

Abstract
Background
In people with acute ischaemic stroke, platelets become activated and can cause blood clots to form and block an artery in the brain, resulting in damage to part of the brain. Such damage gives rise to the symptoms of stroke. Antiplatelet therapy might reduce the volume of brain damaged by ischaemia and also reduce the risk of early recurrent ischaemic stroke, thereby reducing the risk of early death and improving long‐term outcomes in survivors. However, antiplatelet therapy might also increase the risk of fatal or disabling intracranial haemorrhage.
Objectives
To assess the efficacy and safety of immediate oral antiplatelet therapy (i.e. started as soon as possible and no later than two weeks after stroke onset) in people with acute presumed ischaemic stroke.
Search methods
We searched the Cochrane Stroke Group Trials Register, CENTRAL, MEDLINE Ovid, Embase Ovid, and two trials registers, and performed forward reference/cited reference searching in August 2020.
Selection criteria
Randomised controlled trials (RCTs) comparing oral antiplatelet therapy (started within 14 days of the stroke) with control in people with definite or presumed ischaemic stroke.
Data collection and analysis
Two review authors independently applied the inclusion criteria and assessed trial quality. For the included trials, they extracted and cross‐checked the data. They assessed risk of bias of each study using the Risk of Bias 1 (RoB1) tool and overall certainty of the evidence for each outcome using the GRADE approach.
Main results
We included 11 studies involving 42,226 participants. Three new trials have been added since the last update (743 participants). As per the previous version of this review, two trials testing aspirin 160 mg to 300 mg once daily, started within 48 hours of onset, contributed 96% of the data. The risk of bias was low. The maximum follow‐up was six months. With treatment, there was a decrease in death or dependency at the end of follow‐up (odds ratio (OR) 0.95, 95% confidence interval (CI) 0.91 to 0.99; 7 RCTs, 42,034 participants; moderate‐certainty evidence). For every 1000 people treated with aspirin, 13 people would avoid death or dependency (number needed to treat for an additional beneficial outcome 79).
Authors' conclusions
Antiplatelet therapy with aspirin 160 mg to 300 mg daily, given orally (or by nasogastric tube or per rectum in people who cannot swallow) and started within 48 hours of onset of presumed ischaemic stroke, significantly decreased death and dependency, and reduced the risk of early recurrent ischaemic stroke without a major risk of early haemorrhagic complications; long‐term outcomes were improved.
Plain language summary
Oral antiplatelet therapy for acute ischaemic stroke
Review question
We wanted to compare the safety and effectiveness of oral antiplatelet therapy versus placebo or no treatment in people with acute ischaemic stroke to see if oral antiplatelet medicines reduced the number of deaths and improved the long‐term outcomes in survivors.
Background
Most strokes are caused by a sudden blockage of an artery in the brain that is usually due to a blood clot (called an ischaemic stroke). Immediate treatment with antiplatelet medicines such as aspirin may prevent new clots from forming and hence improve recovery after stroke. However, antiplatelet medicines may also cause bleeding in the brain, which could offset any benefits.
Study characteristics
We identified 11 studies, up to August 2020, for inclusion in the review. These studies included 42,226 participants. Three new trials have been added since the last update. As per the previous version of this review, two studies contributed 96% of the data. Most participants in the review were elderly, with a significant proportion over 70 years of age. Males and females were almost equally represented in the trials. There appeared to be some variation in stroke severity among the included trials. The scheduled duration of treatment varied from five days to three months and the scheduled follow‐up period varied from 10 days to six months.
Key results
Aspirin, at a dose of 160 mg to 300 mg daily, started within 48 hours of the onset of stroke symptoms, saved lives and reduced the risk of further stroke occurring in the first two weeks. If treatment was started more than 48 hours after onset but within 14 days, the limited evidence from this review and other external data suggest that aspirin is of benefit even starting at this late stage. Antiplatelet therapy with aspirin 160 mg to 300 mg daily, given orally (or by a tube through the nose and into the stomach or by the rectum in people who cannot swallow) and started within 48 hours of onset of presumed ischaemic stroke, reduced the risk of early recurrent ischaemic stroke without a major risk of early haemorrhagic complications; long‐term outcomes were improved. Almost all the evidence in this review came from trials of aspirin.
Quality of the evidence
The quality of the evidence contributing to these results was generally good.
Summary of findings
Summary of findings 1. Antiplatelet drug compared to control in acute presumed ischaemic stroke for acute ischaemic stroke.
| Antiplatelet drug compared to control in acute presumed ischaemic stroke for acute ischaemic stroke | |||||
| Patient or population: acute ischaemic stroke Setting: secondary care Intervention: antiplatelet drug Comparison: control in acute presumed ischaemic stroke | |||||
| Outcomes | No of participants (studies) | Certainty of the evidence (GRADE) | Relative effect (95% CI) | Anticipated absolute effects* (95% CI) | |
| Risk with control in acute presumed ischaemic stroke | Risk difference with antiplatelet drug | ||||
| Death or dependence at end of follow‐up (primary outcome) | 42,034 (7 RCTs) | ⊕⊕⊕⊝ Moderatea,b | Peto OR 0.95 (0.91 to 0.99) | Study population | |
| 458 per 1000 | 13 fewer per 1000 (23 fewer to 2 fewer) | ||||
| Death from any cause during follow‐up | 41,929 (10 RCTs) | ⊕⊝⊝⊝ Very lowa,c,d | Peto OR 0.93 (0.87 to 0.98) | Study population | |
| 128 per 1000 | 8 fewer per 1000 (15 fewer to 2 fewer) | ||||
| Pulmonary embolism during treatment period | 41,042 (7 RCTs) | ⊕⊝⊝⊝ Very lowa,e,f,g | Peto OR 0.71 (0.53 to 0.96) | Study population | |
| 5 per 1000 | 1 fewer per 1000 (2 fewer to 0 fewer) | ||||
| Recurrent ischaemic/unknown stroke during treatment period | 41,652 (9 RCTs) | ⊕⊝⊝⊝ Very lowa,c,d | Peto OR 0.79 (0.70 to 0.88) | Study population | |
| 32 per 1000 | 7 fewer per 1000 (9 fewer to 4 fewer) | ||||
| Symptomatic intracranial haemorrhage during treatment period | 41,652 (9 RCTs) | ⊕⊝⊝⊝ Very lowa,c,h,i | Peto OR 1.18 (0.97 to 1.44) | Study population | |
| 9 per 1000 | 2 more per 1000 (0 fewer to 4 more) | ||||
| Major extracranial haemorrhage during treatment period | 41,042 (7 RCTs) | ⊕⊝⊝⊝ Very lowa,e,i | Peto OR 1.69 (1.35 to 2.11) | Study population | |
| 6 per 1000 | 4 more per 1000 (2 more to 6 more) | ||||
| Complete recovery from stroke (post hoc) | 40,541 (2 RCTs) | ⊕⊕⊕⊝ Moderatea,j | Peto OR 1.06 (1.01 to 1.11) | Study population | |
| 262 per 1000 | 11 more per 1000 (2 more to 21 more) | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; PetoOR: Peto odds ratio; RCT: randomised controlled trial. | |||||
| GRADE Working Group grades of evidence High certainty: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
aThe CAST study included only participants of Chinese ethnicity and contributed almost 50% of the data in the meta‐analysis. Therefore, the results are mainly applicable to a Chinese population. bDeath or dependence is the primary outcome measure for the majority of acute stroke intervention trials. cTwo studies were at high risk of bias, for one study there was no information on risk of bias, and for one study the risk of bias was unclear. dStudies showed variable results (some increased, reduced or no change in the event). Therefore, results were not consistent between studies, although there was overlap in the confidence intervals and heterogeneity was low (I2 < 25%). eOne study was at high risk of bias, one study was at unclear risk of bias, and for one study information on risk of bias was not available. fThe analysis was based on two small studies and the confidence intervals were wide. gDeep vein thrombosis and pulmonary embolism are important complications following acute stroke, but secondary to death or dependence. hRecurrent stroke and symptomatic intra‐ or extra‐cranial haemorrhage were a commonly reported outcome measures but are secondary to death or dependence. iThe confidence intervals were wide, but data were from two large studies. jComplete recovery from stroke is an important outcome, reported in the two largest trials in this review, but remains secondary to death or dependence which is the most commonly reported outcome measure.
Background
Description of the condition
Stroke is an enormous and serious public health problem. According to the World Health Organization (WHO), 15 million people have stroke worldwide each year. It is also a major cause of death and disability worldwide. Approximately 80% to 87% of all strokes are ischaemic (i.e. due to a blockage of an artery in the brain) in white populations (Jauch 2013; Warlow 2001), and about 67% in Asian populations (Tsai 2013).
Description of the intervention
Platelets become activated in people with acute ischaemic stroke. This review is focused on oral antiplatelet agents. Oral antiplatelet agents work via different mechanisms to inhibit platelet adhesion and aggregation. The types of drugs include cyclo‐oxygenase inhibitors (e.g. aspirin (acetylsalicylic acid; ASA)), thienopyridine derivatives (e.g. ticlopidine, clopidogrel), phosphodiesterase inhibitors (e.g. dipyridamole, cilostazol), and thromboxane A2 antagonists (e.g. ozagrel).
How the intervention might work
Antiplatelet therapy is effective for long‐term secondary prevention of serious vascular events in people at high risk of vascular disease (ATC 1994a; ATC 2002; ATC 2009). In people with acute myocardial infarction, starting antiplatelet therapy immediately after the event, and continuing it for one month, avoids about 38 vascular events for every 1000 people treated (ATC 1994a; ATC 2002). In individuals with ischaemic stroke or transient ischaemic attack (TIA), being on long‐term antiplatelet therapy avoids about 36 serious vascular events for every 1000 people treated for three years (ATC 1994a; ATC 2002). Platelets are activated in the acute phase of ischaemic stroke, releasing neurotoxic and thrombogenic eicosanoids including thromboxane B2 (van Kooten 1994).
Antiplatelet therapy is, therefore, a logical treatment to evaluate in acute ischaemic stroke. It might reduce early deaths and improve outcomes in survivors by reducing the volume of brain damaged by ischaemia and reducing the risk of early recurrent ischaemic stroke and pulmonary embolism (PE) (ATC 1994a; ATC 1994b). However, antiplatelet therapy could also increase the risk of fatal or disabling intracranial haemorrhage (ICH), thus offsetting any benefits (ATC 1994a). However, recent randomised data have suggested that antiplatelets may be safe even after primary intracerebral haemorrhage when risk of recurrent intracerebral haemorrhage is weighed against benefits of preventing occlusive vascular disease (RESTART 2019). The initial data were sufficiently promising that two large‐scale trials were undertaken: the International Stroke Trial (IST 1997), and the Chinese Acute Stroke Trial (CAST 1997), which together included over 40,000 participants. These trials provided reliable evidence of the net benefit from aspirin in this setting. As a result, evidence‐based guidelines in Europe, Canada, and USA now recommend aspirin as the standard antithrombotic treatment for acute ischaemic stroke (AHA 2013; AHA/ASA Guidelines; CSS 2010; ESO 2008; Jauch 2013; RCP Guideline 2016).
Most data relating to orally active antiplatelet agents is derived from trials of aspirin. Data regarding the utility of other single oral antiplatelet agents, including clopidogrel, dipyridamole, or cilostazol, for the treatment of acute stroke are limited (CAIST 2011; Chairangsarit 2005; Suri 2008). Overall, the data do not provide solid evidence about the utility of these antiplatelet agents in the management of people with acute ischaemic stroke. There has been limited experience and no evidence to support the use of ozagrel in the setting of acute stroke (Zhang 2012). Trials have investigated the early use of multiple antiplatelet agents in addition to aspirin in the acute phase of stroke. Early initiation of aspirin plus extended‐release dipyridamole seem to be as safe and effective in preventing disability as later initiation after conventional aspirin monotherapy (EARLY 2010). Ticagrelor did not provide superiority over aspirin and bleeding risk was higher compared to aspirin monotherapy (SOCRATES). However, when ticagrelor and aspirin were combined versus aspirin alone, the risk of the composite of stroke or death within 30 days was lower with the combination (THALES). Other trials have examined aspirin and clopidogrel combination therapy. The combination was only significantly effective in the immediate high‐risk interval after stroke or TIA (CHANCE 2013; FASTER 2007;Hankey 2010). This has been further clarified by recent data from the POINT trial demonstrating greater benefits of recurrent stroke prevention over risks of major bleeding with dual antiplatelet therapy up to 21 days (POINT). Lastly, triple antiplatelet therapy is not recommended in clinical practice due to significant bleeding risk (TARDIS).
Why it is important to do this review
This review is an update of a previously published review in the Cochrane Database of Systematic Reviews of 'Antiplatelet therapy for acute ischaemic stroke' (Sandercock 2014). The previous version of this Cochrane review stated that antiplatelet therapy with aspirin is safe and effective when started within 48 hours after stroke. Since then more trials have been published. For this update, as per previous versions, we did not include parenterally administrated antiplatelet agents. Platelet glycoprotein (GP) IIb/IIIa receptor inhibitors are the subject of a separate review (Ciccone 2014). Therefore, we conducted this updated review to assess the efficacy and safety of oral antiplatelet therapy when administered to people with acute ischaemic stroke to provide more up‐to‐date evidence for clinical practice and to identify trials of newer agents.
Objectives
To assess the efficacy and safety of immediate oral antiplatelet therapy (i.e. started as soon as possible and no later than two weeks after stroke onset) in people with acute presumed ischaemic stroke.
We wished to test the hypotheses that oral antiplatelet therapy:
reduces the risk of a poor outcome (i.e. the risk of death or being dependent on others for activities of daily living) several months after the stroke;
reduces the risk of death several months after ischaemic stroke;
reduces the risk of deep vein thrombosis (DVT) and PE following ischaemic stroke;
reduces the risk of recurrent ischaemic stroke during the scheduled treatment period;
may increase the risk of bleeding, and that the incidence of both ICH and major extracranial haemorrhage may be increased during the scheduled treatment period.
Methods
Criteria for considering studies for this review
Types of studies
We sought to identify all unconfounded randomised controlled trials (RCTs) of early treatment with oral antiplatelet therapy in which treatment allocation was adequately concealed from doctors entering people into the trials. We excluded trials that were not truly random (e.g. alternating or based on date of birth, day of the week, hospital number) or in which allocation to the treatment or control group was not adequately concealed (such as an open random number list) since foreknowledge of treatment allocation might lead to non‐random treatment allocation and consequent bias in the estimation of treatment effects (Odgaard‐Jensen 2011).
Types of participants
We included all trials that recruited people of any age or sex within two weeks of onset of presumed ischaemic stroke. We excluded trials of antiplatelet therapy after known primary intracerebral or subarachnoid haemorrhage, but included trials that did not adequately differentiate between ischaemic and haemorrhagic stroke by computed tomography (CT) or magnetic resonance (MR) scans prior to randomisation on the basis that 80% to 87% of strokes are ischaemic in predominantly white populations (Jauch 2013; Warlow 2001).
Types of interventions
We considered all unconfounded trials that compared either a single oral antiplatelet agent or a combination of oral antiplatelet agents with control (placebo or no treatment) as eligible. We excluded studies either involving 'head‐to‐head' direct comparisons of one agent versus another or comparison of one multiple agent regimen versus a different multiple agent regimen (the latter is the subject of a separate review: Kamal 2012). We broadly defined oral antiplatelet agents as any agents whose principal effects were to inhibit platelet adhesion and aggregation. These included:
cyclo‐oxygenase inhibitors (e.g. aspirin);
thienopyridine derivatives inhibiting adenosine diphosphate (ADP) receptors (e.g. ticlopidine, clopidogrel);
phosphodiesterase inhibitors (e.g. dipyridamole, cilostazol);
thromboxane A2 antagonists (e.g. ozagrel).
For this update, we excluded parenterally administrated antiplatelet agents. GP IIb/IIIa receptor inhibitors are the focus of a separate review (Ciccone 2014).
We did not include agents with multiple modes of action including some antiplatelet activity (e.g. piracetam, prostacyclin, pentoxifylline), and some of these agents have been evaluated in other Cochrane systematic reviews (Bath 2004a; Bath 2004b; Ricci 2012).
Types of outcome measures
We examined death and dependency outcomes at the end of the follow‐up period for each study. In addition, we examined recurrent ischaemic/unknown stroke, symptomatic ICH, any recurrent stroke/ICH, and major ICH.
Primary outcomes
Death or dependence on help from other people for activities of daily living at least one month after their stroke (death or dependence at end of follow‐up). Many people regard this as the most important outcome since the aim of treatment should not only be to prevent death but also to prevent serious disability in survivors. The minimum interval of one month was used to allow time for recovery from the initial stroke.
Secondary outcomes
Death or dependence during the scheduled follow‐up period (as defined by a validated scale or questionnaire, e.g. modified Rankin Scale ≥ 3).
Death from any cause during the scheduled treatment period (generally shorter than the scheduled follow‐up period).
Death from any cause during the scheduled follow‐up period (generally considered to be greater than one month after the stroke).
DVT: objective evidence of DVT detected by the systematic use of imaging techniques such as iodine 125 fibrinogen scanning (I125 scan), ultrasound of the leg, plethysmography, or X‐ray contrast venography in all participants during the scheduled treatment period (these methods detected both clinically suspected and silent DVTs, the outcome was therefore 'symptomatic or asymptomatic DVT'. Screening of participants by clinical observation alone was not considered adequate).
PE: had at least one confirmed symptomatic PE diagnosed by radiological imaging (ventilation‐perfusion scan or CT pulmonary angiogram (CTPA), or at autopsy (symptomatic or not) within the scheduled treatment period.
Recurrent stroke during the treatment period that was either definitely ischaemic (haemorrhage excluded by CT or MR scan or autopsy) or of unknown type (no CT or MR scan or autopsy performed).
Symptomatic intracranial (intracerebral and extracerebral) haemorrhage, including symptomatic haemorrhagic transformation of the cerebral infarct, during the scheduled treatment period (the haemorrhage must have been confirmed by CT (or MR) scanning after clinical deterioration, or by autopsy).
Recurrent stroke (either of ischaemic or unknown type) or symptomatic ICH during the treatment period.
Major extracranial haemorrhage during the scheduled treatment period (the definition of major haemorrhage was usually taken from the original article but if none was given it was defined as any fatal bleed, or bleeding severe enough to require transfusion or operation);
Complete recovery from stroke.
Note, at a prior update, the final outcome was a post‐hoc analysis, and we acknowledge that the addition of post‐hoc data is subject to selection bias. However, at the time, two trials reported data on the number of participants who had made a complete recovery from their stroke, an important functional outcome that was not a widely reported outcome in stroke trials when the protocol for the earlier version of this review was written (CAST 1997; IST 1997). With the report of the effects of thrombolysis on increasing the proportion of people who recover completely from their stroke (e.g. the NINDS trial of tissue plasminogen activator (NINDS 1995)), it seemed reasonable to include this outcome here with allowance for its post‐hoc nature.
Search methods for identification of studies
See the methods for the Cochrane Stroke Group Specialised register (www.dcn.ed.ac.uk/csrg/entity/searchmethods.pdf). We searched for trials in all languages and arranged translation of relevant papers published in languages other than English.
Electronic searches
The most recent search was on 24 August 2020. We searched the Cochrane Stroke Group Trials Register, the Cochrane Central Register of Controlled Trials (CENTRAL) (the Cochrane Library, 2020, Issue 7) (Appendix 1), MEDLINE Ovid (last searched 24 August 2020) (Appendix 2), Embase Ovid (last searched 24 August 2020) (Appendix 3), US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov), WHO International Clinical Trials Registry Platform (ICTRP), and forward reference/cited reference searching.
We developed the search strategies for CENTRAL, MEDLINE Ovid, and Embase Ovid with the help of the Cochrane Stroke Group Information Specialist and we updated the search strategies to include any new vocabulary terms and drug names.
Searching other resources
In 1998, the authors at the time searched the registers of the Antiplatelet Trialists' Collaboration (ATC 1994a; ATC 1994b) and MedStrategy (MedStrategy 1995). They contacted the following pharmaceutical companies who marketed antiplatelet agents for details of any trials, particularly unpublished ones: Roussel‐Uclaf (defibrotide), Syntex and Sanofi Winthrop (ticlopidine), Otsuka (cilostazol), Eisai (satigrel), Tokyo Tanebe Seiyaku (sarpolgrelate), Kanebo (KBT 3022), and Takeda Chemical Company (isbogrel). For this version of the review, we did not update the previous searches of the Antiplatelet Trialists' Collaboration register (no longer available), MedStrategy, or make any further contact with pharmaceutical companies. However, we did contact authors of newly included studies for any additional unpublished data. One group responded with additional data that was not relevant to the immediate question of this review (Zhao 2017).
Data collection and analysis
The review authors of this update performed data collection and analysis as per Cochrane guidelines without deviation from the planned protocol.
Selection of studies
Two review authors operating in pairs (TC and SB formed the first pair and MK and RC formed the second pair) read the titles, abstracts, and keywords of all records identified from the searches of the electronic bibliographic databases and excluded studies that were clearly irrelevant. JM and LB arbitrated disagreements at the screening stage. We obtained the full texts of the remaining studies and LB and JM selected trials for inclusion based on our defined criteria. The two review authors resolved any disagreements by discussion.
Data extraction and management
For each version of the review, two review authors (TC and SB) independently extracted the data on methods, participants, interventions, outcomes, and results, and recorded the information on a data extraction form. We sought data on the number of participants with each outcome event by allocated treatment group, irrespective of compliance and whether or not the participant was subsequently deemed ineligible or otherwise excluded from treatment or follow‐up, to allow an intention‐to‐treat analysis. We also sought data on whether CT or MR scanning was performed prior to randomisation. The same two review authors cross‐checked all extracted data and resolved any disagreements by discussion. If any of the above data were unavailable from the publications, we sought further information by contacting the study authors.
Assessment of risk of bias in included studies
Two review authors (TC and LB) independently assessed risk of bias using Cochrane's tool for assessing risk of bias (RoB1) (Higgins 2011). We resolved disagreements through discussion with all review authors. The RoB1 tool consists of seven categories: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. We have included the RoB1 tool and its components in Appendix 4. We classified risk of bias as low, high, or unclear, according to guidance produced on using the tool and we have included a narrative summary of the number of studies in each of these categories for each domain (Higgins 2011).
Measures of treatment effect
We calculated Peto odds ratios (ORs), that is the ratio of the odds of an outcome among treatment‐allocated participants to the corresponding odds amongst controls) with 95% confidence intervals (CI), using Review Manager 5 (Review Manager 2020).
Unit of analysis issues
There were no specific unit of analysis issues.
Dealing with missing data
If any data were not available from the publications, we sought further information from the authors or the relevant pharmaceutical company. When data were missing and could not be derived, we used the published analysis.
Assessment of heterogeneity
We assessed the extent of heterogeneity between trial results using the I2 statistic, which measures the percentage of the variability in effect estimates attributable to heterogeneity rather than sampling error (Higgins 2020). We considered a value greater than 50% as substantial heterogeneity.
Assessment of reporting biases
We assessed trials for selective outcome reporting and presented the results as risk of bias tables. We assessed publication bias for the primary outcome and for death within the scheduled treatment period using funnel plots.
Data synthesis
We calculated ORs with 95% CIs using the Peto fixed‐effect method (ATC 1994a) in Review Manager 5 (Review Manager 2020). We also calculated the number needed to treat for an additional beneficial outcome (NNTB) and the number of events avoided per 1000 people treated for each outcome if the result was statistically significant. We performed these calculations using the online calculator provided by the Cochrane Stroke Group at www.dcn.ed.ac.uk/csrg/entity/entity_NNT2.asp. The control event rate applied was based on the mean of the relevant control event rates in CAST 1997 and IST 1997.
Subgroup analysis and investigation of heterogeneity
We prespecified the following subgroup analyses for the primary outcome of this review.
Type of oral antiplatelet agent used.
Trials in which all participants had intracerebral haemorrhage excluded by CT or MR scanning prior to trial randomisation.
Trials in which participants were recruited within 48 hours of their stroke.
We performed an additional post‐hoc subgroup analysis among participants with intracerebral haemorrhages inadvertently randomised in the trials. Two trials included a number of participants who did not have a CT scan until after randomisation (CAST 1997; IST 1997). Data on those participants in whom the diagnosis of the initial event leading to randomisation was haemorrhagic stroke and who were dead or dependent at follow‐up were reported in the IST publication (IST 1997), and were kindly supplied on request from the CAST trial (CAST 1997).
Sensitivity analysis
We planned several prespecified sensitivity analyses limited to the primary outcome (death or dependency) of the review, including:
only trials with adequate concealment of randomisation;
only trials with blinding of participants, personnel, and outcome assessment;
only trials at low risk of bias due to completeness of follow‐up.
In the sensitivity analysis, we compared two ORs by assessing whether the difference in the natural logarithms of the two ORs (lnOR) was significantly different from zero using a normal approximation. The variance of each lnOR was estimated as the reciprocal of the variance of the O‐E statistic given in Review Manager 2020.
Following analysis of the available evidence it became apparent that three of the prespecified analyses (trials in which participants were randomised within 48 hours, trials with adequate concealment of randomisation, and trials with CT scans prior to randomisation) were inappropriate; this is explained in the Results section.
Summary of findings and assessment of the certainty of the evidence
We assessed the overall certainty of the evidence for each outcome using the GRADE approach (Schünemann 2013). We assessed the following factors when deciding whether to downgrade or upgrade the certainty of the evidence for each outcome.
Downgrade:
risk of bias;
inconsistency;
indirectness;
imprecision;
publication bias.
Upgrade:
large effect;
dose–response gradient;
plausible confounding effect.
We downgraded the evidence for each outcome by one level where there was a serious limitation, and by two factors where there was a very serious limitation. Our review included only RCTs and so were considered high certainty prior to downgrading. We categorised studies as high, moderate, low, or very low certainty based on these domains. We prepared a summary of findings table using GRADEpro (GRADEpro GDT) and following recommendations in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2020). Two review authors (LB and TC) independently decided GRADE assessments and resolved disagreements by discussion.
We assessed the following outcomes in the summary of findings table:
death or dependence at end of follow‐up;
death from any cause during follow‐up;
confirmed symptomatic PE diagnosed during life, or at autopsy (symptomatic or not) within the scheduled treatment period;
recurrent stroke during treatment period;
symptomatic ICH during treatment period;
major extracranial haemorrhage during treatment period;
complete recovery from stroke.
Results
Description of studies
Randomised trials comparing oral antiplatelet therapy (started within 14 days of the stroke) with control in people with definite or presumed ischaemic stroke.
Results of the search
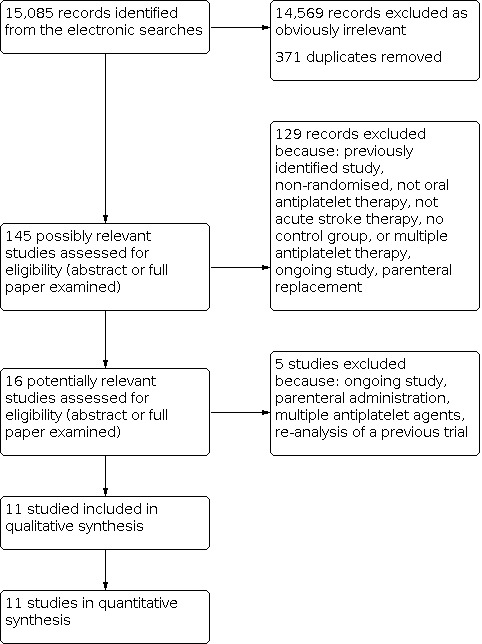
We identified 15,085 records from the electronic searches. After eliminating duplicates and non‐relevant studies from the titles and abstracts, we selected 145 possibly relevant studies. After examining the abstracts, or in some cases the full papers, 129 records did not meet the eligibility criteria for the following reasons: previously identified studies, non‐randomised studies, not of an oral antiplatelet therapy, not acute stroke therapy, no control group, an ongoing study, parenteral replacement used, or multiple antiplatelet agents used (the latter are reviewed in a separate Cochrane Review (Kamal 2012)). This process left 16 potentially relevant studies. Of these, five did not fulfil all the inclusion criteria and are listed in the Characteristics of excluded studies table. We included three new studies (Di Cesare 2016; Khatri 2018; Zhao 2017). A PRISMA flowchart of study selection is shown in Figure 1.
1.
Flow diagram.
Included studies
We included 11 studies involving 42,226 participants (see Characteristics of included studies table). One of the included trials (53 participants) remains unpublished (Turpie 1983). Most participants in the review were elderly, with a significant proportion of participants over 70 years of age. For example, 61% of participants enrolled in the International Stroke Trial were aged 70 years or older (IST 1997). Males and females were almost equally represented in the trials.
Antiplatelet regimens tested
Two studies contributed 96% of the data (CAST 1997; IST 1997). IST 1997 was an open‐treatment, blinded outcome study with a factorial design; participants were allocated to 14 days of treatment with aspirin 300 mg, heparin, both, or neither; that is, the trial tested the effects of aspirin in the presence and absence of heparin (and vice versa) (IST 1996). CAST 1997 was a double‐blind randomised trial of one month's treatment with either aspirin 160 mg or matching placebo. In MAST‐I 1995 (a factorial trial of streptokinase and aspirin involving 309 participants), only those participants randomised to aspirin alone and the no treatment group were included in this review as there was a significant interaction between aspirin and streptokinase which invalidated the aspirin plus streptokinase versus streptokinase alone comparison. Khatri 2018 randomised participants to either oral aspirin and an intravenous (IV) placebo or oral placebo and IV alteplase. Other antiplatelet regimens compared with control were: aspirin (Rödén‐Jüllig 2003), ticlopidine (Ciuffetti 1990; Turpie 1983; Utsumi 1988), clopidogrel loading dose (Zhao 2017), PF‐03049423 (Di Cesare 2016), and aspirin plus dipyridamole (Pince 1981).
Time window for inclusion
Trials included participants randomised within six hours (MAST‐I 1995), 12 hours (Ciuffetti 1990), 24 to 78 hours (Di Cesare 2016),48 hours (CAST 1997; IST 1997, Zhao 2017), 72 hours (Rödén‐Jüllig 2003), or six days (Pince 1981) of stroke onset. In two trials, the formal entry criterion was a stroke within the previous four weeks (Turpie 1983; Utsumi 1988), but, as most participants were entered within two weeks, we included them in this review. Data on only those participants entered within two weeks were not available from the authors or the pharmaceutical company.
Exclusion criteria
The two main trials in the review did not precisely specify exclusion criteria as they used the uncertainty principle, but suggested that these might include participants thought to be at high risk of adverse effects (e.g. clotting disorders, hepatic or renal failure) or those with a small likelihood of worthwhile benefit (CAST 1997; IST 1997).
Computer tomography scanning
Three trials adequately excluded people with intracerebral haemorrhage by CT scanning all possible participants before entry into the trial (Ciuffetti 1990; MAST‐I 1995; Rödén‐Jüllig 2003). Three trials adequately excluded people with intracerebral haemorrhage by including people with confirmed cerebral infarction on either a CT or MR scan (Di Cesare 2016; Khatri 2018; Zhao 2017). Two trials performed a CT scan in almost all participants; in these trials, clinicians had to have a low suspicion of ICH prior to randomisation (CAST 1997; IST 1997). In CAST 1997, 87% had a CT prior to randomisation; by discharge this number had risen to 94%. In IST 1997, 67% were scanned before randomisation and 29% after randomisation, so that overall 96% of participants were scanned. Two trials performed no CT scans (Pince 1981; Turpie 1983), and in Utsumi 1988 the use of CT scanning was uncertain. As a result of the variable use of prerandomisation CT scanning, some people with intracerebral haemorrhage were inadvertently entered in the trials and these were included in the main analyses of this review. This may have biased the results against antiplatelet agents, although this is unlikely given the relatively small numbers of participants involved. Furthermore, the inclusion of these people may actually make the conclusions of the review more broadly applicable, since some hospitals admitting people with acute stroke do not have access to CT scanning and so acute treatment may have to be started without definite knowledge of the pathological type of stroke.
Stroke severity at entry
There appeared to be some variation in stroke severity among the included trials. For example, in the control group of IST 1997 early death was recorded as 9%, but was only 4% in CAST 1997, even though CAST 1997 assessed participants at four weeks versus two weeks for IST 1997. Rödén‐Jüllig 2003 used a Scandinavian Stroke Supervision Scale score of one point or more as the inclusion criterion. Alternatively, Khatri 2018 only included people with deficits judged not to be clearly disabling at presentation.
Scheduled duration of trial treatment
The scheduled duration of treatment varied from five days (Rödén‐Jüllig 2003), to three months (Utsumi 1988). The scheduled follow‐up period varied from 10 days (Pince 1981), to six months (IST 1997; MAST‐I 1995).
Measures of outcome
Clinically important outcomes were poorly reported in the smaller trials. Seven studies evaluated death or dependence at the end of follow‐up (see Table 1). Most trials used comparable definitions of dependence. They included: the modified Rankin Disability Scale (three or greater) (CAST 1997; MAST‐I 1995; Zhao 2017); and needing help from another person with daily activities (IST 1997). For Rödén‐Jüllig 2003, we used 'living in an institution' as equivalent to being dependent. Three trials used validated scales (CAST 1997 used Bamford 1989; IST 1997 used Dennis 1997; MAST‐I 1995 used Candelise 1994). The primary outcome of two trials was favourable functional outcome, defined as modified Rankin Disability Scale less than 2 (Di Cesare 2016) or less than 1 (Khatri 2018). In two trials, the primary outcome was DVT (Pince 1981; Turpie 1983); these trials did not formally evaluate survival free of dependency for activities of daily living. Progression of stroke symptoms measured by the Scandinavian Stroke Supervision Scale was the primary outcome event of Rödén‐Jüllig 2003. Recurrence of stroke or speed of infarct progression was the primary outcome of Zhao 2017. Further additional outcomes included death from all causes at end of follow‐up, PE, symptomatic ICH, major extracranial haemorrhage, or complete recovery from stroke (see Table 1). No trials systematically assessed quality of life.
Excluded studies
We excluded five trials for a variety of reasons (see Characteristics of excluded studies table).
Studies awaiting classification
There are no studies awaiting classification.
Ongoing studies
We found no ongoing studies.
Risk of bias in included studies
Baseline characteristics
Risk of bias of all 11 studies is summarised in Figure 2 and Figure 3. Turpie 1983 could not be accessed, and adequate assessment of risk of bias using the RoB1 tool could not be performed, therefore unclear risk of bias is reported for each category. The large numbers of participants randomised in CAST 1997 and IST 1997 resulted in an equal distribution of baseline participant characteristics between the treatment and control groups. In two smaller trials (MAST‐I 1995; Utsumi 1988), there were significant imbalances between the treatment and control groups in potentially important baseline factors (level of consciousness in Utsumi 1988, and time to treatment in MAST‐I 1995), but these differences cannot bias the overall results due to the small numbers of participants involved.
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Random sequence generation
Eight trials had low risk of bias for this category because they explicitly stated an appropriate method of random sequence generation (CAST 1997; Di Cesare 2016; IST 1997; Khatri 2018; MAST‐I 1995; Rödén‐Jüllig 2003; Utsumi 1988; Zhao 2017). Ciuffetti 1990 had high risk of bias because groups were divided based upon age, sex, and score on Hachinski's Scale, and, therefore, the participants were not randomised. Pince 1981 was deemed unclear risk of bias as a method of random sequence generation was not directly reported. Turpie 1983 could not be accessed.
Allocation concealment
Seven trials had low risk of bias for allocation concealment because they described the method used to conceal the allocation sequence in sufficient detail (CAST 1997; Di Cesare 2016; IST 1997; MAST‐I 1995; Rödén‐Jüllig 2003; Utsumi 1988; Zhao 2017). One trial was at high risk of bias because it was not a randomised study, and so there was no allocation concealment (Ciuffetti 1990). Two studies were at unclear risk of bias as there was no statement regarding allocation concealment (Khatri 2018; Pince 1981). Turpie 1983 could not be accessed.
Blinding of participants and personnel
Four studies had low risk of bias as it was clearly stated that participants and personnel were blinded from knowledge of which intervention a participant received and details of how this was done (Di Cesare 2016; Khatri 2018; Pince 1981; Rödén‐Jüllig 2003). Seven studies had unclear risk of bias because there was insufficient evidence to judge whether participants and personnel were truly blinded (CAST 1997; Ciuffetti 1990; IST 1997; Khatri 2018; MAST‐I 1995; Utsumi 1988; Zhao 2017). Three of these studies reported that they were double‐blind (Ciuffetti 1990; Utsumi 1988; Zhao 2017). However, it was not reported how blinding was done, or whether participants were definitely blinded. Turpie 1983 could not be accessed.
Blinding of outcome assessment
Three studies had low risk of bias as they clearly described the measures used to blind outcome assessors from knowledge of which intervention a participant received (Di Cesare 2016; MAST‐I 1995; Rödén‐Jüllig 2003). Seven studies had unclear risk of bias because there was insufficient evidence to judge whether outcome assessors were blinded or not. Turpie 1983 could not be accessed.
Incomplete outcome data
Ten trials had low risk of bias for incomplete outcome data (CAST 1997; Ciuffetti 1990; Di Cesare 2016; IST 1997; Khatri 2018; MAST‐I 1995; Pince 1981; Rödén‐Jüllig 2003; Utsumi 1988; Zhao 2017). Khatri 2018 was at low risk of bias as, although the trial lost 22% of participants to follow‐up, the missing data were imputed via a hot‐deck method to account for missing outcome data. Turpie 1983 could not be accessed.
Selective reporting
Eight studies had low risk of bias for bias in selection of reported results (CAST 1997; Ciuffetti 1990; Di Cesare 2016; IST 1997; Khatri 2018; MAST‐I 1995; Rödén‐Jüllig 2003; Zhao 2017). Two studies had unclear risk of bias in selection of reported results because a prespecified analysis plan was not clearly reported (Pince 1981; Utsumi 1988). Funnel plots did not suggest substantial publication bias in respect of the primary outcome (Figure 4), or death at the scheduled end of follow‐up (Figure 5). Turpie 1983 could not be accessed.
4.

Funnel plot of comparison: 1 Antiplatelet agent versus control in acute presumed ischaemic stroke, outcome: 1.1 Death or dependence at end of follow‐up.
5.

Funnel plot of comparison: 1 Antiplatelet agent versus control in acute presumed ischaemic stroke, outcome: 1.2 Deaths from all causes during treatment period.
Other potential sources of bias
Turpie 1983 could not be accessed, and, therefore, adequate assessment of risk of bias using the RoB 1 tool could not be done (Figure 2; Figure 3). Pince 1981 was a thesis published in French and other potential sources of bias could not be fully excluded based on the information available.
Effects of interventions
See: Table 1
Outcome 1.1 (primary outcome): death or dependence at end of follow‐up
For the primary outcome, antiplatelet therapy was associated with a significant reduction in the odds of death or being dependent at final follow‐up (OR 0.95, 95% CI 0.91 to 0.99; P = 0.008 7 RCTs, 42,034 participants; moderate‐certainty evidence; Analysis 1.1). For aspirin, for every 1000 people treated, 13 people would avoid death or dependency (NNTB 79; Table 2). A prespecified sensitivity analysis (data not shown in forest plots) showed no difference in the effect of treatment on death or dependence at final follow‐up between trials that were double‐blind (OR 0.95, 95% CI 0.90 to 1.01) or not (OR 0.94, 95% CI 0.89 to 1.00). A post‐hoc subgroup analysis (data not shown in forest plots) restricted to the subset of participants in whom the initial stroke was due to intracerebral haemorrhage and who had been inadvertently randomised in the trials (597 in IST 1997 and 174 in CAST 1997) showed that the odds of a poor outcome were lower among those allocated to aspirin (OR 0.68, 95% CI 0.49 to 0.94), although the CIs were wide (Keir 2002). In CAST 1997, 11 participants in the aspirin group and five participants in the control group were not accounted for in this analysis. Assuming a worst‐case scenario (i.e. where all participants in the experimental group were assumed to be either dead or dependent, and all participants in the control group recovered fully), the result was no longer statistically significant (OR 0.74, 95% CI 0.53 to 1.03). Thus, these data do not provide clear evidence of any harm to people with haemorrhagic stroke inadvertently treated with aspirin.
1.1. Analysis.

Comparison 1: Antiplatelet drug versus control in acute presumed ischaemic stroke, Outcome 1: Death or dependence at end of follow‐up
1. Absolute risk reductions of aspirin treatment in acute stroke.
| Outcome | Control event ratea |
No of events avoidedb (per 1000 people treated (95% CI)) |
NNTB or NNTHb |
| Death or dependence at end of follow‐up | 0.47 | 13 (3 to 23) | NNTB 79 (43 to 400) |
| Deaths from all causes during follow‐up | 0.13 | 9 (2 to 15) | NNTB 108 (66 to 436) |
| Pulmonary embolism during treatment period | 0.01 | 1 (0 to 2) | NNTB 693 (427 to 6700) |
| Recurrent ischaemic/unknown stroke during treatment period | 0.03 | 7 (4 to 10) | NNTB 140 (104 to 248) |
| Symptomatic intracranial haemorrhage during treatment period | 0.01 | −2 (i.e. 2 extra) (−4 to 0) | NNTH 574 (254 to 126,010) |
| Any recurrent stroke/intracranial haemorrhage during treatment | 0.04 | 5 (1 to 8) | NNTB 200 (123 to 868) |
| Major extracranial haemorrhage during treatment period | 0.01 | −4 (i.e. 4 extra) (−7 to −2) | NNTH 245 (153 to 481) |
| Complete recovery from stroke (post hoc) | 0.26 | 11 (2 to 21) | NNTB 89 (49 to 523) |
CI: confidence interval; NNTB: number needed to treat for an additional beneficial outcome; NNTH: number needed to treat for an additional harmful outcome.
aEstimated from the mean of the control event rate in the two largest trials (CAST 1997; IST 1997). bEstimated by applying the Peto odds ratio for the outcome for studies of aspirin. Calculator is available at: www.dcn.ed.ac.uk/csrg/entity/entity_NNT2.asp.
Outcome 1.2: deaths from any cause during treatment period
Antiplatelet therapy was associated with a nominally significant reduction in death at the end of the treatment period (OR 0.92, 95% CI 0.85 to 1.00; P = 0.05; 8 studies, 41,483 participants; very low‐certainty evidence; Analysis 1.2).
1.2. Analysis.

Comparison 1: Antiplatelet drug versus control in acute presumed ischaemic stroke, Outcome 2: Deaths from any cause during treatment period
Outcome 1.3: deaths from any cause during follow‐up
Antiplatelet therapy was associated with a reduction in the odds of death at a final follow‐up of greater than one month (OR 0.93, 95% CI 0.87 to 0.98; P = 0.01; 10 studies, 41,929 participants; very low‐certainty evidence; Analysis 1.3). For aspirin, for every 1000 people treated nine people would avoid death (NNTB 108; Table 2). A prespecified sensitivity analysis showed no difference in the effect of treatment on death at final follow‐up between trials which were of a double‐blind design (OR 0.87, 95% CI 0.76 to 1.00) or not (OR 0.94, 95% CI 0.87 to 1.00).
1.3. Analysis.

Comparison 1: Antiplatelet drug versus control in acute presumed ischaemic stroke, Outcome 3: Deaths from any cause during follow‐up
Outcome 1.4: deep vein thrombosis during treatment period
Two trials that included randomised data from 133 participants (less than 0.3% of participants included in the overall review) sought to systematically determine the effect of antiplatelet agents on the occurrence of symptomatic or asymptomatic DVT at the end of the treatment period, as detected by I125 fibrinogen scanning (Pince 1981; Turpie 1983). DVT occurred in 16/67 (23.9%) of participants allocated to antiplatelet treatment and 19/66 (28.8%) of participants allocated to control (OR 0.78, 95% CI 0.36 to 1.67; P = 0.52; 2 RCTs, 133 participants; very low‐certainty evidence; Analysis 1.4). There was substantial heterogeneity between these two trials (I2 = 82.9%), one of which involved ticlopidine and one a combination of aspirin and dipyridamole. This heterogeneity may have been due to chance or to the fact that the time between stroke onset and starting treatment varied in the two trials: less than six days in Pince 1981, and less than four weeks in Turpie 1983. Sensitivity analyses were not possible for this outcome due to the limited amount of data.
1.4. Analysis.

Comparison 1: Antiplatelet drug versus control in acute presumed ischaemic stroke, Outcome 4: Deep venous thrombosis during treatment period
Outcome 1.5: pulmonary embolism during treatment period
No trial systematically sought asymptomatic PE by performing ventilation‐perfusion scans or using CTPA in all participants at the end of treatment. Antiplatelet therapy was associated with a reduction in the odds of PE (OR 0.71, 95% CI 0.53 to 0.96; P = 0.03; 7 RCTs, 41,042 participants; very low‐certainty evidence; Analysis 1.5). For aspirin, for every 1000 people treated, one person would avoid PE (NNTB 693; Table 2). This may be an underestimate if antiplatelet treatment prevented both major and minor PE since no trial systematically sought minor PE.
1.5. Analysis.

Comparison 1: Antiplatelet drug versus control in acute presumed ischaemic stroke, Outcome 5: Pulmonary embolism during treatment period
Outcome 1.6: recurrent ischaemic or unknown stroke during treatment period
Data on recurrent stroke were available from nine trials, which systematically sought to record early recurrent strokes that were definitely ischaemic (CT scan excluded haemorrhage) or probably ischaemic, that is in which the cerebral pathology was unknown because brain imaging had not been performed. A total of 495/526 reported recurrent ischaemic strokes occurred in CAST 1997 and IST 1997. The use of antiplatelet agents (chiefly aspirin) was associated with a reduction in recurrent ischaemic strokes (OR 0.79, 95% CI 0.70 to 0.88; P < 0.00001; 9 RCTs, 41,625 participants; very low‐certainty evidence; Analysis 1.6). For every 1000 people treated with aspirin, seven people would avoid recurrent ischaemic stroke (NNTB 140; Table 2).
1.6. Analysis.

Comparison 1: Antiplatelet drug versus control in acute presumed ischaemic stroke, Outcome 6: Recurrent ischaemic/unknown stroke during treatment period
Outcome 1.7: symptomatic intracranial haemorrhage during treatment period
There were data for nine trials. It was unclear (even after correspondence) how three small trials detected haemorrhages (Pince 1981; Turpie 1983; Utsumi 1988). However, it was likely that participants who deteriorated neurologically were scanned using CT, or that haemorrhages were found at autopsy. In one trial, four participants, two in each group, were excluded after randomisation because they had intracerebral haemorrhage (Pince 1981). These participants were included as having symptomatic ICH in this analysis. In the trials where participants did not have a CT scan before randomisation, it was difficult to determine whether any ICH first identified after treatment had been started was new or had been present before randomisation. For the purposes of this analysis, we assumed that all such haemorrhages were new. Antiplatelet therapy increased the odds of symptomatic ICH, but this was not statistically significant (OR 1.18, 95% CI 0.97 to 1.44; P = 0.10; 9 RCTs, 41,652 participants; very low‐certainty evidence; Analysis 1.7). For every 1000 people treated with aspirin, two people would have a symptomatic ICH; the number needed to treat to harm (NNTH) was 574 (Table 2). There was the possibility of some bias within these data as there may have been a lower threshold for rescanning participants who had deteriorated clinically if they were known to be receiving antithrombotic treatment (e.g. in IST 1997, which was not blinded).
1.7. Analysis.

Comparison 1: Antiplatelet drug versus control in acute presumed ischaemic stroke, Outcome 7: Symptomatic intracranial haemorrhage during treatment period
Outcome 1.8: recurrent stroke or intracranial haemorrhage during treatment period
Immediate use of antiplatelet agents reduced the odds of ischaemic stroke but also appeared to increase the odds of symptomatic ICH. An outcome which combines these two (without double counting, that is participant allowed only one of ischaemic stroke or ICH with the first event being the one which was included) was useful for assessing the net short‐term effects of antiplatelet agents. However, symptomatic ICHs are more likely to cause death or disability than ischaemic recurrences, and so the severity of the recurrence also needed to be considered. No trial reported the severity of recurrences.
Antiplatelet therapy was associated with a net reduction in the odds of any recurrent stroke/ICH (OR 0.88, 95% CI 0.79 to 0.97; P = 0.01; 7 RCTs, 41,042 participants; very low‐certainty evidence; Analysis 1.8). For every 1000 people treated with aspirin, five people would avoid recurrent ischaemic stroke or symptomatic ICH (NNTB 200; Table 2).
1.8. Analysis.

Comparison 1: Antiplatelet drug versus control in acute presumed ischaemic stroke, Outcome 8: Recurrent stroke/intracranial haemorrhage during treatment period
Outcome 1.9: major extracranial haemorrhage during treatment period
Allocation to antiplatelet agents was associated with a significant increase in major extracranial haemorrhage (OR 1.69, 95% CI 1.35 to 2.11; P < 0.00001; 7 RCTs, 41,042 participants; very low‐certainty evidence; Analysis 1.9). For every 1000 people treated with aspirin, four people would have a symptomatic extracranial haemorrhage (NNTH 245; Table 2).
1.9. Analysis.

Comparison 1: Antiplatelet drug versus control in acute presumed ischaemic stroke, Outcome 9: Major extracranial haemorrhage during treatment period
Outcome 1.10: complete recovery from stroke (post hoc)
Two trials including randomised data on 40,541 participants (98% of participants included in the overall review) reported complete recovery from stroke (CAST 1997; IST 1997). Allocation to antiplatelet therapy increased the odds of a complete recovery (OR 1.06, 95% CI 1.01 to 1.11; P = 0.01; 2 RCTs, 40,541 participants; moderate‐certainty evidence; Analysis 1.10). For every 1000 people treated with aspirin, an extra 11 people would make a complete recovery (NNTB 89; Table 2).
1.10. Analysis.

Comparison 1: Antiplatelet drug versus control in acute presumed ischaemic stroke, Outcome 10: Complete recovery from stroke (post hoc)
Re‐evaluation of the planned sensitivity and subgroup analyses in light of the available data
After an evaluation of the available evidence from the randomised trials, it became apparent that three of the planned subgroup sensitivity analyses were inappropriate. These were the analyses restricted to trials: in which participants were randomised within 48 hours of the stroke; with adequate concealment of randomisation; and with 100% CT scans prior to randomisation. As most data came from trials that randomised participants within 48 hours of stroke onset, the planned subgroup sensitivity analysis evaluating the effects of treatment beyond 48 hours was largely uninformative. Similarly, the analyses based on the concealment of treatment allocation were uninformative about trials with inadequate concealment as these trials contributed so few data. An analysis based on whether or not all participants had brain imaging prior to randomisation to rule out haemorrhage would exclude CAST 1997 and IST 1997, and would, therefore, disregard 98% of the data. An individual participant data analysis has examined the effect subdivided by whether participants had CT prior to randomisation or not; there was no clear heterogeneity of effect (Chen 2000).
Discussion
Strength of evidence of benefit on major outcomes
This systematic review once again reliably emphasised that antiplatelet therapy is safe and effective in the acute phase of ischaemic stroke. The conclusion is based on data from over 40,000 participants. Ninety‐six per cent of the data came from two trials of medium‐dose aspirin, that is 160 mg to 300 mg daily (CAST 1997; IST 1997). Overall, antiplatelet therapy with aspirin started within 48 hours of onset of presumed ischaemic stroke was beneficial. Although associated with a small but definite risk of bleeding, this hazard was offset by the reduction in recurrent ischaemic stroke. The analysis of the effects of aspirin among participants who were first scanned after randomisation and who turned out to have had a haemorrhagic stroke was reassuring.
The benefits of a short course of antiplatelet therapy in acute ischaemic stroke compare very favourably with longer‐term antiplatelet therapy for secondary prevention in vascular disease. Two to four weeks of treatment in IST 1997 and CAST 1997 resulted in about eight fewer deaths per 1000 participants treated, whereas, in long‐term secondary prevention, one month of antiplatelet therapy typically avoids fewer than one death per 1000 (ATC 2002). Similarly, long‐term antiplatelet use prevents about one recurrent stroke per 1000 people per month (ATC 1994a; ATC 2002), whereas, in the acute phase of ischaemic stroke, one month of antiplatelet therapy prevents about four recurrent strokes per 1000 people (seven fewer ischaemic strokes and three extra haemorrhagic strokes).
The main conclusions of this review have not changed from the last update, despite the exclusion of the trials of IV antiplatelet agents. Importantly, there now is no equipose in comparing antiplatelet therapy to placebo therapy given the worldwide acceptance of antiplatelet therapy as the standard of care.
Effects on venous thromboembolism
Aspirin reduced the odds of PE by 29%, but, since the reported rate of PE was low, the absolute benefit, one event prevented per 1000 participants treated, is very small. However, if there was a substantial under‐ascertainment of PE in the trials included in this systematic review, then the absolute benefits of aspirin may have been underestimated. Clinical series report a range of 0% to 3% for symptomatic PE (Davenport 1996). If the observed 29% reduction in the odds of PE was applied to a population with a 3% risk of PE the absolute reduction would increase to eight for every 1000 people treated. It seems reasonable to conclude that routine use of aspirin alone in people with acute ischaemic stroke will reduce the risk of DVT and PE somewhat yet not be associated with any substantial excess of intracerebral haemorrhages. It remains unclear whether aspirin alone is as good as heparin alone at preventing venous thromboembolism in acute ischaemic stroke, but data from IST 1997 suggest no statistically or clinically significant difference between aspirin and heparin in the prevention of PE.
Robustness of the findings
The sensitivity analyses have shown that the conclusions about the benefits of antiplatelet therapy are robust. A meta‐analysis based on individual participant data from CAST 1997 and IST 1997 confirmed this (Chen 2000). It showed no clear heterogeneity of treatment effect with delay in starting aspirin, age, gender, stroke type, infarct subtype, the presence of impaired consciousness or the presence or absence of atrial fibrillation. These results suggest that a wide variety of people with ischaemic stroke are likely to benefit from antiplatelet therapy with aspirin (Chen 2000). As a result of the strength of evidence, aspirin is now recommended as a standard therapy. Four major evidence‐based guidelines make strong recommendations for the routine use of aspirin for all people with acute ischaemic stroke (CSS 2010; ESO 2008; Jauch 2013; RCP Guideline 2016).
Public health impact
It can be argued that, although effective, the net benefits of aspirin are rather small when compared with the effects of stroke unit care (OR of death or dependency 0.79, 95% CI 0.68 to 0.90) (SUTC 2013), and thrombolysis with tissue plasminogen activator within three hours of stroke (OR of death or dependency 0.71, 95% CI 0.52 to 0.96) (Wardlaw 2009). However, aspirin is inexpensive, easy to administer, and safe, which increases its potential public health impact worldwide and especially in low‐ to middle‐income countries. In 2019, stroke ranked second in the leading causes of disability‐adjusted life years (DALYs) in the age groups 50 to 74 years and 75 years and older (GBD 2019). In 2017, there were 11.9 million incident, 104.2 million prevalent, 6.2 million cases of stroke, and 132.1 million stroke‐related DALYs (Krishnamurthi 2020). The risk of death following stroke is highest in the immediate aftermath and treatment strategies should be aimed at lowering the risk of mortality during this period (Minhas 2017). If treatment with aspirin prevents seven deaths per 1000, then an additional 36,400 lives could be saved worldwide per year with substantial numbers of survivors avoiding long‐term disability.
Aspirin dose and route of administration
The benefits of aspirin in acute stroke are drawn from trials that tested a dose of aspirin between 160 mg and 330 mg daily. In acute myocardial infarction, 160 mg is the lowest dose that has been shown to be effective (ATC 1994a; ATC 2002; Dalen 2006; Patrono 1998). Lower doses of aspirin are effective for long‐term secondary stroke prevention but have not been evaluated in acute stroke. There is some (but not abundant) evidence that at least 120 mg of aspirin is needed to acetylate all circulating platelets within a short period of time (Patrono 1994; van Gijn 1992). There is also some experimental evidence that a dose of 160 mg to 300 mg of aspirin daily is required in the acute phase of an ischaemic cerebral or cardiac event in order to achieve rapid inhibition of thromboxane biosynthesis (Patrono 1998; van Kooten 1994; van Kooten 1997). For people who can swallow, aspirin can be given by mouth. However, as many people with stroke are unable to swallow, another route may need to be used on occasions. CAST 1997 gave aspirin via a nasogastric tube, and IST 1997 gave 100 mg of the lysine salt of aspirin as a rectal suppository.
Other antiplatelet agents
The indirect comparisons of different agents in this review showed no evidence of significant heterogeneity of effect between the different agents tested, aspirin alone, ticlopidine alone, the combination of aspirin and dipyridamole. However, the data from the non‐aspirin regimens were extremely limited and such indirect comparisons are unreliable (ATC 1994a). The focus of current research is on comparing the effects of short‐term (30 days to three months) combination therapy with single agents, chiefly in people with TIA and minor stroke (CHANCE 2013; POINT; TARDIS); these regimens are the subject of a separate review (Naqvi 2020). In this update, loading with clopidogrel as compared to maintenance (and placebo) demonstrated no discernible benefit on preventing recurrent stroke (Zhao 2017).
Combination of aspirin with anticoagulants
Another question that remains unanswered is whether the addition of low‐dose subcutaneous heparin to aspirin could further reduce the risk of DVT and PE without unduly increasing the risk of intracranial and extracranial haemorrhage. One systematic review of the randomised trials of anticoagulants in acute myocardial infarction showed that the addition of IV or subcutaneous heparin did not add worthwhile extra benefit to the use of antiplatelet therapy alone (Collins 1996). However, the addition of low‐dose subcutaneous heparin to aspirin might be more effective in acute stroke. The only trial that provided a direct randomised comparison of aspirin with aspirin plus low‐dose heparin was IST 1997, yet the available data did not provide conclusive evidence that the combination was more effective than aspirin alone. The question of whether or not to add low‐dose heparin to aspirin can, therefore, only be answered reliably by a further, much larger trial that randomly allocates participants to aspirin or aspirin plus low‐dose subcutaneous heparin. Symptomatic PE (and ICH) are infrequent in people with ischaemic stroke. Therefore, any proposed trial would need to include several 10s of 1000s of participants in order to provide reliable evidence on the size of any difference in the effects of these two antithrombotic regimens.
Time window for benefit from aspirin
There was clear evidence of net benefit when aspirin therapy was started within 48 hours of stroke onset. A more detailed meta‐analysis based on individual participant data from IST 1997 and CAST 1997 showed no clear evidence that the benefit declined with increasing time from stroke onset up to 48 hours (Chen 2000). The evidence on the effects of starting treatment at more than 48 hours and within 14 days of onset was extremely limited in this review. However, taken with the data from the Antithrombotic Trialists Collaboration, the evidence is very strongly suggestive that starting after 48 hours but within 14 days of onset and continuing long term is highly likely to be of net benefit (ATC 2002).
Interaction with thrombolytic therapy
Thrombolytic therapy for acute ischaemic stroke within 4.5 hours of symptom onset has received regulatory approval (or is recommended in guidelines) in many places, and is the subject of ongoing research. Since antiplatelet and thrombolytic therapy can cause serious bleeding, it is important to assess the evidence for any interaction between the two agents. The subject is dealt with in some detail in the Cochrane systematic review of thrombolytic therapy (Wardlaw 2014). The interaction between thrombolytic drugs and antithrombotic drugs given simultaneously (or the latter very soon after the former) was only tested by random allocation in MAST‐I 1995, which therefore provides the only truly valid evidence. In MAST‐I 1995, there was a clinically important adverse interaction between aspirin and streptokinase when given simultaneously, resulting in a substantial increase in case fatality (early and late), which was not offset by a reduction in the number of dead or dependent participants at the end of follow‐up; 28% of those allocated to streptokinase alone versus 43% of those allocated to streptokinase plus aspirin were dead by the end of follow‐up (P < 0.001), and 62% were dead and 63% were dependent (versus 68% in the control group). The actual cause of the increase in early and total deaths with streptokinase and aspirin appeared largely to be due to neurological events. Aspirin with streptokinase significantly increased the number of deaths in hospital from all causes (OR 2.2, 95% CI 1.3 to 3.8), neurological causes (OR 2.0, 95% CI 1.1 to 3.7), and ICH on CT scan or at autopsy (OR 2.2, 95% CI 1.0 to 5.0) when compared with the group who received streptokinase alone. There was no difference in deaths from neurological causes without ICH, but note that more participants in the streptokinase plus aspirin group died of neurological causes without a CT scan or autopsy so they could also have had an ICH. That is, the increase in ICH with aspirin and streptokinase may be even greater. Information is also available on antithrombotic drug use in 12 other trials. The case fatality comparison was non‐significant (P values or CIs), though frequency was higher the nearer to the administration of thrombolysis the concomitant antithrombotic drug use was (OR 1.95 when all participants received antithrombotic drugs within 24 hours of thrombolysis; 1.27 when some participants received antithrombotic drugs within 24 hours; 1.21 when no participants received antithrombotic drugs within 24 hours but some thereafter; and 0.89 for no antithrombotic drugs within the first 10 to 14 days). Although these data are based mainly on non‐randomised comparisons, they do support the evidence of a clinically significant adverse interaction between the concurrent use of thrombolysis and antithrombotic drugs as found in MAST‐I 1995. This is confirmed by the ARTIS 2012 trial comparing recombinant tissue plasminogen activator (rTPA) plus IV aspirin with rTPA alone. In those with minor neurological deficits (National Institutes of Health Stroke Scale 0 to 5), treatment with alteplase compared with aspirin did not increase the likelihood of a favourable outcome at 90 days (Khatri 2018).
New developments
The concept of acute stroke (and the differentiation of stroke from TIA) is changing as people with acute cerebral ischaemia are assessed and treated increasingly earlier and more aggressively. The boundary between acute treatment and very early initiation of secondary prevention is becoming blurred, as evidenced by the CHANCE 2013, POINT, and TARDIS trials. There is clearly a place for further trials of more intensive antiplatelet regimens, started as soon after symptom onset as possible. However, since aspirin will remain the comparator treatment, such trials will need to be even larger than current trials if they are to produce reliable results.
Summary of main results
Two trials testing aspirin 160 mg to 300 mg once daily, started within 48 hours of onset, contributed 96% of the data. The risk of bias was low. Antiplatelet therapy with aspirin 160 mg to 300 mg daily, given orally (or by nasogastric tube or per rectum in people who cannot swallow) and started within 48 hours of onset of presumed ischaemic stroke, reduced the risk of early recurrent ischaemic stroke without a major risk of early haemorrhagic complications; long‐term outcomes were improved.
Overall completeness and applicability of evidence
We used GRADE to assess the certainty of evidence for each outcome (see Table 1). Death or dependence at end of follow‐up and complete recovery from stroke were both assessed as moderate GRADE. The remaining six outcomes had very low GRADE. All outcomes received "serious" concern for indirectness of evidence because CAST 1997 included only participants of Chinese ethnicity and contributed almost 50% of the data in the meta‐analysis. Therefore, the results are mainly applicable to a Chinese population. The outcomes which were deemed very low were for various reasons, including inclusion of studies of high or uncertain risk or bias, showing variable results, and CIs being wide. For most outcomes, there were not enough studies included to accurately detect publication bias. However, publication bias was strongly suspected for the following outcomes: recurrent stroke during treatment period, any recurrent stroke or symptomatic ICH during treatment period, and major extra cranial haemorrhage during treatment period.
Quality of the evidence
The conclusions are based on overall good‐quality evidence, provided by two large well‐conducted studies. The overall risk of bias was low.
Potential biases in the review process
The review could be subject to publication bias as only published studies were included and, therefore, we may not have identified unpublished studies, or studies where there was no published abstract in English. We attempted to reduce publication bias by a comprehensive search strategy. In addition, we attempted to contact authors to obtain original data and query methodology where it was unclear; however, not all authors responded (Khatri 2018; Turpie 1983; Zhao 2017). This resulted in the study methodology of one study in particular being unclear, and so we were unable to assess the risk of bias (Turpie 1983).
Agreements and disagreements with other studies or reviews
We are unaware of any recently published reviews with which we can draw comparison.
Authors' conclusions
Implications for practice.
The review provided strong evidence for the benefits of aspirin 160 mg to 300 mg, given as soon as is practicable (and continued as a once daily dose), in people with suspected acute ischaemic stroke. This evidence applied chiefly to people seen within 48 hours of stroke onset and in whom intracranial haemorrhage had been excluded, or was thought to be clinically unlikely, and had no definite contraindications to aspirin. In people who are unable to swallow safely, aspirin may be given per rectum as a suppository or via a nasogastric tube.
The assessment of the safety and efficacy of antiplatelet agents in people with primary intracranial haemorrhage was not the aim of this review. However, it did provide limited evidence on the effects of aspirin in people in whom intracranial haemorrhage had not been ruled out by brain scanning before treatment was started and who subsequently were shown to have had an intracranial haemorrhage. There was no evidence of net harm in such people. Thus, if there is likely to be a delay before computer tomography or magnetic resonance brain scanning can be performed to exclude intracranial haemorrhage it may be reasonable to give aspirin until the scan result is known. If the scan shows intracranial haemorrhage, then aspirin should probably be discontinued.
In people who cannot tolerate aspirin, an alternative antiplatelet agent should be considered in the acute stage of stroke, although the evidence for other agents is inadequate at present.
This review confirmed the benefit of continuing treatment in hospital, and external evidence supports its continuation after hospital discharge.
Implications for research.
The overall treatment effect of antiplatelet agents in acute ischaemic stroke is not large and better acute therapies are therefore necessary. The question of whether any particular antiplatelet agent is superior to aspirin 160 mg to 300 mg in the treatment of acute ischaemic stroke remains to be determined, and would require a very large randomised trial to be answered reliably.
In people with unstable coronary artery disease, trials have evaluated the addition of low molecular‐weight heparin or another antiplatelet agent (such as a glycoprotein IIb/IIIa inhibitor or clopidogrel) to aspirin. There is a case for such trials to be undertaken in acute ischaemic stroke. There is also a case for further trials of low‐dose subcutaneous heparin (or low‐dose low molecular‐weight heparin) plus aspirin versus aspirin alone in the prevention of poststroke deep vein thrombosis and pulmonary embolism, and in reducing neurological disability from the original or recurrent strokes. Such trials would need to include several 10s of 1000s of participants.
Future trials comparing more intense antiplatelet or antithrombotic regimens with aspirin in acute ischaemic stroke will need to include several 10s of 1000s of participants and should also test the effects and interactions during treatments such as intravenous thrombolysis and mechanical thrombectomy.
Feedback
Are trials of anticoagulant therapy for acute ischaemic stroke ethical?, 26 June 2007
Summary
The Implications for research section states: "There is also a case for further trials of low‐dose subcutaneous heparin (or low‐dose low‐molecular‐weight heparin) plus aspirin versus aspirin alone in the prevention of post‐stroke deep vein thrombosis and pulmonary embolism, and in reducing neurological disability from the original or recurrent strokes. Such trials would need to include several tens of thousands of patients". This review should be updated to reflect that, given the lack of efficacy of anticoagulants in multiple trials and high bleeding risk in stroke patients, further trials with low‐dose heparin or low‐dose low‐molecular‐weight heparin would be unethical.
Reply
This comment was submitted in response to the previous version of this review (this response to feedback was delayed by a number of unavoidable administrative factors). We do not agree that the data are sufficiently robust to support a statement that 'further trials with low‐dose heparin or low‐dose low‐molecular‐weight heparin in acute ischemic stroke would be unethical.' Such decisions should rest with the relevant research ethics committees and the trialists (advised by their steering and data monitoring and safety committees).
Contributors
Commenter: David A Cundiff MD
Reply: Peter Sandercock
Feedback and response 2014, 24 June 2014
Summary
I read with interest the Cochrane Review by Sandercock et al which reviewed the use of oral antiplatelet therapy for acute ischemic stroke, and commend the authors on doing an excellent job filtering through the literature and analyzing all available data1. While I do agree with the majority of the authors' conclusions and the overall trend of their therapeutic recommendations, I believe that some conclusion statements regarding use of aspirin post‐stroke are stronger than the data supporting them.
The majority of data in this review (98%) were drawn from two large trials in 1997, CAST2 and IST3. The authors acknowledge that 601 total participants from these trials were lost to follow‐up (300 treatment and 301 control), with the majority coming from CAST (219 treatment and 232 control), but claim that due to the relatively small percentage of patients missing, they can safely assume that these patients did not have an outcome event for the primary analysis. Unfortunately, using Review Manager 5.2 to run sensitivity analyses on several comparisons revealed that results found to be statistically significant in this review became non‐statistically significant when only a few events were added to a group. The CAST trial was used for my analyses due to the larger amount of missing data, and I specifically analyzed the comparisons of death or dependence at the end of follow‐up, all‐cause death during treatment, all‐cause death at follow‐up, pulmonary embolism, and symptomatic intracranial hemorrhage. The primary comparison of death or dependence at end of follow‐up was relatively robust, and required an almost worst‐case scenario of all 219 missing patients in the aspirin group to have had an event to push the result to statistical non‐significance. On the other hand, only five more deaths in the aspirin group for the comparison of all‐cause death during treatment period pushed the upper end of the CI to 1.01. All‐cause death at follow‐up became non‐significant when 50 deaths were added to the treatment group. The finding of reduced pulmonary embolism became non‐significant when only two events were added to the treatment group. Adding 27 events to the aspirin group for the outcome of any recurrent stroke during treatment period similarly results in non‐significance. Interestingly, adding only one symptomatic intracranial hemorrhage to the control group for the outcome looking at this event during treatment period pushed the confidence interval to non‐significance. I believe the results of this review will be viewed in a more accurate light if a discussion of the potential confounding effect of the missing data was included, especially for the outcomes where only a handful of missing events could result in non‐significant data.
There also appears to be an underlying issue with the methodology of the IST study. The IST study was deemed to be at "low risk of bias" by the Cochrane group, even though there was no use of placebo, and trial participants/assessors were not blinded during treatment. They do mention the fact that at follow‐up, the majority of patients appear to not remember what treatment they received and are therefore effectively blinded towards the primary endpoint of death and disability at six months; however, there is no mention of the fact that the open design could have introduced significant bias. It is feasible that clinicians may have been more likely to conduct CT scans on patients who deteriorate clinically while on an antiplatelet, increasing the likelihood of detecting intracranial hemorrhages. On the other hand, clinicians who knew their patient was not receiving an antiplatelet may have tended to follow these patients more closely or found other ways to counterbalance what they may have believed was suboptimal therapy. Sensitivity analyses were done for each comparison, including only double‐blinded studies which essentially excluded IST data and reported CAST results in isolation. This resulted in six comparisons (including the primary) to become statistically non‐significant. I believe it is important to mention how the open design of the IST trial may have affected results in either a positive to negative direction in either the section discussing blinding of trials or in a separate limitations section.
To summarize, I appreciate the effort and dedication put into this periodically updated Cochrane review, but feel that there should be more discussion on the limitations inherent to the two main studies which this review is based on to avoid overestimation of the resulting data.
I certify that I have no affiliations with or involvement in any organisation or entity with a direct financial interest in the subject matter of my criticisms.
Harrison Jefferey Lee, B.Sc(Pharm); Joan Chung Yan Ng, B.Sc(Pharm)
References:
Sandercock PAG, Counsell C, Tseng MC, Cecconi E. Oral antiplatelet therapy for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2014, Issue 3. Art. No.: CD000029. DOI: 10.1002/14651858.CD000029.pub3.
CAST: randomised placebo‐controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. CAST (Chinese Acute Stroke Trial) Collaborative Group. Lancet 1997; 7;349(9066):1641‐9.
Sandercock P, Collins R, Counsell C, Farrell B, Peto R, Slattery J, et al. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19 435 patients with acute ischaemic stroke. Lancet 1997;349(9065):1569‐81.
Reply
Thank you for these comments on the review. Lee and Ng's comment focus on two points.
1. That the estimates of effect of aspirin are not robust in various sensitivity analyses, applying 'worst case scenario methods' to examine the effect of missing data on some of the outcomes. While this is one approach to assessing the plausibility of the effects of aspirin observed in patients with acute ischaemic stroke, it is important to view the estimates in the context of the effects of aspirin in other patients with acute vascular events (e.g. acute MI) and in secondary prevention after an ischaemic event of the brain heart or peripheral circulation. From that perspective, the effects observed in acute stroke are consistent with those observed in other categories of patients at high risk, which we mention in the discussion.
2. The lack of blinding in IST is a potential source of bias that was not sufficiently discussed in the review. The lack of blinding is discussed, but not exhaustively, partly because, as set out in the primary report of the IST trial, the impact on the primary outcome was likely to be small and the estimates of effect on the secondary outcomes were remarkably similar in the unblinded (IST) and blinded (CAST) studies. The 1997 report of the IST in the Lancet stated: "To minimise bias in the assessment of the 6 month outcome the assessors in most countries were blind to treatment allocation. Moreover, the pilot phase of the study indicated that most patients could not recall their treatment allocation at 6 months,3 so they too were effectively blinded. Estimates of treatment effects among those with central follow‐up (which is likely to be largely blinded) and those without were not significantly different. Thus, lack of blinding probably did not materially affect the main findings for the primary outcomes. Clinicians might, however, have been more likely to arrange repeat CT scanning in patients on active treatment who worsened clinically, detecting more intracranial haemorrhages, so the open design may have introduced some bias in the assessment of the secondary outcomes. However, the apparent effects of aspirin in the open IST were similar to those in CAST, which was placebo‐controlled."
Contributors
Feedback: Harrison Jefferey Lee, B.Sc(Pharm); Joan Chung Yan Ng, B.Sc(Pharm)
Response: Peter Sandercock
What's new
| Date | Event | Description |
|---|---|---|
| 6 March 2021 | New citation required but conclusions have not changed | Updated searches from new authorship team ‐ prior review updated. |
| 6 March 2021 | New search has been performed | We included 11 studies involving 42,226 participants. Three new trials have been added since the last update. As per the previous version of this review, two trials testing aspirin 160 mg to 300 mg once daily, started within 48 hours of onset, contributed 96% of the data. The risk of bias was low. The maximum follow‐up was six months. |
History
Protocol first published: Issue 1, 1995 Review first published: Issue 1, 1995
| Date | Event | Description |
|---|---|---|
| 27 September 2019 | Amended | Revised 'Declarations of Interest' statement added |
| 25 June 2014 | Feedback has been incorporated | User feedback and authors' responses incorporated. |
| 24 October 2013 | New citation required but conclusions have not changed | Title and inclusion criteria changed. Change to authorship: a new co‐author, Emanuela Cecconi, has replaced Gordon Gubitz. |
| 22 October 2013 | New search has been performed | The searches of CENTRAL, MEDLINE and EMBASE have been updated to May 2013, and the search of the Cochrane Stroke Group Trials Register to October 2013. No new studies have been added. Four studies included in the previous review have been excluded for this update because they assessed parenterally administrated antiplatelet agents, which are now the subject of a separate review. The title of this review was therefore changed to 'Oral antiplatelet agents for acute ischaemic stroke'. There are now eight included trials with 41,483 participants. |
Acknowledgements
We thank Hazel Fraser (Managing Editor) for her valuable support with the Cochrane Stroke Review Group's methodological clarifications, and Joshua Cheyne for help with trial searching.
Ongoing trials
Any clinician who knows of additional trials that we have omitted please write to Jatinder S Minhas.
Appendices
Appendix 1. CENTRAL search strategy
#1 [mh ^"cerebrovascular disorders"] or [mh ^"basal ganglia cerebrovascular disease"] or [mh ^"brain ischemia"] or [mh "brain infarction"] or [mh ^"hypoxia‐ischemia, brain"] or [mh ^"carotid artery diseases"] or [mh ^"carotid artery thrombosis"] or [mh ^"carotid artery, internal, dissection"] or [mh ^"intracranial arterial diseases"] or [mh ^"cerebral arterial diseases"] or [mh ^"infarction, anterior cerebral artery"] or [mh ^"infarction, middle cerebral artery"] or [mh ^"infarction, posterior cerebral artery"] or [mh "intracranial embolism and thrombosis"] or [mh stroke] or [mh ^"vertebral artery dissection"]
#2 isch*mi* near/6 (stroke* or apoplex* or cerebral next vasc* or cerebrovasc* or cva or attack*):ti,ab,kw (Word variations have been searched)
#3 (brain or cerebr* or cerebell* or vertebrobasil* or hemispher* or intracran* or intracerebral or infratentorial or supratentorial or middle next cerebr* or mca* or "anterior circulation") near/5 (isch*mi* or infarct* or thrombo* or emboli* or occlus* or hypoxi*):ti,ab,kw (Word variations have been searched)
#4 #1 or #2 or #3
#5 [mh "Platelet aggregation inhibitors"]
#6 [mh "Cyclooxygenase Inhibitors"] or [mh Thienopyridines] or [mh "Phosphodiesterase Inhibitors"] or [mh "Thromboxane A2"/AI] or [mh "Purinergic P2Y Receptor Antagonists"]
#7 [mh "Platelet activation"/DE]
#8 [mh "Blood platelets"/DE]
#9 antiplatelet* or anti‐platelet* or antithrombocytic or "anti‐thrombocytic":ti,ab,kw (Word variations have been searched)
#10 (platelet* or thrombocyte*) near/5 (inhibit* or antagonist* or antiaggreg* or anti‐aggreg*):ti,ab,kw (Word variations have been searched)
#11 cyclooxygenase next inhibitor* or thienopyridine* or phosphodiesterase next inhibitor*:ti,ab,kw (Word variations have been searched)
#12 "thromboxane A2" near/3 (inhib* or antag*):ti,ab,kw (Word variations have been searched)
#13 aspirin* or "acetyl salicylic acid" or "acetylsalicylic acid":ti,ab,kw (Word variations have been searched)
#14 ARC1779 or AZD6140 or alprostadil or asasantin or carnitine or cilostazol or clopidogrel or cloricromene or cv4151 or "cv‐4151" or defibrotide or dilazep or dipyridamol* or disintegrin* or ditazol or E5880 or E5510 or epoprostenol* or fluribrofen or "fut‐175" or iloprost* or indobufen or isbogrel or kbt3022 or "kbt‐3022" or ketanserin* or ketoprofen or ketorolac or levamisol* or ligustrazine* or tromethamine* or milrinone* or mopidamol* or naudicelle or nimesulide or ozagrel* or oky046 or "oky‐046" or "oky‐1581" or phthalzinol or picotamide or policosanol or prasugrel or procainamide or sarpogrelate or satigrel or sulphinpyrazone or sulfinpyrazone or suloctadil or terutroban or ticagrelor or ticlopidine or trapidil or triflusal or vorapaxar:ti,ab,kw (Word variations have been searched)
#15 {or #5‐#14}
#16 #4 and #15
#17 cardiac or aneurysm* or angina or "atrial fibrillation" or cancer or arthritis or diabetes or coronary or myocardial:ti (Word variations have been searched)
#18 #16 not #17
Appendix 2. MEDLINE Ovid search strategy
1. cerebrovascular disorders/ or basal ganglia cerebrovascular disease/ or brain ischemia/ or exp brain infarction/ or hypoxia‐ischemia, brain/ or carotid artery diseases/ or carotid artery thrombosis/ or carotid artery, internal, dissection/ or intracranial arterial diseases/ or cerebral arterial diseases/ or infarction, anterior cerebral artery/ or infarction, middle cerebral artery/ or infarction, posterior cerebral artery/ or exp "intracranial embolism and thrombosis"/ or exp stroke/ or vertebral artery dissection/
2. (isch?emi$ adj6 (stroke$ or apoplex$ or cerebral vasc$ or cerebrovasc$ or cva or attack$)).tw.
3. ((brain or cerebr$ or cerebell$ or vertebrobasil$ or hemispher$ or intracran$ or intracerebral or infratentorial or supratentorial or middle cerebr$ or mca$ or anterior circulation) adj5 (isch?emi$ or infarct$ or thrombo$ or emboli$ or occlus$ or hypoxi$)).tw.
4. 1 or 2 or 3
5. exp Platelet aggregation inhibitors/
6. exp Cyclooxygenase Inhibitors/ or exp Thienopyridines/ or exp Phosphodiesterase Inhibitors/ or Thromboxane A2/ai or exp Purinergic P2Y Receptor Antagonists/
7. exp Platelet activation/de
8. exp Blood platelets/de
9. (antiplatelet$ or anti‐platelet$ or antithrombocytic or anti‐thrombocytic).tw.
10. ((platelet$ or thrombocyte$) adj5 (inhibit$ or antagonist$ or antiaggreg$ or anti‐aggreg$)).tw.
11. (cyclooxygenase inhibitor$ or thienopyridine$ or phosphodiesterase inhibitor$).tw.
12. (thromboxane A2 adj3 (inhib$ or antag$)).tw.
13. (aspirin$ or acetyl salicylic acid$ or acetyl?salicylic acid$).tw,nm.
14. (ARC1779 or AZD6140 or alprostadil or asasantin or carnitine or cilostazol or clopidogrel or cloricromene or cv4151 or cv‐4151 or defibrotide or dilazep or dipyridamol$ or disintegrin$ or ditazol or E5880 or E5510 or epoprostenol$ or fluribrofen or fut‐175 or iloprost$ or indobufen or isbogrel or kbt3022 or kbt‐3022 or ketanserin$ or ketoprofen or ketorolac or levamisol$ or ligustrazine$ or tromethamine$ or milrinone$ or mopidamol$ or naudicelle or nimesulide or ozagrel$ or oky046 or oky‐046 or oky‐1581 or phthalzinol or picotamide or policosanol or prasugrel or procainamide or sarpogrelate or satigrel or sulphinpyrazone or sulfinpyrazone or suloctadil or terutroban or ticagrelor or ticlopidine or trapidil or triflusal or vorapaxar).tw,nm.
15. or/5‐14
16. Randomized Controlled Trials as Topic/
17. random allocation/
18. Controlled Clinical Trials as Topic/
19. control groups/
20. clinical trials as topic/ or clinical trials, phase i as topic/ or clinical trials, phase ii as topic/ or clinical trials, phase iii as topic/ or clinical trials, phase iv as topic/
21. double‐blind method/
22. single‐blind method/
23. Placebos/
24. placebo effect/
25. Therapies, Investigational/
26. Drug Evaluation/
27. Research Design/
28. randomized controlled trial.pt.
29. controlled clinical trial.pt.
30. (clinical trial or clinical trial phase i or clinical trial phase ii or clinical trial phase iii or clinical trial phase iv).pt.
31. (random$ or RCT or RCTs).tw.
32. (controlled adj5 (trial$ or stud$)).tw.
33. (clinical$ adj5 trial$).tw.
34. ((control or treatment or experiment$ or intervention) adj5 (group$ or subject$ or patient$)).tw.
35. (quasi‐random$ or quasi random$ or pseudo‐random$ or pseudo random$).tw.
36. ((control or experiment$ or conservative) adj5 (treatment or therapy or procedure or manage$)).tw.
37. ((singl$ or doubl$ or tripl$ or trebl$) adj5 (blind$ or mask$)).tw.
38. (placebo$ or sham).tw.
39. trial.ti.
40. (assign$ or allocate$).tw.
41. or/16‐40
42. 4 and 15 and 41
43. exp animals/ not humans.sh.
44. 42 not 43
Appendix 3. Embase Ovid search strategy
1. cerebrovascular disease/ or brain infarction/ or brain stem infarction/ or cerebellum infarction/ or exp brain ischemia/ or carotid artery disease/ or exp carotid artery obstruction/ or cerebral artery disease/ or exp cerebrovascular accident/ or exp occlusive cerebrovascular disease/ or stroke patient/
2. (isch?emi$ adj6 (stroke$ or apoplex$ or cerebral vasc$ or cerebrovasc$ or cva or attack$)).tw.
3. ((brain or cerebr$ or cerebell$ or vertebrobasil$ or hemispher$ or intracran$ or intracerebral or infratentorial or supratentorial or middle cerebr$ or mca$ or anterior circulation) adj5 (isch?emi$ or infarct$ or thrombo$ or emboli$ or occlus$ or hypoxi$)).tw.
4. 1 or 2 or 3
5. exp Antithrombocytic agent/
6. thienopyridine derivative/ or exp phosphodiesterase inhibitor/ or thromboxane A2 receptor blocking agent/ or exp purinergic receptor blocking agent/
7. (antiplatelet$ or anti‐platelet$ or antithrombocytic or anti‐thrombocytic).tw.
8. ((platelet$ or thrombocyte$) adj5 (inhibit$ or antagonist$ or antiaggreg$ or anti‐aggreg$)).tw.
9. (cyclooxygenase inhibitor$ or thienopyridine$ or phosphodiesterase inhibitor$).tw.
10. (thromboxane A2 adj3 (inhib$ or antag$)).tw.
11. (aspirin$ or acetyl salicylic acid$ or acetyl?salicylic acid$).tw.
12. (ARC1779 or AZD6140 or alprostadil or asasantin or carnitine or cilostazol or clopidogrel or cloricromene or cv4151 or cv‐4151 or defibrotide or dilazep or dipyridamol$ or disintegrin$ or ditazol or E5880 or E5510 or epoprostenol$ or fluribrofen or fut‐175 or iloprost$ or indobufen or isbogrel or kbt3022 or kbt‐3022 or ketanserin$ or ketoprofen or ketorolac or levamisol$ or ligustrazine$ or tromethamine$ or milrinone$ or mopidamol$ or naudicelle or nimesulide or ozagrel$ or oky046 or oky‐046 or oky‐1581 or phthalzinol or picotamide or policosanol or prasugrel or procainamide or sarpogrelate or satigrel or sulphinpyrazone or sulfinpyrazone or suloctadil or terutroban or ticagrelor or ticlopidine or trapidil or triflusal or vorapaxar).tw.
13. or/5‐12
14. Randomized Controlled Trial/
15. Randomization/
16. Controlled Study/
17. control group/
18. clinical trial/ or phase 1 clinical trial/ or phase 2 clinical trial/ or phase 3 clinical trial/ or phase 4 clinical trial/ or controlled clinical trial/
19. Double Blind Procedure/
20. Single Blind Procedure/ or triple blind procedure/
21. placebo/
22. drug comparison/ or drug dose comparison/
23. "types of study"/
24. random$.tw.
25. (controlled adj5 (trial$ or stud$)).tw.
26. (clinical$ adj5 trial$).tw.
27. ((control or treatment or experiment$ or intervention) adj5 (group$ or subject$ or patient$)).tw.
28. (quasi‐random$ or quasi random$ or pseudo‐random$ or pseudo random$).tw.
29. ((control or experiment$ or conservative) adj5 (treatment or therapy or procedure or manage$)).tw.
30. ((singl$ or doubl$ or tripl$ or trebl$) adj5 (blind$ or mask$)).tw.
31. (placebo$ or sham).tw.
32. trial.ti.
33. (assign$ or allocat$).tw.
34. (RCT or RCTs).tw.
35. or/14‐34
36. 4 and 13 and 35
37. exp animals/ or exp invertebrate/ or animal experiment/ or animal model/ or animal tissue/ or animal cell/ or nonhuman/
38. human/ or normal human/ or human cell/
39. 37 not 38
40. 36 not 39
41. (cardiac or aneurysm$ or angina or atrial fibrillation or cancer or arthritis or diabetes or coronary or myocardial).ti.
42. 40 not 41
Appendix 4. Risk of bias tool
| Source of bias | Support for judgment | Review authors’ judgement (assess as low, unclear or high risk of bias) | |
| Selection bias |
Random sequence generation | Describe the method used to generate the allocation sequence in sufficient detail to allow an assessment of whether it should produce comparable groups. | Selection bias (biased allocation to interventions) due to inadequate generation of a randomised sequence. |
| Allocation concealment | Describe the method used to conceal the allocation sequence in sufficient detail to determine whether intervention allocations could have been foreseen before or during enrolment. | Selection bias (biased allocation to interventions) due to inadequate concealment allocations prior to assignment. | |
| Performance bias | Blinding of participants and personnel | Describe all measures used, if any, to blind trial participants and researchers from knowledge of which intervention a participant received. Provide any information relating to whether the intended blinding was effective. | Performance bias due to knowledge of the allocated interventions by participants and personnel during the study. |
| Detection bias | Blinding of outcome assessment | Describe all measures used, if any, to blind outcome assessment from knowledge of which intervention a participant received. Provide any information relating to whether the intended blinding was effective. | Detection bias due to knowledge of the allocated interventions by outcome assessment. |
| Attrition bias | Incomplete outcome data | Describe the completeness of outcome data for each main outcome, including attrition and exclusions from the analysis. State whether attrition and exclusions were reported, the numbers in each intervention group (compared with total randomised participants), reasons for attrition or exclusions where reported, and any reinclusions in analyses for the review. | Attrition bias due to amount, nature, or handling of incomplete outcome data. |
| R eporting bias | Selective reporting | State how selective outcome reporting was examined and what was found | Reporting bias due to selective outcome reporting |
| Other bias | Anything else, ideally prespecified | State any important concerns about bias not covered in the other domains in the tool | Bias due to problems not covered elsewhere |
Risk of bias tool used in the review (Higgins 2011).
Appendix 5. World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP)
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/en) (last searched 25 August 2020)
Appendix 6. US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.clinicaltrials.gov) ("First posted from 06/03/2020 to 08/24/2020"; last searched 24 August 2020)
Data and analyses
Comparison 1. Antiplatelet drug versus control in acute presumed ischaemic stroke.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Death or dependence at end of follow‐up | 7 | 42034 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.95 [0.91, 0.99] |
| 1.1.1 Aspirin versus control | 5 | 41604 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.95 [0.91, 0.99] |
| 1.1.2 PF‐03049423 versus control | 1 | 133 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.15 [0.58, 2.28] |
| 1.1.3 Clopidogrel loading dose versus control | 1 | 297 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.80 [0.45, 1.42] |
| 1.2 Deaths from any cause during treatment period | 8 | 41483 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.92 [0.85, 1.00] |
| 1.2.1 Aspirin versus control | 4 | 41291 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.92 [0.85, 1.00] |
| 1.2.2 Aspirin plus dipyridamole versus control | 1 | 80 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.47 [0.43, 4.99] |
| 1.2.3 Ticlopidine versus control | 3 | 112 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.12 [0.01, 1.20] |
| 1.3 Deaths from any cause during follow‐up | 10 | 41929 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.93 [0.87, 0.98] |
| 1.3.1 Aspirin versus control | 5 | 41604 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.92 [0.87, 0.98] |
| 1.3.2 Aspirin plus dipyridamole versus control | 1 | 80 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.47 [0.43, 4.99] |
| 1.3.3 Ticlopidine versus control | 3 | 112 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.12 [0.02, 0.88] |
| 1.3.4 PF‐03049423 versus control | 1 | 133 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.91 [0.74, 4.93] |
| 1.4 Deep venous thrombosis during treatment period | 2 | 133 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.78 [0.36, 1.67] |
| 1.4.1 Aspirin plus dipyridamole versus control | 1 | 80 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.35 [0.13, 0.95] |
| 1.4.2 Ticlopidine versus control | 1 | 53 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 2.37 [0.72, 7.73] |
| 1.5 Pulmonary embolism during treatment period | 7 | 41042 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.71 [0.53, 0.96] |
| 1.5.1 Aspirin versus control | 3 | 40850 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.71 [0.53, 0.97] |
| 1.5.2 Aspirin plus dipyridamole versus control | 1 | 80 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 7.39 [0.15, 372.38] |
| 1.5.3 Ticlopidine versus control | 3 | 112 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.13 [0.01, 2.06] |
| 1.6 Recurrent ischaemic/unknown stroke during treatment period | 9 | 41652 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.79 [0.70, 0.88] |
| 1.6.1 Aspirin versus control | 4 | 41163 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.78 [0.69, 0.88] |
| 1.6.2 Aspirin plus dipyridamole versus control | 1 | 80 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Not estimable |
| 1.6.3 Ticlopidine versus control | 3 | 112 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Not estimable |
| 1.6.4 Clopidogrel loading dose versus control | 1 | 297 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.10 [0.59, 2.06] |
| 1.7 Symptomatic intracranial haemorrhage during treatment period | 9 | 41652 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.18 [0.97, 1.44] |
| 1.7.1 Aspirin versus control | 4 | 41163 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.17 [0.96, 1.43] |
| 1.7.2 Aspirin plus dipyridamole versus control | 1 | 80 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.00 [0.14, 7.38] |
| 1.7.3 Ticlopidine versus control | 3 | 112 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 2.70 [0.36, 20.26] |
| 1.7.4 Clopidogrel loading dose versus control | 1 | 297 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.99 [0.14, 7.12] |
| 1.8 Recurrent stroke/intracranial haemorrhage during treatment period | 7 | 41042 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.88 [0.79, 0.97] |
| 1.8.1 Aspirin versus control | 3 | 40850 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 0.87 [0.79, 0.97] |
| 1.8.2 Aspirin plus dipyridamole versus control | 1 | 80 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.00 [0.14, 7.38] |
| 1.8.3 Ticlopidine versus control | 3 | 112 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 2.70 [0.36, 20.26] |
| 1.9 Major extracranial haemorrhage during treatment period | 7 | 41042 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.69 [1.35, 2.11] |
| 1.9.1 Aspirin versus control | 3 | 40850 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.69 [1.35, 2.11] |
| 1.9.2 Aspirin plus dipyridamole versus control | 1 | 80 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Not estimable |
| 1.9.3 Ticlopidine versus control | 3 | 112 | Peto Odds Ratio (Peto, Fixed, 95% CI) | Not estimable |
| 1.10 Complete recovery from stroke (post hoc) | 2 | 40541 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.06 [1.01, 1.11] |
| 1.10.1 Aspirin versus control | 2 | 40541 | Peto Odds Ratio (Peto, Fixed, 95% CI) | 1.06 [1.01, 1.11] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
CAST 1997.
| Study characteristics | ||
| Methods | Concealment: centrally produced, prepacked, sequentially numbered envelopes Exclusions during trial: 0 Losses to follow‐up: 451 (219 treatment, 232 control) at 4 weeks |
|
| Participants | China 21,106 participants 63% male 28% aged > 70 years 87% had CT before entry Ischaemic stroke < 48 hours since stroke onset |
|
| Interventions | Treatment: aspirin 160 mg once daily orally or via nasogastric tube Control: placebo Duration: 4 weeks, or until death or earlier discharge |
|
| Outcomes |
|
|
| Funding source | Medical Research Council supported the Clinical Trial Service Unit, Oxford. Trial tablets donated by Shandong Xinhua Pharmaceuticals. |
|
| Notes | Exclusions not specified by protocol but by responsible physician, possibly including increased risk of adverse effects, or little likelihood of any worthwhile benefit in hospital. Follow‐up: 4 weeks. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random component in the sequence generation described. |
| Allocation concealment (selection bias) | Low risk | Sequentially numbered envelopes used. |
| Blinding of participants and personnel (performance bias) all outcomes | Unclear risk | Unclear whether there was blinding of participants and personnel. |
| Blinding of outcome assessment (detection bias) all outcomes | Unclear risk | Unclear whether there was blinding of outcome assessment. |
| Incomplete outcome data (attrition bias) all outcomes | Low risk | Missing outcome data balanced in numbers across intervention groups. |
| Selective reporting (reporting bias) | Low risk | Study protocol available. |
| Other bias | Low risk | No other sources of bias identified. |
Ciuffetti 1990.
| Study characteristics | ||
| Methods | Randomisation: random number list Double blind Exclusions during trial: 0 Losses to follow‐up: 0 |
|
| Participants | Italy 30 participants 14 (47%) male Mean age: 73 years (all > 65 years) 100% CT before entry Hemiparetic ischaemic stroke < 12 hours since stroke onset |
|
| Interventions | Treatment: ticlopidine 250 mg orally 12 hourly Control: placebo Duration: 3 weeks |
|
| Outcomes |
|
|
| Funding source | No information available | |
| Notes | Exclusions: cerebral oedema Follow‐up: 3 weeks |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Groups divided by research team based on predetermined factors, e.g. age and sex. |
| Allocation concealment (selection bias) | High risk | Groups divided by research team based on predetermined factors, e.g. age and sex. |
| Blinding of participants and personnel (performance bias) all outcomes | Unclear risk | Double‐blind trial but it was not stated explicitly who was blinded. |
| Blinding of outcome assessment (detection bias) all outcomes | Unclear risk | Double‐blind trial but it was not stated explicitly who was blinded. |
| Incomplete outcome data (attrition bias) all outcomes | Low risk | No missing outcome data. |
| Selective reporting (reporting bias) | Low risk | Study protocol not found but expected outcomes included and prespecified. |
| Other bias | Low risk | No other sources of bias identified. |
Di Cesare 2016.
| Study characteristics | ||
| Methods | Double blind Block randomisation Losses to follow‐up: 13 deaths, 4 serious AEs, 1 after therapy |
|
| Participants | 43 sites across Bulgaria, Canada, Czech Republic, France, Germany, Hungary, India, Republic of Korea, Taiwan, and the USA 133 participants 62.4% male Treatment: 68; 42 male, 28 female; mean age: 64.2 (SD 13.1) years Placebo: 65; 41 male, 26 female; mean age 65.6 (SD 11.3) years |
|
| Interventions | Treatment: PF‐03049423 6 mg (phosphodiesterase‐5‐inhibitor) Control: placebo Duration: 90 days |
|
| Outcomes | Primary outcome
Secondary outcomes
|
|
| Funding source | No comment on source of funding available. | |
| Notes | Study terminated early due to futility. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Web‐based or telephone call in drug management system used for randomisation. |
| Allocation concealment (selection bias) | Low risk | Sponsor‐generated randomisation code used to allocate a randomisation number. |
| Blinding of participants and personnel (performance bias) all outcomes | Low risk | Sponsor, investigator, and participant blinded. |
| Blinding of outcome assessment (detection bias) all outcomes | Low risk | No concerns in blinding of outcome assessment. |
| Incomplete outcome data (attrition bias) all outcomes | Low risk | No concerns regarding missing outcome data. |
| Selective reporting (reporting bias) | Low risk | Study protocol available. |
| Other bias | Low risk | No other sources of bias identified. |
IST 1997.
| Study characteristics | ||
| Methods | Concealment: telephone randomisation Unblinded; dependency assessment mainly blinded Exclusions during trial: none Losses to follow‐up: 2 at 14 days (1 treatment, 1 control); 150 at 6 months (81 treatment, 69 control) |
|
| Participants | International 19,435 participants 54% male 61% aged > 70 years 67% CT prior to randomisation, 29% CT after randomisation Ischaemic stroke < 48 hours since stroke onset |
|
| Interventions | Treatment 1: subcutaneous heparin (5000 IU or 12,500 IU 12 hourly) Treatment 2: aspirin 300 mg Treatment 3: subcutaneous heparin (5000 IU or 12,500 IU 12 hourly) + aspirin 300 mg Control: no treatment (factorial design) Duration: 14 days or until discharge from hospital Aspirin by mouth if able to swallow, if not then by rectal suppository or by injection of 100 mg of the lysine salt of aspirin |
|
| Outcomes |
|
|
| Funding source | Principally funded by the UK Medical Research Council (who also funded P Sandercock, J Slattery, and B Farrell), the UK Stroke Association, and the European Union BIOMED‐1 programme. Support for collaborators' meetings and travel was provided by Eli Lilly, Sterling Winthrop (now Bayer USA), Sanofi, and Bayer UK. Follow‐up in Australia was supported by a grant from the National Heart Foundation to G Hankey. Follow‐up in Canada was supported by a Nova Scotia Heart and Stroke Foundation grant to S Phillips. Czech Republic IST was supported by a grant from the IGA Ministry of Health to Z Ambler. India IST was supported by the McMaster INCLEN program and the All India Institute of Medical Sciences. The IST in New Zealand was funded by the Julius Brendel Trust and the Lottery Grants Board. The IST was supported in Norway by the Norwegian Council on Cardiovascular Disease and Nycomed (for insurance). |
|
| Notes | Exclusions: small likelihood of worthwhile benefit; high risk of AE (e.g. hypersensitivity of aspirin, recent GI bleed or peptic ulcer disease, already on long‐term anticoagulation) Follow‐up: 6 months |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Central randomisation service at clinical trial service used. |
| Allocation concealment (selection bias) | Low risk | Computer allocated based on a minimisation algorithm. |
| Blinding of participants and personnel (performance bias) all outcomes | Unclear risk | Participants and personnel were not blinded, but the authors stated lack of blinding probably did not affect the main findings for the primary outcomes. |
| Blinding of outcome assessment (detection bias) all outcomes | Unclear risk | No blinding of the outcome assessment, but the authors stated lack of blinding probably did not affect the main findings for the primary outcomes. |
| Incomplete outcome data (attrition bias) all outcomes | Low risk | Outcome data were 99.99% complete for 14‐day follow‐up and 99.2% complete for 6‐month follow‐up. |
| Selective reporting (reporting bias) | Low risk | Study protocol available. |
| Other bias | Low risk | No sources of other bias identified. |
Khatri 2018.
| Study characteristics | ||
| Methods | Double blind Step forward randomisation procedure, ratio of 1:1 Losses to follow‐up: 22% |
|
| Participants | Acute ischaemic stroke with deficits not clearly disabling at presentation 313 participants 54% male Aspirin group: 157; 92 male, 65 female; mean age: 61 (SD 13) years Placebo group: 156; 77 male, 79 female; mean age: 61 (SD 14) years Duration: 90 days |
|
| Interventions | Treatment: oral aspirin 325 mg + IV placebo Control: oral placebo + IV alteplase |
|
| Outcomes | Primary outcomes
Secondary outcomes
|
|
| Funding source | No comment on source of funding available. | |
| Notes | Study terminated early. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Step‐forward randomisation procedure used. |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement. |
| Blinding of participants and personnel (performance bias) all outcomes | Low risk | Blinding of participants and personnel. |
| Blinding of outcome assessment (detection bias) all outcomes | Unclear risk | Only reported CT scans as blinded, not other outcomes. |
| Incomplete outcome data (attrition bias) all outcomes | Low risk | Missing outcome data was imputed via hot‐deck method. |
| Selective reporting (reporting bias) | Low risk | Study protocol available. |
| Other bias | Low risk | No sources of other bias identified. |
MAST‐I 1995.
| Study characteristics | ||
| Methods | Concealment: telephone central office Assessor blind (telephone follow‐up) Exclusions during trial: none Losses to follow‐up: none |
|
| Participants | Europe 309 participants 163 (53%) male 22% aged < 60 years, 46% aged 61–75 years 100% CT before entry Ischaemic stroke < 6 hours since stroke onset |
|
| Interventions | Factorial design of streptokinase and aspirin vs no treatment; only aspirin alone vs no aspirin included to prevent confounding influence of streptokinase Treatment: aspirin 300 mg oral (or IV/rectal) 24 hourly Control: no treatment Duration: 10 days |
|
| Outcomes |
|
|
| Funding source | Partly supported by Pierrel SpA, Italy and Pharmacia Therapeutics, Sweden. Pharmacia provided streptokinase and Rhône‐Poulenc Rorer and Sanofi‐Winthrop supplied aspirin. The Stroke Association supported the UK centres (unclear what this involved). |
|
| Notes | Exclusions: coma, bleeding risk Follow‐up: 6 months |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation lists were generated by computer and stratified by centre. |
| Allocation concealment (selection bias) | Low risk | 2 × 2 factorial study design used for randomisation. |
| Blinding of participants and personnel (performance bias) all outcomes | Unclear risk | Unclear if participants were blinded. |
| Blinding of outcome assessment (detection bias) all outcomes | Low risk | No concerns regarding blinding of outcome assessment. |
| Incomplete outcome data (attrition bias) all outcomes | Low risk | No missing outcome data. |
| Selective reporting (reporting bias) | Low risk | Study protocol available. |
| Other bias | Low risk | No sources of other bias identified. |
Pince 1981.
| Study characteristics | ||
| Methods | Randomisation: sealed envelope Double blind Exclusions during trial: 9 (5 treatment, 4 control) Losses to follow‐up: none |
|
| Participants | France 80 participants 50 (62%) male Mean age: 66 years No CT before entry; 100% had lumbar puncture Presumed ischaemic stroke < 6 days since stroke onset |
|
| Interventions | Treatment: aspirin 330 mg 8 hourly (oral) + dipyridamole 75 mg 8 hourly (oral) Control: placebo Duration: 1 week |
|
| Outcomes |
|
|
| Funding source | No information available | |
| Notes | Exclusions: bleeding risk, aspirin allergy Follow‐up: 10 days |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient information to permit judgement. |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information to permit judgement. |
| Blinding of participants and personnel (performance bias) all outcomes | Low risk | Participants and personnel blinded. |
| Blinding of outcome assessment (detection bias) all outcomes | Unclear risk | Not explicitly reported whether outcome assessors were aware of the intervention participants received. |
| Incomplete outcome data (attrition bias) all outcomes | Low risk | No concerns regarding missing outcome data. |
| Selective reporting (reporting bias) | Unclear risk | Prespecified analysis plan unclear. |
| Other bias | Unclear risk | Unpublished thesis in French, unclear of statistical plan. |
Rödén‐Jüllig 2003.
| Study characteristics | ||
| Methods | Randomisation: randomisation tables, stratified for gender Concealment: sequentially numbered containers from pharmacy Double blind Exclusions during trials: none Losses to follow‐up: none |
|
| Participants | Sweden 441 participants 226 (51%) male 100% CT before entry Ischaemic stroke < 72 hours since stroke onset SSSS ≥ 1 point |
|
| Interventions | Treatment: aspirin 325 mg orally once daily Control: placebo Duration: 5 days |
|
| Outcomes |
|
|
| Funding source | The trial was supported by grants from the Serafimer Hospital Foundation, the County Council of Stockholm, Department of Research, Development & Education, the Claes Groschinsky Foundation, the Loo and Hans Osterman Foundation, the Eirs 50‐year Foundation, the SALUS 50‐year Foundation, the 1987 Foundation for Stroke Research, the Tore Nilsson Foundation for Medical Research and the Karolinska Institutet Foundations for Research. Miles Inc through Bayer AG provided the placebo tablets free of charge. The aspirin tablets were purchased from Miles Inc. These companies were not involved in the conduct of this trial in any other way. |
|
| Notes | Exclusions: specified in protocol – severe concomitant medical conditions or pre‐existing neurological illness, bleeding risk, blood pressure > 240/140 mmHg Follow‐up: 3 months |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Standard randomisation tables used. |
| Allocation concealment (selection bias) | Low risk | Packages taken in numerical order. |
| Blinding of participants and personnel (performance bias) all outcomes | Low risk | Participants and personnel blinded. |
| Blinding of outcome assessment (detection bias) all outcomes | Low risk | No concerns regarding blinding of outcome assessment. |
| Incomplete outcome data (attrition bias) all outcomes | Low risk | No missing outcome data. |
| Selective reporting (reporting bias) | Low risk | Study protocol noted. |
| Other bias | Low risk | No sources of other bias identified. |
Turpie 1983.
| Study characteristics | ||
| Methods | Randomisation: identical, sequentially numbered bottles from pharmacy Double blind Exclusions during trial: 4 (2 treatment, 2 control) Losses to follow‐up: none |
|
| Participants | Canada 53 participants 21 (40%) male Age range: 33–92 years No CT before entry Any stroke with leg paresis < 4 weeks since stroke onset (most < 2 weeks) |
|
| Interventions | Treatment: ticlopidine 250 mg orally 12 hourly Control: placebo Duration: 10–21 days |
|
| Outcomes |
|
|
| Funding source | No information available | |
| Notes | Exclusions: unknown Follow‐up: 21 days |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Unable to assess risk of bias. |
| Allocation concealment (selection bias) | Unclear risk | Unable to assess risk of bias. |
| Blinding of participants and personnel (performance bias) all outcomes | Unclear risk | Unable to assess risk of bias. |
| Blinding of outcome assessment (detection bias) all outcomes | Unclear risk | Unable to assess risk of bias. |
| Incomplete outcome data (attrition bias) all outcomes | Unclear risk | Unable to assess risk of bias. |
| Selective reporting (reporting bias) | Unclear risk | Unable to assess risk of bias. |
| Other bias | Unclear risk | Unable to assess risk of bias. |
Utsumi 1988.
| Study characteristics | ||
| Methods | Randomisation: unknown Not blind Exclusions during trial: 1 (control) Losses to follow‐up: 0 |
|
| Participants | Japan 29 participants 5 (17%) male Mean age: 63 years CT scanning not stated Ischaemic stroke < 4 weeks since stroke onset (only 1 > 2 weeks) |
|
| Interventions | Treatment: ticlopidine 100 mg orally 8–12 hourly Control: no treatment Duration: up to 3 months (median 1 month) |
|
| Outcomes |
|
|
| Funding source | No information available | |
| Notes | Exclusions: unknown Follow‐up: 3 months |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Blocked randomisation code used. |
| Allocation concealment (selection bias) | Low risk | No concerns in allocation concealment. |
| Blinding of participants and personnel (performance bias) all outcomes | Unclear risk | Double‐blind trial but not stated explicitly who was blinded. |
| Blinding of outcome assessment (detection bias) all outcomes | Unclear risk | Double‐blind trial but unclear if outcome assessors were blinded. |
| Incomplete outcome data (attrition bias) all outcomes | Low risk | No concerns regarding missing outcome data. |
| Selective reporting (reporting bias) | Unclear risk | Prespecified analysis plan not included. |
| Other bias | Low risk | No sources of other bias identified. |
Zhao 2017.
| Study characteristics | ||
| Methods | Double blind Randomising scheme performed by CLASS‐China randomisation |
|
| Participants | From 17 clinical centres in mainland southern China 297 participants Acute ischaemic stroke of non‐cardioembolic origin 66.3% male Loading dose group given 48 hours after symptom onset: 149; 105 males, 44 females; mean age: 64 (SD 10.7) years Placebo group: 148; 92 male, 56 female; mean age: 63.5 (SD 11) years |
|
| Interventions | Treatment: loading dose clopidogrel 300 mg (all participants received 75 mg daily days 2–28) Control: placebo |
|
| Outcomes | Primary outcome
Secondary outcomes
|
|
| Funding source | This study received funding from the Medical Science and Technology Research of Guangdong Province (No. A2015461). | |
| Notes | Study terminated early as recruitment below target. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Automated system used. |
| Allocation concealment (selection bias) | Low risk | Allocated to a number corresponding to a medication kit. |
| Blinding of participants and personnel (performance bias) all outcomes | Unclear risk | Double‐blind trial but it was not stated explicitly who was blinded. |
| Blinding of outcome assessment (detection bias) all outcomes | Unclear risk | Double‐blind trial but it was unclear if outcome assessors were blinded. |
| Incomplete outcome data (attrition bias) all outcomes | Low risk | No concerns regarding missing outcome data. |
| Selective reporting (reporting bias) | Low risk | Study protocol available. |
| Other bias | Low risk | No sources of other bias identified. |
ADL: activities of daily living; AE: adverse event; BI: Barthel Index; CT: computer tomography; DVT: deep vein thrombosis; GI: gastrointestinal; IV: intravenous; MI: myocardial infarction; mRS: modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; SD: standard deviation; SIP: speed of infarct progression; SSSS: Scandinavian Stroke Supervision Scale; systematic: outcome sought by systematically scanning all participants at a predefined time, irrespective of presence or absence of symptoms.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Maestrini 2018 | Non‐acute population |
| Mehta 2015 | Intravenous administration. |
| Nguyen 2020 | Re‐analysis of existing study data (International Stroke Trial) |
| TARDIS | Multiple antiplatelet agents. |
| Wang 2019 | Lack of appropriate comparator |
Differences between protocol and review
We added the GRADE criteria detail for included studies with summary of findings and generated risk of bias tables. We revised the risk of bias assessments using the RoB 1 tool in keeping with Cochrane guidance on risk of bias assessments. We did not conduct prespecified sensitivity and subgroup analyses where it was inappropriate to do so.
Contributions of authors
Carl Counsell, Gord Gubitz, Mei‐Cium Tseng, Emanuela Cecconi, and Peter Sandercock designed and performed prior versions of this Cochrane Review, which form the basis of this update.
For this update
TC, SB, RC, and MK performed the literature searches and extracted the data.
XW performed the statistical analysis.
JM, TC, XW, LB, and TR updated the text and analyses, and commented on the review.
Sources of support
Internal sources
-
National Institute for Health Research Biomedical Research Centre, Leicester, UK
Funder
External sources
-
National Institute for Health Research, UK
Academic Clinical Fellowship (MK), Academic Clinical Lectureship (JSM), and Senior Investigator Award (TGR). The views expressed in this publication are those of the author(s) and not necessarily those of the National Health Service, the National Institute for Health Research, the Department of Health, or the authors' respective institutions.
Declarations of interest
JM: work as a health professional: NIHR Clinical Lecturer, University of Leicester. Affiliations: I am part of a topic group contributing to the 6th RCP National Clinical Guideline for Stroke. TC: work as a health professional: Clinical Fellow, Leicester, Northampton, Rutland Deanery. XW: grants and contracts: investigator grant, post‐doctoral fellowship, investigator grant development funding, NHMRC National Heart Foundation, NSW Health Commission. SB: work as health professional: previous work as a junior doctor in the stroke unit, University Hospitals Leicester, from August to December 2019. RC: none. MK: work as a health professional: NIHR Academic Clinical Fellow, University of Leicester. LB: work as a health professional: NIHR Clinical Lecturer, University of Leicester. TR: grants and contracts: National Lead, PACIFIC‐Stroke Trial, Population Health Research Institute, Hamilton, Canada (factor XIa inhibitor trial in acute ischaemic stroke). Work as health professional: Honorary Consultant Physician in Stroke Medicine, University Hospitals of Leicester NHS Trust: "As a health professional, I treat patients according to relevant national guidelines with antiplatelet therapy to reduce their risk of recurrent ischaemic stroke/TIA". Affiliations: Past President, British Association of Stroke Physicians: "I represent BASP on the Intercollegiate Stroke Working Party, which oversees the RCP National Clinical Guidelines for Stroke".
Joint first author
Joint first author
Joint senior author
Joint senior author
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
CAST 1997 {published and unpublished data}
- CAST (Chinese Acute Stroke Trial) Collaborative Group. A randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. Lancet 1997;349:1641-9. [PubMed] [Google Scholar]
Ciuffetti 1990 {published and unpublished data}
- Ciuffetti G, Aisa G, Mercuri M, Lombardini R, Paltriccia R, Neri C, et al. Effects of ticlopidine on the neurologic outcome and the hemorheologic pattern in the postacute phase of ischemic stroke: a pilot study. Angiology 1990;41:505-11. [DOI] [PubMed] [Google Scholar]
Di Cesare 2016 {published data only}
- Di Cesare F, Mancuso J, Woodward P, Bednar MM, Loudon PT. Phosphodiesterase-5 inhibitor PF-03049423 effect on stroke recovery: a double-blind, placebo-controlled randomized clinical trial. Journal of Stroke and Cerebrovascular Diseases 2016;25:642-9. [DOI] [PubMed] [Google Scholar]
IST 1997 {published and unpublished data}
- International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. Lancet 1997;349:1569-81. [PubMed] [Google Scholar]
Khatri 2018 {published data only}
- Khatri P, Kleindorfer DO, Devlin T, Sawyer RN, Starr M, Mejilla J, et al. Effect of alteplase vs aspirin on functional outcome for patients with acute ischemic stroke and minor nondisabling neurologic deficits. JAMA 2018;320:156-66. [DOI] [PMC free article] [PubMed] [Google Scholar]
MAST‐I 1995 {published and unpublished data}
- Multicentre Acute Stroke Trial-Italy (MAST-I) Group. Randomised controlled trial of streptokinase, aspirin, and combination of both in treatment of acute ischaemic stroke. Lancet 1995;346:1509-14. [PubMed] [Google Scholar]
Pince 1981 {unpublished data only}
- Pince J. Thromboses Veineuses des Membres Inferieures et Embolies Pulmonaires au Cours des Accidents Vasculaires Cerebraux. A Propos d'un Essai Comparatif de Traitment Preventif [these pour le Doctorat d'Etat en Medicine]. Toulouse (France): Universite Paul Sabatier, 1981. [Google Scholar]
Rödén‐Jüllig 2003 {published data only}
- Rödén-Jüllig Å, Britton M, Malmkvist K, Leijd B. Aspirin in the prevention of progressing stroke: a randomized controlled study. Journal of Internal Medicine 2003;254:584-90. [DOI] [PubMed] [Google Scholar]
Turpie 1983 {unpublished data only}
- Turpie AG, Dobkin B, McKenna R. A trial of ticlopidine, an antiplatelet agent, for acute cerebral infarction. Guildford: Sanofi Winthrop (Sanofi internal report 1983.001.6.188) 1983.
Utsumi 1988 {unpublished data only}
- Utsumi H. Evaluation of utility of ticlopidine, an antiplatelet agent, for acute cerebral infarction. Guildford: Sanofi Winthrop (Sanofi internal report 001.6.128) 1984.
Zhao 2017 {published data only}
- Zhao Y, Yang W, Tan Z, Wang W, Xiao W, Zeng J, et al. Clopidogrel loading dose versus maintenance dose to treat patients with acute ischaemic stroke in China (CLASS-China): results from a prospective double-blind randomised clinical trial. Stroke and Vascular Neurology 2017;2:e000072. [DOI] [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Maestrini 2018 {published data only}
- Maestrini I, Altieri M, Di Clemente L, Vicenzini E, Pantano P, Raz E, et al. Longitudinal study on low-dose aspirin versus placebo administration in silent brain infarcts: the Silence Study. Stroke Research and Treatment 2018:7532403. [DOI: 10.1155/2018/7532403] [DOI] [PMC free article] [PubMed]
Mehta 2015 {published data only}
- Mehta S, Ahmad J, Hussain M, Brar J, Chahal H, Shah Y, et al. Safety and efficacy of intravenous eptifibatide as standalone therapy for select acute ischemic stroke patients (SIESTA-I trial). Stroke 2015;46:AWP61. [Google Scholar]
Nguyen 2020 {published data only}
- Nguyen TL, Collins GS, Landais P, Le Manach Y. Counterfactual clinical prediction models could help to infer individualized treatment effects in randomized controlled trials-An illustration with the International Stroke Trial. J Clin Epidemiol 2020;125:47-56. [DOI: 10.1016/j.jclinepi.2020.05.022] [DOI] [PubMed] [Google Scholar]
TARDIS {published data only}
- Bath P. Triple Antiplatelets for Reducing Dependency After Ischaemic Stroke (TARDIS). www.controlled-trials.com/ISRCTN47823388 (first received 24 October 2008).
Wang 2019 {published data only}
- Wang X, Yan Y, Song Y, Ma C. Efficacy of argatroban in the treatment of acute cerebral infarction. Int J Clin Exp Med 2019;12(5):5454-5460. [Google Scholar]
Additional references
AHA/ASA Guidelines
- American Heart Association Stroke Council. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019;50:344-418. [Google Scholar]
AHA 2013
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics – 2013 update: a report from the American Heart Association. Circulation 2013;127:e6-e245. [DOI: 10.1161/CIR.0b013e31828124ad] [DOI] [PMC free article] [PubMed] [Google Scholar]
ATC 1994a
- Antiplatelet Trialists' Collaboration. Collaborative overview of randomised trials of antiplatelet therapy – I: prevention of death, myocardial infarction, and stroke by prolonged antiplatelet therapy in various categories of patients. BMJ 1994;308:81-106. [PMC free article] [PubMed] [Google Scholar]
ATC 1994b
- Antiplatelet Trialists' Collaboration. Collaborative overview of randomised trials of antiplatelet therapy – III: reduction in venous thrombosis and pulmonary embolism by antiplatelet prophylaxis among surgical and medical patients. BMJ 1994;308:235-46. [PMC free article] [PubMed] [Google Scholar]
ATC 2002
- Antithrombotic Trialists' Collaboration. Collaborative meta-analysis of antiplatelet therapy for prevention of death, myocardial infarction and stroke in high-risk patients. BMJ 2002;324:71-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
ATC 2009
- Antithrombotic Trialists' Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009;373:1849-60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bamford 1989
- Bamford J, Sandercock P, Warlow C, Slattery J. Inter-observer agreement for the assessment of handicap in stroke patients. Stroke 1989;20:8. [DOI] [PubMed] [Google Scholar]
Bath 2004a
- Bath PM. Prostacyclin and analogues for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2004, Issue 3. Art. No: CD000177. [DOI: 10.1002/14651858.CD000177.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bath 2004b
- Bath PM, Bath-Hextall FJ. Pentoxifylline, propentofylline and pentifylline for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2004, Issue 3. Art. No: CD000162. [DOI: 10.1002/14651858.CD000162.pub2] [DOI] [PubMed] [Google Scholar]
CAIST 2011
- Lee YS, Bae HJ, Kang DW, Lee SH, Yu K, Park JM, et al. Cilostazol in Acute Ischemic Stroke Treatment (CAIST Trial): a randomized double-blind non-inferiority trial. Cerebrovascular Diseases 2011;32:65-71. [DOI: 10.1159/000327036] [DOI] [PubMed] [Google Scholar]
Candelise 1994
- Candelise L, Pinardi G, Aritzu E, Musicco M. Telephone interview for stroke outcome assessment. Cerebrovascular Diseases 1994;4:341-3. [Google Scholar]
Chairangsarit 2005
- Chairangsarit P, Sithinamsuwan P, Niyasom S, Udommongkol C, Nidhinandana S, Suwantamee J. Comparison between aspirin combined with dipyridamole versus aspirin alone within 48 hours after ischemic stroke event for prevention of recurrent stroke and improvement of neurological function: a preliminary study. Journal of the Medical Association of Thailand 2005;88:S148-54. [PubMed] [Google Scholar]
CHANCE 2013
- Wang Y, Wang Y, Zhao X, Liu L, Wang D, Wang C, CHANCE Investigators. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. New England Journal of Medicine 2013;369:11-9. [DOI: 10.1056/NEJMoa1215340] [DOI] [PubMed] [Google Scholar]
Chen 2000
- Chen ZM, Sandercock P, Pan HC, Counsell C, Collins R, Liu LS, et al. Indications for early aspirin use in acute ischemic stroke: a combined analysis of 40,000 randomized patients from the Chinese Acute Stroke Trial and the International Stroke Trial. On behalf of the CAST and IST Collaborative Groups. Stroke 2000;31:1240-9. [DOI] [PubMed] [Google Scholar]
Ciccone 2014
- Ciccone A, Motta C, Abraha I, Cozzolino F, Santilli I. Glycoprotein IIb‐IIIa inhibitors for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2014, Issue 3. Art. No: CD005208. [DOI: 10.1002/14651858.CD005208.pub3] [DOI] [PubMed] [Google Scholar]
Collins 1996
- Collins R, MacMahon S, Flather M, Baigent C, Remviq L, Mortensen S, et al. Clinical effects of anticoagulant therapy in suspected acute myocardial infarction: systematic review of randomised trials. BMJ 1996;313:652-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
CSS 2010
- Canadian Stroke Network and Heart and Stroke Foundation of Canada. Canadian best practice recommendations for stroke care: update 2010. www.canadianstrokenetwork.ca/ (accessed prior to 24 November 2021).
Dalen 2006
- Dalen JE. Aspirin to prevent heart attack and stroke: what's the right dose? American Journal of Medicine 2006;119:198-202. [DOI] [PubMed] [Google Scholar]
Davenport 1996
- Davenport R, Dennis M, Wellwood I, Warlow C. Complications after acute stroke. Stroke 1996;27:415-20. [DOI] [PubMed] [Google Scholar]
Dennis 1997
- Dennis M, Wellwood I, Warlow C. Are simple questions a valid measure of outcome after stroke? Cerebrovascular Diseases 1997;7:22-7. [Google Scholar]
EARLY 2010
- Dengler R, Diener HC, Schwartz A, Grond M, Schumacher H, Machnig T, EARLY Investigators. Early treatment with aspirin plus extended-release dipyridamole for transient ischaemic attack or ischaemic stroke within 24 h of symptom onset (EARLY trial): a randomised, open-label, blinded-endpoint trial. Lancet Neurology 2010;9:159-66. [DOI: 10.1016/S1474-4422(09)70361-8] [DOI] [PubMed] [Google Scholar]
ESO 2008
- The European Stroke Organisation Executive Committee and the ESO Writing Committee. Guidelines for management of ischaemic stroke and transient ischaemic attack 2008. Cerebrovascular Diseases 2008;25::457-507. [DOI: 10.1159/000131083] [DOI] [PubMed] [Google Scholar]
GBD 2019
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020;396(10258):1204-22. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- GRADEpro GDT. Hamilton (ON): McMaster University (developed by Evidence Prime), (accessed 24 February 2021). Available at gradepro.org.
Hankey 2010
- Hankey GJ, Hacke W, Easton JD, Johnston SC, Mas JL, Brennan DM, CHARISMA Trial Investigators. Effect of clopidogrel plus ASA vs. ASA early after TIA and ischaemic stroke: a substudy of the CHARISMA trial. International Journal of Stroke 2010;41:1679-83. [DOI: 10.1161/STROKEAHA.110.586727] [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from training.cochrane.org/handbook/archive/v5.1/.
Higgins 2020
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.1.0 (updated March 2020). Cochrane, 2020. Available from training.cochrane.org/handbook/archive/v6.1.
IST 1996
- International Stroke Trial Pilot Study Collaborative Group. Study design of the International Stroke Trial (IST), baseline data and outcome in 984 randomised patients in the pilot study. Journal of Neurology, Neurosurgery, and Psychiatry 1996;60:371-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Jauch 2013
- Jauch EC, Saver JL, Adams HP Jr, Bruno A, Connors JJ, Demaerschalk BM, American Heart Association Stroke Council, Council on Cardiovascular Nursing, Council on Peripheral Vascular Disease, Council on Clinical Cardiology. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44:870-947. [DOI: 10.1161/STR.0b013e318284056a] [DOI] [PubMed] [Google Scholar]
Keir 2002
- Keir S, Wardlaw J, Sandercock PA, Chen Z. Antithrombotic therapy in patients with any form of intracranial haemorrhage: a systematic review of the available controlled studies. Cerebrovascular Diseases 2002;14(3-4):197-206. [DOI] [PubMed] [Google Scholar]
Krishnamurthi 2020
- Krishnamurthi RV, Ikeda T, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the Global Burden of Disease Study 2017. Neuroepidemiology 2020;54:171-9. [DOI: ] [DOI] [PubMed] [Google Scholar]
MedStrategy 1995
- Dick E. Stroke: a Focus of Opportunity. St Louis (MO): MedStrategy, 1995. [Google Scholar]
Minhas 2017
- Minhas JS, Robinson TG. Latest developments in clinical stroke care. Journal of the Royal College of Physicians of Edinburgh 2017;47(4):360-3. [DOI: 10.4997/JRCPE.2017.413] [DOI] [PubMed] [Google Scholar]
Naqvi 2020
- Naqvi IA, Kamal AK, Rehman HNaqvi IA, Kamal AK, Rehman H. Multiple versus fewer antiplatelet agents for preventing early recurrence after ischaemic stroke or transient ischaemic attack. Cochrane Database of Systematic Reviews 2020;8(8):CD009716. [DOI: 10.1002/14651858.CD009716.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
NINDS 1995
- The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischaemic stroke. New England Journal of Medicine 1995;333:1581-7. [DOI] [PubMed] [Google Scholar]
Odgaard‐Jensen 2011
- Odgaard-Jensen J, Vist GE, Timmer A, Kunz R, Akl EA, Schünemann H, et al. Randomisation to protect against selection bias in healthcare trials. Cochrane Database of Systematic Reviews 2011, Issue 4. Art. No: MR000012. [DOI: 10.1002/14651858.MR000012.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Patrono 1994
- Patrono C. Aspirin as an antiplatelet drug. New England Journal of Medicine 1994;330:1287-94. [DOI] [PubMed] [Google Scholar]
Patrono 1998
- Patrono C, Coller B, Dalen JE, Fuster V, Gent M, Harker LA, et al. Platelet-active drugs: the relationships among dose, effectiveness, and side effects. Chest 1998;114:470S-88S. [DOI] [PubMed] [Google Scholar]
POINT
- POINT Investigators. Clopidogrel and aspirin in acute ischemic stroke and high-risk TIA. New England Journal of Medicine 2018;379:215-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
RCP Guideline 2016
- Royal College of Physicians. National Clinical Guidelines for Stroke, Fifth Edition 2016. www.rcplondon.ac.uk/resources/stroke-guidelines (accessed prior to 24 November 2021).
RESTART 2019
- RESTART Collaboration. Effects of antiplatelet therapy after stroke due to intracerebral haemorrhage (RESTART): a randomised, open-label trial. Lancet 2019;393(10191):2613-23. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Review Manager 2020 [Computer program]
- Review Manager (RevMan). Version 5.4. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2020.
Ricci 2012
- Ricci S, Celani MG, Cantisani TA, Righetti E. Piracetam for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2012, Issue 9. Art. No: CD000419. [DOI: 10.1002/14651858.CD000419.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schünemann 2013
- Schünemann H, Brożek J, Guyatt G, Oxman A, editor(s). Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach (updated October 2013). GRADE Working Group, 2013. Available from gdt.guidelinedevelopment.org/app/handbook/handbook.html.
SOCRATES
- Johnston SC, Amarenco P, Albers GW, Denison H, Easton JD, Evans SR, SOCRATES Steering Committee and Investigators. Ticagrelor versus aspirin in acute stroke or transient ischemic attack. New England Journal of Medicine 2016;375(1):35-43. [DOI] [PubMed] [Google Scholar]
Suri 2008
- Suri MF, Hussein HM, Abdelmoula MM, Divani AA, Qureshi AI. Safety and tolerability of 600 mg clopidogrel bolus in patients with acute ischemic stroke: preliminary experience. Medical Science Monitor 2008;14:I39-44. [PubMed] [Google Scholar]
SUTC 2013
- Stroke Unit Trialists' Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database of Systematic Reviews 2013, Issue 9. Art. No: CD000197. [DOI: 10.1002/14651858.CD000197.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
TARDIS
- Bath PM, Woodhouse LJ, Appleton JP, Beridze M, Christensen H, Dineen RA, TARDIS Investigators. Antiplatelet therapy with aspirin, clopidogrel, and dipyridamole versus clopidogrel alone or aspirin and dipyridamole in patients with acute cerebral ischaemia (TARDIS): a randomised, open-label, phase 3 superiority trial. Lancet 2018;391(10123):850-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
THALES
- Johnston SC, Amarenco P, Denison H, Evans SR, Himmelmann A, James S, THALES Investigators. Ticagrelor and aspirin or aspirin alone in acute ischemic stroke or TIA. New England Journal of Medicine 2020;383(3):207-17. [DOI] [PubMed] [Google Scholar]
Tsai 2013
- Tsai CF, Thomas B, Sudlow CL. Epidemiology of stroke and its subtypes in Chinese vs white populations: a systematic review. Neurology 2013;81(3):264-72. [DOI] [PMC free article] [PubMed] [Google Scholar]
van Gijn 1992
- Gijn J. Aspirin: dose and indications in modern stroke prevention. Neurologic Clinics 1992;10:193-209. [PubMed] [Google Scholar]
van Kooten 1994
- Kooten F, Ciabattone G, Patrono C, Schmitz PI, Gijn J, Koudstaal PJ. Evidence for episodic platelet activation in acute ischaemic stroke. Stroke 1994;25:278-81. [DOI] [PubMed] [Google Scholar]
van Kooten 1997
- Kooten F, Ciabattoni G, Patrono C, Dippel DW, Koudstaal PJ. Platelet activation and lipid peroxidation in patients with acute ischaemic stroke. Stroke 1997;28:1557-63. [DOI] [PubMed] [Google Scholar]
Wardlaw 2009
- Wardlaw JM, Murray V, Berge E, Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2009, Issue 4. Art. No: CD000213. [DOI: 10.1002/14651858.CD000213.pub2] [DOI] [PubMed] [Google Scholar]
Wardlaw 2014
- Wardlaw JM, Murray V, Berge E, Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2014, Issue 7. Art. No: CD000213. [DOI: 10.1002/14651858.CD000213.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Warlow 2001
- Warlow C. Stroke, transient ischaemic attacks, and intracranial venous thrombosis. In: Donaghy M, editors(s). Brain's Diseases of the Nervous System. 11th edition. Oxford (UK): Oxford University Press, 2001:775-896. [Google Scholar]
Zhang 2012
- Zhang J, Yang J, Chang X, Zhang C, Zhou H, Liu M. Ozagrel for acute ischemic stroke: a meta-analysis of data from randomized controlled trials. Neurological Research 2012;34:346-53. [DOI: 10.1179/1743132812Y.0000000022] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Sandercock 2003
- Sandercock P, Gubitz G, Foley P, Counsell C. Antiplatelet therapy for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2003, Issue 2. Art. No: CD000029. [DOI: 10.1002/14651858.CD000029] [DOI] [PubMed] [Google Scholar]
Sandercock 2014
- Sandercock PA, Counsell C, Tseng MC, Cecconi E. Oral antiplatelet therapy for acute ischaemic stroke. Cochrane Database of Systematic Reviews 2014, Issue 3. Art. No: CD000029. [DOI: 10.1002/14651858.CD000029.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]