray, for their earlier work on coding and harmonizing interventions and outcomes, and Helene R. White for her valuable conceptual and methodological contributions in the early years of Project INTEGRATE.
Project INTEGRATE Team: The Project INTEGRATE team consists of the following contributors in alphabetical order: John S. Baer, Department of Psychology, The University of Washington, and Veterans’ Affairs Puget Sound Health Care System; Nancy P. Barnett, Center for Alcohol and Addiction Studies, Brown University; M. Dolores Cimini, University Counseling Center, The University at Albany, State University of New York; William R. Corbin, Department of Psychology, Arizona State University; Kim Fromme, Department of Psychology, The University of Texas, Austin; Joseph W. LaBrie, Department of Psychology, Loyola Marymount University; Mary E. Larimer, Department of Psychiatry and Behavioral Sciences, The University of Washington; Matthew P. Martens, Department of Educational, School, and Counseling Psychology, The University of Missouri; James G. Murphy, Department of Psychology, The University of Memphis; Scott T. Walters, Department of Health Behavior and Health Systems, The University of North Texas Health Science Center; Helene R. White, Center of Alcohol and Substance Use Studies, Rutgers, The State University of New Jersey and the late Mark D. Wood, Department of Psychology, The University of Rhode Island.
Contributor Information
Eun-Young Mun, Department of Health Behavior and Health Systems, University of North Texas Health Science Center, Fort Worth, TX 76107, USA.
Xiaoyin Li, Department of Health Behavior and Health Systems, University of North Texas Health Science Center, Fort Worth, TX 76107, USA.
Shelby Lineberry, Department of Biostatistics and Epidemiology, University of North Texas Health Science Center, Fort Worth, TX 76107, USA.
Zhengqi Tan, Department of Biostatistics and Epidemiology, University of North Texas Health Science Center, Fort Worth, TX 76107, USA.
David Huh, School of Social Work, University of Washington, Seattle, WA 98105, USA.
Scott T Walters, Department of Health Behavior and Health Systems, University of North Texas Health Science Center, Fort Worth, TX 76107, USA.
Zhengyang Zhou, Department of Biostatistics and Epidemiology, University of North Texas Health Science Center, Fort Worth, TX 76107, USA.
Mary E Larimer, Department of Psychiatry and Behavioral Sciences, University of Washington, Seattle, WA 98105, USA.
Funding
The project described was supported by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) (Award Number R01 AA019511). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIAAA or the National Institutes of Health.
Conflict of interest
None declared.
References
*Studies included in the meta-analysis are marked in the References with an asterisk.
- *Baer JS, Kivlahan DR, Blume AW. et al. (2001) Brief intervention for heavy-drinking college students: 4-year follow-up and natural history. Am J Public Health 91:1310–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Barnett NP, Murphy JG, Colby SM. et al. (2007) Efficacy of counselor vs. computer-delivered intervention with mandated college students. Addict Behav 32:2529–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, Hustad JTP, Mastroleo NR et al. (2012) Addressing alcohol use and problems in mandated college students: a randomized clinical trial using stepped care. J Consult Clin Psychol 80:1062–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caldeira KM, Arria AM, Allen HK et al. (2017) Continuity of drunk and drugged driving behaviors four years post-college. Drug Alcohol Depend 180:332–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey KB, Scott-Sheldon LA, Carey MP et al. (2007) Individual-level interventions to reduce college student drinking: a meta-analytic review. Addict Behav 32:2469–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey KB, Scott-Sheldon LAJ, Garey L et al. (2016) Alcohol interventions for mandated college students: a meta-analytic review. J Consult Clin Psychol 84:619–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheung MW-L. (2015) Meta-Analysis: A Structural Equation Modeling Approach. New York: Wiley. [Google Scholar]
- *Cimini MD, Martens MP, Larimer ME et al. (2009) Assessing the effectiveness of peer-facilitated interventions addressing high-risk drinking among judicially mandated college students. J Stud Alcohol Drugs Suppl 16:57–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper H, Patall EA. (2009) The relative benefits of meta-analysis conducted with individual participant data versus aggregated data. Psychol Methods 14:165–76. [DOI] [PubMed] [Google Scholar]
- Cronce JM, Larimer ME. (2011) Individual-focused approaches to the prevention of college student drinking. Alcohol Res Health 34:210–21. [PMC free article] [PubMed] [Google Scholar]
- Dimeff LA. (1999) Brief Alcohol Screening and Intervention for College Students (BASICS): A Harm Reduction Approach. New York: Guilford Press. [Google Scholar]
- Donovan JE. (1993) Young adult drinking-driving: behavioral and psychosocial correlates. J Stud Alcohol 54:600–13. [DOI] [PubMed] [Google Scholar]
- Foxcroft DR, Coombes L, Wood S et al. (2016) Motivational interviewing for the prevention of alcohol misuse in young adults. Cochrane Database Syst Rev . [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Fromme K, Corbin W. (2004) Prevention of heavy drinking and associated negative consequences among mandated and voluntary college students. J Consult Clin Psychol 72:1038–49. [DOI] [PubMed] [Google Scholar]
- Hingson R, Zha W, Smyth D. (2017) Magnitude and trends in heavy episodic drinking, alcohol-impaired driving, and alcohol-related mortality and overdose hospitalizations among emerging adults of college ages 18-24 in the United States, 1998-2014. J Stud Alcohol Drugs 78:540–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huh D, Mun E-Y, Larimer ME et al. (2015) Brief motivational interventions for college student drinking may not be as powerful as we think: an individual participant-level data meta-analysis. Alcohol Clin Exp Res 39:919–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huh D, Mun E-Y, Walters ST et al. (2019) A tutorial on individual participant data meta-analysis using Bayesian multilevel modeling to estimate alcohol intervention effects across heterogeneous studies. Addict Behav 94:162–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ioannidis JPA. (2016) Evidence-based medicine has been hijacked: a report to David Sackett. J Clin Epidemiol 73:82–6. [DOI] [PubMed] [Google Scholar]
- Jackson D, Riley R, White IR. (2011) Multivariate meta-analysis: potential and promise. Stat Med 30:2481–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jewett A, Shults RA, Banerjee T et al. (2015) Alcohol-impaired driving among adults—United States, 2012. Morb Mortal Wkly Rep 64:814–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jiao Y, Mun E-Y, Trikalinos TA et al. (2020) A CD-based mapping method for combining multiple related parameters from heterogeneous intervention trials. Stat Interface 13:533–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kahler CW, Strong DR, Read JP. (2005) Toward efficient and comprehensive measurement of the alcohol problems continuum in college students: the Brief Young Adult Alcohol Consequences questionnaire. Alcohol Clin Exp Res 29:1180–9. [DOI] [PubMed] [Google Scholar]
- *LaBrie JW, Huchting K, Tawalbeh S. et al. (2008a) A randomized motivational enhancement prevention group reduces drinking and alcohol consequences in first-year college women. Psychol Addict Behav 22:149–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *LaBrie JW, Huchting KK, Lac A. et al. (2009) Preventing risky drinking in first-year college women: further validation of a female-specific motivational-enhancement group intervention. J Stud Alcohol Drugs Suppl 16:77–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *LaBrie JW, Hummer JF, Neighbors C. et al. (2008b) Live interactive group-specific normative feedback reduces misperceptions and drinking in college students: A randomized cluster trial. Psychol Addict Behav 22:141–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LaBrie JW, Napper LE, Ghaidarov TM. (2012). Predicting driving after drinking over time among college students: The emerging role of injunctive normative perceptions. J Stud Alcohol Drugs 73(5): 726–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Larimer ME, Lee CM, Kilmer JR. et al. (2007) Personalized mailed feedback for college drinking prevention: a randomized clinical trial. J Consult Clin Psychol 75:285–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- *Larimer ME, Turner AP, Anderson BK. et al. (2001) Evaluating a brief alcohol intervention with fraternities. J Stud Alcohol Drugs 62:370–80. [DOI] [PubMed] [Google Scholar]
- *Lee CM, Kaysen DL, Neighbor C. et al. (2009) Feasibility, Acceptability, and Efficacy of Brief Interventions for College Drinking: Comparison of Group, Individual, and Web-based Alcohol Prevention Formats . Unpublished manuscript. Seattle, Washington: University of Washington. [Google Scholar]
- Li X, Walters ST, Mun E-Y. (2019) Partial outcome reporting in brief alcohol interventions for college students. Alcohol Clin Exp Res 76A:43. [Google Scholar]
- Marlatt GA, Witkiewitz K. (2002) Harm reduction approaches to alcohol use. Addict Behav 27:867–86. [DOI] [PubMed] [Google Scholar]
- Martens MP, Smith AE, Murphy JG. (2013) The efficacy of single-component brief motivational interventions among at-risk college drinkers. J Consult Clin Psychol 81:691–701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller WR, Rollnick S. (2013) Motivational Interviewing: Helping People Change, 3rd edn. New York: Guilford. [Google Scholar]
- Mun E-Y, Atkins DC, Walters ST. (2015a) Is motivational interviewing effective at reducing alcohol misuse in young adults? A critical review of Foxcroft et al. (2014). Psychol Addict Behav 29:836–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mun E-Y, Bates ME, Vaschillo EG. (2010) Closing the gap between person-oriented theory and methods. Dev Psychopathol 22:261–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mun E-Y, de la Torre J, Atkins DC et al. (2015b) Project INTEGRATE: an integrative study of brief alcohol interventions for college students. Psychol Addict Behav 29:34–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mun E-Y, Li X, Lineberry S et al. (2021) Do brief alcohol interventions reduce driving after drinking among college students? A two-step meta-analysis of individual participant data. Mendeley Data V1. doi: 10.17632/j45wkj23c5.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mun E-Y, Ray AE. (2018) Integrative data analysis from a unifying research synthesis perspective. In Fitzgerald HE, Puttler LI (eds). Alcohol Use Disorders: A Developmental Science Approach to Etiology. New York: Oxford University Press, 341–53. [Google Scholar]
- Murphy JG, Dennhardt AA, Skidmore JR et al. (2010) Computerized versus motivational interviewing alcohol interventions: impact on discrepancy, motivation, and drinking. Psychol Addict Behav 24:628–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Center for Statistics and Analysis . (2018) 2017 Data: Alcohol-impaired Driving (DOT HS 812 630). Washington, DC: National Highway Traffic Safety Administration. [Google Scholar]
- National Center for Statistics and Analysis . (2019) 2018 Data: State Alcohol-impaired-Driving Estimates (DOT HS 812 917). Washington, DC: National Highway Traffic Safety Administration. [Google Scholar]
- Nguyen N, Walters ST, Wyatt TM et al. (2013) Do college drinkers learn from their mistakes? Effects of recent alcohol-related negative consequences on planned protective drinking strategies among college freshmen. Subst Use Misuse 48:1463–8. [DOI] [PubMed] [Google Scholar]
- Patrick ME, Terry-McElrath YM, Lanza ST et al. (2019) Shifting age of peak binge drinking prevalence: historical changes in normative trajectories among young adults aged 18 to 30. Alcohol Clin Exp Res 43:287–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ray AE, Kim S-Y, White HR et al. (2014) When less is more and more is less in brief motivational interventions: characteristics of intervention content and their associations with drinking outcomes. Psychol Addict Behav 15:1026–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- R Core Development Team . (2020) R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing. [Google Scholar]
- Riley RD, Lambert PC, Abo-Zaid G. (2010) Meta-analysis of individual participant data: rationale, conduct, and reporting. BMJ 340:c221. [DOI] [PubMed] [Google Scholar]
- Schulenberg JE, Johnston LD, O’Malley PM et al. (2019) Monitoring the Future National Survey Results on Drug Use, 1975–2018, Vol. 2, College Students and Adults Ages 19–60. Ann Arbor: Institute for Social Research, The University of Michigan. [Google Scholar]
- Simmonds M, Stewart G, Stewart L. (2015) A decade of individual participant data meta-analyses: a review of current practice. Contemp Clin Trials 45:76–83. [DOI] [PubMed] [Google Scholar]
- Steinka-Fry KT, Tanner-Smith EE, Hennessy EA. (2015) Effects of brief alcohol interventions on drinking and driving among youth: a systematic review and meta-analysis. J Addict Prev 3:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sutton AJ, Higgins JPT. (2008) Recent developments in meta-analysis. Stat Med 27:625–50. [DOI] [PubMed] [Google Scholar]
- Teeters JB, Borsari B, Martens MP et al. (2015) Brief motivational interventions are associated with reductions in alcohol-impaired driving among college drinkers. J Stud Alcohol Drugs 76:700–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Viechtbauer W. (2010) Conducting meta-analyses in R with the metafor package. J Stat Softw 36:1–48. [Google Scholar]
- von Eye A, Mun E-Y. (2003) Characteristics of measures for 2× 2 tables. Understanding Statistics 4:243–66. [Google Scholar]
- *Walters ST, Vader AM, Harris TR. (2007) A controlled trial of web-based feedback for heavy drinking college students. Prev Sci 8:83–8. [DOI] [PubMed] [Google Scholar]
- *Walters ST, Vader AM, Harris TR. et al. (2009) Dismantling motivational interviewing and feedback for college drinkers: a randomized clinical trial. J Consult Clin Psychol 77:64–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White HR, Labouvie EW. (1989) Towards the assessment of adolescent problem drinking. J Stud Alcohol 50:30–7. [DOI] [PubMed] [Google Scholar]
- *White HR, Mun E-Y, Morgan TJ. (2008) Do brief personalized feedback interventions work for mandated students or is it just getting caught that works? Psychol Addict Behav 22:107–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams AF, McCartt AT, Sims LB. (2016) History and current status of state graduated driver licensing (GDL) laws in the United States. J Saf Res 56:9–15. [DOI] [PubMed] [Google Scholar]