

Abstract
Objective:
To quantify the three-dimensional moments and forces produced by pretorqued nickel-titanium (NiTi) rectangular archwires fully engaged in 0.018- and 0.022-inch slots of central incisor and molar edgewise and prescription brackets.
Materials and Methods:
Ten identical acrylic dental models with retroclined maxillary incisors were fabricated for bonding with various bracket-wire combinations. Edgewise, Roth, and MBT brackets with 0.018- and 0.022-inch slots were bonded in a simulated 2 × 4 clinical scenario. The left central incisor and molar were sectioned and attached to load cells. Correspondingly sized straight and pretorqued NiTi archwires were ligated to the brackets using 0.010-inch ligatures. Each load cell simultaneously measured three force (Fx, Fy, Fz) and three moment (Mx, My, Mz) components. The faciolingual, mesiodistal, and inciso-occluso/apical axes of the teeth corresponded to the x, y, and z axes of the load cells, respectively. Each wire was removed and retested seven times. Three-way analysis of variance (ANOVA) examined the effects of wire type, wire size, and bracket type on the measured orthodontic load systems. Interactions among the three effects were examined and pair-wise comparisons between significant combinations were performed.
Results:
The force and moment components on each tooth were quantified according to their local coordinate axes. The three-way ANOVA interaction terms were significant for all force and moment measurements (P < .05), except for Fy (P > .05).
Conclusion:
The pretorqued wire generates a significantly larger incisor facial crown torquing moment in the MBT prescription compared to Roth, edgewise, and the straight NiTi wire.
Keywords: Pretorque, NiTi, Wire, Force, Moment
INTRODUCTION
To reduce traditional first, second, and third order compensating bends, modern orthodontics utilizes straight wires and prescription brackets.1–3 In some malocclusions, it is desirable to have complete expression of the facial crown torque (FCT) in the bracket prescription. However, studies confirm that even with a full-size archwire, there is considerable torsional play within the bracket slot,2,4,5 thus requiring manually added torque in the wires.5 To ameliorate this problem, commercial rectangular nickel-titanium (NiTi) archwires with 20° FCT manufactured into the anterior (canine to canine) segment have become available.6 These pretorqued archwires are designed to increase the FCT without bending in heavier and stiffer stainless steel or beta-titanium wires. Pretorqued wires may be advantageous in decompensating lingually tipped incisors; however, there are no studies on the loads (moments and forces) that they generate.
Traditional edgewise brackets do not contain built-in prescriptions, so studies of maxillary anterior torque with edgewise brackets have involved manually bent torquing arches.7,8 Roth and McLaughlin-Bennett-Trevisi (MBT) are two frequently used prescription bracket systems with +12° and +17° of central incisor FCT built into the brackets, respectively. Additionally, studies fail to consider that brackets are available in two slot sizes, 0.018 × 0.025-inch and 0.022 × 0.028-inch. The effects of stainless steel, straight NiTi, and beta-titanium wires on torque expression in self-ligating brackets have been explored.4,9 Although the studies utilize prescription brackets and various wire types, they do not evaluate torque in full archwires within prescription brackets. Studies of force systems such as a 2 × 4 setup of two permanent maxillary first molars and four permanent maxillary incisors do not quantify the moments and forces in three-dimensions (3D).10 3D finite element analysis of incisor torque did not consider the compliance of the bracket and ligatures,11 which needs to be validated experimentally.
Therefore, there is a need for studies that evaluate the 20° anteriorly pretorqued NiTi archwire in a clinically relevant 3D system. To do so, it is necessary to quantify the three moment and three force components that are generated when the wire is ligated into brackets.12,13 Clinical relevance is established with actual dental models, common 0.018-inch and 0.022-inch slot bracket prescriptions, full-sized archwires, and stainless steel ligatures.
MATERIALS AND METHODS
Ten identical stone models were fabricated with retroclined incisors to simulate a mixed dentition case in which a pretorqued NiTi wire would be used (Figure 1). Edgewise, Roth, and MBT brackets (Apollo series, G&H Wire, Franklin, Ind) in 0.018-inch and 0.022-inch slot sizes were bonded to the four permanent incisors and two permanent first molars in 10 combinations to explore all clinical scenarios and determine the most appropriate approach to express FCT (Table 1). To ensure uniform placement, an average of the clinical crown sizes was obtained, the brackets were symmetrically applied at the center of this height, and a straight NiTi wire of an arch form similar to the models (Orthoforce G4 nickel-titanium Europa I, G&H Orthodontics) was used to verify alignment. Medium-body polyvinylsiloxane material (Examix NDS, GC America, Tokyo, Japan) was injected over the teeth, followed by an alginate impression. Duplicate brackets were placed in the polyvinylsiloxane and autopolymerizing tooth, and gingiva-colored acrylics (Duralay, Reliance, Worth, Ill and Repair Material, Dentsply, York, Pa) were packed into the impression and allowed to cure. The custom dentoforms were attached to an orthodontic force tester14 with two screws. The orthodontic force tester utilizes two load cells (Multiaxis force/torque Nano17, ATI Industrial Automation, Apex, NC) to measure the three force and three moment components applied to two target teeth. The force range of each load cell was 0–20 N with a ±0.025 N resolution, and the moment range was 0–100 N-mm with a ±0.003 N-mm resolution in the three mutually perpendicular axes. The target teeth (left maxillary central incisor and molar) were attached to the load cells with epoxy adhesive (Loctite E-120HP Hysol Epoxy Adhesive, Henkel, Rocky Hill, Conn) and then were completely separated from the acrylic dentoform, thus maintaining their original positions and orientations (Figure 2).
Figure 1.
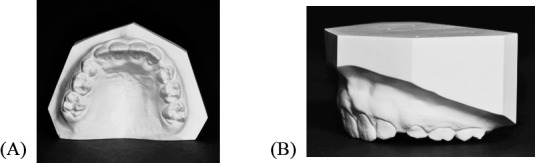
Ten identical stone models fabricated with retroclined incisors. (A) Occlusal view. (B) Left lateral view.
Table 1.
Two Size, 0.017 × 0.025-inch and 0.021 × 0.025-inch, Straight and Pretorqued NiTi Wires Were Engaged in 0.018 × 0.025-inch and 0.022 × 0.028-inch Slot Brackets, Respectively, With Three Different Bracket Prescriptions.

Figure 2.

Target teeth attached to orthodontic force testing load cells and then fully separated from the model. (A) Left central incisor. (B) Left molar. (C) The pretorqued wire ligated into brackets.
The rectangular NiTi pretorqued wire (Orthoforce G4 nickel-titanium Europa I, G&H Wire) featured a 34-mm wide, 20° torqued anterior segment connected to two flat 0° posterior segments. The straight rectangular NiTi and the pretorqued NiTi wires were 0.017 × 0.25-inch and 0.021 × 0.025-inch to correspond to the 0.018-inch and 0.022-inch bracket slots, respectively.
The load system was expressed at the center of the bracket, which was defined locally relative to each tooth. The faciolingual, mesiodistal, and inciso-occluso/apical axes of the teeth corresponded to the x, y, and z axes of the load cells, respectively. The transformation of the load system from the load cell to the bracket was accomplished by finding offset distances in the x, y, and z directions between the two coordinate systems as mentioned below:
A pure Fy was applied to the center of the bracket. The force (Fx, Fy, Fz) and moment (Mx, My, Mz) components along three axes were measured by the load cell. Since the force components were identical and their corresponding axes were parallel between the load cell and the bracket, the offsets in the x and z directions, Xoffset and Zoffset, were calculated as:
A pure Fx was then applied to the center of the bracket and the six load components were measured. The offset in the y direction, Yoffset, was calculated as:
The Xoffset, Yoffset, and Zoffset were input into the manufacturer software. The load component measured at the load cell coordinate systems was converted to the coordinate system on the bracket through Jacobian load system transformation. To validate the load transformation, a Fx was applied to the center of the bracket. If the Mz reading was negligible, the Yoffset was correct. Then, a Fy was applied to the center. If the Mx and Mz readings were negligible, the other two offsets were correct.
The load cells were initially zeroed. Each wire was manually inserted into the brackets and secured with 0.010-inch ligatures (Figure 2). Once secured, the two load cells' simultaneously measured force (Fx, Fy, Fz) and moment (Mx, My, Mz) components were recorded by a computer. To account for variability, each wire was removed after testing and visually inspected for damage, the orthodontic force tester was zeroed, the wire was reinserted and ligated in the same sequence, and then was retested. In total, this procedure was performed seven times per dentoform.
The sample size of seven observations for each of the 10 treatment combinations was estimated to reach 80% statistical power based on a previous study.13 This was sufficient to detect differences between any two treatment combinations of 0.7 N for Fx, 1.6 N for Fy, 0.5 N for Fz, 2.9 N-mm for Mx, 1.0 N-mm for My, and 4.1 N-mm for Mz, assuming two-sided tests each conducted at a 5% significance level. Three-way analysis of variance (ANOVA) was used to examine the effects of wire type, wire size/bracket slot size, and bracket type on the measurements. Interactions among the three effects were examined, and pair-wise comparisons between treatment combinations were performed when statistically significant. If no interactions were significant, overall comparisons of the three factors were performed.
RESULTS
Local coordinate axes for the forces and moments are shown in Figure 3. The force and moment components corresponding to the straight and pretorqued NiTi wires for 0.018-inch and 0.022-inch bracket slot sizes are shown in Figures 4 and 5. The three-way ANOVA interaction terms were significant for all force and moment measurements (P < .05), except for Fy. For Fy, the wire size/bracket type and wire type/wire size interactions were significant for incisors (P < .0001), and the wire type/bracket type interaction was significant for molars (P = .0109).
Figure 3.
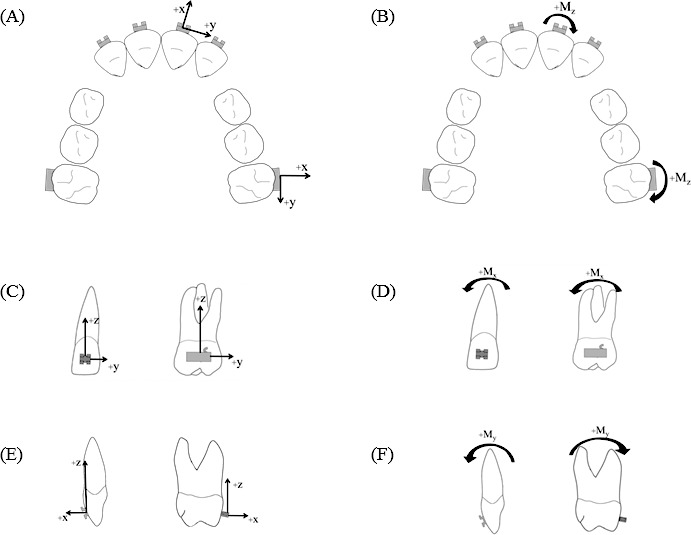
Local coordinate axes and moments on target teeth. (A) x and y axes, occlusal view. (B) +Mz direction, occlusal view. (C) z and y axes, facial view. (D) +Mx direction, facial view. (E) z and x axes, left lateral view. (F) +My direction, left lateral view.
Figure 4.
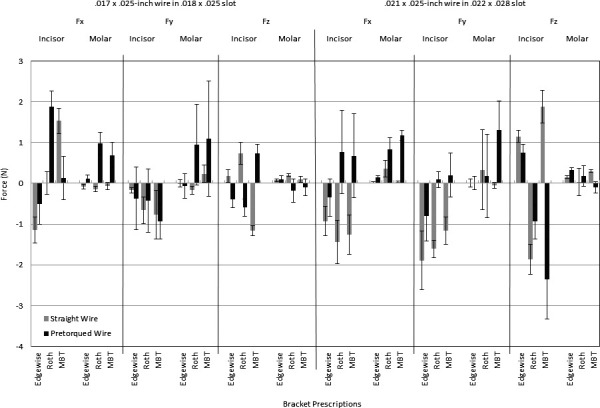
Three force components of the 0.017 × 0.025-inch and 0.021 × 0.025-inch sized wires engaged in the 0.018 × 0.025-inch and 0.022 × 0.028-inch slot brackets on the central incisor and the molar corresponding to the three bracket prescriptions.
Figure 5.
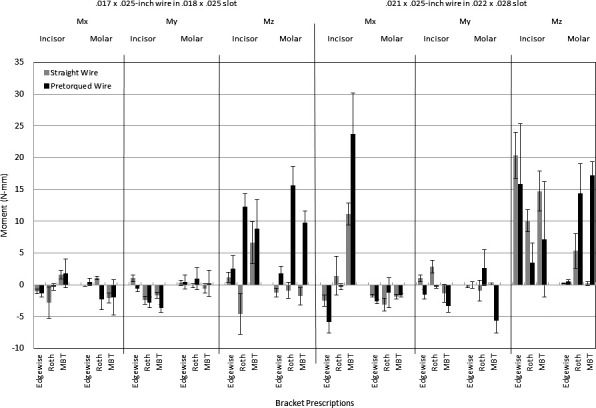
Three moment components of the 0.017 × 0.025-inch and 0.021 × 0.025-inch sized wires engaged in the 0.018 × 0.025-inch and 0.022 × 0.028-inch slot brackets on the central incisor and the molar corresponding to the three bracket prescriptions.
For both teeth, Fx was directed facially, except for the incisor with the 0.018-inch and 0.022-inch edgewise brackets (Figure 4). Compared to the straight NiTi counterparts, the Fx with pretorqued NiTi wires was significantly higher, except when considering the 0.022-inch molar and incisor edgewise brackets (nonsignificant) and 0.018-inch MBT incisor brackets (straight NiTi was significantly higher). In addition, the Roth prescription with the 0.017 × 0.025-inch pretorqued NiTi wire exhibited a significantly higher Fx than either the edgewise or the MBT prescriptions of the central incisor.
Although the three-way interaction was not significant for Fy, in general the incisor was directed mesial when a 0.017 × 0.025-inch wire was tied into all three bracket types (Figure 4). This is in contrast to the molar, which was directed distal with the 0.017 × 0.025-inch pretorqued NiTi wire in the Roth and MBT bracket types. The 0.021 × 0.025-inch pretorqued wire in the Roth and MBT prescriptions resulted in distal forces on the incisor; however, the large standard deviation needs to be considered. Both sizes of straight NiTi wires resulted in a mesially directed force on the incisor, while the molar demonstrated variable results depending on the bracket type.
The forces in the z direction experienced by the incisor were greater than the molar for both bracket sizes. Both sizes of the pretorqued NiTi wires in the MBT brackets experienced significantly greater Fz forces than the Roth and edgewise prescription brackets, with 0.021 × 0.025-inch exhibiting the highest (Figure 4).
Figure 5 depicts the three moment components for each bracket slot size. The incisor exhibited a significantly larger distal crown Mx moment (23.7 N-mm) with a 0.021 × 0.025-inch pretorqued NiTi wire in the MBT bracket compared to the edgewise and Roth brackets. A similarly directed distal crown moment on the central incisor occurred with the 0.017 × 0.025-inch pretorqued NiTi wire in the MBT bracket, however to a lesser magnitude (1.8 N-mm). Irrespective of wire and bracket type, the molar was directed with mesial crown moments in the 0.022-inch bracket size.
Moments in a negative My direction indicate FCT. With the 0.017 × 0.025-inch or 0.021 × 0.025-inch pretorqued wire, the incisor crown experienced a facial torquing moment (Figure 5). Except for the 0.022-inch Roth bracket, there was a significant difference in the incisor FCT between the straight and the pretorqued NiTi for both wire sizes such that the latter generated greater FCT. For both sizes of pretorqued NiTi wires, the incisor FCT was highest (P < .05) with the MBT bracket compared to the Roth and edgewise brackets (Figure 5). Furthermore, there was no significant difference in the FCT between the two wire sizes in the MBT bracket for the central incisor. The molar for both 0.018-inch and 0.022-inch brackets generally experienced small (<1.0 N-mm) My moments, except for those with pretorqued NiTi wires in the 0.022-inch Roth and 0.022-inch MBT brackets, which experienced larger and variable My moments.
When a pretorqued wire of either size was tested, both the incisor and molar experienced moments in a mesial out direction, as shown by the positive Mz moments in (Figure 5). However, with a 0.017 × 0.025-inch straight NiTi wire, the molar received a mesial in moment (−Mz). The 0.021 × 0.025-inch straight NiTi wire caused significantly higher mesial out moments than the pretorqued NiTi wire on the central incisor, except in the edgewise bracket (no difference between the two wires). In contrast, the 0.021 × 0.025-inch pretorqued NiTi wire caused significantly higher mesial out moments than the straight NiTi wire on the molar, except for the insignificant difference in the edgewise bracket.
DISCUSSION
With the evaluation of 20° pretorqued NiTi wire in a 3D clinically relevant load system, this study fills a void in the current literature. These data serve as the baseline for the quantification of two sizes of pretorqued NiTi wires in three bracket systems, and as such, it is difficult to draw direct comparisons with previous studies.
As indicated by the positive Fx, there was a significant amount of anterior and posterior facial force with the pretorqued wire in Roth and MBT. Isaacson et al.7 reported a facial movement when evaluating the torquing arch and thus recommended cinching the wire distal to the molar. Although they used the traditional edgewise system, it may be advisable to cinch the wire distal to the molar if facial movement is not a clinical objective. Additionally, despite efforts to select a wire form (Europa I) which approximated the arch form of the retroclined incisors, there was still a discrepancy between the two. As the flexible NiTi wires were engaged into the brackets, the arch form was distorted from its original shape, particularly in the anterior. This may explain the mesial incisor (−Fy) and distal (+Fy) molar forces and the mesial out (+Mz) moments (Figures 3 through 5).
The effects of bracket prescriptions are important to consider as well (Table 2). The molar brackets in Roth and MBT prescriptions feature, 8° and 10° mesial out offsets, respectively, thus contributing to the mesial out (+Mz) moments with the pretorqued wire. The MBT prescription elicited a significant distal crown/mesial root (+Mx) incisor moment, particularly with the 0.021 × 0.025-inch pretorqued wire. The 20° of FCT in the wire combined with the 17° built in the MBT prescription may result in a mesial convergence of the incisor roots, referred to by Andrews15 as the “wagon wheel” effect. With regard to FCT (−My) moments, there is an advantage to utilizing the MBT prescription with the pretorqued wire, as the amount of FCT was significantly higher than in the Roth and edgewise prescriptions. The 17° of FCT built into the MBT prescription compared to the 8° in Roth was sufficient to cause a significant difference in the amount of torque between the two with the pretorqued wire. There was no difference between wire sizes in the MBT prescription, which allows for practitioners of either bracket slot sizes to accomplish the same objective. Previously reported values on incisor FCT range from 5 to 20 N-mm.17 However, sources agree that the amount of clinically relevant incisor torque is unknown,4,17 especially when considering a flexible NiTi wire.5,11 Thus, the amounts of 3.6 and 3.3 N-mm of FCT from this study, although lower than previously reported values, may still be appropriate for clinical results.
Table 2.
Prescription Values as Given by the Manufacturer for the Roth and MBT Bracket Systems.

Potentially harmful in vivo side effects in the apical-occlusal/incisal directions (Fz) need to be closely monitored and evaluated with the pretorqued wire. Particularly for the incisor with the MBT prescription, the values were unpredictable, ranging from an extrusion of 2.3 N with the 0.021 × 0.025-inch wire to intrusion of 0.7 N with the 0.017 × 0.025-inch wire. For patients with excessive gingival incisor display, a 2 × 4 intrusion arch has been shown effective to intrude incisors.18 Since the pretorqued wire can possibly deliver extrusion forces, it might not be appropriate to use the pretorqued wire on patients with excessive gingival display. However, further investigations are still needed.
Although the experiment closely replicates a clinical situation, it fails to take into account several clinically relevant factors such as the effect of saliva, intraoral temperature effects, permanent damage to brackets or wires, long-term wire deactivation, variable interbracket distances, freedom of adjacent teeth, and the presence of a vital periodontal ligament. The lack of simulation of the buffering effects on the apparatus structures surrounding teeth might explain the high great variations in some force and moment measurements. Kroczek et al.15 utilized distilled water and silicon adhesive to simulate saliva and a periodontal ligament, however attributed no clinical significance. Additionally, due to current limitations of the number and size of load cells, the teeth adjacent to the target teeth could not be evaluated. Badawi et al.19 have shown promise of an orthodontic simulator utilizing 14 simultaneous load cells. Incorporation of these factors would increase the clinical significance of future studies with the pretorqued NiTi wire.
CONCLUSIONS
The pretorqued nickel-titanium wire in the MBT bracket prescription significantly shows the greatest incisor torquing moment, irrespective of wire size.
Side effects of the wire may need to be monitored closely in vivo.
Acknowledgments
We would like to thank G&H Wire Company for generous donation of supplies, Dr Thomas R. Katona for assistance with revisions, George Eckert for statistical analysis, and Feifei Jiang and Tom St. Clair for model setup.
REFERENCES
- 1.Meyer M, Nelson G. Preadjusted edgewise appliances: theory and practice. Am J Orthod. 1978;73:485–498. doi: 10.1016/0002-9416(78)90239-7. [DOI] [PubMed] [Google Scholar]
- 2.Thickett E, Taylor NG, Hodge T. Choosing a pre-adjusted orthodontic appliance prescription for anterior teeth. J Orthod. 2007;34:95–100. doi: 10.1179/146531207225021996. [DOI] [PubMed] [Google Scholar]
- 3.Miethke RR. Third order tooth movements with straight wire appliances. Influence of vestibular tooth crown morphology in the vertical plane. J Orofac Orthop. 1997;58:186–197. doi: 10.1007/BF02679959. [DOI] [PubMed] [Google Scholar]
- 4.Archambault A, Lacoursiere R, Badawi H, Major PW, Carey J, Flores-Mir C. Torque expression in stainless steel orthodontic brackets. Angle Orthod. 2010;80:201–210. doi: 10.2319/080508-352.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gioka C, Eliades T. Materials-induced variation in the torque expression of preadjusted appliances. Am J Orthod Dentofacial Orthop. 2004;125:323–328. doi: 10.1016/j.ajodo.2003.02.007. [DOI] [PubMed] [Google Scholar]
- 6.Brosius DJ, inventor 7244121, assignee. Torqued titanium-based archwire. 2007 [Google Scholar]
- 7.Isaacson RJ, Lindauer SJ, Rubenstein LK. Moments with the edgewise appliance: incisor torque control. Am J Orthod Dentofacial Orthop. 1993;103:428–438. doi: 10.1016/S0889-5406(05)81793-7. [DOI] [PubMed] [Google Scholar]
- 8.Isaacson RJ, Rebellato J. Two-couple orthodontic appliance systems: torquing arches. Semin Orthod. 1995;1:31–36. doi: 10.1016/s1073-8746(95)80086-7. [DOI] [PubMed] [Google Scholar]
- 9.Archambault A, Major TW, Carey JP, Heo G, Badawi H, Major PW. A comparison of torque expression between stainless steel, titanium molybdenum alloy, and copper nickel titanium wires in metallic self-ligating brackets. Angle Orthod. 2010;80:884–889. doi: 10.2319/102809-604.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Isaacson RJ, Lindauer SJ, Rubenstein LK. Activating a 2 × 4 appliance. Angle Orthod. 1993;63:17–24. doi: 10.1043/0003-3219(1993)063<0017:AAA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Jayade V, Annigeri S, Jayade C, Thawani P. Biomechanics of torque from twisted rectangular archwires. A finite element investigation. Angle Orthod. 2007;77:214–220. doi: 10.2319/0003-3219(2007)077[0214:BOTFTR]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Chen J, Bulucea I, Katona TR, Ofner S. Complete orthodontic load systems on teeth in a continuous full archwire: the role of triangular loop position. Am J Orthod Dentofacial Orthop. 2007;132:143.e1–e8. doi: 10.1016/j.ajodo.2006.10.016. [DOI] [PubMed] [Google Scholar]
- 13.Chen J, Isikbay SC, Brizendine EJ. Quantification of three-dimensional orthodontic force systems of T-loop archwires. Angle Orthod. 2010;80:566–570. doi: 10.2319/082509-484.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chen J, inventor Advanced Research and Technology Institute Inc, assignee. Apparatus and method for measuring orthodontic force applied by an orthodontic appliance. Sept 17, 2000 [Google Scholar]
- 15.Kroczek C, Kula K, Stewart K, Baldwin J, Fu T, Chen J. Comparison of the orthodontic load systems created with elastomeric power chain to close extraction spaces on different rectangular archwires. Am J Orthod Dentofac. 2012;141:262–268. doi: 10.1016/j.ajodo.2011.09.007. [DOI] [PubMed] [Google Scholar]
- 16.Andrews LF. The six keys to normal occlusion. Am J Orthod. 1972;62:296–309. doi: 10.1016/s0002-9416(72)90268-0. [DOI] [PubMed] [Google Scholar]
- 17.Gmyrek H, Bourauel C, Richter G, Harzer W. Torque capacity of metal and plastic brackets with reference to materials, application, technology and biomechanics. J Orofac Orthop. 2002;63:113–128. doi: 10.1007/s00056-002-0065-x. [DOI] [PubMed] [Google Scholar]
- 18.Senışık NE, Türkkahraman H. Treatment effects of intrusion arches and mini-implant systems in deepbite patients. Am J Orthod Dentofacial Orthop. 2012;141:723–733. doi: 10.1016/j.ajodo.2011.12.024. [DOI] [PubMed] [Google Scholar]
- 19.Badawi HM, Toogood RW, Carey JP, Heo G, Major PW. Three-dimensional orthodontic force measurements. Am J Orthod Dentofacial Orthop. 2009;136:518–528. doi: 10.1016/j.ajodo.2009.02.025. [DOI] [PubMed] [Google Scholar]