

Abstract
BACKGROUND:
Most household air pollution (HAP) interventions in developing countries of sub-Saharan Africa have focused on a single source, such as replacing polluting cooking sources with cleaner burning cooking stoves. Such interventions, however, have resulted in insufficient reductions in HAP levels and respiratory health risks in children. In this study we determined how multiple HAP combustion sources and exposure-mitigation factors in the home environment influence child respiratory health alone and in combination.
METHODS:
We carried out a case-control study to determine associations between multiple indicators of HAP and persistent cough among children (<15 years of age) seeking care at three primary-care clinics in Kampala, Uganda. HAP indicators included self-report of combustion sources inside the home (e.g., stove type, fuel type, and smoking); housing characteristics and cooking practices that mitigate HAP exposure (e.g., use of windows, location of cooking, location of children during cooking) and perceptions of neighborhood air quality. To explore joint associations between indicators of HAP, we applied a Bayesian clustering technique (Bayesian profile regression) to identify HAP indicator profiles most strongly associated with persistent cough in children.
RESULTS:
Most HAP indicators demonstrated significant positive bivariate associations with persistent cough among children, including fuel-type (kerosene), the number of hours burning solid fuels, use of polluting fuels (kerosene or candles) for lighting the home, tobacco smoking indoors, cooking indoors, cooking with children indoors, lack of windows in the cooking area, and not opening windows while cooking. Bayesian cluster analysis revealed 11 clusters of HAP indicator profiles. Compared to a reference cluster that was representative of the underlying study population cough prevalence, three clusters with profiles characterized by highly adverse HAP indicators resulted in ORs of 1.72 (95% credible interval: 1.15, 2.60), 4.74 (2.88, 8.0), and 8.6 (3.9, 23.9). Conversely, at least two clusters of HAP indicator-profiles were protective compared to the reference cluster, despite the fact that these protective HAP indicator profiles used solid fuels for cooking in combination with an unimproved stove (cooking was performed predominantly outdoors in these protective clusters).
CONCLUSIONS:
In addition to cooking fuel and type of cook stove, multiple HAP indicators were strongly associated with persistent cough in children. Bayesian profile regression revealed that the combination of HAP sources and HAP exposure-mitigating factors was driving risk of adverse cough associations in children, rather than any single HAP source at the home.
Keywords: household air pollution, clustering, respiratory, lung, Africa, urban
1. Introduction
Exposure to household air pollution (HAP) from combustion of solid fuels is recognized as a major health risk factor in developing countries (Health Effects Institute, 2018; Stanaway et al., 2018). Interventions designed to lower HAP levels or HAP-relevant respiratory health risks have largely been ineffective (Li et al., 2016; Mortimer et al., 2017; Quansah et al., 2017; Thomas et al., 2015; Yip et al., 2017). While stand-alone interventions like introduction of less-polluting cook stoves or cooking fuels into homes are generally capable of lowering HAP levels inside the home, such reductions may not be sufficient due to a variety of countervailing factors (Quansah et al., 2017). For instance, use of multiple polluting fuels (fuel stacking) combined with other relevant cooking practices and housing characteristics are capable of influencing HAP levels in conjunction with cooking fuel usage, which in turn influences childhood exposures and respiratory health effects to HAP indoors (Bruce et al., 2015; Sharma and Jain, 2019)(Fig. 1). The potential for public health benefits of HAP interventions in lower-income countries may therefore be hindered by a limited focus on cooking fuel or stove design alone (Pope et al., 2017; Quansah et al., 2017; Safdar, 2016).
Figure 1.
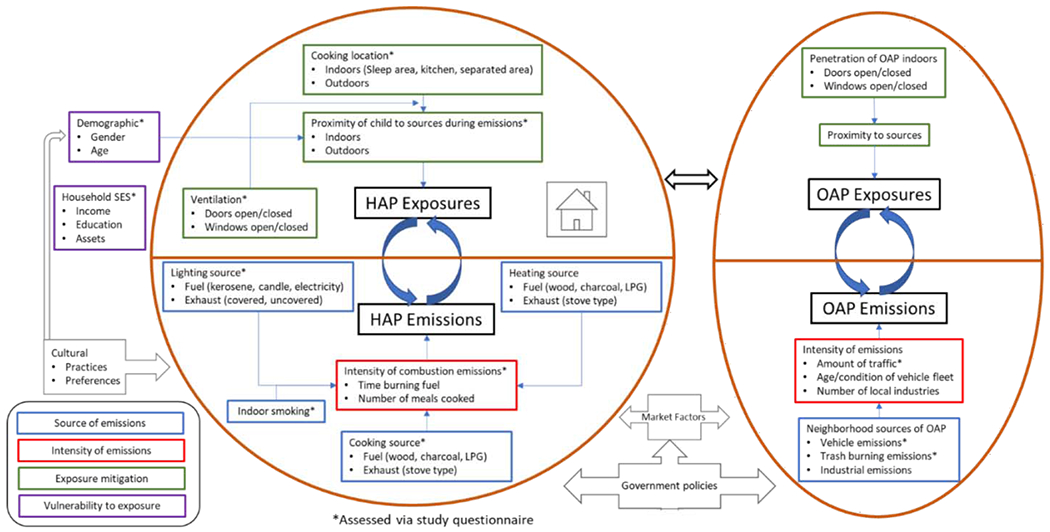
Viewing the complexities of childhood exposure to HAP as a consequence of multiple combustion source-emissions at the household-level, exposure mitigation-factors at the individual- and household-level, and intensity of fuel-use at the household level. Exposure to OAP may also influence added exposure intensity to air pollution while also influencing HAP levels inside the home. Exposure vulnerability may be further influenced by household SES and individual-level demographic factors. More peripheral factors, such as market forces and government policies, further influence emissions sources at the household and neighborhood level. Abbreviations: HAP, household air pollution; LPG, liquified petroleum gas; OAP, outdoor air pollution; SES, socioeconomic status.
To address this limitation, future HAP interventions in developing countries may need to be directed by data from epidemiologic studies that expand the scope of HAP factors such as including multiple household emission sources and exposure mitigating factors together with cooking-related emissions. The primary objective of our study is to assess the relationship of combined HAP emission sources and exposure factors on cough in children, including the type of cooking energy source and cook stove, the location of cooking (outside vs. indoors), ventilation from opening windows during cooking activities, proximity of children to cooking combustion sources in the home during cooking, use of kerosene for lighting the home, and second-hand smoke exposure from indoor tobacco smoking. The conceptual framework depicted in Figure 1 illustrates the plausibly correlated nature of the multiple HAP indicators considered in our study. As suggested in Fig. 1, the overarching hypothesis in our study is that, rather than exposure to any single source of HAP, such as exposure to solid fuels used for cooking at the home, it is the combination of HAP emission sources and HAP exposure-mitigating factors that drive associations with adverse respiratory health in children.
Figure 1 further suggests an analytic approach is critically needed that is capable of leveraging they type of high-dimensional and correlated HAP exposure assessment and socioeconomic status (SES) data derived from study questionnaires. Although the limitations of questionnaire-based exposure assessment for defining exposure-response relationships in HAP studies has long been recognized (Clark et al., 2013), there is still a role for questionnaire-based HAP exposure assessments in the developing country context. Collection of personal air pollution monitoring data, such as use of personal PM2.5 and CO monitors, is considered the gold-standard for exposure assessment in HAP epidemiology studies because it inherently integrates the multiple HAP sources and exposure factors into a single exposure metric. However, it is important to acknowledge that precise air pollution exposure assessment, which requires high quality personal air monitors and/or laboratory instruments, is often not feasible in many developing country settings. This lack of feasibility is due to the logistics involved with procuring the monitoring equipment, the limited availability of laboratory measurement instruments in-country, the high cost of the instruments, the technical expertise required for implementing personal exposure monitoring, the temporal/seasonal variability of HAP levels that personal exposure monitoring is typically unable to capture, and the complications inherent with personal exposure monitoring of vulnerable populations including children (Clark et al., 2013). In the face of such challenges, we propose the application of flexible multivariable epidemiological analysis frameworks for the developing country context—such as Bayesian profile regression (a model-based clustering approach)—that can better leverage the multidimensional and correlated that are inherent with questionnaire-based exposure assessments. Bayesian profile regression is a dimension-reduction, multivariable approach capable of handling data characterized by high dimensionality, multiple correlated variables (e.g., socioeconomic factors), and capable of handling both numerical and categorical data that are typical of questionnaire-based exposure assessment data. In the present study, we applied Bayesian profile regression as a means to comprehensively integrate multiple factors involved in the generation of HAP, combined with personal exposure factors and SES ascertained from a HAP exposure assessment questionnaire.
Against this backdrop, we carried out a case-control study to assess the association between multiple HAP indicators and persistent cough in children attending primary care clinics in Kampala, Uganda. We selected persistent cough as the study outcome primarily because of the large volume of children reporting to outpatient clinics with persistent cough in sub-Saharan Africa (KCCA, 2017; Kizito et al., 2018; Shields and Thavagnanam, 2013; Worrall, 2011). In addition, chronic or persistent cough in children can involve multiple factors including environmental triggers (Jo and Song, 2019; Morice, 2004), and such conditions may also be an indication of an underlying chronic respiratory disease (Morice, 2004; Shields and Thavagnanam, 2013), such as asthma, and chronic cough during childhood has been linked with chronic lung diseases in adulthood (Wang et al., 2018).
2.0. MATERIALS and METHODS
2.1. Study design and setting.
We conducted a case-control study in Kampala, Uganda, at three of the seven outpatient primary care clinics operated by the Kampala Capital City Authority (KCCA) in the urban communities of Kawaala, Kisenyi, and Kiswa. Kampala has 1.5 million residents and is the largest urban and commercial center of Uganda (UBOS, 2017). At KCCA facilities, children are seen in the pediatric outpatient department by a pediatrician, a medical officer, or one of several clinical officers. The most common conditions that patients seek care for at these clinics include acute conditions such as malaria and cold/flu symptoms (KCCA, 2017).
2.2. Study population and sampling design.
Between January 22, 2018 and May 30, 2018, trained community health workers—serving ass research staff—screened all consecutive children under the age of 15 years in the Pediatric Outpatient Department whose names were recorded in the Outpatient Register. Screened participants were eligible for our study if the parent or guardian of the child spoke and understood Luganda or English. Parents were asked if their child currently had a persistent cough of at least two weeks’ duration as part of universal screening for tuberculosis. We enrolled children with persistent cough as cases, and then identified two controls for every case among all children found to be without persistent cough. After we enrolled each case, we selected and enrolled controls nearest in time and age-matched to the case within the following age categories: (a) 0-4 years; (b) 5-9 years; and (c) 10-14 years. We selected controls from the same outpatient clinic as the respective cases and were seeking care for illnesses other than cough. Therefore, we expected that controls would be from the same source population. Parents gave written informed consent to participate in the study as approved by the institutional review boards of the University of California, Berkeley (Committee for Protection of Human Subjects; #2017-05-10001) and the Makerere University School of Public Health (Higher Degrees, Research and Ethics Committee; #535).
2.3. Questionnaire and data collection.
Trained community health workers pilot-tested the questionnaire on parents of eligible children for feasibility and comprehension. The community health workers interviewed parents of study participants at the clinics and in their preferred language (English or Luganda) using a standardized questionnaire that captured demographic, clinical, and household information about participants, including household socioeconomic status (SES), household crowding (number of people, number of rooms), respiratory symptoms of child participants, and an assessment of multiple HAP indicators (see Supporting Information for Study Questionnaire).
2.3.1. Assessment of HAP indicators
The study questionnaire assessed two types of HAP indicators: those that are considered combustion emission sources and those that can mitigate exposure of children to HAP (Fig. 1)(WHO, 2002). Indicators of HAP emission source were determined by assessing: (1) primary energy source for household cooking (wood, charcoal, kerosene, electricity, gas, or other); (2) primary energy source used for lighting the home (electricity, kerosene, candle, or other); (3) the type of cook stove typically used in the home (open fire without vent [locally known as ‘sigiri’], open fire with vent, closed fire without vent, closed fire with vent, electric stove); (4) an estimate of the length of time (in hours) spent burning solid fuel for cooking each day; (5) parental report on whether any household members smoked indoors; and (6) parental report about traffic-related air pollution in the neighborhood. Due to low cell numbers for cooking with wood and cooking with liquefied petroleum gas (LPG), we combined wood fuel and charcoal (‘solid fuel’) and combined LPG and electricity (‘improved fuel’) for the final regression analyses. Participants were asked about neighborhood sources of air pollution because the city of Kampala has no existing network for monitoring air quality. To assess this outdoor air pollution (OAP) source indicator we adapted previously validated questions from Piro et al. (2008) that asks participants about the level of concern (‘very concerned’, ‘somewhat concerned’, or ‘not concerned’) regarding air pollution from traffic in their neighborhood (Piro et al., 2008).
Indicators for mitigating child exposure to HAP were assessed (Fig. 1) by asking participants about the location of household cooking (indoors in the sleeping/main living area, indoors in a designated kitchen area, indoors in a structure separated from the home, or outdoors) and whether children were typically indoors or outdoors during cooking times. These indicators serve as surrogates of proximity to a HAP emissions from cooking (Fig. 1). As a surrogate for ventilation, we also asked parents about whether there is a window in the area where indoor cooking occurred. Among those with a window, we asked participants about frequency of opening windows during cooking (never, sometimes or rarely, most of the time, or always).
2.4. Statistical analysis
2.4.1. Covariate selection using Bayesian variable selection.
Candidate covariates were selected from the available literature of epidemiological studies conducted in sub-Saharan Africa that investigated associations between HAP and lower respiratory outcomes in children (Buchner and Rehfuess, 2015; Mustapha et al., 2011; Rehfuess et al., 2013). Candidate household-level covariates included monthly income, a summation of assets (as conducted by Young et al., 2019), educational attainment, and crowding (defined by number of occupants per room). Candidate individual-level covariates were child sex and age. A Bayesian variable selection approach was applied to determine final covariates for adjustment in the logistic regression models that evaluated associations between HAP indicators (e.g., indoor tobacco smoking) and cough. We used Bayesian variable selection because, unlike stepwise approaches, it accounts for model uncertainty through Markov chain Monte Carlo (MCMC) methods. We implemented Bayesian variable selection using the spikeSlabGAM package in R (version 1.1-11). Using the posterior inclusion probability (PIP) output from Bayesian variable selection, we selected a covariate as an ‘important’ covariate for adjustment if it resulted in a PIP ≥0.10. We fit continuous variables (e.g., income) in their original form but also included as a categorical factor variable and fit as a smoothed term. We selected whichever variable type resulted in the highest PIP (e.g., income continuous vs. income categorical). Hence, covariate adjustment was based on model fit as indicated by PIP. Additional detail on Bayesian variable selection is provided in the Supporting Information. This approach has been reviewed extensively elsewhere (Ishwaran and Rao, 2005; Malsiner-Walli and Wagner, 2018; Scott and Berger, 2010). Covariates selected for inclusion into adjusted models underwent multiple imputation with classification and regression trees (CART) (Burgette and Reiter, 2010) using the mice package (version 3.3.0) in R.
2.4.2. Fully adjusted logistic regression models
Fully adjusted logistic regression models were fit to assess exposure-response relationships for each HAP emission source and exposure-mitigating indicator. We fit all HAP indicator variables together in the same fully adjusted models, including the household SES and crowding indicator covariates. For example, indoor smoking was a covariate in the fully adjusted models in tandem with all other HAP indicator variables. Although we evaluated the associations between stove-type and persistent cough and between cooking fuel-type and cough, stove-type and fuel-type could not be evaluated in the same regression models due to collinearity between these two HAP indicators (97% of unimproved cook stove users used solid fuels). In Model 1 we included fuel-type in conjunction with all other HAP indicators. In Model 2 we included stove-type (unimproved versus improved) in conjunction with all other HAP indicators. We ran supplemental logistic regression models to characterize associations for HAP indicators that were relevant only under the scenario of indoor cooking, such as the association between cough and windows and opening of windows. We also tested the association between cough and length of cooking time among those who cooked with solid fuels because, compared to cooking with kerosene or improved energy sources, cooking with solid fuels necessitates lengthy fuel combustion periods to generate radiant heat and adequate cooking temperature. A statistical test for interaction between cooking location (an exposure mitigating factor) and exposure to type of cook stove and between cooking location and cooking fuel-type were also performed. Interaction terms with a p-value <0.05 were then analyzed in stratified models to assess the association with cough when cooking indoors only. A sub-analysis, stratified by different age groups (under five years of age and ages 5-14 years of age), was also performed using the above logistic regression approach (Tables S1 and S2). All summary statistics and regression analyses were computed using R (version 3.4.1).
2.4.3. Bayesian profile regression to assess joint effects
We used a Bayesian clustering approach, referred to as Bayesian profile regression (BPR), to explore possible joint effects between multiple HAP indicators and childhood cough. We implemented a cluster analysis because conventional regression methods are limited in their ability to capture joint effects for a large number of covariates (“the curse of dimensionality”). This limitation manifests as a loss of statistical power and a necessity for multiple comparisons when testing for interactions. In addition, analyses for interactions are challenging in the presence of collinearity between co-exposures of interest. BPR enables the analysis of correlated data (Liverani et al., 2016) by not only clustering individuals together with similar exposure profiles but simultaneously associating each cluster with the probability of an outcome (cough) at each iteration of the MCMC modeling (Coker et al., 2016; Molitor et al., 2010). Other advantages of using BPR, compared with other clustering algorithms like k-means, include the ability to analyze categorical as well as continuous covariates for clustering and the fact that there is no need to specify the number of clusters prior to analysis.
We implemented BPR using the same set of HAP and SES categorical variables that were used in logistic regression models. In the presentation of BPR results, we highlight the following: (1) the joint distribution of the HAP and SES indicator variables; (2) the posterior probabilities of cough for each cluster relative to the study population’s average probability of cough; and (3) computed odds ratios (OR) of cough for each cluster compared to a reference cluster (with uncertainty) as done in our previous work (Coker et al., 2017). To help with interpretation of the complex nature of the joint distribution of HAP and SES indicators, we generated heat-maps to display the intensity of HAP and SES indicators for each cluster in terms of adversity. BPR was implemented using the PReMiuM package (Liverani et al., 2015) in R (version 3.1.4).
3. Results
Between January 2018 and May 2018, 1314 parents were contacted for recruitment. Of these, 1311 parents were eligible for enrollment to serve as surrogates of child participants and 1294 were consented into the study (438 persistent cough cases and 856 controls). Characteristics of study participants and households overall and for cases and controls are summarized in Table 1. Compared to controls, children with cough ≥2 weeks (cases) were significantly more likely to come from more crowded homes (p<0.001) and households with lower income (p=0.007) and lower assets (p<0.001). There were no significant differences between cases and controls with respect to child characteristics such as age or sex or by parental age or preferred language (Table 1). According to the Bayesian variable selection results, household crowding (linear) and income (quartiles) were selected as covariates for the adjusted logistic regression models.
Table 1.
Characteristics of households, children, and parents, by case-control status.
| Characteristics (n, %a) | Total n=1294 | Caseb n=438 | Controlb n=856 | p-value |
|---|---|---|---|---|
| Household Characteristics | ||||
| Household crowding (#occupants/room) | <0.001 | |||
| 1-2 | 353 (27) | 93 (21) | 260 (30) | |
| 2-4 | 468 (36) | 156 (36) | 312 (37) | |
| 4-11 | 468 (36) | 186 (43) | 282 (33) | |
| Household education-level | 0.08 | |||
| None or < primary-level | 343 (28) | 129 (33) | 214 (26) | |
| Completed primary-level | 534 (44) | 164 (41) | 370 (46) | |
| Completed ordinary- or advanced-level | 332 (27) | 103 (26) | 229 (28) | |
| Monthly household income (converted to US currency) | 0.007 | |||
| 0 – 39 | 466 (40) | 186 (47) | 280 (36) | |
| 40 – 79 | 427 (36) | 125 (31) | 302 (39) | |
| 80 – 159 | 230 (20) | 73 (18) | 157 (20) | |
| >159 | 52 (4) | 16 (4) | 36 (5) | |
| Household assets indexc | <0.001 | |||
| 6 - 7 | 412 (32) | 175 (40) | 412 (28) | |
| 7 - 8 | 512 (40) | 154 (36) | 512 (42) | |
| 8 - 9 | 248 (19) | 77 (18) | 248 (20) | |
| 9 - 12 | 108 (8) | 27 (6) | 108 (10) | |
|
| ||||
| Child Characteristics | ||||
| Sex | 0.81 | |||
| Boy | 572 (52) | 189 (51) | 381 (52) | |
| Girl | 523 (48) | 178 (49) | 345 (48) | |
| Age groups | 0.91 | |||
| <5 years | 900 (69) | 307 (70) | 589 (69) | |
| 5-9 years | 310 (24) | 102 (23) | 208 (24) | |
| 10-14 years | 87 (7) | 29 (7) | 57 (7) | |
|
| ||||
| Parental participant characteristics | ||||
| Age groups | 0.43 | |||
| 18-20 years | 110 (9) | 34 (8) | 76 (9) | |
| 21-25 years | 346 (27) | 108 (25) | 238 (28) | |
| 26-30 years | 450 (35) | 158 (36) | 292 (34) | |
| 31-35 years | 222 (17) | 74 (17) | 148 (17) | |
| 36-69 years | 164 (13) | 64 (15) | 100 (12) | |
| Language preference of participant | >0.99 | |||
| Luganda | 1178 (92) | 398 (92) | 780 (92) | |
| English | 108 (8) | 36 (8) | 72 (8) | |
Column totals may not add up uniformly due to missing observations.
Cases defined as child with a current cough lasting at least 2 weeks. Controls are those without a current cough for 2 weeks.
Household assets index is a composite summation score of multiple assets reported for each study household, including electricity, a television, a motor vehicle, a closet (‘wardrobe), a CD or DVD player, and a Bicycle (range: 6-12; no=1 and yes=2 for each asset). An increasing assets index indicates an increasing number of household assets.
3.1. Associations between source of HAP and persistent cough
Table 2 summarizes frequencies of source-specific HAP indicators overall in addition to cough prevalence for each category of HAP indicators. Crude and adjusted ORs are reported in Table 3. Unadjusted logistic regression models (Table 3) showed significant persistent cough associations for children in households where kerosene was used for cooking, an energy source other than electricity was used for lighting, and where another occupant smoked indoors. There were no significant unadjusted associations between cough and type of cooking stove used in the household or between cough and exposure to cooking with solid fuels. Relative to using an improved cooking fuel (electricity or LPG), the adjusted odds of cough were higher with use of kerosene for cooking (aOR 4.18, 95%CI 1.54, 12.1, p=0.006) but not with use of solid fuels (charcoal or wood) for cooking (aOR 1.60, 95%CI 0.87, 3.09, p=0.14). Exposure to cooking with an unimproved stove was also not significantly associated with cough in the adjusted model (aOR 1.26, 95%CI 0.72, 2.30, p=0.43). Exposure to indoor cigarette smoking compared to no smoking exposure was strongly associated with higher cough prevalence (aOR=4.59 [2.87, 7.50], p<0.001), as was exposure to a polluting fuel (a candle or kerosene) for lighting the home compared to exposure to electricity for lighting (aOR=1.44 [1.20, 2.03], p=0.04). In both unadjusted and adjusted models, relative to reporting no concern over traffic-related air pollution in the neighborhood, being very concerned was associated with significantly higher odds of persistent cough (aOR=2.12 [1.57, 2.86], p<0.001) (Table 3). Among those who cooked with solid fuels, a 10% increase in the number of hours cooking with solid fuels was also positively associated with persistent cough (aOR=1.03 [1.01, 1.06]).
Table 2.
Frequency of HAP indicators and frequency of cases and controls by HAP indicators.
| HAP Indicators (n, % a) | Overall | Case n=438 | Control n=856 | χ2 p-value |
|---|---|---|---|---|
|
Source of HAP Emissions
| ||||
| Cooking fuel-type | <0.001 | |||
| Electricity | 46 (4) | 16 (4) | 30 (4) | |
| Charcoal | 1116 (86) | 361 (82) | 755 (88) | |
| Wood | 82 (6) | 37 (8) | 45 (5) | |
| Kerosene | 33 (3) | 24 (5) | 9 (1) | |
| LPG | 14 (1) | 0 (0) | 14 (2) | |
| Other | 2 (<1) | 0 (0) | 2 (<1) | |
| Cooking stove-type | 0.77 | |||
| Improved stove | 68 (6) | 21 (5) | 47 (6) | |
| Traditional stove | 1142(94) | 381 (95) | 761(94) | |
| Energy source for lighting home | <0.001 | |||
| Electricity | 1062(84) | 323 (76) | 739 (88) | |
| Kerosene – open wick | 41 (3) | 25 (6) | 16 (2) | |
| Kerosene lantern | 53 (4) | 30 (7) | 23 (3) | |
| Candle | 113 (9) | 49 (11) | 64 (8) | |
| Indoor tobacco smoking | <0.001 | |||
| No | 1186 (92) | 361 (83) | 825 (96) | |
| Yes | 106 (8) | 76 (17) | 30 (4) | |
|
| ||||
|
Mitigation of HAP Exposures
| ||||
| Cooking location | <0.001 | |||
| Outdoors | 533 (41) | 118 (27) | 415 (49) | |
| Indoor – sleeping area | 359 (28) | 183 (42) | 176 (21) | |
| Indoors – kitchen in home | 272 (21) | 82 (19) | 190 (22) | |
| Indoors – separate room/unattached | 129 (10) | 55 (13) | 74 (9) | |
| Child indoors during cooking | <0.001 | |||
| No | 573 (44) | 156 (36) | 417 (49) | |
| Yes | 715 (56) | 279 (64) | 436 (51) | |
| Use of windows while cookingc | <0.001 | |||
| Always or most of the time | 284 (51) | 86 (39) | 198 (59) | |
| About half or sometimes | 197 (35) | 100 (45) | 97 (29) | |
| Never | 75 (15) | 37 (16) | 38 (12) | |
| Windows in cooking aread | <0.001 | |||
| Yes | 559 (75) | 225 (71) | 334 (77) | |
| No | 189 (25) | 92 (29) | 97 (23) | |
|
| ||||
|
Emissions intensity
| ||||
| Number of hours cookinge | 0.05 | |||
| 1-2 | 407 (34) | 113 (28) | 294 (36) | |
| 2-3 | 235 (19) | 79 (20) | 156 (19) | |
| 3-6 | 387 (32) | 137 (35) | 250 (31) | |
| 6-12 | 181 (15) | 68 (17) | 113 (14) | |
| Self-reported concern over traffic-related OAP | <0.001 | |||
| Not concerned | 717 (56) | 197 (45) | 520 (61) | |
| Somewhat concerned | 185 (21) | 90 (21) | 185 (22) | |
| Very concerned | 296 (23) | 149 (34) | 147(17) | |
Notes: The case and control columns summarize the number and percentage of cases or controls within each level of a particular categorical variable. Chi-squared test statistic tests differences in cases between different levels of the categorical variables.
Column totals may not add up uniformly due to missing observation and skip patterns in the study questionnaire.
Traditional stove is an unvented solid fuel stove (‘sigiri’), three-stone fire or kerosene stove, and an improved stove is an electric, LPG, or a vented solid fuel stove.
Among those who cook indoor and have a window in the cooking area
Among those who cook indoors
Among those who cook with wood or charcoal
Abbreviations: HAP, household air pollution; LPG, liquified petroleum gas; OAP, outdoor air pollution
Table 3.
Crude and adjusted associations between HAP indicators and cough.
| Crude OR (95% CI) | Model 1 aOR (95% CI)a,b | Model 2 aOR (95% CI)a,b | |
|---|---|---|---|
|
Source of HAP emissions
| |||
| Cooking fuel | |||
| Electricity/LPG | Reference | Reference | - |
| Kerosene | 7.33 (2.91, 19.9) | 4.18 (1.54, 12.1) | |
| Solid fuel (wood or charcoal) | 1.37 (0.78, 2.53) | 1.60 (0.87, 3.09) | - |
| Unimproved stovec | - | ||
| Yes | 1.12 (0.67, 1.94) | - | 1.26 (0.72, 2.30) |
| Smoking inside the home | |||
| Yes | 5.79 (3.77, 9.12) | 4.59 (2.87, 7.50) | 4.80 (2.91, 8.11) |
| Energy source for lighting the home | |||
| Electricity | Reference | Reference | Reference |
| Polluting fuel (candle or kerosene) | 2.31 (1.71, 3.13) | 1.44 (1.20, 2.03) | 1.35 (0.93, 1.96) |
|
| |||
|
Mitigation of HAP exposure
| |||
| Cooking location | |||
| Outdoors | Reference | Reference | Reference |
| Sleeping/Living area | 3.66 (2.74, 4.90) | 2.79 (2.01, 3.88) | 3.14 (2.04, 4.83) |
| Separate structure | 2.61 (1.74, 3.91) | 2.66 (1.72, 4.11) | 2.74 (1.54, 4.88) |
| Kitchen | 1.52 (1.09, 2.11) | 1.58 (1.10, 2.27) | 2.33 (1.45, 3.75) |
| Child indoors during cooking | |||
| Yes | 1.71 (1.35, 2.17) | 1.47 (1.12, 1.92) | 1.42 (1.08, 1.88) |
|
| |||
|
OAP emission source
| |||
| Traffic-related air pollution | |||
| Not concerned | Reference | Reference | Reference |
| Very concerned | 2.68 (2.02, 3.55) | 2.12 (1.55, 2.90) | 2.04 (1.40, 2.99) |
| Somewhat concerned | 1.28 (0.95, 1.73) | 1.13 (0.81, 1.56) | 1.16 (0.76, 1.77) |
|
| |||
|
Household SES
| |||
| Number of occupants per room | 1.14 (1.06, 1.24) | 1.09 (0.99, 1.20) | 1.09 (0.99, 1.20) |
| Monthly household income (in USD) | |||
| 0 - 39 | Reference | Reference | Reference |
| 40 - 79 | 0.65 (0.50, 0.84) | 0.76 (0.56, 1.04) | 0.83 (0.61, 1.13) |
| 80 - 159 | 0.69 (0.50, 0.94) | 1.00 (0.70; 1.44) | 1.15 (0.80, 1.66) |
| >159 | 0.66 (0.35, 1.20) | 0.89 (0.44, 1.73) | 0.97 (0.48, 1.88) |
Model 1 includes type of cooking fuel as a covariate and Model 2 includes type of cook stove as a covariate. Cooking fuel and stove type could not be assessed in the same model due to collinearity (99% of those who cooked with solid fuels used an unimproved stove and 100% of those who cooked with kerosene used an unimproved stove). In addition, by definition cooking with electricity was classified as an improved stove.
Adjusted for household crowding and household income quartiles.
Unimproved stove was defined as a stove used for cooking that has an open combustion flame but does not have a chimney or hood.
Abbreviations: HAP, household air pollution; LPG, liquified petroleum gas; OAP, outdoor air pollution
3.2. Associations between HAP exposure mitigating factors and persistent cough
Unadjusted logistic regression models (Table 3) indicated persistent cough was significantly more prevalent among children from homes where cooking was performed indoors, including in the sleeping area, a designated kitchen, or a separate room unattached to the home. Unadjusted odds of cough were also significantly higher among children who were typically indoors during cooking times. Results from adjusted models—summarized in Table 3—were consistent with unadjusted results. Compared to cooking outside, cooking in the sleeping or main living area was associated with higher adjusted odds of cough (aOR=2.79 [2.01, 3.88], p<0.001), while cooking in a designated kitchen (aOR=1.58 [1.10, 2.27], p=0.01) or in a separate structure (aOR=2.66 [1.72, 4.11], p<0.001) also were associated with significantly higher adjusted odds of persistent cough. Children being indoors during cooking times was associated with higher odds of cough (OR=1.44 [1.20, 2.03], p=0.006).
According to separate models that tested for interaction between cooking location (outdoors vs. indoors) and cooking-related HAP sources (cooking fuel or stove-type), we observed significant interactions (p<0.01). Stratified models showed that exposure to cooking indoors with an unimproved stove, compared to cooking indoors with an improved stove, resulted in an adverse association (OR=1.85 [0.99, 3.57]). Conversely, using an unimproved stove outdoors compared to using an improved stove outdoors resulted in a protective association (OR=0.11 [0.02, 0.47]). Exposure to cooking indoors with solid fuel resulted in increased odds of persistent cough (OR=2.37 [1.22, 4.94]) compared to exposure to cooking indoors with an improved fuel. Conversely, exposure to solid fuels outdoors compared to an improved fuel outdoors resulted in a protective association (OR=0.05 [0.002, 0.33]). It should be noted that while exposure to cooking outdoors with an unimproved stove or solid fuel was protective compared to improved stove or fuel, just eight participants with an improved stove (reference group) and just five participants with an improved fuel cooked outdoors. Therefore, associations for outdoor cooking should be interpreted with caution given such few number of participants in the reference group for this outdoor cooking strata. Similarly, the association between cooking with kerosene and cough strengthened among those who cooked indoors also (OR=7.09 [2.48, 22.07]), compared to regression models that included both indoor and outdoor cooking. Also of note, only one participant who reported cooking with kerosene also reported cooking outdoors, thus making the comparison stratified outdoors kerosene cooking association (data not shown) an unreliable effect estimate.
When restricting the analysis to children from households where cooking occurs indoors only, we compared to those who reported using a window always or most of the time during cooking, and found that having no windows (aOR=1.90 [1.24, 2.91]), never using windows (aOR=1.62 [0.88, 2.96]), and using windows only some or half of the time (aOR=1.73 [1.13, 2.65]) were each associated with higher adjusted odds of persistent cough.
3.3. Associations between HAP indicator profiles and persistent cough
BPR analysis resulted in 11 clusters. Table 4 summarizes the number of participants and prevalence of cough cases for each cluster. The full posterior distributions from the MCMC output, for the 12 HAP and SES indicators, are presented in the Supplemental Materials (Fig. S1). As summarized in Table 4, the observed prevalence of cough was highest for cluster 11 (91%) and cluster 10 (80%) and lowest for clusters 1 (20%), 2 (21%) and 3 (20%). Fig. 2a displays the ORs for each cluster, when setting cluster 5 as a reference cluster. Cluster 5 was selected as a reference cluster because it has a cough prevalence (32%) closest to the underlying cough prevalence for the study population. Clusters with the highest odds ratios with a credible intervals (CrI) that does not overlap with the null include cluster 9 (OR=1.72 [95% CrI: 1.15, 2.60]), cluster 10 (OR=4.74 [95% CrI: 2.88, 8.0]), and cluster 11 (OR=8.61 [95% CrI: 3.87, 23.9]). According to Fig. 2a, two clusters resulted in cough odds ratios below 1 that did not include the null. Specifically, cluster 1 (OR=0.52 [95% credible interval: 0.34, 0.77]) and cluster 2 (OR=0.55 [0.36, 0.84]) resulted in lower odds of cough. While clusters 3 and 4 resulted in lower odds of cough compared to cluster 5, the 95% CrIs included the null. Even though cluster 7 resulted in elevated cough prevalence (80%), this cluster was comprised of just 5 children and therefore does not lend itself to an informed interpretation (wide CrIs; Fig. 2a) given the small sample size (Table 4).
Table 4.
Summary of clusters based on households with similar profiles of HAP indicators as derived from Bayesian Profile Regression.
| Cluster Number | Number of cluster membersa | Percent with cougha | Odds Ratio (95% credible interval)b |
|---|---|---|---|
| 1 | 283 | 20.3% | 0.52 (0.34, 0.77) |
| 2 | 221 | 21.3% | 0.55 (0.36, 0.84) |
| 3 | 54 | 20.4% | 0.63 (0.30, 1.25) |
| 4 | 147 | 25.2% | 0.86 (0.56, 1.32) |
| 5 | 198 | 32.3% | Reference |
| 6 | 24 | 37.5% | 1.16 (0.47, 2.58) |
| 7 | 5 | 80.0% | 1.84 (0.41, 29.52) |
| 8 | 87 | 35.6% | 1.39 (0.84, 2.28) |
| 9 | 140 | 46.4% | 1.72 (1.15, 2.60) |
| 10 | 100 | 80.0% | 4.74 (2.88, 8.0) |
| 11 | 35 | 91.4% | 8.61 (3.87, 23.9) |
Notes: Cluster number has no inherent meaning beyond labeling of distinct clusters identified in the BPR analysis.
Does not incorporate the uncertainty propagated by BPR’s MCMC method because it uses the final “hard” cluster assignments from the BPR output.
Incorporates the uncertainty propagated by BPR’s MCMC method.
Figure 2.
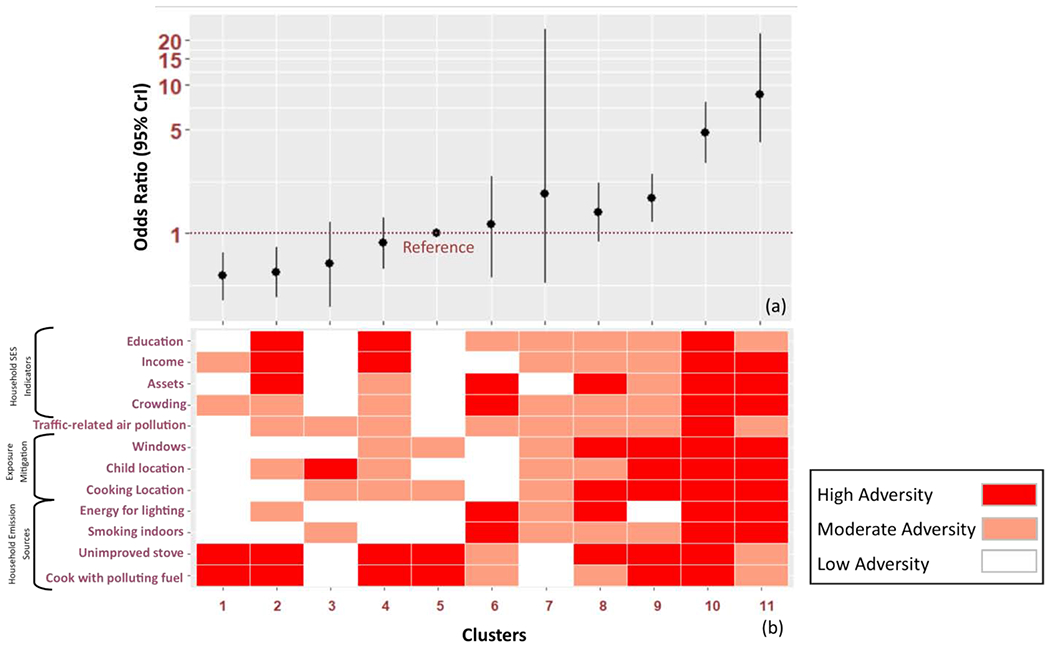
Exposure profile results from Bayesian profile regression (BPR). Panel (a) displays the cough OR for each cluster and corresponding 95% credible intervals, with cluster number 5 set as the reference cluster. Panel (b) displays a qualitative characterization of HAP/SES indicator profiles for each cluster, with darker red colors characteristic of high adversity conditions and lighter colors characteristic of low adversity conditions for a particular indicator. Adversity for the HAP indicators, in this context, was derived from interpretations of the logistic regression models indicating whether the HAP indicator variable resulted in an adverse association with cough. Figure S1 in the appendix displays the full quantitative posterior distributions of the exposure profile output from the BPR analysis.
In Fig. 2b we use a heat-map to indicate the relative adversity of HAP and SES indicators (rows) for each cluster (columns). The variables shown in this heat-map are ordered by HAP sources or exposure mitigation factors, and the colors represent the established cut points within each category in terms of indicating low adversity (white tiles), moderate adversity (light red tiles), or high adversity (dark red tiles). Compared to the overall study population frequencies (or average) for each HAP indicator (Table 2), the joint distribution of HAP sources, exposure mitigating factors, and traffic-related air pollution was highly adverse (dark red tiles) for clusters 10 and 11 (Fig. 2). In cluster 11, for example, 97% used solid fuel or kerosene for cooking, 53% had an occupant who smoked indoors, and 97% used a polluting energy source for lighting the home. In terms of exposure mitigation, 100% cooked indoors, 89% had children indoors during cooking (89%), and 100% had no window in the cooking area. Nearly half (40%) of cluster 11 participants reported being very concerned about traffic-related air pollution. Cluster 10 had even higher levels of solid fuel or kerosene for cooking (100%) and using an unimproved stove (98%). Cluster 10 also had the highest percentages for cooking indoors in the area where occupants sleep (99%), child indoors during cooking (95%), never or only sometimes opening a window during cooking (81%). More than half (51%) in cluster 10 reported being very concerned over traffic-related air pollution. The other cluster with significantly elevated cough, cluster 9, differed from clusters 10 and 11 on key HAP sources. For instance, 100% of the cluster 9 participants used electricity for lighting (protective against HAP) and only 9% of cluster 9 participants had an occupant that smoked indoors. When comparing the clusters with elevated cough against the reference cluster (cluster 5), a few HAP indicators stand out as substantially different. Specifically, children were predominantly indoors during cooking for all three of the elevated cough clusters, whereas children were outdoors during cooking for the reference cluster (even though participants in cluster 5 report high levels of exposure to solid fuels [99%] and unimproved stoves [99%] for cooking and cooking indoors [91%]). Other important differences for the reference cluster include low indoor tobacco smoking (4.5%), high usage of electricity for lighting (100%), and low levels of concern about traffic-related air pollution (17%), high usage of always opening windows low crowding (63%), and high SES.
Clusters 1, 2 and 3 resulted in low cough prevalence of 20%, 21% and 20%, respectively, which are all well below the average cough percentage of 34% for the study population. As indicated in Fig. 2b, these three clusters resulted in low levels of risk factors for most HAP indicators. Although nearly all households in cluster 1 and cluster 2 were exposed to cooking with solid fuels and cooking an unimproved cook stove, 100% of households in these two clusters cooked outdoors. Similar to the reference cluster 5, clusters 1 and 2 had very low indoor tobacco smoking indoors and low use of polluting fuels for lighting. The major difference between clusters 1 and 2 compared to the reference cluster was cooking location. While cluster 3 was also characterized by low cough prevalence, yet resulted in an association that included the null, this cluster was relatively small (N=54) which contributed to the large CrI. The major difference between cluster 3 and the reference cluster 5 was cooking fuel and stove type, with 100% of participants in cluster 3 reporting use of an improved fuel (electricity or gas) as well as an improved stove and 76% of participants reporting having the child indoors during cooking (child indoors was just 39% in cluster 5).
DISCUSSION
Among children who reside in mostly low-income households in Kampala, we show that cooking-related HAP sources, such as cooking with polluting fuels and unimproved stoves indoors, are adversely associated with persistent cough. The data also show other indicators of HAP and OAP emissions sources —unrelated to cooking— and exposure mitigating factors have equally large (if not larger) adverse associations with cough. Moreover, our analyses suggest strong joint effects between indicators of multiple emission sources and exposure-mitigating factors.
Importantly, we found that the association between cough and exposure to cooking with solid fuels could be dependent on cooking location. Specifically, we observed an adverse association with cough only when children were exposed to cooking with solid fuels indoors only (relative to cooking indoors with an improved fuel). This finding is supported by recent findings in the literature. A recent study conducted in Rwanda (Das et al., 2018) similarly found the adverse association between solid fuel and childhood cough only occurred in those exposed to indoor cooking. Another study, which combined survey data from 18 different African countries (including data from Uganda), found that exposure to kerosene fuel for cooking and solid fuel for cooking were most strongly associated with acute lower respiratory infection; during the rainy season when cooking is more often performed indoors (Buchner and Rehfuess, 2015). Another study (Akunne et al., 2006), which assessed the attributable fraction of various cooking-related HAP interventions among children under 5 years old, found that, compared to improvements in cook stove technology or improved ventilation indoors only, cooking outdoors resulted in the largest reductions in the fraction of acute respiratory infections attributable to cooking with solid fuels. A HAP intervention trial conducted in South Africa (Barnes et al., 2017), which focused on community counseling on behavioral change such as keeping children outdoors during cooking or opening windows for ventilation as a means to mitigate HAP exposure among children, found that personal exposure measures for both CO and PM10 reduced significantly in the intervention community compared to the control community. Our analysis, as well as others, suggests factors that can mitigate against childhood exposure to HAP, such as cooking outdoors, opening windows for ventilation, and proximity of the child (outdoors versus indoors) to fuel combustion sources, represent potentially important points for intervention that could be easier and less costly to implement compared to cleaner cook stove technologies (Langbein et al., 2017).
We also found, compared to all other indoor cooking locations, cooking in the same area where household occupants slept resulted in the strongest adverse associations for cough, confirming that cooking in confined spaces may be especially hazardous (Bruce et al., 2004; Sharma and Jain, 2019). This finding is supported by another study conducted in sub-Saharan Africa, which found that cooking indoors, in a home without a designated kitchen during the rainy season, was significantly associated with higher acute lower respiratory infection compared to homes with a designated kitchen.
Other sources of HAP emissions, that are unrelated to cooking, were adversely associated with childhood cough. These included the type of energy source (kerosene or candles) used for lighting the home and having a household occupant that smoked tobacco indoors. Unfortunately, little is known about the respiratory health effects from household kerosene fuel-use (Acharya et al., 2017; Buchner and Rehfuess, 2015; Lam et al., 2012). To our knowledge, ours is the first epidemiological study conducted in sub-Saharan Africa to investigate associations between child respiratory health and kerosene used for lighting the home. Household air pollution monitoring studies conducted in Kenya and Uganda found that, among rural homes that cooked with solid fuels outdoors exclusively, lighting the home using a kerosene lantern was associated with PM2.5 levels that exceeded WHO air quality guidelines (Muindi et al., 2016; Muyanja et al., 2017). Acharya et al. found that using a kerosene lantern for lighting the home was associated with higher ALRI among young children in India (Acharya et al., 2017). In our study, 19% of cases and 10% of controls (13% overall) were exposed to kerosene for lighting the home, showing that kerosene for household lighting is not uncommon among Uganda’s urban poor. Although prevalence of indoor smoking was low overall for the study population (8%), it had the strongest association with cough among all sources of HAP.
With Bayesian cluster analysis we observed a strong clustering pattern of multiple HAP and SES indicators as well as combined effects between emission and exposure-mitigation factors on persistent cough. For households that had profiles with multiple HAP indoor sources yet lacked exposure-protective factors, such as cooking indoors without opening windows and the child being indoors during cooking, these households exhibited the highest prevalence of cough.
Conversely, households with high usage of HAP cooking sources (e.g., solid fuel or kerosene) but where cooking occurred outdoors, resulted in the lowest cough prevalence. Our cluster analysis further revealed that children from cluster 9 households, which tended to cook indoors with polluting fuels and unimproved stoves, had indoor tobacco smokers, had children indoors during cooking, and lacked or did not open windows during cooking, resulted in elevated cough prevalence (see cluster 9, Fig. 2b) compared to the reference cluster that also mostly cooked indoors with polluting fuels and unimproved stoves but tended to have their child outdoors during cooking, lacked indoor tobacco smokers, and were more likely to open windows during cooking. While the clusters with by far the highest cough prevalence (cluster 10 and 11) had similar profiles to cluster 9, the major differences between cluster 9 and the highest cough clusters was using a polluting fuel for lighting the home and higher indoor smoking prevalence (see Fig. 2b). These complex combined effects imply that HAP interventions with a strict focus on a single household factor, such as replacing a traditional cook stove with an improved cook stoves, may not have as substantial positive impact in terms of reducing HAP levels or related health burdens as would otherwise be expected. For instance, replacing a traditional stove with an improved stove among those who live in a neighborhood with already high levels of outdoor air pollution, who cook outdoors, and use kerosene for lighting the home, is unlikely to improve indoor air quality to health-protective levels. Our findings strongly suggest that more comprehensive HAP interventions need to be assessed—i.e. interventions that address multiple air pollution emissions sources (e.g., lighting and cooking fuels) and HAP exposure factors (e.g., cooking outdoors or using ventilation) in concert with improved cooking fuels and stove-types.
Importantly, our use of Bayesian profile regression (BPR) enabled these complex analyses of joint effects in spite of a relatively limited sample size, and represents a key innovation for health studies of HAP. Conventional regression analyses, used in most epidemiologic studies of HAP, are typically incapable of investigating effects beyond anything more than two-way interactions largely due to limited statistical power to explore such complex interaction effects. Cluster analysis using BPR, in contrast, enabled dimension reduction to a smaller number of features for regression analysis which then enabled us to explore combined effects of three or more HAP sources in addition to exposure-mitigating and SES factors together. A major drawback with BPR, however, is its relative inability to evaluate independent effects of any single risk factor compared to conventional regression techniques. In addition, BPR in general does not incorporate a formal statistical test for synergistic or antagonistic effects. Despite such limitations, future HAP epidemiology studies could use BPR (or an analogous clustering approach) in combination with conventional regression techniques in order to assess independent and joint effects of multiple HAP sources as well as exposure mitigation factors and SES indicators. In addition to use of BPR in formal epidemiology studies, BPR can also be applied in HAP area or personal exposure assessment studies that objectively measure indoor air pollution concentrations to help elucidate the combination of household emissions and time-activity patterns that explain variations in HAP levels.
Another strength of our analysis was to explicitly incorporate SES indicators into the BPR cluster analysis, in order to determine if low SES tended to cluster together with high levels of HAP adversity. While this was shown to be mostly true, we did observe some exceptions. For instance, cluster 2 was a very low SES grouping of households, however, these households were characterized as having multiple protective HAP exposure factors as well as very low cough prevalence. In other words, there is evidence from our data to show that cough prevalence differed significantly among similarly low SES households but that differed mostly in terms of HAP indicators. This finding suggests that SES is unlikely to fully account for the observed differences in our outcome of interest.
There are a number of limitations to our study. One major limitation is that we assessed only the primary source of fuel or type of stove used for cooking instead of assessing the possibility of secondary or tertiary household cooking emission sources. Since it is well-established that stove-stacking for cooking is commonplace in less-developed regions, our study is limited in that we did not assess the totality of household cooking emission sources. In addition, we did not assess neighbor’s use of solid fuels which may further impact HAP levels. Our assessment of ventilation when cooking indoors was also limited because we only assessed opening of windows during cooking. There are a number of other ventilation factors that could have been assessed via the questionnaire, such as opening of doors during cooking or the number of windows kept open during cooking. We also relied on self-reported indicators of HAP rather than objective air monitoring measurements. Such indirect measures of exposure based on parental report may introduce non-differential bias because they are less accurate than direct measures, reducing statistical power and leading to false-negative associations, or Type II error. Second, in the context of the case-control study design, indirect measures of exposure based on parental reports may also lead to differential bias toward an association with cough, because of recall bias, thereby leading to false-positive associations. For example, self-report of traffic-related air pollution, while validated in more developed countries, has not been validated in sub-Saharan Africa and is an example of a self-report indicator susceptible to recall bias. Secondarily to recall bias, we conducted a case-control study at an outpatient primary health care facility, which has the potential to induce selection bias (Wacholder et al., 1992). While acknowledging this limitation, selection of controls from the same study clinic as cases suggests that cases and controls were derived from similar if not the same source population (i.e. KCCA clinics serve the surrounding general population seeking outpatient services), which is likely to limit selection bias. In addition, the most common conditions/reasons for seeking care at these outpatient clinics include acute conditions such as malaria and cold/flu symptoms. Such outpatient clinics do not typically manage complex medical conditions. Given that outpatient clinics receive fairly uncomplicated medical (mostly acute) conditions, and that the population is quite homogenous, the risk of selection bias—though still present—should be mitigated by these factors.. Matching on age and time was also conducted to further reduce confounding bias by age or seasonality, or differences in the population based on the reasons for the outpatient visit. External validity, or generalizability, is another potential limitation of our study. To mitigate this limitation, we drew our study sample from three different KCCA health facilities and recruited a large number of participants from each facility (N>350 from each health facility) (Carlson and Morrison, 2009). Nevertheless, the replication of our findings in a different study population would certainly lend support to the generalizability of our findings. Future prospective cohort studies are therefore needed that look at associations between indoor HAP concentrations, exposure-mitigation factors, and relevant health outcomes, with exposure variables measured both objectively and by self-report at baseline. Such an approach, especially when analyzed using a multivariable framework as done here, could potentially aid in the development of more comprehensive and effective HAP interventions.
As already noted, the major innovation of our study is the multivariable analysis of multiple HAP indicators assessed via a study questionnaire. To reiterate, a strict consideration of only one source of HAP, such as cooking fuel, overlooks the combination of HAP emission sources and behavioral, household, and neighborhood factors that can mitigate exposure or intensify HAP exposure. A multivariable analytic approach can help reveal the combination of interventions that can be tailored to specific households or communities to reduce exposure to HAP and its adverse health effects. Another important strength of our study is our focus on an urban low-income population. The dramatic growth of urban populations in developing countries—where over 90% of urban growth is occurring (World Bank, 2016)—represents an emerging public health challenge, and the health effects from exposure to HAP among sub-Saharan Africa’s urban poor is not well understood. Our study reveals the diverse and complex ways in which HAP emission sources and exposure-mitigating factors manifest among the urban poor of Kampala. We recommend that such multivariable data be used in future epidemiology studies to help inform HAP interventions in the urban developing country context.
CONCLUSIONS
Several HAP emissions sources, beyond simply cooking fuel-type or stove-type, were strongly associated with persistent cough in children. These included using kerosene as a household source of lighting as well as having a household occupant who smokes indoors. In addition to multiple HAP emission sources, factors capable of mitigating childhood exposure to HAP, such as cooking outdoors versus indoors, opening windows for ventilation, and proximity of children to cooking emission sources, all exhibited strong associations with persistent cough. Such exposure-mitigating factors represent practical intervention that, when combined together, hold the potential to reduce HAP exposure in children. Moreover, cluster analysis using Bayesian profile regression revealed large joint effects from multiple HAP emission sources and exposure-mitigating factors on childhood cough. In order to provide epidemiological data that maximizes the public health benefits from HAP interventions in low-income countries of sub-Saharan Africa, longitudinal HAP epidemiology research should better elucidate the effects of multiple household emissions sources and exposure-mitigating factors in combination, rather than focusing on any single factor such as the cooking emissions source alone.
Supplementary Material
HIGHLIGHTS.
Multiple correlated HAP indicators were jointly associated with childhood cough
Exposure to cooking with solid fuels outdoors was associated with lower cough
Exposure to kerosene used for cooking or lighting was associated with higher cough
Strong clustering of multiple HAP indicators at the household level was observed
HAP interventions should address exposure factors and emission sources jointly
ACKNOWLEDGMENTS:
Special thanks go to those who assisted in this study, including the Community Health Workers (Ms. Leah Nanziri, Ms. Agnes Sanyu and Ms. Catherine Nakafeero), research and medical staff within the Uganda TB Implementation Research Consortium and Kampala Capital City Authority health centers, and the many study participants and their children.
Funding: This study was supported by the Global Health Equity Scholars Program, Fogarty NIH TW009338 along with support from the Health Resources and Services Administration, Maternal and Child Health Bureau (Award ID: T76MC00002).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declarations of competing financial interests: Authors report no competing financial interests.
REFERENCES
- Acharya N, Mishra P, Gupta V, 2017. Indoor Air Pollution as a Risk Factor of Acute Lower Respiratory Tract Infection in Children. Journal of Nepalgunj Medical College 13, 5–7. 10.3126/jngmc.v13i1.16398 [DOI] [Google Scholar]
- Akunne AF, Louis VR, Sanon M, Sauerborn R, 2006. Biomass solid fuel and acute respiratory infections: The ventilation factor. International Journal of Hygiene and Environmental Health 209, 445–450. 10.1016/j.ijheh.2006.04.009 [DOI] [PubMed] [Google Scholar]
- Barnes B, Mathee A, Thomas E, 2017. The impact of health behaviour change intervention on indoor air pollution indicators in the rural North West Province, South Africa. J. energy South. Afr 22, 35–44. 10.17159/2413-3051/2011/v22i3a3220 [DOI] [Google Scholar]
- Bruce N, McCracken J, Albalak R, Scheid M, Smith KR, Lopez V, West C, 2004. Impact of improved stoves, house construction and child location on levels of indoor air pollution exposure in young Guatemalan children. Journal Of Exposure Analysis And Environmental Epidemiology 14, S26. [DOI] [PubMed] [Google Scholar]
- Bruce N, Pope D, Rehfuess E, Balakrishnan K, Adair-Rohani H, Dora C, 2015. WHO indoor air quality guidelines on household fuel combustion: Strategy implications of new evidence on interventions and exposure—risk functions. Atmospheric Environment 106, 451–457. 10.1016/j.atmosenv.2014.08.064 [DOI] [Google Scholar]
- Buchner H, Rehfuess EA, 2015. Cooking and Season as Risk Factors for Acute Lower Respiratory Infections in African Children: A Cross-Sectional Multi-Country Analysis. PLOS ONE 10, e0128933. 10.1371/journal.pone.0128933 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burgette LF, Reiter JP, 2010. Multiple Imputation for Missing Data via Sequential Regression Trees. American Journal of Epidemiology 172, 1070–1076. 10.1093/aje/kwq260 [DOI] [PubMed] [Google Scholar]
- Carlson MDA, Morrison RS, 2009. Study design, precision, and validity in observational studies. J Palliat Med 12, 77–82. 10.1089/jpm.2008.9690 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark ML, Peel JL, Balakrishnan K, Breysse PN, Chillrud SN, Naeher LP, Rodes CE, Vette AF, Balbus JM, 2013. Health and Household Air Pollution from Solid Fuel Use: The Need for Improved Exposure Assessment. Environmental Health Perspectives 121, 1120–1128. 10.1289/ehp.1206429 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coker E, Gunier R, Bradman A, Harley K, Kogut K, Molitor J, Eskenazi B, 2017. Association between Pesticide Profiles Used on Agricultural Fields near Maternal Residences during Pregnancy and IQ at Age 7 Years. International Journal of Environmental Research and Public Health 14, 506. 10.3390/ijerph14050506 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coker E, Liverani S, Ghosh JK, Jerrett M, Beckerman B, Li A, Ritz B, Molitor J, 2016. Multipollutant exposure profiles associated with term low birth weight in Los Angeles County. Environment International 91, 1–13. 10.1016/j.envint.2016.02.011 [DOI] [PubMed] [Google Scholar]
- Das I, Pedit J, Handa S, Jagger P, 2018. Household air pollution (HAP), microenvironment and child health: Strategies for mitigating HAP exposure in urban Rwanda. Environmental Research Letters 13, 045011. 10.1088/1748-9326/aab047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Health Effects Institute, 2018. State of Global Air 2018. Special Report. Health Effects Institute, Boston, MA. [Google Scholar]
- Ishwaran H, Rao JS, 2005. Spike and slab variable selection: Frequentist and Bayesian strategies. The Annals of Statistics 33, 730–773. 10.1214/009053604000001147 [DOI] [Google Scholar]
- Jo E-J, Song W-J, 2019. Environmental triggers for chronic cough. Asia Pac Allergy 9, e16. 10.5415/apallergy.2019.9.e16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- KCCA, 2017. KCCA Ministerial Policy Statement for Financial Year 2017/18. Kampala, Uganda. [Google Scholar]
- Kizito S, Katamba A, Marquez C, Turimumahoro P, Ayakaka I, Davis JL, Cattamanchi A, 2018. Quality of care in childhood tuberculosis diagnosis at primary care clinics in Kampala, Uganda. The International Journal of Tuberculosis and Lung Disease 22, 1196–1202. 10.5588/ijtld.18.0043 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lam NL, Smith KR, Gauthier A, Bates MN, 2012. Kerosene: A Review of Household Uses and their Hazards in Low- and Middle-Income Countries. Journal of Toxicology and Environmental Health, Part B 15, 396–432. 10.1080/10937404.2012.710134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Langbein J, Peters J, Vance C, 2017. Outdoor cooking prevalence in developing countries and its implication for clean cooking policies. Environ. Res. Lett 12, 115008. 10.1088/1748-9326/aa8642 [DOI] [Google Scholar]
- Li Z, Commodore A, Hartinger S, Lewin M, Sjödin A, Pittman E, Trinidad D, Hubbard K, Lanata CF, Gil AI, Mäusezahl D, Naeher LP, 2016. Biomonitoring Human Exposure to Household Air Pollution and Association with Self-reported Health Symptoms – A Stove Intervention Study in Peru. Environment International 97, 195–203. 10.1016/j.envint.2016.09.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liverani S, Hastie D, Azizi L, Papathomas M, Richardson S, 2015. PReMiuM: An R Package for Profile Regression Mixture Models Using Dirichlet Processes 64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liverani S, Lavigne A, Blangiardo M, 2016. Modelling collinear and spatially correlated data. Spatial and Spatio-temporal Epidemiology 18, 63–73. 10.1016/j.sste.2016.04.003 [DOI] [PubMed] [Google Scholar]
- Malsiner-Walli G, Wagner H, 2018. Comparing Spike and Slab Priors for Bayesian Variable Selection. arXiv:1812.07259 [stat]. [Google Scholar]
- Molitor J, Papathomas M, Jerrett M, Richardson S, 2010. Bayesian profile regression with an application to the National survey of children’s health. Biostatistics 11, 484–498. 10.1093/biostatistics/kxq013 [DOI] [PubMed] [Google Scholar]
- Morice AH, 2004. The diagnosis and management of chronic cough. European Respiratory Journal 24, 481–492. 10.1183/09031936.04.00027804 [DOI] [PubMed] [Google Scholar]
- Mortimer K, Ndamala CB, Naunje AW, Malava J, Katundu C, Weston W, Havens D, Pope D, Bruce NG, Nyirenda M, Wang D, Crampin A, Grigg J, Balmes J, Gordon SB, 2017. A cleaner burning biomass-fuelled cookstove intervention to prevent pneumonia in children under 5 years old in rural Malawi (the Cooking and Pneumonia Study): a cluster randomised controlled trial. The Lancet 389, 167–175. 10.1016/S0140-6736(16)32507-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muindi K, Kimani-Murage E, Egondi T, Rocklov J, Ng N, 2016. Household Air Pollution: Sources and Exposure Levels to Fine Particulate Matter in Nairobi Slums. Toxics 4, 12. 10.3390/toxics4030012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mustapha BA, Blangiardo M, Briggs DJ, Hansell AL, 2011. Traffic Air Pollution and Other Risk Factors for Respiratory Illness in Schoolchildren in the Niger-Delta Region of Nigeria. Environmental Health Perspectives 119, 1478–1482. 10.1289/ehp.1003099 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muyanja D, Allen JG, Vallarino J, Valeri L, Kakuhikire B, Bangsberg DR, Christiani DC, Tsai AC, Lai PS, 2017. Kerosene lighting contributes to household air pollution in rural Uganda. Indoor Air 27, 1022–1029. 10.1111/ina.12377 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piro FN, Madsen C, Næss Ø, Nafstad P, Claussen B, 2008. A comparison of self reported air pollution problems and GIS-modeled levels of air pollution in people with and without chronic diseases. Environmental Health 7. 10.1186/1476-069X-7-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pope D, Bruce N, Dherani M, Jagoe K, Rehfuess E, 2017. Real-life effectiveness of ‘improved’ stoves and clean fuels in reducing PM 2.5 and CO: Systematic review and meta-analysis. Environment International 101, 7–18. 10.1016/j.envint.2017.01.012 [DOI] [PubMed] [Google Scholar]
- Quansah R, Semple S, Ochieng CA, Juvekar S, Armah FA, Luginaah I, Emina J, 2017. Effectiveness of interventions to reduce household air pollution and/or improve health in homes using solid fuel in low-and-middle income countries: A systematic review and meta-analysis. Environment International 103, 73–90. 10.1016/j.envint.2017.03.010 [DOI] [PubMed] [Google Scholar]
- Rehfuess EA, Best N, Briggs DJ, Joffe M, 2013. Diagram-based Analysis of Causal Systems (DACS): elucidating inter-relationships between determinants of acute lower respiratory infections among children in sub-Saharan Africa. Emerging Themes in Epidemiology 10, 13. 10.1186/1742-7622-10-13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Safdar DMT, 2016. SYSTEMS THINKING FOR IMPROVED COOKSTOVE DISSEMINATION 12. [Google Scholar]
- Scott JG, Berger JO, 2010. Bayes and empirical-Bayes multiplicity adjustment in the variable-selection problem. The Annals of Statistics 38, 2587–2619. 10.1214/10-AOS792 [DOI] [Google Scholar]
- Sharma D, Jain S, 2019. Impact of intervention of biomass cookstove technologies and kitchen characteristics on indoor air quality and human exposure in rural settings of India. Environment International 123, 240–255. 10.1016/j.envint.2018.11.059 [DOI] [PubMed] [Google Scholar]
- Shields MD, Thavagnanam S, 2013. The difficult coughing child: prolonged acute cough in children. Cough 9, 11. 10.1186/1745-9974-9-11 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanaway JD, Afshin A, Gakidou E, Lim SS, Abate D, Abate KH, Abbafati C, Abbasi N, Abbastabar H, Abd-Allah F, Abdela J, Abdelalim A, Abdollahpour I, Abdulkader RS, Abebe M, Abebe Z, Abera SF, Abil OZ, Abraha HN, Abrham AR, Abu-Raddad LJ, Abu-Rmeileh NM, Accrombessi MMK, Acharya D, Acharya P, Adamu AA, Adane AA, Adebayo OM, Adedoyin RA, Adekanmbi V, Ademi Z, Adetokunboh OO, Adib MG, Admasie A, Adsuar JC, Afanvi KA, Afarideh M, Agarwal G, Aggarwal A, Aghayan SA, Agrawal A, Agrawal S, Ahmadi A, Ahmadi M, Ahmadieh H, Ahmed MB, Aichour AN, Aichour I, Aichour MTE, Akbari ME, Akinyemiju T, Akseer N, Al-Aly Z, Al-Eyadhy A, Al-Mekhlafi HM, Alahdab F, Alam K, Alam S, Alam T, Alashi A, Alavian SM, Alene KA, Ali K, Ali SM, Alijanzadeh M, Alizadeh-Navaei R, Aljunid SM, Alkerwi A, Alla F, Alsharif U, Altirkawi K, Alvis-Guzman N, Amare AT, Ammar W, Anber NH, Anderson JA, Andrei CL, Androudi S, Animut MD, Anjomshoa M, Ansha MG, Antó JM, Antonio CAT, Anwari P, Appiah LT, Appiah SCY, Arabloo J, Aremu O, Ärnlöv J, Artaman A, Aryal KK, Asayesh H, Ataro Z, Ausloos M, Avokpaho EFGA, Awasthi A, Ayala Quintanilla BP, Ayer R, Ayuk TB, Azzopardi PS, Babazadeh A, Badali H, Badawi A, Balakrishnan K, Bali AG, Ball K, Ballew SH, Banach M, Banoub JAM, Barac A, Barker-Collo SL, Bärnighausen TW, Barrero LH, Basu S, Baune BT, Bazargan-Hejazi S, Bedi N, Beghi E, Behzadifar, Masoud, Behzadifar, Meysam, Béjot Y, Bekele BB, Bekru ET, Belay E, Belay YA, Bell ML, Bello AK, Bennett DA, Bensenor IM, Bergeron G, Berhane A, Bernabe E, Bernstein RS, Beuran M, Beyranvand T, Bhala N, Bhalla A, Bhattarai S, Bhutta ZA, Biadgo B, Bijani A, Bikbov B, Bilano V, Bililign N, Bin Sayeed MS, Bisanzio D, Biswas T, Bjørge T, Blacker BF, Bleyer A, Borschmann R, Bou-Orm IR, Boufous S, Bourne R, Brady OJ, Brauer M, Brazinova A, Breitborde NJK, Brenner H, Briko AN, Britton G, Brugha T, Buchbinder R, Burnett RT, Busse R, Butt ZA, Cahill LE, Cahuana-Hurtado L, Campos-Nonato IR, Cárdenas R, Carreras G, Carrero JJ, Carvalho F, Castañeda-Orjuela CA, Castillo Rivas J, Castro F, Catalá-López F, Causey K, Cercy KM, Cerin E, Chaiah Y, Chang H-Y, Chang J-C, Chang K-L, Charlson FJ, Chattopadhyay A, Chattu VK, Chee ML, Cheng C-Y, Chew A, Chiang PP-C, Chimed-Ochir O, Chin KL, Chitheer A, Choi J-YJ, Chowdhury R, Christensen H, Christopher DJ, Chung S-C, Cicuttini FM, Cirillo M, Cohen AJ, Collado-Mateo D, Cooper C, Cooper OR, Coresh J, Cornaby L, Cortesi PA, Cortinovis M, Costa M, Cousin E, Criqui MH, Cromwell EA, Cundiff DK, Daba AK, Dachew BA, Dadi AF, Damasceno AAM, Dandona L, Dandona R, Darby SC, Dargan PI, Daryani A, Das Gupta R, Das Neves J, Dasa TT, Dash AP, Davitoiu DV, Davletov K, De la Cruz-Góngora V, De La Hoz FP, De Leo D, De Neve J-W, Degenhardt L, Deiparine S, Dellavalle RP, Demoz GT, Denova-Gutiérrez E, Deribe K, Dervenis N, Deshpande A, Des Jarlais DC, Dessie GA, Deveber GA, Dey S, Dharmaratne SD, Dhimal M, Dinberu MT, Ding EL, Diro HD, Djalalinia S, Do HP, Dokova K, Doku DT, Doyle KE, Driscoll TR, Dubey M, Dubljanin E, Duken EE, Duncan BB, Duraes AR, Ebert N, Ebrahimi H, Ebrahimpour S, Edvardsson D, Effiong A, Eggen AE, El Bcheraoui C, El-Khatib Z, Elyazar IR, Enayati A, Endries AY, Er B, Erskine HE, Eskandarieh S, Esteghamati A, Estep K, Fakhim H, Faramarzi M, Fareed M, Farid TA, Farinha C.S.E. sá, Farioli A, Faro A, Farvid MS, Farzaei MH, Fatima B, Fay KA, Fazaeli AA, Feigin VL, Feigl AB, Fereshtehnejad S-M, Fernandes E, Fernandes JC, Ferrara G, Ferrari AJ, Ferreira ML, Filip I, Finger JD, Fischer F, Foigt NA, Foreman KJ, Fukumoto T, Fullman N, Fürst T, Furtado JM, Futran ND, Gall S, Gallus S, Gamkrelidze A, Ganji M, Garcia-Basteiro AL, Gardner WM, Gebre AK, Gebremedhin AT, Gebremichael TG, Gelano TF, Geleijnse JM, Geramo YCD, Gething PW, Gezae KE, Ghadimi R, Ghadiri K, Ghasemi Falavarjani K, Ghasemi-Kasman M, Ghimire M, Ghosh R, Ghoshal AG, Giampaoli S, Gill PS, Gill TK, Gillum RF, Ginawi IA, Giussani G, Gnedovskaya EV, Godwin WW, Goli S, Gómez-Dantés H, Gona PN, Gopalani SV, Goulart AC, Grada A, Grams ME, Grosso G, Gugnani HC, Guo Y, Gupta, Rahul, Gupta, Rajeev, Gupta T, Gutiérrez RA, Gutiérrez-Torres DS, Haagsma JA, Habtewold TD, Hachinski V, Hafezi-Nejad N, Hagos TB, Hailegiyorgis TT, Hailu GB, Haj-Mirzaian, Arvin, Haj-Mirzaian, Arya, Hamadeh RR, Hamidi S, Handal AJ, Hankey GJ, Hao Y, Harb HL, Harikrishnan S, Haro JM, Hassankhani H, Hassen HY, Havmoeller R, Hawley CN, Hay SI, Hedayatizadeh-Omran A, Heibati B, Heidari B, Heidari M, Hendrie D, Henok A, Heredia-Pi I, Herteliu C, Heydarpour F, Heydarpour S, Hibstu DT, Higazi TB, Hilawe EH, Hoek HW, Hoffman HJ, Hole MK, Homaie Rad E, Hoogar P, Hosgood HD, Hosseini SM, Hosseinzadeh M, Hostiuc M, Hostiuc S, Hoy DG, Hsairi M, Hsiao T, Hu G, Hu H, Huang JJ, Hussen MA, Huynh CK, Iburg KM, Ikeda N, Ilesanmi OS, Iqbal U, Irvani SSN, Irvine CMS, Islam SMS, Islami F, Jackson MD, Jacobsen KH, Jahangiry L, Jahanmehr N, Jain SK, Jakovljevic M, James SL, Jassal SK, Jayatilleke AU, Jeemon P, Jha RP, Jha V, Ji JS, Jonas JB, Jonnagaddala J, Jorjoran Shushtari Z, Joshi A, Jozwiak JJ, Jürisson M, Kabir Z, Kahsay A, Kalani R, Kanchan T, Kant S, Kar C, Karami M, Karami Matin B, Karch A, Karema C, Karimi N, Karimi SM, Kasaeian A, Kassa DH, Kassa GM, Kassa TD, Kassebaum NJ, Katikireddi SV, Kaul A, Kawakami N, Kazemi Z, Karyani AK, Kefale AT, Keiyoro PN, Kemp GR, Kengne AP, Keren A, Kesavachandran CN, Khader YS, Khafaei B, Khafaie MA, Khajavi A, Khalid N, Khalil IA, Khan G, Khan MS, Khan MA, Khang Y-H, Khater MM, Khazaei M, Khazaie H, Khoja AT, Khosravi A, Khosravi MH, Kiadaliri AA, Kiirithio DN, Kim C-I, Kim D, Kim Y-E, Kim YJ, Kimokoti RW, Kinfu Y, Kisa A, Kissimova-Skarbek K, Kivimäki M, Knibbs LD, Knudsen AKS, Kochhar S, Kokubo Y, Kolola T, Kopec JA, Kosen S, Koul PA, Koyanagi A, Kravchenko MA, Krishan K, Krohn KJ, Kromhout H, Kuate Defo B, Kucuk Bicer B, Kumar GA, Kumar M, Kuzin I, Kyu HH, Lachat C, Lad DP, Lad SD, Lafranconi A, Lalloo R, Lallukka T, Lami FH, Lang JJ, Lansingh VC, Larson SL, Latifi A, Lazarus JV, Lee PH, Leigh J, Leili M, Leshargie CT, Leung J, Levi M, Lewycka S, Li S, Li Y, Liang J, Liang X, Liao Y, Liben ML, Lim L-L, Linn S, Liu S, Lodha R, Logroscino G, Lopez AD, Lorkowski S, Lotufo PA, Lozano R, Lucas TCD, Lunevicius R, Ma S, Macarayan ERK, Machado ÍE, Madotto F, Mai HT, Majdan M, Majdzadeh R, Majeed A, Malekzadeh R, Malta DC, Mamun AA, Manda A-L, Manguerra H, Mansournia MA, Mantovani LG, Maravilla JC, Marcenes W, Marks A, Martin RV, Martins SCO, Martins-Melo FR, März W, Marzan MB, Massenburg BB, Mathur MR, Mathur P, Matsushita K, Maulik PK, Mazidi M, McAlinden C, McGrath JJ, McKee M, Mehrotra R, Mehta KM, Mehta V, Meier T, Mekonnen FA, Melaku YA, Melese A, Melku M, Memiah PTN, Memish ZA, Mendoza W, Mengistu DT, Mensah GA, Mensink GBM, Mereta ST, Meretoja A, Meretoja TJ, Mestrovic T, Mezgebe HB, Miazgowski B, Miazgowski T, Millear AI, Miller TR, Miller-Petrie MK, Mini GK, Mirarefin M, Mirica A, Mirrakhimov EM, Misganaw AT, Mitiku H, Moazen B, Mohajer B, Mohammad KA, Mohammadi M, Mohammadifard N, Mohammadnia-Afrouzi M, Mohammed S, Mohebi F, Mokdad AH, Molokhia M, Momeniha F, Monasta L, Moodley Y, Moradi G, Moradi-Lakeh M, Moradinazar M, Moraga P, Morawska L, Morgado-Da-Costa J, Morrison SD, Moschos MM, Mouodi S, Mousavi SM, Mozaffarian D, Mruts KB, Muche AA, Muchie KF, Mueller UO, Muhammed OS, Mukhopadhyay S, Muller K, Musa KI, Mustafa G, Nabhan AF, Naghavi M, Naheed A, Nahvijou A, Naik G, Naik N, Najafi F, Nangia V, Nansseu JR, Nascimento BR, Neal B, Neamati N, Negoi I, Negoi RI, Neupane S, Newton CRJ, Ngunjiri JW, Nguyen AQ, Nguyen G, Nguyen, Ha Thu, Nguyen HLT, Nguyen, Huong Thanh, Nguyen M, Nguyen NB, Nichols E, Nie J, Ningrum DNA, Nirayo YL, Nishi N, Nixon MR, Nojomi M, Nomura S, Norheim OF, Noroozi M, Norrving B, Noubiap JJ, Nouri HR, Nourollahpour Shiadeh M, Nowroozi MR, Nsoesie EO, Nyasulu PS, Obermeyer CM, Odell CM, Ofori-Asenso R, Ogbo FA, Oh I-H, Oladimeji O, Olagunju AT, Olagunju TO, Olivares PR, Olsen HE, Olusanya BO, Olusanya JO, Ong KL, Ong SK, Oren E, Orpana HM, Ortiz A, Ota E, Otstavnov SS, Øverland S, Owolabi MO, P A M, Pacella R, Pakhare AP, Pakpour AH, Pana A, Panda-Jonas S, Park E-K, Parry CDH, Parsian H, Patel S, Pati S, Patil ST, Patle A, Patton GC, Paudel D, Paulson KR, Paz Ballesteros WC, Pearce N, Pereira A, Pereira DM, Perico N, Pesudovs K, Petzold M, Pham HQ, Phillips MR, Pillay JD, Piradov MA, Pirsaheb M, Pischon T, Pishgar F, Plana-Ripoll O, Plass D, Polinder S, Polkinghorne KR, Postma MJ, Poulton R, Pourshams A, Poustchi H, Prabhakaran D, Prakash S, Prasad N, Purcell CA, Purwar MB, Qorbani M, Radfar A, Rafay A, Rafiei A, Rahim F, Rahimi Z, Rahimi-Movaghar A, Rahimi-Movaghar V, Rahman M, Rahman M.H. ur, Rahman MA, Rai RK, Rajati F, Rajsic S, Raju SB, Ram U, Ranabhat CL, Ranjan P, Rath GK, Rawaf DL, Rawaf S, Reddy KS, Rehm CD, Rehm J, Reiner RC, Reitsma MB, Remuzzi G, Renzaho AMN, Resnikoff S, Reynales-Shigematsu LM, Rezaei S, Ribeiro ALP, Rivera JA, Roba KT, Rodríguez-Ramírez S, Roever L, Román Y, Ronfani L, Roshandel G, Rostami A, Roth GA, Rothenbacher D, Roy A, Rubagotti E, Rushton L, Sabanayagam C, Sachdev PS, Saddik B, Sadeghi E, Saeedi Moghaddam S, Safari H, Safari Y, Safari-Faramani R, Safdarian M, Safi S, Safiri S, Sagar R, Sahebkar A, Sahraian MA, Sajadi HS, Salam N, Salamati P, Saleem Z, Salimi Y, Salimzadeh H, Salomon JA, Salvi DD, Salz I, Samy AM, Sanabria J, Sanchez-Niño MD, Sánchez-Pimienta TG, Sanders T, Sang Y, Santomauro DF, Santos IS, Santos JV, Santric Milicevic MM, Sao Jose BP, Sardana M, Sarker AR, Sarmiento-Suárez R, Sarrafzadegan N, Sartorius B, Sarvi S, Sathian B, Satpathy M, Sawant AR, Sawhney M, Saylan M, Sayyah M, Schaeffner E, Schmidt MI, Schneider IJC, Schöttker B, Schutte AE, Schwebel DC, Schwendicke F, Scott JG, Seedat S, Sekerija M, Sepanlou SG, Serre ML, Serván-Mori E, Seyedmousavi S, Shabaninejad H, Shaddick G, Shafieesabet A, Shahbazi M, Shaheen AA, Shaikh MA, Shamah Levy T, Shams-Beyranvand M, Shamsi M, Sharafi H, Sharafi K, Sharif M, Sharif-Alhoseini M, Sharifi H, Sharma J, Sharma M, Sharma R, She J, Sheikh A, Shi P, Shibuya K, Shiferaw MS, Shigematsu M, Shin M-J, Shiri R, Shirkoohi R, Shiue I, Shokraneh F, Shoman H, Shrime MG, Shupler MS, Si S, Siabani S, Sibai AM, Siddiqi TJ, Sigfusdottir ID, Sigurvinsdottir R, Silva DAS, Silva JP, Silveira DGA, Singh JA, Singh NP, Singh V, Sinha DN, Skiadaresi E, Skirbekk V, Smith DL, Smith M, Sobaih BH, Sobhani S, Somayaji R, Soofi M, Sorensen RJD, Soriano JB, Soyiri IN, Spinelli A, Sposato LA, Sreeramareddy CT, Srinivasan V, Starodubov VI, Steckling N, Stein DJ, Stein MB, Stevanovic G, Stockfelt L, Stokes MA, Sturua L, Subart ML, Sudaryanto A, Sufiyan MB, Sulo G, Sunguya BF, Sur PJ, Sykes BL, Szoeke CEI, Tabarés-Seisdedos R, Tabuchi T, Tadakamadla SK, Takahashi K, Tandon N, Tassew SG, Tavakkoli M, Taveira N, Tehrani-Banihashemi A, Tekalign TG, Tekelemedhin SW, Tekle MG, Temesgen H, Temsah M-H, Temsah O, Terkawi AS, Tessema B, Teweldemedhin M, Thankappan KR, Theis A, Thirunavukkarasu S, Thomas HJ, Thomas ML, Thomas N, Thurston GD, Tilahun B, Tillmann T, To QG, Tobollik M, Tonelli M, Topor-Madry R, Torre AE, Tortajada-Girbés M, Touvier M, Tovani-Palone MR, Towbin JA, Tran BX, Tran KB, Truelsen TC, Truong NT, Tsadik AG, Tudor Car L, Tuzcu EM, Tymeson HD, Tyrovolas S, Ukwaja KN, Ullah I, Updike RL, Usman MS, Uthman OA, Vaduganathan M, Vaezi A, Valdez PR, Van Donkelaar A, Varavikova E, Varughese S, Vasankari TJ, Venkateswaran V, Venketasubramanian N, Villafaina S, Violante FS, Vladimirov SK, Vlassov V, Vollset SE, Vos T, Vosoughi K, Vu GT, Vujcic IS, Wagnew FS, Waheed Y, Waller SG, Walson JL, Wang, Yafeng, Wang, Yanping, Wang Y-P, Weiderpass E, Weintraub RG, Weldegebreal F, Werdecker A, Werkneh AA, West JJ, Westerman R, Whiteford HA, Widecka J,Wijeratne T, Winkler AS, Wiyeh AB, Wiysonge CS, Wolfe CDA, Wong TY, Wu S, Xavier D, Xu G, Yadgir S, Yadollahpour A, Yahyazadeh Jabbari SH, Yamada T, Yan LL, Yano Y, Yaseri M, Yasin YJ, Yeshaneh A, Yimer EM, Yip P, Yisma E, Yonemoto N, Yoon S-J, Yotebieng M, Younis MZ, Yousefifard M, Yu C, Zaidi Z, Zaman SB, Zamani M, Zavala-Arciniega L, Zhang AL, Zhang H, Zhang K, Zhou M, Zimsen SRM, Zodpey S, Murray CJL, 2018. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet 392, 1923–1994. 10.1016/S0140-6736(18)32225-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thomas E, Wickramasinghe K, Mendis S, Roberts N, Foster C, 2015. Improved stove interventions to reduce household air pollution in low and middle income countries: a descriptive systematic review. BMC Public Health 15. 10.1186/s12889-015-2024-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- UBOS, 2017. The National Population and Housing Census 2014 - National Analytic Report. Uganda Bureau of Statistics, Kampala, Uganda. [Google Scholar]
- Wacholder S, McLaughlin JK, Silverman DT, Mandel JS, 1992. Selection of controls in case-control studies. I. Principles. Am. J. Epidemiol 135, 1019–1028. [DOI] [PubMed] [Google Scholar]
- Wang C, Xu J, Yang L, Xu Y, Zhang Xiangyan, Bai C, Kang J, Ran P, Shen H, Wen F, Huang K, Yao W, Sun T, Shan G, Yang T, Lin Y, Wu S, Zhu J, Wang R, Shi Z, Zhao J, Ye X, Song Y, Wang Q, Zhou Y, Ding L, Yang T, Chen Y, Guo Y, Xiao F, Lu Y, Peng X, Zhang B, Xiao F, Chen C-S, Wang Z, Zhang H, Bu X, Zhang Xiaolei, An L, Zhang S, Cao Z, Zhan Q, Yang Y, Cao B, Dai H, Liang L, He J, 2018. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. The Lancet 391, 1706–1717. 10.1016/S0140-6736(18)30841-9 [DOI] [PubMed] [Google Scholar]
- WHO, 2002. World Healht Survey 2002: B - Individual Questionnaire. World Health Organization. [Google Scholar]
- World Bank, 2016. Urban Poverty and Slum Upgrading - Urban Poverty: An Overview [WWW Document], URL http://web.worldbank.org/WBSITE/EXTERNAL/TOPICS/EXTURBANDEVELOPMENT/EXTURBANPOVERTY/0,,contentMDK:20227679~menuPK:7173704~pagePK:148956~piPK:216618~theSitePK:341325,00.html (accessed 4.11.19).
- Worrall G, 2011. Acute cough in children. Canadian Family Physician 57, 315–8. [PMC free article] [PubMed] [Google Scholar]
- Yip F, Christensen B, Sircar K, Naeher L, Bruce N, Pennise D, Lozier M, Pilishvili T, Loo Farrar J, Stanistreet D, Nyagol R, Muoki J, de Beer L, Sage M, Kapil V, 2017. Assessment of traditional and improved stove use on household air pollution and personal exposures in rural western Kenya. Environment International 99, 185–191. 10.1016/j.envint.2016.ll.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Young BN, Clark ML, Rajkumar S, Benka-Coker ML, Bachand A, Brook RD, Nelson TL, Volckens J, Reynolds SJ, L’Orange C, Good N, Koehler K, Africano S, Osorto Pinel AB, Peel JL, 2019. Exposure to household air pollution from biomass cookstoves and blood pressure among women in rural Honduras: A cross-sectional study. Indoor Air 29, 130–142. 10.1111/ina.12507 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.