

Abstract
To summarize the limitations of commonly used space maintainers (SMs) and provide an insight into the field's technological advances to overcome them, this review was conducted. With the rapid advancement of digital technologies, there is always something new to learn while also redefining the current fads. Digital workflow is not a new concept in dentistry, but it has only just begun to be used in pediatric dentistry. The curiosity to explore has led to the development of digital devices as SMs. They appear potential for usage in children because of their impressive advantages of precision, comfort, and a time-saving approach. This workflow helps lessen fear and improve children's cooperation and enthusiasm for dental appointments by cutting down on chairside time and shortening procedures.
How to cite this article: Dhanotra KGS, Bhatia R. Digitainers—Digital Space Maintainers: A Review. Int J Clin Pediatr Dent 2021;14(S-1):S69–S75.
Keywords: 3D printing, CAD/CAM, Digital technology, Pediatric dentistry, Space maintainers
Background
The importance of maintaining the primary dentition until its normal physiological exfoliation is not only in terms of esthetics, mastication, speech but also in aiding the normal eruption and guidance of their permanent successors.1 It is possible that ectopic eruption or premature primary tooth loss from caries and/or trauma will cause undesirable primary and permanent tooth movements, including a loss in arch length.2 If you do not have enough arch length, you are more likely to have malocclusions such as crowding and ectopic eruption as well as tooth impaction.3 Effective maintenance of the edentulous space is necessary to avoid or eliminate these negative effects.4 As stated by the American Academy of Pediatric Dentistry (AAPD), space maintenance is the preservation of present dentition placement to avoid loss of arch length, width, and perimeter.5
After using the term “Space maintenance”, in 1941, JC Brauer went on to explain that it was the process of preserving a space in the mouth that had previously been filled with one or more teeth. Fixable or moveable, unilateral or bilateral, space maintainers (SMs) are all options. Fixed space maintainers (FSMs) can be more difficult to keep clean, whereas removable space maintainers (RSMs) are more convenient.1 Fixed space maintainers, on the other hand, need less patient compliance, are easier to maintain, and are more comfortable for the patient. Determining whether to employ removable or fixed equipment is dependent on various criteria, such as the stage as a stage of dental development, number of lost teeth, occlusion, dental arch involved, age of the child, and ability to cooperate.6 Fixed unilateral SMs include the band and loop (B&L), crown and loop (C&L), direct bonded (DB), glass fiber-reinforced composite resin (GFRCR), and distal end shoe (DES). Fixed bilateral SMs include the lower lingual arch (LLA), Nance, and transpalatal arch (TPA).
Drawbacks of Conventional Space Maintainers
Pediatric dentists have long used and recommended conventional SMs, but there are several drawbacks to this approach. Researchers have found a link between RSM and FSMs and an increased periodontal index score and an increased risk of oral cavity bacteria growth.7–9 Nickel is a common and severe allergen. Nickel sensitivity was found to be higher in children who had intraoral devices that contained nickel.10 Those with SMs have a higher nickel release than patients with stainless steel crowns.11 In their investigation, Bhaskar and Subba Reddy found that in an artificial salivary media, B&L SMs release nickel at concentrations ranging from 4.95 to 7.78 ppm and chromium at concentrations ranging from 1.70 to 4.54 ppm.12 To avoid any probable health risks to children, the authors recommend using an alternative stainless steel alloy or covering it with a biocompatible substance.
The drawbacks associated with the commonly used SMs are discussed below.
Band and Loop
When a single, unilateral, or bilateral maxillary or mandibular primary molar is lost early, B&L SMs are most typically utilized.13 It has some disadvantages and failures, despite high patient compliance, like
Loss of cement or de-cementation: The most prevalent reason for failure as cited.14–18
Breakage: Poor construction quality is the second documented reason for B&L SM failures. This includes overheating the wire while soldering, thinning of the wire by polishing, flux residue on the wire, and failing to enclose the wire in the solder.14,19
Soft tissue lesions: Plaque retentive areas in poorly constructed SM loops cause calculus development and tissue overgrowth. Ulceration of the buccal mucosa due to loop impingement causes discomfort. Lingual displacement and blanching around the teeth are also caused by the ill-fitting band.20,21
Lower Lingual Arch Space Maintainer
In comparison to unilateral SM, bilateral SMs are said to endure less. Among the most common adverse effects associated with these appliances were tongue interferences, increased occlusal load, and a longer arm span, all of which could interfere with the eruption of permanent teeth.13,14,22,23
Nance Space Maintainer
Soft tissue lesions: The acrylic button that makes contact with the anterior palate is thought to be a major cause of appliance failure.13,21
Besides the drawbacks discussed, conventional SMs also present with limitations such as:24
Requires a minimum of two appointments to be made.
Gives the impression that children who are uncooperative or who have a gag reflex would find it difficult.
Expensive and time-consuming laboratory work is necessary.
Technique-sensitive stages of processing, such as band displacement during cast pouring.
Evolution of Space Maintainers
The disadvantages of conventional SM led to the development of its variants such as DB SMs, fiber-reinforced composite (FRC) SMs, and prefabricated SMs. Clinicians prefer resin-bonded SMs because of their ease of fabrication, reduced appointment count, and consequently improved patient comfort. They also do not need an annual inspection like other FSMs; thus, they can be utilized instead of conventional FSMs.25 These procedures are also long-lasting, low-risk, and low-cost in terms of repair and reversibility. Their long-term viability, on the other hand, is still debatable.16 Resin fiber SMs can be considered as successful only for a short period, according to Saravanakumar et al.26
The majority of FRC SM failures occur due to:
Debonding at the enamel-composite interface. This is because of the primary tooth's prismless enamel, which may interfere with resin retention,24,27–29 poor surface preparation, moisture contamination, and disruptions during the adhesive setting process. These are all factors to consider.30
Debonding of fiber-composite interface/fracture of fiber frame: It is possible that the bonding margins between teeth and FRC at either end of the framework will be weakened by the compressive and tangential forces of the fiber frame.17,28,31
New designs and materials for SMs are required to overcome the aforementioned disadvantages. Space maintainer appliances are now being fabricated using digital workflow instead of the traditional analog workflow because of the advantages this offers.
Digital Workflow in Pediatric Dentistry
Dentistry adopted the digital workflow in the 1980s and has been using it ever since. The use of CAD-CAM technology in pediatric dentistry has shown tremendous success in recent years. Improved patient compliance and acceptance of treatments are two main advantages. There are a few published case studies demonstrating the effectiveness of digital restorations in pediatric patients over the short and long term. Esthetic dentistry for adults and children is increasingly utilizing ceramic materials and CAD/CAM technologies. Numerous studies have found indications of the use of CAD/CAM technology in primary and permanent tooth structures.
A case study examined the benefits of resin nanoceramic CAD/CAM restoration for the primary second molar of a patient with a missing permanent second premolar successor.15 This restoration had a 3-year follow-up that showed the resin nanoceramic CAD/CAM restoration had both esthetics and function.32 CAD/CAM PICN (polymer-infiltrated ceramic network) endocrown on a primary second molar with pulpotomy exhibited excellent marginal fit, anatomical shape, and minimal discoloration 9 months later.33 A 2-year follow-up showed that using in-office CAD/CAM technology on a young patient with amelogenesis imperfecta improved quality of life and resulted in satisfactory results. Smile restoration, less clinical work, and dental structure preservation were all possible with this procedure.34 The digital impression approach, according to Yilmaz and Aydin, is more convenient and preferred by youngsters than the traditional impression method.35
This opens the door to using modern metal-free ceramic constructs to restore children's dentition, resulting in stronger, more attractive, and more effective restorations.36 In the long run, CAD-CAM technology that is quick, precise, and does not require a lot of time may be the best option for pediatric patients.
Digital Space Maintainers
Space maintainers that use CAD-CAM or 3D print technology with modern and biocompatible materials are called “Digital Space Maintainers”. The above-mentioned challenges and drawbacks of traditional manufacturing could be overcome by using this technology.
Materials Used for Fabrication of a Digital Space Maintainer
PEEK Polymer
Materials made from polyetheretherketone have a unique mix of strong mechanical properties and are rigid, opaque, and biocompatible. Chemical resistance, high-temperature stability, dimensional stability, and a wide range of processing possibilities are all provided by the material.37 Patients who are allergic to metals or dislike the metallic taste or weight can use this material because it has a natural tooth-colored appearance.38 PEEK offers several favorable features in orthodontics, according to a 2015 study, making it a potential candidate for usage as an esthetically pleasing metal-free orthodontic wire.39 The framework and prosthetic teeth can be developed in the same design module for detachable, functional varieties of SMs, releasing a fully integrated design. As a result, this technique is preferable to others that use self-curing resin and artificial teeth.40
Using PEEK polymer for the production of CAD-CAM SMs was the subject of a study done by Ierardo et al.40 They created a lingual arch (Fig. 1), a B&L (Fig. 2), and a removable plate (Fig. 3). After a 9-month follow-up, it became clear that all three patients were extremely pleased with the devices. Digital B&L SMs made of PEEK polymer were evaluated by Kun et al.41 in children with unilateral loss of either the first or second molars and were found to be 75% lighter than conventional SMs. In an in vitro investigation, Guo et al.42 compared digitally produced RSMs made of PEEK polymer to traditional RSMs. Study results showed that digitally created RSMs fit the model well, indicating that the technique was suitable for clinical applications.42 This is because the conventional technique of manufacturing has too many steps that can lead to errors during polymerization shrinkage of self-curing resin and requires grinding and polishing of the RSM, which digitally designed RSMs would not require.
Figs 1A to D.

“First case report” by Gaetano Ierardo, Source is licensed under CC BY-NC-SA 4.0
Figs 2A to D.

“Second case report” by Gaetano Ierardo, Source is licensed under CC BY-NC-SA 4.0
Figs 3A to D.

“Third case report” by Gaetano Ierardo, Source is licensed under CC BY-NC-SA 4.0
BruxZir
BruxZir is three to five times more fracture-tough than standard zirconia, with a flexural strength of up to 1,465 MPa.43 This gives the material an excellent impact resistance to the masticatory forces in the mouth. Because of its minimal thermal expansion, the material will stay in the mouth without shifting shape or becoming loose in your teeth. The first published paper on using digital technology to fabricate an SM was by Soni.44 While treating a 6-year-old female patient, the author employed BruxZir as the material for the device (Fig. 4). To keep the appliance in place, the SM was designed so that it was supported by both the canine and the primary second molar. This allowed for better appliance retention, prevented tooth tipping, and ensured that masticatory forces were distributed equally across the extracted tooth's region. There were no issues with the appliance after 6 months of testing.
Fig. 4.
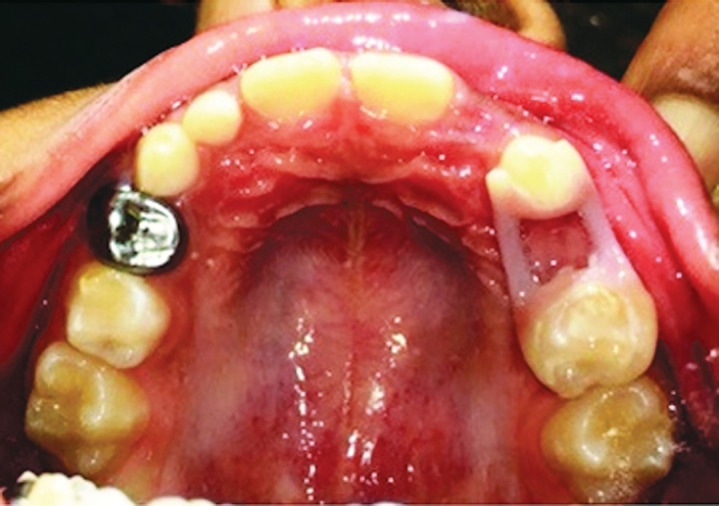
“Intraoral photograph 6 months after placement of appliance.” by HK Soni, Source is licensed under CC BY-NC-SA 4.0
Trilor
Trilor is a CAD/CAM-processed FRC resin. Metal and zirconia are heavy materials; this metal-free, biocompatible alternative weighs 3–5 times less. Durability, elastic property, low weight, biocompatibility, and repairability are some of the benefits.45 Beretta and Cirulli46 developed a metal-free CAD-CAM device intending to produce safe appliances for special needs patients, who require regular magnetic resonance imaging (MRI) in the head region to monitor certain diseases such as epilepsy or vascular problems. They fabricated a Nance palatal arch SM using Trilor and directly bonded on the palatal surface of the first primary molar.
Steps in Fabrication Using CAD/CAM Technology
By using the CAD-CAM method, restorations can be virtually designed and then milled on an automated milling machine.47 A dental laboratory is often where fabrication takes place. CAD-CAM processing begins with a traditional impression from the dentist, which is then digitized in the lab.48 Sirona introduced the first chairside CAD-CAM technology, the CEREC system, which allows dentists to design and fabricate restorations right in the dental office.49 By using chairside and laboratory CAD-CAM manufacturing methods, dental restorations can be made more rapidly.
There are three general steps in the digital restoration workflow: (1) Scanning the tooth geometry to capture digital data; (2) Digital data manipulation with a software program to build the volume model for the restoration; and (3) Production technology to transform the volume model into the restoration.50
The procedure used to fabricate a digital SM by Ierardo et al. (Fig. 5) is described below:40
Figs 5A to D.

“Digital pattern acquisition, thanks to CAD software and design of the devices” by Gaetano Ierardo, Source is licensed under CC BY-NC-SA 4.0
Step 1: After taking a dental impression and pouring the model, the models are digitalized using an additional oral scanner.
Step 2: Light beams strike the scanned object from all angles, and miniature cameras film it. The outcome is a cloud of points because the scans are multiple and detected across the entire model. The virtual model is created by connecting the dots and reconstructing a pattern of tiny polygons.
Step 3: After obtaining a virtual model, it is instantly integrated into the CAD (computer-aided design) software system. Using the zoom, rotate, and panning tools, the model can be viewed from various angles and magnifications, making it easier to analyze it and develop a personalized device. This technology enables the creation of devices and the determination of numerous variables such as material thickness, retention, undercuts, and cementation space.
Step 4: At this point, the file is transferred to the CAM, where milling begins the device's fabrication. This is a manufacturing method that involves subtracting a block of chosen material from a previously specified form using CAD software (in about 1 hour).
Three-dimensional (3D) Print Technology
Additive manufacturing, layered manufacturing, and solid freeform fabrication are other terms for 3D printing. The basic notion behind this new technology is that a digital file may be used to construct a layer-by-layer design for a 3D object of any shape or geometry. A cross-section of the final object is represented by each of these layers. Pawar51 was the first to employ digital 3D printing to create SMs (Fig. 6), with one using titanium-based powdered metal and the other clear photopolymer resin. As the author pointed out, 3D printing in pediatric dentistry has significant potential.
Figs 6A to D.

“(A and B) Metallic three-dimensional-printed space maintainer of titanium-based powdered metal material and (C and D) using a clear photopolymer resin” by Bhaggyashri Pawar, Source is licensed under CC BY-NC-SA 4.0
Advantages40–46
The advantages of using a digitally fabricated SM device and its impact are summarized in Table 1:
Table 1.
Advantages of digitally fabricated SM devices and their impact
| Advantages | Impact/outcome |
|---|---|
| 1. Esthetic | Increased patient outcome |
| 2. Metal-free | Especially advantageous for patients with metal allergy, nickel allergy and special care needs patient who periodically requires to undergo MRI in the head ‘REGION’ to monitor to specific disease as epilepsy or vascular problems. |
| 3. Precise | Reduced deformation and errors, breakage and decementation |
| 4. Quick fabrication time | Reduced no. of visits hence improved patients compliance |
| 5. Single unit appliance | High strength of the device thus avoiding fracture and reducing the failure rate. |
| 6. Smooth surface | Makes it easy to clean and polish causing less plaque accumulation leading to better gingival health. |
| 7. Lightweight | Increased comfort |
| 8. No band pinching required | No gingival lacerations/Trauma |
Disadvantages44
Expensive.
Lab assistance is required.
Fabrication expertise is required.
Expensive equipment is required.
Future Research
To determine the longevity, influence on gingival health, patient compliance, and acceptability of digitally manufactured SMs, or “Digitainers”, additional clinical and comparative research is required. Future research should concentrate on low-cost materials. Furthermore, 3D printing in pediatric dentistry has yet to be fully investigated. Using it allows us to make innovative advancements because of its accuracy and perfection.
Conclusion
Dentistry's digital workflow is continually evolving and revealing fresh techniques. Pediatric dentistry's SMs have taken a giant stride towards custom orthodontics. Devices made using digital fabrication techniques be reliable and long-lasting. Time-consuming manual fabrication stages are eliminated thanks to CAD-CAM technology. It is possible that in the future, this way of investigating more materials will be used to develop more complicated appliances. Since the digital age has arrived and offers various advantages, more and more `CLINICIANS' will likely begin to use it in their daily practices.
Footnotes
Source of support: Nil
Conflict of interest: None
References
- 1.Barberia E, Lucavechi T. Free end space maintainers: design utilisation and advantages. J Clin Pediatr Dent. 2006;31(1):5–8. doi: 10.17796/jcpd.31.1.p87112173240x80m. [DOI] [PubMed] [Google Scholar]
- 2.Tunison W, Flores-Mir C, ElBadrawy H, et al. Dental arch space changes following premature loss of primary first molars: a systematic review. Pediatr Dent. 2008;30(4):297–302. [PubMed] [Google Scholar]
- 3.Brothwell DJ. Guidelines on the use of space maintainers following premature loss of primary teeth. J Can Dent Assoc. 1997;63(10):753–766. [PubMed] [Google Scholar]
- 4.Bijoor RR, Kohli K. Contemporary space maintenance for the pediatric patient. N Y State Dent J. 2005;71(2):32–35. [PubMed] [Google Scholar]
- 5.American Academy of Pediatric Dentistry. Management of the developing dentition and occlusion in pediatric dentistry. The reference manual of pediatric dentistry. Chicago, Ill: American Academy of Pediatric Dentistry; 2020. pp. 393–409. [Google Scholar]
- 6.Christensen JR, Fields HW. In: Pediatric dentistry – infancy through adolescence. 5th edn., Casamassimo SP, Fields HW, McTigue DJ, et al., editors. St. Louise, MO: Elsevier Inc.; 2013. Space maintenance in the primary dentition. p. 379. [Google Scholar]
- 7.Arikan V, Kizilci E, Ozalp N, et al. Effects of fixed and removable space maintainers on plaque accumulation, periodontal health, candidal and Enterococcus faecalis carriage. Med Princ Pract. 2015;24(4):311. doi: 10.1159/000430787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hosseinipour ZS, Poorzandpoush K, Heidari A, et al. Assessment of periodontal parameters following the use of fixed and removable space maintainers in 6-12-year olds. Int J Clin Pediatr Dent. 2019;12(5):405–409. doi: 10.5005/jp-journals-10005-1606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kundu R, Tripathi AM, Jaiswal JN, et al. Effect of fixed space maintainers and removable appliances on oral microflora in children: an in vivo study. J Indian Soc Pedod Prev Dent. 2016;34(1):3–9. doi: 10.4103/0970-4388.175498. [DOI] [PubMed] [Google Scholar]
- 10.Feasby WH, Ecclestone ER, Grainger RM. Nickel sensitivity in pediatric dental patients. Pediatr Dent. 1988;10(2):127–129. [PubMed] [Google Scholar]
- 11.Kulkarni P, Agrawal S, Bansal A, et al. Assessment of nickel release from various dental appliances used routinely in pediatric dentistry. Indian J Dent. 2016;7(2):81–85. doi: 10.4103/0975-962X.184649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bhaskar V, Subba, Reddy VV. Biodegradation of nickel and chromium from space maintainers: an in vitro study. J Indian Soc Pedod Prev Dent. 2010;28(1):6–12. doi: 10.4103/0970-4388.60484. [DOI] [PubMed] [Google Scholar]
- 13.Simsek S, Yilmaz Y, Gurbuz T. Clinical evaluation of simple fixed space maintainers bonded with flowable composite resin. J Dent Child. 2004;71(2):163–168. [PubMed] [Google Scholar]
- 14.Millett DT, McCabe JF, Bennett TG, et al. The effect of sandblasting on the retention of first molar orthodontic bands cemented with glass ionomer cement. Br J Orthod. 1995;22(2):161–169. doi: 10.1179/bjo.22.2.161. [DOI] [PubMed] [Google Scholar]
- 15.Baroni C, Franchini A, Rimondini L. Survival of different types of space maintainers. Pediatr Dent. 1994;16(5):360–361. [PubMed] [Google Scholar]
- 16.Qudeimat MA, Fayle SA. The longevity of space maintainers: a retrospective study. Pediatr Dent. 1998;20(4):267–272. [PubMed] [Google Scholar]
- 17.Fathian M, Kennedy DB, Nouri MR. Laboratory-made space maintainers: a 7-year retrospective study from private pediatric dental practice. Pediatr Dent. 2007;29(6):500–506. [PubMed] [Google Scholar]
- 18.Sasa IS, Hasan AA, Qudeimat MA. Longevity of band and loop space maintainers using glass ionomer cement: a prospective study. Eur Archi Pediat Dentis. 2009;10(1):6–10. doi: 10.1007/BF03262659. [DOI] [PubMed] [Google Scholar]
- 19.Tunc ES, Bayrak S, Tuloglu N, et al. Evaluation of survival of 3 different fixed space maintainers. Pediatr Dent. 2012;34:97–102. [PubMed] [Google Scholar]
- 20.Nidhi C, Jain RL, Neeraj M, et al. Evaluation of the clinical efficacy of glass fiber reinforced composite resin as a space maintainer and its comparison with the conventional band and loop space maintainer. An in vivo study. Minerva Stomatol. 2012;61(1-2):21–30. [PubMed] [Google Scholar]
- 21.Chandra H, Krishnamoorthy S, Johnson J, et al. ILL effects of conventional band and loop space maintainers: time to revolutionise. Int Dent Med J Adv Res. 2018;4(1):1–3. doi: 10.15713/ins.idmjar.83. [DOI] [Google Scholar]
- 22.Rajab LD. Clinical performance and survival of space maintainers: evaluation over a period of 5 years. ASDC J Dent Child. 2002;69(2):156–160. 124. [PubMed] [Google Scholar]
- 23.Moore TR, Kennedy DB. Bilateral space maintainers: a 7-year retrospective study from private practice. Pediatr Dent. 2006;28(6):499–505. [PubMed] [Google Scholar]
- 24.Tahririan D, Safaripour M, Eshghi A, et al. Comparison of the longevity of prefabricated and conventional band and loops in children's primary teeth. Dent Res J (Isfahan) 2019;16(6):428–434. doi: 10.4103/1735-3327.270784. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kargul B, Caglar E, Kabalay U. Glass fiber-reinforced composite resin as fixed space maintainers in children: 12-month clinical follow-up. J Dent Child (Chic) 2005;72(3):109–112. [PubMed] [Google Scholar]
- 26.Saravanakumar MS, Siddaramayyal J, Gugnanai N, et al. Fiber technology in space maintainer: a clinical follow-up study. J Contemp Dent Pract. 2013;14(6):1070–10755. doi: 10.5005/jp-journals-10024-1453. [DOI] [PubMed] [Google Scholar]
- 27.Kirzioglu Z, Çiftçi ZZ, Yetis CÇ. Clinical success of fiber-reinforced composite resin as a space maintainer. J Contemp Dent Pract. 2017;18(3):188–193. doi: 10.5005/jp-journals-10024-2014. [DOI] [PubMed] [Google Scholar]
- 28.Subramaniam P, Babu G, Sunny R. Glass fiber-reinforced composite resin as a space maintainer: a clinical study. J Indian Soc Pedod Prev Dent. 2008;26((Suppl 3):):S98–S103. [PubMed] [Google Scholar]
- 29.Garg A, Samadi F, Jaiswal JN, et al. ‘Metal to resin’: a comparative evaluation of conventional band and loop space maintainer with the fiber reinforced composite resin space maintainer in children. J Indian Soc Pedod Prev Dent. 2014;32(2):111–116. doi: 10.4103/0970-4388.130783. [DOI] [PubMed] [Google Scholar]
- 30.Zachrisson BU. Clinical experience with direct bonding in orthodontics. Am J Orthod. 1977;71(4):440–448. doi: 10.1016/0002-9416(77)90247-0. [DOI] [PubMed] [Google Scholar]
- 31.Setia V, Kumar Pandit I, Srivastava N, et al. Banded vs bonded space maintainers: finding better way out. Int J Clin Pediatr Dent. 2014;7(2):97–104. doi: 10.5005/jp-journals-10005-1245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Demirel A, Bezgin T, Akaltan F, et al. Resin nanoceramic CAD/CAM restoration of the primary molar: 3-year follow-up study. Case Rep Dent. 2017;2017:3517187. doi: 10.1155/2017/3517187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bilgin M, Erdem A, Tanrıver M. CAD/CAM endocrown fabrication from a polymer-infiltrated ceramic network block for primary molar: a case report. J Clin Pediat Dentis. 2016;40(4):264–268. doi: 10.17796/1053-4628-40.4.264. [DOI] [PubMed] [Google Scholar]
- 34.Halal R, Nohra J, Akel H. Conservative anterior treatment with CAD-CAM technology and polymer-infiltrated ceramic for a child with amelogenesis imperfecta: a 2-year follow up. J Prosthet Dent. 2018;119(5):710–712. doi: 10.1016/j.prosdent.2017.07.018. [DOI] [PubMed] [Google Scholar]
- 35.Yilmaz H, Aydin MN. Digital versus conventional impression method in children: Comfort, preference and time. Int J Paediatr Dent. 2019 Nov;29(6):728–735. doi: 10.1111/ipd.12566. 31348834 Epub 2019 Aug 13. [DOI] [PubMed] [Google Scholar]
- 36.Georgieva M, Dimitrov E, Andreeva R, et al. Use of CAD/CAM technologies in pediatric dentistry. Scripta Scient Med Dent. 2017;3(2):23. doi: 10.14748/ssmd.v3i2.4306. [DOI] [Google Scholar]
- 37.Rigby RB., editor; Margolis JM, editor. Engineering thermoplastics: properties and applications. New York: Marcel Dekker, Inc; 1985. Polyetheretherketone. pp. 299–314. [Google Scholar]
- 38.Stawarczyk B, Beuer F, Wimmer T, et al. Polyetheretherketone-a suitable material for fixed dental prostheses? J Biomed Mater Res B Appl Biomater. 2013;101(7):1209–1216. doi: 10.1002/jbm.b.32932. [DOI] [PubMed] [Google Scholar]
- 39.Maekawa M, Kanno Z, Wada T, et al. Mechanical properties of orthodontic wires made of super engineering plastic. Dent Mater J. 2015;34(1):114–119. doi: 10.4012/dmj.2014-202. [DOI] [PubMed] [Google Scholar]
- 40.Ierardo G, Luzzi V, Lesti M, et al. PEEK polymer in orthodontics: a pilot study on children. J Clin Exp Dent. 2017;9(10):e1271–e1275. doi: 10.4317/jced.54010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Kun J, Dinggui Z, Wei L, et al. Clinical application of digital space maintainer fabricated by polyetherketoneketone for premature loss of deciduous teeth [J/CD]. Chin J Stomatol. 2019;13:368–372. [Google Scholar]
- 42.Guo H, Wang Y, Zhao Y, et al. Computer-aided design of polyetheretherketone for application to removable pediatric space maintainers. BMC Oral Health. 2020;20(1) doi: 10.1186/s12903-020-01184-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.What is BruxZir Solid Zirconia? View Technical Information. [Internet]. BruxZir. 2021. https://bruxzir.com/technical-information. https://bruxzir.com/technical-information [cited 19 February 2021]. Available from: )
- 44.Soni HK. Application of CAD-CAM for fabrication of metal-free band and loop space maintainer. J Clin Diagn Res. 2017;11(2):ZD14–ZD16. doi: 10.7860/JCDR/2017/23459.9246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Trilor® – The most innovative technopolymer for dental prosthesis [Internet]. Dentist Channel Online. 2021. https://dentistchannel.online/2020/02/22/trilor-the-most-innovative-technopolymer-for-dental-prosthesis/ https://dentistchannel.online/2020/02/22/trilor-the-most-innovative-technopolymer-for-dental-prosthesis/ [cited 19 February 2021]. Available from: )
- 46.Beretta M, Cirulli N. Metal free space maintainer for special needs patients. Adv Dentis Oral Health. 2017;6(2) doi: 10.19080/ADOH.2017.06.555683. [DOI] [Google Scholar]
- 47.Fasbinder DJ. Clinical performance of chairside CAD/CAM restorations. J Am Dent Assoc. 2006;137((suppl):):22S–31S. doi: 10.14219/jada.archive.2006.0395. [DOI] [PubMed] [Google Scholar]
- 48.Christensen GJ. Impressions are changing: deciding on conventional, digital or digital plus in-office milling. J Am Dent Assoc. 2009;140(10):1301–1304. doi: 10.14219/jada.archive.2009.0054. [DOI] [PubMed] [Google Scholar]
- 49.Fasbinder DJ. The CEREC system: 25 years of chairside CAD/CAM dentistry. J Am Dent Assoc. 2010;141((suppl 2):):3S–4S. doi: 10.14219/jada.archive.2010.0354. [DOI] [PubMed] [Google Scholar]
- 50.Beuer F, Schweiger J, Edelhof FD. Digital dentistry; an overview of recent developments for CAD/CAM generated restorations. Br Dent J. 2008;204(9):505–511. doi: 10.1038/sj.bdj.2008.350. [DOI] [PubMed] [Google Scholar]
- 51.Pawar B. Maintenance of space by innovative three-dimensional-printed band and loop space maintainer. J Indian Soc Pedod Prevent Dentis. 2019;37(2):205. doi: 10.4103/JISPPD.JISPPD_9_19. [DOI] [PubMed] [Google Scholar]