

Abstract
Objective:
To test the null hypothesis that orthodontic therapy with or without premolar extraction does not result in any difference in third molar impaction.
Materials and Methods:
Two groups were formed: 22 patients in one group with first premolar extractions and 22 patients in the other group without extractions. All patients were nongrowing subjects who had normal gonial angles and were skeletal Class I at the beginning of treatment. The available space for third molars, inclination of second and third molars, and angle between the second and third molars were evaluated. Also, the correlation of measured parameters and type of orthodontic therapy with the eruption of third molars was evaluated.
Results:
Of the third molars, 81.8% were impacted in the nonextraction group and 63.6% were impacted in the extraction group. Impaction of mandibular third molars was significantly correlated to the pretreatment and posttreatment inclination of third molars and the angle between the second and third molars. In the extraction therapy group, the retromolar distance increased significantly with a mean of 1.30 ± 1.25 mm.
Conclusions:
When the inclination of the third molar is inconvenient, the tooth may remain impacted even if there is enough retromolar space.
Keywords: Third molar, Impaction, Extraction therapy
INTRODUCTION
Questions such as “Will the extraction therapy affect the eruption of my wisdom teeth?” are often asked of clinicians by orthodontic patients. This is generally an uncertain situation among orthodontists, and in most cases, we have limited data on why third molars do not erupt and also on whether the extraction of premolars benefits the eruption of third molars.
Third molars exhibit great variation in size, shape, position, root formation, time of development, and path of eruption.1 The prevalence of impaction of at least one impacted lower third molar has been reported as 72.7% in a cohort aged 20–30 years.2 Today, third molar impaction is the most common of all tooth impactions.3 In primitive mankind, excessive interproximal attrition allowed mesial drift of the posterior teeth and made the incidence of third molar impaction relatively low.4,5
The mandibular third molar is the most frequently impacted tooth after the maxillary third molar.4 The lack of space between the second molar and the ramus has long been cited as a major etiologic factor of mandibular third molar impaction.6–8 Björk et al.9 stated that the alveolar arch space behind the second molar is deficient in 90% of mandibular third molar impaction cases. In their study, they examined 243 cases to investigate the correlation between mandibular third molar impaction and some cephalometric parameters. They reported that factors that affect the space of third molars were mandibular length, backward direction of eruption of the dentition, and vertical direction of condylar growth, which were associated with the degree of resorption on the anterior aspect of the mandibular ramus.
Richardson10 stated that a skeletal Class II relationship with a shorter, narrower, more acute angled mandible was found in association with impacted third molars. The author also noted that there was a reduced amount of mandibular growth in impacted third molar cases. In contrast, Hattab and Alhaija1 did not find any relationship between gonial angle and third molar impaction, while Capelli11 reported that in patients with impacted third molars, the total length of the mandible was less than in patients without impacted molars. Besides the morphology of the mandible, the mesiodistal width of the third molars may affect the impaction of third molars. Some studies reported that patients with larger third molars had a higher impaction rate.1,12 Mandibular premolar extraction may result in the mesial movement of molars.13 Some studies, using lateral cephalometric and panoramic radiographs, found that nonextraction therapy was associated with the impaction of third molars5,7,14,15 and extraction therapy improves the mandibular third molar angulations.16 Other long-term studies have reported no or little difference between extraction or nonextraction treatment.17,18
Third molar impaction has been associated with several factors. While researching the effect of extraction therapy on the impaction of third molars, it is important to distinguish the role of factors such as growth, morphology, and anchorage needs. In previous studies, these factors were not eliminated, and it is hard to know the absolute effect of extraction therapy on third molars. The aim of this study was to test the null hypothesis that orthodontic therapy with or without premolar extraction does not cause any difference on third molar impaction.
MATERIALS AND METHODS
This retrospective study sample included pretreatment (T1) and posttreatment (T2) panoramic and lateral cephalometric radiographs of 44 white patients from the archives of Gazi University Faculty of Dentistry Department of Orthodontics who were previously treated with a straight wire technique. Two groups were formed: 22 patients in one group who had been treated with first premolar extractions with moderate anchorage need and 22 patients in the other group treated without extractions. The extraction group consisted of 10 males and 12 females and the nonextraction group of 13 males and 9 females. All patients were nongrowing subjects (Ru growth phase in hand-wrist radiographs) who had a normal gonial angle (ArGoMe = 130° ± 7°) and skeletal Class I (ANB = 2° ± 2°) at the beginning of the treatment. The mean age in the extraction group was 18.43 ± 1.52 years and in the nonextraction group was 19.59 ± 1.49 years. Independent t-tests revealed no significant age difference between groups at T1 (P = .66). In all patients, a 0.018″ Roth prescription bracket system was used, and space closure was maintained with retraction arches and Ni-Ti closed coil springs. All patients had mandibular third molar buds with forming roots at T1, and apex closure of third molars was fully completed at T2. Both the left and right mandibular third molars of all 44 patients were evaluated, making a total of 88 teeth. Any patient with history of dentofacial trauma or orthodontic treatment, who had deformities, missing teeth, a developmental anomaly, or any pathology in the mandible, was excluded from the study. Patient records of poor-quality radiographs were also excluded.
Evaluated parameters are shown in Figure 1. All radiographs were traced by the same researcher after tracing 10 pilot radiographs for orientation. On panoramic radiographs, an occlusal line was drawn through the tips of the mandibular teeth, and the intersection of this line with the ramus was marked as the J point. Available space for the third molar (D7-J) was calculated as the distance between the J point and the point (D7) where a perpendicular line intersects the occlusal line from the most distal of mandibular second molar. A line tangent to the lower border of the corpus of the mandible and lines representing the long axis of second and third molars were drawn. Inclination of the third molar (β angle), second molar (γ angle), and the angle between the second and third molar (α angle) were calculated.8 To evaluate the homogeneity of the pretreatment inclination of third molars between extraction and nonextraction groups, an independent t-test was used.
Figure 1.
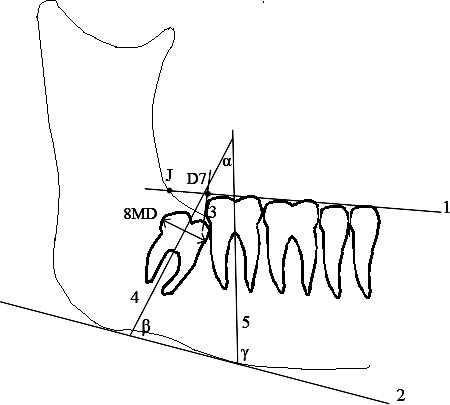
Linear and angular measurements used in the study.
The reliability and reproducibility of the measurements were calculated by statistically analyzing the Pearson correlation coefficient between measurements taken 2 weeks apart on 10 subjects. Five of the second measured subjects were randomly selected from the extraction cases, and 5 were selected from the nonextraction cases. Reliability coefficients for the analyzed parameters are given in Table 1.
Table 1.
Reliability Coefficients

The effect of extraction and nonextraction treatment on the impaction of mandibular third molars was also investigated. Impacted molars were scored as 0, and erupted molars were scored as 1 at T1 and T2. These scores were used for correlating the measured parameters with impaction. Third molar eruption was defined as the presence of buccal or lingual cusps at the level of the occlusal plane.7 Also, correlation of the measured parameters with the eruption of third molars was evaluated.
Statistical evaluation of the raw research data was made with SPSS 20.0 (SPSS, IBM, New York, NY) software. The Kolmogorov-Smirnov test was used to evaluate the homogenity of variances. As all of the variables were distributed equally; parametric tests were applied to the data set. A paired-sample t-test was used for intragroup and an independent samples t-test was used for intergroup evaluations. To evaluate the relation of extraction and nonextraction therapy on the impaction of third molars, a chi-square test was used. To evaluate the correlation of eruption with the measured parameters, the Pearsons correlation analysis was used. The level of significance was set at P < .05.
RESULTS
Results of the chi-square test showed that extraction and nonextraction treatment significantly correlated with the eruption of the mandibular third molars (P < .05; Table 2). A total of 81.8% of the third molars were impacted in the nonextraction group, while this ratio was significantly lower in the extraction group, with 63.6%. The eruption rate was doubled with a significance level of P = .046. Therefore, the null hypothesis of this study was rejected.
Table 2.
Results of the Chi-Square Test to Evaluate the Effect of Treatment Type on Eruption of Mandibular Third Molars

Table 3 shows the significance of Pearson's correlation between the measured parameters and eruption. Eruption of mandibular third molars is significantly correlated with the pretreatment and posttreatment inclination of third molars (β angle) and the angle between the second and third molars (α angle). Eruption was not correlated with the inclination of the second molar (γ angle) or D7-J distance.
Table 3.
Pearson's Correlation of the Parameters to the Eruption of Mandibular Third Molars

Table 3 shows that the T1 and T2 α angle and eruption are negatively correlated in a medium (P = .002) and strong (P = .000) manner, respectively. In other words, if the α angle is low, the mandibular third molar tends to errupt, and—vice versa—it remains impacted if its inclination to the second molar is high.
Table 3 also shows that the T1 and T2 inclination of mandibular third molars, namely, β angle, is positively and strongly correlated to eruption (P = .000). If the pretreatment or posttreatment inclination of the mandibular third molar to the mandible corpus is high, this means their inclination is in favor of the path mandibular molars tend to erupt.
In the extraction therapy group, the D7-J distance increased significantly (P < .001) with a mean of 1.30 ± 1.25 mm, while none of the measured parameters have changed at a significance level in the nonextraction group (Table 4). The increase in D7-J was significantly greater in the extraction group (P < .001; Table 5).
Table 4.
Changes From T1 to T2 in Both Groups

Table 5.
Intergroup Evaluation of the Changes From T1 to T2

The mean pretreatment β angles of the extraction and nonextraction groups were 73.18° ± 13.39° and 79.00° ± 15.87°, respectively, with an insignificant P value of .067. Distribution of impacted teeth according to the initial inclination of third molars is given in Table 6. If the mesial tipping exceeds 60°, no eruption was recorded in either group.
Table 6.
Number of Impacted Mandibular Third Molar Distributed According to Initial Inclination (β Angle) in Groups

DISCUSSION
The reason for third molar impaction is not absolutely clear. Several factors such as morphology,10 mesiodistal width of teeth,1,12 alveolar arch space behind the second molars,6–9 unfavorable path of eruption, and unsatisfactory uprighting during eruption19 have been associated with third molar impaction. It is also unclear if orthodontic therapy benefits third molar eruption or not. While researching the effect of orthodontic therapy on the impaction of third molars, it may be important to distinguish factors such as growth, morphology, and anchorage needs. In this study, we tried to eliminate these factors by choosing the sample from nongrowing patients who had a normal sagittal and vertical skeletal relationship and moderate anchorage needs.
Eliminating cases with limited ability for root development eliminates the potential of eruption and is also a reliable key. Impacted third molars that still have root development potential may lead to overdiagnosis of impaction. It has been reported that the bud formation of third molars ranges from 17 to 21 years of age, but the roots are not fully formed until 18 to 25 years old.20,21 In this study, the mean age of patients at the beginning of the treatment was 18.43 ± 1.52 years in the extraction group and 19.59 ± 1.49 years in the nonextraction group. To prevent overdiagnosis of impaction, cases were selected in which the third molars had not completed their root formation at the beginning of treatment and had nearly or fully completed their root development at the end of treatment.
Richardson13 stated that the retromolar space was increased in mandibular first premolar extraction cases when compared with the nonextraction cases. Behbehani et al.7 also reported that increased retromolar space and mesial molar movement during orthodontic treatment reduced the risk of third molar impaction. The data of the current study revealed that premolar extraction therapy increased the retromolar space (D7-J) and that the impaction rate of third molars was significantly reduced in this group, which is in accordance with previous studies.7,13
In clinical practice, not only premolar extraction but also first and second molar extraction can be performed to gain arch space. Ay et al.22 reported that unilateral mandibular first molar extraction might lead to an increase in retromolar space. Bayram et al.23 also reported that first molar extraction decreases the third molar impaction rate by increasing the retromolar space.
A chi-square test (Table 2) revealed that orthodontic treatment with premolar extraction benefited mandibular third molar eruption. During orthodontic treatment, 18.2% of the third molars erupted in the nonextraction group, but in the extraction group, this ratio was doubled to 36.4%, which is statistically significant at a level of P = .046. The mean increase of 1.3 mm D7-J distance in the premolar extraction group may be the leading factor in this result. Although there is no correlation between eruption and D7-J distance, there is a strong correlation between eruption and α and β angles (Table 3). We suggest that the third molars with appropriate α and β angles that cannot erupt due to inadequate D7-J distance may erupt because of the increase in this dimension caused by the mesial movement of second molars with orthodontic treatment. Similarly, even though there is enough D7-J distance, if the third molar is poorly angulated, it might be impacted. Kim et al.5 stated that the increase in retromolar space due to premolar extraction may be one of the leading factors for third molar eruption. However, the inclination of the posterior teeth was not investigated in their study. Our study revealed that the leading factor for impaction may not be the retromolar space itself but that the inclination of the third molar is also important.
One concept for the development of mandibular retromolar space is resorption at the anterior border of the ramus.6,9 Within the concept of bone remodeling, the trabeculae adapt to stress and strain formed by external forces.24 The third molar teeth with appropriate α and β angles may maintain the necessary external force to remodel the retromolar region by expanding the bone in all three dimensions and forming resorption of the ramal region, thus increasing the D7-J dimension. This may be another factor contributing to the increase in retromolar arch space.
The α and β angles did not show any significant changes during the treatment period (T1–T2) in both groups of this study, which is in contradiction with some previous studies.16,25 However, Tarazona et al.26 and Staggers et al.27 found results similar to our findings. The cephalometric reference points, the development phase, the type of space closure mechanism, and anchorage needs may be among the factors that can lead to different findings. Also, one major point in finding different results might be the type of radiograph used in a study. Superimposed contralateral images of third molars on lateral cephalograms may be the cause of angulation differences in the previous studies, but panoramic radiographs with the same magnification may eliminate this difficulty. Although Tronje et al.28 suggested that rotational panoramic radiography causes inbuilt distortion effect, they also stated that panoramic radiographic images can be reliable for geometric measurements in clinical practice. Akcam et al.29 suggested that angular measurements on lateral cephalograms are less reliable, but Stramotas et al.30 noted that linear vertical measurements, ratio calculations, and angular measurements can be made on a panoramic radiograph with consistent accuracy. They also stated that most of the elongation error is due to the magnification factor and that if the panoramic radiographs are exposed on the same machine at different times, the lengths of the teeth and implants remain constant. All panoramic radiographs used in this study were taken on the same cephalostat and with the same magnification.
Hattab31 evaluated the changes in angular position of impacted third molars over a 4-year observation period and reported that if the inclination between the second and third molars exceeds 30°, the chance of eruption might be limited. Our data revealed that if the β angle is lower than 60°, all teeth in both groups remained impacted, parallel to Hattab's findings, and this confirms the idea that if the initial angle of third molars is not favorable, there is a tendency for impaction.
CONCLUSIONS
Although there is enough retromolar space, if the inclination of the third molar is inconvenient, the tooth may remain impacted.
The retromolar space was significantly higher in the premolar extracted orthodontic treatment group.
The third molar impaction rate was significantly higher in the nonextracted group when compared with the extraction group.
The inclination of the third molar was strongly correlated with the impaction.
If the angle between the third molar and lower mandibular border is less than 60°, there is a tendency for impaction.
REFERENCES
- 1.Hattab FN, Alhaija ES. Radiographic evaluation of mandibular third molar eruption space. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:285–291. doi: 10.1016/s1079-2104(99)70029-6. [DOI] [PubMed] [Google Scholar]
- 2.Hugoson A, Kugelberg CF. The prevalence of third molars in a Swedish population: an epidemiological study. Community Dent Health. 1988;5:121–138. [PubMed] [Google Scholar]
- 3.Bishara SE. Third molars: a dilemma! Or is it. Am J Orthod Dentofacial Orthop. 1999;115:628–633. doi: 10.1016/s0889-5406(99)70287-8. [DOI] [PubMed] [Google Scholar]
- 4.Alling CC, Helfrick JF, Alling RD. Impacted Teeth. Philadelphia, Pa: W.B. Saunders; 1993. [Google Scholar]
- 5.Kim TW, Artun J, Behbehani F, Artese F. Prevalence of third molar impaction in orthodontic patients treated nonextraction and with extraction of 4 premolars. Am J Orthod Dentofacial Orthop. 2003;123:138–145. doi: 10.1067/mod.2003.13. [DOI] [PubMed] [Google Scholar]
- 6.Bjork A. Variations in the growth pattern of the human mandible: longitudinal radiographic study by the implant method. J Dent Res. 1963;42(1 Pt 2):400–411. doi: 10.1177/00220345630420014701. [DOI] [PubMed] [Google Scholar]
- 7.Behbehani F, Artun J, Thalib L. Prediction of mandibular third-molar impaction in adolescent orthodontic patients. Am J Orthod Dentofacial Orthop. 2006;130:47–55. doi: 10.1016/j.ajodo.2006.03.002. [DOI] [PubMed] [Google Scholar]
- 8.Abu Alhaija ES, AlBhairan HM, AlKhateeb SN. Mandibular third molar space in different antero-posterior skeletal patterns. Eur J Orthod. 2011;33:570–576. doi: 10.1093/ejo/cjq125. [DOI] [PubMed] [Google Scholar]
- 9.Björk A, Jensen E, Palling M. Mandibular growth and third molar impaction. Acta Odontologica Scandinavica. 1956;14:231–272. [Google Scholar]
- 10.Richardson ME. The etiology and prediction of mandibular third molar impaction. Angle Orthod. 1977;47:165–172. doi: 10.1043/0003-3219(1977)047<0165:TEAPOM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Capelli J., Jr Mandibular growth and third molar impaction in extraction cases. Angle Orthod. 1991;61:223–229. doi: 10.1043/0003-3219(1991)061<0223:MGATMI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Venta I, Murtomaa H, Ylipaavalniemi P. A device to predict lower third molar eruption. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:598–603. doi: 10.1016/s1079-2104(97)90358-9. [DOI] [PubMed] [Google Scholar]
- 13.Richardson ME. The effect of mandibular first premolar extraction on third molar space. Angle Orthod. 1989;59:291–294. doi: 10.1043/0003-3219(1989)059<0291:TEOMFP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 14.Dierkes DD. An investigation of the mandibular third molars in orthodontic cases. Angle Orthod. 1975;45:207–212. doi: 10.1043/0003-3219(1975)045<0207:AIOTMT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Kaplan RG. Some factors related to mandibular third molar impaction. Angle Orthod. 1975;45:153–158. doi: 10.1043/0003-3219(1975)045<0153:SFRTMT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 16.Saysel MY, Meral GD, Kocadereli I, Tasar F. The effects of first premolar extractions on third molar angulations. Angle Orthod. 2005;75:719–722. doi: 10.1043/0003-3219(2005)75[719:TEOFPE]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 17.Haavikko K, Altonen M, Mattila K. Predicting angulational development and eruption of the lower third molar. Angle Orthod. 1978;48:39–48. doi: 10.1043/0003-3219(1978)048<0039:PADAEO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 18.Artun J, Thalib L, Little RM. Third molar angulation during and after treatment of adolescent orthodontic patients. Eur J Orthod. 2005;27:590–596. doi: 10.1093/ejo/cji049. [DOI] [PubMed] [Google Scholar]
- 19.Peterson LJ, Ellis E, Hupp JR, Tucker MR. Contemporary Oral and Maxillofacial Surgery. St Louis, Mo: Mosby; 1998. [Google Scholar]
- 20.Proffit WR, Fields HW. Contemporary Orthodontics. St Louis, Mo: Mosby Year Book; 1993. [Google Scholar]
- 21.Ash MMJ. Wheeler's Dental Anatomy Physiology and Occlusion. Philadelphia Pa: W.B. Saunders; 1993. [Google Scholar]
- 22.Ay S, Agar U, Bicakci AA, Kosger HH. Changes in mandibular third molar angle and position after unilateral mandibular first molar extraction. Am J Orthod Dentofacial Orthop. 2006;129:36–41. doi: 10.1016/j.ajodo.2004.10.010. [DOI] [PubMed] [Google Scholar]
- 23.Bayram M, Ozer M, Arici S. Effects of first molar extraction on third molar angulation and eruption space. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:e14–20. doi: 10.1016/j.tripleo.2008.10.011. [DOI] [PubMed] [Google Scholar]
- 24.Wolff J. The Law of Bone Remodelling. Berlin, Germany: Springer-Verlag; 1986. [Google Scholar]
- 25.Elsey MJ, Rock WP. Influence of orthodontic treatment on development of third molars. Br J Oral Maxillofac Surg. 2000;38:350–353. doi: 10.1054/bjom.2000.0307. [DOI] [PubMed] [Google Scholar]
- 26.Tarazona B, Paredes V, Llamas JM, Cibrian R, Gandia JL. Influence of first and second premolar extraction or non-extraction treatments on mandibular third molar angulation and position: a comparative study. Med Oral Patol Oral Cir Bucal. 2010;15:e760–e766. doi: 10.4317/medoral.15.e760. [DOI] [PubMed] [Google Scholar]
- 27.Staggers JA, Germane N, Fortson WM. A comparison of the effects of first premolar extractions on third molar angulation. Angle Orthod. 1992;62:135–138. doi: 10.1043/0003-3219(1992)062<0135:ACOTEO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 28.Tronje G, Welander U, McDavid WD, Morris CR. Image distortion in rotational panoramic radiography. I. General considerations. Acta Radiol Diagn (Stockh) 1981;22:295–299. doi: 10.1177/028418518102203a14. [DOI] [PubMed] [Google Scholar]
- 29.Akcam MO, Altiok T, Ozdiler E. Panoramic radiographs: a tool for investigating skeletal pattern. Am J Orthod Dentofacial Orthop. 2003;123:175–181. doi: 10.1067/mod.2003.3. [DOI] [PubMed] [Google Scholar]
- 30.Stramotas S, Geenty JP, Darendeliler MA, Byloff F, Berger J, Petocz P. The reliability of crown-root ratio, linear and angular measurements on panoramic radiographs. Clin Orthod Res. 2000;3:182–191. doi: 10.1034/j.1600-0544.2000.030404.x. [DOI] [PubMed] [Google Scholar]
- 31.Hattab FN. Positional changes and eruption of impacted mandibular third molars in young adults: a radiographic 4-year follow-up study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84:604–608. doi: 10.1016/s1079-2104(97)90359-0. [DOI] [PubMed] [Google Scholar]