

Abstract
Objective:
To evaluate and compare the root surface morphological changes after 980-nm diode laser–aided circumferential supracrestal fiberotomy (CSF) on fluorosed and non-fluorosed teeth.
Materials and Methods:
The sample comprised 27 orthodontic patients (14 males and 13 females; mean age = 17.3 years) with and without fluorosis, from whom 40 fluorosed and 40 non-fluorosed premolar teeth were extracted for orthodontic reasons. Conventional (control group) and laser-aided (experimental group) CSF was performed on fluorosed and non-fluorosed teeth indicated for orthodontic extraction, using a scalpel and a 980-nm diode laser at 2.5 W power, respectively. Subsequently, teeth were extracted, sectioned, and examined by scanning electron microscope to assess the ultrastructural changes.
Results:
There were differences in surface morphology among fluorosed and non-fluorosed roots in the control group. The root specimens of both fluorosed and non-fluorosed teeth irradiated by diode laser exhibited no evidence of smear layer, laser-induced pitting or cavitation, linear cuts/markings, carbonization of surface, and heat-induced surface cracking. However, a glazed or slightly melted appearance was observed in root specimens of fluorosed teeth after diode laser irradiation.
Conclusions:
These findings suggest that the diode laser–aided CSF procedure is free from thermal hazard on non-fluorosed root surfaces but may provoke some thermal changes on fluorosed root surfaces.
Keywords: Circumferential supracrestal fiberotomy, Diode laser, Fluorosis, Orthodontic, Scanning electron microscopy
INTRODUCTION
The objective of the retention phase of orthodontic treatment is to maintain teeth in their corrected positions after active tooth movement.1 Retention is achieved by placing appliances, called retainers, on the teeth; by undertaking additional or adjunctive procedures; or by applying combination of these techniques.2 These adjunctive procedures include interproximal stripping or circumferential supracrestal fiberotomy (CSF), which are applied to the teeth or surrounding periodontium to aid the retention process.1
The conventional CSF technique consists of inserting a surgical blade into the gingival sulcus and severing the epithelial attachment surrounding the involved teeth.3,4 The blade also transects the transeptal fibers by interdentally entering the periodontal ligament space.4 Recently, a laser-aided CSF procedure using diode, carbon dioxide (CO2), and erbium-doped yttrium aluminum and garnet (Er:YAG) lasers has been attempted in an in vivo study5 that evaluated and compared the effects of this procedure on the morphology and chemical composition of the root surface of teeth extracted for orthodontic reasons. The results showed that laser-aided procedures, when used at appropriate laser settings, preserve the original morphology and chemical composition of cementum.
Dental fluorosis is a common complaint of patients from the Davangere District of Karnataka, India, which has naturally occurring high fluoride levels in the water. Dental fluorosis is known to cause hypomineralization of enamel6 and dentin.7 However, the impact of fluorosis on root cementum and periodontal ligament has not been adequately reported in the dental literature. A single in vitro study8 has compared the cementum and periodontal ligament changes in two groups of periodontally healthy fluorosed (HF) and healthy non-fluorosed (HNF) root surfaces by scanning electron microscope (SEM). Results showed that globular mineralized debris was 37.5% in the HF group compared with 6.25% in the HNF group. Likewise, partial/initial mineralization of connective tissue fibers (periodontal ligament area) was more extensive in the HF group (43.75%) than in the HNF group (18.75%).
Dentists, especially orthodontists working in regions where fluorosis is endemic, frequently experience difficulties in bonding brackets to fluorosed teeth as enamel fluorosis has been found to significantly decrease the bond strength of orthodontic brackets.9–12 The effect of diode lasers on fluorosed root cementum during laser-aided CSF needs to be investigated in cases where orthodontic patients with fluorosis are referred to a periodontist for a laser-aided CSF procedure. Therefore, an initial attempt has been made in this clinical study to evaluate and compare the root surface morphological changes after a 980-nm diode laser–aided CSF on fluorosed and non-fluorosed teeth.
MATERIALS AND METHODS
Teeth
Forty fluorosed and 40 non-fluorosed fresh human premolar teeth were used in this study. All the teeth had been extracted from patients undergoing orthodontic treatment with full-mouth brackets (bands or bonds) and archwires. The subjects for this study were selected from the departments of orthodontics and were treated in the department of periodontics at the College of Dental Sciences, Davangere, Karnataka, India, and Sri Venkateshwara Dental College, Bangalore, Karnataka, India. The study was conducted between October 2011 and January 2012. Of the 96 orthodontic patients examined, 27 subjects (14 males and 13 females; mean age = 17.3 years) met the inclusion criteria and agreed to participate in the study. From these 27 subjects, 3 subjects, each with fluorosed and non-fluorosed teeth, were randomly selected and assigned (by computer-generated tables) to the conventional CSF (control) group. This patient sample size yielded a total of 10 control and 30 experimental (diode laser–aided CSF) teeth each in the HF and HNF study groups (Table 1).
Table 1.
Characteristics of the Study Groupsa

Subjects were enrolled if they had a medical history showing good general health and at least 24 natural teeth in the mouth, excluding the third molars. Subjects were excluded from the study owing to any of the following reasons: if they were pregnant or were planning a pregnancy within the next 3 months, if they were taking antibiotics, if they had periodontitis or rampant dental caries based on a noninvasive examination, and if they were smokers. The study protocol, consent form, and instructions were approved by the Ethical Committee, Rajiv Gandhi University of Health Sciences, Karnataka, India, and the study was conducted on the basis of the principles outlined in the Declaration of Helsinki of 1975, as revised in 2008, on experimentation involving human subjects. The teeth were collected after receiving verbal and written consent to retain them for this study.
The extracted teeth had to meet the following inclusion criteria: for fluorosed teeth, fluorotic enamel stains were confirmed on the basis of clinical examination and history of the subjects hailing from areas in and around Davangere, Karnataka, India, with high amounts of fluoride naturally occurring in the water (fluoride concentration 1.5–3.0 ppm). Exclusion criteria were teeth with proximal caries extending to the cementum; root fractures; anatomical abnormalities; calculus deposits; restorations extending beyond the cementoenamel junction; and intrinsic stains caused by other reasons, such as porphyria, erythroblastosis fetalis, and tetracycline therapy.
The classification of fluorosed teeth was made by the consensus of two investigators (Dr Dhingra and Dr Vandana) using the Thylstrup-Fejerskov Index (TFI) index.13 These teeth were mildly fluorosed (TFI = 3) and were obtained from an area endemic for dental fluorosis (Davangere, Karnataka, India). The non-fluorosed teeth were acquired from a nonendemic area (Bangalore, Karnataka, India).
Treatment
Before beginning the CSF procedure, all the study patients received oral hygiene instructions and thorough supragingival scaling. Two weeks later, after resolution of clinical inflammation, the control group patients were subjected to a conventional CSF procedure under local anesthesia, as outlined by Edwards.3,4 The sulcus depth and biologic width were determined using a periodontal probe for each tooth (premolar) indicated for orthodontic extraction. The surgical blade (conventional CSF) or laser fiber tip (diode laser–aided CSF) was inserted intrasulcularly and interdentally up to the combination of this depth, just above the alveolar crest. No surgical dressing was placed after the conventional and diode laser–aided CSF procedures.
For the diode laser–aided CSF procedure, a 980-nm diode laser (Unilase Diode Laser, Unicorn Denmart Ltd, New Delhi, India) was used for the laser treatment in continuous focused mode at 2.5 W of power with a flexible glass fiber optic guide with a 400-µm spot diameter and power density of 1984 W/cm2. Similar to the previous study by Lee et al.,5 a laser-aided CSF procedure (without any anesthesia administration) was performed in a coronal-apical direction using parallel passes with the delivery tip angled at approximately 15°–20° to the root surface (Figure 1). This procedure was repeated until the full circumference of the tooth was irradiated. In cases of bleeding during the procedure, thorough saline irrigation was performed to prevent thermal damage to the root surface. The total working time for each tooth was 3 minutes. After surgery for one patient, the end of the fiber (2–3 mm) was cleaved to expose a fresh tip. The glass fiber optic was scored and removed to prevent cross-contamination between successive treatments.
Figure 1.

Diode laser–aided CSF.
The patients experienced no discomfort or pain during the conventional and diode laser–aided CSF procedures. Immediately after these procedures were completed, the treated teeth were atraumatically extracted (under local anesthesia) and immediately washed in running tap water and then stored in bottles containing 0.9% saline. Using a sterile diamond disk running at low speed with sterile water coolant, tooth specimens were sectioned at the cementoenamel junction to separate the crown from the root. This was followed by sectioning of the root, buccolingually, to yield two halves. This resulted in 80 root specimens in each group. Out of these 80 specimens, 60 root specimens served as the experimental group and 20 root specimens served as the control group.
Scanning Electron Microscopic Analysis
The root specimens were placed in 2.5% glutaraldehyde in 0.1 M phosphate buffer (pH 7.4) for a minimum of 24 hours. The specimens were then rinsed using three irrigation cycles with 10 mL of a 0.1 M phosphate-buffered solution. They were then dehydrated by 10-minute immersions in increasing concentrations of ethyl alcohol, that is, 70%, 80%, 90%, and 100%. After dehydration, the specimens were mounted on aluminum SEM stubs. Mounted specimens were air-dried for 48 hours and sputter coated with 30 to 40 nm of gold. Specimens were examined by SEM (JEOL-JSM-840A, operating at an accelerating voltage of 20 kV). Representative photomicrographs were obtained at ×50 and ×750 magnifications at the cervical region for all the experimental and control root specimens. One investigator (Dr Cobb), an experienced electron microscopist, was blinded to specimen treatment and evaluated all the photographs.
The SEM photomicrographs were assessed for the following findings: (a) surface melting or presence of smear layer, (b) laser-induced pitting or cavitation, (c) linear cuts/markings, (d) carbonization of surface, and (e) heat-induced surface cracking.
The findings of the SEM analysis were not statically analyzed, because the objective of the analysis was to perform a visual and qualitative comparison of the morphological effects of a 980-nm diode laser–aided CSF procedure on the HF and HNF root specimens.
RESULTS
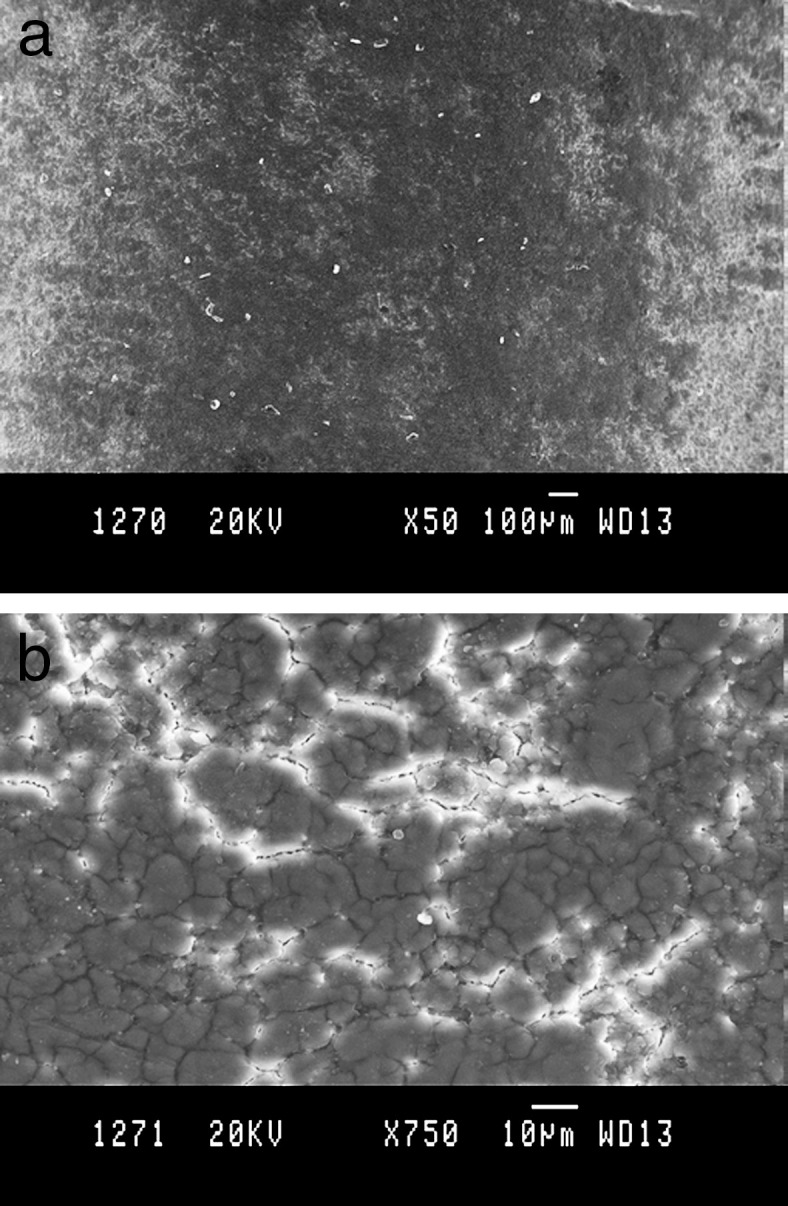
HF control specimens presented an undulating but smooth topography (Figures 2 and 3), whereas the HNF control specimens featured a relatively rough topography consisting of evenly distributed globular mounds of cementum of varying diameters (Figures 4 and 5).
Figure 2.
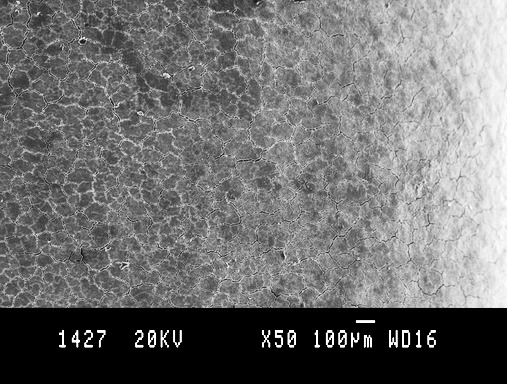
Untreated HF control specimen showing a smooth surface topography. Bar = 100 µm at an original magnification of 50×.
Figure 3.
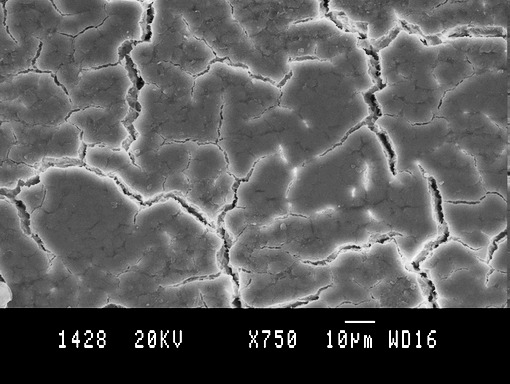
Higher magnification view of an untreated HF control specimen showing a smooth surface topography. Cracks are artifacts induced by dehydration during tissue processing. Bar = 10 µm at an original magnification of 750×.
Figure 4.
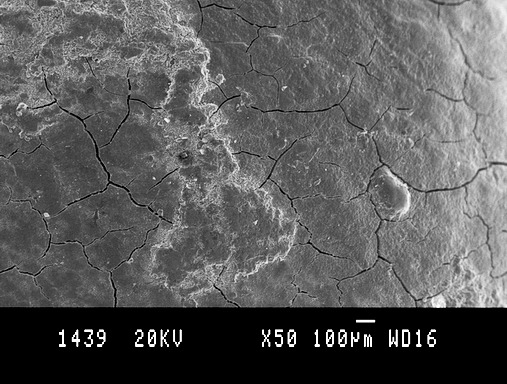
Low magnification view of an untreated HNF control specimen showing a relatively smooth surface. Bar = 100 µm at an original magnification of 50×.
Figure 5.
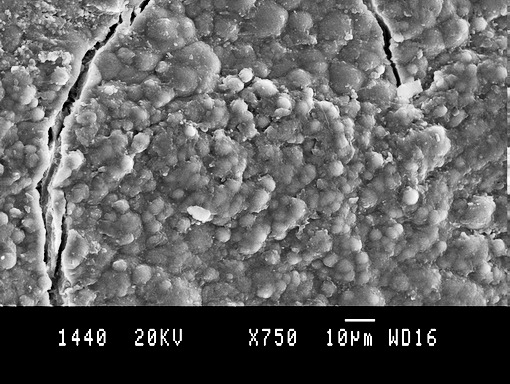
High magnification view of an untreated HNF control specimen showing a surface topography of evenly distributed globular mounds of cementum of varying diameters. Bar = 10 µm at an original magnification of 750×.
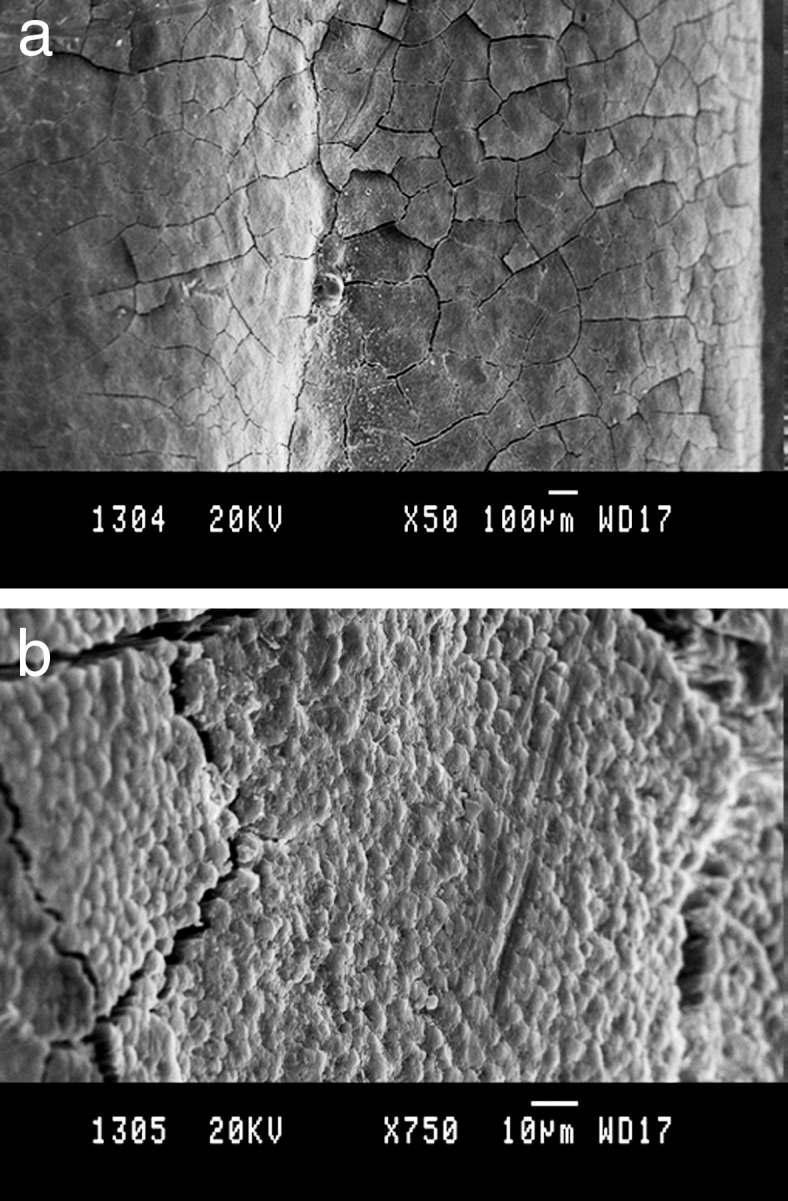
In both laser-treated HF and HNF specimens, there was no evidence of the presence of a smear layer, laser-induced pitting or cavitation, linear cuts/markings, carbonization of surface, or heat-induced surface cracking (Figures 6 and 7). However, root specimens in the HF group consistently exhibited a glazed or slightly melted appearance (Figure 6a,b).
Figure 6.
Lased HF specimen showing glazed or slightly melted appearance with absence of smear layer, laser-induced pitting or cavitation, linear cuts/markings, carbonization of surface, or heat-induced surface cracking. Bar = 10 µm at an original magnification of (a) 50× and (b) 750×.
Figure 7.
Lased HNF specimen featuring absence of surface melting/smear layer, laser-induced pitting or cavitation, linear cuts/markings, carbonization of surface, or heat-induced surface cracking. Bar = 10 µm at an original magnification of (a) 50× and (b) 750×.
DISCUSSION
Recently, in the field of orthodontics, diode lasers have been increasingly used in various procedures such as gingivectomy, frenectomy, operculectomy, papilla flattening, uncovering temporary anchorage devices, ablation of aphthous ulcerations, exposure of impacted teeth, and even tooth whitening.14 The reported advantages of diode lasers include excellent soft-tissue absorption and hemostasis, no interaction with hard tissues, ability to be used in contact mode providing tactile feedback, ability to be used for tooth bleaching, low cost, and small size.14 CSF, which was traditionally performed using a scalpel, was attempted with lasers in a recent study.5 In this study, laser-aided CSF procedure performed using an 808-nm diode laser showed no thermal changes on root surfaces of teeth (indicated for orthodontic extraction) extracted subsequently after the CSF procedure was performed. Using the same principles of laser-aided CSF by Lee et al.,5 we have attempted to evaluate and compare the root surface changes on root structure of periodontally healthy fluorosed (TFI = 3) and non-fluorosed teeth (indicated for orthodontic extraction) after irradiation with a 980-nm wavelength diode laser during a laser-aided CSF procedure.
Compared with HNF specimens, the HF root specimens exhibited higher, globular-shaped mineralized debris and partial/initial mineralization of connective tissue fibers in the periodontal ligament area.8 Furthermore, SEM images in the present study showed that the HF control group specimens have a smooth topography as opposed to the relatively rough topography (with evenly distributed globular mounds of cementum) in HNF control group root specimens.
The SEM observations of the diode laser–irradiated HF and HNF root specimens revealed the absence of smear layer, laser-induced pitting or cavitation, linear cuts/markings, carbonization of surface, and heat-induced surface cracking. Interestingly, a glazed or slightly melted appearance was noted in the HF root specimens. Although a conclusive interpretation of such results would be invalid, one might conjecture that the higher fluorapatite content or the higher energy settings possibly used in this study may have rendered the HF root specimens more susceptible to the melting of the mineral component. This melting phenomenon may also alter the biocompatibility of the root surfaces. However, to ascertain definitive evidence for these hypotheses, future studies need to evaluate temperature variations on the root surface and pulp, changes in chemical composition of the cementum, along with biocompatibility of such root surfaces through the adhesion and growth of cultured gingival fibroblasts after diode laser irradiation on the fluorosed roots (using similar or lower energy settings than this study). Furthermore, the clinical effects of these morphological and chemical root surface changes also need to be investigated by assessing such parameters as gingival inflammation, attachment loss, bone loss, and so on around the fluorosed teeth treated with laser-aided CSF.
The SEM observations in the present study were contradictory to those of Er:YAG laser irradiation (140 mJ/pulse and 10 Hz) on HF and HNF roots wherein, except for surface melting, surface alterations such as smear layer, open dentinal tubules, surface etching, and exposure of collagen tufts were noted with greater frequency in the HNF specimens than in the HF specimens.15 This variability of effect in HF and HNF specimens after diode laser and Er:YAG laser irradiation is analogous to the variable response to acid etching reported by Vandana et al.,16 who studied the effects of acid-induced surface etching on HF and HNF specimens using tetracycline hydrochloride (TCH), ethylenediaminetetraacetic acid (EDTA), and citric acid (CA). They reported that the HF group specimens exhibited more etching and smear layer formation when treated with TCH and CA than did HNF specimens. In contrast, when EDTA was used, the HNF specimens exhibited more surface etching and smear layer formation. Thus, it can be concluded that the variability between HF and HNF specimens after treatment by the diode laser, the Er:YAG laser, or mild acidic solutions indicates the need for a more refined research approach to determine possible clinical implications.
Only teeth specimens with a TFI score of 3 were used in this study as teeth with higher TFI scores are uncommon in Davangere district of Karnataka, India, and were therefore unavailable for the study. Therefore, further studies are required to assess the influence of high-intensity diode lasers on the root surfaces of fluorosed teeth with higher TFI scores and to evaluate and compare the surface and subsurface morphological and chemical changes after diode laser irradiation on HF and HNF root specimens during a laser-aided CSF procedure.
CONCLUSION
A laser-aided CSF procedure performed using a 980-nm diode laser showed no thermal changes on root surfaces of HNF teeth but slight melting was observed on the HF root surfaces.
Acknowledgment
The authors express their sincere thanks to Mr Gurulinga, Indian Institute of Science, Bangalore, Karnataka, India, for providing the scanning electron microscope facilities. The authors report no funding or conflicts of interest related to this study.
REFERENCES
- 1.Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Orthodontic retention: a systematic review. J Orthod. 2006;33:205–212. doi: 10.1179/146531205225021624. [DOI] [PubMed] [Google Scholar]
- 2.Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV. Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Syst Rev. 2006;Jan 25(1):CD002283. doi: 10.1002/14651858.CD002283.pub3. [DOI] [PubMed] [Google Scholar]
- 3.Edwards JG. A surgical procedure to eliminate rotational relapse. Am J Orthod. 1970;57:35–46. doi: 10.1016/0002-9416(70)90203-4. [DOI] [PubMed] [Google Scholar]
- 4.Edwards JG. A long-term prospective evaluation of the circumferential supracrestal fiberotomy in alleviating orthodontic relapse. Am J Orthod Dentofacial Orthop. 1988;93:380–387. doi: 10.1016/0889-5406(88)90096-0. [DOI] [PubMed] [Google Scholar]
- 5.Lee JW, Park KH, Chung JH, Kim SJ. Effects of laser-aided circumferential supracrestal fiberotomy on root surfaces. Angle Orthod. 2011;81:1021–1027. doi: 10.2319/121710-727.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fejerskov O, Manji F, Baelum V. The nature and mechanism of dental fluorosis in man. J Dent Res. 1990;69:692–700. doi: 10.1177/00220345900690S135. [DOI] [PubMed] [Google Scholar]
- 7.Vieira AP, Hancock R, Dumitriu M, Schwartz M, Limeback H, Grynpas M. Fluoride's effect on human dentin ultrasound velocity (elastic modulus) and tubule size. Eur J Oral Sci. 2006;114:83–88. doi: 10.1111/j.1600-0722.2006.00267.x. [DOI] [PubMed] [Google Scholar]
- 8.Vandana KL, George P, Cobb CM. Periodontal changes in fluorosed and non-fluorosed teeth by scanning electron microscopy. Fluoride. 2007;40:128–133. [Google Scholar]
- 9.Miller RA. Bonding fluorosed teeth: new materials for old problems. J Clin Orthod. 1995;29:424–427. [PubMed] [Google Scholar]
- 10.Adanir N, Türkkahraman H, Güngör AY. Effects of fluorosis and bleaching on shear bond strengths of orthodontic brackets. Eur J Dent. 2007;1:230–235. [PMC free article] [PubMed] [Google Scholar]
- 11.Noble J, Karaiskos NE, Wiltshire WA. In vivo bonding of orthodontic brackets to fluorosed enamel using an adhesion promoter. Angle Orthod. 2008;78:357–360. doi: 10.2319/020207-53.1. [DOI] [PubMed] [Google Scholar]
- 12.Adanir N, Türkkahraman H, Güngör AY. Effects of adhesion promoters on the shear bond strengths of orthodontic brackets to fluorosed enamel. Eur J Orthod. 2009;31:276–280. doi: 10.1093/ejo/cjn093. [DOI] [PubMed] [Google Scholar]
- 13.Thylstrup A, Fejerskov O. Clinical appearance of dental fluorosis in permanent teeth in relation to histologic changes. Community Dent Oral Epidemiol. 1978;6:315–328. doi: 10.1111/j.1600-0528.1978.tb01173.x. [DOI] [PubMed] [Google Scholar]
- 14.Kravitz ND, Kusnoto B. Soft-tissue lasers in orthodontics: an overview. Am J Orthod Dentofacial Orthop. 2008;133:S110–S114. doi: 10.1016/j.ajodo.2007.01.026. [DOI] [PubMed] [Google Scholar]
- 15.Dhingra K, Vandana KL, Shah A, Cobb CM. Effect of Er:YAG laser irradiation on fluorosed and nonfluorosed root surfaces: an in vitro study. J Oral Laser Applications. 2010;10:87–97. [Google Scholar]
- 16.Vandana KL, Sadanand K, Cobb CM, Desai R. Effects of Tetracycline, EDTA and citric acid application on fluorosed dentin and cementum surfaces: an in vitro study. Open Corrosion J. 2009;2:88–95. doi: 10.2174/1874210601610010109. [DOI] [PMC free article] [PubMed] [Google Scholar]