

Abstract
Objective:
To investigate the torque capabilities of passive and active self-ligating (SL) brackets on mandibular incisors and canines using three-dimensional (3D) imaging analysis.
Materials and Methods:
Two types of SL bracket systems were analyzed: a passive and an active. Both brackets had a 0.022 × 0.028-inch slot size. Treatment protocol and wire sequences were followed as recommended by the manufacturers. Twenty-six patients were included in the passive group and 20 were included in the active group; all received pretreatment and posttreatment cone-beam computed tomography (CBCT) scanning. Based on the CBCT scans, a customized 3D analysis was developed to assess labiolingual inclination of the roots of mandibular canines and incisors with respect to the occlusal plane before and after treatment.
Results:
Following treatment, a statistically significant labiolingual proclination of the teeth was seen in both groups. Moreover, in both SL systems the roots exhibited a large variation in labiolingual inclination between adjacent teeth even after treatment.
Conclusions:
A significant proclination was seen for the mandibular front teeth; the claimed third-order torque control of SL systems could not be demonstrated. Therefore, a considerable play between the wire and the brackets could be hypothesized, even more in relation to the passive than the active SL brackets.
Keywords: Self-ligating brackets, Orthodontics, CBCT, Three-dimensional analysis
INTRODUCTION
Torque is described by Rauch1 as a moment generated by the torsion (twisting) of a rectangular wire in the bracket slot, thereby determining the labiolingual inclination. Initially, a twist was bent into the wire,2 but Andrews3 proposed that the control of the individual teeth in all planes of space (ie, first, second, and third order) should be included in the design of the bracket, thereby introducing prescription brackets. However, the definition of an optimal prescription has varied considerably between authors. In addition to the prescription, several other factors have an influence on how well the appliance is able to deliver the planned buccolingual inclination. The play between bracket and wire can be calculated knowing the slot and the wire dimension, yet variation in curvature of the crown, bracket positioning, and variation in the thickness of the adhesive will affect the final buccolingual inclination as well.4–7
The influence of bracket material, dimensional precision, and wire-slot interaction have been studied in vitro.8–11 Type of ligation and consistency in ligation have been assigned importance for the torque obtained.12–14 On the other hand, the interoperator variation can be neglected in self-ligating (SL) systems, due to the modus operandi of the closing mechanism of SL brackets (SLBs).
In relation to the nonextraction approach, control of labiolingual inclination of the lower incisors has been considered of paramount importance for a successful orthodontic treatment, as lack of control may result in undesirable flaring.15
Manufacturers of both active and passive SLBs have indicated the advantage of their solution for better torque control: while the passive brackets are claimed to produce a “lip-bumper effect” resulting in a better torque control of the lower incisors, the manufacturers of the active clip claimed that this renders a better torque control. First and foremost, the size of the final wire and bracket will determine the wire-to-slot third-order play responsible for the variation in torque between adjacent teeth.8,16–20 The 0.019 × 0.025-inch stainless steel wire frequently recommended is delivering a theoretical wire-to-slot play of about 10°, but the play has been shown to be larger due to variation in the actual size and edges shape of wires as well as oversized bracket slot.9,21–24
The assessment of incisor inclination is frequently done based on lateral head films. Due to the inherent uncertainty caused by the superimposing of all four incisors on the radiograph, this method is not suitable for torque quality control.25 On the other hand, the cone-beam computed tomography (CBCT) scan does allow for visualization and evaluation of each tooth individually.26
The aim of the present study was to evaluate the in vivo capability of active and passive SL bracket systems in delivering the desired labiolingual inclination of lower incisors and canines in relation to the occlusal plane.
MATERIALS AND METHODS
This study is part of a randomized controlled trial project on passive and active SL systems started at the Orthodontic Department of Aarhus Dental School.26 Consent to undergo the CBCT radiographic examinations and to use the material for the present investigation was obtained from all patients. CBCT scans were taken following the protocol approved by the Radiological Department, School of Dentistry, Aarhus University. Sixty-four patients with full permanent dentition and with Class I, II, and mild Class III were allocated randomly and symmetrically in two age-matched parallel groups (mean age 15.5 and 14.4 years, respectively) treated either with:
passive SLBs (Damon 3MX, Standard torque: incisors 1°, canines 0°; Ormco Corporation, Orange, Calif) (group 1) or
active SLBs (In-Ovation R, Roth prescription: incisors +1°, canines −11°; GAC International Inc, Bohemia, NY) (group 2).
Patients with severe Class III, obvious need for extraction, periodontal problems, and major skeletal discrepancies were excluded.
The wire sequence prescribed by the manufacturers of the two SL systems was followed exactly. All patients received a CBCT scan (NewTom 3G, QR-Verona, Italy) before (T0) and after treatment completion (T1). All CBCT scans were reconstructed with an isotropic voxel dimension of 0.36-mm. Raw data obtained from CBCT scanning were exported via the DICOM format and imported into specific software (Mimics 13.1, Materialise, Belgium).
The labiolingual inclinations of mandibular canine and lateral, and central incisors were measured in relation to the occlusal plane, which was created modifying the Björk “occlusal line inferior.”27 The occlusal plane was thus defined as the plane passing through two “molar points” placed at the tip of the distofacial cusp of the most distal molar in occlusion in each side and an “average incisor point” created as the interpolation of the right and left incisal edges of the lower central incisors. This has been done to minimize the effect of different labiolingual and mesiodistal inclination as well as vertical position between the left and the right incisors.
The following reference points were defined (Figure 1):
Figure 1.
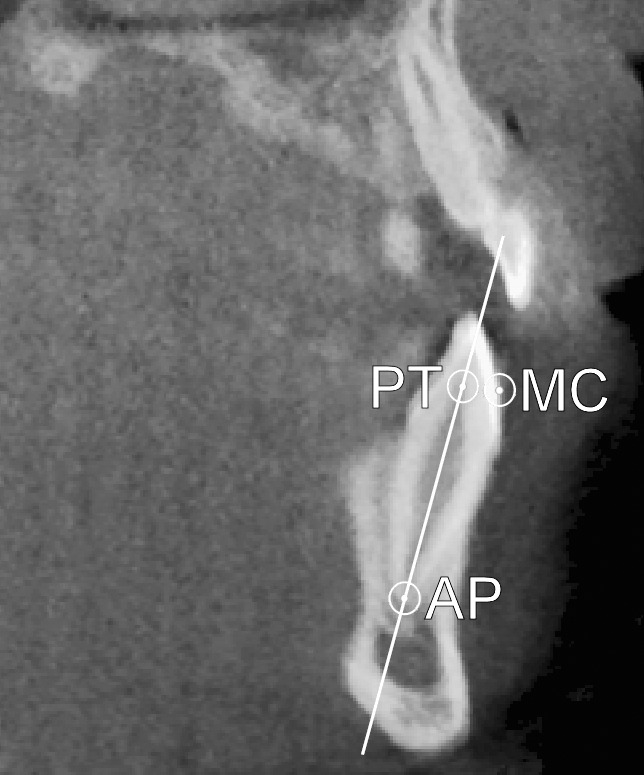
The pulp-crown (PT) and the pulp-apex (AP) points: the most superior and the most caudal point of the pulp canal, respectively. The mid-crown point (MC): located on the facial surface of the crown, equidistant both with respect to the occlusogingival and mesiodistal direction. The long axis of the tooth is defined as the line passing through PT and AP.
PT: pulp-crown point, placed at the most superior pulp canal point;
AP: pulp-apex point, placed at the most caudal point of the pulp canal; and
MC: mid-crown point, placed on the facial surface of the crown, equidistantly located with respect to the “occlusogingival and mesiodistal direction.”
The long axis of each tooth was then defined as the line passing through PT and AP. The tooth sagittal plane was defined as the labiolingual plane passing through PT, AP, and MC points separating the tooth into a mesial and a distal part as described by Andrews.3 The tooth frontal plane of each tooth, likewise according to Andrews,3 was defined as the mesial-distal plane passing through the PT and AP points, perpendicular to the tooth sagittal plane. This plane separates the tooth into a facial and a lingual component (Figure 2). The labiolingual inclination of each tooth was assessed by calculating the angle between the frontal plane of each tooth and the occlusal plane.
Figure 2.

The tooth sagittal plane (purple) is defined by PT, AP, and MC points. The tooth frontal plane (green) passes through PT and AP points, and it is perpendicular to the tooth sagittal plane.
The changes in lower intercanine width during treatment were assessed by measuring the distance between the cusp of the right and left canine at T0 and T1. One investigator blinded with respect to the SLB type identified all the necessary points.
Statistical Analysis
Statistical analysis was performed with SPSS version 13.0 for Windows (SPSS Inc, Chicago, Ill). The normal distribution of the data was checked using Q-Q plot and the Kolmogorov-Smirnov test. Differences between the two groups at baseline with respect to age, labiolingual inclination of the mandibular canine, and central and lateral incisors were compared by independent samples t-test. Within each group, the changes in labiolingual inclination of the four incisors and bilateral canines occurring from T0 to T1 were assessed by paired t-tests. The variation in inclination within each patient was calculated and compared between the two bracket types with independent samples t-test. The significance level was set at .05.
The error of the method was calculated on double measurements of 10 randomly selected patient CBCT scans taken at T0 using the Dahlberg formula (s = √∑d2 / 2n, where d = difference between the first and second measurements).28 The coefficient of reliability was calculated as CoR = 1 − s2 / SD2, where standard deviation (SD) is calculated at T0.
RESULTS
Enrollment started in December 2004 and was completed by May 2010. From the original 32 patients in group 1, three had to be excluded as they prematurely interrupted the treatment, while three patients had premolar extraction. In group 2, 12 patients had to be excluded: three of them had premolar extraction, one had severe slenderizing, two were reoriented toward surgery, four needed segmented appliance because of asymmetry, one dropped out before the end of the treatment, and one did not show up for the final CBCT scan.
The error of the method was found to be small for all the angular measurements: 0.62° (CoR = 0.993) for canine, 0.78° (CoR = 0.988) for lateral incisors, and 0.59° (CoR = 0.992) for central incisors. As no differences in inclination were found between the right and left analogous teeth, the right and left measurements were pooled. All data were normally distributed.
No statistically significant differences were found between the groups regarding age and labiolingual inclination of the lower front dentition at T0. A pronounced variation in labiolingual inclination among both canines and incisors within and between individuals in both groups was seen and reflected in the large standard deviation (Table 1).
Table 1.
Baseline (T0) and Treatment Outcome (T1) for the Two Parallel Groupsa,b

When evaluating the changes occurring during treatment, a decrease in labiolingual inclination in relation to the occlusal plane (flaring) was detected in both systems. At T1, in both groups the canines were proclined the least (3.9° in group 1; 3.2° in group 2) followed in order by lateral incisors and central incisors (Figure 3). The change in intercanine width was 2.0 mm (SD 1.6) and 1.6 mm (SD 2.2) for the passive and active SLB, respectively. In addition, at T1 a general decrease in the spread was seen for all teeth apart from the central incisors in group 1, with group 2 exhibiting less intragroup variation (Table 1).
Figure 3.

Mean and range values of labiolingual inclination of mandibular incisors and canines with respect to the occlusal plane for the passive and active SLB groups at T0 and T1.
From T0 to T1, the changes in the labiolingual inclination were statistically significant for all teeth in both bracket systems, while no statistically significant difference in inclination was detected between the two groups (Table 1). A marked variation between the labiolingual inclinations of the teeth was measured within each individual patient following treatment with both passive and active brackets systems. Moreover, the maximum difference in inclination between the incisors, despite a reduction in average, increased during treatment in eight of 26 patients in group 1, and four of 20 patients in group 2 (Figure 4 a,b).
Figure 4.

Trend graphs depicting the maximum difference in labiolingual inclination between the four incisors for each patient before (T0) and after treatment (T1) for the passive (a) and the active SLB group (b).
DISCUSSION
The aim of this study was to evaluate whether the use of passive or active SLBs would lead to the desired labiolingual inclination of the mandibular anterior teeth and canines at the end of treatment. The inclination was measured as the angle between the long axis of the mandibular front teeth and the occlusal plane, as the brackets' prescription torque is originally defined in relation to this plane. However, the present method is somehow different from the method originally described by Andrews3 who specifically looked at the angulation of the crown to a line bearing 90° from the occlusal plane. Therefore, the present results have to be interpreted with this difference in mind. The rationale behind the use of the tooth long axis instead of the crown long axis is related to resolution and artifact problems especially seen at the crown level, which characterized CBCT images.
The general response of the lower anterior teeth to the treatment in “nonextraction” patients performed with both SL systems was an almost true proclination. This finding is in agreement with that of Pandis et al.29 who stated that alignment with both SL systems and conventional brackets led to a proclination of the anterior teeth; it is also in agreement with the conclusions of Morina et al.13 that only minor differences exist between the various bracket systems with respect to their efficiency in torque correction. Therefore, the present results failed to produce evidence for the lip-bumper effect as suggested by the manufacturer of the passive SLBs.
Both passive and active SLB-based treatments produced proclination indicating that the uprighting effect of both bracket systems is somehow missing. There was no significant difference in torque expression between passive SLBs and active SLBs, though the latter had a tendency towards a better torque control, educed by the smaller intra-arch variation of teeth inclination seen for the active brackets. Badawi et al.14 compared the third-order torque moment delivered by a 0.019 × 0.025-inch stainless steel arch-wire engaged into active and passive SLBs. Though their setup is slightly different (ie, it is an in vitro study where only one bracket was studied at a time), their results corroborate the conclusion of the present study, at least for angles that are clinically relevant.
At the start of treatment, the crowding for which the patients were treated was reflected in a significant intra-arch variation in labiolingual inclination of the anterior teeth. Following treatment, both groups still displayed a noticeable divergence in inclination between the incisors, hence suggesting a pronounced play between wire and bracket slot, thus confirming what previously was described in relation to torque play.30 The difference in labiolingual alignment was small, and none of the brackets resulted in satisfactory leveling of the labiolingual inclination, clinically confirming an earlier statement by Morina et al.13 This result might have been influenced by inaccurate vertical bonding of the brackets and/or by the different tooth crown morphology,5 thus hindering the expression of a specific torque prescription. Finally, labiolingual inclination values could not be compared directly with standard torque prescriptions because in the present study teeth inclination was measured at the root level with respect to the occlusal plane, while the bracket torque prescription is typically reported for the crown. Indeed, a certain variation in the angulation of crown, root, and longitudinal axis of a tooth does exist.17
In both groups, the change in inclination of the canines was about half that of the incisors. This result might be related to the fact that the canines are surrounded by a thicker bony alveolar envelope and have a longer and thicker root when compared to the lower incisors. Moreover, the canines are positioned at the corner of the dental arch, thus the canines are tipped along both the mesial and buccal direction. The difference in Damon Optimal arch form and In-Ovation Sentalloy Accuform medium arch form did not lead to any difference in canine torque corrections.
CONCLUSIONS
The relief of mandibular anterior crowding predominantly occurred as a result of buccal tipping, independent of bracket type.
Major intra-arch variation in inclination after treatment among the anterior teeth was more pronounced in the case of the passive than the active bracket.
REFERENCES
- 1.Rauch ED. Torque and its application to orthodontics. Am J Orthod. 1959;45:817–830. [Google Scholar]
- 2.Tweed CH. Clinical Orthodontics. St Louis, Mo: CV Mosby; 1966. pp. 6–13. [Google Scholar]
- 3.Andrews LF. Straight Wire The Concept and Appliance. San Diego, Calif: LA Wells Co; 1989. [Google Scholar]
- 4.Mestriner MA, Enoki C, Mucha JN. Normal torque of the buccal surface of mandibular teeth and its relationship with bracket positioning: a study in normal occlusion. Braz Dent J. 2006;17:155–160. doi: 10.1590/s0103-64402006000200014. [DOI] [PubMed] [Google Scholar]
- 5.Miethke RR, Melsen B. Effect of variation in tooth morphology and bracket position on first and third order correction with preadjusted appliances. Am J Orthod Dentofacial Orthop. 1999;116:329–335. doi: 10.1016/s0889-5406(99)70246-5. [DOI] [PubMed] [Google Scholar]
- 6.van Loenen M, Degrieck J, De Pauw G, Dermaut L. Anterior tooth morphology and its effect on torque. Eur J Orthod. 2005;27:258–262. doi: 10.1093/ejo/cji007. [DOI] [PubMed] [Google Scholar]
- 7.Sondhi A. Efficient and effective indirect bonding. Am J Orthod Dentofacial Orthop. 1999;115:352–359. doi: 10.1016/s0889-5406(99)70252-0. [DOI] [PubMed] [Google Scholar]
- 8.Sebanc J, Brantley WA, Pincsak JJ, Conover JP. Variability of effective root torque as a function of edge bevel on orthodontic arch wires. Am J Orthod. 1984;86:43–51. doi: 10.1016/0002-9416(84)90275-6. [DOI] [PubMed] [Google Scholar]
- 9.Cash AC, Good SA, Curtis RV, McDonald F. An evaluation of slot size in orthodontic brackets—are standards as expected. Angle Orthod. 2004;74:450–453. doi: 10.1043/0003-3219(2004)074<0450:AEOSSI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 10.Kusy RP, Whitley JQ. Resistance to sliding of orthodontic appliances in the dry and wet states: influence of archwire alloy, interbracket distance, and bracket engagement. J Biomed Mater Res. 2000;52:797–811. doi: 10.1002/1097-4636(20001215)52:4<797::aid-jbm25>3.0.co;2-9. [DOI] [PubMed] [Google Scholar]
- 11.Feldner JC, Sarkar NK, Sheridan JJ, Lancaster DM. In vitro torque-deformation characteristics of orthodontic polycarbonate brackets. Am J Orthod Dentofacial Orthop. 1994;106:265–272. doi: 10.1016/S0889-5406(94)70046-X. [DOI] [PubMed] [Google Scholar]
- 12.Hirai M, Nakajima A, Kawai N, et al. Measurements of the torque moment in various archwire-bracket-ligation combinations. Eur J Orthod. 2012;34:374–380. doi: 10.1093/ejo/cjr022. [DOI] [PubMed] [Google Scholar]
- 13.Morina E, Eliades T, Pandis N, Jager A, Bourauel C. Torque expression of self-ligating brackets compared with conventional metallic, ceramic, and plastic brackets. Eur J Orthod. 2008;30:233–238. doi: 10.1093/ejo/cjn005. [DOI] [PubMed] [Google Scholar]
- 14.Badawi HM, Toogood RW, Carey JP, Heo G, Major PW. Torque expression of self-ligating brackets. Am J Orthod Dentofacial Orthop. 2008;133:721–728. doi: 10.1016/j.ajodo.2006.01.051. [DOI] [PubMed] [Google Scholar]
- 15.Young TM, Smith RJ. Effects of orthodontics on the facial profile: a comparison of changes during nonextraction and four premolar extraction treatment. Am J Orthod Dentofacial Orthop. 1993;103:452–458. doi: 10.1016/S0889-5406(05)81796-2. [DOI] [PubMed] [Google Scholar]
- 16.Archambault A, Major TW, Carey JP, Heo G, Badawi H, Major PW. A comparison of torque expression between stainless steel, titanium molybdenum alloy, and copper nickel titanium wires in metallic self-ligating brackets. Angle Orthod. 2010;80:884–889. doi: 10.2319/102809-604.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fischer-Brandies H, Orthuber W, Es-Souni M, Meyer S. Torque transmission between square wire and bracket as a function of measurement, form and hardness parameters. J Orofac Orthop. 2000;61:258–265. doi: 10.1007/s000560050011. [DOI] [PubMed] [Google Scholar]
- 18.Huang Y, Keilig L, Rahimi A, et al. Numeric modeling of torque capabilities of self-ligating and conventional brackets. Am J Orthod Dentofacial Orthop. 2009;136:638–643. doi: 10.1016/j.ajodo.2009.04.018. [DOI] [PubMed] [Google Scholar]
- 19.Kusy RP. On the use of nomograms to determine the elastic property ratios of orthodontic arch wires. Am J Orthod. 1983;83:374–381. doi: 10.1016/0002-9416(83)90321-4. [DOI] [PubMed] [Google Scholar]
- 20.Odegaard J, Meling T, Meling E. An evaluation of the torsional moments developed in orthodontic applications. An in vitro study. Am J Orthod Dentofacial Orthop. 1994;105:392–400. doi: 10.1016/S0889-5406(94)70134-2. [DOI] [PubMed] [Google Scholar]
- 21.Archambault A, Lacoursiere R, Badawi H, Major PW, Carey J, Flores-Mir C. Torque expression in stainless steel orthodontic brackets. A systematic review. Angle Orthod. 2010;80:201–210. doi: 10.2319/080508-352.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bhalla NB, Good SA, McDonald F, Sherriff M, Cash AC. Assessment of slot sizes in self-ligating brackets using electron microscopy. Aust Orthod J. 2010;26:38–41. [PubMed] [Google Scholar]
- 23.Isaacson RJ. Torque or third order mechanics. Am J Orthod Dentofacial Orthop. 1994;106:21A–23A. doi: 10.1016/S0889-5406(05)80544-X. [DOI] [PubMed] [Google Scholar]
- 24.Kang BS, Baek SH, Mah J, Yang W. S. Three-dimensional relationship between the critical contact angle and the torque angle. Am J Orthod Dentofacial Orthop. 2003;123:64–73. doi: 10.1067/mod.2003.55. [DOI] [PubMed] [Google Scholar]
- 25.Baumrind S, Frantz RC. The reliability of head film measurements. 2. Conventional angular and linear measures. Am J Orthod. 1971;60:505–517. doi: 10.1016/0002-9416(71)90116-3. [DOI] [PubMed] [Google Scholar]
- 26.Cattaneo PM, Treccani M, Carlsson K, et al. Transversal maxillary dento-alveolar changes in patients treated with active and passive self-ligating brackets: a randomized clinical trial using CBCT-scans and digital models. Orthod Craniofac Res. 2011;14:222–233. doi: 10.1111/j.1601-6343.2011.01527.x. [DOI] [PubMed] [Google Scholar]
- 27.Björk A. Sutural growth of the upper face studied by the implant method. Rep Congr Eur Orthod Soc. 1964;40:49–65. [PubMed] [Google Scholar]
- 28.Harris EF, Smith RN. Accounting for measurement error: a critical but often overlooked process. Arch Oral Biol. 2009;54(suppl 1):S107–S117. doi: 10.1016/j.archoralbio.2008.04.010. [DOI] [PubMed] [Google Scholar]
- 29.Pandis N, Polychronopoulou A, Makou M, Eliades T. Mandibular dental arch changes associated with treatment of crowding using self-ligating and conventional brackets. Eur J Orthod. 2010;32:248–253. doi: 10.1093/ejo/cjp123. [DOI] [PubMed] [Google Scholar]
- 30.Carlsson R, Ronnerman A. Crown-root angles of upper central incisors. Am J Orthod. 1973;64:147–154. doi: 10.1016/s0002-9416(73)90306-0. [DOI] [PubMed] [Google Scholar]