

ABSTRACT
The objective of this collection of essays is to gain insights into the different national-level state responses to COVID-19 around the world and the conditions that shaped them. The pandemic offers a natural experiment wherein the policy problem governments faced was the same but the responses they made were different, creating opportunities for comparison of both the kinds of policy tools being used and the factors that accounted for their choice. Accordingly, after surveying on-line databases of policy tools used in the pandemic and subjecting these to topic modelling to reveal the characteristics of a ‘standard’ national pandemic response, we discuss the similarities and differences found in specific responses. This is done with reference to the nature and level of policy capacity of respective governments, highlighting the critical roles played by (in)adequate preparation and lesson-drawing from past experiences with similar outbreaks or crises. Taken together the articles show how the national responses to the COVID-19 pandemic were shaped by the opportunity and capacity each government had to learn from previous pandemics and their capacity to operationalize and build political support for the standard portfolio of policy measures deployed to deal with the crisis. However, they also show how other factors such as the nature of national leadership, the organization of government and civil society, and blindspots towards the vulnerabilities of certain population segments also helped to shape policy responses to the pandemic.
Keywords: COVID-19, policy capacity, pandemics, policy tools, policy mixes, policy styles, crisis management
Introduction: the nature of the COVID-19 problem and state-level policy responses
Pandemics are a difficult policy problem to conceptualize and structure. This is especially true in the case of the 2019–2020 outbreak of SARS-CoV-2 coronavirus caused COVID-19 respiratory disease (World Health Organization [WHO], 2020a). Importantly in the case of such novel diseases, knowledge about the nature of the problem and the best ways to address it was particularly inadequate at the outset as much about the disease and potential solutions to its virulence and spread was poorly understood. This is quite different from many other crises, such as those caused by floods or earthquakes, where the causes are clear, the central problem obvious, and the solutions and emergency responses, from a policy standpoint, clear (Boin, ‘T Hart, Stern, & Sundelius, 2016).
In the case of a novel pandemic, the knowledge base required to design interventions is uncertain. It is only after several months of intensive study and experience grappling with COVID-19, for example, that knowledge about key parameters of the pandemic – such as how it is transmitted, the symptoms it causes, the period it takes for symptoms to emerge and subside, the number of victims who are likely to recover and succumb, and the population segments that are particularly vulnerable – were known with any degree of certainty. And even after this period much still remained unknown, such as why some communities and individuals suffered higher rates of infection and/or fatality than others, and why some individuals had few symptoms (or remained asymptomatic) and to what extent and for how long they were able to transmit the disease in this condition.
It thus bears repeating that at the outset of the COVID-19 pandemic governments had to act without this knowledge if they wished to intervene to prevent the rapid spread of the disease. And that at the time they were presented with many forecasts suggesting potentially enormous numbers of victims in the event they did little or nothing to slow down the spread (Adam, 2020; Ferguson 2020; Flaxman et al., 2020; Hsiang et al., 2020).
But determining exactly what should be done is difficult in such contexts. Disease outbreaks of this kind, of course, are a public health problem affecting large segments of the population in empirically verifiable ways. And some experience with past or similar diseases can provide some guidance as to what courses of action are likely to be effective from a public health perspective. But in the case of a global pandemic another entire range of issues lies beyond the aetiology and epidemiology of the disease itself, including how to deal with the social, economic and political crises which result from its spread, and from the public health interventions undertaken to prevent or control it (Boin et al., 2016, 2018; t’Hart, Heyse, & Boin, 2001; Weible et al., 2020).
While both effective treatments and preventative pharmaceutical interventions still remained distant, after 6-month experience with the disease the range of non-pharmaceutical interventions deployed by public health authorities around the world; from full-scale to partial lockdowns, quarantine measures of various intensity and models, social or physical distancing, various kinds of ‘track, test and trace’ measures, as well-economic policies to help offset the economic and social impact of the pandemic, have become clear. And it is also clear that early and strict enforcement of these traditional public health measures allowed some less-developed countries like Viet Nam avoid the worst of the epidemic and developed countries such as New Zealand to virtually eliminate it (Nguyen, 2020; Parker, 2020).
As Weible et al. (2020) have pointed out, there are many policy-related aspects to the COVID-19 pandemic which require research including aspects such as the effects of the disease and crisis on the emotional and mental health impact on populations; the nature of citizen compliance with public health measures and other social behaviours which allowed some preventative measures to be effective, or not; the nature and impact of partisanship on government reactions; the role of public leadership; how civil society organizations reacted to the unfolding pandemic; and its trans-national character (Boin, 2019).
From a policy perspective, however, a key concern is around detailing and understanding the responses of national and state-level governments to the arrival of COVID-19. This includes understanding the actual versus appropriate timing and sequencing of instruments to mitigate its transmission, or determining the reasons for differences between actual and optimal intensity of policy measures adopted to affect public health outcomes (Kettl, 2020; Moon, 2020). That is, as press coverage and website data from around the world have detailed (Blavatnik School of Government, 2020; OECD, 2020), all governments responded to the crisis but not at the same time, in exactly the same way, or with the same strength or rigor. Understanding why this was the case and whether such responses can be improved for future crises is a critical issue for policy studies (t’Hart et al., 2001).
Studying governmental responses to COVID-19 from such a policy perspective comprises two parts. The first is simply to catalogue the policy measures adopted to date in order to define the dependent variable; that is, what policies were actually adopted and put into place by governments to deal with the pandemic. Fortunately, many research groups, universities, and organizations launched efforts early in the onset of the disease to gather such information (Dong, Du, & Gardner, 2020; Hale, Petherick, Phillips, & Webster, 2020; OECD, 2020). This data serves to inventory the full range of tools deployed – but in raw form, without systematically highlighting their inter-relationships or important variables such as their timing or sequencing (Howlett, 2019; Taeihagh, Givoni, & René, 2013).
These interventions cover a vast range of issues, well beyond those related to purely public health and disease mitigation or prevention. They include those specifically directed at the health issues related to the disease such as ‘lock-downs’ and other forms of quarantine cited above to other measures put in place to deal with the unemployment and business losses triggered by the appearance of the disease and the public health measures taken to control its outbreak or lessen its impacts both on health and upon the medical systems delegated to deal with them (Fong et al., 2020; World Health Organization Writing Group, 2012).
Cataloging these tools is useful but insufficient, as we need to take the second step and seek to understand the reasons behind the selection of some tools rather than others and the implications of those choices on disease control and prevention; that is, to define and understand the independent variables which went into such choices (Salamon, 2002; Hood, 1986; Capano & Lippi, 2017; Howlett, 2019a, 2019b; Flaxman et al., 2020; Hsiang et al., 2020).
The articles in this special issue advances work on both these parts of the understanding of national responses to the COVID-19 pandemic. With respect to the first issue, the papers in the collection review the inventories of policy tools found in targeted countries and focus on unpacking the design and decision processes and patterns of action which led to their adoption. The issue features detailed case studies of responses to the coronavirus pandemic from the earliest affected countries – China and Italy – to countries initially considered to be very successful in dealing with the pandemic but which turned out to be less so – Singapore and Israel – to countries with less successful responses – the United States and Sweden – as well as those of several others which proved reasonably successful in holding off or turning around outbreaks – Canada, South Korea, Turkey and Hong Kong – although sometimes with significant blindspots and failures in key areas such as the protection of specific vulnerable populations (Bach & Wegrich, 2019).
This second issue – determining not only how national responses differed but also why different responses occurred in the first place – is also addressed in these case studies. How policymakers come to view a problem and the consequences of how it is portrayed to them by experts is critical to policy-making but is usually difficult to disentangle when issues arise over a long period of time and key aspects of decision-making are buried in the mists of time (Grødem & Hippe, 2019). With the COVID-19 case, however, policy scholars are presented with the highly unusual opportunity to study virtually simultaneous but different government responses to the same problem and thus tease out the key factors which drove those decisions and their implications for both policy success and future practice. The case studies detail how the problem of the pandemic was constructed at the cognitive and ideological level by national and international governing elites and epistemic communities (Peters, 2005, 2018; Haas, 1992; Zito, 2018; Dunlop, 2009) and with how traditional mechanisms for dealing with problems – national policy styles (Howlett & Tosun, 2019) – were over-ridden or came to the fore in specific national circumstances.
Dealing with COVID-19 uncertainties: the novel nature of the crisis and its policy significance
There are many aspects of the COVID-19 crisis which make it a thorny policy problem. As pointed out above it involves and involved many types of uncertainty, issues around immediacy; data limitations; lack of consensus among experts and variations in expertise; the possibility of over and under reactions; and different levels of trust in government, technical know-how, political support for certain kinds of interventions, and many others.
One key aspect of the COVID-19 pandemic, however, is its novel character. That is, while there have been other pandemics and similar large-scale, fast-moving crises in the past – from wars to natural or financial disasters – it bears repeating that the processes of problem definition and solution articulation around the emergence of the SARS-CoV-2 coronavirus were unique in that many aspects of this particular virus were unknown (Russell et al., 2020).
This novel character meant that the nature of the policy responses around COVID-19 were not only unknown but also contested and highly uncertain, more so than with many crises such as bushfires, earthquakes or outbreaks of better-known diseases like cholera, where standard operating practices incorporating best practices from past experience exist.
While the COVID-19 crisis may be an extreme case; however, it is not uncommon for governments to act in the face of uncertainty (Manski, 2013) and it is only the extent of the ambiguity around the impact and effects of the coronavirus which is important here. That is, regardless of the extent and degree of uncertainty, governments must either act or not and then afterwards face the consequences of their actions or inactions. And societies must always accept some of the risk associated with any course of governmental action or inaction due to the impossibility or enormous cost and time typically needed to reduce uncertainties to zero (Walker, Marchau, & Kwakkel, 2013). This is true whether the issue is correcting homelessness or defeating a virulent disease, but both societies and government differ in the level of risk they may accept and how societies react to errors or governmental over- and under-reaction to crises (Hood, Jennings, & Copeland, 2016; Leong & Howlett, 2017; Maor, 2020; Maor, Tosun, & Jordan, 2017).
The high level of uncertainty caused by the novel nature of the COVID-19 disease opened up more discretion in the political and official responses to expert advice than would normally be the case for crises with better-known causes and outcomes.
In some countries, like Taiwan which had a similar experience with the earlier 2002–2004 SARS-CoV-1 outbreak (Lai, 2018) and where discussion and policy debate was framed in national security terms, no risk of mass contagion and state or social breakdown was acceptable (Huang, 2020). However, in many others ‘framing’ and ‘blaming’ struggles linked to government action and inaction played out around the development and use of epidemiological models developed by experts and government agencies trying to clarify and quantify risks based on analogies to past epidemics and infections, and then later through the comparison of early predictions and estimates with official health statistics of actual rates of disease incidence, hospitalization and death (Ferguson et al., 2020; Rhodes & Lancaster, 2020).
This process was compounded by issues concerning the need to disentangle the empirically verifiable natural dimensions of the pandemic from the socially and psychologically constructed ones surrounding a health problem occurring within an existing public health system which could prove capable of affecting the ‘natural’ course and spread of the disease (George, Verschuere, Wayenberg, & Zaki, 2020; Johnson, Dawes, Fowler, & Smirnov, 2020). Indeed, it proved very difficult to gather empirical evidence on disease impacts due to both the manner in which public health statistics are kept and how epidemiological and other models are constructed and interpreted (Michaud, Kates, & Levitt, 2020; Van Dooren, 2020)
There are some aspects of the natural history of the disease on which there was considerable agreement at the outset of the pandemic; however, which affected public perceptions of the threat of the disease and government efforts to counter it. Based on what was known from early encounters with the disease, for example, it was agreed by all parties early on that the natural susceptibility of individuals to infection was more or less the same everywhere. That is, all models and statements agreed that no one was immune naturally, that there was no vaccine immediately available and not likely to be one for some time, if ever, and that no effective therapeutic strategies existed for patient management (CDC, 2020). Thus, to some extent at least, the basic elements of problem definition around COVID-19 were determined by the expectation that, ceteris paribus, identical populations in identical situations and infected in identical ways would experience more or less identical outcomes, including whatever variations in susceptibility of serious infection or death might exist by age, gender, and other human characteristics.
This agreement on the nature of the disease and its impacts are important in assessing government responses to the crisis. First, they provide a baseline against which the behaviour of citizens, leaders and organizations can be assessed, since the failure to accept or recognize these facts is a telltale sign of the extent to which decision-making and policy-making was driven less by public health knowledge and concerns than by other factors.
Second, given the reality of equal epidemiological and biological susceptibility, cross-national variations in rates of infection, recovery and death can be considered to be the result of differences not in the natural but in the socially constructed realms of the disease. These include, for example, lifestyle and diet-related co-morbidities whose occurrence varies by country; the nature of previously existing levels of social interactions which also vary in effected jurisdictions and affect interpersonal transmission rates; environmental factors such as different levels of pollution which also affect respiration and differ by country; as well as differences in a government or society’s capacity to stop or suppress the spread of the disease through the use of non-pharmaceutical interventions, such as its ability to trace and isolate infected persons and carriers of the disease. The only naturally occurring phenomenon expected to affect the severity of infection and recovery from the disease was the society’s demographic structure, particularly the share of the aged population who proved to be particularly vulnerable to the disease due to the higher instance of other medical conditions which affected their ability to withstand and recover from the coronavirus (Chopera, 2020).
Given these natural and social differences, it was hard to generalize about the conditions that affect the introduction and the rate of spread of the virus, two key factors that any solution must address. Two laboratory-like situations which were by many experts and governments to estimate the infection or attack rate were two outbreaks on cruise ships in Japan in early February 2020 and in California in early March. In these cases, mingling and many other social aspects were ‘controlled’ and passengers were quarantined after an initial more or less standard level of exposure to the infection. These ships had an infection rate of between 15% and 20% of passengers with 90% of the cases being mild and about 10% critical, and first indicated a propensity to more severely affect elderly persons (Russell et al., 2020). The results for a similar case but with repeated mingling occurred later on an infected US navy aircraft carrier where 60% of the crew were found afterwards to have antibodies to the virus – indicating previous exposure – although the younger and fitter crew had a much lower percentage of acute cases than did the more elderly cruise ship passengers, and only one death (Payne et al., 2020). A similar level of infection was subsequently found in Bergamo, Italy (57%), one of the earliest and repeatedly hard-hit cities and provinces in the country (Amante, 2020). Estimating the mortality or overall death rate in a population is critical and in Italy, where many acute cases were hospitalized and tracked, about 25% of critical cases subsequently succumbed to the virus (El Sahly, 2020).
Although the cruise ship figures for actual cases were lower than those originally reported out of China, where the disease was first noted, the absolute magnitude of possible infections and direct fatalities was enormous. Taken together, these figures suggested to most observers that the percentage of the population dying from a single infection episode for a population living in fairly close proximity – such as a city – would be around 0.4–0.5% and the absolute number would increase with each round of infection. This data, along with associated evidence of the exponential growth of infections once cases had begun to appear, quickly and understandably prompted consternation and demands for action among most public health communities, publics and governments (Mallapaty, 2020).
That is, in a real-world situation with no restrictions on social interactions and thus more frequent mingling of infected and uninfected individuals, with no treatments or vaccines, the number of mortalities would be very high in a very short period of time. These numbers would of course decline, perhaps to zero, if effective vaccination and drug therapies were found or if previous exposure provided some level of immunity to re-exposure.
But barring those eventualities, which were very uncertain and unlikely, most if not all governments realized some policy interventions were needed. This was both in order to try to prevent many untimely deaths from the disease itself and also to avoid overwhelming hospitals and critical care units with affected patients which would in turn result in more indirect deaths among people affected by non-COVID-19 ailments (e.g., heart disease, cancer), who would encounter difficulties receiving needed treatments. These possibilities led in many countries to calls for public action to ‘flatten the curve’ or reduce the exponential growth of the disease by whatever means possible (Specktor, 2020). Exactly what each country did in this effort, how much these actions were similar, and why and how they differed, are the questions the articles in this issue address. The general picture, however, is set out below.
A standard policy response: the policy mix for pandemics
Once a decision had been made to respond; however, there remained the choice of which kinds of interventions or policy instruments to employ. The range of policy tools available to policymakers for responding to any crisis is limited, although there is an almost limitless means of combining these, as well as varying degrees to which tools can be applied (intensity) and sequenced (Capano, Pritoni, & Vicentini, 2019; Howlett & del Rio, 2015).
The general pattern of the onset of the disease in different countries around the world is set out in Figure 1. This outlines the basic timeline for state-level responses after the discovery and onset of the disease as it spread to each jurisdiction.
Figure 1.
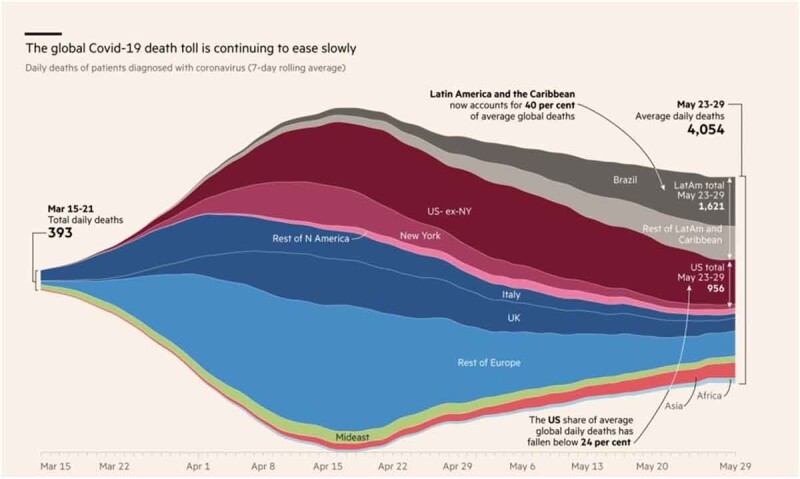
Onset of COVID-19 by country or region.
Source: https://www.ft.com/content/a26fbf7e-48f8-11ea-aeb3-955839e06441.
As is common with many policy problems, government responses to the appearance of COVID-19 involved the adoption of a ‘mix’ or bundle of tools in a variety of policy areas – social, health, medical, economic – rather than just a single tool (such as a quarantine) (Howlett & del Rio, 2015; Moon, 2020).
As mentioned above, the specific policy tools and their calibrations used by different governments in the COVID-19 pandemic varied and in order to ascertain a clear picture of which kinds of tools were used and why it is necessary to first catalogue and classify them. Several datasets exist which can be used for this purpose. Each provides different kinds of information on government responses (see Dong et al., 2020; Hale et al., 2020; OECD, 2020) which can be subjected to quantitative and qualitative analysis to shed light not only on the general configuration of national-level state policy responses but also around key questions such as the timing, speed of adoption and application, and stringency of the measures adopted.
To examine the themes around which the policy responses to COVID-19 were clustered, we employed topic modeling – specifically, a structural topic model (Roberts, Stewart, & Tingley, 2014; R Core Team 2019). This is a machine learning technique effective in ‘discovering’ latent or hidden common topics in text documents including the descriptions of policy tools contained in the databases mentioned above (Blei, Ng, & Jordan, 2003; also see Walker, Chandra, Zhang, & Witteloostuijn, 2019; Valdez, Pickett, & Goodson, 2018; Nowlin, 2016).
In the area of public health and safety, the CoronaNet dataset (Cheng, Barceló, Hartnett, Kubinec, & Messerschmidt, 2020) records over 8,000 COVID-19 related policy announcements from 190 countries between 31 December 2019 and 23 April 2020 when it was examined for this study. Using topic modelling, these records can be decomposed into thirteen-topics (Roberts et al., 2014) which outline the basic parameters of the ‘standard’ national-level COVID-19 public health response.
The 13 health-related themes uncovered in the CoronaNet dataset, ranked in descending order of prevalence, are:
External travel restriction;
Health facilities;
Quarantine, tracking, and testing;
Advisory systems;
Public awareness;
Nonessential businesses;
Government services;
Mass gatherings;
School and university closure;
Curfew;
Health screening;
State of emergency; and,
Internal travel restriction.
Not all governments adopted these instruments in the same order or at the same point in time, however. And they also did not apply them with the same level of stringency: some applications were ‘strong’ and mandated, while others were ‘weak’ or less directive. The earliest health-related response in this dataset was recorded in the week of 29 December – when the China office of the World Health Organization (WHO, 2020b) noted the emergence of ‘a pneumonia of unknown cause’ in Wuhan, China. China and its neighbouring countries – Russia, Taiwan, Singapore, South Korea, and Thailand – responded soon after with external travel restrictions, public awareness campaigns, and health screening.
This pattern of health interventions is shown in Figure 2.
Figure 2.
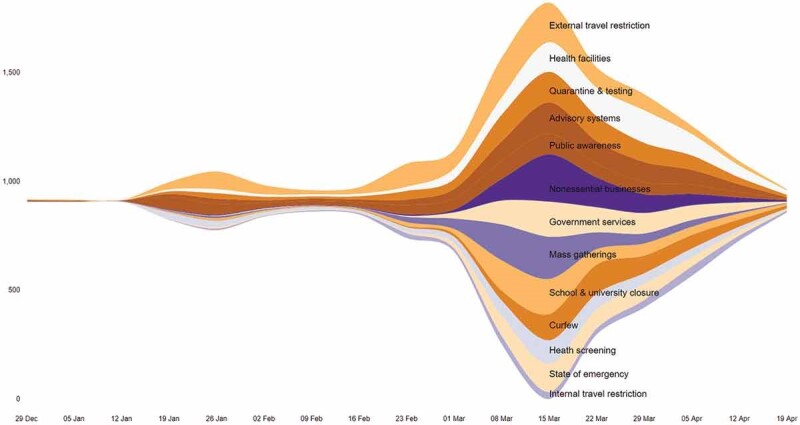
Policy announcements over time.
The y-axis represents the number of policy announcements, offset around the middle of the range for ease of visualization. The x-axis represents time with week as the unit. The colour of each band represents a public health and safety theme in the response.
As this figure shows, a first spurt in the number of policy announcements – largely relying on the same policy tools – occurred the week of 12 January when the first confirmed case of a ‘novel coronavirus’ was recorded outside of China. The largest slew of policy announcements, signaling the deployment of a more diverse policy mix relying particularly on social distancing, occurred the week of 8 March, by which time COVID-19 had spread to several countries – including, most significantly, Iran and Italy – and the number of confirmed cases globally crossed 100,000. In the subsequent week, as the WHO (2020b) declared COVID-19 a pandemic, over 1,800 policy announcements were made around the world covering every type of response. While the number of policy announcements reduced gradually thereafter, several of the policy tools adopted continued to remain active till the end of April.
This meta-visualisation shows a pattern of similar timing in the adoption of health interventions; however, it also hides significant national variations in the timing of specific responses. As Figure 3 shows, for example, countries such as Singapore and South Korea acted earlier and more quickly than many countries in adopting tough measures such as travel restrictions, health screening, quarantine and testing, and public awareness. In contrast, countries such as Italy and Israel had a more gradual response to the pandemic, with less emphasis on health screening and, to some extent, even on public awareness campaigns. Meanwhile, countries such as the US and Canada responded later (though not necessarily slowly once they started) and initially focused more on select measures of social distancing rather than travel restrictions and public awareness. Finally, countries such as Sweden and Turkey in many of their responses reacted late, but deliberately.
Figure 3.

National variation in policy response.
The y-axis represents the number of health policy announcements while the x-axis represents time with month as the unit. The colour of each band represents a public health and safety theme in the response.
As discussed above, however, public health interventions formed only one component of the portfolio of government responses to COVID-19, with many other interventions undertaken in other sectors to offset the economic and social damage caused by the disease and by some of the health-related measures – such as business closures and lock-downs which severely impacted industries from tourism and air travel to night clubs and symphonies – deployed in the effort to slow down the spread of the disease.
A dataset compiled by the OECD (2020) is more useful in understanding the full breadth of policy responses to the COVID-19 pandemic as it covers a wider-range of policy areas. These include fiscal and monetary initiatives, employment and social initiatives, health policy, science and innovation policy, and tax policy, even though data on some of these is limited to OECD countries (OECD, 2020).
An analysis of the OECD database using similar techniques as with the CoronaNet data identified 18 topics which were found to be common in the text of the policy interventions listed in the dataset. The 18 themes resulting from the topic modeling are shown in Table 1.
Table 1.
Ranked list of 18 policy tools commonly used in response to the COVID-19 crisis.
| 1. Tax payment deferral |
| 2. Tax regulation relaxation |
| 3. Leave & underemployment |
| 4. Business loan |
| 5. Social distancing |
| 6. Travel advisory & restriction |
| 7. Health facilities |
| 8. Monetary policy |
| 9. Social security |
| 10. Medical supplies |
| 11. Patient care |
| 12. Immunization & treatment |
| 13. Support for the vulnerable |
| 14. Information & advice |
| 15. School & university closure |
| 16. Financing relief |
| 17. Health-care spending |
| 18.COVID-19 epidemiology |
Source: Authors' analysis using OECD (2020).
As the data in Table 1 shows, although they might be thought of as ‘secondary’ to the public health initiatives, the most commonly deployed government tools were economic in nature and the single most prevalent government responses in the dataset focussed not on public health, per se, but rather on tax policy treatments to offset economic damage. Tax payment deferrals (Theme 1) extended tax payment deadlines and provide 0% interest on owed amounts, while tax regulation relaxation (Theme 2) provided preferential tax rates for select taxpayers and VAT (value-added tax) exemption for small-scale industries. Other prominent fiscal and monetary interventions involved supporting businesses through new loans and changes in the conditions of lending (Theme 4) and injecting liquidity into the economy using relaxation of loan conditions, interest rate cuts, and additional forms of liquidity support (Theme 8).
Similarly, several responses focussed on social policy. For instance, Theme 3 on leave and underemployment involved the adoption of short-time work compensation, relaxing eligibility requirements for unemployment insurance, compensation for dependents’ care, and compensatory sick pay for those affected by COVID-19. Relatedly, another response focused on social security (Theme 9), deploying tools to protect labour income, pay for social contribution of employees by the government, wage subsidies, and enhancing workplace health and safety regulations to reduce the risk of COVID-19. A third area of social policy specifically targeted economically vulnerable people (Theme 13) using policy instruments such as cash transfers to poor families, exemption from utility bills for households, extra payment to pensioners, and the provision of food supplies and vouchers.
As one might expect, of course, the OECD data also display similar health interventions to those listed above in the CoronaNet data. Thus, the fifth most prominent theme focused on social (or physical) distancing through both a positive list of activities that are permitted and a negative list of activities that were prohibited in order to reduce population mingling and disease spread. A related theme emphasizes travel advisory and restrictions, including complete bans, as another way of reducing the spread of the virus and disease (Theme 6). The theme of school and university closure (Theme 15) also similarly aimed to reduce the risk of infection in population massing and the use of alternatives such as online education, remote learning through public service broadcast, and television schooling.
Additional health responses to the pandemic focused on health facilities (Theme 7), medical supplies (Theme 10), and patient care (Theme 11). To prepare health facilities for expected large increases in patient numbers, countries have classified hospitals as COVID-19-exclusive, augmented testing capacity, mobilized additional health-care staff, and used telemedicine to keep non-COVID-19 cases away from hospitals, protect health workers and doctors, and reduce the spread of COVID-19. In addition, to shore up medical supplies, some governments banned the export of essential commodities, coordinated with domestic industries to create local supply chains, controlled procurement and distribution of personal protective equipment, and facilitated the import of medical equipment. Further, to streamline patient care, policies have focused on changing the rules of appointment for health staff, increasing staffing in intensive care facilities, enhancing resources for efficient patient flow, re-organizing pharmacy activities to avoid social contact, and postponing other medical hospitalizations.
Several themes also demonstrate an effort to enhance the role of science in responding to the pandemic. Theme 12 on immunization and treatment, for example, emphasized the extension of funding for the development of a vaccine, initiation of research programmes, and open data sharing. Similarly, another line of response involved promoting additional research into COVID-19 epidemiology (Theme 18), including pathogen mechanisms, immune responses, and prevalence in the population. Moreover, several countries have emphasized their reliance on policy advice – from health professionals, scientific advisory groups, and standing committees – for decision-making and used press conferences, social media, targeted advertisements, and the web for creating public awareness.
Finally, two themes capture the budgetary implications of responses to COVID-19. Theme 16 on financing relief mentions the use of tools such as the suspension of fiscal responsibility, parliamentary approval for additional borrowing, temporary reduction in salaries, and use of national savings fund to inject of money into the economy. Meanwhile, theme 17 on healthcare spending highlights that countries have issued emergency calls for funding on pandemic response, accepted public donation, and reprioritized their budgets to provide additional resources for the health sector.
While the prominence of each theme in the policy response varies from country to country, the composition of the average national response to COVID-19 can be gauged through a country-level correlation network of these 18 themes (Figure 4).
Figure 4.
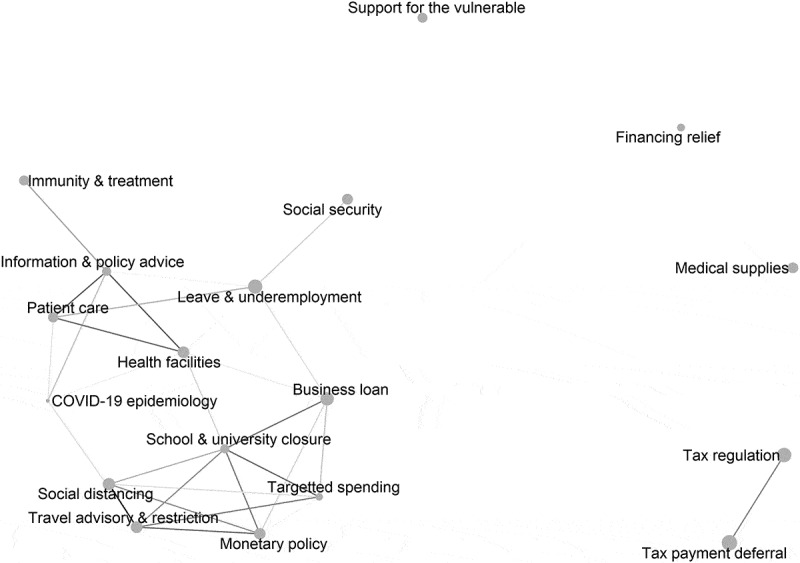
Structure of the standard COVID-19 policy response mix.
Each node represents a major topic, or theme, in the response. The size of the node indicates its prevalence in the dataset. An edge connecting two nodes indicates a correlation coefficient of >0.20. The colour intensity of the edge indicates the strength of the correlation.
As Figure 4 shows, several themes co-occur frequently within national responses, indicating that a standard, or typical, response was comprised not only of multiple policy tools within each theme but also across the mix of policy objectives and areas that were targeted. And the public health and safety response to the pandemic – in the form of social distancing, travel advisories and restrictions, school and university closures, and healthcare spending – were highly correlated not only with one another but also with the economic response; specifically, loans to businesses and monetary policy (Van Bavel et al., 2020). Similarly, the medical responses to COVID-19 also show high correlations; with health facilities, patient care, information and policy advice, immunity and treatment, and epidemiology co-occurring frequently, and also connected to social policy through its implications for leave provisions and underemployment mitigation. In contrast, interventions in tax regulation, financing relief, medical supplies, and support for the vulnerable stand out from the ‘average’ policy mix, indicating that they were not as well integrated into the general set of responses made by many countries.
Variations in the start, speed, and scope of response
While the standard response to the pandemic can be decomposed into the 18 themes outlined above, the response from one country to another varied not only in the composition of the policy mix but also in the timing of policy adoption as well as in the ‘intensity’ or ‘stringency’ with which various tools were deployed – from compulsory quarantines to voluntary ‘lockdowns’ and social distancing measures (Attwell & Navin, 2019; Knill, Schulze, & Tosun, 2012; Ritchie, Roser, Ortiz-Ospina, & Hasell, 2020; Schaffrin, Sewerin, & Seubert, 2015). Explaining national variations in responses thus involves explaining not only variations in adoption of the standard package but also differences in the timing, sequencing and speed of adoption, and in the intensity of application found among different countries.
The literature on policy capacity offers some clues to understanding these variations (Painter & Pierre, 2005; Wu, Ramesh, & Howlett, 2015). Policy capacity is defined here, similar to Gleeson et al. in their work on public health (2009, 2011), as the set of skills and resources – or competences and capabilities – necessary to perform policy functions across different sectors. At least in the abstract, whether or not a government moves early, quickly, and strongly in any policy area depends on its capacity to galvanize its administration and society into action and execute its decisions effectively. While this capacity may not be exercised and mistakes may be made, decisive and effective response would be impossible in its absence (Wu et al., 2015).
Following Moore’s (1995) analysis, key skills or competences which comprise policy capacity can be categorized into three types: analytical, operational, and political. Each of these three competences involves resources or capabilities at three different levels – individual, organizational, and systemic – generating nine basic types of policy-relevant capacity, as shown in Table 2 (Wu et al., 2015).
Table 2.
Policy capacity: skills and resources.
| Skills and competences | |||||
| Analytical | Operational | Political | |||
| Levels of Resources and Capabilities | Individual | Individual Analytical Capacity | Individual Operational Capacity | Individual Political Capacity | |
| Organizational | Organizational Analytical Capacity | Organizational Operational Capacity | Organizational Political Capacity | ||
| Systemic | Systemic Analytical Capacity | Systemic Operational Capacity | Systemic Political Capacity | ||
Source: Wu et al. (2015).
In the case of their response to the COVID-19 crisis, the key capabilities of governments relate to their preparation and planning for such pandemics, which is another way of describing the managerial and organizational resources they had at their disposal when first encountering the virus (McConnell & Drennan, 2006). Past experience, on the other hand, is a proxy for different levels of existing skills and competences.
In general, as t’Hart, Heyse & Boin (2001) have pointed out, explaining variations in the timing and nature of governments interventions in a crisis vary according to the nature of the crisis: rapid and severe crises demand more from leaders and systems than their ‘slow-onset’ counterparts (Kehinde, 2014; Staupe-Delgado, 2019). And, as Boin (2019) noted, transnational crises also engender different dynamics than purely national or localized ones.
There is no doubt that the COVID-19 pandemic began as a fast-moving, severe, transnational crisis and the articles in this issue demonstrate how the two dimensions of capacity set out above – preparation and past experience – impacted leaders and decision-makers in different systems in different ways depending on the configuration of these factors.
Governments which were prepared for pandemics and had recent similar past experiences, such as those in Asia which had dealt with SARS-CoV-1, H1N1 and MERS, were most likely to have been prudent and have a realistic level of confidence in the capability of their existing public health and financial systems to handle new communicable diseases. They were well informed about their actual capabilities and also of the potentially very dangerous nature of the disease. This led them to be wary of the disease and, ceteris paribus, pushed them towards relatively early, slow but steady and strong responses in terms of rolling out elements of the standard portfolio of policy tools listed above.
Other governments were prepared in the sense of having high performing medical systems but had no or only out-dated relevant past experiences with such pandemics. Some of these were confident in their capacity to handle a new disease but lacked the competences, including in decision-making, required to do so effectively. They tended to feature later, slower and weaker responses than their more experienced counterparts. This was the case, for example, in some countries in Europe and North America which had well-developed and high capacity public health systems but had been only lightly touched by recent epidemics such as SARS-CoV-1 or H1N1.
Thirdly, there were those governments that were unprepared in the sense of having scant-dedicated resources directed towards emergencies but who had recent past experience dealing with similar kinds of diseases and crises. Leaders in such countries, like those in Africa which had recently dealt with Ebola and HIV crises, had a very realistic lack of confidence in their existing system capabilities to handle a well-entrenched pandemic and instead reacted early and quickly and in a very strong fashion to quell a newly emerging threat before it could get established.
The final type of response was from countries which were both unprepared and had no recent relevant past experience. Such countries were complacent initially and then shocked as the true nature of the pandemic and their lack of preparedness was revealed, as occurred in some European countries like Italy and in Latin America. They were late and slow in responding and then had a strong (panic) response.
These patterns may be diagrammatically illustrated as follows (Table 3).
Table 3.
A capacity model explaining different country responses.
| Relevant past experience | |||
| High | Low | ||
| Pre-Existing Levels of Preparation | High | Prudent or realistic level of confidence in existing system capabilities to handle new disease. Well-Informed but wary of disease → intervened relatively early with a slow but steady and strong response. e.g. Many Asian Countries |
Prepared but with no or outdated past experience. Somewhat justified (over) confidence in existing system capabilities to handle new disease. Well informed about resources but not epidemiology → late, slow, and weaker response. e.g. Some North American and European Countries |
| Low | Realistic lack of confidence in existing system capabilities to handle new disease. Well-Informed about problems with system and disease and knowledgeable of weaknesses → early, fast and strong responses. e.g. Many African countries |
Shocked. Not well informed or prepared and taken by surprise → late, slow but ultimately strong panic response. e.g. Some European, North American and Latin American countries |
|
Country case summaries
This is only a general model of possible national or state-level responses. Many local conditions also affected the transmission and response to the diseases; such as whether or not many cases appeared quickly in the country, how much attention leaders and publics were paying to other issues at the time of outset, the specific nature and timing of any past experiences they had had with similar diseases, and others. And in many cases, overall performance levels were brought down by ‘blindspots’ in otherwise well-performing systems where vulnerable sections of populations failed to be cared for adequately. This was the case in many countries, for example, with ‘captive’ populations such as seniors, prisoners or migrant workers who were initially ignored by some public health efforts even in otherwise well-organized countries and suffered proportionally very high infection and mortality rates as a result (Bach & Wegrich, 2019).
Given these kinds of idiosyncrasies, in order to attain a better picture of exactly what happened and why in different countries there is a need for detailed case studies which can supplement and enrich large-n comparative studies of national-level responses to COVID-19 (Toshkov, Yesilkagit, & Carroll, 2020). And that is what each of the 10 studies of national-level state responses to COVID-19 does in this special issue.
The discussion begins with two largely unprepared countries, China and Italy – which reacted slowly at the outset of the pandemic. This is followed by eight additional case studies of countries which were more prepared for the event, six of which acted strongly when challenged by the disease – Singapore, South Korea, Canada, Hong Kong, Turkey and Israel – and two of which did not – US, Sweden.
The case studies support the general propositions set out above with respect to the significance of degrees of preparation and the significance of past experience in affecting the timing, speed and strength of responses. But they also highlight a wide-range of factors responsible for the different pathways and trajectories each took towards the establishment of the standard policy mix found in the pandemic. These additional factors highlighted by the authors of each chapter are listed in Table 4.
Table 4.
Case findings: additional factors affecting state-level responses.
| China | Social values, community resilience and past experience with SARS-CoV-1 led to an initial period of chaos until central control was reasserted in the COVID-19 case |
| Italy | Existing poor policy design and institutional arrangements favouring discord along with no recent relevant experience with similar diseases |
| Singapore | High Policy capacity but societal blind spots regarding foreign workers negatively affected the national-level COVID-19 response. |
| South Korea | Organizational learning from recent past experiences with similar events such as SARS-CoV-1, H1N1 and MERS led to effective anti-COVID-19 measures. |
| Canada | Well-functioning federalism and lesson-drawing from SARS-CoV-1 and H1N1 but with a serious blind spot towards vulnerable senior populations in long-term care facilities led to a less than satisfactory response. |
| Hong Kong | Social values, community resilience and experience with similar diseases and other crises led to an effective response. |
| Turkey | Authoritarian legacies and processes allowing rapid and strong responses to perceived threats also functioned in the COVID-19 case. |
| Israel | The COVID-19 response was coloured by local politics and a history of deliberate over-reactions to threats for electoral and other purposes. |
| USA | The vagaries of federalism led to disjointed responses across the nation and ineffective responses to the pandemic. |
| Sweden | Social values and governments favouring nudging combined with health decentralization undermined co-ordinated national action and led to a more ‘laissez-faire’ approach to pandemic management. |
China, where the virus first appeared, was not well prepared to deal with it at first but had enough recent experience with similar diseases such as SARS-CoV-1 and H1N1 to realize the danger it faced. As the first country stricken by the COVID-19 pandemic, Ciqi Mei notes, China’s policy response featured chaos at the start and effectiveness in the end. By examining the record of this policy turn in China’s fight with the pandemic, Mei shows that the pandemic was an exogenous shock which overcame the normal policy logic followed by Chinese policy actors, resulting in some initial policy inconsistency. Nevertheless, when centralized control was re-asserted, the policy mix adopted in the country comprised of traditional public health measures such as strict community lockdowns, cross-jurisdictional mobilization of resources and the firing of poorly performing officials contributed to the country’s eventual return to effectiveness.
Another country which was also affected early and was similarly unprepared was Italy. As Giliberto Capano argues, Italy was the first big epicentre of the COVID-19 pandemic in the Western world and had few precedents to draw from in fashioning its response. Since it had not had any serious recent experience with this kind of disease, the Italian response showed how a lack of specific preparedness measures drove the country to deal with this kind of crisis through existing political means, with all of their attendant strengths and weaknesses. In the Italian case, this meant that the political games characteristic of existing institutional arrangements drove the process and the content of the national response and led to a partially chaotic and slow response.
Other countries which, like China, had faced similar epidemics from SARS-CoV-1 to H1N1 and MERS in recent years included Singapore and South Korea. Drawing on this experience, both countries moved early, quickly and strongly to deal with the COVID-19 crisis. Backed by its excellent public healthcare system and efficient public administration, Singapore’s efforts to manage and contain the COVID-19 outbreak ensured minimal community transmission of the virus and low levels of COVID-related fatalities from initial infections. However, JJ. Woo notes that administrative blindspots led to the emergence of several large infection clusters in the country’s foreign worker dormitories, giving rise to subsequent high infection rates.
This was different from the situation in South Korea where a similarly high capacity and seasoned public health and state administration mobilized massive testing and tracing resources to manage the COVID-19 (Moon, 2020). As M. Jae Moon and his colleagues argue, the Korean government’s learning from past infections allowed it to effectively tame COVID-19 without forced nationwide interruptions (i.e., lockdowns) of citizens’ daily lives. Extending the theory of organizational learning, Moon, Lee and Hwang propose the Korean government engaged in a form of ‘quadruple-loop’ learning to find solutions to COVID-19; taking advantage of institutional memories and learning from its own past experiences and that of other governments as well as adaptively responding to the constantly changing targets presented by the disease. Their study also highlights the positive impacts other critical factors had such as leadership, transparency, and citizen participation, all of which contributed to effective learning and eventually to effective South Korean COVID-19 crisis management.
Canada was another highly capable state with a well-prepared health and banking system in place to respond to the crisis but, like Singapore, had weak spots in its system – namely around poorly regulated long-term care facilities. These proved especially susceptible to outbreaks of the disease. In his article, Andrea Migone explores how Canadian federalism, with its complex mix of competencies, and the country’s punctuated gradualism policy style interfaced with the need for urgent, complex decision-making in response to the COVID-19 pandemic. He finds that while the normal Canadian policy style limits national responses to crises, lessons drawn from the SARS-CoV-1 and H1N1 cases emphasized the need for coordination and resourcing to be undertaken in crisis situations and that those lessons were put into practice in the effective management of the COVID-19 crisis, albeit imperfectly.
Hong Kong is another case of a well-prepared and experienced state but one in which political and institutional legitimacy – usually thought to be crucial determinants of effective crisis management – were low due to recent clashes between the public and Hong Kong government over the territory’s relationship with mainland China. As Darryl S.L. Jarvis and Kris Hartley point out, although failure to respond effectively could have been expected in Hong Kong for this reason, in fact, its crisis responses were unexpectedly successful. The authors call for a more nuanced understanding of how social behaviours and norms are structured and reproduced amidst existential uncertainties and policy ambiguities caused by sudden and convergent crises, and how these can themselves generate resources that bolster non-state capacities to fight pandemics.
Turkey is another case of a strong state prepared for action and with recent experience in dealing with major disruptions and crises around large-scale refugee and migration problems stemming from the Syrian civil war. The Turkish state, Caner Bakir argues, responded well to limit the public health effects of the COVID-19 pandemic. He argues that ‘presidentialisation’ of executive, and the ‘presidential bureaucracy’ in Turkey’s were critical to the quick introduction of anti-COVID-19 policies which avoided being vetoed or watered down as would normally have occurred in a parliamentary system of government. In normal times these features of Turkey’s impositional and exclusive policy style pose risks of policy design and implementation failures when policy problems are poorly diagnosed, policy solutions are wrong, and/or complementary policy instrument mixes are implemented ineffectively. However, the Turkish style excels when a policy issue is esoteric (i.e., technical, scientific, and expert-led) and framed as an existential crisis under high uncertainty that requires expert-led, inclusive, quick and decisive responses to policy problems.
Another country which was wary of the pandemic from the start due to past experiences with other kinds of crises and emergencies, was Israel. In their article Moshe Maor, Raanan Sulitzeanu-Kenan and David Chinitz describe the efforts made by the Israeli government to contain the spread of COVID-19, which were implemented amidst a constitutional crisis and a yearlong electoral impasse under the leadership of Prime Minister Benjamin Netanyahu, who was awaiting trial for charges of fraud, bribery, and breach of trust. Their chapter draws on the disproportionate policy perspective to ascertain the ideas and sensitivities that placed key national COVID-19 policy responses on trajectories which prioritized differential policy responses over general, nation-wide solutions, even though data in the public domain supported the selection of less severe policy solutions based on epidemiological or social welfare grounds. They argue that during the crisis Netanyahu enjoyed wide political leeway to employ disproportionate policy responses, and the general public exhibited a willingness to tolerate this.
In the final two papers, the experiences of two states with worse outcomes – the US and Sweden – are examined. As Daniel Beland, Philip Rocco and Alex Wadden argue, in the US case, as in Canada, federalism played a foundational role in structuring how the United States responded to the COVID-19 pandemic. As in prior crises, state governments were expected to be the primary sites of governing authority, especially with regard to immediate public-health needs, while the federal government was expected to supply critical counter-cyclical measures to stabilize the economy and make up for major revenue shortfalls in the states. Yet while the US response to COVID-19 roughly followed this pattern, the expectations of an efficient and effective response were not fulfilled (Kettl, 2020). Evidence on the US response to COVID-19 to date suggests the need for major revisions in the architecture of both public health systems and intergovernmental fiscal policy.
Finally, in Sweden, Jon Pierre notes that the key objective in fighting the COVID-19 pandemic was to alter social behavior in order to minimize inter-personal contact and thereby reduce the spread of the virus. While changing social behavior in some countries required coercive and thoroughly enforced rules and regulations, in other countries, this could be accomplished with more subtle signaling from government. In both these aspects of containment – the strategic objectives and the selection of instruments to alter social behavior – Sweden stood out from the majority of countries as its containment strategy was not centered around a complete lockdown but rather included more selective measures such as minimizing people’s visits to areas where a high density of people could be expected. Government agencies preferred to issue recommendations and advice on the appropriate social behavior rather than enact legislation or coercive regulations. While these aspects of the Swedish approach triggered the most international curiosity and their effectiveness to date remains uncertain, other relevant aspects like the unpreparedness of local governments and the problems of coordinating a highly decentralized healthcare system have been less often noted but also played an important role in determining the outcome of Sweden’s late and weak response to the COVID-19 crisis.
Giliberto Capano is Professor of Public Policy at the University of Bologna, Italy. He specializes in public administration, public policy analysis, and comparative higher education. His research focuses on governance dynamics and performance in higher education and education, policy design and policy change, policy instruments’ impact, the social role of political science, and leadership as an embedded function of policy making.
Michael Howlett is Burnaby Mountain Professor and Canada Research Chair at Simon Fraser University in Vancouver, Canada. He specializes in policy analysis and studies of policy design and policy tool use.
Darryl S.L. Jarvis is Professor in the Department of Asian and Policy Studies at the Education University of Hong Kong. His research focuses on comparative political economy and comparative public policy.
M. Ramesh is Professor and UNESCO Chair of Social Policy Design in Asia at the Lee Kuan Yew School of Public Policy, National University of Singapore.
Nihit Goyal is a postdoctoral fellow at the Yale-NUS College in Singapore. His research interests lie in comparative public policy, the use of data science, and the energy transition.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Adam, D. (2020, April 2). Special report: The simulations driving the world’s response to COVID-19. How epidemiologists rushed to model the coronavirus pandemic. Nature, 580(7803), 316–318. Retrieved from https://www.nature.com/articles/d41586-020-01003-6 [DOI] [PubMed] [Google Scholar]
- Amante, A. (2020, June 8). Over half of people tested in Italy’s Bergamo have COVID-19 antibodies. Reuters. Retrieved from https://www.reuters.com/article/us-health-coronavirus-italy-antibodies/over-half-of-people-tested-in-italian-city-of-bergamo-have-covid-19-antibodies-idUSKBN23F2JV
- Attwell, K., & Navin, M. C. (2019, December). Childhood vaccination mandates: Scope, sanctions, severity, selectivity, and salience. The Milbank Quarterly, 97(4), 978–1014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bach, T., & Wegrich, K. (eds). (2019). The blind spots of public bureaucracy and the politics of non‐coordination. London: Palgrave Macmillan. [Google Scholar]
- Blavatnik School of Government . (2020). Coronavirus government response tracker, 2020. Retrieved from https://www.bsg.ox.ac.uk/research/research-projects/coronavirus-government-response-tracker
- Blei, D. M., Ng, A. Y., & Jordan, M. I. (2003, January). Latent dirichlet allocation. Journal of Machine Learning Research, 3, 993–1022. [Google Scholar]
- Boin, A., T’ Hart, P., & Kuipers, S. (2018). The crisis approach. In H. Rodríguez, W. Donner, & J. E. Trainor (Eds.), Handbook of disaster research (pp. 23–38). Cham: Springer International Publishing. [Google Scholar]
- Boin, A. (2019, January). The transboundary crisis: Why we are unprepared and the road ahead. Journal of Contingencies and Crisis Management, 27(1), 94–99. [Google Scholar]
- Boin, A., ‘T Hart, P., Stern, E., & Sundelius, B. (2016). The politics of crisis management: Public leadership under pressure (2nded.). Cambridge: Cambridge University Press. [Google Scholar]
- Capano, G. (2018). Policy design spaces in reforming governance in higher education: The dynamics in Italy and The Netherlands. Higher Education, 75(4), 675–694. [Google Scholar]
- Capano, G., & Lippi, A. (2017). How policy instruments are chosen: Patterns of decision makers’ choices. Policy Sciences, 50(2), 269–293. [Google Scholar]
- Capano, G., Pritoni, A., & Vicentini, G. (2019, March 5). Do Policy instruments matter? Governments’ choice of policy mix and higher education performance in Western Europe. Journal of Public Policy, 1–27. doi: 10.1017/S0143814X19000047 [DOI] [Google Scholar]
- CDC . (2020, February 11). Information for clinicians on investigational therapeutics for patients with COVID-19. Centers for Disease Control and Prevention. Retrieved from https://www.cdc.gov/coronavirus/2019-ncov/hcp/therapeutic-options.html [Google Scholar]
- Cheng, C., Barceló, J., Hartnett, A., Kubinec, R., & Messerschmidt, L.. 2020. COVID-19 government response event dataset (CoronaNet v1.0). Retrieved from https://www.coronanet-project.org. [DOI] [PubMed]
- Chopera, D. (2020, March 24). Can Africa withstand COVID-19? | By Denis Chopera. Project Syndicate. Retrieved from https://www.project-syndicate.org/commentary/africa-covid19-advantages-disadvantages-by-denis-chopera-2020-03-2020-03.
- Dong, E., Du, H., & Gardner, L. (2020). An interactive web-based dashboard to track COVID-19 in real time. Lancet Infectious Diseases, 20(5), 533–534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunlop, C. A. (2009). Policy transfer as learning: Capturing variation in what decision-makers learn from epistemic communities. Policy Studies, 30(3), 289–311. [Google Scholar]
- El Sahly, H. M. (2020). Clinical outcomes of patients with COVID-19 pneumonia in intensive care in Lombardy. Retrieved from https://www.jwatch.org/na51334/2020/04/14/clinical-outcomes-patients-with-covid-19-pneumonia.
- Ferguson, N, D Laydon, G Nedjati Gilani, N Imai, K Ainslie, M Baguelin, S Bhatia, et al. “Report 9: Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand.” Imperial College London, March 16, 2020. 10.25561/77482 [DOI] [Google Scholar]
- Ferguson, N., Laydon, D., Nedjati Gilani, G., Imai, N., Ainslie, K., Baguelin, M., … & Dighe, A. (2020, March 16). Report 9: Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand. London: Imperial College. doi: 10.25561/77482 [DOI] [Google Scholar]
- Flaxman, S., Mishra, S., Axel Gandy, H., Unwin, J. T., Mellan, T. A., Coupland, H., … & Monod, M. (2020, June 8). Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature, 1–8. doi: 10.1038/s41586-020-2405-7 [DOI] [PubMed] [Google Scholar]
- Fong, M. W., Huizhi Gao, J. Y., Wong, J. X., Eunice, Y. C., Shiu, S. R., & Cowling, B. J. (2020, May). Nonpharmaceutical measures for pandemic influenza in nonhealthcare settings—Social distancing measures. Emerging Infectious Diseases Journal - CDC, 26(5), 976–984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- George, B., Verschuere, B., Wayenberg, E., & Zaki, B. L. (2020). A guide to benchmarking COVID-19 performance data. Public Administration Review. doi: 10.1111/puar.13255 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gleeson, D., Legge, D., O’Neill, D., & Pfeffer, M. (2011, June). Negotiating tensions in developing organizational policy capacity: Comparative lessons to be drawn. Journal of Comparative Policy Analysis: Research and Practice, 13(3), 237–263. [Google Scholar]
- Gleeson, D. H., Legge, D. G., & O’Neill, D. (2009, February). Evaluating health policy capacity: Learning from international and Australian experience. Australia and New Zealand Health Policy, 6(1), 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grødem, A. S., & Hippe, J. M. (2019, October). The expertise of politicians and their role in epistemic communities. Policy & Politics, 47(4), 561–577. [Google Scholar]
- Haas, P. M. (1992). Introduction: Epistemic communities and international policy coordination. International Organization, 46(1), 1–36. [Google Scholar]
- Hale, T., Petherick, A., Phillips, T., & Webster, S. (2020, April 7). Variation in government responses to COVID-19ʹ version 4.0. Blavatnik School of Government Working Paper. Retrieved from http://www.bsg.ox.ac.uk/covidtracker
- Hood, C. (1986). The tools of government. Chatham: Chatham House Publishers. [Google Scholar]
- Hood, C., Jennings, W., & Copeland, P. (2016, June). Blame avoidance in comparative perspective: Reactivity, staged retreat and efficacy. Public Administration, 94(2), 542–562. [Google Scholar]
- Howlett, M. (2019). The temporal dimension(s) of policy designs: Resilience, robustness and the sequencing of tools in policy mixes. International Review of Public Policy, 1(1), 27–45. [Google Scholar]
- Howlett, M. (2019a). Designing public policies: Principles and instruments (2nded.). London: Routledge. [Google Scholar]
- Howlett, M. (2019b). The policy design primer: Choosing the right tool for the job. New York: Routledge. [Google Scholar]
- Howlett, M., & del Rio P. (2015). The parameters of policy portfolios: Verticality and horizontality in design spaces and their consequences for policy mix formulation. Environment and Planning C, 33(5), 1233–1245. [Google Scholar]
- Howlett, M., & Tosun, J. (eds). (2019). Policy styles and policy-making: Exploring the linkages. London: Routledge. [Google Scholar]
- Hsiang, S., Allen, D., Annan-Phan, S., Bell, K., Bolliger, I., Chong, T., … Lau, P. (2020, June 8). The effect of large-scale anti-contagion policies on the COVID-19 pandemic. Nature. doi: 10.1038/s41586-020-2404-8 [DOI] [PubMed] [Google Scholar]
- Huang, I. Y.-F. (2020). Fighting against COVID-19 through government initiatives and collaborative governance: Taiwan experience. Public Administration Review. doi: 10.1111/puar.13239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson, T., Dawes, C., Fowler, J., & Smirnov, O. (2020, April 24). Slowing COVID-19 transmission as a social dilemma: Lessons for government officials from interdisciplinary research on cooperation. Journal of Behavioral Public Administration, 3(1). doi: 10.30636/jbpa.31.150 [DOI] [Google Scholar]
- Kehinde, B. (2014, January 1). Applicability of risk transfer tools to manage loss and damage from slow-onset climatic risks. Procedia economics and finance, 4th international conference on building resilience, incorporating the 3rd annual conference of the ANDROID disaster resilience network, 8–11th September 2014 (Vol. 18, pp. 710–717). Salford Quays, UK. [Google Scholar]
- Kettl, D. F. (2020). States divided: The implications of American federalism for Covid-19. Public Administration Review. doi: 10.1111/puar.13243 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Knill, C., Schulze, K., & Tosun, J. (2012, December). Regulatory policy outputs and impacts: Exploring a complex relationship: Regulatory policy outputs and impacts. Regulation & Governance, 6(4), 427–444. [Google Scholar]
- Lai, A. Y.-H. (2018, October). Agility amid uncertainties: Evidence from 2009 A/H1N1 pandemics in Singapore and Taiwan. Policy and Society, 37(4), 459–472. [Google Scholar]
- Leong, C., & Howlett, M. (2017). On credit and blame: Disentangling the motivations of public policy decision-making behaviour. Policy Sciences, 50(4), 599–618. [Google Scholar]
- Mallapaty, S. (2020, March 26). What the cruise-ship outbreaks reveal about COVID-19. Nature, 580(7801), 18. Retrieved from https://www.nature.com/articles/d41586-020-00885-w [DOI] [PubMed] [Google Scholar]
- Manski, C. F. (2013). Public policy in an uncertain world: Analysis and decisions. Cambridge, MA: Harvard University Press. [Google Scholar]
- Maor, M. (2020, May 16). Policy over- and under-design: An information quality perspective. Policy Sciences. doi: 10.1007/s11077-020-09388-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maor, M., Tosun, J., & Jordan, A. (2017, November). Proportionate and disproportionate policy responses to climate change: Core concepts and empirical applications. Journal of Environmental Policy & Planning, 19(6), 599–611. [Google Scholar]
- McConnell, A., & Drennan, L. (2006). Mission impossible? Planning and preparing for crisis 1. Journal of Contingencies and Crisis Management, 14(2), 59–70. [Google Scholar]
- Michaud, J., Kates, J., & Levitt, L. (2020, April 16). COVID-19 models: Can they tell us what we want to know? Retrieved from https://www.kff.org/coronavirus-policy-watch/covid-19-models/
- Moon, M. J. (2020). Fighting against COVID-19 with agility, transparency, and participation: Wicked policy problems and new governance challenges. Public Administration Review. doi: 10.1111/puar.13214 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Moore, M. H. (1995). Creating public value: Strategic management in government. Cambridge: Harvard University Press. [Google Scholar]
- Nguyen, T. (Mae). (2020, June 4). Vietnam’s astonishing success at curbing COVID-19 outbreaks. The Regulatory Review. Retrieved from https://www.theregreview.org/2020/06/04/nguyen-vietnam-astonishing-success-curbing-covid-19-outbreaks/.
- Nowlin, M. C. (2016, August). Modeling issue definitions using quantitative text analysis: Nowlin: modeling issue definitions. Policy Studies Journal, 44(3), 309–331. [Google Scholar]
- OECD . (2020). OECD country policy tracker. Retrieved from https://www.oecd.org/coronavirus/en/
- Painter, M., & Pierre, J. (eds). (2005). Challenges to state policy capacity: Global trends and comparative perspectives. London: Palgrave Macmillan. [Google Scholar]
- Parker, R. W. (2020, June 9). Lessons from New Zealand’s COVID-19 success. The Regulatory Review. Retrieved from https://www.theregreview.org/2020/06/09/parker-lessons-new-zealand-covid-19-success/
- Payne, D. C., Smith-Jeffcoat, S. E., Nowak, G., Chukwuma, U., Geibe, J. R., Hawkins, R. J., Johnson, J. A., Thornburg, N.J, J Schiffer, J., Weiner, Z., Bankamp, B., Bowen, M.D., MacNei, A., Patel, M.R., and Deussing, R. (2020). SARS-CoV-2 infections And Serologic Responses From A Sample of U.S. navy service members — USS Theodore Roosevelt, April 2020. MMWR. Morbidity and Mortality Weekly Report, 69(23), 714–721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peters, B. G. (2018). Policy problems and policy design. Northampton, MA: Edward Elgar Pub. [Google Scholar]
- Peters, G. B. (2005). The Problem of Policy Problems. Journal of Comparative Policy Analysis: Research and Practice, 7(4), 349–370. [Google Scholar]
- R Core Team (2019). R: A language and environment for statistical computing. R Foundation for Statistical Computing: Vienna. https://www.R-project.org/. [Google Scholar]
- Rhodes, T., & Lancaster, K. (2020, May 13). Mathematical models as public troubles in COVID-19 infection control: Following the numbers. Health Sociology Review, 1–18. doi: 10.1080/14461242.2020.1764376 [DOI] [PubMed] [Google Scholar]
- Ritchie, H., Roser, M., Ortiz-Ospina, E., & Hasell, J. (2020). Policy responses to the coronavirus pandemic - Statistics and research. In E. Ortiz-Ospina & J. Hasell (Eds.), Our world in data. Retrieved from https://ourworldindata.org/policy-responses-covid [Google Scholar]
- Roberts, M. E., Stewart, B. M., & Tingley, D. (2014). stm: R package for structural topic models. Journal of Statistical Software, 10(2), 1–40. [Google Scholar]
- Russell, T. W., Hellewell, J., Jarvis, C. I., Van-Zandvoort, K., Abbott, S., Ratnayake, R., … Kucharski, A. J. (2020, March 8). Estimating the infection and case fatality ratio for COVID-19 using age-adjusted data from the outbreak on the diamond princess cruise ship. Epidemiology [Preprint]. doi: 10.1101/2020.03.05.20031773 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Salamon, L. M. (2002). The tools of government: A guide to the new governance. New York: Oxford University Press. [Google Scholar]
- Schaffrin, A., Sewerin, S., & Seubert, S. (2015, January). Toward a Comparative measure of climate policy output. Policy Studies Journal, 43(2), 257–282. [Google Scholar]
- Specktor, B. (2020, March 16). Coronavirus: What is ‘flattening the curve,’ and will it work? LiveScience. Retrieved from https://www.livescience.com/coronavirus-flatten-the-curve.html [Google Scholar]
- Staupe-Delgado, R. (2019, October). Progress, traditions and future directions in research on disasters involving slow-onset hazards. Disaster Prevention and Management: An International Journal, 28(5), 623–635. [Google Scholar]
- t’Hart, P., Heyse, L., & Boin, A. (2001). New trends in crisis management practice and crisis management research: Setting the agenda. Journal of Contingencies and Crisis Management, 9(4), 181–188. [Google Scholar]
- Taeihagh, A., Givoni, M., & René, B.-A. (2013). Which policy first? A network-centric approach for the analysis and ranking of policy measures. Environment and Planning B: Planning and Design, 40(4), 595–616. [Google Scholar]
- Toshkov, D., Yesilkagit, K., & Carroll, B. (2020). Government capacity, societal trust or party preferences? What accounts for the variety of national policy responses to the COVID-19 pandemic in Europe? Working Paper. The Netherlands: Institute of Public Administration, Faculty of Governance and Global Affairs, Leiden University. Retrieved from https://osf.io/7chpu/ [Google Scholar]
- Valdez, D., Pickett, A. C., & Goodson, P. (2018, November). Topic modeling: Latent semantic analysis for the social sciences: Topic modeling. Social Science Quarterly, 99(5), 1665–1679. [Google Scholar]
- Van Bavel, J. J., Boggio, P., Capraro, V., Cichocka, A., Cikara, M., Crockett, M., … & Drury, J. (2020, March 24). Using social and behavioural science to support COVID-19 pandemic response [Preprint]. PsyArXiv. doi: 10.31234/osf.io/y38m9 [DOI] [PubMed]
- Van Dooren, W. (2020). Staging science: Authoritativeness and fragility of models and measurement in the Covid-19 crisis. Public Administration Review. doi: 10.1111/puar.13219 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walker, R. M., Chandra, Y., Zhang, J., & Witteloostuijn, A. (2019, November). Topic modeling the research‐Practice gap in public administration. Public Administration Review, 79(6), 931–937. [Google Scholar]
- Walker, W. E., Marchau, V. A. W. J., & Kwakkel, J. H. (2013). Uncertainty in the framework of policy analysis. In W. A. H. Thissen & W. E. Walker (Eds.), Public policy analysis: New developments (pp. 215–260). New York: Springer. [Google Scholar]
- Weible, C. M., Nohrstedt, D., Cairney, P., Carter, D. P., Crow, D. A., Durnová, A. P., … Stone, D. (2020, June). COVID-19 and the policy sciences: Initial reactions and perspectives. Policy Sciences, 50, 1–17 [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Health Organization (WHO) . (2020a). Q&A on coronaviruses (COVID-19). Author. Retrieved from https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-coronaviruses [Google Scholar]
- World Health Organization (WHO) . 2020b. Coronavirus (COVID-19): Events as they happen. Author. Retrieved from https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen [Google Scholar]
- World Health Organization Writing Group . (2012. January). Nonpharmaceutical interventions for pandemic influenza, national and community measures. Emerging Infectious Diseases, 12(1), 88–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu, X., Ramesh, M., & Howlett, M. (2015, September). Policy capacity: A conceptual framework for understanding policy competences and capabilities. Policy and Society, 34(3–4), 165–171. [Google Scholar]
- Zito, A. R. (2018, January). Instrument constituencies and epistemic community theory. Policy and Society, 37(1), 36–58. [Google Scholar]