

Abstract
Recent findings suggest that the current COVID-19 pandemic has a potential negative impact in several areas of life, including sexual health. However, less is known about the psychological dimensions that may work as vulnerability/protective factors for the development of sexual problems in the current pandemic. The current study used a longitudinal design to examine the role played by personality trait factors (neuroticism, extraversion) as well as psychosexual factors (sexual beliefs) in predicting sexual functioning and sexual distress across time during the current pandemic crisis. A total of 528 individuals (337 women) completed a web survey assessing sexual health indicators and psychological factors. The first wave was conducted during the confinement period in Portugal (N = 528) between May and June 2020 and the second four months later (N = 146), when strict confinement rules were over. Generalized estimating equations (GEE) were used to examine the ability of psychological factors to predict sexual functioning and distress across time, while controlling for age and gender. Results indicated that sexual distress at time point 2 was lower than during confinement, and men had lower levels of sexual functioning post-confinement while no significant difference was observed for women. Moreover, higher levels of neuroticism and age-related beliefs significantly predicted lower sexual functioning as well as higher sexual distress, whereas lower levels of extraversion predicted lower sexual functioning after controlling for age and gender effects. Findings support the role of psychological vulnerability factors to predict sexual problems across time and may have important implications in the prevention and treatment of sexual dysfunctions.
Keywords: Sexual functioning, Sexual distress, Personality factors, Sexual beliefs, COVID-19 pandemic
Introduction
The context of COVID-19 and confinement measures has brought great (mental) health challenges. We have seen how such crisis scenario has negatively impacted individuals’ mental health conditions (e.g., Brooks et al., 2020; Rodríguez-Rey et al., 2020; Smith & Lim, 2020), corroborating previous evidence on the detrimental effects of crisis and social isolation in psychological and interpersonal adjustment (Roychowdhury, 2020). These effects seem to expand to the sexuality domain. Recent evidence suggested a relationship between confinement and impaired sexual functioning in women (Schiavi et al., 2020) or decreased sexual satisfaction in both men and women (Cocci et al., 2020; Yuksel & Ozgor, 2020). Sexual difficulties and sexual distress emerging during COVID-19 were deemed a result of the complex interplay between mental health conditions and relationship dynamics during lockdown (Pascoal et al., 2021). Indeed, lower psychological adjustment during lockdown was found to impact sexual functioning in men and women up and beyond the effects of confinement levels (Carvalho et al., 2021). Such evidence supports current pandemic as a crisis context shaping complex dynamics underpinning human sexual health. Accordingly, using COVID-19 confinement period as a frame to research psychological vulnerability factors for sexual dysfunction (sexual functioning and sexual distress) can be of great value.
Psychological Dimensions as Vulnerability Factors for Sexual (Dys)Function
In the last few decades, several studies have been investigating the role of psychological traits as predisposing and maintaining factors for sexual dysfunction in men and women. Among the hypothesized predisposing factors are general trait factors such as personality traits (Barlow, 2002; Nobre, 2017), as well as more specific (sexual) trait factors such as sexual beliefs (Nobre, 2017; Nobre & Pinto‐Gouveia, 2006) (see Brotto et al., 2016 for a review).
Personality traits are conceptualized as global predispositions, consistent across time, that are responsible for guiding human behavior (McCrae & Costa, 2004). Research using the Five Factor Model of Personality (Costa Jr & McCrae, 1992) has been consistently developed in the area of psychopathology, including sexual problems.
Barlow (2002) has proposed a triple vulnerability model for emotional disorders (including sexual dysfunction) where he hypothesized that neuroticism would play an important role in predicting anxiety related disorders. Findings on different emotional disorders seem to corroborate this hypothesis (Barlow et al., 2013; Zinbarg & Barlow, 1996). In line with these findings, research conducted in individuals with and without sexual dysfunction has indicated that neuroticism is significantly higher in clinical samples compared to sexually healthy samples (Costa Jr & McCrae, 1992; Eysenck, 1971; Fagan et al., 1991; Quinta Gomes & Nobre, 2011). More specifically, high neuroticism has been related to sexual performance anxiety and erectile dysfunction in men (Rosenheim & Neumann, 1981) and impaired global sexual functioning (Crisp et al., 2015), sexual arousal (Kennedy et al., 1999), and orgasmic difficulties in women (Harris et al., 2008; Kennedy et al., 1999). Additionally, regression analysis indicated neuroticism as the best predictor of sexual functioning in men (Quinta Gomes & Nobre, 2011). Finally, a study with non-heterosexual samples indicated that gay men and lesbian women with sexual problems scored higher on neuroticism compared to healthy controls (Peixoto & Nobre, 2014b).
Besides neuroticism, low extraversion has also been found to be associated with lower levels of sexual functioning, sexual desire, sexual arousal, orgasm, and sexual satisfaction in men and women (Costa Jr & McCrae, 1992; Crisp et al., 2015; Harris et al., 2008; Kennedy et al., 1999; Quinta Gomes & Nobre, 2011; Schenk et al., 1983). Moreover, lesbian women with sexual dysfunction reported lower levels of extraversion compared to sexually healthy controls (Peixoto & Nobre, 2014b).
These findings are also in line with research on depression and anxiety disorders suggesting that the considerable comorbidity between these clinical conditions is accounted for by common higher-order dimensions such as high neuroticism and low extraversion that work as global vulnerability traits for the development of emotional disorders (Barlow et al., 2013).
Besides personality traits, dysfunctional sexual beliefs have also been suggested as specific vulnerability factors for the development and maintenance of sexual problems. Zilbergeld (1999) listed a number of myths associated with unrealistic and highly demanding male sexual performance (e.g., “a man always wants and is ready to have sex,” “a real man is sexually functional”) that would predispose men to develop sexual difficulties (particularly erectile dysfunction). Additionally, Heiman and LoPiccolo (1988) proposed a set of myths typical of women with sexual dysfunction, including beliefs related to female sexual conservatism, as well as the role of age and physical appearance (“sex is only for younger women,” “women’s sexual life ends with menopause”).
Findings from cross-sectional studies have suggested that men and women with sexual dysfunction endorse significantly more dysfunctional sexual beliefs compared to controls. Women with sexual dysfunction endorse significantly more beliefs related to the role of age on female sexual functioning (e.g., after menopause women lose their sexual desire) and body image beliefs (e.g., women who are not physically attractive can’t be sexually satisfied) (Nobre & Pinto‐Gouveia, 2006). Moreover, when studying specific sexual dysfunctions, findings have shown that age-related beliefs were significantly more endorsed by women with low sexual desire and vaginismus, sexual conservative beliefs were more endorsed by women with vaginismus, and body image beliefs were more common in women with orgasmic disorders, compared to sexually healthy women (Borg et al., 2011; Nobre & Pinto-Gouveia, 2008). Studies with non-clinical samples have also shown an association between sexual beliefs and female sexual function. In particular, age-related beliefs and sexual conservative beliefs were significantly associated with lower levels of sexual functioning, lower sexual desire, and higher levels of sexual pain in women (Carvalho & Nobre, 2010; Morton & Gorzalka, 2013; Nimbi et al., 2019a, 2019b; Nobre, 2009; Pascoal et al., 2017).
Additionally, men with sexual dysfunction (e.g., low sexual desire, erectile dysfunction) reported higher concordance with male sexual beliefs, particularly related to performance demands (e.g., “macho” beliefs: “a real man is always ready for sex and must be capable of satisfying any partner”) or conservative beliefs (e.g., “there is only one acceptable way of having sex—missionary position,” “foreplay is a waste of time”) (Baker & Silva, 1988; Beckwith et al., 2009; Nimbi et al., 2018, 2019a, 2019b; Peixoto & Nobre, 2014a). Also, men who endorse more dysfunctional sexual beliefs (e.g., sexual conservatism, macho beliefs) tend to present with lower levels of sexual functioning (Carvalho & Nobre, 2011; Dang & Gorzalka, 2015; Nimbi et al., 2018, 2019a, 2019b; Nobre, 2010; Pascoal et al., 2017) (see Moura et al., 2021).
Based on cognitive theories of psychopathology (e.g., Beck, 1996), as well as findings from previous research above described, Nobre (2009, 2010, 2017) has proposed a conceptual model to explain sexual dysfunctions in men and women. In this model, personality traits such as neuroticism as well as sexual beliefs play an important role as vulnerability factors for the development and maintenance of sexual dysfunction. Personality traits are conceptualized as global (transdiagnostic) factors and sexual beliefs as specific factors.
So far, partial evidence for the role of these vulnerability factors is based only on cross-sectional studies. There are yet no studies of longitudinal nature that could test the ability of such trait dimensions to predict sexual problems or sexual distress across time. Also, there are no studies that test the ability of specific vulnerability factors (sexual beliefs) to predict sexual problems after controlling for more global factors (e.g., neuroticism, low extraversion).
The COVID-19 Pandemic Crisis as a Stressor
The current COVID-19 pandemic, with all its associated biopsychosocial implications (e.g., confinements, restrictions to social interaction, major health concerns, concerns related to safe sexual interactions, concerns related to finances, new family dynamics and roles, etc.), constitutes a major long-term stressor with increased potential to work as precipitant factor for the development of sexual problems and sexual distress in both men and women. Therefore, using the current pandemic context to further examine the role played by trait psychological dimensions as vulnerability/protective factors for developing/worsening sexual difficulties across time constitutes an opportunity to bring new insights into our knowledge of the mechanisms involved in sexual problems, but more importantly, may also contribute for refining interventions to prevent them and promote sexual health and well-being.
The current longitudinal study is the first ever conducted to examine the role of psychological factors (neuroticism, extraversion, sexual beliefs) on the development of subsequent sexual difficulties and sexual distress in a sample of men and women, during an extremely critical life period (COVID-19 pandemic and its associated implications).
Based on existing theoretical models of sexual dysfunction (Nobre, 2017) as well as previous findings from cross-sectional studies, we expect that personality factors (neuroticism, low extraversion) as well as dysfunctional sexual beliefs (typical male and female conservative sexual beliefs, age-related beliefs, and “macho beliefs”) measured at time point 1 (i.e., confinement period) predict lower levels of sexual functioning and higher levels of sexual distress across time (at time point 1 and time point 2–4 months later, i.e., post-confinement period). We also predict that these effects are statistically significant after controlling for important demographic factors (age) and that the pattern is similar in men and women in regards to personality factors (no significant interactions between personality factors and gender), but not in regards to sexual beliefs (although there are no previous studies on the association between typically female and male beliefs and sexual health indicators on the opposite gender, we expect to find some gender specificity on the effect of sexual beliefs). Moreover, we expect sexual beliefs to predict sexual functioning and sexual distress across time (at time point 1 and time point 2) after controlling for personality factors.
Method
Participants
Participants were recruited online from May to October 2020. Inclusion criteria for eligible participants were: (1) age over 18; (2) able to read and write in Portuguese; (3) access to a personal email account. For the current analysis, additional inclusion criteria included the completion of the second wave of the survey 4 months later. The final sample comprised 528 individuals who ranged in age from 18 to 76 years old (women: M = 34.3, SD = 10.48; men: M = 41.9, SD = 12.57). One hundred and forty-six participants completed the second survey. Although the study was advertised as inclusive of couples of all genders and identities, most participants were cisgender (except 3) and heterosexual (75%). Sociodemographic characteristics of the sample are included in Table 1.
Table 1.
Sociodemographic Characteristics (N = 528)
| Men (n = 188) | Women (n = 337) | |||
|---|---|---|---|---|
| M | SD | M | SD | |
| Age | 41.9 (18–76) | 12.57 | 34.3 (18–73) | 10.48 |
| n | % | n | % | |
| Sexual orientation | ||||
| Exclusively heterosexual | 145 | 77.1 | 249 | 73.9 |
| Mostly heterosexual | 11 | 5.9 | 65 | 19.3 |
| Bisexual | 5 | 2.6 | 17 | 5.0 |
| Mostly gay/lesbian | 9 | 4.8 | 2 | .6 |
| Exclusively gay/lesbian | 18 | 9.6 | 4 | 1.2 |
| Marital status | ||||
| Single | 42 | 22.3 | 151 | 44.8 |
| Living together | 42 | 22.3 | 88 | 26.1 |
| Married | 85 | 45.2 | 78 | 23.1 |
| Divorced | 19 | 10.1 | 18 | 5.3 |
| Widowed | – | – | 2 | .6 |
| Professional status | ||||
| Student | 17 | 9.0 | 56 | 16.6 |
| Employed | 140 | 74.5 | 520 | 65.3 |
| Unemployed | 12 | 6.4 | 30 | 8.9 |
| Layoff | 12 | 6.4 | 30 | 8.9 |
| Retired | 7 | 3.7 | 1 | .3 |
| School education | ||||
| 4 years (1st cycle) | 1 | .5 | – | – |
| 6 years (2nd cycle) | 1 | .5 | – | – |
| 9 years (3rd cycle) | 3 | 1.6 | – | – |
| 12 years (high school) | 45 | 23.9 | 33 | 9.8 |
| Graduation (university degree) | 128 | 68.1 | 281 | 83.4 |
| PhD degree | 10 | 5.3 | 23 | 6.8 |
Procedure
The research protocol of this study was approved by the Ethical Committee of the authors’ university and was part of a larger project aimed at assessing sexual health during COVID-19 pandemic in Portugal. All respondents provided written informed consent prior to participating. Participants were recruited through advertisement using various online networks of both authors’ research group and Portuguese national public agencies/institutions who collaborated in the dissemination of the study (e.g., Portuguese College of Psychologists, national media). Recruitment materials disclosed the study purpose as “to assess sexual health during the COVID-19 pandemic,” asked for participation of individuals who met the described inclusion criteria, and included a link to the online questionnaire. Once participants accessed the link of the online questionnaire, they read a detailed information sheet providing information on the study aim and procedures, which included an informed consent form. After this step, and having agreed to these terms, participants had access to the survey questions. At the end of the first survey, participants could indicate their interest in participating in a second wave of the survey by accessing a separate page in which they wrote their e-mail address. Only interested participants were contacted for the second survey. Respondents’ answers to both surveys were linked using an individual identifying code. Participation in the present study was voluntary and no compensation was provided. The survey took an average of 30 min to complete.
Individuals completed the first survey between May 8 and June 18, 2020, a period of strict government-imposed measures due to the COVID-19 pandemic (i.e., the “emergency” confinement in Portugal occurred from March 18 until June 1 and included restrictions such as stay at home/work from home measures, restrictions to circulation, and closing of facilities other than essential services, including schools). Individuals completed the follow-up survey 4 months later, between September 24 and October 28, 2020, a period of less strict social distancing measures. All surveys were completed online using an open-source online survey application (https://www.limesurvey.org/). Data confidentiality and anonymity were guaranteed since no personal information that could identify the respondents was collected and their IP addresses were not recorded. After completion of the study, individuals received a list of resources related to sexual health to which they could refer to if needed.
Measures
Sociodemographic Characteristics
Participants reported on relevant sociodemographic information (e.g., age, sex, gender, marital status, education, professional status) in the baseline survey.
Personality Traits
The Big Five Inventory (BFI; John & Srivastava, 1999; John et al., 1991) is a brief, well-validated, and widely used self-report measure that assesses the dimensions of the Five-Factor Model of personality as proposed by McCrae and Costa (2004). For the purpose of this study, participants reported only on the Extraversion and Neuroticism dimensions, which have shown the strongest links to sexual dimensions, including sexual dysfunction (e.g., Quinta Gomes & Nobre, 2011). Respondents are asked to indicate their level of agreement with short statements (e.g., “I’m emotionally stable, not easily upset,” reversed) in a 5-point rating scale (1 = disagree strongly to 5 = agree strongly). The Portuguese version of the questionnaire presents good psychometric properties (Brito-Costa et al., 2015). In the current sample, the instrument showed good internal consistency for both dimensions (αExtraversion = .80, αNeuroticism = .84).
Sexual Beliefs
The Sexual Dysfunctional Beliefs Questionnaire (SDBQ; Nobre et al., 2003) is a self-report instrument that assesses a series of sexual beliefs and stereotypes considered as predisposing factors to the development of sexual dysfunction. The SDBQ assesses a range of sexual beliefs but, for the purpose of this study, participants reported only on sexual beliefs dimensions shown to be more strongly implicated in sexual (dys)function (Nobre & Pinto-Gouveia, 2006, 2008): sexual conservatism (e.g., “Masturbation is wrong and sinful”); female age-related beliefs (e.g., “As women age the pleasure they get from sex decreases”); male sexual conservative beliefs (e.g., “There is only one acceptable way of having sex—missionary position”) and ‘macho’ beliefs (e.g., “A man must be capable of maintaining an erection until the end of any sex”). Participants indicate their level of agreement with each specific item in a 5-point rating scale (1 = completely disagree to 5 = completely agree). This measure has demonstrated good psychometric properties and the capacity to discriminate between a clinical and a community group without sexual dysfunctions (Nobre et al., 2003). In the present sample, all factors presented adequate internal consistency (Cronbach α range = .71 to .73).
Sexual Distress
The well-validated Female Sexual Distress Scale-Revised (FSDS-R) (Derogatis et al., 2002) is a self-report measure that measures the distress associated with one’s sexual life in the previous month. The FSDS-R comprises 13-items rated on 5-point rating scales (e.g., “How often did you feel distressed about your sex life?” 0 = never to 4 = always). Total scores range from 0 to 52. Higher scores denote higher sexual distress; clinically significant distress associated with sexual problems is considered with a total score greater than 15 (Derogatis et al., 2002). The FSDS has demonstrated good psychometric properties (Derogatis et al., 2002) and showed excellent internal consistency in the current sample (α = .93).
Sexual Functioning
Participants’ sexual functioning was assessed using the Portuguese versions of the well-validated International Index of Erectile Function (IIEF; Quinta Gomes & Nobre, 2012; Rosen et al., 1997) and Female Sexual Functioning Index (FSFI; Pechorro et al., 2009; Rosen et al., 2000). The IIEF is a 15-item self-report measure assessing men’s sexual functioning across five domains (sexual desire, erectile function, orgasmic function, intercourse satisfaction, and overall satisfaction); total scores range from 5 to 75 with higher scores indicating better men’s sexual function. The FSFI is a 19-item self-report measure assessing women’s sexual functioning across six domains (desire, arousal, lubrication, orgasm, satisfaction, and pain); total scores range from 2 to 36 with higher scores indicating better women’s sexual function. Thirty participants did not report any sexual activity in the 4 weeks prior to the first survey time point, and 23 to the second time point, precluding the calculation of interpretable FSFI and IIEF total scores (e.g., Meyer-Bahlburg & Dolezal, 2007). In the current study, both measures demonstrated excellent internal consistency (αIIEF = .95; αFSFI = .96).
Statistical Analysis
Firstly, as with all longitudinal data, sample attrition was a concern. At time 1, there were minimal missing data for all variables (0.2%), except for sexual functioning (6.0%). However, the attrition rate between time points 1 and 2 was high (74.6%). Overall, just 19.75% of our sample had complete data at both time points. Visual analysis of missing data suggested Missing Completely At Random (MCAR) and, therefore, were kept for subsequent analyses (Hedecker & Gibbons, 2006).
Secondly, mean, standard deviation and range (minimum and maximum) scores for each measure were calculated for both assessment moments. Prior to statistical analysis, the total scores of the scales of sexual functioning of men and women (IIEF and FSFI) were both normalized linearly in the interval [0,1] based on the following formula f (x) = (x-Min) / (Max–Min) as they have different score range.
Finally, as MCAR held, generalized estimating equations (GEE), which are considered an unbiased approach (Heitjan, 1997), were used to examine how a set of 9 variables (sociodemographic: age (control) and gender; personality traits: neuroticism and extraversion, sexual beliefs: female conservatism, female age-related beliefs, male conservatism and “macho” beliefs; and moment: during the first lockdown and 4 months later after lockdown during COVID-19 pandemic) can predict sexual functioning and sexual distress. The moderating effect of gender was also examined for all predictors except age. GEE are a multivariate generalization of quasi-likelihood estimation that allows to specify a model for the mean and variance for each measurement, without requiring knowledge of the distribution of the measurements (Agresti, 2002). The GEE presents some advantages in comparison to the traditional repeated-measures ANOVA approach, as:(1) it presents more robustness in parameter estimation in within-subject designs; (2) it needs no imputation method; and (3) does not require the outcome variable to have a particular distribution (Rosa et al., 2019; Ziegler, 2011). A linear scale response (normal distribution with identity link function) was chosen. An exchangeable working correlation structure was used to obtain the robust sandwich variance estimates of the regression coefficients in the GEE models. This type of working correlation structure was preferred as the Correct Quasi-likelihood under the Independence model Criterion (CQIC) presented the lowest value (Cui & Qian, 2007; Rosa et al., 2019). Indicator variable coding, also known as dummy coding, was applied to our categorical predictors (sex and moment). The Wald test was used for inference. Pairwise comparisons of the predicted marginal means were used to examine the statistical significance of changes in the outcomes (sexual functioning and sexual distress) for the categorical predictors only. All p values correspond to two-sided tests, with a level of significance of 5%. All statistical procedures were performed with IBM SPSS v.26 (SPSS Inc., Chicago, IL, USA).
Results
Descriptive statistics (mean, and standard deviation) were examined for each psychological predictors and outcomes used in the analysis in both time points (see Table 2).
Table 2.
Means and SDs for predictor and outcome variables (N = 528)
| Variables | M | SD |
|---|---|---|
| Personality | ||
| Neuroticism | 22.40 | 6.60 |
| Extraversion | 27.18 | 5.90 |
| Sexual beliefs | ||
| Female sexual conservatism | 10.50 | 2.29 |
| Female age-related beliefs | 5.97 | 2.45 |
| Male sexual conservatism | 9.64 | 1.47 |
| Macho beliefs | 7.05 | 2.94 |
| Sexual functioning | ||
| FSFI (T1) | 29.20 | 4.49 |
| FSFI (T2) | 28.80 | 4.89 |
| IIEF (T1) | 64.70 | 8.50 |
| IIEF (T2) | 63.80 | 10.10 |
| Sexual distress (T1) | 11.60 | 9.78 |
| Sexual distress (T2) | 11.00 | 10.20 |
FSFI Female Sexual Function Inventory, IIEF International Index of Sexual Function
Table 3 shows the inter-correlations between all the predictors and the levels of sexual functioning and sexual distress measured at both time points. Results indicated that, with a few exceptions, all psychological predictors are significantly associated with sexual functioning and sexual distress measured at both time points (small to medium effect sizes).
Table 3.
Pearson correlations for predictor and outcome variables (N = 528)
| Predictors | Outcomes at T1 | Outcomes at T2 | ||
|---|---|---|---|---|
| Sexual functioningª | Distress | Sexual functioningª | Distress | |
| Age | .001 | − .048 | .069 | − .003 |
| Personality | ||||
| Neuroticism | − .327** | .330** | − .281** | .227** |
| Extraversion | .211** | − .166** | .056 | − .006 |
| Sexual beliefs | ||||
| Female sexual conservatism | − .202** | .178** | − .345** | .203* |
| Female age-related beliefs | − .240** | .275** | − .295** | .271** |
| Male sexual conservatism | − .147** | .164** | − .458** | .387** |
| Macho beliefs | − .037 | .100* | − .293** | .349** |
aIn order to be comparable, the scales of sexual functioning for men (IIEF) and women (FSFI) were normalized linearly in the interval [0,1]; *p < .05, **p < .01
Prediction of Sexual Functioning and Sexual Distress
The GEE analyses revealed that age (B = − 0.01, Wald’s χ2(1) = 6.11, p = .013), neuroticism (B = − 0.01, Wald’s χ2(1) = 24.21, p < .001), extraversion (B = − 0.01, Wald’s χ2(1) = 8.07, p = .005), and female age-related beliefs (B = − 0.02, Wald’s χ2(1) = 13.73, p < .001) are significant predictors of sexual functioning as shown in Table 4.
Table 4.
Results of GEE models to the data (N = 528)
| Sexual functioning | Sexual distress | |||||
|---|---|---|---|---|---|---|
| B | Wald test (df) | p | B | Wald test (df) | p | |
| Intercept | 1.05 | 180.29(1) | < .001 | − 11.01 | 3.57(1) | .059 |
| Sociodemographic factors | ||||||
| Age (control) | − 0.01 | 6.11(1) | .013 | 0.04 | 1.33(1) | .249 |
| Gendera | 0.05 | 0.12(1) | .734 | 9.21 | 9.21(1) | .254 |
| Personality traits | ||||||
| Neuroticism | − 0.01 | 24.21(1) | < .001 | 0.44 | 28.97(1) | < .001 |
| Extraversion | 0,01 | 8.07(1) | .005 | − 0.03 | 0.20(1) | .652 |
| Sexual beliefs | ||||||
| Female sexual conservatism | − 0.01 | 2.81(1) | .093 | 0.34 | 0.91(1) | .340 |
| Female age-related beliefs | − 0.02 | 13.73(1) | < .001 | 0.87 | 12.23(1) | < .001 |
| Male sexual conservatism | 0.00 | 0.02(1) | .882 | 0.53 | 0.71(1) | .400 |
| “Macho” beliefs | 0.00 | 0.16(1) | .678 | − 0.27 | 1.21(1) | .270 |
| Momentb | 0.01 | 0.59(1) | .443 | − 2.10 | 6.75(1) | .009 |
| Interaction effects | 0.00 | 0.50(1) | .479 | |||
| Gender * Neuroticisma | 0.00 | 0.09(1) | .754 | − 0.10 | 0.56(1) | .545 |
| Gender * Extraversiona | 0.00 | 0.50(1) | .479 | − 0.17 | 1.43(1) | .233 |
| Gender * Female conservatisma | 0.01 | 0.40(1) | .535 | − 0.70 | 1.94(1) | .164 |
| Gender * Female age beliefsa | 0.02 | 3.37(1) | .053 | − 0.17 | 0.14(1) | .706 |
| Gender * Male conservatisma | − 0.02 | 2.60(1) | .106 | 0.50 | 0.37(1) | .542 |
| Gender * Macho beliefsa | 0.00 | 0.23(1) | .668 | 0.27 | 0.59(1) | .444 |
| Gender * momenta, b | − 0.08 | 4.24(1) | .026 | 2.05 | 1.56(1) | .211 |
| Scale parameter Φ | 0.28 | 82.77 | ||||
aWomen as reference category, b moment 1 as reference category
df degrees of freedom
An interaction effect between gender and moment was found and the simple effects based on predicted marginal means were examined. As depicted in Fig. 1, significant decrease on sexual functioning across time was found in men (Wald’s χ2(1) = 2.10, p = .036), but no significant differences on sexual functioning between the two moments were found in women (Wald’s χ2(1) = 0.77, p = .443). No other significant effects were found.
Fig. 1.
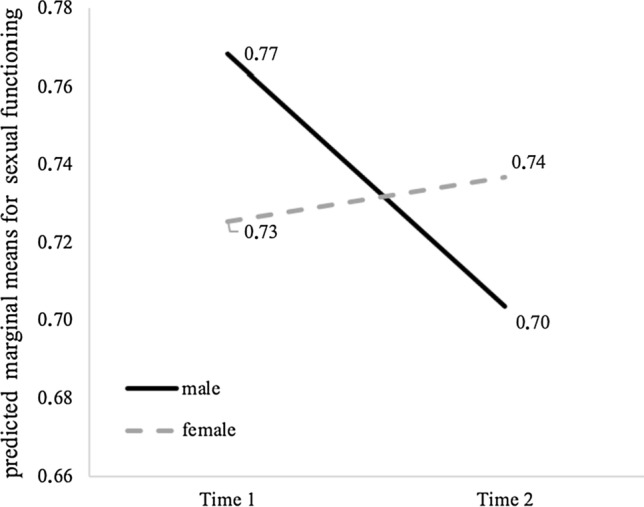
Predicted marginal means of sexual functioning according to gender and time. Note Time 1 was collected between May and June 2020 and time 2 between September and October 2020
Concerning sexual distress, results also showed that neuroticism (B = 0.44, Wald’s χ2(1) = 28.97, p < .001) and female age-related beliefs (B = 0.87, Wald’s χ2(1) = 12.23, p < .001) were significant predictors. Interestingly, moment was found to be a significant predictor (B = − 2.10, Wald’s χ2 (1) = 6.75, p = .009). The predicted marginal means indicated that the sexual distress was lower after lockdown (M = 10.12) than during the first lockdown (M = 11.67) as shown in Fig. 2. No other significant effects were found.
Fig. 2.
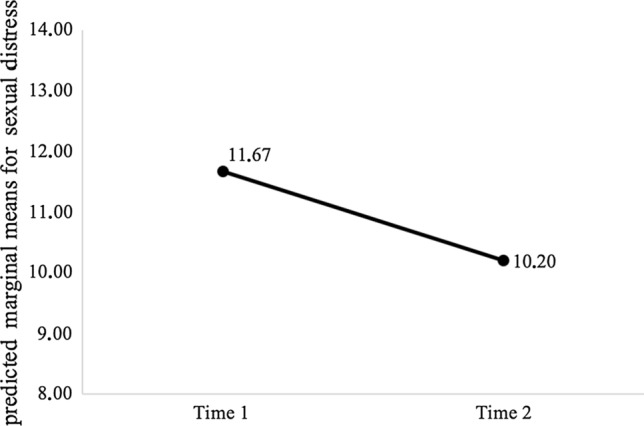
Predicted marginal means of sexual distress across time. Note Time 1 was collected between May and June 2020 and time 2 between September and October 2020
Discussion
The current study was aimed at researching the ability of global (personality) and specific (sexual beliefs) psychological vulnerability factors to predict sexual functioning and distress during the crisis context of COVID-19. Results have indicated that personality traits as well as sexual beliefs predict sexual function and sexual distress in men and women regardless of age and gender.
Regarding global trait factors (personality), results indicated that higher levels of neuroticism (measured at time point 1) significantly predicted lower sexual functioning as well as higher sexual distress, whereas lower levels of extraversion (measured at time point 1) significantly predicted lower sexual functioning, after controlling for age effects. Likewise, no interaction effects were found regarding gender, suggesting that global vulnerability factors act similarly across men and women. In line with our hypothesis on neuroticism, findings supported the role of this personality trait predicting sexual functioning and sexual distress during a long-term stressor such as the current pandemic crisis. This finding is further consistent with previous cross-sectional studies that indicated higher levels of neuroticism in men and women with sexual dysfunction compared with sexually healthy individuals (Costa et al., 1992; Crisp et al., 2015; Eysenck, 1971; Fagan et al., 1991; Peixoto & Nobre, 2014b; Quinta Gomes & Nobre, 2011; Rosenheim & Neumann, 1981). As for extraversion, findings partially supported our hypothesis, as this trait did not predict sexual distress. A recent meta-analysis investigating the role of personality factors on sexual health indicated that extraversion was positively related to sexual activity and negatively related to symptoms of sexual dysfunction (Allen & Walter, 2018). In fact, most studies on the association between extraversion and sexual health use measures of sexual functioning or sexual dysfunction symptoms, and not sexual distress. It may be that extraversion is an important factor in promoting increased sexual activity and higher levels of sexual functioning, but its role in protecting from sexual distress is less strong, particularly when neuroticism is considered simultaneously. Indeed, neuroticism is, by its own definition, the personality trait capturing psychological distress and poor coping skills; accordingly, its ability to predict sexual distress may surpass and suppress the role of extraversion when both are entered together in the equation. In fact, zero-order correlations indicated a significant negative association between extraversion and sexual distress at time point 1. This possible explanation needs further testing but may have important clinical implications.
Although this is the first longitudinal study, we are aware of, examining the effects of neuroticism and extraversion on sexual functioning and distress, there are a few longitudinal studies testing the impact of these trait factors in predicting affective disorders and in particular anxiety and depression (Spinhoven et al., 2011, 2013; Struijs et al., 2018). Overall, studies support the role of high neuroticism and low extraversion in various affective disorders across time. Our findings lend support to transdiagnostic theories of psychological disorders suggesting that these personality dimensions may work as global/common vulnerability factors for the onset and maintenance of several affective disorders (e.g., anxiety and depression) (Barlow et al., 2013; Brown & Barlow, 2009; Kotov et al., 2010; Ormel et al., 2013), including sexual dysfunction. Recent studies have used transdiagnostic approaches to test the existence of higher-order latent factors that are common to anxiety, depression and sexual dysfunctions, with findings partially supporting the inclusion of sexual dysfunction as part of the internalizing spectrum, which accounts for the high comorbidity among the depressive and anxiety disorders (Forbes et al., 2015, 2017).
These findings also have important clinical implications since they suggest that sexual dysfunctions may benefit from transdiagnostic interventions that target common psychological vulnerability factors such as neuroticism and low extraversion. Recent findings support the ability of psychological intervention to change trait factors (Barlow et al., 2013; Roberts et al., 2017). Moreover, randomized control trial studies using a unified treatment protocol (UP; transdiagnostic intervention) have indicated similar symptom reduction and less attrition compared to evidence-based specific cognitive-behavioral interventions in a clinical sample of individuals with mixed anxiety disorders (Barlow et al., 2017). In addition, after treatment, participants in the UP condition exhibited significantly lower levels of neuroticism than participants in the symptom-focused CBT (Sauer-Zavala et al., 2021). Taken together, these findings suggest that sexual dysfunctions may also benefit from a transdiagnostic intervention approach targeting global psychological vulnerability factors such as neuroticism and low extraversion.
Additionally, findings on specific trait factors (sexual beliefs) indicated that higher endorsement of female age-related beliefs significantly predicted lower levels of sexual functioning as well as higher sexual distress in men and women, after controlling for the effects of age and gender. Furthermore, age-related beliefs significantly predicted sexual functioning and sexual distress when simultaneously controlling for the effects of more global trait factors such as neuroticism and extraversion. Indeed, it is worth noting that the absence of interaction effects with gender reveals that despite this being a typical female sexual belief (i.e., expected to be mostly endorsed by women), its negative impact is observed in women’s as well as in men’s sexual functioning and distress, suggesting a common psychological vulnerability pattern. None of the other sexual beliefs (i.e., female sexual conservatism, male sexual conservatism, “macho” beliefs) predicted sexual functioning or distress; neither there were any significant interactions between those beliefs and gender.
Female age-related beliefs are characterized by the idea that women’s sexual activity, sexual interest/desire, pleasure, or orgasm is strongly dependent on age and tend to inevitably decrease in particular after menopause (e.g., “after menopause women can’t reach orgasm,” “after menopause women lose their sexual desire,” “as women age the pleasure they get from sex decreases”). Previous cross-sectional studies have consistently found a significant association between age-related beliefs and sexual (dys)function in women. Women with mixed sexual dysfunctions, low sexual desire, and vaginismus endorsed significantly more age-related beliefs compared to sexually healthy women (Nobre & Pinto-Gouveia, 2008; Nobre & Pinto‐Gouveia, 2006). In addition, correlational studies indicated that age-related beliefs were significantly associated with lower levels of sexual functioning, lower sexual desire, and higher levels of sexual pain in women (Carvalho & Nobre, 2010; Nimbi et al., 2019a, 2019b). Despite these cross-sectional findings, the current study is the first to suggest that age-related beliefs measured at a given time point are able to predict lowered levels of sexual functioning and higher sexual distress across time during a critical continuous life stressor such as the ongoing pandemic. This finding lends support to the role of age-related beliefs as specific vulnerability traits for the development of sexual (dys)function and distress besides the contribution of other global trait vulnerability factors such as neuroticism and extraversion. Moreover, the fact that the effect of female age-related beliefs was observed not only in women but also in men’s sexual functioning and distress suggests that men who endorse these beliefs may me more prone to develop sexual difficulties, particularly at a critical long-term stressor such as the pandemic crisis. There are no previous studies testing the association between female age-related beliefs and men’s sexual health, but we may speculate that men who tend to believe that women’s sexual interest/desire, pleasure, and orgasm inevitably decrease with age are more prone to interpret possible signs of lowered sexual interest from female partners (particularly long-term menopausal or peri-menopausal partners) as a sign of an inevitable end of sexual life that may lead to decreased investment and disengagement from partnered sexual activity with its accompanied distress.
Contrary to our hypotheses, the remaining sexual beliefs did not predict sexual functioning or sexual distress across time. In fact, previous studies have indicated significant associations between both male and female sexual conservatism, and “macho” beliefs and sexual (dys)function (Carvalho & Nobre, 2010, 2011; Dang & Gorzalka, 2015; Nimbi et al., 2018, 2019a, 2019b; Nobre, 2010; Pascoal et al., 2017). It may be that these sexual beliefs are associated with sexual (dys)function in cross-sectional studies, but that their role in predicting sexual health indicators longitudinally are less relevant when compared to age-related beliefs (in particular when all predictors are included simultaneously). In fact, when we analyze zero-order correlations in the current study, we find that male and female sexual conservatism is significantly associated with lowered sexual functioning and increased sexual distress across time while “macho” beliefs are also significantly related to the sexual distress across time and to lowered sexual functioning at time point 2. Additionally, it would be worth of exploring whether specific sexual beliefs could be prompted by extreme contexts such as the current pandemic, as (sexual)beliefs are expected to be shaped by individuals’ life experiences. As such, the predictive role of sexual beliefs could be context dependent. Finally, although this study did not assess the rigidity/inflexibility of the sexual beliefs, it may be that besides its content, the level of rigidity of the beliefs plays also a role in predicting sexual functioning and distress. Recent findings suggest that psychological inflexibility is associated with lower relationship satisfaction (Daks & Rogge, 2020) and that flexibility sexual scripts are linked to sexual satisfaction and lowered sexual distress (Gauvin & Pukall, 2018).
Besides the role of the main psychological vulnerability predictors, results indicated a significant effect of age on sexual functioning (such that older age predicted lower levels of sexual functioning) but not on sexual distress. Findings regarding the role of age on sexual functioning are consistent with the literature, emphasizing that older individuals (regardless of gender) are more prone to have lower levels of sexual functioning (Laumann et al., 2005). However, the negative impact of age was not observed for sexual distress, suggesting that despite the trend for lowered levels of sexual functioning in older individuals, the perceived sexual distress associated is not significantly higher. Although research on the impact of age on sexual distress is less common compared to sexual functioning, previous findings are in line with this result, suggesting that, particularly in women, lower levels of sexual functioning and increased sexual difficulties associated with age are not always perceived as distressful (Graham et al., 2020; Hayes & Dennerstein, 2005).
As for the effect of time (time point 1 vs time point 2), we observed a significant effect on sexual distress indicating that, regardless of gender, the sexual distress measured at time point 2 was lower than at time point 1. The higher sexual distress at time point 1 may have been related to the fact that data from this first moment were collected during the first confinement period (May to early June), whereas time point 2 was collected 4 months later (when no strict confinement measures were in place). Interestingly, despite that no significant time effect was observed for sexual functioning, there was a significant time*gender interaction effect. Sexual functioning was significantly lower for men at time point 2, but it remained stable for women. This finding suggests that the effects of the COVID-19 pandemic crisis with its associated stressors (e.g., restrictions to social interaction, increased health, financial and relationship concerns, etc.) may have had a more negative long-term impact on men’s sexual functioning compared to women. Alternatively, higher levels of sexual functioning at time point 1 in men (compared to time point 2) may eventually mirror a coping mechanism during confinement stressors. Indeed, the crisis context of COVID-19 was deemed a potential trigger of sexual outlets as means to regulate psychological distress (Carvalho & Pascoal, 2020). In line with this assumption, previous findings on the effects of COVID-19 and social isolation measures showed that sexual activity was positively associated with number of days under social isolation (Li et al., 2020) and that mental distress predicted casual sex in men, during confinement measures (Shilo & Mor, 2020). Similarly, individuals reported increased pornography consumption, autoeroticism, or even sexual desire, after lockdown (Cocci et al., 2020). In the context of COVID-19 lockdown measures, sexual activity seemed to have played a protective role in individuals’ anxiety and mood disorders (Mollaioli et al., 2021).
The current study presents some limitations that must be outlined. Over 70% of the sample dropped out the study after the first wave of assessment, precluding accurate conclusions regarding time effects. Similarly, the study included only 2 time points, preventing us from capturing the long-term effects of the crisis. Also, there was a gender imbalance with much more women than men completing the survey. In addition, during the confinement period (March-June), individuals went through different levels of confinement; such differentiating effects were not accounted in the current study. Despite the exclusive focus on psychological vulnerability factors (personality traits, sexual beliefs), it is worth mentioning that relationship dynamics are believed to be particularly at play during current pandemic; these variables were not accounted in the current study. Moreover, we did not control for potential important confounders such as changes of employment status or financial stress during the pandemic, which may have had an impact on sexual health. Additionally, the role of sexual beliefs, which are strongly shaped by sociocultural factors, may differ according to the cultural context. The study used self-report measures to assess sexual functioning and distress which precludes interpretations about the impact of predictors on clinical diagnoses of sexual dysfunctions. Finally, despite that GEE parameter estimates are consistent irrespective of the chosen correlation structure, this approach has some limitations that include challenges with model selection due to lack of absolute goodness-of-fit tests to aid comparisons among several plausible models. In the present study, we could not test whether the set of sexual beliefs would significantly improve the prediction of sexual functioning and sexual distress over the personality traits as it is usually done via the general linear model (GLM) approach when hierarchical linear regressions are performed.
Despite these limitations, the current study is the first to examine the role of psychological vulnerability factors on sexual functioning and distress in both men and women, using a longitudinal design, during a particularly unique long-term stressor such as the COVID-19 pandemic. Findings lend some support to psychological theoretical models of sexual dysfunction (Barlow, 2002; Nobre, 2009, 2010, 2017), emphasizing the ability of global trait factors such as neuroticism and low extraversion, as well as specific factors such as age-related beliefs to predict sexual functioning and distress across time. The longitudinal nature of the study allows to infer that these psychological traits work as vulnerability factors, predisposing men and women to develop lower levels of sexual functioning and sexual distress (the two main markers of sexual dysfunction) across time. Moreover, results from this study have important clinical implications and may help, not only refining existing psychological interventions for sexual dysfunctions (e.g., Cognitive behavioral interventions aimed at changing cognitive dimensions such as sexual beliefs) but also developing new intervention strategies such as the use of transdiagnostic treatments (e.g., unified protocol treatment) (Barlow et al., 2013) that have been used successfully across different psychological disorders (Barlow et al., 2017).
Funding
This research was supported by the Center for Psychology at the University of Porto, Portuguese Science Foundation (FCT UIDB/00050/2020).
Declarations
Conflict of interest
There is no conflict of interests.
Ethical Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of the Faculty of Psychology and Educational Sciences at University of Porto.
Availability of Data and Material
The data that support the findings of this study are available on request from the corresponding author (PN). The data are not publicly available due to (restrictions, e.g., their containing information that could compromise the privacy of research participants).
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Agresti, A. (2002). Categorical data analysis (Second ed.). Wiley. 10.1002/0471249688
- Allen MS, Walter EE. Linking Big Five personality traits to sexuality and sexual health: A meta-analytic review. Psychological Bulletin. 2018;144(10):1081–1110. doi: 10.1037/bul0000157. [DOI] [PubMed] [Google Scholar]
- Baker CD, Silva PD. The relationship between male sexual dysfunction and belief in Zilbergeld’s myths: An empirical investigation. Sexual and Marital Therapy. 1988;3(2):229–238. doi: 10.1080/02674658808407714. [DOI] [Google Scholar]
- Barlow, D. H. (2002). Anxiety and its disorders: The nature and treatment of anxiety and panic (2nd ed.) Guilford Press.
- Barlow DH, Farchione TJ, Bullis JR, Gallagher MW, Murray-Latin H, Sauer-Zavala S, Bentley KH, Thompson-Hollands J, Conklin LR, Boswell JF, Ametaj A, Carl JR, Boettcher HT, Cassiello-Robbins C. The unified protocol for transdiagnostic treatment of emotional disorders compared with diagnosis-specific protocols for anxiety disorders. JAMA Psychiatry. 2017;74(9):875–884. doi: 10.1001/jamapsychiatry.2017.2164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barlow DH, Sauer-Zavala S, Carl JR, Bullis JR, Ellard KK. The nature, diagnosis, and treatment of neuroticism: Back to the future. Clinical Psychological Science. 2013;2(3):344–365. doi: 10.1177/2167702613505532. [DOI] [Google Scholar]
- Beck, A. T. (1996). Beyond belief: A theory of modes, personality, and psychopathology. In P. M. Salkovskis (Ed.), Frontiers of cognitive therapy (pp. 1–25). The Guilford Press.
- Beckwith ACE, Green J, Goldmeier D, Hetherton J. Dysfunctional ideas (‘male myths’) are a result of, rather than the cause of, psychogenic erectile dysfunction in heterosexual men. International Journal of STD & AIDS. 2009;20(9):638–641. doi: 10.1258/ijsa.2008.008468. [DOI] [PubMed] [Google Scholar]
- Borg C, de Jong PJ, Weijmar Schultz W. Vaginismus and dyspareunia: Relationship with general and sex-related moral standards. Journal of Sexual Medicine. 2011;8(1):223–231. doi: 10.1111/j.1743-6109.2010.02080.x. [DOI] [PubMed] [Google Scholar]
- Brito-Costa S, Bem-Haja P, Moisão A, Alberty A, Castro FV, De Almeida H. Psychometric properties of Portuguese version of Big Five Inventory (BFI) International Journal of Developmental and Educational Psychology. 2015;1(2):83–94. [Google Scholar]
- Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, Rubin GJ. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi: 10.1016/S0140-6736(20)30460-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brotto L, Atallah S, Johnson-Agbakwu C, Rosenbaum T, Abdo C, Byers ESS, Graham C, Nobre PJ, Wylie K. Psychological and interpersonal dimensions of sexual function and dysfunction. Journal of Sexual Medicine. 2016;13(4):538–571. doi: 10.1016/j.jsxm.2016.01.019. [DOI] [PubMed] [Google Scholar]
- Brown TA, Barlow DH. A proposal for a dimensional classification system based on the shared features of the DSM-IV anxiety and mood disorders: Implications for assessment and treatment. Psychological Assessment. 2009;21(3):256–271. doi: 10.1037/a0016608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carvalho J, Campos P, Carrito M, Moura C, Quinta-Gomes A, Tavares I, Nobre P. The relationship between COVID-19 confinement, psychological adjustment, and sexual functioning, in a sample of portuguese men and women. Journal of Sexual Medicine. 2021;18(7):1191–1197. doi: 10.1016/j.jsxm.2021.04.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carvalho J, Nobre PJ. Predictors of women’s sexual desire: The role of psychopathology, cognitive-emotional determinants, relationship dimensions, and medical factors. Journal of Sexual Medicine. 2010;7(2):928–937. doi: 10.1111/j.1743-6109.2009.01568.x. [DOI] [PubMed] [Google Scholar]
- Carvalho J, Nobre PJ. Biopsychosocial determinants of men’s sexual desire: Testing an integrative model. Journal of Sexual Medicine. 2011;8(3):754–763. doi: 10.1111/j.1743-6109.2010.02156.x. [DOI] [PubMed] [Google Scholar]
- Carvalho J, Pascoal PM. Challenges in the practice of sexual medicine in the time of COVID-19 in Portugal. Journal of Sexual Medicine. 2020;17(7):1212–1215. doi: 10.1016/j.jsxm.2020.05.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cocci A, Giunti D, Tonioni C, Cacciamani G, Tellini R, Polloni G, Cito G, Presicce F, Di Mauro M, Minervini A, Cimino S, Russo GI. Love at the time of the Covid-19 pandemic: Preliminary results of an online survey conducted during the quarantine in Italy. International Journal of Impotence Research. 2020;32(5):556–557. doi: 10.1038/s41443-020-0305-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costa Jr, P. T., & McCrae, R. R. (1992). Revised NEO Personality Inventory (NEO-PI-R) and NEO Five-Factor (NEO-FFI) Inventory Professional Manual. Psychological Assessment Resources.
- Costa PTJ, Fagan PJ, Piedmont RL, Ponticas Y, Wise TN. The five-factor model of personality and sexual functioning in outpatient men and women. Psychiatric Medicine. 1992;10(2):199–215. [PubMed] [Google Scholar]
- Crisp C, Vaccaro C, Fellner A, Kleeman S, Pauls R. The influence of personality and coping on female sexual function: A population survey. Journal of Sexual Medicine. 2015;12(1):109–115. doi: 10.1111/jsm.12735. [DOI] [PubMed] [Google Scholar]
- Cui J, Qian G. Selection of working correlation structure and best model in GEE analyses of longitudinal data. Communications in Statistics - Simulation and Computation. 2007;36(5):987–996. doi: 10.1080/03610910701539617. [DOI] [Google Scholar]
- Daks JS, Rogge RD. Examining the correlates of psychological flexibility in romantic relationship and family dynamics: A meta-analysis. Journal of Contextual Behavioral Science. 2020;18:214–238. doi: 10.1016/j.jcbs.2020.09.010. [DOI] [Google Scholar]
- Dang SS, Gorzalka BB. Insecure attachment style and dysfunctional sexual beliefs predict sexual coercion proclivity in university men. Sexual Medicine. 2015;3(2):99–108. doi: 10.1002/sm2.60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Derogatis LR, Rosen R, Leiblum S, Burnett A, Heiman J. The Female Sexual Distress Scale (FSDS): Initial validation of a standardized scale for assessment of sexually related personal distress in women. Journal of Sex & Marital Therapy. 2002;28(4):317–330. doi: 10.1080/00926230290001448. [DOI] [PubMed] [Google Scholar]
- Eysenck HJ. Personality and sexual adjustment. British Journal of Psychiatry. 1971;118(547):593–608. doi: 10.1192/bjp.118.547.593. [DOI] [PubMed] [Google Scholar]
- Fagan PJ, Wise TN, Schmidt CW, Jr, Ponticas Y, Marshall RD, Costa PT., Jr A comparison of five-factor personality dimensions in males with sexual dysfunction and males with paraphilia. Journal of Personality Assessment. 1991;57(3):434–448. doi: 10.1207/s15327752jpa5703_4. [DOI] [PubMed] [Google Scholar]
- Forbes MK, Baillie AJ, Eaton NR, Krueger RF. A place for sexual dysfunctions in an empirical taxonomy of psychopathology. Journal of Sex Research. 2017;54(4–5):465–485. doi: 10.1080/00224499.2016.1269306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forbes MK, Baillie AJ, Schniering CA. A structural equation modeling analysis of the relationships between depression, anxiety, and sexual problems over time. Journal of Sex Research. 2015;53(8):942–954. doi: 10.1080/00224499.2015.1063576. [DOI] [PubMed] [Google Scholar]
- Gauvin S, Pukall CF. The SexFlex scale: A measure of sexual script flexibility when approaching sexual problems in a relationship. Journal of Sex and Marital Therapy. 2018;44(4):382–397. doi: 10.1080/0092623X.2017.1405304. [DOI] [PubMed] [Google Scholar]
- Graham CA, Štulhofer A, Lange T, Hald GM, Carvalheira AA, Enzlin P, Træen B. Prevalence and predictors of sexual difficulties and associated distress among partnered, sexually active older women in Norway, Denmark, Belgium, and Portugal. Archives of Sexual Behavior. 2020;49(8):2951–2961. doi: 10.1007/s10508-020-01742-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Harris JM, Cherkas LF, Kato BS, Heiman JR, Spector TD. Normal variations in personality are associated with coital orgasmic infrequency in heterosexual women: A population-based study. Journal of Sexual Medicine. 2008;5(5):1177–1183. doi: 10.1111/j.1743-6109.2008.00800.x. [DOI] [PubMed] [Google Scholar]
- Hayes R, Dennerstein L. The impact of aging on sexual function and sexual dysfunction in women: A review of population-based studies. Journal of Sexual Medicine. 2005;2(3):317–330. doi: 10.1111/j.1743-6109.2005.20356.x. [DOI] [PubMed] [Google Scholar]
- Hedecker D, Gibbons RD. Longitudinal data analysis. John Wiley and Sons; 2006. [Google Scholar]
- Heiman, J., & LoPiccolo, J. (1988). Becoming orgasmic: A sexual and personal growth program for women. Prentice Hall.
- Heitjan DF, Basu S. Distinguishing “missing at random” and “missing completely at random”. American Statistician. 1996;50:207–213. [Google Scholar]
- John, O. P., Donahue, E. M., & Kentle, R. L. (1991). Big Five Inventory. Journal of Personality and Social Psychology, 75, 729–750.
- John, O. P., & Srivastava, S. (1999). The Big Five trait taxonomy: History, measurement, and theoretical perspectives. In L. A. Pervin & O. P. John (Eds.), Handbook of personality: Theory and research (pp. 102–138). Guilford Press.
- Kennedy SH, Dickens SE, Eisfeld BS, Bagby RMM. Sexual dysfunction before antidepressant therapy in major depression. Journal of Affective Disorders. 1999;56(2–3):201–208. doi: 10.1016/s0165-0327(99)00050-6. [DOI] [PubMed] [Google Scholar]
- Kotov R, Gamez W, Schmidt F, Watson D. Linking “big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychological Bulletin. 2010;136(5):768–821. doi: 10.1037/a0020327. [DOI] [PubMed] [Google Scholar]
- Laumann EO, Nicolosi A, Glasser DB, Paik A, Gingell C, Moreira E, Wang T. Sexual problems among women and men aged 40–80 y: Prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. International Journal of Impotence Research. 2005;17(1):39–57. doi: 10.1038/sj.ijir.3901250. [DOI] [PubMed] [Google Scholar]
- Li W, Li G, Xin C, Wang Y, Yang S. Challenges in the practice of sexual medicine in the time of COVID-19 in China. Journal of Sexual Medicine. 2020;17(7):1225–1228. doi: 10.1016/j.jsxm.2020.04.380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCrae RR, Costa PT. A contemplated revision of the NEO Five-Factor Inventory. Personality and Individual Differences. 2004;36(3):587–596. doi: 10.1016/s0191-8869(03)00118-1. [DOI] [Google Scholar]
- Meyer-Bahlburg HFL, Dolezal C. The Female Sexual Function Index: A methodological critique and suggestions for improvement. Journal of Sex & Marital Therapy. 2007;33(3):217–224. doi: 10.1080/00926230701267852. [DOI] [PubMed] [Google Scholar]
- Mollaioli D, Sansone A, Ciocca G, et al. Benefits of sexual activity on psychological, relational, and sexual health during the COVID-19 breakout. Journal of Sexual Medicine. 2021;18:35–49. doi: 10.1016/j.jsxm.2020.10.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morton H, Gorzalka BB. Cognitive aspects of sexual functioning: Differences between east Asian-Canadian and Euro-Canadian women. Archives of Sexual Behavior. 2013;42(8):1615–1625. doi: 10.1007/s10508-013-0180-3. [DOI] [PubMed] [Google Scholar]
- Moura, C., Vasconcelos, P., Carrito, M., Tavares, I., Teixeira, P., & Nobre, P. J. (2021). The role of men’s sexual beliefs on sexual function/dysfunction: A systematic review and meta-analysis. Manuscript submitted for publication.
- Nimbi FM, Tripodi F, Rossi R, Michetti PM, Simonelli C. Which psychosocial variables affect drive the most? Analysis of sexual desire in a group of Italian men. International Journal of Impotence Research. 2019;31(6):410–423. doi: 10.1038/s41443-018-0105-8. [DOI] [PubMed] [Google Scholar]
- Nimbi FM, Tripodi F, Rossi R, Simonelli C. Expanding the analysis of psychosocial factors of sexual desire in men. Journal of Sexual Medicine. 2018;15(2):230–244. doi: 10.1016/j.jsxm.2017.11.227. [DOI] [PubMed] [Google Scholar]
- Nimbi FM, Tripodi F, Simonelli C, Nobre PJ. Sexual Dysfunctional Beliefs Questionnaire (SDBQ): Translation and psychometric properties of the Italian version. Sexologies. 2019;28(2):e11–e27. doi: 10.1016/j.sexol.2018.09.003. [DOI] [Google Scholar]
- Nobre PJ. Determinants of sexual desire problems in women: Testing a cognitive-emotional model. Journal of Sex & Marital Therapy. 2009;35(5):360–377. doi: 10.1080/00926230903065716. [DOI] [PubMed] [Google Scholar]
- Nobre PJ. Psychological determinants of erectile dysfunction: Testing a cognitive–emotional model. Journal of Sexual Medicine. 2010;7(4):1429–1437. doi: 10.1111/J.1743-6109.2009.01656.X. [DOI] [PubMed] [Google Scholar]
- Nobre, P. J. (2017). Sexual dysfunctions. In S. Hofmann (Ed.), Clinical psychology: A global perspective (pp. 225–241). Wiley-Blackwell.
- Nobre PJ, Gouveia JP, Gomes FA. Sexual dysfunctional beliefs questionnaire: An instrument to assess sexual dysfunctional beliefs as vulnerability factors to sexual problems. Sexual and Relationship Therapy. 2003;18(2):171–204. doi: 10.1080/1468199031000061281. [DOI] [Google Scholar]
- Nobre PJ, Pinto-Gouveia J. Cognitive and emotional predictors of female sexual dysfunctions: Preliminary findings. Journal of Sex and Marital Therapy. 2008;34(4):325–342. doi: 10.1080/00926230802096358. [DOI] [PubMed] [Google Scholar]
- Nobre PJ, Pinto-Gouveia J. Dysfunctional sexual beliefs as vulnerability factors for sexual dysfunction. Journal of Sex Research. 2006;43(1):68–75. doi: 10.1080/00224490609552300. [DOI] [PubMed] [Google Scholar]
- Ormel J, Jeronimus BF, Kotov R, Riese H, Bos EH, Hankin B, Rosmalen JGM, Oldehinkel AJ. Neuroticism and common mental disorders: Meaning and utility of a complex relationship. Clinical Psychology Review. 2013;33(5):686–697. doi: 10.1016/j.cpr.2013.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pascoal PM, Alvarez M-J, Pereira CR, Nobre PJ. Development and initial validation of the Beliefs about Sexual Functioning Scale: A gender invariant measure. Journal of Sexual Medicine. 2017;14(4):613–623. doi: 10.1016/j.jsxm.2017.01.021. [DOI] [PubMed] [Google Scholar]
- Pascoal, P. M., Carvalho, J., Raposo, C. F., Almeida, J., & Beato, A. F. (2021). The impact of COVID 19 on sexual health: A preliminary framework based on a qualitative study with clinical sexologists. Sexual Medicine, 9. 10.1016/j.esxm.2020.100299 [DOI] [PMC free article] [PubMed]
- Pechorro P, Diniz A, Almeida S, Vieira R. Validação portuguesa do índice de Funcionamento Sexual Feminino (FSFI) Laboratório De Psicologia. 2009;7(1):33–44. [Google Scholar]
- Peixoto MM, Nobre PJ. Dysfunctional sexual beliefs: A comparative study of heterosexual men and women, gay men, and lesbian women with and without sexual problems. Journal of Sexual Medicine. 2014;11(11):2690–2700. doi: 10.1111/jsm.12666. [DOI] [PubMed] [Google Scholar]
- Peixoto MM, Nobre PJ. Personality traits, sexual problems, and sexual orientation: An empirical study. Journal of Sex & Marital Therapy. 2014;42(3):199–213. doi: 10.1080/0092623x.2014.985352. [DOI] [PubMed] [Google Scholar]
- Quinta Gomes AL, Nobre P. The International Index of Erectile Function (IIEF-15): Psychometric properties of the Portuguese version. Journal of Sexual Medicine. 2012;9(1):180–187. doi: 10.1111/j.1743-6109.2011.02467.x. [DOI] [PubMed] [Google Scholar]
- Quinta Gomes AL, Nobre PJ. Personality traits and psychopathology on male sexual dysfunction: An empirical study. Journal of Sexual Medicine. 2011;8(2):461–469. doi: 10.1111/j.1743-6109.2010.02092.x. [DOI] [PubMed] [Google Scholar]
- Roberts BW, Luo J, Briley DA, Chow PI, Su R, Hill PL. A systematic review of personality trait change through intervention. Psychological Bulletin. 2017;143(2):117–141. doi: 10.1037/bul0000088. [DOI] [PubMed] [Google Scholar]
- Rodríguez-Rey R, Garrido-Hernansaiz H, Collado S. Psychological impact and associated factors during the initial stage of the coronavirus (COVID-19) pandemic among the general population in Spain. Frontiers in Psychology. 2020;11:1540. doi: 10.3389/fpsyg.2020.01540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosa PJ, Lopes P, Oliveira J, Pascoal P. Does length really matter? Effects of number of pages in the informed consent on reading behavior: An eye-tracking study. In: Fardoun HM, Hassan AAM, de la Guía ME, editors. New technologies to improve patient rehabilitation. Springer International Publishing; 2019. pp. 116–125. [Google Scholar]
- Rosen RC, Brown J, Heiman S, Leiblum C, Meston R, Shabsigh D, Ferguson R, D’Agostino R. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. Journal of Sex and Marital Therapy. 2000;26(2):191–208. doi: 10.1080/009262300278597. [DOI] [PubMed] [Google Scholar]
- Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The International Index of Erectile Function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49(6):822–830. doi: 10.1016/S0090-4295(97)00238-0. [DOI] [PubMed] [Google Scholar]
- Rosenheim E, Neumann M. Personality characteristics of sexually dysfunctioning males and their wives. Journal of Sex Research. 1981;17(2):124–138. doi: 10.1080/00224498109551107. [DOI] [Google Scholar]
- Roychowdhury D. 2019 novel coronavirus disease, crisis, and isolation. Frontiers in Psychology. 2020;11:1958. doi: 10.3389/fpsyg.2020.01958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sauer-Zavala S, Fournier JC, Jarvi Steele S, Woods BK, Wang M, Farchione TJ, Barlow DH. Does the unified protocol really change neuroticism? Results from a randomized trial. Psychological Medicine. 2021;51:2378–2387. doi: 10.1017/s0033291720000975. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schenk J, Pfrang H, Rausche A. Personality traits versus the quality of the marital relationship as the determinant of marital sexuality. Archives of Sexual Behavior. 1983;12(1):31–42. doi: 10.1007/bf01542114. [DOI] [PubMed] [Google Scholar]
- Schiavi MC, Spina V, Zullo MA, Colagiovanni V, Luffarelli P, Rago R, Palazzetti P. Love in the time of COVID-19: Sexual function and quality of life analysis during the social distancing measures in a group of Italian reproductive-age women. Journal of Sexual Medicine. 2020;17(8):1407–1413. doi: 10.1016/j.jsxm.2020.06.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shilo G, Mor Z. COVID-19 and the changes in the sexual behavior of men who have sex with men: Results of an online survey. Journal of Sexual Medicine. 2020;17:1827–1834. doi: 10.1016/j.jsxm.2020.07.085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith, B., & Lim, M. (2020). How the COVID-19 pandemic is focusing attention on loneliness and social isolation. Public Health Research and Practice, 30. 10.17061/phrp3022008 [DOI] [PubMed]
- Spinhoven P, Roelofs K, Hovens JGFM, Elzinga BM, van Oppen P, Zitman FG, Penninx BWJH. Personality, life events and the course of anxiety and depression. European Journal of Personality. 2011;25(6):443–452. doi: 10.1002/per.808. [DOI] [Google Scholar]
- Spinhoven P, van der Does W, Ormel J, Zitman FG, Penninx BWJH. Confounding of Big Five personality assessments in emotional disorders by comorbidity and current disorder. European Journal of Personality. 2013;27(4):389–397. doi: 10.1002/per.1885. [DOI] [Google Scholar]
- Struijs SY, Lamers F, Spinhoven P, van der Does W, Penninx BWJH. The predictive specificity of psychological vulnerability markers for the course of affective disorders. Journal of Psychiatric Research. 2018;103:10–17. doi: 10.1016/j.jpsychires.2018.04.017. [DOI] [PubMed] [Google Scholar]
- Yuksel B, Ozgor F. Effect of the COVID-19 pandemic on female sexual behavior. International Journal of Gynecology & Obstetrics. 2020;150(1):98–102. doi: 10.1002/ijgo.13193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ziegler, A. (2011). Generalized estimating equations. Springer. 10.1007/978-1-4614-0499-6
- Zilbergeld, B. (1999). The new male sexuality. Bantam.
- Zinbarg RE, Barlow DH. Structure of anxiety and the anxiety disorders: A hierarchical model. Journal of Abnormal Psychology. 1996;105(2):181–193. doi: 10.1037/0021-843x.105.2.181. [DOI] [PubMed] [Google Scholar]