

Abstract
Objective:
To determine if repeated sterilization has deleterious effects on the clinical stability of mini-screws.
Materials and Methods:
Thirty each of the following mini-screws were tested: Aarhus (American Orthodontics, Sheboygan, Wisc), VectorTAS (Ormco Corporation, Orange, Calif), Dual-Top (RMO, Denver, Colo), and Ortho Anchor (KLS Martin, Jacksonville, Fla). Controls were sterilized once using a steam autoclave (Statim 5000, SciCan USA, Canonsburg, Pa). Each group of mini-screws was divided into three groups: the control (n = 10) and two test groups (n = 10, each). Test groups were cycled five and 10 times respectively. All screws were inserted into custom-designed synthetic blocks that simulated mandibular bone. Maximum insertion torque and lateral displacement force data were recorded and subjected to statistical testing. Two-way analysis of variance (ANOVA) and three-way mixed ANOVA were used for statistical analyses for maximum insertion torque data and lateral displacement force data, respectively. Level of significance was established at P < .05.
Results:
Insertion torque values displayed significant differences between both of the groups and sterilization cycles (P < .05). Significant differences were observed between American Aarhus mini-screws and both RMO and KLS Martin mini-screws. Ormco Vector mini-screws also differed significantly from the KLS Martin mini-screws in this comparison (P < .05). For lateral displacement, there was a significant main effect of groups, F(1,36) = 14.5 (P < .05). Significant differences were observed between American Aarhus mini-screws and all three of the other groups (P < .05).
Conclusions:
The examined groups displayed statistical differences of variable quality that may not affect their clinical stability.
Keywords: Mini-screws, Sterilization, Stability
INTRODUCTION
The introduction of temporary anchorage devices (TADs), including plates and screws, has helped to solve one of the fundamental challenges encountered by clinicians and has provided a system approaching absolute anchorage during orthodontic movement of teeth.1 In just the short period since their introduction, mini-screws have been used in various applications and orthodontic mechanic setups, such that the possibilities for treatment of simple and complex cases with their aid are virtually limitless.2–4 Eighty percent of orthodontists in a recent survey5 reported that they had at least one active case involving TADs in their practice. With each new year this percentage is rising, and as more and more orthodontists are beginning to regularly incorporate the use of this innovative technology into their practice, it is important to fully understand their biomechanical properties, protocols for placement, and procedures for proper infection control and sterilization. As is often the case with technological advancements within orthodontics and other medical fields, it is important to be cautious and to remember that sometimes “The ‘state of the art’ is [also] ‘clinician beware.’”6 As a profession, it is important that we continue to demand scientific rigor and quality research in the further development of skeletal anchorage devices.
Although some TAD products are being made available as single-dose sterile packages, many still remain as part of clinical kits with multiple screw lengths and diameters or as single units that require prior sterilization by the clinician. Exposure to nonsterile conditions and or improper technique at placement may occur. Thus, the mini-screws may need to undergo further sterilization cycles. It is, however, possible that the microstructure of the mini-screws may be altered after one or more additional cycles, and this in turn could affect their integration and stability during use. Whether or not mini-screws should be regularly exposed to sterilization cycles and packaged in single kits or in clinical kits with multiple screws is currently a characteristic of these products that appears to be based largely on manufacturer preference and past precedence. With more and more options from myriad manufacturers and marketers of mini-screws, it is important that orthodontists have a clear understanding of what is behind the various packaging materials, sterilization, and placement protocol recommendations. Such an understanding will better allow for prudent clinical practice based on sound, unbiased research rather than simple adherence to untested norms and preferences.
Ample data exist in the literature regarding the effects of sterilization on other orthodontic products, such as nickel-titanium archwires and various pliers, yet there are a lack of data in regard to sterilization effects on titanium alloy mini-screws and subsequent changes in their mechanical properties and clinical function.7–11 Previous studies12–15 have established the use of insertion torque and lateral displacement from applied forces as reliable parameters for stability measurement with regard to mini-screws. This study will focus on the use of those parameters in order to compare the effects of sterilization based on mini-screw stability. In doing so, we hope to provide the clinician with valuable information on the number of times a mini-screw or similar temporary anchorage device may be sterilized safely and successfully, while also ensuring maximum cost benefit and efficiency to the orthodontic practice. We aimed to test the null hypothesis that there is no difference in the stability of mini-screws following a number of sterilization applications.
MATERIALS AND METHODS
The following four popular groups of mini-screws were chosen for this study based on similarities in titanium alloy composition, size, shape (cylindrical), and diameter:
Vector TAS (Ormco Corporation, Orange, Calif); 1.4 mm in diameter and 8 mm long;
Aarhus (American Orthodontics, Sheboygan, Wisc); 1.5 mm in diameter and 8 mm long;
Dual-Top (RMO, Denver, Colo); 1.4 mm in diameter and 8 mm long; and
Ortho Anchor (KLS Martin, Jacksonville, Fla); 1.5 mm in diameter and 8 mm long.
Thirty mini-screws per group were divided into groups of 10 each. Within each group, a control group was exposed to one cycle of sterilization and compared with two experimental groups that were exposed to five and 10 cycles of sterilization, respectively. The mini-screws were placed into metal cartridges designed specifically for the sterilization of mini-screws of their size and diameter. All groups were sterilized according to the American Dental Association recommendations for critical instruments using steam sterilization in sealed bags with the Statim 5000 autoclave system (SciCan USA, Canonsburg, Pa). Cycles were performed at 132° for 6 minutes. Chemical and biological indicator tests were included to insure proper sterilization using systems in place at the University of Texas at Houston School of Dentistry.
Poststerilization, all mini-screws were inserted into synthetic bone samples to obtain maximum insertion torque readings. A random sequence generator was used to determine the order of insertion of the mini-screw groups to avoid bias. The synthetic bone was custom made for the study to simulate the density and physical properties of alveolar cancellous and cortical bone and was manufactured specifically for this study by Sawbones Worldwide (Vashon, Wash). Each biomechanical test block had a simulated cortical bone thickness of 1.5 mm (0.48 g/cc), with the remaining 18.5 mm (0.16 g/cc) of height simulated for cancellous bone. Compressive, tensile, and shear strength for the cortical bone layer were 18, 12, and 7.6 MPa, respectively, and for the cancellous bone layer these values were 2.2, 2.1, and 1.6 MPa, respectively. Corresponding driver attachments from the individual manufacturers were inserted into the chuck of an Imada HTG-2 Torque Wrench (Northbrook, Ill). All mini-screws were inserted by a single operator at a 90° angle to the synthetic bone for uniformity. Data were recorded for maximum insertion torque for the individual mini-screws using the peak mode setting of the torque wrench. The operator was blinded to these data during insertion of the mini-screws, and a separate researcher recorded readings at the time of insertion.
All samples were then sectioned and mounted in acrylic bases to be used in the next portion of the experiment. Instron Model 4655 (Norwood, Mass) technology was then used to apply uniform compression force perpendicular to the mini-screws to investigate stability based on lateral displacement within the synthetic bone (Figure 1). Preset levels of displacement were set at 0.025, 0.05, 0.1, 0.5, and 1.0 mm, and data were produced using Instron software for the amount of force in milligrams recorded at each level of displacement.
Figure 1.
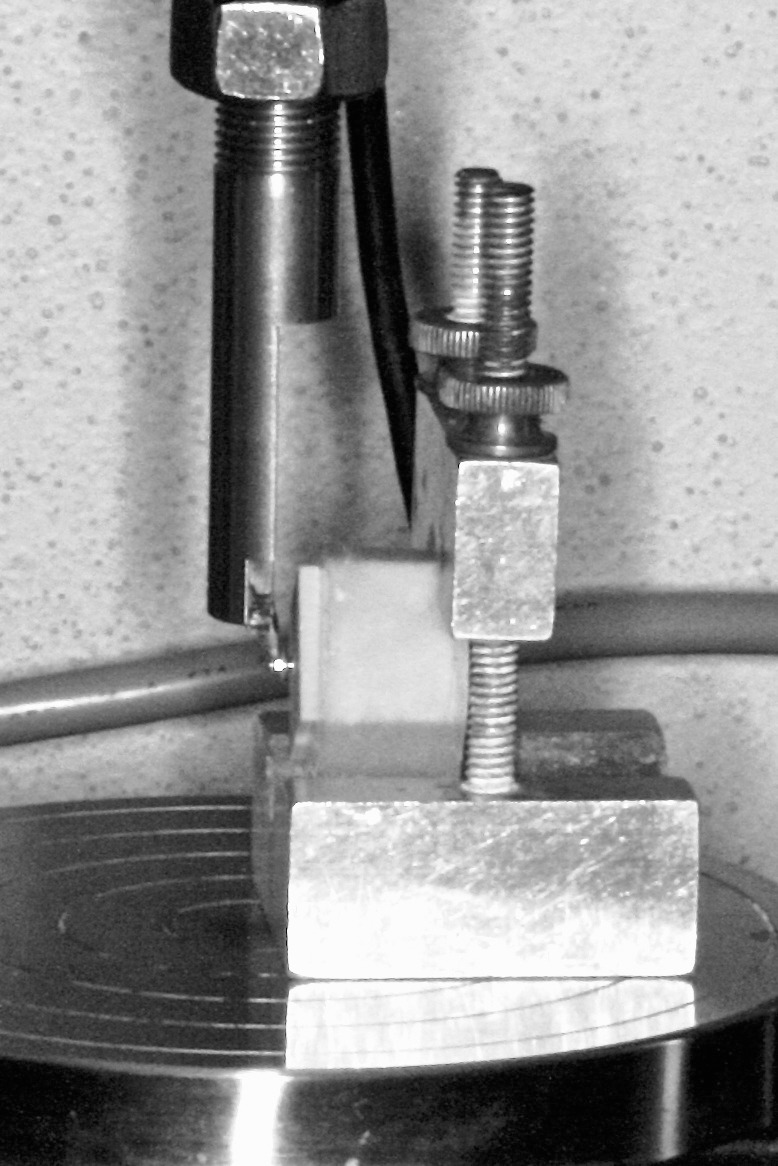
Application of uniform compression force perpendicular to the mini-screws by Instron Model 4465 (Norwood, Mass).
Statistical Analysis
A preliminary study indicated that the sample size should include a total of 118 mini-screws in order to have 80% power with an alpha (P-value) equal to .05, an effect size of 0.35, and a numerator of df equal to 6 in order to find significant differences between the groups. Upon the laboratory testing, data were converted using Log10 transformation using SPSS Version 20 (SPSS Inc, Chicago, Ill). Two-way analysis of variance (ANOVA) and three-way mixed ANOVA were used for statistical analyses for maximum insertion torque data and lateral displacement force data, respectively. Level of significance was established at P < .05. Post hoc Bonferroni comparisons were performed for multiple comparisons.
RESULTS
The descriptive statistics for maximum insertion torque are presented in Table 1. Two-way ANOVA analysis (Table 2) indicated significant differences between the four groups and the three sterilization cycles (P < .05). Statistical variation between the groups may be attributed to the fabrication differences between the brands. However, group and cycle interaction also was significant (P < .05). This actually means that the effect of repeated sterilization cycles on maximum insertion torque was different between the investigated groups. Post hoc comparisons for the four groups are shown in Table 3. Significant differences were observed between American Aarhus mini-screws and both RMO and KLS Martin mini-screws. Ormco Vector mini-screws also differed significantly from the KLS Martin mini-screws in this comparison (P < .05). Post hoc comparisons for the different cycles are shown in Table 4. Significant differences were noted between one and 10 sterilization cycles as well as between five and 10 sterilization cycles (P < .05).
Table 1.
Descriptive Statistics of the Maximum Insertion Torque at One, Five, and 10 Sterilization Cycles for All Four Tested Brandsa

Table 2.
Analysis of Variance of the Maximum Insertion Torque Data

Table 3.
Bonferroni Post Hoc Multiple Comparisons Test of the Maximum Insertion Torque Between the Groups

Table 4.
Bonferroni Post Hoc Multiple Comparisons Test of the Maximum Insertion Torque Between the Cycles

The descriptive statistics for lateral displacement data are presented in Table 5. Three-way mixed ANOVA (Table 6) indicated a significant main effect of groups, F(1,36) = 14.5 (P < .05). This variability may potentially be due to the brand-specific differences between the groups since sterilization cycle as a main effect was not significant. Furthermore, none of the interactions that included ‘cycle’ as an effect revealed any significant differences. Taken altogether, these findings indicate that the number of sterilizations did not significantly alter lateral displacement force values of mini-screws. Post hoc comparisons for the four groups are presented in Table 7. Significant differences were observed between American Aarhus mini-screws and all three other groups (P < .05).
Table 5.
Descriptive Statistics of the Lateral Displacement Force at Preset Displacement Distances for All Groupsa

Table 6.
Analysis of Variance of the Lateral Displacement Force Data

Table 7.
Bonferroni Post Hoc Multiple Comparisons Test of the Lateral Displacement Force Between Groups

DISCUSSION
Repeated cycles of sterilization altered the surface characteristics of the mini-screws, as evidenced by the significant changes in their maximum insertion torque. However, sterilization cycle as a main effect did not significantly affect lateral displacement force values. Furthermore, a thorough evaluation of the findings observed in this laboratory study did not indicate major structural damage to the mini-screws that may actually affect their clinical stability and consistency as they are sterilized up to 10 cycles.
Maximum Insertion Torque
It has been suggested16–19 that maximum insertion torque can be used as a reliable parameter to determine whether primary mini-screw stability can be achieved. In 2006 Motoyoshi et al.20 tried to determine an ideal range for placement torque that would yield improved mini-screw success rates. This study demonstrated that implants placed with maximum insertion torques ranging from 5 Ncm to 10 Ncm were significantly higher than those placed above or below that range.20 A follow-up study21 performed in 2007 by the same group found that mini-screws placed with torques between 8 Ncm and 10 Ncm achieved 100% success rates clinically. Although statistical differences were observed for maximum insertion torque both between groups and between cycles in our study, our results showed that maximum insertion torque values did not deteriorate after repeated sterilization cycles. In fact, in the Vector and KLS Martin groups mean maximum insertion torque values actually increased from 4.11 Ncm to 6.42 Ncm and from 5.79 Ncm to 6.67 Ncm, respectively (Table 1). Recently, McManus13 found that in vitro, the anchorage resistance offered by mini-screws placed with higher maximum insertion torque was, on average, greater than the anchorage resistance offered by mini-screws placed at lower maximum insertion torque. This finding simply indicates that repeated cycles of sterilization do not affect the maximum insertion torque values of mini-screws negatively and may, rather, have a positive outcome.
Lateral Displacement Force
Studies have shown that the forces used to move teeth can range from approximately 0.3 to 0.4 Newtons depending on the tooth movement desired. As a result, the force applied to an individual mini-screw will vary based on differing treatment choices.22 Systematic review of mini-screw loading times has shown that forces ranging from 150 to 500 g applied immediately postinsertion have been used successfully in treatment.23 All mean values observed for lateral displacement force in this study ranged from 113 g at .0025 mm to 9848 g at 1.0 mm, representing forces far above the clinical norms for applied forces with orthodontic appliances. This would indicate that although there is the potential for displacement because of the fact that mini-screws are not designed or intended for osseointegration, it would take forces in substantial excess of the clinical standard of care to displace the mini-screws a clinically significant distance, independent of the sterilization cycle number or brand design.1
Furthermore, the results of our study concur with those of previous sterilization studies10,11,24 performed for other orthodontic materials, such as nickel-titanium and beta-titanium wires, which demonstrated no deleterious effects on most biomechanical properties post–autoclave sterilization. The results of our study also reflect the conclusion made by Adelson et al.25 that multiple cycles of sterilization—up to 50 times in their study—had no clinically significant effect on the titanium plates and screws under investigation.
The main weakness of our study is that it was carried out in the laboratory setting and thus cannot be directly translated into a purely clinical context. However, the advantage of the study in a lab setting was that many variables could be controlled and made uniform for the most accurate assessment of results. Although up to 10 cycles of sterilization may not frequently occur in practice, our study was able to demonstrate that the mini-screws can confidently be sterilized multiple times without compromising their overall stability. Further research is needed to evaluate possible microstructural effects of autoclave sterilization on mini-screws. Despite the fact that mechanical properties were not negatively affected from a clinical standpoint, it would be useful to see if changes such as deleterious effects on thread sharpness and angulation or the presence of chemical or corrosive buildup between threads could be observed following repeated sterilization cycles from a microscopic view.
CONCLUSIONS
It is evident from our findings that brand-specific differences exist between mini-screw groups.
However, statistical variability in maximum insertion torque and lateral displacement force of the investigated mini-screws when they were sterilized up to 10 times indicate that sterilization bears no clinical relevance to stability.
REFERENCES
- 1.English JD, Peltomaki T, Pham-Litschel K. Mosby's Orthodontic Review. St Louis, Mo: Mosby Elsevier; 2009. [Google Scholar]
- 2.Chung KR, Choo HR, Kim SH, Ngan P. Timely relocation of mini-implants for uninterrupted full-arch distalization. Am J Orthod Dentofacial Orthop. 2010;138:839–849. doi: 10.1016/j.ajodo.2009.02.035. [DOI] [PubMed] [Google Scholar]
- 3.Hyde JD, King GJ. Survey of orthodontists' attitudes and experiences regarding miniscrew implants. J Clin Orthod. 2010;44:481–486. [PMC free article] [PubMed] [Google Scholar]
- 4.Paquette DE. Miniscrew-supported transitional tooth replacement: an esthetic alternative. J Clin Orthod. 2010;44:321–325. [PubMed] [Google Scholar]
- 5.Buschang P, Carrillo R, Ozenbaug B, Rossouw P. 2008 Survey of AAO Members on Miniscrew Usage. J Clin Orthod. 2008;42:513–518. [PubMed] [Google Scholar]
- 6.Nanda R, Uribe FA. Temporary Anchorage Devices in Orthodontics. St Louis, Mo: Mosby Elsevier; 2009. [Google Scholar]
- 7.Mazzocchi AR, Paganelli C, Morandini C. Effects of three types of sterilization on orthodontic pliers. J Clin Orthod. 1994;28:644–647. [Google Scholar]
- 8.Buckthal JE, Kusy RP. Effects of cold disinfectants on the mechanical properties and the surface topography of nickel-titanium arch wires. Am J Orthod Dentofacial Orthop. 1988;94:117–122. doi: 10.1016/0889-5406(88)90359-9. [DOI] [PubMed] [Google Scholar]
- 9.Kapila S, Haughen JW, Watanabe LG. Load-deflection characteristics of nickel-titanium alloy wires after clinical recycling and dry heat sterilization. Am J Orthod Dentofacial Orthop. 1992;102:120–126. doi: 10.1016/0889-5406(92)70023-4. [DOI] [PubMed] [Google Scholar]
- 10.Mayhew MJ, Kusy RP. Effects of sterilization on the mechanical properties and the surface topography of nickel-titanium arch wires. Am J Orthod Dentofacial Orthop. 1988;93:232–236. doi: 10.1016/s0889-5406(88)80008-8. [DOI] [PubMed] [Google Scholar]
- 11.Staggers JA, Margeson D. The effects of sterilization on the tensile strength of orthodontic wires. Angle Orthod. 1993;63:141–144. doi: 10.1043/0003-3219(1993)063<0141:TEOSOT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Mattos CT, Ruellas AC, Sant'Anna EF. Effect of autoclaving on the fracture torque of mini-implants used for orthodontic anchorage. J Orthod. 2011;38:15–20. doi: 10.1179/14653121141200. [DOI] [PubMed] [Google Scholar]
- 13.McManus M. Effect of MiniScrew Maximum Insertion Torque on Skeletal Orthodontic Anchorage [master's thesis] Iowa City, Iowa: University of Iowa; 2010. [Google Scholar]
- 14.Pithon MM, Nojima MG, Nojima LI. In vitro evaluation of insertion and removal torques of orthodontic mini-implants. Int J Oral Maxillofac Surg. 2011;40:80–85. doi: 10.1016/j.ijom.2010.09.013. [DOI] [PubMed] [Google Scholar]
- 15.Hong C, Lee H, Webster R. Stability comparison between commercially available mini-implants and a novel design. Angle Orthod. 2011;81:692–699. doi: 10.2319/092410-556.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wilmes B, Drescher D. Impact of insertion depth and predrilling diameter on primary stability of orthodontic mini-implants. Angle Orthod. 2009;79:609–614. doi: 10.2319/071708-373.1. [DOI] [PubMed] [Google Scholar]
- 17.Cho K, Baek S. Effects of predrilling depth and implant shape on the mechanical properties of orthodontic mini-implants during the insertion procedure. Angle Orthod. 2012;82:618–624. doi: 10.2319/080911-503.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Heo Y, Cho K, Baek S. Angled-predrilling depth and mini-implant shape effects on the mechanical properties of self-drilling orthodontic mini-implants during the angled insertion procedure. Angle Orthod. 2012;82:881–888. doi: 10.2319/100711-629.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Shah AH, Behrents RG, Kim KB, Kyung HM, Buschang PH. Effects of screw and host factors on insertion torque and pullout strength. Angle Orthod. 2012;82:603–610. doi: 10.2319/070111-427.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Motoyoshi M, Hirabayashi M, Uemura, Shimizu N. Recommended placement torque when tightening an orthodontic mini-implant. Clin Oral Implant Res. 2006;17:109–114. doi: 10.1111/j.1600-0501.2005.01211.x. [DOI] [PubMed] [Google Scholar]
- 21.Motoyoshi M, Yoshida T, Ono A, Shimizu N. Effect of cortical bone thickness and implant placement torque on stability of orthodontic mini-implants. Int J Oral Maxillfac Implants. 2007;22:779–784. [PubMed] [Google Scholar]
- 22.Ren Y, Maltha JC, Kuijpers-Jagtman AM. Optimum force magnitude for orthodontic tooth movement: a systematic literature review. Angle Orthod. 2003;73:86–92. doi: 10.1043/0003-3219(2003)073<0086:OFMFOT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 23.Ohashi E, Pecho OE, Moron M, Lagravere MO. Implant vs. screw loading protocols in orthodontics. Angle Orthod. 2006;76:721–727. doi: 10.1043/0003-3219(2006)076[0721:IVSLPI]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 24.Pernier C, Grosgogeat B, Ponsonnet L, Benay G, Lissac M. Influence of autoclave sterilization on the surface parameters and mechanical properties of six orthodontic wires. Eur J Orthod. 2005;27:72–81. doi: 10.1093/ejo/cjh076. [DOI] [PubMed] [Google Scholar]
- 25.Adelson RT, Defatta RJ, Ducic Y. Integrity of craniofacial plating systems after multiple sterilization procedures. J Oral Maxillofac Surg. 2007;65:940–944. doi: 10.1016/j.joms.2005.12.059. [DOI] [PubMed] [Google Scholar]